New Consensus Guidelines on Management of Dementia 7 May 2008 Symposium on the Changes & Challenges...
58
New Consensus Guidelines on Management of Dementia 7 May 2008 Symposium on the Changes & Challenges in Geriatric Care Waterloo, Ontario Michael Borrie, MB ChB, FRCPC Aging Brain and Memory Clinic Division of Geriatric Medicine, UWO Parkwood Site, St. Joseph’s Health Care
Transcript of New Consensus Guidelines on Management of Dementia 7 May 2008 Symposium on the Changes & Challenges...

New Consensus Guidelines onManagement of Dementia
7 May 2008Symposium on the Changes & Challenges in Geriatric Care
Waterloo, Ontario
Michael Borrie, MB ChB, FRCPC
Aging Brain and Memory Clinic
Division of Geriatric Medicine, UWO
Parkwood Site, St. Joseph’s Health Care

Disclosure Statement
Research Support Clinical Trials FundingCIHR Purdue-PharmaAlzheimer Society Canada NeotherapeuticsPhysician Services Incorporated HMRLawson Health Research Institute Pharmacia
Boehringer-IngelheimConsultant and CME Programs Sanofi-SynthelaboPfizer Myriad
PharmaceuticalsJanssen-Ortho ONO Pharma USANovartis NeurochemLundbeck Elan
Elan/Wyeth

Objectives
Using case scenarios, review and discuss relevant guidelines from the 3rd Canadian Consensus Conference on Diagnosis and Treatment of Dementia, March 2006.

3rd Canadian Consensus Conference onDiagnosis and Treatment of Dementia
CCCDTD3 March 9-11, 2006. Montreal
Specialists & Family Physicians.
140 guidelines.
Translation of Research to practice.
Clinical scenarios to illustrate how guidelines can
inform practice.

Criteria for assigning levels of evidence
Level Criteria
1. Evidence obtained from at least 1 properly randomized controlled trial.
2a.Evidence obtained from well-designed controlled trials without randomization.
2b.Evidence obtained from well-designed cohort or case-control analytic studies, preferably from more than 1 centre or research group.
2c. Evidence obtained from comparisons between times or places with or without the intervention. Dramatic results in uncontrolled experiments are included in this category.
3. Opinions of respected authorities, based on clinical experience, descriptive studies or reports of expert committees.

Grades of recommendations
Grade Criteria
A. There is good evidence to support this manœuvre.
B. There is fair evidence to support this manœuvre.
C. There is insufficient evidence to recommend for or against this manœuvre, but recommendations may be made on other grounds.
D. There is fair evidence to recommend against this procedure.
E. There is good evidence to recommend against this procedure.

Spectrum of Cognitive Decline
Adapted from Chertkow & Murtha, 1998
Super Normal•no deterioration from young
Age-consistent loss•average for age
Mild Cognitive Impairment•1.5 SD > Normal of age and education matched controls
Dementia

Serge Gauthier, 2001
MCI

Not normal, not demented (Does not meet criteria (DSM IV, ICD 10) for a dementia syndrome)
Cognitive decline• Self and/or informant report and impairment on objective cognitive tasks
and/or• Evidence of decline over time on objective cognitive tasks
Preserved basic activities of daily living / minimal impairment in complex instrumental functions
Recommendations for the General Criteria for Mild Cognitive Impairment – Consensus Report 2004
Winblad B, Palmer K, Kivipelto M et al. Mild cognitive impairment – beyond controversies, towards a consensus report of the International Working Group on Mild Cognitive Impairment. Journal of Internal Medicine 2004;256:240-246

Diagnostic Criteria for Dementia of the Alzheimer’s Type (DSM IV)
1) The development of multiple cognitive deficits manifested by both 1) memory impairment, and 2) one or more of the following cognitive disturbances:
– Language disturbance (Aphasia)– Impaired ability to carry out motor behaviours despite intact
motor function (Apraxia)– Failure to recognize or identify objects (Agnosia)– Disturbance in planning, organizing, sequencing, abstracting
(Executive Functioning)
2) Cognitive deficits cause significant impairment in social or occupational functioning
3) Gradual onset and continual decline
4) Cognitive deficits are not due to a) other CNS conditions, b) other Systemic conditions known to cause dementia, c) substance induced dementia, d) delirium, and e) another primary psychiatric disorder

Types of Dementia
• Alzheimer’s (AD)– Gradual on-set of memory and functional loss
• Vascular Dementia (VaD)– Step wise decline of memory and functional loss– Often occurring 3 months or so after a stroke
• Mixed Dementia (AD + VaD)– Now the most common form of dementia– When AD and VaD (cerebrovascular disease) co-exist
Reference: Patterson C, et al. The recognition, assessment and management of dementing disorders: Conclusions from the Canadian Consensus Conference in Dementia. Can J Neurol Sci. 2001;28(Suppl. 1): S3-S16.

Types (continued)
• Fronto-temporal Dementia (FTD)– The mirror image of AD with pronounced behaviour
problems initially and memory problems later
• Lewy Body Dementia (LBD)– Hallucinations (visual)– Parkinson-like symptoms– Fluctuations in level of consciousness


MEMORY Read list of words, subject must repeat them. Do 2 trials. FACE VELVET CHURCH DAISY RED

XXXXXXXXXXXXXXXXXX
XXXXXXXXXXXXXXXXXXXX
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
Xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx

Dementia Risk Factors
• Age
• Family history
• Vascular risk factorsHigh blood pressureDiabetesSmokingObesityHigh CholesterolAtrial Fibrillation
• Low education• Head injury/concussion

The Doubling Rule (Think 2) For Dementia Risk
< 65 = 1%
65 = 2%
70 = 4%
75 = 8%
80 = 16%
85 = 32%
* Risk Doubles every 5 years

The Doubling Rule (Think 2) For Dementia Risk
< 65 = 1%
65 = 2%
70 = 4%
75 = 8%
80 = 16%
85 = 32%
* Risk Doubles every 5 years
* But each additional risk factor approximately doubles the risk
* Positive family history doubles the risk

CS #2
75 year old woman, retired secretary, grade 12 education
- Sudden confusion with slurred speech for 1 hour,
5 years ago
- Forgetting names, 3 years
- gradually worse.
- Falls x 3 (2 trips) in last 12 months
- gait slower and less certain (cane), 6 months

CS #2
Collateral History – spouse and daughter - gradual progression since onset. - stopped driving 1 month ago. Getting disoriented & ran a red
light - purchasing several unneeded grocery items, 1 year - cooking quality changed - forgetting medications
Past History - High blood pressure, 15 years, on meds - Diabetes, 10 years, on meds - Elevated cholesterol, 5 years, on meds - Atrial Fibrillation, 3 years, on meds
P/S – no alcohol, no smoking - less energy. No initiative. Depressed? 1 year

Is this history suggestion of:
Mild cognitive impairment? White
Dementia? Black
Unsure Red
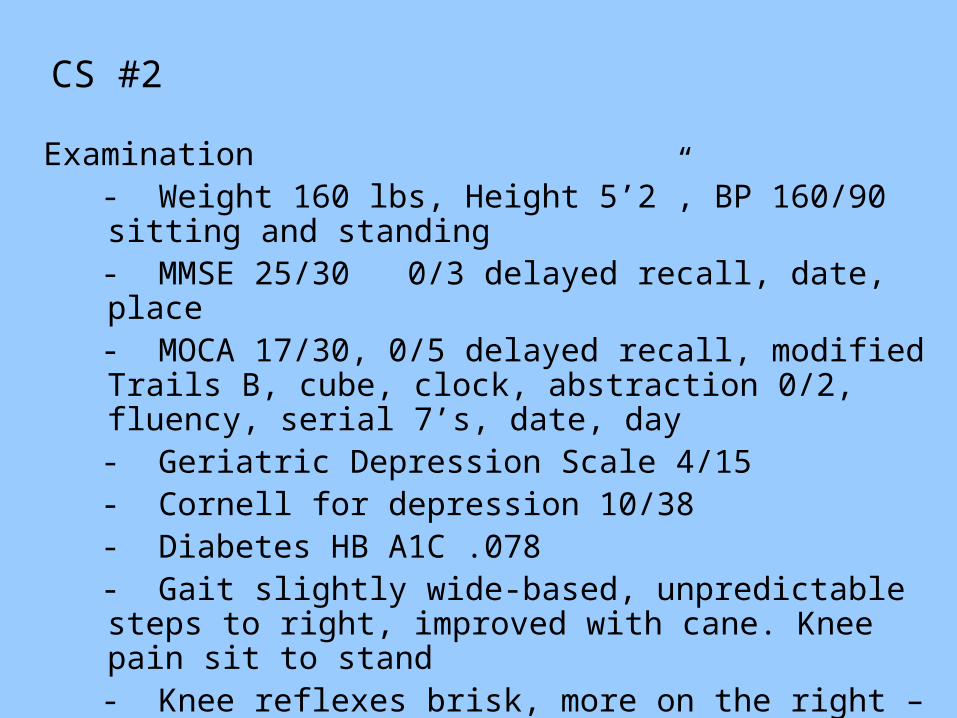
CS #2
Examination - Weight 160 lbs, Height 5’2”, BP 160/90 sitting and standing - MMSE 25/30 0/3 delayed recall, date, place - MOCA 17/30, 0/5 delayed recall, modified Trails B, cube,
clock, abstraction 0/2, fluency, serial 7’s, date, day - Geriatric Depression Scale 4/15 - Cornell for depression 10/38 - Diabetes HB A1C .078 - Gait slightly wide-based, unpredictable steps to right,
improved with cane. Knee pain sit to stand - Knee reflexes brisk, more on the right – Babinski flexor right
& left - hip flexion strength 4/5 right & left

Clinically, is the dementia likely due to:
Alzheimer disease (AD)? White
Vascular dementia (VaD)? Black
Mixed AD/VaD? Blue
Unsure Red

CS #2
Clinical Impression
1. Dementia – Mild. Mixed (AD VaD).2. Early OA knees3. Quadriceps weakness4. Vascular risk factors5. Depressive symptoms

CCCDTD3 Recommendations

Should this person and their family be referred to the Alzheimer Society?
Yes White
No Black
Unsure Red

CS#2 Recommendations
T5 #1a - All patients with dementia and their families who consent should be referred to the local chapter of the Alzheimer Society (eg: First Link program where available); and
T5 #1b - Primary care physicians should be aware of the resources available for the care of those with dementia in their community (eg: support groups, adult day program) and to make appropriate referrals to them. (GB, L3)

Should the diagnosis of dementia be disclosed to the person and their family?
Yes White
No Black
Unsure Red

CS #2 Ethico-legal recommendations T5 #6a – Although each case should be considered individually, in general, the diagnosis of dementia should be disclosed to the patient and family. This process should include a discussion of prognosis, diagnostic uncertainty, advance planning, driving issues, treatment options, support groups, and future plans. (GB, L3)
T5 #6b – Primary care physicians should be aware of the pertinent laws in their jurisdiction about informed consent, the assessment of capacity, the identification of a surrogate decision-maker, and the responsibilities of physicians in these matters. (GB, L3)
T5 #6c – While patients with AD (dementia) retain capacity, they should be encouraged to update their will and to enact both an advance directive and an enduring power of attorney. (GB, L3)

CS#2 Recommendations
Other therapeutic interventions
T7 #2 Investigations for vascular risk factors. It is recommended that vascular risk factors are identified in all patients with vascular cognitive impairment. (GC, L3)
T7 #3 Treating hypertension. There is some evidence that treating hypertension may prevent further cognitive decline associated with cerebrovascular disease. There is no compelling evidence that one class of agent is superior to another; calcium channel blockers or ACE-inhibitors may be considered (Grade B, Level I). Treatment for hypertension should be implemented for other reasons, including the prevention of recurrent stroke. (GA, LI)

In a person with mild dementia, will cognitive training/rehab improve and/or maintain cognitive and or function performance?
Yes White
No Black
Unsure Red
CS #2 Recommendations – non-pharmacological therapy in Mild AD
T5 #7a – There is insufficient evidence to come to any firm conclusions about the effectiveness of cognitive training/cognitive rehabilitation in improvement and/or maintaining cognitive and/or functional performance in persons with mild to moderate dementia. (GC, L1)

Could an individualized exercise program have an impact on functional performance?
Yes White
No Black
Unsure Red

CS #2 Recommendations – non-pharmacological therapy in Mild AD
T5 #7d - There is good evidence to indicate that
individualized exercise programs have an impact
on functional performance in persons with mild to
moderate dementia. (GA, L1)

Should a cholinesterase inhibitor be prescribed?
Yes White
No Black
Unsure Red

CS#2 Recommendations – Use of cholinesterase inhibitors
T7 #7 - Use of cholinesterase inhibitors in dementia due to combined Alzheimer’s and Cerebrovascular Disease: There is fair evidence of benefits of small magnitude for Galantamine in cognitive, functional, behavioural and global measures in AD with CVD. Galantamine can be considered a treatment option for mixed Alzheimer’s with Cerebrovascular Disease. (GB, LI)

Should neuroimaging be requested?
Yes White
No Black
Unsure Red

T3 Structural neuroimaging #2 - There is fair evidence to support use of structural neuroimaging to rule in concomitant cerebrovascular disease that can affect patient management. (GB, L2)

CS #2
Plan
• Alzheimer Society referral• Caregiver education• Control/monitor vascular risk factors. BP,
cholesterol• Weight loss• Exercise program• Head CT/MRI scan• Symptomatic treatment of dementia• Depressive symptoms – non drug approaches - medications?
CS #4
78-year-old retired truck driver/grade 10 education “a bit forgetful, just old age” 1 year
- Collateral hx. Wife.- Repeating stories and questions – 3 yrs- Gave up woodworking – 2 yrs “not interested”- Not as handy about house – 1 yr- Difficulty reassembling lawn mower – 2 mths ago- More irritable, easily angered at other drivers – 1 yr- Rolling stops – 1 yr- Late to pick up grandson from school x 3 - 2 mths

CS#4
Past History- 2 yrs ago, confused after prostate surgery- Diabetes – diet only – 5 yrs
P/S- Alcohol – 2-4 beers at the Legion 1 x /week-drives- Smoker – 40 pk yrs, stopped at age 60
Medication – Acetaminophen 1 gram 3x/day (sometimes forgets it)
Examination- Weight 220 lbs, Height 5’9”- BP 130/80- Osteoarthritis in hips and knees- Normal neurological exam

Could this man have:
Mild cognitive impairment? White
Dementia, probable Alzheimer Disease? Black
Vascular Dementia? Blue
Unsure Red

CS#4
MMSE 23/30 (1/3 recall, 3/5 world, day, date, place)
MoCA 16/30 (0/5 recall, trails, hands on clock, fluency, abstraction, date, 7’s)
Geriatric Depression Scale 0/15
Cornell 2/38 irritability
Fasting glucose 12, N<7
Hb A1C 0.074, N<0.06

What do you think the diagnosis is now?
Mild cognitive impairment? White
Dementia, probable Alzheimer Disease? Black
Vascular Dementia? Blue
Unsure Red

CS#4
Clinical Impression
Alzheimer Disease – mildOver weightDiabetesStill drivingDrinking while driving

CCCDTD3 Recommendations

CS#4 Recommendations
T5 #1b – Primary care physicians should be aware of the resources available for the care of those with dementia in their community (eg, support groups, adult day programs) and to make appropriate referrals to them. (GB, L3)
T3 #3 - “Mild” Alzheimer’s disease can be diagnosed with a high degree of specificity, when the presenting clinical picture is one of memory impairment (GB, L1)
T5 #7d - There is good evidence to indicate that individualized exercise programs have an impact on functional performance in persons with mild to moderate dementia (GA, L1).

Should a cholinesterase inhibitor be prescribed?
Yes White
No Black
Unsure Red
CS#4 Recommendations – on cholinesterase inhibitors
T5 #14a - All three cholinesterase inhibitors available in Canada are modestly efficacious for mild to moderate AD. They are all viable treatment option for most patients with mild to moderate AD. (GA, LI)
T5 #14b – While all three cholinesterase inhibitors available in Canada have efficacy for mild to moderate AD, equivalency has not been established in direct comparisons. Selection of which agent to be used will be based on adverse effect profile, ease of use, familiarity, and benefits about the importance of the differences between the agents in their pharmacokinetics and other mechanisms of action. (GB, L1)

CS#4 RecommendationsNeuropsychology testing
T3 Neuropsych #6 - The diagnosis and differential diagnosis of dementia is currently a clinically integrative one. Neuropsychological testing alone cannot be used for this purpose and should be used selectively in clinical settings (GB, L3)

Should people and their families be counselled about eventually giving up driving?
Yes White
No Black
Unsure Red
Does an abnormal score on the MMSE mean a person should not drive?
Yes White
No Black
Unsure Red

CS#4 Driving Recommendations
T5 #25a – Clinicians should counsel persons with a progressive dementia (and their families) that giving up driving will be an inevitable consequence of their disease. Strategies to ease this transition should occur early in the clinical course of the disease. (GB, L2)
T5 #25b - No single brief cognitive test (e.g. MMSE) or combination of brief cognitive tests has sufficient sensitivity or specificity to be used as a sole determinant of driving ability. Abnormalities on cognitive tests such as the MMSE, clock drawing and Trails B should result in further in-depth testing of driving ability. (GB, L2)
People with cognitive impairment and impaired instrumental activities of daily living should stop driving.
Yes White
No Black
Unsure Red

T5 #25c - Driving is contraindicated in persons who, for cognitive reasons, have an inability to independently perform multiple instrumental activities of daily living (e.g. medication management, banking, shopping, telephone use cooking) or any of the basic activities of daily living (e.g. toileting, dressing). (GB, L3)
T5 #25d - The driving ability of persons with earlier stages of dementia should be tested on an individual basis (GB, L3)

An on-road driving assessment is the best method of driving assessment.
Yes White
No Black
Unsure Red

CS#4 Driving Recommendations
T5 #25e - A health professional-based comprehensive off and on-road driving evaluation is the fairest method of individual testing (GB, L3)
T5 #25f - In places where comprehensive off and on-road driving evaluations are not available, clinicians must rely on their own judgment. (GB, L3)
T5 #25g - For persons deemed safe to drive, reassessment of their ability to drive should take place every 6-12 months. (GB, L3)
T5 #25h - Compensatory strategies are not appropriate for those deemed unsafe to drive. (GB, L3)

CS#4 Plan
1. First link Alzheimer Society/CCAC2. Nutritional counselling3. Weight loss4. Exercise5. Oral meds for diabetes?6. Driving testing – DriveABLE7. Lipid profile8. EC ASA 81mg

Summary
1. Identify Mild Cognitive Impairment early by listening to concerns about memory loss (patient and
caregiver).
2. Follow memory impairment with a sensitive measure MoCA.
3. Address vascular risk factors and depressive symptoms.
4. Treat symptoms of dementia (except FTD) with cholinesterase inhibitors.
5. Begin discussion about driving early and assessment with on-road assessment.