Neuropathology of fetal stage Seckel syndrome: A case report providing a morphological correlate for...
6
Case report Neuropathology of fetal stage Seckel syndrome: A case report providing a morphological correlate for the emerging molecular mechanisms Brendan Fitzgerald a , Mark O’Driscoll b , Karen Chong c , Sarah Keating a , Patrick Shannon a,⇑ a Department of Pathology and Laboratory Medicine, Mount Sinai Hospital, Toronto, Canada b Human DNA Damage Response Disorders Group, Genome Damage & Stability Centre, University of Sussex, Brighton, UK c Department of Prenatal Diagnosis & Medical Genetics, Mount Sinai Hospital, Toronto, Canada Received 5 July 2010; received in revised form 16 May 2011; accepted 17 May 2011 Abstract Seckel syndrome is a rare autosomal recessive disorder characterized by intrauterine growth retardation, dwarfism, microcephaly and mental retardation. Pathological descriptions of fetal stage Seckel syndrome are rare and pre-date the evolving understanding of the genetic and molecular mechanisms involved. The autopsy findings in a case of fetal Seckel syndrome at 30 weeks gestation are presented, with detailed description of the neuropathological findings. Severe neurological abnormalities in a male fetus were observed that included microencephaly, cortical neuronal migration disor- der, white matter tract hypoplasia/aplasia, premature depletion of the germinal matrix with cystic transformation and patchy absence of the external granular cell layer of the cerebellum. The striking neuropathological finding in this case was evidence of failure of the developing brain’s germinal elements, providing rare morphological insight into the abnormal development of the Seckel syndrome fetal brain. The selective failure of this proliferating cell population correlates with the emerging molecular evidence that Seckel syn- drome is caused by defects in ATR-dependent DNA damage signaling with resultant premature death of proliferating cells. Ó 2011 The Japanese Society of Child Neurology. Published by Elsevier B.V. All rights reserved. Keywords: Seckel syndrome; Microcephaly; Micrencephaly; Involution of germinal matrix; External granular layer of the cerebellum 1. Introduction Seckel syndrome is a rare autosomal recessive disor- der characterized by dwarfism, microcephaly and mental retardation. The facial features are distinctive and include a prominent nose with micrognathia and a receding forehead resulting in what a “bird-like” appearance [1,2]. Seckel syndrome is genetically heterogeneous with at least four known loci [3] (OMIM 210600, 606744, 608664, 601215, 605925). Seckel syndrome has been shown to be caused by defects in the ataxia telangiecta- sia and rad3-related protein (ATR) mediated response to DNA damage. The ATR-signaling pathway has a role in the response to DNA damage due to replication fork stalling and helix distorting DNA adducts [3,4]. To date, mutations in two components of this pathway have been identified, one involving ATR and the other involving the gene encoding pericentrin (PCNT) [5,6]. Homozygous disruption of ATR results in early embry- onic lethality, and adult deletion in mice leads to accel- 0387-7604/$ - see front matter Ó 2011 The Japanese Society of Child Neurology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.braindev.2011.05.007 ⇑ Corresponding author. Address: Pathology and Laboratory Medicine, Mount Sinai Hospital, 600 University Avenue, Toronto, ON, Canada M5G 1X5. Tel.: +1 416 586 5600x4101, fax: +1 416 586 8628. E-mail address: [email protected] (P. Shannon). www.elsevier.com/locate/braindev Brain & Development 34 (2012) 238–243
-
Upload
brendan-fitzgerald -
Category
Documents
-
view
212 -
download
0
Transcript of Neuropathology of fetal stage Seckel syndrome: A case report providing a morphological correlate for...

www.elsevier.com/locate/braindev
Brain & Development 34 (2012) 238–243
Case report
Neuropathology of fetal stage Seckel syndrome: A casereport providing a morphological correlate for the
emerging molecular mechanisms
Brendan Fitzgerald a, Mark O’Driscoll b, Karen Chong c, Sarah Keating a,Patrick Shannon a,⇑
a Department of Pathology and Laboratory Medicine, Mount Sinai Hospital, Toronto, Canadab Human DNA Damage Response Disorders Group, Genome Damage & Stability Centre, University of Sussex, Brighton, UK
c Department of Prenatal Diagnosis & Medical Genetics, Mount Sinai Hospital, Toronto, Canada
Received 5 July 2010; received in revised form 16 May 2011; accepted 17 May 2011
Abstract
Seckel syndrome is a rare autosomal recessive disorder characterized by intrauterine growth retardation, dwarfism, microcephalyand mental retardation. Pathological descriptions of fetal stage Seckel syndrome are rare and pre-date the evolving understanding ofthe genetic and molecular mechanisms involved. The autopsy findings in a case of fetal Seckel syndrome at 30 weeks gestation arepresented, with detailed description of the neuropathological findings.
Severe neurological abnormalities in a male fetus were observed that included microencephaly, cortical neuronal migration disor-der, white matter tract hypoplasia/aplasia, premature depletion of the germinal matrix with cystic transformation and patchy absenceof the external granular cell layer of the cerebellum. The striking neuropathological finding in this case was evidence of failure of thedeveloping brain’s germinal elements, providing rare morphological insight into the abnormal development of the Seckel syndromefetal brain. The selective failure of this proliferating cell population correlates with the emerging molecular evidence that Seckel syn-drome is caused by defects in ATR-dependent DNA damage signaling with resultant premature death of proliferating cells.� 2011 The Japanese Society of Child Neurology. Published by Elsevier B.V. All rights reserved.
Keywords: Seckel syndrome; Microcephaly; Micrencephaly; Involution of germinal matrix; External granular layer of the cerebellum
1. Introduction
Seckel syndrome is a rare autosomal recessive disor-der characterized by dwarfism, microcephaly and mentalretardation. The facial features are distinctive andinclude a prominent nose with micrognathia and areceding forehead resulting in what a “bird-like”
appearance [1,2].
0387-7604/$ - see front matter � 2011 The Japanese Society of Child Neuro
doi:10.1016/j.braindev.2011.05.007
⇑ Corresponding author. Address: Pathology and LaboratoryMedicine, Mount Sinai Hospital, 600 University Avenue, Toronto,ON, Canada M5G 1X5. Tel.: +1 416 586 5600x4101, fax: +1 416 5868628.
E-mail address: [email protected] (P. Shannon).
Seckel syndrome is genetically heterogeneous with atleast four known loci [3] (OMIM 210600, 606744,608664, 601215, 605925). Seckel syndrome has beenshown to be caused by defects in the ataxia telangiecta-sia and rad3-related protein (ATR) mediated responseto DNA damage. The ATR-signaling pathway has arole in the response to DNA damage due to replicationfork stalling and helix distorting DNA adducts [3,4]. Todate, mutations in two components of this pathway havebeen identified, one involving ATR and the otherinvolving the gene encoding pericentrin (PCNT) [5,6].Homozygous disruption of ATR results in early embry-onic lethality, and adult deletion in mice leads to accel-
logy. Published by Elsevier B.V. All rights reserved.

B. Fitzgerald et al. / Brain & Development 34 (2012) 238–243 239
erated aging and stem cell depletion [7]. ATR deficientcells exhibit impaired phosphorylation of ATR-depen-dant substrates with impaired G2/M checkpoint arrest,and exhibit a novel form of cell death (nuclear fragmen-tation) that is thought to follow from a failure to recoverfrom replication stalling, and have increased endoge-nous numbers of centrosomes in replicating cells.Impaired phosphorylation of ATR substrates is acommon feature of Seckel cell lines, but mutations inother components of the ATR pathway apart fromATR itself result in defective ATR signaling and Seckelsyndrome [6] and cells with such mutations sharefeatures with ATR deficient cells, suggesting that defectsin ATR-signaling result in premature death of replicat-ing cells. The vulnerability of rapidly replicating cellsto defects in ATR pathway signaling might lead one toexpect specific morphological evidence of failure ingerminal elements. The single previous case report onthe neuropathology of fetal stage Seckel syndromedescribed scarcity of sub-ependymal matrix cells andconcluded that microencephaly was caused by a primarydeficiency in neuroblast production [8].
2. Case report
The mother of the affected fetus was a healthy 29 yearold woman. Her partner was her first cousin. Antenatalultrasound revealed severe intrauterine growth restric-tion, arthrogryposis and microcephaly. The karyotypewas 46,XY. The pregnancy was terminated at 29 weeks6 days gestation.
3. General autopsy findings
The male fetus was small with a weight of 444 g(expected weight for gestation = 1115 g). The dysmor-phic features were typical of Seckel syndrome (Fig. 1A)with microcephaly, sloping forehead, micrognathia anda prominent nose. Eyelashes and eyebrows were absentwith scaling of the skin of the forehead and eyelids.The mouth was small with a high arched palate. Therewere joint contractures involving shoulders, elbows,wrists, hips, knees and ankles, and camptodactyly andadducted thumbs with absent palmar creases. The bowelwas malrotated. A urachal cyst was present at bladderapex.
4. Neuropathology
There was extreme microencephaly with the brainweighing 21 g (expected weight for gestation = 160 g).The cerebral convexities were entirely smooth and thetemporal lobes relatively hypoplastic (Fig. 1B and C).The ventricles were relatively large. The anterior com-missure was present. The corpus callosum was relativelyshortened in the antero-posterior dimension and only
extended posteriorly as far as the anterior thalamus.More posteriorly, longitudinal white matter bundlescoursed on either side of the midline (Fig. 1C) beforejoining the corpus callosum rostrally. The hippocampalformation was short and under-rotated but displayednormal cytoarchitectural progression. The germinalmatrices were cystic and essentially absent, but for verysmall rests of tissue (Fig. 2A and B). The cerebral cortexwas thin and showed poor demarcation from the sub-plate and areas of disorganization particularly posteri-orly and laterally on the temporal lobes, andcircumferentially around the occipital poles (Fig. 2E).Within the molecular layer of the cerebral cortex ante-ro-posteriorly directed bundles of axons were identified(Fig. 2F); these were bundles of unmyelinated cell pro-cesses that did not stain for vimentin and stained for nes-tin. Synaptophysin immunoreactivity was generallyweak in the cerebrum, but demonstrated intense reactiv-ity in the molecular layer, with decoration of Cajal Retz-ius neurons and of deep, but not superficial neocorticalneurons. Vertically oriented synaptophysin positiveaxons were present but sparse, indicating impaired mat-uration [9]. Immunohistochemistry for calretinin demon-strated intense reactivity among Cajal Retzius andsubplate neurons. The major nuclear groups of the cere-brum, thalamus, cerebellum and brainstem were readilyidentified, although small. The cerebral peduncles andmiddle cerebellar peduncles were thinned. The cortico-pontine and corticospinal tracts were severely hypoplas-tic and the cerebellar cortex thinned with shallow folia(Fig. 1D and E). The external granular cell layer of thecerebellum was irregularly thinned or absent (Fig. 2D)and laterally and dorsally there were areas in which thePurkinje cell layer was not discernable. The dentatenucleus was poorly convoluted and fragmented, andthe inferior olivary nucleus lacked crenellations(Fig. 1D). Myelination of the spinal cord and brainstemappeared appropriate for gestational age (Fig. 1E).Immunohistochemical staining for vimentin revealednormal radial and Bergmann glial cytology and normalmicrovascular throughout the brain.
Within the external granular cell layer of the cerebel-lum, we noted numerous hyperchromatic micronuclei(Fig. 3). These were also present in hyaline cartilageand the germinal layer of the kidney. They appeared tobe isolated nuclear fragments, were single, and lackedeosinophilic cytoplasm or immunohistochemical stain-ing for caspase 3a. There was no morphologically typicalapoptosis.
5. ATR-dependent G2-M checkpoint assay
Primary skin fibroblasts were cultured in MEMsupplemented with 15% FCS, L-Gln and antibiotics(Pen-Strep) and maintained in 5% CO2 at 37 �C. DNAisolated from cultured fibroblasts were extracted and

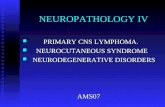
Fig. 1. (A) Autopsy photograph of intact fetus, demonstrating marked microcephaly and characteristic bird like facies, with multiple jointcontractures. (B) Intact fixed brain, demonstrating smooth hemispheres, with relative hypoplasia of temporal and (C) whole mount of hemispheresdemonstrating incomplete corpus callosum at mid thalamic level, with posterior corpus callosum replaced by parasagittal tracks (*) coursing in ananteroposterior direction, with ventriculomegaly and temporal lobe hypoplasia. (D) Whole mount of pons, demonstrating hypoplasia of basis pontis,simplification and hypoplasia of cerebellar folia and fracturing of dentate nucleus into clusters of neurons (arrows) or a thinned and irregularlycrenellated structure (arrowheads). (E) Section of rostral medulla stained with antibodies to myelin basic protein, demonstrating myelination of nerveroots and tracts, internal arcuate fibers, and the inner division of the inferior cerebellar peduncle. The inferior olivary nucleus lacks crenellations andits long axis is oriented dorsoventrally (arrowhead). Note the absence of pyramidal tracts.
240 B. Fitzgerald et al. / Brain & Development 34 (2012) 238–243
amplified for sequencing of the PCN gene: no mutationswere found. To assay for defects in the ATR signalingpathway, fibroblasts grown on coverslips were irradiatedwith 5 J/m2 UV-C in air before being re-immersed incomplete medium supplemented with nocodazole(1.5 lM) and incubated for 24 h. Cells were fixed with3.7% paraformaldehyde for 10 min, stained with DAPIand mitotic index was determined by direct fluorescencemicroscopy (Zeiss AxioPlan system). The cultured cellsdemonstrated impaired G2 checkpoint arrest (Fig. 3)
compared to controls, supporting the phenotypic diag-nosis of Seckel syndrome.
6. Discussion
Pathological descriptions of fetal stage Seckel syn-drome are rare and pre-date the evolving understandingof the genetic and molecular mechanisms involved[5,6,8,10]. The findings here suggest that the germinalelements were normally located and more voluminous

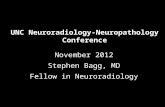
Fig. 2. Photomicrographs (original magnification �15) of germinal matrix in (A) age matched control compared to (B) cystic germinal matrix withresidual rests (arrowhead) in Seckel syndrome. (C) Cerebellar vermis in age matched control and (D) Seckel syndrome. Note that folia are present inSeckel syndrome but external granular cell layer is attenuated in multiple areas (arrowhead). (E) Temporal lobe (original magnification �12) indemonstrating (arrowhead) irregular neuronal migration with deep heterotopic neuronal masses. (F) The molecular layer contained bundles oflongitudinally directed cell processes (arrowheads, original magnification �100).
B. Fitzgerald et al. / Brain & Development 34 (2012) 238–243 241
earlier in gestation and then prematurely becamedepleted. In the germinal matrix this resulted in thenearly complete absence of germinal matrix and itsreplacement by cysts, and the external granular layerof the cerebellum was thinned and showed regions ofcomplete absence.
The molecular understanding of Seckel syndromeindicates that cell survival is reduced in due to the pres-ence of defects in the cellular response to DNA damagein proliferating cells. Indeed, cell culture studies in thisindividual demonstrated defective ATR-dependent G2-M checkpoint arrest following UV-irradiation of prolif-erating fibroblasts. The germinal components of theCNS may be susceptible to ATR defects in an additionalmanner because of the role ATR plays in centrosomestability. Within the germinal matrix symmetric mitoticcleavages result in increased neuroblast numbers
whereas asymmetric cleavages result in the generationof one neuroblast cell and one daughter neuron. Any-thing that disrupts spindle organization such as numbermay interfere with this process and reduce neuron for-mation [11,12].
Although it is difficult to identify the exact nature ofthe micronuclei noted in paraffin sections the findingsare evidence of nuclear degeneration and are notablefor their presence in areas of cellular proliferation innormal fetuses and germinal tissue hypoplasia in thisfetus. The lack of apoptosis is consistent with themodel of Seckel syndrome in which the cells do notdie by apoptosis but by nuclear fragmentation [5–7].We speculate that proliferating cell populations failedto undergo normal DNA repair in this fetus, and sounderwent nuclear fragmentation and premature celldeath.

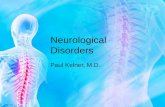
Fig. 3. Photomicrographs (hematoxylin and eosin, original magnification�400) of fetal (A) kidney, (B) cartilage and (C) cerebellar external granularcell layer, demonstrating hyperchromatic micronuclei (arrow heads). (D) Primary fetal fibroblasts from this case (Proband) exhibit a failure toactivated the ART-dependent G2-M checkpoint arrest following UV-irradiation, unlike fibroblasts from a normal individual (WT; wild-type). Afunctional checkpoint is illustrated by a UV-induced reduction in the mitotic index (mitosis %) as a consequence of arrest in G2 phase (WT).
242 B. Fitzgerald et al. / Brain & Development 34 (2012) 238–243
This autopsy provides a rare glimpse at fetal stageSeckel syndrome. We have shown a reduction in the ger-minal elements of the fetal central nervous system andexplain the reduction as due to loss and failure of thegerminal elements rather than simply ab initio reductionin their numbers. These pathological features have notbeen previously demonstrated in human material.
Our observations provide direct morphological evi-dence for premature depletion of germinal elements inthe developing brain of Seckel syndrome and thus cor-roborate the emerging ideas on molecular causation inthis syndrome.
Conflict of interest statement
None of the authors have any actual or potential con-flict of interest including any financial, personal or otherrelationships with other people or organizations withinthree (3) years of beginning the work submitted thatcould inappropriately influence (bias) this work.
Acknowledgments
The authors would like to thank the skilled services ofMs. M. Thompson and M. Cook of this department.
References
[1] Seckel HPG. Bird-headed dwarfs: studies in developmentalanthropology including human proportions. Basel, Switzer-land: Springer Karger; 1960.
[2] Majewski F, Goecke T. Studies of microcephalic primordialdwarfism I: approach to a delineation of the Seckel syndrome. AmJ Med Genet 1982;12:7–21, [Review] [49 refs].
[3] Alderton GK, Joenje H, Varon R, Borglum AD, Jeggo PA,O’Driscoll M. Seckel syndrome exhibits cellular features demon-strating defects in the ATR-signalling pathway. Hum Mol Genet2004;13:3127–38.
[4] Auclair Y, Rouget R, Affar el B, Drobetsky EA. ATR kinase isrequired for global genomic nucleotide excision repair exclusivelyduring S phase in human cells. Proc Natl Acad Sci USA2008;105:17896–901.
[5] O’Driscoll M, Ruiz-Perez VL, Woods CG, Jeggo PA, GoodshipJA. A splicing mutation affecting expression of ataxia-telangiec-tasia and Rad3-related protein (ATR) results in Seckel syndrome.Nat Genet 2003;33:497–501.
[6] Griffith E, Walker S, Martin CA, Vagnarelli P, Stiff T, Vernay B,et al. Mutations in pericentrin cause Seckel syndrome withdefective ATR-dependent DNA damage signaling. Nat Genet2008;40:232–6.
[7] Ruzankina Y, Pinzon-Guzman C, Asare A, Ong T, Pontano L,Cotsarelis G, et al. Deletion of the developmentally essential geneATR in adult mice leads to age-related phenotypes and stem cellloss. Cell Stem Cell 2007;1:113–26.
[8] Hori A, Tamagawa K, Eber SW, Westmeier M, Hansmann I.Neuropathology of Seckel syndrome in fetal stage with evidenceof intrauterine developmental retardation. Acta Neuropathol1987;74:397–401.

B. Fitzgerald et al. / Brain & Development 34 (2012) 238–243 243
[9] Sarnat HB, Flores-Sarnat L, Trevenen CL. Synaptophysinimmunoreactivity in the human hippocampus and neocortexfrom 6 to 41 weeks of gestation. J Neuropathol Exp Neurol2010;69:234–45.
[10] O’Driscoll M, Dobyns WB, van Hagen JM, Jeggo PA. Cellularand clinical impact of haploinsufficiency for genes involved inATR signaling. Am J Hum Genet 2007;81:77–86.
[11] Lu B, Jan L, Jan YN. Control of cell divisions in the nervoussystem: symmetry and asymmetry. Annu Rev Neurosci2000;23:531–56, [Review] [150 refs].
[12] O’Driscoll M, Jackson AP, Jeggo PA. Microcephalin: a causallink between impaired damage response signalling and micro-cephaly. Cell Cycle 2006;5:2339–44.