New Approaches to, and Indications for, Antiplatelet … Approaches to, and Indications for,...
32
New Approaches to, and Indications for, Antiplatelet Therapy Kenneth A. Bauer, MD Professor of Medicine, Harvard Medical School Chief, Hematology Section, VA Boston Healthcare System Director, Thrombosis Clinical Research, Beth Israel Deaconess Medical Center
Transcript of New Approaches to, and Indications for, Antiplatelet … Approaches to, and Indications for,...

New Approaches to, andIndications for, Antiplatelet Therapy
Kenneth A. Bauer, MDProfessor of Medicine, Harvard Medical School
Chief, Hematology Section, VA Boston Healthcare System
Director, Thrombosis Clinical Research,
Beth Israel Deaconess Medical Center

DisclosuresConsultant
Bayer HealthcareJanssen PharmaceuticalsBristol Myers SquibbPfizerBoehringer IngelheimInstrumentation Laboratory
Acknowledgement
Deepak Bhatt, MD

Atherothrombosis:Clinical Manifestations
Stroke/TIA
Carotid artery disease
Renal artery stenosis
Peripheral arterial diseaseAcute limb ischemiaClaudicationEndovascular stentingPeripheral bypass
Acute coronary syndromes– STEMI– NSTEMI– Unstable anginaStable CADAngioplastyBare metal stentDrug eluting stentCABG
Abdominal aortic aneurysm (AAA)
Meadows TA, Bhatt DL. Circ Res. 2007;100:1261-1275.

Meadows TA, Bhatt DL. Circ Res. 2007;100:1261
Platelet and Thrombus Formation:Vascular Injury

Desai NR, Bhatt DL. JACC Intervention 2010
Antiplatelet Agents

Mechanism Of Aspirin In Reducing Risks Of Cardiovascular Disease
Aspirin irreversibly acetylates the active site of cyclooxygenase (COX-1 and COX-2), which is required for the production of thromboxane A2 by platelets, which promotes platelet aggregation.

Efficacy of Aspirin at Various Doses in Reducing Vascular Events in High-Risk Patients
Vascular events included nonfatal MI, nonfatalstroke, and death from vascular causes.
Antithrombotic Trialists’ Collaboration. BMJ. 2002;324:71-86.
0.5 1.0 1.5 2.0
500-1500 34 19
160-325 19 26
75-150 12 32
<75 3 13
Any aspirin 65 23
Antiplatelet Better
Antiplatelet Worse
Aspirin (mg daily) Odds Ratio
0
No. of Trials
% Odds Reduction
Treatment effect P<.0001

Effect of Antiplatelet Therapy in Reducing Vascular Events in Diabetic Patients
Antiplatelet Trialists Collaboration BMJ 1994
Benefit/1000 pts (SD): 36 (3) 38 (12)2P: <0.00001 <0.002
No Diabetes Diabetes
Adj
uste
d (%
) of p
ts (+
1 SD
)w
ith v
ascu
lar
even
ts
0
10
20
30 ControlAntiplatelet therapy

ADP ReceptorsReceptorsubtype
Molecularstructure
Intrinsicion channel
GPCRGq
GPCRGi
Secondarymessenger
system[Na+/Ca2+]i PLC/IP3
[Ca2+]i
AC[cAMP]
Functionalresponse
Shape changeaggregation
Shape change transient aggregation
Sustained aggregation
secretion
G protein G protein
P2Y1
Clopidogrel
P2Y12 Activemetabolite
Bhatt DL et al. Nat Rev Drug Discov. 2003;2:15-28.
P2X1

Ticlopidine
Thienopyridine derivative: converted to active metabolites by liver cytochrome P450 isozymes
Irreversible P2Y12 receptor inhibitorLabeled indication: To reduce the risk of recurrent
stroke in patients who have had a stroke or a TIADosage: 250 mg bidIn combination with aspirin, demonstrated to be more
effective than anticoagulation (heparin/warfarin) in the prevention of stent thrombosis
Replaced by clopidogrel due to hematologic side effects:Neutropenia (2%)Thrombotic thrombocytopenic purpura (TTP)

CAPRIE: Superior Efficacy of Clopidogrel versus ASA
*MI, ischemic stroke or vascular death†Intent-to-treat analysis (n=19,185)
CAPRIE Steering Committee. Lancet 1996; 348: 1329–1339.
0
4
8
12
16
0 3 6 9 12 15 18 21 24 27 30 33 36Months of follow-up
Cum
ulat
ive
even
t rat
e* (%
)
ASA
Clopidogrel
8.7%† RRR (p=0.043)
20
Patients with recent ischemic stroke, recent MI or symptomatic PAD

CAPRIE: Clopidogrel Provided Amplified Benefit in Patients with Diabetes
Bhatt DL et al. Am J Cardiol 2002; 90: 625628.
*MI, stroke, vascular death or rehospitalization for ischemic events/bleeding†Number of events prevented per 1000 patients per year compared with ASA
ASAClopidogrel
12.7%
17.7%
21.5%
11.8%15.6%
17.7%
0
5
10
15
20
25
Patients without diabetes (n=15,233)
Patients with diabetes (n=3866)
Patients treated with insulin (n=1134)
Even
t rat
e*/y
ear (
%)
9†
21†
38†
p=0.096
p=0.042
p=0.106

Dual Antiplatelet Therapy
Clopidogrel adds to the benefit of aspirin in some circumstances (coronary artery disease).
Benefits and risks:Aspirin + Clopidogrel
Issues with ClopidogrelClopidogrel versus PrasugrelClopidogrel versus Ticagrelor
Cangrelor (investigational) – P2Y12 receptor antagonist
Aspirin + Dipyrimadole (Aggrenox) – sustained releaseASA (25 mg bid)/dipyrimadole (200 mg bid)Approved indication: ischemic stroke or TIA

Issues with ClopidogrelIrreversible P2Y12 receptor: dosage 75 mg qdPharmacokinetics: Oral absorption 1 h, t1/2 8 hOnset: 4-6 hours (after loading dose)Offset: 5-7 daysVariable response: 25-30% of patients achieve
less than 25% inhibition of platelet activityUndergoes 2 step metabolism (CYP3A4/2C19
mediated) to active agent (genetic variability)Potential drug interaction (e.g., PPIs)

CURE: Primary Efficacy Results(MI/Stroke/CV Death)
Randomized trial in acute MI
Yusuf S et al. N Engl J Med 2001; 345: 494–502.
0.00
0.02
0.04
0.06
0.08
0.10
0.12
0.14
0 3 6 9 12
Months of follow-up
Cum
ulat
ive
Haz
ard
Rat
e Placebo*
(n = 6,303)
Clopidogrel*(n = 6,259)
20% Relativerisk reduction
p = 0.00009
N=12,562
*On top of standard therapy (including ASA)

CURE: Clopidogrel in Patients with ACS and Diabetes
*Number of events prevented/1,000 patients treated/9 months†On top of standard therapy (including ASA)
Myocardial Infarction, Stroke, or Vascular Death
No previous diabetesn = 9,721
Diabetesn = 2,840
18
Cum
ulat
ive
even
t rat
e (%
)
9.9%
16.7%
7.9%
14.2%
Placebo†
Clopidogrel†
2
4
6
8
10
12
14
16
20*
25*
Yusuf S et al. N Engl J Med 2001; 345: 494–502.

CHARISMAA randomized, double-blind placebo controlled trial of
15,603 patients (79% ) with established CVD and 21% with multiple risk factors designed to test whether clopidogrel should be continued beyond 1 year in addition to aspirin.
All patients received daily aspirin (75-162 mg) and were randomized to daily clopidogrel (75 mg) or placebo
Clopidogrel patients had an event rate of 6.8% and placebo patients had an event rate of 7.3%.
CHARISMA demonstrated no significant benefit long term when clopidogrel is added to aspirin.
Rates of severe bleeding were similar, but clopidogrel patients experienced significantly higher rates of moderate bleeding.
Bhatt DL, et al; N Engl J Med. 2006. 54: 1706-1717

CHARISMA: Proportion of Diabetic Patients in Subgroups
Diabetics
42%Diabetics
31%Diabetics
83%
Non Diabetics
58%
Non Diabetics
17%
Non Diabetics
69%
Overall population
Secondary prevention
Primary prevention
N=15,613 N=12,153 N=3,284

Population RR (95% CI) p value
Qualifying CAD, CVD or PAD * 0.88 (0.77, 0.998) 0.046(n=12,153)
Multiple Risk Factors * 1.20 (0.91, 1.59) 0.20 (n=3,284)
Overall Population† 0.93 (0.83, 1.05) 0.22 (n=15,603)
Primary Efficacy Results (MI/Stroke/CV Death) by Pre-Specified Entry Category
0.6 0.8 1.41.2Clopidogrel + ASA
BetterPlacebo + ASA
Better
1.60.4
* A statistical test for interaction showed marginally significant heterogeneity (p=0.045) in treatment response for these pre-specified subgroups of patients† 166 patients did not meet any of the main inclusion criteria
Bhatt DL, Fox KA, Hacke W, et al. NEJM 2006.

Overall populationN=15,603
Secondary preventionN=12,152
Primary preventionN=3,284
Non Diabetics
N=9,047
Diabetics
N=6,556
Non Diabetics
N=8,380
Diabetics
N=3,773
Non Diabetics
N=569
Diabetics
N=2,715
Primary Efficacy – Diabetics vs Non Diabetics
Placebo + ASA Clopidogrel + ASA
0%
2%
4%
6%
8%
10%
6.7%
5.87%
8.24% 8.17%
6.73%
5.89%
10.04%9.23%
6.98%5.97%
5.14%
6.69%
p-value for interaction: 0.283 p-value for interaction: 0.923 p-value for interaction: 0.255

Mechanism of Action of Prasugrel
Bhatt DL. N Engl J Med 2009.

0
5
10
15
0 30 60 90 180 270 360 450
HR 0.81(0.73-0.90)P=0.0004
Prasugrel
Clopidogrel
HR 0.80P=0.0003
HR 0.77P=0.0001
Days
Prim
ary
Endp
oint
(%)
12.1(781)
9.9 (643)
Primary EndpointCV Death,MI,Stroke
NNT= 46
ITT= 13,608 LTFU = 14 (0.1%)
Wiviott et al. NEJM 2007.

Stent Thrombosis(ARC Definite + Probable)
0
1
2
3
0 30 60 90 180 270 360 450
HR 0.48P <0.0001
Prasugrel
Clopidogrel2.4
(142)
NNT= 77
1.1 (68)
Days
Endp
oint
(%)
Any Stent at Index PCIN= 12,844
Wiviott SD et al NEJM 2007. Slide courtesy of Dr. Elliott Antman

1.8
0.9 0.9
0.1 0.3
2.4
1.41.1
0.4 0.3
0
2
4
TIMI MajorBleeds
LifeThreatening
Nonfatal Fatal ICH
Bleeding Events - Safety Cohort(N=13,457)
% E
vent
s
ARD 0.6%HR 1.32P=0.03
NNH=167
ClopidogrelPrasugrel
ARD 0.5%HR 1.52P=0.01
ARD 0.2%P=0.23
ARD 0%P=0.74
ARD 0.3%P=0.002
ICH in Pts w Prior Stroke/TIA
(N=518)Clop 0 (0) %Pras 6 (2.3)%
(P=0.02)
Slide courtesy of Dr. Elliott Antman

Diabetic Subgroup
0
2
4
6
8
10
12
14
16
18
0 30 60 90 180 270 360 450
HR 0.70P<0.001
Days
Endp
oint
(%)
CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
NNT = 21
N=314617.0
12.2
Prasugrel
Clopidogrel
Prasugrel
Clopidogrel 2.62.5
Wiviott et al. Circulation 2008.

Mechanism of Action of Ticagrelor(a cyclopentyl triazolopyrimidine)
Bhatt DL. Nature Reviews Cardiology. 2009;6:737-38.

CV Death, MI, or Stroke
No. at risk
ClopidogrelTicagrelor
9,2919,333
8,5218,628
8,3628,460
8,124
Days after randomisation
6,7436,743
5,0965,161
4,0474,147
0 60 120 180 240 300 360
1211109876543210
13C
umul
ativ
e in
cide
nce
(%)
9.8
11.7
8,219
HR 0.84 (95% CI 0.77–0.92), p=0.0003
Clopidogrel
Ticagrelor
Wallentin L, et al. N Engl J Med. 2009.
No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,560
8,678
8,405
8,520
8,177
Days after randomisation
6,703
6,796
5,136
5,210
4,109
4,191
0 60 120 180 240 300 360
6
5
4
3
2
1
0
7
Cum
ulat
ive
inci
denc
e (%
)
Clopidogrel
Ticagrelor
5.8
6.9
8,279
HR 0.84 (95% CI 0.75–0.95), p=0.005
0 60 120 180 240 300 360
6
4
3
2
1
0
Clopidogrel
Ticagrelor
4.0
5.1
HR 0.79 (95% CI 0.69–0.91), p=0.001
7
5
9,291
9,333
8,865
8,294
8,780
8,822
8,589
Days after randomisation
7079
7119
5,441
5,482
4,364
4,4198,626
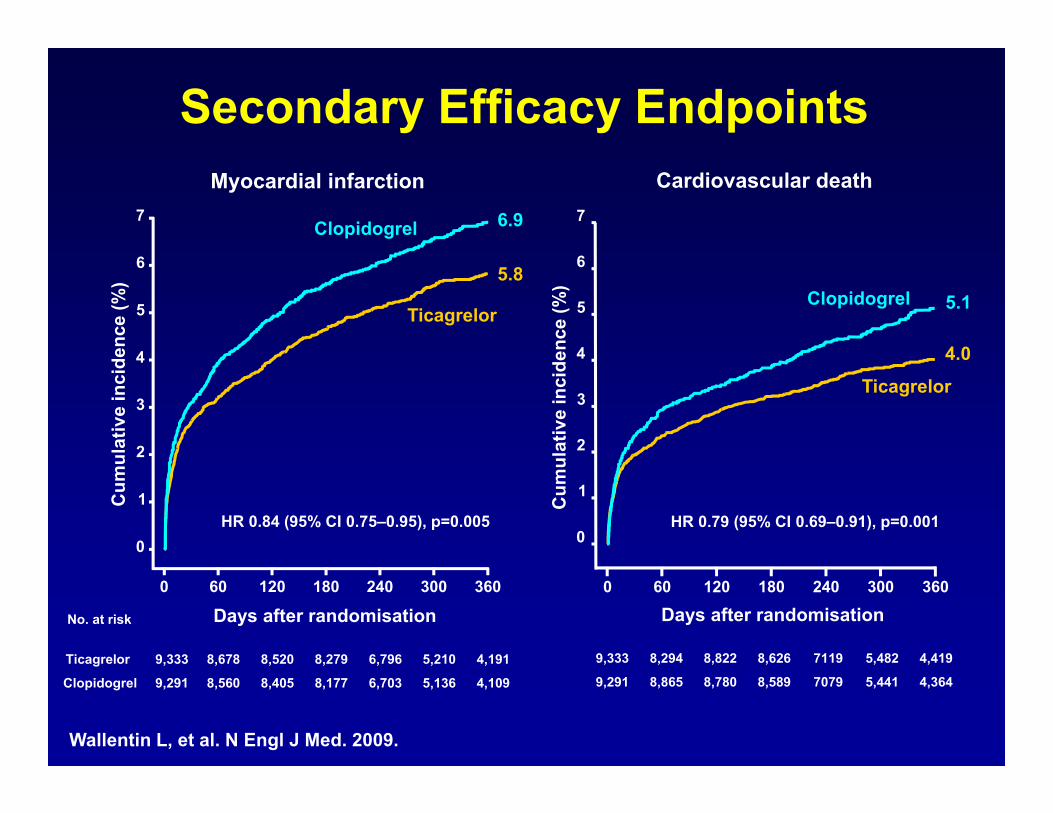
Myocardial infarction Cardiovascular death
Cum
ulat
ive
inci
denc
e (%
)
Secondary Efficacy Endpoints
Wallentin L, et al. N Engl J Med. 2009.
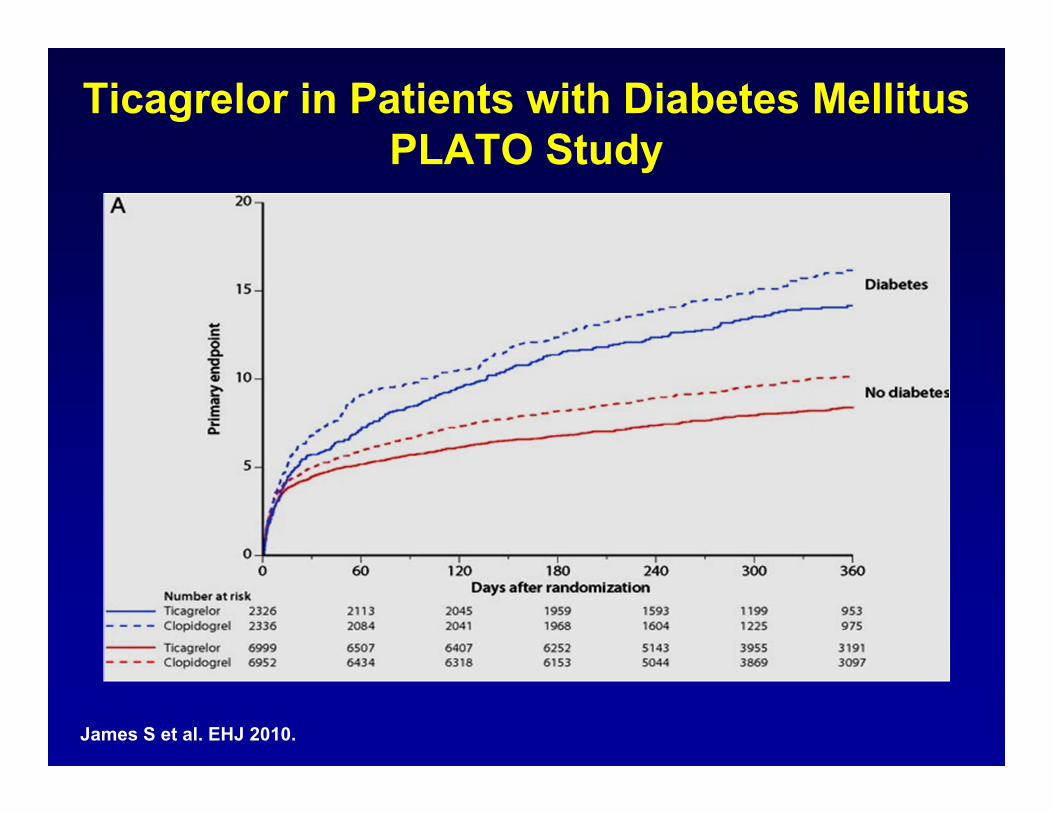
Ticagrelor in Patients with Diabetes Mellitus PLATO Study
James S et al. EHJ 2010.

CURRENT-OASIS= Clopidogrel Optimal Loading Dose Usage to Reduce Recurrent Events Optimal Antiplatelet Strategy for Interventions; PCI=percutaneous intervention; PLATO= A Study of Platelet Inhibition and Patient Outcomes; TRITON-TIMI= Trial To Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition With Prasugrel Thrombolysis in Myocardial Infarction.Ferreiro JL, Angiolillo DJ. Circulation 2011. 123:798-813.
Efficacy of New Drugs/Approaches in Reducing Adverse Outcomes in Diabetes Mellitus From Large-Scale Clinical Trials
TRITON-TIMI 38 17.0 12.2 0.70 (0.58 – 0.85)
PLATO 16.2 14.1 0.88 (0.76 – 1.03)
CURRENT OASIS 7 5.6 4.9 0.87 (0.66 – 1.15)(PCI Cohort)
Study % of Events Hazard Ratio (95% confidence interval)Standard New Drug/Approach
New Drug/ApproachBetter
Standard ClopidogrelBetter
0 0.5 1 1.5

DUAL ANTIPLATELET THERAPY AND INCREASED RISKS OF BLEEDING
In a meta-analysis of 18 randomized trials which included 129,314 patients
Those assigned to dual antiplatelet therapy have about a 50% increase in risk of major bleeding compared with those given single agent therapy
The magnitude of this excess risk is about as high as the approximately 60% increase observed in the trials comparing single antiplatelet agents to placebo
These excess risks of major bleeding should be considered in relation to the benefits on occlusive CVD events in choosing the optimal antiplatelet strategy, especially for long-term treatment of patients with prior events or those at high risk of developing CVD.
Fund Clin Pharm 2008; 22:315-321
Conclusions
Increased platelet activation/aggregation in diabetic patient
contributes to their increased rate of ischemic events
Clear role for aspirin in secondary prevention, ? “primary” prevention
Dual antiplatelet therapy indicated for at least 1 year after ACS or PCI
More potent P2Y12 receptor antagonists likely of greater benefit in
diabetics, if bleeding risk not too high