Neuroplasticity in the Clinic
12
4/18/12 1 Neuroplasticity in the Clinic: U(lizing Evidence To Maximize Par(cipa(on in Occupa(on for Individuals With Stroke Christine Griffin, OTR/L MS,BCPR Ohio State University Medical Center – Dodd Hall [email protected] Evolu(on of Rehab Interven(on • Evidence Based Prac(ce – Are we able to prove that what we are doing is effec(ve? • AOTA Centennial Vision • Closely examine what our interven(on for survivors of stroke require and what is effec(ve Neurofacilitation Techniques • Brunnstrom’s Movement Theory – Limited Evidence • Wagennar et al. (1990) – Brunnstrom phases vs NDT phases, n = 7 – One par(cipant performed be]er with Brunnstrom than NDT • Sawner & LaVigne, 1992 – Studies cited to support the approach were published between 18981960 Neurofacilitation Techniques • Propriocep(ve Neuromuscular Facilita(on – Smedes, 2006 Systema(c review of 4 RCT • In a home and structured program Inclusive PNF is effec(ve, treadmill training is more effec(ve than PNF on gait, and NMES is more effec(ve than PNF on hand func(on • Rood – No Evidence Neurofacilitation Techniques • NDT/Bobath – Langhammer et al, 2000 • Motor learning be]er than Bobath – Tang et al, 2005 • Task oriented approach be]er than NDT – Hafsteonsdodr et al, 2005 n=324 • Bobath vs standard therapy • No difference, Bobath group had more treatment sessions – Systema(c Review – Kollen et al. (2009) Bobath Concept is not superior to other approaches – Rao (2011) Lack of effec(veness of the Bobath approach when compared with a taskoriented approach Neurofacilitation Techniques • Proprioceptive Neuromuscular Facilitation, Rood, and Brunnstrom Approach – Evidence “sparse and inconclusive” (Sabari, 2010) – Based on outdated views of motor recovery and motor control (Ma & Trombly, 2002; Pollock, Baer, Pomeroy, & Langhorne, 2007; Steultjens et al., 2003) • Neurodevelopment Treatment – No evidence of significantly better outcomes for NDT when compared with other treatments to improve upper limb motor function (Luke, Dodd, & Brock, 2004; Packi, 2003)
Transcript of Neuroplasticity in the Clinic

4/18/12
1
Neuroplasticity in the Clinic: U(lizing Evidence To Maximize Par(cipa(on in Occupa(on for Individuals With Stroke
Christine Griffin, OTR/L MS,BCPR Ohio State University Medical
Center – Dodd Hall [email protected]
Evolu(on of Rehab Interven(on
• Evidence Based Prac(ce – Are we able to prove that what we are doing is effec(ve?
• AOTA Centennial Vision • Closely examine what our interven(on for survivors of stroke require and what is effec(ve
Neurofacilitation Techniques
• Brunnstrom’s Movement Theory – Limited Evidence
• Wagennar et al. (1990) – Brunnstrom phases vs NDT phases, n = 7 – One par(cipant performed be]er with Brunnstrom than NDT
• Sawner & LaVigne, 1992 – Studies cited to support the approach were published between 1898-‐1960
Neurofacilitation Techniques
• Propriocep(ve Neuromuscular Facilita(on – Smedes, 2006 Systema(c review of 4 RCT
• In a home and structured program Inclusive PNF is effec(ve, treadmill training is more effec(ve than PNF on gait, and NMES is more effec(ve than PNF on hand func(on
• Rood – No Evidence
Neurofacilitation Techniques • NDT/Bobath
– Langhammer et al, 2000 • Motor learning be]er than Bobath
– Tang et al, 2005 • Task oriented approach be]er than NDT
– Hafsteonsdodr et al, 2005 n=324 • Bobath vs standard therapy • No difference, Bobath group had more treatment sessions
– Systema(c Review – Kollen et al. (2009) Bobath Concept is not superior to other
approaches – Rao (2011) Lack of effec(veness of the Bobath approach when
compared with a task-‐oriented approach
Neurofacilitation Techniques
• Proprioceptive Neuromuscular Facilitation, Rood, and Brunnstrom Approach – Evidence “sparse and inconclusive”
(Sabari, 2010) – Based on outdated views of motor recovery and motor control
(Ma & Trombly, 2002; Pollock, Baer, Pomeroy, & Langhorne, 2007; Steultjens et al., 2003)
• Neurodevelopment Treatment – No evidence of significantly better outcomes for NDT when
compared with other treatments to improve upper limb motor function (Luke, Dodd, & Brock, 2004; Packi, 2003)

4/18/12
2
Shig in Rehabilita(on Approach
• Self Examina(on • Interven(on supported by Evidence and Research
• Paradigm shig from tradi(onal theories to Neuroplas(city
Neuroplasticity – What is it?
• Neuroplas(city à Changing the brain • Capability of CNS to alter func(on and structure in response to use and motor learning
• Reorganiza(on of undamaged systems in the brain
• The brain responds to func(onal/ environmental demands
• Occurs ager Repe((ve Prac(ce (Lundy-‐ Ekman, 2007, Kass, 1991, Donoghue et al, 1991)
Neuroplasticity
• Borders of neuro mapping are not defined – Brain is moldable according to the will and
actions of the individual • Nudo (2001)
– Adaptive plasticity in motor cortex – Functional and structural dynamic nature of
the cerebral cortex
Neuroplasticity • Possible Explanations
– Areas of the brain assume functions that were once the responsibility of a damaged area of the brain
– Areas of the brain lay dormant until needed to assume functioning for damaged regions
– Creating new pathways for the connections between neurons
(Gutman, 2008)
Repetitive Practice
• High Intensity/ High Repetition → Cortical Changes
• Motivational Strategies for Patient – Self control vs. External Control
• Patient education – Importance of intensity of repetition – Intensive HEP
Learned Non- Use
• Decrease is muscle/ motor activity → decrease in function → frustration → avoidance of activity
• What happens cortically? • Kleim (1998)
– Motor cortex representation diminishes with immobilization beyond nine days

4/18/12
3
Neuroplasticity is Skill/ Activity Dependent
• Nudo, 2001 – Plasticity is limited to behavioral experiences
• Nudo, 2003 – Plasticity of the motor cortex are skill-
dependent rather than simply use dependent. • Cauragh, 2005
– Upper extremity gains evolve from motor experiences and activity-dependent interventions
Chronic Recovery
• Thickbroom, 2004 – Purpose: Investigate the relationship between
changes in motor cortex organization and degree of motor function after stroke
– Subjects: 27 pt’s with upper limb motor deficits up to 23 yrs after onset
– Intervention: The hand’s corticomotor area was mapped with transcranial magnetic stimulation. Motor Assessment Scale and grip strength measurement were used as functional assessments. Task oriented treatment was provided
Thickbroom (Clin Neurophysiol 2004)
– Results: After treatment, motor maps of the hand showed displacement in 17 pt’s. Ten pt’s showed normalization of corticospinal conduction and a positive correlation between the magnitude of the map shift and grip strength in the affected hand.
– Conclusion: The present findings provide evidence that cortical plasticity and reorganization occurring after a stroke is functionally significant.
Neuroplasticity
• Active repetitive task oriented motion
Methods of Neuroplasticity
• Constraint Induced Movement Therapy • Task Based Practice • Mental Practice • Mirror Therapy • NMES • Bilateral Training
Constraint Induced Movement Therapy (CIMT)
• Forced use to counteract learned nonuse – Pa(ent unsuccessful with use of affected limb, so would stop ini(a(ng use of limb during tasks
• Restraint of unaffected hand/ arm
• Motor inclusion criteria – 10 MCP extension and 20° wrist extension – Distal func(on is a cri(cal factor
(Wolf, 2006)

4/18/12
4
Constraint Induced Movement Therapy (CIMT)
• Main factor – Massed prac(ce during repe((ve func(onal ac(vi(es • Restric(on of less effected arm 90% of day during a 2 week period
• Par(cipa(on in upper limb therapy program 6hrs/day during the 2 week period
• Shaping is very important (picking appropriate ac(vi(es) – Select tasks that address the motor impairment and pa(ent is able to carry out parts of the motor sequence
– Has direct rela(onship to success of treatment (Taub et al, 1999)
EXCITE: Trial, Wolf et al, 2006
• EXCITE: Extremity Constraint – Induced Therapy Evaluation – Multi-Center, 222 subjects, over 3 yrs – 6 hrs/ day, 5 days/ week, 2 weeks – Significant improvement in Wolf Motor
Function Test and Motor Activity Log – Lasted 24 months later
CIMT
• Neuroplas(cty – Induces cor(cal representa(on of the affected upper limb
• Effects sustained for at least 2 years ager interven(on • Beneficial treatment for pa(ents with some ac(ve wrist
and hand mo(on • Taub et al, 2006 • Boake et al, 2007 • Dahl et al, 2008 • Myint et al, 2008
Modified CIMT
• Dosing – Restric(on of less effected arm 5 hrs/day, 5 days/wk
– Par(cipa(on in upper limb therapy program 1 hr/ day, 3 days/ week, 10 weeks
• mCIMT performed be]er on Fugl-‐Meyer and Ac(on Research Arm test than “usual care” following treatment and at 12 month follow up
(Page et al, 2002, 2004, 2005)
CIMT -‐Timing • Teasel, ebrsr.com • Acute
– “There is conflic(ng evidence of benefit of CIMT in comparison to tradi(onal therapies in the acute stage of stroke”
• Chronic – “There is strong evidence of benefit of CIMT and mCIMT in comparison to tradi(onal therapies in the chronic stage of stroke. Benefits appear to be confined to stroke pa(ents with some ac(ve wrist and hand movements, par(cularly those with sensory loss and neglect”
Task Oriented Approach
• Based on systems model of motor control and theories of motor learning
• Therapist is a teacher of motor skills – Select contextually appropriate func(onal tasks – Vary tasks to increase transfer of learning – Structure the environment the condi(ons of the task are present
– Provide feedback (Carr and Shepherd, 2003, and Gen(le, 2000)

4/18/12
5
Posi(ve Effects of Task Oriented Approach on Impairment level and Func(on
• Barker et al., 2008 • Blennerhasset et al., 2004 • Caraugh et al., 2006 • Michaelson et al., 2006 • Nelles et al.,2001 • Stinear et al., 2008 • Theilman et al., 2004 • Winstein et al, 2004
Task Oriented Approach
• Hubbard et al, 2009, Systema(c Review – “We recommend that task-‐specific training be rou(nely applied by occupa(onal therapists as a component of their neuromotor interven(ons, par(cularly in management related to post-‐stroke upper limb recovery”
Task Based Practice Opportunities
• Improved function of hemiplegic upper limb when using functional objects and activities vs. performing similar movement sequences in the absence of task performance – (Wu, Trombly, Lin, and Tickle-Degnen, 1998; Trombly and
Wu, 1999; Wu, Trombly, Lin, and Tickle-Degnen, 2000; Fasoli, Trombly, Tickle-Degnen, and Verfaellie, 2002; Smedley et al., 1986; Winstein et al., 2004)
• Client’s are not making connection between non-functional activities and functional outcomes
Occupa(onal Therapist Determines
• Each client’s current poten(al to relearn motor and cogni(ve skills
• How to match task-‐based challenges to each person's current poten(al
• How to modify each person’s environment to provide the appropriate balance between challenge and compensa(on – (Sabari, 2011)
Real Life Challenges
• Busy caseload • Produc(vity standards • Limited (me • Challenging pa(ents and family members • Non-‐produc(ve (me: Documenta(on, mee(ngs, in-‐services, etc.
Occupa(on Kits • Treatment kits made prior to treatment session • Lower Level – Gross Grasp
– Placing ea(ng utensils in organizer – Placing magazines in organizer – Table sedng for 8 – Removing dishes from drying rack – Placing tools in tool box – Placing CD’s in rack – Placing cooking utensils in tall container – Placing folded socks in bin/ drawer – Placing cans/jars on shelving

4/18/12
6
Occupa(on Kits Higher Level – Bilateral coordina(on and fine motor coordina(on
– Folding clothes in laundry basket
– Hanging clothes on retractable clothes line
– Packing a suitcase with clothes – Pudng ba]eries in remote
control – Pudng toilet paper on holder
and pull off a sheet – Installing toilet paper holder
on base – Sanding plywood – Installing a door knob – Installing a smoke alarm
– Sor(ng and assembling assorted sized nuts and bolts
– Separa(ng and placing play money in wallet
– Coins in coin bank or change purse
– Medica(on into pill organizer – Wrapping a gig/ package – Stuffing envelopes – Sor(ng paper clips – Cudng and stapling paper – Sor(ng coupons – Scrap booking
Mental Practice - Imagery
• Rehearsing task or series of tasks mentally – Cognitive Rehearsal
• No physical activity • Athletes – Sports psychology • Supplement conventional therapy • Used at any stage in recovery
• (Braun et al., 2006, & Jackson et al., 2001)
Mental Practice
• Activates the musculature in the same pattern that correlates with imagined movements – measurable on EMG
• Activates the cortical representation in the same pattern that correlates with imagined movements – measurable on fMRI
• Improves learning & performance • Reorganizes motor cortex - Neuroplasticity
Mental Practice
• Most plausible mechanism to explain – “Stored motor plans for executing movements
can be accessed and reinforced during mental practice”
(Page, 2001)
Mental Practice – How is it done?
• Audio recording 1. Period of deep relaxation (3-5 min.) 2. Mental Practice Portion
• Involve every aspect of the experience including size of room, and full description of the movement including the feel of the movement.
• “Imaging you are sitting in your favorite chair. The room is quite. There is a table in front of the chair” “imagine there is a cup of that table with fresh apple juice in it. Feel yourself reaching for the cup. Feel the weight of your arm as you reach out. Feel your elbow straightening and your wrist extending. Your hand opens, and your fingertips touch the cool china cup” etc.
3. Practice in the real world. Three listening sessions to one practice session
(Levine, 2009)
Page et al 2000, 2001, 2005, 2007
• Method – Tape recorded guided imagery + traditional
therapy vs. audio placebo + traditional therapy – Mentally perform series of tasks
• Ex: reach for cup – 20 min – 1 hr/ day, 2-5 sessions/ week, 4-6
weeks • Results
– Significant improvement in Fugl-Meyer and Action Research Arm Test Scores

4/18/12
7
Liu et al, 2005
• Mental imagery of specific task + traditional therapy vs. Functional training of specific task + traditional therapy
• Method – Over 3 weeks, trained to perform 3 sets of
daily tasks for 1 hr./ day • Results
– Mental imagery group had higher ADL function than functional training, no difference in Fugl-Meyer scores
Visual Mental Practice Ertelt et al, 2007
• Method – Watch video of upper limb movement &
perform movement VS. watch video of geometric shapes & perform movement
• Results – Significant improvement in video group of
upper limb movement that sustained for at least 8 weeks
Ietswaart et al, 2011
• 3 groups • Motor mental rehearsal of upper-limb motion vs
placebo non-motor mental rehearsal vs usual care • 45 min/ day, 3 sessions/ week, 4 weeks • No difference among groups on Ac(on Research Arm Test
Mental Prac(ce Evidence
• Cocharane review, 2011-‐RCT’s only – “Limited evidence that mental prac(ce in addi(on to other rehabilita(on therapies is effec(ve compared with the same therapies without mental prac(ce”
Mental Prac(ce Evidence
• Nilsen, et al., 2010 – “Consistent and posi(ve outcomes have been documented, including decreased upper extremity impairment, increased upper extremity func(on, and increase in everyday use of the limb outside of structured therapy”
• Jackson, 2001 – “Data from psychophysical, neurophysiological, and brain imaging studies support the existence of a similarity between executed and imagined ac(ons”
Systematic Reviews • Teasel, 2011 ebrsr.com
– “There is conflicting evidence that mental practice may improve upper-extremity motor and ADL performance following stroke”
– “Mental practice may result in improved motor and ADL functioning after stroke”
• Nilsen, et al., 2010 – “When added to physical practice, mental
practice is an effective intervention. Further research is warranted to determine who will benefit, dosing, and most effective protocols.”

4/18/12
8
Mirror Therapy
• Uses visual feedback about motor performance to improve rehabilita(on outcomes
• Viewing the reflec(on of unaffected arm in the mirror may act as a subs(tute for the decreased or absent propriocep(ve input
Mirror Therapy • Pa(ent seated close to table with a mirror (35 cm x 35 cm) placed ver(cally
• Involved arm behind mirror, noninvolved in front of mirror
• Complete movements with noninvolved arm • Pa(ent watching movements of noninvolved seeing the reflec(on of the hand mo(on projected over the involved hand
• Pa(ent asked to try to do the same movements with the involved hand while moving the noninvolved
• (Yavuzer et al, 2008)
Mirror Box
Photo from personal collec(on of Chris(ne Griffin. Used with permission.
Mirror Therapy -‐ Evidence • Yavuzer et al, 2008
– Standard therapy + mirror therapy vs. standard therapy – Mirror therapy group had increased hand func(on and FIM scores compared to standard therapy at 4 weeks 6 months
• Dohle et al, 2009 – Standard therapy + mirror therapy vs. standard therapy – Pa(ents with distal impairment only – Mirror therapy group regained more distal func(on, improved recovery of surface sensibility, s(mulated recovery from hemineglect
Mirror Therapy -‐ Evidence • Michielsen et al, 2011
– Standard therapy + mirror therapy vs. standard therapy
– Mirror therapy group had increased Fugl-‐Meyer scores compared to standard therapy, but did not persist at follow up. No differnece found in ARAT or ADL func(on
• Teasel, 2011 ebrsr.com – 3 RCT’s only – “There is conflic(ng evidence that mirror therapy improves motor func(on following stroke and moderate evidence that it does not reduce spas(city”
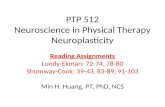
Motor Recovery and Electrical S(mula(on ager Stroke
Low
Low
High
High
Client centered
Task Specific
Cyclic E-stim
EMG- Triggered
E-stim
Functional E-stim
(Page, 2010)

4/18/12
9
Cyclic Neuro Muscular Electrical S(mula(on (NMES)
• Contracts muscles on a preset schedule, does not require active participation
• Goals – Decrease spasticity – Muscle strength – Reduce edema – Improves motor impairment in mild to
moderate stroke (Hill-‐Herman, 2010)
Electro Myograph Generated (EMG) -‐ Triggered
• Must actively move to reach established threshold to “trigger” NMES to activate
• Outcome – Increased function – Decreased motor impairment – Increase ability to concentrate (specifically on
using the affected side of the body) – Enhance behavioral training (active pt
participation) – Marked increase in reaction time – Increase AROM
(Hill-‐Herman, 2010)
EMG – Triggered NMES
• How does it work? – Set s(mula(on intensity and EMG threshold – Electrodes sense trace contrac(on/muscular a]empt – Device rewards pa(ent with s(mula(on – Begin sequence again…
(Hill-‐Herman, 2010)
EMG – Triggered NMES
Photos from personal collection of Christine Griffin. Used with permission.
EMG – Triggered NMES Video Exercise & Functional Use
Videos from personal collec(on of Chris(ne Griffin. Used with permission.
Func(onal Electrical S(mula(on (FES)
• Cyclic NMES during functional movements and functional activity
• Goals: – Improve or restore the grasp and manipulation functions
required for typical ADL task – Facilitate neuromuscular reeducation – Regulate muscle tone (decrease spasticity) – Prevent atrophy- muscle strengthening – Initiate and regain voluntary motor functions (muscle
reeducation) (Hill-Herman, 2010, Popovic et al, 2002)

4/18/12
10
FES purpose
• Adaptive • Similar to an adaptive device to be used in order to
engage in functional activity
• Therapeutic • Used during therapy in order to retrain brain and
muscles how to work and how to work together
• Supplemental • Can be used above and beyond what is done in
treatment and can be combined with other interventions
(Hill-Herman, 2010)
Traditional FES
• E-Stim applied to muscles to elicit limb movement in specific sequence during functional tasks
• NMES units, splints, and other supports may be used
• Patient actively moves limb to engage in activity (task specific and client centered)
Neuroprosthetic for FES
• Orthoses with embedded electrodes • Custom fit to individual
– Extensor panel – Flexor panel – Thumb electrode – Inserts – Straps
Neuroprosthetic for FES
Photos from personal collection of Christine Griffin. Used with permission.
Video for FES Functional Use & Gravity Eliminated AAROM
Videos from personal collec(on of Chris(ne Griffin. Used with permission.
NMES Evidence –Systematic Review
• “There is strong (Level 1a) evidence that FES treatment improves upper extremity function in acute and chronic stroke” (Teasell, 2011)
• “There is moderate evidence that EMG-triggered NMES is not superior to cyclic NMES” – Majority of studies included acute and chronic stages
of stroke – “Hypothesized that there may be a critical 5 week
time window following stroke which dexterity is most likely to be gained”
(Meilink et al, 2008)

4/18/12
11
Active Scapular Stability Home Exercise Program
(For patient with low active mobility in upper limb)
Images from Ohio State University Medical Center. Used with permission
Gravity Eliminated AAROM – Pre-Functional Level
• For patient with low active mobility in upper limb
• Stability of scapula on thoracic wall with emphasis on upward rotation
• Improves shoulder function and subluxation
Photos from personal collec(on of Chris(ne Griffin. Used with permission.
Gravity Eliminated AAROM – Pre-Functional Level
• Shoulder abduc(on • Elbow flexion and extension
• Supina(on/ Prona(on • Gross grasp
Ques(ons? • Barker RN, Brauer SG, Carson RG. (2008). Training of reaching in stroke survivors with severe and chronic upper limb paresis using a
novel nonrobotic device: a randomized clinical trial. Stroke;39:1800-1807 • Blennerhassett J, Dite W (2004). Additional task-related practice improves mobility and upper limb function early after stroke: a
randomized control trial. Australian Journal of Physiotherapy 50(4):219-224. • Boake C, Noser EA, Ro T, et al (2007). Constraint induced movement therapy during early stroke rehabilitation. Neurorehabil Neural
Repair 21(1):14-24 • Braun SM, Beurskens AJ, Borm PJ, et al: The effects of mental practice in stroke rehabilitation: a systematic review. Arch Phys Med
Rehabilitation 87(6):842-852, 2006 • Carr, JH, Shephard, RB. (2003). Stroke Rehabilitation: guidelines for exercise and training to optimize motor skill, Oxford, Butterworth-
Heinermann • Cauraugh JH, Kim SB. (2003). Stroke motor recovery: active neuromuscular stimulation and repetitive practice schedules. J Neurol
Neurosurg Psychiatry;74(11):1562-6. • Dahle AE, Askim T, Stock R, et al (2008). Short and long term outcome of constraint induced induced movement therapy after stroke: a
randomized control feasibility trial. Clin Rehabil 22(5):436-447. • Dohle C, Pullen J, Nakaten A, et al: Mirror Therapy Promotes Recovery From Severe Hemiparesis: A Randomized Controlled Trial. Neurorehabil
Neural Repair 3(3): 209-‐217, 2009. • Donoghue JP, Hess G, Sanes JN. Motor cortical substrates and mechanics for learning. In: Bloedel JR, Ebner TJ, Wise SP (Eds),
Acquisition of motor behavior in vertbrates. MIT 1991;Cambridge MA:363-86. • Ertelt D, Small S, Solodkin A, De]mers C, McNamara A, Binkofski F. (2007) Ac(on Observa(on has posi(ve impact on rehabilita(on of motor
deficits ager stroke. Neuroimage;36:164-‐173. • Fasoli, S.E, Trombly, C.A., Tickle-Degnen, L., & Verfaellie, M.H. (2002) Effect of instructions on functional reach in persons with and
without cerebrovascular accident. American Journal of Occupational Therapy, 56, 380-390. • Gentile, AM. (2000). Skill acquisition: action, movement, and neuromotor process. In Carr J, Shepard RB, editors: Movement science:
foundations for physical therapy in rehabilitation, Gaithersburg, MD 2000, Aspen. • Gillen, G. (2011). Upper extremity function and management. In Gillen, G. (ed) Stroke Rehabilitation: A Function-Based Approach, 3rd
edition, St. Louis, Elsevier Science/Mosby • Gutman, Sharon. (2008) Quick Reference Neuroscience for Rehabilitation Professionals: The Essential Neurologic Principles
Underlying Rehabilitation Practices. (2nd ed.) Slack Incorporated: Thorofore, NJ, 221. • Hafsteinsdottir TB, Algra A, Kappelle JL, Grypdonck MHF: Neurodevelopmental treatment after a stroke: a comparative study. J Neurol
Neurosurg Psychiatry 76(6):788-792. • Hill-Herman, V. (2010). Maximizing Participation in Occupation for Individuals With Stroke: The Hemiplegic Shoulder and Incorporating
Functional Electrical Stimulation Into Practice. AOTA Conference, Orlando FL
• Hubbard IJ, Parsons MW, Neilson C, Carey LM. (2009). Task-specific training: evidence for and translation to clinical practice. Occupational Thearpy International 16(3-4):175-89.
• Ietswaart M, Johnston M, Dijkerman HC, Joice S, Scott CL, MacWalter RS et al. (2011). Mental practice with motor imagery in stroke recovery: randomized controlled trial of efficacy. Brain; 134(Pt 5):1373-1386.
• Jackson PL, Lafleur MF, Malouin F, et al: Potential role o mental practice using motor imagery in neurological rehabilitation. Arch Phys Med Rehabilitation 82(8):1133-1341, 2001.
• Kleim, J., Barbay S., and Nudo, R.J. (1998). Functional reorganization of the rat motor cortex following motor skill learning. Journal of europhysiology, 80(6):3321-5.
• Kraft GH, Fitts SS, Hammond MC (1992). Techniques to improve function of the arm and hand in chronic hemiplegia. Archives of Physical Medicine and Rehabilitation 73:220-227.
• Langhammer B, Stanghelle JK (2000). Bobath or motor learning program? A comparison of two different approaches of physiotherapy in stroke rehabilitation: a randomized controlled study. Clinical Rehabilitation 14(4):361-369
• Levine, P. (2009). Stronger after stroke: Your roadmap to recovery, Demos Medical Publishing, New York. • Liu, K. P., Chan, C. C., Lee, T. M., & Hui-Chan, C. W. (2004). Mental imagery for promoting relearning for people after stroke: A
randomized controlled trial. Archives of Physical Rehabilitation, 85, 1403-1408. • Luke, C., Dodd, K. J., & Brock, K. (2004). Outcomes of the Bobath concept on upper limb recovery following stroke. Clinical
Rehabilitation, 18, 952-959. • Lundy- Ekman, Laurie. (2007) Neuroscience: Fundamentals for Rehabilitation. (3rd ed.) Chapter 4: Neuroplasticity. Saunders
Elsevier: St. Louis, MO. • Ma, H-I., & Trombly, C.A. (2002). A synthesis of the effects of occupational therapy for persons with stroke, part II: Remediation.
American Journal of Occupational Therapy, 56, 260-274. • Meilink A, Hemmen B, Seelen HA, Kwakkel G (2008). Impact of EMG-triggered neuromuscular stimulation of the wrist and finger
extensors of the paretic hand after stroke: a systematic review of the literature. Clin Rehabil 22:291-305. • Michaelsen SM, Dannenbaum R, Levin MF. (2006). Task-specific Training With Trunk Restraint on Arm Recovery in Stroke.
Stroke;37:186-192. • Michielsen ME, Selles RW, van der Geest JN, Eckhardt M, Yavuzer G, Stam HJ et al. (2011) Motor recovery and cortical
reorganization after mirror therapy in chronic stroke patients: a phase II randomized controlled trial. Neurorehabil Neural Repair, 25(3):223-233.
• Myint JM, Yuen GF, Yu TK, et al (2008). A study of constraint induced movement therapy in subacute stroke patients in Hong Kong. Clin Rehabil 22(2):112-124.
• Nelles G, Jentzen W, Jueptner M, et al (2001) Arm training induced brain plasticity in stroke studied with serial positron emission tomography. Neuroimage 13(6 pt 1):1146-1154,
• Nilsen, D.M., Gillen, G., & Gordon, A.M. (2010). Use of mental practice to improve upper-limb recovery after stroke: A systematic review. American Journal of Occupational Therapy, 64, 604-708.
• Nudo R., (2003). Adaptive plasticity in motor cortex: implications for rehabilitation after brain injury, Journal of Rehabilitation Medicine 41 Suppl:7-10.
• Nudo RJ, Plautz EJ, Frost SB. (2001) Role of Adaptive plasticity in recovery of function after damage to motor cortex. Muscle Nerve 24(8):1000-1019
• Packi, M. (2003). Physiotherapy based on the Bobath concept for adults with post stroke hemiplegia: A review of effectiveness studies. Journal of Rehabilitation Medicine, 35, 2-7.
• Page, S. J. (2000). Imagery improves upper extremity motor function in chronic stroke patients: A pilot study. OTJR: Occupation, Participation and Health, 20, 201-213.
• Page, S. J., Levine, P., Sisto, S. A., & Johnston, M. V. (2001). Mental practice combined with physical practice for upper-limb motor deficits in subacute stroke. Physical Therapy, 81, 1455-1462.
• Page, S. J., Levine, P., & Leonard, A. C., (2005). Effects of mental practice on affected limb use and function in chronic stroke. Archives of Physical Medicine and Rehabilitation, 86, 399-402.
• Page, S. J., Levine, P., & Leonard, A. C., (2005). Modified constraint induced movement therapy in acute stroke: a randomized controlled pilot sudy. Neurorehabil Neural Repair 19(1):27-32
• Page, S. J., Levine, P., & Hill, V. (2007). Mental practice as a gateway to modified constraint-induced movement therapy: A promising combination to improve function. American Journal of Occupational Therapy, 61, 321-327.
• Page, S.L., & Levine, P. (2006). Back from the brink: Electromyography-triggered stimulation combined with modified constraint –induced movement therapy in chronic stroke. Archives of Physical Medicine and Rehabilitation, 87, 27-31.
• Page SJ, Sisto SA, Johnston MV et al (2002). Modified constraint induced movement therapy after subacute stroke: a preliminary study. Neurorehabil Neural Repair 16(3):290-295.
• Page SJ, Sisto SA, Lavine P et al (2001). Modified constraint induced movement therapy: a randomized feasibility and efficacy study. J Rehabil Res Dev 38(5):583-590.
• Page SJ, Sisto SA, Lavine P, McGrath RE (2004). Efficacy of modified constraint induced movement therapy in chronic stroke: a single blinded randomized controlled trial. Arch Phys Med Rehabil 85(1):14-18.
• Page SJ (2010) in Hill-Herman, V. (2010). Maximizing Participation in Occupation for Individuals With Stroke: The Hemiplegic Shoulder and Incorporating Functional Electrical Stimulation Into Practice. AOTA Conference, Orlando FL
• Pollock, A., Baer, G., Pomeroy, V., & Langhorne, P. (2007) Physiotherapy treatment approaches for the recovery of postural control and lower limb function following stroke. Cochrane Database of Systemic Reviews, Issue No 1, Art. No. CD001920.

4/18/12
12
• Popovic MR, Popovic DB, Keller T (2002). Neuroprostheses for grasping. Neurol Res, 24(5):443-452. • Sabari, J (2011) Activity-Based Intervention in Stroke Rehabilitation In Gillen, G. (ed) Stroke Rehabilitation: A Function-Based Approach, 3rd edition,
St. Louis, Elsevier Science/Mosby • Sebari, J, (2010). Occupational Therapy Practice Guidelines for Adults with Stroke, Bethesda, AOTA Press • Steultjens, E. M. J., Dekker, J., Bouter, L.M., van de Nes, J. C. M., Cup E. H. D., & van de Ende, C. H. M. (2003). Occupational therapy for stroke
patients: A systematic review. Stroke, 34, 678-687. • Stinear CM, Barber PA, Coxon JP, Fleming MK, Byblow WD. (2008). Priming the motor system enhances the effects of upper limb therapy in chronic
stroke. Brain;131:1381-1390. • Tang QP, Yang QD, Wu YH, et al (2005). Effects of problem oriented willed movement therapy on motor abilities for people with post stroke cognitive
deficits. Physical therapy 85(10):1020-1033 • Taub E, Uswa]e G, Pidiki( R: Constraint-‐induced movement therapy: a new family of techniques with broad applica(on to physical rehabilita(on. J Rehabil Res
Dev 6(3):237-‐251, 1999. • Taub E, Uswatte G, King DK et al. (2006). A placebo controlled trial of constraint-induced movement therapy for upper extremity after stroke. Stroke
37(4):1045=1049 • Teasell, R. (2011). Evidence based review of stroke rehabilitation, The efficacy of stroke rehabilitation. 10th ed., Canadian Stroke Network,
www.ebrsr.com • Thickbroom GW, Byrnes ML, Archer SA, Mastaglia FL (2004). Motor outcomes after subcortical stroke correlates with the degree of cortical
reorganization. Clinical Neurophysiology 115(9):2144-2150 • Theilman, G. T., Dean, C. M., & Gentile, A. M. (2004). Rehabilitation of reaching after stroke: Task-related training versus progressive resistive
exercise. Archives of Physical Medicine and Rehabilitation, 85, 1613-1618. • Weganaar RC, Meijer OG, van Wieringen PC, Kuik DJ, Hazenberg GJ, Lindeboom J, Wichers F, Rijswijk H (1990). The functional recovery of stroke:
a comparison between neuro-developmental treatment and the Brunnstrom method. Scandinavian Journal of Rehabilitation Medicine 22(1):1-8 • Winstein, C. J., Rose, D. K., Tans, S. M., Lewthwaite, R., Chui, H. C., & Azen, S. P. (2004). A randomized comparison of upper-extremity
rehabilitation strategies in acute stroke: A pilot study of immediate and long-term outcomes. Archives of Physical Medicine and Rehabilitation, 85, 620-628.
• Wolf SL, Winstein CJ, Miller JP et al: Effect of constraint induced movement therapy on upper extremity func(on 3 to 9 months ager stroke: the EXCITE randomized clinical trial. JAMA 296(17):2095-‐2104, 2006.
• Wu, C., Trombly, C. A., Lin, K., and Tickle-Degnen, L. (1998). Effects of objects affordances on reaching performance in persons with and without cerebrovascular accident. American Journal of Occupational Therapy, 52, 179-187.
• Wu, C., Trombly, C. A., Lin, K., and Tickle-Degnen, L. (2000). A kinematic study of contextual effects on reaching performance in persons with and without stroke: Influences of object availability. Archives of Physical Medicine and Rehabilitation, 81, 95-101.
• Yavuzer G, Selles R, Sezer N, et al: Mirror therapy improves hand func(on in subacute stroke: a randomized controlled trial. Arch Phys Med Rehabilita9on 89(3):393-‐398, 2008