
New and Expectant Mothers Risk Assessment Policy … and... · 2 Policy Title: New and Expectant...
18
New and Expectant Mothers Risk Assessment Policy Including Breast Feeding Mothers
Transcript of New and Expectant Mothers Risk Assessment Policy … and... · 2 Policy Title: New and Expectant...

New and Expectant Mothers Risk Assessment Policy
Including Breast Feeding Mothers
2
Policy Title:
New and Expectant Mothers Risk Assessment Policy, Including Breast-Feeding Mothers
Executive Summary:
East Cheshire NHS Trust is committed to delivering a quality service. The Trust recognises the importance of managing and supporting new and expectant mothers in a positive and supportive manner, in accordance with current legislation. The Trust is also aware of its obligations under specific health and safety legislation and will ensure that all risks that could affect new, expectant or breast feeding women are satisfactorily controlled The prime aim of this policy is ensure that new, expectant and breastfeeding mother’s health and the health of the child are not compromised due to the mother’s employment.
Supersedes: V4
Description of Amendment(s):
Reused format, adjustments to monitoring responsibilities.
This policy will impact on: All staff working within the Trust
Financial Implications: Limited financial impact. Resources required in authors time to review their policies to ensure that they meet the standard outlined in this document.
Policy Area: Trust Wide Document Reference:
Version Number:
5 Effective Date: Oct.2016
Issued By: Director of Corporate Affairs & Governance
Review Date: Sept 2019
Author: Health & Safety Manager
Impact Assessment Date:
Sept 2016
APPROVAL RECORD
Committees / Group Date
Consultation: Risk Management Sub-committee members Michelle Moran - Clinical Governance Midwife Occupational Health Team
Sept 2016 Aug 2016
Approved by Director: Director of Corporate Affairs & Governance
Sept 2016
Received for information:
Cascaded via Central policy cascade process to service leads
3
Table of Contents
1. Introduction
Page 4
2. Purpose
Page 4
3. Roles and Responsibilities
Page 4
4. Implementation
Page 5
5. Monitoring Compliance with the Document
Page 8
6. References
Page 8
1. Communication Page 11
Page 12
Appendix 1 Equality Analysis Appendix 2 Work factors for Management Consideration Appendix 3 Pregnant Employee Risk assessment

4
1. Introduction
East Cheshire NHS Trust is committed, through its Health and Safety and Risk Management Policies to the maintenance of safe working practices and the provision of an environment, which is safe for staff, patients and others, in accordance with good clinical practice and the requirements of Health and Safety, Fire Safety, Security and Environmental Legislation. This policy applies to all new/expectant mothers employed by East Cheshire NHS Trust. The policy relates to the requirements of all staff including new/expectant mothers to adhere to this policy in line with heir contractual responsibilities and current legislation.
2. Purpose
The aim of this Policy to establish the importance of early and continued risk assessment which will ensure that any hazards specific to new or expectant mothers and breast-feeding mothers are identified and known to the employee and employer and correct control measures are implemented.
Consideration will be given to identify risks within the work place that may affect any new/expectant mother. Its recognised by this policy that pregnancy is not any form of ill health and this policy must not be used in any way to justify that view. Consideration must be given to the identification of any hazards to the expectant or new mother employee that may be present in the workplace
3.0 Responsibilities
3.1 The Chief Executive:
Ultimate accountability for health and safety lies with the Trust Chief Executive; this responsibility maybe delegated. 3.2 Director of Corporate Affairs & Governance
Delegated accountability for ensuring that Health and Safety arrangements are in place across the Trust.
3.3 Human Resources:
It is the responsibility of Human Resources to assist and support both employees and managers in cases where significant risk may mean removal of the employee from her normal work. Regulation 16 Management of Health and Safety at Work Regulations 1999.
Liaise with Managers where risk assessment reveals that work could harm women of childbearing capacity with regard to restrictions and temporary redeployment issues.
3.4 Trust Managers: All managers with expectant or new/breast-feeding mothers must:
Ensure the risk assessment for new and expectant mothers is completed as soon as pregnancy is confirmed.
Ensure the risk assessment is updated if the condition of the women changes significantly and or new potential risks is identified.
5
Refer to the Occupational Health Service if there are any concerns in undertaking the risk assessment or establishing effective controls. (The Occupational Health Service will be happy to assist any manager in completion of risk assessments)
Ensure a copy of the risk assessment is provided to the worker.
Refer any employee with identified gestational related conditions for formal assessment by the Occupational Health Service; this should be done using the standard Management referral form.
Encourage the employee to attend the Occupational Health Service to discuss any concerns
Ensure that rest areas and lavatory facilities are available and opportunity is provided for breast-feeding if requested and storage facilities for breast-milk if required.
3.5 Employee:
Written confirmation of pregnancy is mandatory. This should be provided within the 1st trimester of pregnancy or as early as feasibly possible to enable adequate risk assessment to be performed.
If requested employees must attend for formal assessment by the Occupational Health Service.
Employees must assist with the risk assessment and answer questions honestly.
It is the responsibility of the employee to notify their employer on return from maternity leave if it is greater than 6 months since delivery and she is continuing to breastfeed.
Follow Trust policies on PPE, COSHH and safe working practices with ionising radiation.
Agree the timing and flexibility of rest breaks with the employer in conjunction with the Risk Assessment Process.
3.6 Occupational Health Service:
Provide professional advice to departmental managers regarding completion of Pregnant Employee Risk Assessments and subsequent management of new and expectant mothers.
Advise employees and managers regarding pregnancy related illness or issues. 3.7 Health and Safety Manager:
Contact relevant managers and/or employees if there are particular hazards or problems identified in the risk assessment that the Occupational Health Service identifies need further specialist assessment.
Ensure that adequate controls are in place subject to COSHH risk assessment
Assist managers in identifying and controlling risks in the workplace that maybe hazardous to gestational or breastfeeding women.
The Health & Safety Department will ensure that this policy and related risk assessment is reviewed regularly and in light of new Department of Health, RIDDOR, COSHH regulations or Health and Safety Executive directives and changes in domestic and European law.
Ensure copies of this policy and risk assessment are available for use by departmental managers.
Advice the organisation of changes in legislation that may affect application of this policy.
4.0 Implementation
4.1. Scope/Definitions: This policy is produced in accordance with:
The European Community Directive (82/85/L22)
The Health and Safety at Work Act 1974
Health Service Managers Regulations 1999
Control of Substances Hazardous to Health regulation 2004
RIDDOR 1995.
Management of Health and Safety at Work Regulations 1999 (MHSW)

6
Equality Act 2010
The Workplace (Health, Safety & Welfare) Regulations 1992 Specific Legal Duties Under Above Regulations:
Regulation 16 of the Management of Health and Safety Regulations (MHSW) 1999 requires employers to take particular account of risks to new and expectant mothers when assessing risks in work activity.
Under the Equality Act 2010, if an employer fails to protect the health and safety of their pregnant workers, it is automatically considered sex discrimination.
Under Regulation 16 Management of Health and Safety at Work Regulations 1999. If suitable alternative work cannot be provided for pregnant workers when risks in their substantive role cannot be control satisfactorily, then the employee must be suspended from work on full pay.
Under Regulation 17 Management of Health and Safety at Work Regulations 1999. If a new or expectant mother is provided with a certificate from a medical practitioner / midwife stating that it is necessary for her health and safety that she should not perform night work, then the employee should be offered suitable alternative day work.
Workplace Regulations 1992 require employers to provide suitable rest facilities for new, breastfeeding and expectant mothers
MHSW Regulation 3 places a legal duty on all employers to assess the Health and Safety risks that may affect employees.
Who do the regulations cover? The regulations cover female employees who are, or in the future could be, a new or expectant mother. Essentially, women of childbearing age who are or in the future could be pregnant, have given birth within the previous six months, or are breastfeeding. This policy is relevant to:
Trust Managers
The Occupational Health Service
Human Resources
Health and Safety
New and expectant mothers (including employees, temporary staff, contractors and students)
A New or expectant mother:
Is pregnant
Has given birth within the previous 6 months
Continues to breast feed beyond 6 months of delivery
Birth: An employee who has:
Delivered a live baby
Delivered of a stillbirth at full or after 24-weeks gestation.
Does not include employees where miscarriage or termination of pregnancy has occurred before 24 weeks gestation.
Related Policies: Maternity, Adoption and Paternity Pay and Leave Policy COSHH Policy Personal Protective Equipment Policy Manual Handling Policy Infection Prevention and Control Policies Employee Emotional Well-Being and Work Related Stress Policy

7
4.2. Essential Elements of Risk Assessment: (Reference: Appendix 1, 2, 3) The risk assessment must be completed using the pre-printed Pregnant Employee Risk Assessment document available directly from the Occupational Health Service or on the intranet. (Appendix e) The risk assessment should be performed with the woman it pertains to present, the completing manager must be aware of relevant COSHH risk assessments in their area and potential hazards that may exist for gestating women. (If any uncertainty then discuss with the Health and Safety Manager) 4.2.1. Risk assessment includes: Physical agents: that may affect the employee; this includes the environment, manual handling, ionising radiation, and potential for physical violence issues. Biological agents: that could affect the employee that pose a potential hazard to the employee, these include exposure to contagious disease and blood borne viruses, home visits or work in hospitals or clinics. Also is the worker likely to be exposed to biological agents that can cause abortion; if this found to be the case then the worker must be removed from the area immediately and Occupational Health advice sought immediately. Chemical agents: With the aid of the COSHH risk assessments for the area the manager must establish if the employee could be exposed to chemical substances with the labelling R40, R45, R46, R61, R63, or R64; or mercury or its derivatives, lead or its derivatives, or any chemical substance which can be absorbed through the skin (Reference: Appendix B) If the answer is yes to any of these questions then every attempt should be made to isolate the employee from them; if for any reason this is not possible or if the employee expresses concern working in an area where these substances exist then the employee should be removed, and temporary re-deployment considered. Immediate referral to the Consultant in Occupational Medicine should be made. Working Condition: this includes shift patterns, on-call commitments, DSE work and driving on trust business; special consideration should be made when completing the risk assessment for the fact that the employee’s ability to cope with the physical demands of their job will vary with the advancement of the pregnancy and reasonable rest facilities should be considered. Physiological factors: Certain physiological factors which affect women when they are expectant should be considered such as morning sickness, back pain, hypertension and bladder weakness. Some of the more common risks that must be considered are:
Lifting/carrying of heavy loads
Standing or sitting for long lengths of time
Exposure to infectious diseases
Exposure to lead
Work-related stress
Workstations and posture
Exposure to radioactive material
Other people’s smoke in the workplace
Threat of violence in the workplace
Long working hours
Excessively noisy workplaces.
Stress and Anxiety
Drugs that may potentially cause harm/miscarriage

8
Once all sections of the Pregnant Employee Risk Assessment have been completed all hazards that have been identified must be priority listed on the back sheet. Once hazards have been identified the manager must establish methods of either reducing or removing the risk to the employee. It is essential that any identified hazard have reasonable and effective recommendations implemented to eliminate risk.
4.2.2. On Return to Work: The risk assessment should be reviewed if the woman returns to work within 6 months of delivery or if they declare they are continuing to breastfeed.
5.0 Monitoring Compliance with the Document
5.1 Performance
KPIs Monitored by Monitoring Frequency
Information reported to
No. of incidents reported relating to New & Expectant mothers
Health & Safety Team meeting
Weekly Risk Management Sub-committee on exception
5.2. Audit The policy will be audited annually in relation to:
Referrals to Health and Safety Manager for further assessment and advice.
Incident trends relating to New & Expectant Mothers including Breast Feeding Mothers.
Completion of New and Expectant Mothers risk assessment by line Managers. All outcomes to be reported back to Risk Management Sub-committee by the Health and Safety Manager.
REVIEW This policy will be reviewed on a 3-year basis by the Health and Safety Manager and necessary amendments will be carried out, in line with changes in domestic and European laws which have a direct effect up on it and following instruction from the Department of Health, or in response to organisational change.
6.0 References
1. Health and Safety at Work Regulations 1999 2. Management of Health and Safety at Work Regulation 1999 3. Management of Health and Safety at Work. Management of Health and Safety at
Work Regulations 1999. Approved Code of Practice and guidance L21 (Second Edition) HSE Books 2000 ISBN 978 0 7176 2488 1
4. Workplace Health, Safety and Welfare. Workplace (Health, Safety and Welfare) Regulations 1992. Approved Code of Practice L24 HSE Books 1992 ISBN 978 0 7176 0413 5
5. Five steps to risk assessment Leaflet INDG163 (rev2) HSE Books 2006 6. New and expectant mothers at work: A guide for employers HSG122 (Second
Edition) HSE Books 2002 ISBN 978 0 7176 2583 3 7. New and expectant mothers at work: A guide for health professionals available at
www.hse.gov.uk/pubns/indg373hp.pdf 8. Guidance giving information on rights for pregnant women available at

9
www.berr.gov.uk 9. Working safely with ionising radiation: Guidance for expectant or breastfeeding
Mothers Leaflet INDG334 HSE Books 2001 www.hse.gov.uk 10. Infection risks to new and expectant mothers in the workplace: A guide for 11. Employers Guidance booklet HSE Books 1997 ISBN 978 0 7176 1360 1 12. Sex Discrimination Act 1975 the Stationery Office 1975 ISBN 978 0 1054 6575 1
NHS Plus, Royal College of Physicians, Faculty of Occupational Medicine. Physical and shift work in pregnancy: occupational aspects of management. A National Guideline. London: RCP, 2009. www.nhsplus.nhs.uk
13. The Health and Safety Executive. A Guide for New and Expectant Mothers Who Work.
London: HSE, 2003. www.hse.gov.uk 14. The Health and Safety Executive. New and expectant mothers at work – a guide for health
professionals. London: HSE, 2003. www.hse.gov.uk 15. The Law Management of Health and Safety at Work Regulations 1999 (MHSW) accessed
13th July 2016 from www.hse.gov.uk/mothers/law.htm
10
Appendix 1
WORK FACTORS FOR MANAGEMENT CONSIDERATION A. Physical Agents 1. Shock / Vibration: Increases risk of miscarriages – Avoid. 2. Working hours: Pregnant women should be informed about the generally consistent evidence suggesting that long working hours carry no more than a small to moderate risk of preterm birth, and Low birth weight/Small Gestational Age (SGA) There is limited and inconsistent evidence for pre-eclampsia. Managers should reduce long working hours for pregnant workers particularly in late pregnancy. Where possible, hours should be limited to about 40 per week. However, if a pregnant worker who has been informed of the possible risk wishes to continue then there are insufficient grounds to impose restrictions against her will. 2.1 Shift work: There is insufficient evidence of a risk to pregnant women to make recommendations to restrict shift work, including rotating shifts or night/ evening work. 3. Manual Handling: increases in hormonal changes as pregnancy advances lead to softening of ligaments and may cause risk of strains and sprains for up to three months post delivery. While physical activity and maintaining fitness is beneficial during pregnancy, excessive physical work or heavy lifting may pose a risk especially towards the end of pregnancy. If work involves manual handling of weights greater than 10 kilograms, prolonged standing, repetitive lifting or maintaining awkward postures, then you should seek further advice from Occupational Health.
Pregnant women should be informed that evidence suggests:
That at most, heavy physical work and lifting carry no more than a moderate risk of low birth weight/intrauterine growth restriction/small for gestational age
There is limited and inconsistent evidence of risk from manual handling for preterm birth and pre-eclampsia.
Managers should reduce very heavy physical activities and lifting for pregnant workers where possible, particularly in late pregnancy. However, if a pregnant worker who has been informed of the possible risk wishes to continue then there are insufficient grounds to impose restrictions against her will. 4. Noise: risk to hearing, increasing tiredness and increase in blood pressure in pregnancy. Consider noise monitoring / PPE. 5. Ionising Radiation: significant risk to pregnant and nursing mothers, therefore avoid exposure. Levels of exposure to ionizing radiation that do not harm a pregnant woman may harm the developing foetus, particularly between 8 - 25 weeks gestation. As many women are uncertain of their conception date during the early weeks of pregnancy, special consideration must be given to the use of ionizing radiation. It is very important for the woman and her foetus that she notifies her Supervisor or Radiation Safety Officer (RSO) or Occupational Health as soon as she can, to ensure that her work is assessed and modifications promptly made to reduce radiation exposure.
If work includes using ionizing radiation and an employee becomes pregnant, she has a choice to either continue working with ionizing radiation or take on other tasks. It is possible to work with ionizing radiation provided that the RSO has undertaken an assessment and has defined the actions that must be taken to ensure that the risk to her and her foetus is as low as possible.

11
If an employee works with non-ionizing radiation and she is pregnant, or planning to become pregnant, then she should seek advice. 6. Non-Ionising Radiation / Electromagnetic fields / waves: no greater risk than other workers. 8. Temperature: extreme heat and cold should be avoided as fainting and heat stress may occur in pregnancy. 9. Movement /Posture: excessive physical activity has been associated with miscarriage, low-birth weight and increases in blood pressure. Strain and sprain injuries can occur from working in unsuitable positions. Co-ordination and dexterity may be impaired. Pregnant women should be informed about the generally consistent evidence suggesting that:
Prolonged standing (more than three hours) carries no more than a small risk of preterm birth and low birth weight/ Intrauterine growth restriction/Small for gestational age
Limited evidence suggests that prolonged standing has no effect on pre-eclampsia. Managers should reduce standing for longer than three hours for pregnant workers where possible, particularly in late pregnancy. However, if a pregnant worker who has been informed of the possible risk wishes to continue, then there are insufficient grounds to impose restrictions against her will 10. Travel: risk of fatigue therefore consider hours of work. Pregnant individuals should wear adjustable seatbelts after 24 weeks of pregnancy, if travelling on business, via car. More than 28 weeks pregnant, a statement of fitness to fly is often required from the employee’s GP. International airline companies don’t permit pregnant women to fly after 34 weeks pregnancy. B. Biological Agents – groups 2, 3 and 4 1. Pregnancy: Infection can be passed through the placenta from mother to foetus. Biological agents present a risk of abortion of the foetus or may lead to physical damage to the foetus. Consider colleagues who may have infections e.g. chickenpox or rubella (German measles). Pregnant workers should not come into close contact with other workers who have or suspect chickenpox or rubella. 2. Breastfeeding: Infection can be passed from the mother to the baby through breast milk or by close physical contact. Consider laboratory practices, control measures, and look to reduce any possibility of exposure. C. Chemical Agents – substances with particular banding endangering health If chemicals are labelled with the following labels, a risk to new and expectant mothers should be considered: R40 – possible irreversible effects R45 – carcinogenic R46 – may cause genetic damage R47 – may cause birth defects R61 – harm to unborn child R63 – possible risk of harm to unborn child R64 – may cause harm to breast fed infants With the exception of lead and asbestos these substances fall within the COSHH regulations and may be subject to change. Eliminate the employee from working with the above substances. 1. Mercury: Risk of retarded growth of the unborn child. Eliminate risk to unborn child and infant by removing pregnant and nursing mothers from working with mercury.

12
2. Cytotoxic substances: Risk of damage to genetic information of the female reproductive system. Remove employee from such work. Inhalation is the most common route of exposure to chemicals in the typical working environment at East Cheshire Trust. The use of safe work procedures and facilities such as local exhaust ventilation should provide satisfactory protection. Skin absorption and ingestion are generally less significant routes of exposure, provided safe work practices are observed. Under the Health and Safety at Work Act 1974, everyone is required to use appropriate safe work procedures when handling chemicals.
Exposure to chemicals at levels below recognised exposure limits should not present a risk to the employee or her foetus during pregnancy or while breast-feeding, however once you an employee knows she is pregnant, she is encouraged to advise her supervisor or the Occupational Health Service as soon as possible. If there are any concerns about a chemical in usage, or the procedures for its safe use during pregnancy or whilst breast-feeding, you must seek advice straight away from the Health and Safety Manager. D. Display Screen Equipment – unnecessary to stop pregnant women from working with visual display units Review visual display assessment. Where pregnant women wish to discuss concern about working with such equipment refer to Occupational Health.

13
Appendix 2
RISKS AND MITIGATIONS OF PREGNANCY
Aspect
Advice Work Aspects
Morning Sickness
Eat easily digestible food 2 hourly Ensure adequate fluid intake Avoid hunger Seek medical advice
Early shift work Nauseating smells Snack facility
Heartburn
As above When resting use pillows to prop up upper body
As above
Backache
Avoid manual handling Avoid standing for long periods Seek medical advice See advice from physiotherapist
Standing Manual Handling
Varicose Veins Avoid constrictive garments Avoid standing for long periods When sitting try to elevate feet using a foot stool Seek medical advice
Standing / Sitting
Tiredness Frequent rest periods Gentle exercise
Overtime / shifts
Frequent visits to the toilet Maintain good fluid intake Access to toilet
Increasing abdominal size Frequent rest periods Use of PPE Working space Manual Handling
Fainting Avoid sudden changes in posture Avoid standing for long periods Seek medical advice
Confined space Sharps
Balance Avoid rushing Wear suitable footwear / clothing
Slippery / wet surfaces
14
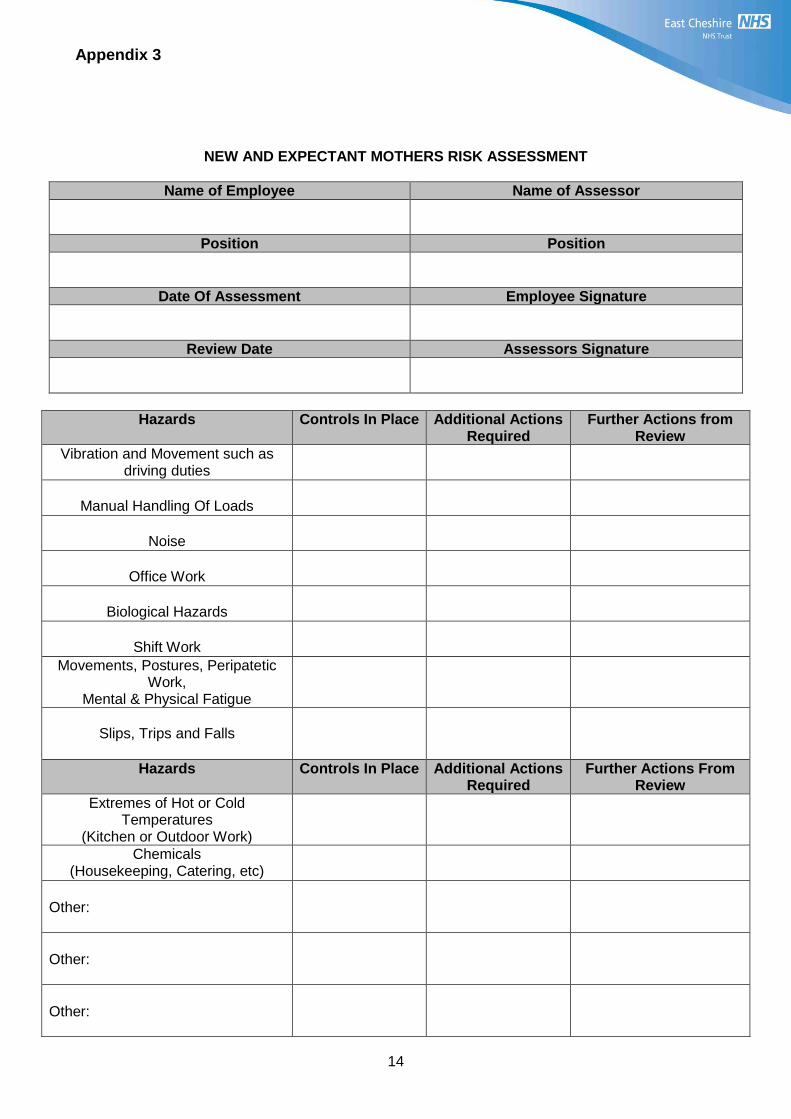
Appendix 3
NEW AND EXPECTANT MOTHERS RISK ASSESSMENT
Name of Employee Name of Assessor
Position Position
Date Of Assessment Employee Signature
Review Date Assessors Signature
Hazards Controls In Place Additional Actions Required
Further Actions from Review
Vibration and Movement such as driving duties
Manual Handling Of Loads
Noise
Office Work
Biological Hazards
Shift Work
Movements, Postures, Peripatetic Work,
Mental & Physical Fatigue
Slips, Trips and Falls
Hazards Controls In Place Additional Actions Required
Further Actions From Review
Extremes of Hot or Cold Temperatures
(Kitchen or Outdoor Work)
Chemicals (Housekeeping, Catering, etc)
Other:
Other:
Other:

15
Appendi
Equality Analysis (Impact assessment) Please START this assessment BEFORE writing your policy, procedure, proposal, strategy or service so that you can identify any adverse impacts and include action to mitigate these in your finished policy, procedure, proposal, strategy or service. Use it to help you develop fair and equal services. Eg. If there is an impact on Deaf people, then include in the policy how Deaf people will have equal access. 1. What is being assessed?
New and Expectant Mothers Risk Assessment Policy
Details of person responsible for completing the assessment:
Name:Tina Platt
Position:Health and Safety Manager
Team/service: Health & Safety
State main purpose or aim of the policy, procedure, proposal, strategy or service: (usually the first paragraph of what you are writing. Also include details of legislation, guidance, regulations etc which have shaped or informed the document)
To ensure the Health and Safety of New and Expectant Mothers in the Workplace
2. Consideration of Data and Research
To carry out the equality analysis you will need to consider information about the people who use the service and the staff that provide it. Think about the information below – how does this apply to your policy, procedure, proposal, strategy or service
2.1 Give details of RELEVANT information available that gives you an understanding of who will be affected by this document
Cheshire East (CE) covers Eastern Cheshire CCG and South Cheshire CCG. Cheshire West & Chester (CWAC) covers Vale Royal CCG and Cheshire West CCG. In 2011, 370,100 people resided in CE and 329,608 people resided in CWAC.
Age: East Cheshire and South Cheshire CCG’s serve a predominantly older population than the national average, with 19.3% aged over 65 (71,400 people) and 2.6% aged over 85 (9,700 people). Vale Royal CCGs registered population in general has a younger age profile compared to the CWAC average, with 14% aged over 65 (14,561 people) and 2% aged over 85 (2,111 people). Since the 2001 census the number of over 65s has increased by 26% compared with 20% nationally. The number of over 85s has increased by 35% compared with 24% nationally. Race:

16
In 2011, 93.6% of CE residents, and 94.7% of CWAC residents were White British
5.1% of CE residents, and 4.9% of CWAC residents were born outside the UK – Poland and India being the most common
3% of CE households have members for whom English is not the main language (11,103 people) and 1.2% of CWAC households have no people for whom English is their main language.
Gypsies & travellers – estimated 18,600 in England in 2011. Gender: In 2011, c. 49% of the population in both CE and CWAC were male and 51% female. For CE, the assumption from national figures is that 20 per 100,000 are likely to be transgender and for CWAC 1,500 transgender people will be living in the CWAC area. Disability:
In 2011, 7.9% of the population in CE and 8.7% in CWAC had a long term health problem or disability
In CE, there are c.4500 people aged 65+ with dementia, and c.1430 aged 65+ with dementia in CWAC. 1 in 20 people over 65 has a form of dementia
Over 10 million (c. 1 in 6) people in the UK have a degree of hearing impairment or deafness.
C. 2 million people in the UK have visual impairment, of these around 365,000 are registered as blind or partially sighted.
In CE, it is estimated that around 7000 people have learning disabilities and 6500 people in CWAC.
Mental health – 1 in 4 will have mental health problems at some time in their lives. Sexual Orientation:
CE - In 2011, the lesbian, gay, bisexual and transgender (LGBT) population in CE was estimated at18,700, based on assumptions that 5-7% of the population are likely to be lesbian, gay or bisexual and 20 per 100,000 are likely to be transgender (The Lesbian & Gay Foundation).
CWAC - In 2011, the LGBT population in CWAC is unknown, but in 2010 there were c. 20,000 LGB people in the area and as many as 1,500 transgender people residing in CWAC.
Religion/Belief: The proportion of CE people classing themselves as Christian has fallen from 80.3% in 2001 to 68.9% In 2011 and in CWAC a similar picture from 80.7% to 70.1%, the proportion saying they had no religion doubled in both areas from around 11%-22%.
Christian: 68.9% of Cheshire East and 70.1% of Cheshire West & Chester
Sikh: 0.07% of Cheshire East and 0.1% of Cheshire West & Chester
Buddhist: 0.24% of Cheshire East and 0.2% of Cheshire West & Chester
Hindu: 0.36% of Cheshire East and 0.2% of Cheshire West & Chester
Jewish: 0.16% of Cheshire East and 0.1% of Cheshire West & Chester
Muslim: 0.66% of Cheshire East and 0.5% of Cheshire West & Chester
Other: 0.29% of Cheshire East and 0.3% of Cheshire West & Chester
None: 22.69%of Cheshire East and 22.0% of Cheshire West & Chester
Not stated: 6.66% of Cheshire East and 6.5% of Cheshire West & Chester
Carers: In 2011, nearly 11% (40,000) of the population in CE are unpaid carers and just over 11% (37,000) of the population in CWAC.

17
2.2 Evidence of complaints on grounds of discrimination: (Are there any complaints or concerns raised either from patients or staff (grievance) relating to the policy, procedure, proposal, strategy or service or its effects on different groups?)
No
2.3 Does the information gathered from 2.1 – 2.3 indicate any negative impact as a result of this document?
No
3. Assessment of Impact Now that you have looked at the purpose, etc. of the policy, procedure, proposal, strategy or service (part 1) and looked at the data and research you have (part 2), this section asks you to assess the impact of the policy, procedure, proposal, strategy or service on each of the strands listed below.
RACE: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, racial groups differently? Yes No x
Explain your response: No differential impact identified. ______________________________________________________________________________
GENDER (INCLUDING TRANSGENDER): From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, different gender groups differently? Yes x No
Explain your response: Due to the nature of pregnancy only female staff are affected by this policy, however this would be considered a positive impact.
DISABILITY From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, disabled people differently? Yes No x
Explain your response: No differential impact identified.
______________________________________________________________________________
AGE: From the evidence available does the policy, procedure, proposal, strategy or service, affect, or have the potential to affect, age groups differently? Yes No x
Explain your response: No differential impact identified.
LESBIAN, GAY, BISEXUAL: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, lesbian, gay or bisexual groups differently? Yes No x
Explain your response: No differential impact identified. -______________________________________________________________________________

18
RELIGION/BELIEF: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, religious belief groups differently? Yes No x
Explain your response: No differential impact identified. _____________________________________________________________________________
CARERS: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, carers differently? Yes No x
Explain your response: No differential impact identified. ______________________________________________________________________________
OTHER: EG Pregnant women, people in civil partnerships, human rights issues. From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect any other groups differently? Yes x No
Explain your response: Positive impact as this policy aims to protect the Health and Safety of pregnant women.-_____________________________________________________________________________
4. Safeguarding Assessment - CHILDREN
a. Is there a direct or indirect impact upon children? Yes x No
b. If yes please describe the nature and level of the impact (consideration to be given to all children; children in a specific group or area, or individual children. As well as consideration of impact now or in the future; competing / conflicting impact between different groups of children and young people: Positive impact due to protection of expectant and breast feeding mothers by ensuring that satisfactory control measures are in place where risks have been identified.
c. If no please describe why there is considered to be no impact / significant impact on children
5. Relevant consultation
Having identified key groups, how have you consulted with them to find out their views and that the made sure that the policy, procedure, proposal, strategy or service will affect them in the way that you intend? Have you spoken to staff groups, charities, national organisations etc?
Indirect positive impact due to protection of expectant and breast feeding mothers by ensuring that satisfactory control measures are in place where risks have been identified.
6. Date completed: 18/08/16 Review Date: 18/08/19 7. Any actions identified: Have you identified any work which you will need to do in the future to ensure that the document has no adverse impact?
Action Lead Date to be Achieved
8. Approval – At this point, you should forward the template to the Trust Equality and Diversity Lead [email protected]
Approved by Trust Equality and Diversity Lead: Date: 18.8.16


















