New Drugs for Old Bugs
40
Session on Pneumonia Management Strategies: Hype or Real? Topic: New Drugs for Old Bugs? Through a CME Grant sponsored by
Transcript of New Drugs for Old Bugs

Session on Pneumonia Management
Strategies: Hype or Real?
Topic: New Drugs for Old Bugs?
Through a CME Grant sponsored by

JAIME C. MONTOYA, MD, MSc
Professor V, Department of Medicine
University of the Philippines College of Medicine
Executive Director
Philippine Council for Health Research and Development
Department of Science and Technology
Consultant, Clinical Department
Research Institute for Tropical Medicine
Department of Health
RONPAKU Fellow for PhD, Juntendo University College of Medicine
Tokyo, Japan
Master of Science, Clinical Tropical Medicine, London School of Hygiene and
Tropical Medicine, University of London
Fellowship in Infectious Diseases, UP-PGH Medical Center
Doctor in Medicine, UP College of Medicine

New Drugs for Old Bugs
Jaime C. Montoya, MD, MSc, PhD
Professor V, UP College of Medicine

Outline of Talk
• Background on Antibiotics
• Problem of Antimicrobial Resistance
• Core Strategies in Prevention of Antimicrobial Resistance
• Issues in Drug Development
• New Antibiotics in the Pipeline
• New Trends in Management of Infections

Antibiotics
• Represent a special class of therapeutic agents whose misuse affects not just the individual patient but the broader community.
• This is due to the almost inevitable selection for antibiotic-resistant bacteria that arise in clinically significant waves at some point after widespread introduction and use of a new antibiotic (both in veterinary and human populations).

Antimicrobial Resistance
• Extensive use, misuse and overuse in both animal and human health have raised levels of antimicrobial resistance in a wide range of pathogens (bacteria, viruses, fungi and parasites).
• Increasing travel and trade in food have facilitated the spread of antimicrobial resistance

Antimicrobial Resistance
• NDM-1, a metallo-beta-lactamase which confers resistance to carbapenems was first detected in India in 2008 but has now been found in all continents
• New resistance mechanisms are emerging
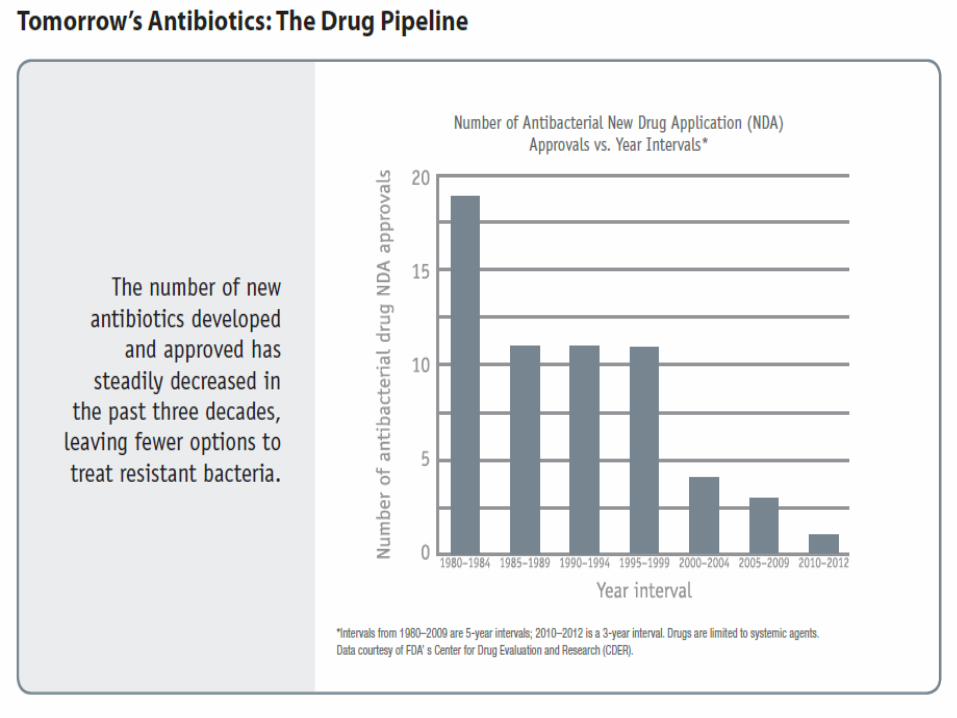
• Development of new antibiotics and interventions not keeping pace

Antimicrobial Resistance
• Infections caused by drug-resistant pathogens increase mortality across all settings leading to prolonged stay in hospitals and ICUs
• Beyond the immediate public health impact, antibiotic resistance incurs substantial health economic costs
• Losses of GDP from antimicrobial resistance range from 0.4% to 1.6%






Philippine Resistance Data 2012
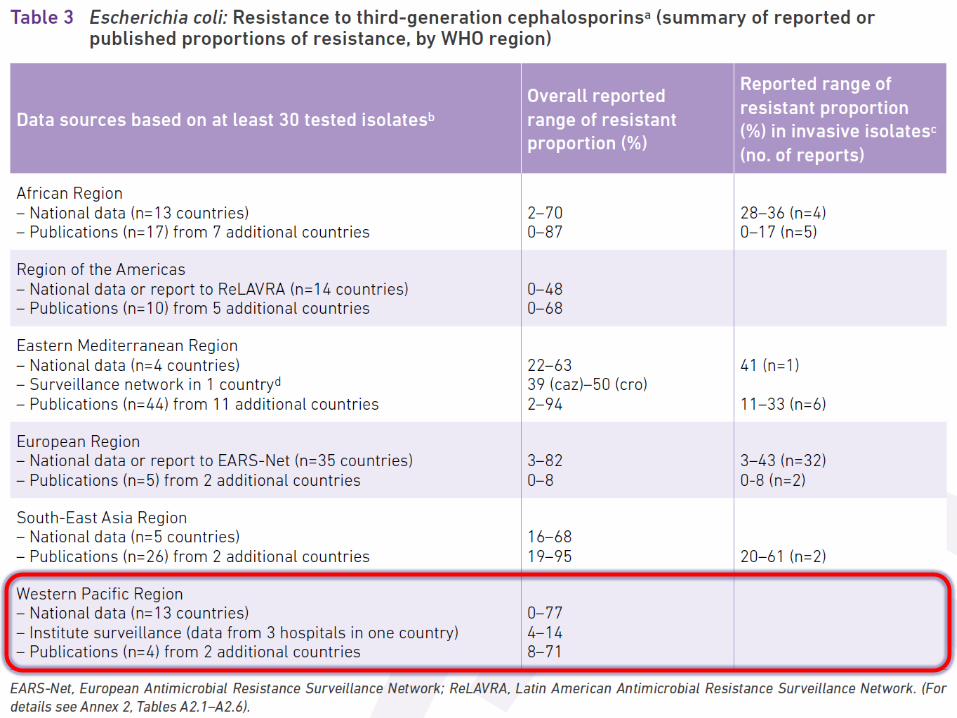
• E. coli resistant to 3rd Gen Ceph 26.7%
• E. coli resistant to Fluoroquinolones 40.9%
• Kleb pneumoniae R to 3rd Gen Ceph 30%
• Kleb pneumoniae R to carbapenems 3.8%
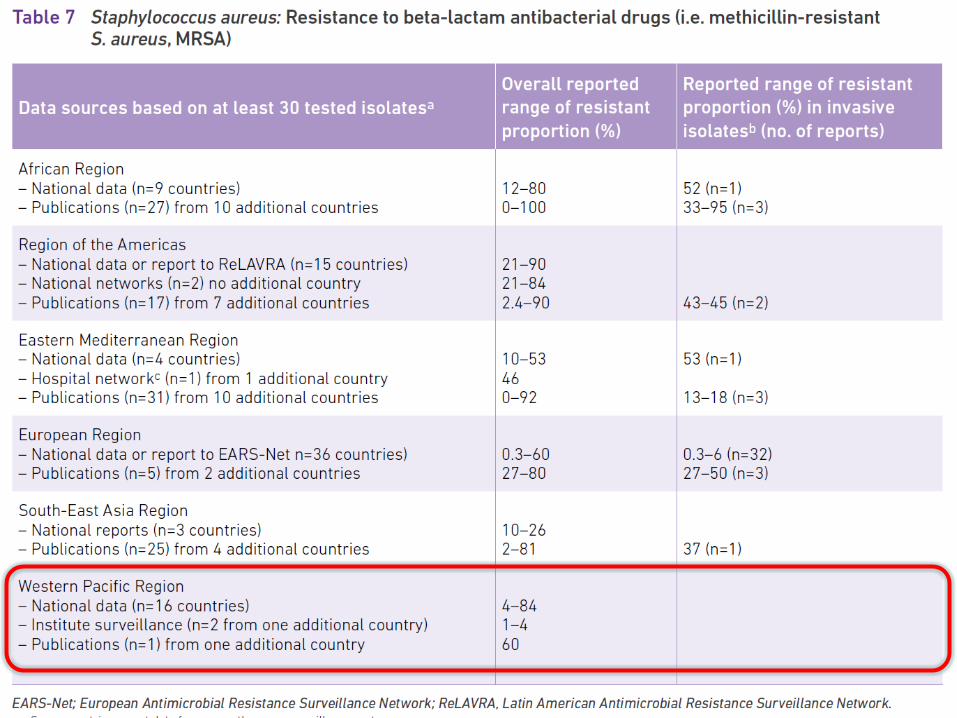
• Methicillin Resistant Staph aureus 54.9%
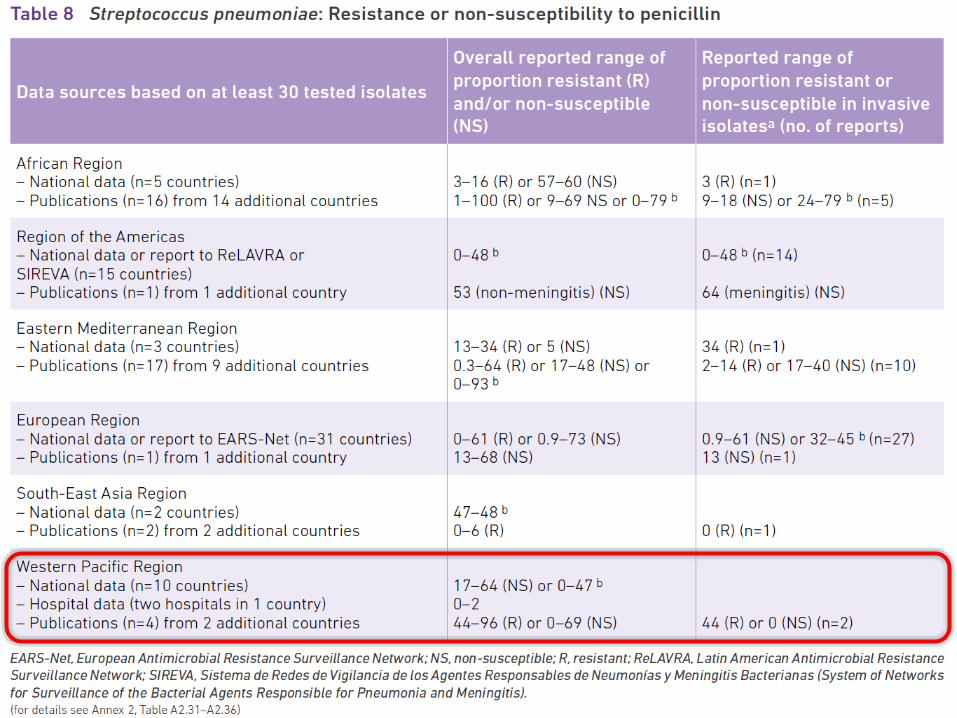
• Penicillin Resistant Strep pneumo 0

Core Actions on the Prevention of Drug Resistance• Prevent Infections
• Track Resistance Patterns
• Improve the Use of Antibiotics
• Develop New Antibiotics and Diagnostic Tests

Antimicrobial Stewardship
Involves selecting an appropriate drug andoptimizing its dose and duration to cure aninfection while minimizing toxicity andconditions for selection of resistant bacterialstrains
Fishman. Am J Med 2006;119(6A):S53-S61

Antimicrobial Stewardship
1) Educational programs2) Restricted antimicrobial formularies3) Prior approval programs4) Streamlining programs5) Antibiotic cycling/mixing6) Differentiation of infection,
contamination and colonization7) Discontinuation of antibiotic therapy8) Infection Control

Use Local Data
Fact: The prevalence of resistance can vary by locale, patient population, hospital unit, and length of stay.
Actions:
know your local antibiogram
know your patient population

Antibiotic Cycling vs Antibiotic Mixing
•Same protocol Cycling Mixing

Cycling versus Mixing
Cycling
• Greater heterogeneity at the level of the ward
• Difficult to implement
• Controversial results
Mixing
• Greater heterogenityat the level of the patient
• Easy implementation

Treat infection, not contaminationFact: A major cause of antimicrobial overuse is
“treatment” of contaminated cultures. Clinical correlation is very important
Actions:
use proper antisepsis for blood & other cultures
culture the blood, not the skin or catheter hub
use proper methods to obtain & process all cultures

Interpreting a “Positive” Blood Culture
True Bacteremia:
Unlikely Uncertain LikelyCorynebacterium spp. Coag negative Staph Staph aureus
Non-anthracis Bacillus spp. Strep pneumoniae
Propionibacterium acn Enterobacteriaceae
Pseudo aeruginosa
Candida albicans

Treat infection, not colonizationFact: A major cause of antimicrobial overuse is
treatment of colonization. Clinical correlation is very important.
Actions:
treat pneumonia, not the tracheal aspirate
treat bacteremia, not the catheter tip or hub
treat urinary tract infection, not the indwelling catheter

Know when to say “no” to broad spectrum antibiotics
Fact: Broad spectrum antibiotics overuse promotes emergence, selection, and spread of resistant pathogens through effect on normal host flora
Actions:
Target only most probable etiologic organisms
Use narrow spectrum antibiotics whenever possible

Stop antimicrobial treatment
Fact: Failure to stop unnecessary antimicrobial treatment contributes to overuse and resistance .
Actions:
when infection is cured
when cultures are negative and infection is unlikely
when infection is not diagnosed

Isolate the pathogen
Fact: Patient-to-patient spread of pathogens can be prevented.
Actions:
use standard infection control precautions
contain infectious body fluids
(use approved airborne/droplet/contact isolation precautions)
when in doubt, consult infection control experts
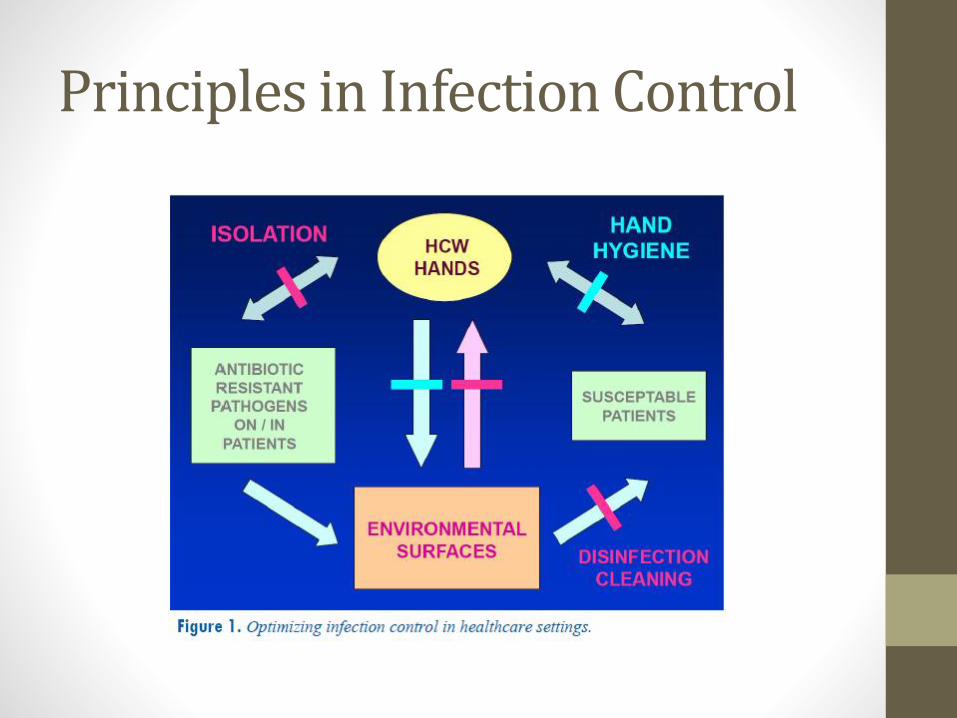
Principles in Infection Control

New Antibiotics in the PipelineTedizolid (Cubist)
• Noninferior to linezolid in treating acute bacterial skin and skin structure infections (ABSSSIs) caused by several organisms, including MRSA.
• Given once daily for 6 days, compared with twice-daily linezolid for 10 days
Oritavancin (The Medicine Group)
• A randomized, phase-3 noninferiority trial showed that oritavancin, a licoglycopeptide that is given as a single dose, was noninferior to vancomycin in the treatment of ABSSSIs.
• Also effective against MRSA
Corey GR et al. N Engl J Med 2014;370:2180-90.

New Antibiotics in the Pipeline
Ceftolozane/Tazobactam (Cubist)
• Antimicrobial combination has demonstrated effectiveness against bacteria that cause urinary tract infections and intra-abdominal infections, specifically Pseudomonas aeruginosa, extended-spectrum beta-lactamase–producing Escherichia coli and Klebsiellapneumonia
Ceftobiprole (Basilea)
• Fifth-generation cephalosporin has demonstrated noninferiority to the combined therapy of ceftazidime and linezolid in the treatment of hospital-acquired pneumonia, with the exception of ventilator-associated pneumonia.
• Approved for use in Europe but has seen some regulatory hurdles in the US
New Antibiotics in the PipelineDelamanid (Otsuka)
• Anti-tuberculosis drug was recently approved for use in Europe
• Can be used as part of a treatment regimen for patients with TB who are resistant to other medications

New Ways of Treating InfectionsUse of Bacteriophages to kill bacteria• Bacteriophages or "phage" are viruses that
invade bacterial cells and, in the case of lytic phages, disrupt bacterial metabolism and cause the bacterium to lyse [destruct].
• Phage Therapy is the therapeutic use of lytic bacteriophages to treat pathogenic bacterial infections

New Ways of Treating InfectionsBacteriophage therapy is quite attractive for killing bacteria for the following reasons:• phage particles are narrow spectrum agents, which
means they posses an inherent mechanism to not only infect bacteria but specific strains
• other pathogens may be targeted through manipulation of phage DNA
• exponential growth and natural mutational ability make bacteriophages great candidates for thwarting bacterial resistance
• minimal side effects


THANK YOU VERY MUCH!!!

Session on Pneumonia Management
Strategies: Hype or Real?
Topic: New Drugs for Old Bugs?
Through a CME Grant sponsored by