Neuromuscular DiseasesNeuromuscular Diseases Numbness + weakness could for once be the interesting...
52
Neuromuscular Diseases Numbness + weakness could for once be the interesting chart in the rack Bryan Madden PGY2 01/10/2012 Henry Ford Hospital Detroit, Michigan
Transcript of Neuromuscular DiseasesNeuromuscular Diseases Numbness + weakness could for once be the interesting...
Neuromuscular
DiseasesNumbness + weakness could for once be the interesting
chart in the rack
Bryan Madden PGY2
01102012
Henry Ford Hospital
Detroit Michigan
Objectivesbull To help you determine when to take vague complaints
such as weakness and numbness seriously
bull Ensure you get all the inservice exam questions on
neuromuscular diseases correct
bull Provide you with the differences in history and
examination that can lead you to the correct diagnosis
Case 1bull 40-year-old African American female presented to ED with
a 2 month history of worsening generalized weakness
dyspnea and that progressively worsens throughout the
day Has been to her PCP multiple times and diagnosed
with chronic fatigue
Differentialbull Myasthenic Gravis
bull Anticholinesterase Overdose
bull Guillain-Barre
bull Transverse Myelitis
bull Lambert-Eaton Myasthenic Syndrome
bull Botulism
bull Neuroparalytic envemonation (eg tick or snake bite)
bull Drug Induced Myasthenic Syndrome
bull Multiple Sclerosis
bull Vitamin B12 E or copper deficiency
Myasthenia Gravisbull Myasthenia gravis (MG) is an autoimmune disorder
affecting neuromuscular transmission leading to
generalized or localized weakness characterized by
fatigability
bull It is the most common disorder of the neuromuscular
junction
o Prevalence 20100000 in United States
Drachman DB Myasthenia gravis N Engl J Med 1994 3301797
Myasthenia Gravisbull Most common form characterized by antibodies against
post-synaptic acetylcholine receptors
bull Second group characterized by autoantibodies against
muscle specific tyrosine kinase (MuSK)o Typically more severe
bull A third group of patients has antibodies to neither AChR
nor MuSK and these patients are considered seronegative
Symptomsbull Fluctuating skeletal muscle weakness with muscle fatigue
o Usually worse in the evening or after exercise
bull Ptosis andor diplopia initial symptom in gt50
bull Weakness with prolonged chewing
bull Dropped head syndrome
bull Respiratory weakness
Diagnosisbull Tensilon (edrophonium test)
bull Ice Test
bull Serologic testing Ach-R Ab MuSK-Abo Titers correlate poorly with disease severity
bull Repetitive nerve stimulationo Progressive decline in compound muscle action potential (CMAP)
o Positive if decrement gt10
Chan KH Lachance DH Harper CM Lennon VA Frequency of seronegativity in adult-acquired generalized myasthenia gravis Muscle Nerve 200736(5)651
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Objectivesbull To help you determine when to take vague complaints
such as weakness and numbness seriously
bull Ensure you get all the inservice exam questions on
neuromuscular diseases correct
bull Provide you with the differences in history and
examination that can lead you to the correct diagnosis
Case 1bull 40-year-old African American female presented to ED with
a 2 month history of worsening generalized weakness
dyspnea and that progressively worsens throughout the
day Has been to her PCP multiple times and diagnosed
with chronic fatigue
Differentialbull Myasthenic Gravis
bull Anticholinesterase Overdose
bull Guillain-Barre
bull Transverse Myelitis
bull Lambert-Eaton Myasthenic Syndrome
bull Botulism
bull Neuroparalytic envemonation (eg tick or snake bite)
bull Drug Induced Myasthenic Syndrome
bull Multiple Sclerosis
bull Vitamin B12 E or copper deficiency
Myasthenia Gravisbull Myasthenia gravis (MG) is an autoimmune disorder
affecting neuromuscular transmission leading to
generalized or localized weakness characterized by
fatigability
bull It is the most common disorder of the neuromuscular
junction
o Prevalence 20100000 in United States
Drachman DB Myasthenia gravis N Engl J Med 1994 3301797
Myasthenia Gravisbull Most common form characterized by antibodies against
post-synaptic acetylcholine receptors
bull Second group characterized by autoantibodies against
muscle specific tyrosine kinase (MuSK)o Typically more severe
bull A third group of patients has antibodies to neither AChR
nor MuSK and these patients are considered seronegative
Symptomsbull Fluctuating skeletal muscle weakness with muscle fatigue
o Usually worse in the evening or after exercise
bull Ptosis andor diplopia initial symptom in gt50
bull Weakness with prolonged chewing
bull Dropped head syndrome
bull Respiratory weakness
Diagnosisbull Tensilon (edrophonium test)
bull Ice Test
bull Serologic testing Ach-R Ab MuSK-Abo Titers correlate poorly with disease severity
bull Repetitive nerve stimulationo Progressive decline in compound muscle action potential (CMAP)
o Positive if decrement gt10
Chan KH Lachance DH Harper CM Lennon VA Frequency of seronegativity in adult-acquired generalized myasthenia gravis Muscle Nerve 200736(5)651
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Case 1bull 40-year-old African American female presented to ED with
a 2 month history of worsening generalized weakness
dyspnea and that progressively worsens throughout the
day Has been to her PCP multiple times and diagnosed
with chronic fatigue
Differentialbull Myasthenic Gravis
bull Anticholinesterase Overdose
bull Guillain-Barre
bull Transverse Myelitis
bull Lambert-Eaton Myasthenic Syndrome
bull Botulism
bull Neuroparalytic envemonation (eg tick or snake bite)
bull Drug Induced Myasthenic Syndrome
bull Multiple Sclerosis
bull Vitamin B12 E or copper deficiency
Myasthenia Gravisbull Myasthenia gravis (MG) is an autoimmune disorder
affecting neuromuscular transmission leading to
generalized or localized weakness characterized by
fatigability
bull It is the most common disorder of the neuromuscular
junction
o Prevalence 20100000 in United States
Drachman DB Myasthenia gravis N Engl J Med 1994 3301797
Myasthenia Gravisbull Most common form characterized by antibodies against
post-synaptic acetylcholine receptors
bull Second group characterized by autoantibodies against
muscle specific tyrosine kinase (MuSK)o Typically more severe
bull A third group of patients has antibodies to neither AChR
nor MuSK and these patients are considered seronegative
Symptomsbull Fluctuating skeletal muscle weakness with muscle fatigue
o Usually worse in the evening or after exercise
bull Ptosis andor diplopia initial symptom in gt50
bull Weakness with prolonged chewing
bull Dropped head syndrome
bull Respiratory weakness
Diagnosisbull Tensilon (edrophonium test)
bull Ice Test
bull Serologic testing Ach-R Ab MuSK-Abo Titers correlate poorly with disease severity
bull Repetitive nerve stimulationo Progressive decline in compound muscle action potential (CMAP)
o Positive if decrement gt10
Chan KH Lachance DH Harper CM Lennon VA Frequency of seronegativity in adult-acquired generalized myasthenia gravis Muscle Nerve 200736(5)651
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Differentialbull Myasthenic Gravis
bull Anticholinesterase Overdose
bull Guillain-Barre
bull Transverse Myelitis
bull Lambert-Eaton Myasthenic Syndrome
bull Botulism
bull Neuroparalytic envemonation (eg tick or snake bite)
bull Drug Induced Myasthenic Syndrome
bull Multiple Sclerosis
bull Vitamin B12 E or copper deficiency
Myasthenia Gravisbull Myasthenia gravis (MG) is an autoimmune disorder
affecting neuromuscular transmission leading to
generalized or localized weakness characterized by
fatigability
bull It is the most common disorder of the neuromuscular
junction
o Prevalence 20100000 in United States
Drachman DB Myasthenia gravis N Engl J Med 1994 3301797
Myasthenia Gravisbull Most common form characterized by antibodies against
post-synaptic acetylcholine receptors
bull Second group characterized by autoantibodies against
muscle specific tyrosine kinase (MuSK)o Typically more severe
bull A third group of patients has antibodies to neither AChR
nor MuSK and these patients are considered seronegative
Symptomsbull Fluctuating skeletal muscle weakness with muscle fatigue
o Usually worse in the evening or after exercise
bull Ptosis andor diplopia initial symptom in gt50
bull Weakness with prolonged chewing
bull Dropped head syndrome
bull Respiratory weakness
Diagnosisbull Tensilon (edrophonium test)
bull Ice Test
bull Serologic testing Ach-R Ab MuSK-Abo Titers correlate poorly with disease severity
bull Repetitive nerve stimulationo Progressive decline in compound muscle action potential (CMAP)
o Positive if decrement gt10
Chan KH Lachance DH Harper CM Lennon VA Frequency of seronegativity in adult-acquired generalized myasthenia gravis Muscle Nerve 200736(5)651
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Myasthenia Gravisbull Myasthenia gravis (MG) is an autoimmune disorder
affecting neuromuscular transmission leading to
generalized or localized weakness characterized by
fatigability
bull It is the most common disorder of the neuromuscular
junction
o Prevalence 20100000 in United States
Drachman DB Myasthenia gravis N Engl J Med 1994 3301797
Myasthenia Gravisbull Most common form characterized by antibodies against
post-synaptic acetylcholine receptors
bull Second group characterized by autoantibodies against
muscle specific tyrosine kinase (MuSK)o Typically more severe
bull A third group of patients has antibodies to neither AChR
nor MuSK and these patients are considered seronegative
Symptomsbull Fluctuating skeletal muscle weakness with muscle fatigue
o Usually worse in the evening or after exercise
bull Ptosis andor diplopia initial symptom in gt50
bull Weakness with prolonged chewing
bull Dropped head syndrome
bull Respiratory weakness
Diagnosisbull Tensilon (edrophonium test)
bull Ice Test
bull Serologic testing Ach-R Ab MuSK-Abo Titers correlate poorly with disease severity
bull Repetitive nerve stimulationo Progressive decline in compound muscle action potential (CMAP)
o Positive if decrement gt10
Chan KH Lachance DH Harper CM Lennon VA Frequency of seronegativity in adult-acquired generalized myasthenia gravis Muscle Nerve 200736(5)651
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Myasthenia Gravisbull Most common form characterized by antibodies against
post-synaptic acetylcholine receptors
bull Second group characterized by autoantibodies against
muscle specific tyrosine kinase (MuSK)o Typically more severe
bull A third group of patients has antibodies to neither AChR
nor MuSK and these patients are considered seronegative
Symptomsbull Fluctuating skeletal muscle weakness with muscle fatigue
o Usually worse in the evening or after exercise
bull Ptosis andor diplopia initial symptom in gt50
bull Weakness with prolonged chewing
bull Dropped head syndrome
bull Respiratory weakness
Diagnosisbull Tensilon (edrophonium test)
bull Ice Test
bull Serologic testing Ach-R Ab MuSK-Abo Titers correlate poorly with disease severity
bull Repetitive nerve stimulationo Progressive decline in compound muscle action potential (CMAP)
o Positive if decrement gt10
Chan KH Lachance DH Harper CM Lennon VA Frequency of seronegativity in adult-acquired generalized myasthenia gravis Muscle Nerve 200736(5)651
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Symptomsbull Fluctuating skeletal muscle weakness with muscle fatigue
o Usually worse in the evening or after exercise
bull Ptosis andor diplopia initial symptom in gt50
bull Weakness with prolonged chewing
bull Dropped head syndrome
bull Respiratory weakness
Diagnosisbull Tensilon (edrophonium test)
bull Ice Test
bull Serologic testing Ach-R Ab MuSK-Abo Titers correlate poorly with disease severity
bull Repetitive nerve stimulationo Progressive decline in compound muscle action potential (CMAP)
o Positive if decrement gt10
Chan KH Lachance DH Harper CM Lennon VA Frequency of seronegativity in adult-acquired generalized myasthenia gravis Muscle Nerve 200736(5)651
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
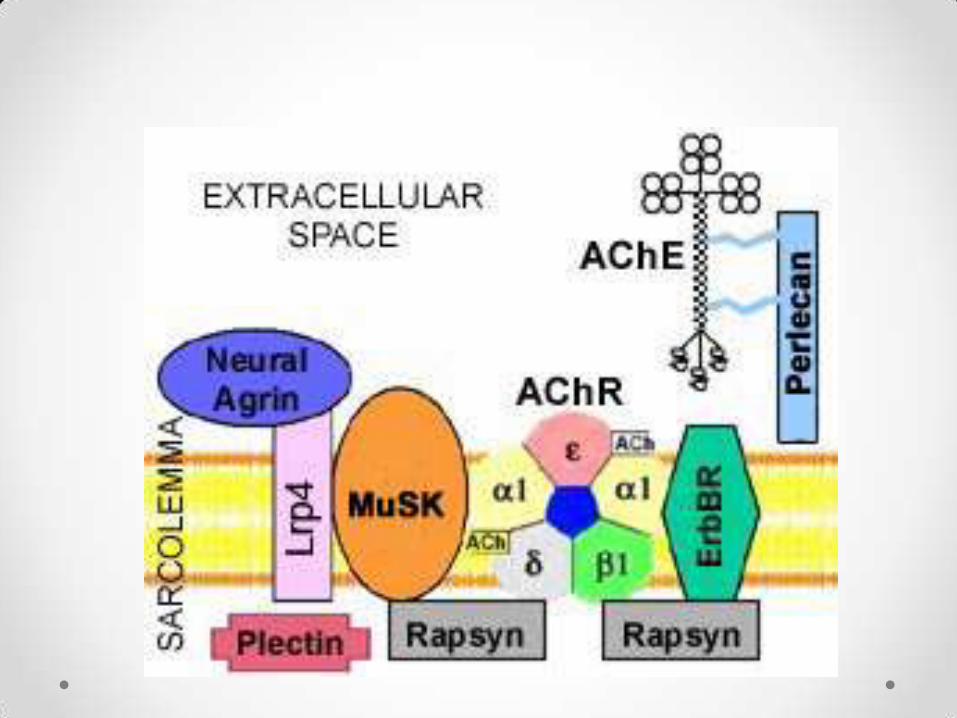
Diagnosisbull Tensilon (edrophonium test)
bull Ice Test
bull Serologic testing Ach-R Ab MuSK-Abo Titers correlate poorly with disease severity
bull Repetitive nerve stimulationo Progressive decline in compound muscle action potential (CMAP)
o Positive if decrement gt10
Chan KH Lachance DH Harper CM Lennon VA Frequency of seronegativity in adult-acquired generalized myasthenia gravis Muscle Nerve 200736(5)651
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Ice Pack Test
Browning J Wallace M Booth J Bedside testing for myasthenia gravis the ice-test Emerg Med J201128709-711 doi101136emj0620103091rep
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Myasthenic Crisisbull Complication of Myasthenia Gravis characterized by
worsening muscle weakness resulting in respiratory
failure
bull Often diagnosed byo Vital capacity (VC) lt1L (20-25mLkg)
o Negative inspiratory force (NIF) lt-20cm H2O
o Positive expiratory force (PEF) lt40cm H2O
Ahmed S Kirmani JF Janjua N et al An update on myasthenic crisis Curr Treat Options Neurol 2005 Mar7(2)129-141
Rabinstein AA Wijdicks EF Warning signs of imminent respiratory failure in neurological patients Semin Neurol 20032397-104
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
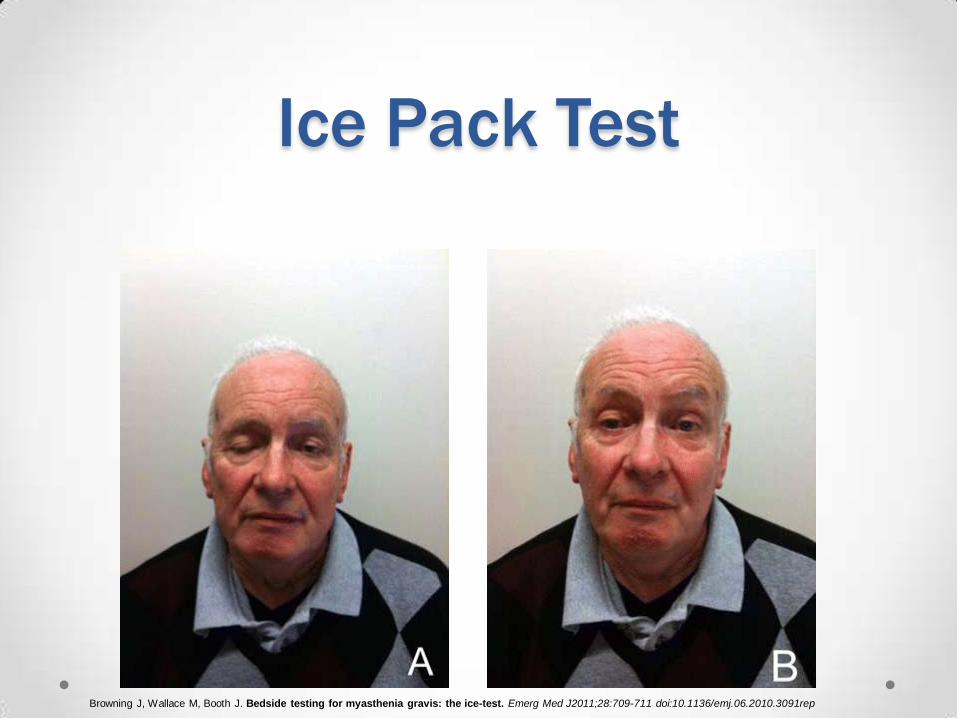
Myasthenic Crisisbull 15-20 of MG patients have at least one crisis in their
lives
bull Median time to the first crisis from onset of MG is 8-12
monthso May be the initial presentation in 15 MG patients
bull Bimodal Distributiono Early peak lt55yo women 41
o Later peak gt55yo affects men and women 11
Thomas CE Mayer SA Gungor Y et al Myasthenic crisis clinical features mortality complications and risk factors for prolonged intubation Neurology 1997481253-1260
Rabinstein AA Mueller-Kronast N Risk of extubation failure in patients with myasthenic crisis Neurocrit Care 2005 3213-215
OrsquoRiordan JI Miller DH Mottershead JP Hirsch NP Howard RS The management and outcome of patients with myasthenia gravis treated acutely in a neurological intensive care
unit Eur J Neurol 19985137-142
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Precipitantsbull Infection
bull Physical stress
bull Aspiration pneumonitis
bull Pregnancy
bull Sleep deprivation
bull Surgery
bull Emotional stress
bull Pain
bull Temperature extremes
bull α-Interferon
bull Abx (AMG ampicillin
macrolides ciprohellip)
bull Antiepileptics
bull β-Blockers
bull Ca Channel blockers
bull Contrast media
Wendell L Levine J Myasthenic Crisis The Neurohospitalist I 16-20
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Management
bull Over 20 require intubation in the ED
o Succinylcholine is less potent
o Nondepolarizing agents have increased potency
bull Noninvasive Positive-Pressure Ventilation (NPPV)
o Reduces the need for intubation
o PCO2gt 50 mmHG at baseline is predictor of failure
Kirmani JF Yahia AM Qureshi AI Myasthenic crisis Curr Treat Options Neurol 200463-15
Rabinstein A Wijdicks EF BiPAP in acute respiratory failure due to myasthenic crisis may prevent intubation Neurology 2002 59(10) 1647-1649
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Management
Intravenous Immunoglobulin (IVIg) Plasma Exchange
bull 12-2 gkg over 2-5d
bull Improvement in 4-5d
bull Contraindications
o IgA deficiency
bull Serious Complications
o Aseptic meningitis arrhythmias
thrombocytopenia thrombotic events
ATN anaphylaxis
bull One exchange every other day over
10d
bull Improvement in 2d
bull Contraindications
o Hemodynamic instability unstable
coronary diseases internal bleeding
bull Serious Complications
o Hemodynamic instability arrhythmias
myocardial infarction hemolysis
catheter related
Bertorini TE Nance AM Horner LH Greene W Gelfand MS Jaster JH Complications of intravenous gammaglobulin in neuromuscular and other diseases Muscle Nerve 1996
19388-391
Grillo JA Gorson KC Ropper AH Lewis J Weinstein R Rapid infusion of intravenous immune globulin in patients with neuromuscular disorders Neurology 2001571699-1701
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Managementbull Anticholinesterase inhibitors should be temporarily stopped
o Avoid excessive secretions in resp failure
bull Corticosteroids
o 1-15 mgkgd
o May initially worsen symptoms in 9-75
o Begins working after 2wks
bull Thymectomy
o Thymus tumors in 15-32 of people with myasthenic crisis
Pascuzzi RM Coslett HB Johns TR Long-term corticosteroid treatment of myasthenia gravis report of 116 patients Ann Neurol 198415291-298
Bae JS Go SM Kim BJ Clinical predictors of steroid-induced exacerbation in myasthenia gravis J Clin Neurosci 200631006-1010
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
St Johns MI
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Case 2bull 29yo male had a 1wk history of diarrhea 5wks ago
Presents with a 2 day history of ascending weakness
beginning in his legs
bull On examination his leg strength is 15 and his knees are
areflexic
GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

GuillainndashBarreacute Syndromebull Heterogenous group of disorders characterized by acute
polyneuropathy affecting the peripheral nervous system
Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Subtypesbull Acute inflammatory demyelinating polyradiculoneuropathy
(AIDP)
o Most common
bull Acute motor axonal neuropathy (AMAN)
o Purely motor
bull Acute motor and sensory axonal neuropathy (AMSAN)
o Sensory + motor
bull Fisherrsquos Syndromeo Triad of acute opthalmoplegia ataxia and areflexia
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
GuillainndashBarreacute Syndromebull Preceding infections
o Campylobacter jejuni Cytomegalovirus Epstein-Barr virus Mycoplasma pneumonia
Haemophilus influenza
bull Pathogenesiso Activated macrophages target antigens on Schwann cells nodes of Ranvier or
myelin sheath
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
Chiograve A Guillain-Barreacute syndrome a prospective population-based incidence and outcome survey Neurology 2003 Apr 860(7)1146-50
Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Symptomsbull First symptoms usually pain numbness parathesia or
weakness in limbs
bull Stereotypically an ascending paralysis beginning in hands
or feet
bull Infants inability suck and swallow floppy neck
generalized flaccidity
bull 25 develop respiratory weakness requiring mechanical
ventilation
bull Autonomic involvement common
Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Diagnosisbull CSF Findings elevated protein
bull Electromyography amp nerve conduction studieso Early electrodiagnostic studies abnormal in gt85
o Motor studies abnormal earliest
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
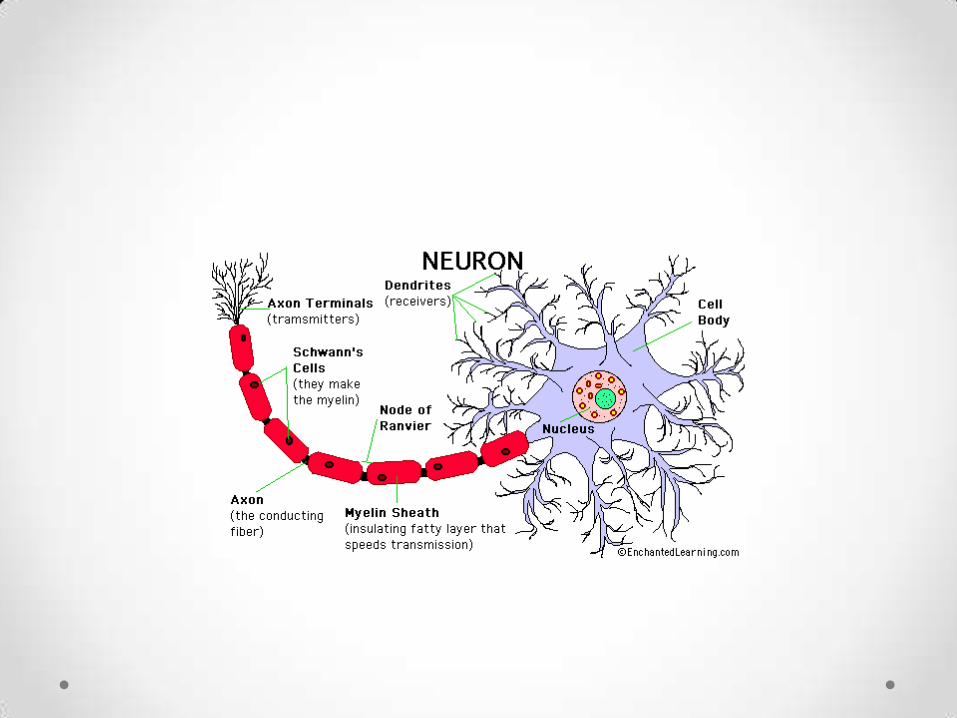
Managementbull Airway support
bull Cardiac monitoring
bull Plasma exchange (gold standard)
bull IVIg
bull Corticosteroids not recommended
Hughes RA van Doorn PA Corticosteroids for Guillain-Barreacute syndrome Cochrane Database Syst Rev 2012 Aug 158CD001446 doi
10100214651858CD001446pub4
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Prognosisbull Between 4-15 dies
bull Up to 20 are disabled after 1 yr despite treatment
bull Outcome worse in elderly
bull In children recovery is more rapid and complete
Hughes R Comblath D GuillainndashBarreacute Syndrome The Lancet Vol 366 2005
St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

St Johns MI
Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Case 3bull 35yo female awoke with dry mouth and blurred vision
which rapidly progressed over the next 2hrs to include
diplopia dysphagia and bilateral arm weakness
bull Earlier there was unrelated 20yo male who presented with
similar symptoms was immediately intubated cause
undetermined
bull Both ate at the same Italian restaurant 3 days ago
bull Vital signs normal sensation intact
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Botulismbull A rare naturally occurring disease caused by exposure to
botulism
bull Botulism is a sporulating obligate anaerobic gram-
positive bacillus ubiquitous to soil and aquatic sediment
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Chalk C Benstead TJ Keezer M Medical treatment for botulism Cochrane Database Syst Rev 2011 Mar 16(3)CD008123
Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Botulismbull Foodborne botulism
bull Infant intestinal botulism
bull Adult intestinal toxemia
bull Wound
bull Inhalation
bull Iatrogenic
Shapiro RL Hatheway C Swerdlow DL Botulism in the United States a clinical and epidemiologic review Ann Intern Med 1998 Aug 1129(3)221-8 Review
Sobel J Diagnosis and treatment of botulism a century later clinical suspicion remains the cornerstone Clin Infect Dis 2009 Jun 1548(12)1674-5
Spika JS Shaffer N Risk factors for infant botulism in the United States Am J Dis Child 1989 Jul143(7)828-32
Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Pathogenesis
bull 7 immunologically
distinct toxins (A-G)
httpmicrobewikikenyoneduindexphpFileBOTULINUM_TOXI
N_A_Mechanism_of_Actionjpg
Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Symptomsbull First nausea + vomiting
bull All forms produce syndrome of symmetrical cranial nerve
palsies followed by descending symmetric flaccid
paralysis of voluntary muscles
bull Sensory system + intellectual function unaffected
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities
Disaster Med Public Health Prep 2007 Nov1(2)122-34
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Diagnosisbull History and examination
o 2 or more cases with similar symptoms pathognomonic
bull Serum stool and any left over suspect food tested for
presence of toxin
bull C botulinum culture
bull Bioassay
Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Management
bull Call public health department if suspected
bull Human-derived botulinum immune globulin
bull Equine-derived botulinum antitoxin
bull Guanidine hydrochloride
bull 34 Diaminopyridine
bull Plasmapharesis
Kaplan JE Davis LE Narayan V Botulism type A and treatment with guanidine Ann Neurol 1979 Jul6(1)69-71
Sato Y Miyahara S Extracorporeal adsorption as a new approach to treatment of botulism ASAIO J 2000 Nov-Dec46(6)783-5
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Prognosis
bull Untreated mortality 40-50
bull Current mortality 3-5
bull With intensive care survival near 100 with or with
out antitoxin
Dembek ZF Smith LA Rusnak JM Botulism cause effects diagnosis clinical and laboratory identification and treatment modalities Disaster Med Public Health Prep 2007
Nov1(2)122-34
Gangarosa EA Boutlism in the US 1899-1969 Am J Epidemiology 1971 93 93-101
Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Mackinac City MI
Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Case 4bull 45yo female with no PMHx presented to her PCP 2 day
prior for urinary retention 1 liter was drained and she was
discharged home with antibiotics for a UTI since that time
she has developed an ascending numbness that began in
her legs and moved up to her waist
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Acute Transverse Myelitisbull Is a medical emergency
bull Focal inflammation of spinal cord of different etiologies
bull Progressive inflammation of the spinal cord over minute
hours days or even weeks
bull Incidence 46millionyear
Greenberg BM Treatment of acute transverse myelitis and its early complications Continuum (Minneap Minn) 2011 Aug17(4)733-43
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
httpimageradiologyblogspotcom201206spinal-cord-cross-sectional-anatomyhtml201206spinal-cord-cross-sectional-anatomyhtml
Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Pathogenesisbull Inflammatory infiltrates cytokines demyelination
inhibition of signal propagation neurological deficits
Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Pathogenesis
Trapp BD Axonal Transection in the Lesions of Multiple Sclerosis N Engl J Med 1998 338278-285 January 29 1998
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
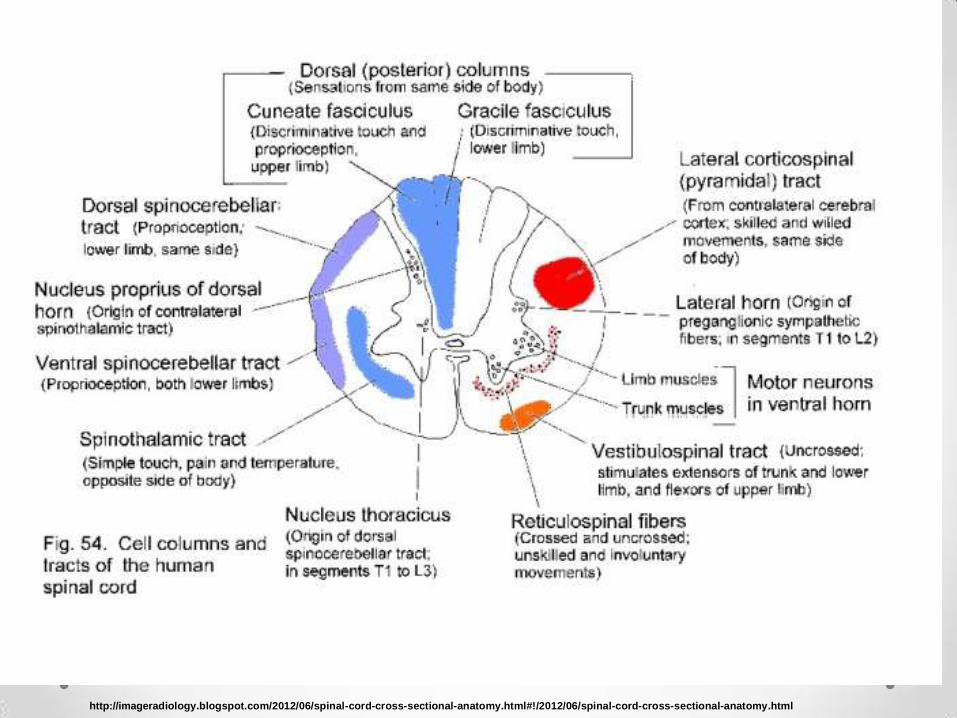
Symptomsbull Bladder dysfunction (gt99)
bull Lower limb parathesias (80-95)
bull Paraparesis (50)
bull Back pain (30-50)
bull Sensory level (eg band-like sensationpressure around
abdomen or chest ) (80)
Awad Idiopathic transverse myelitis and neuromyelitis optica clinical profiles pathophysiology and therapeutic choices Curr Neuropharmacol 2011 Sep9(3)417-28
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Diagnosisbull Hyperintense lesions on MRI (75)
bull CSF elevated protein (50) oligoclonal bands
bull May see oligoclonal bands if multiple sclerosis
A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

A 9-year-old boy suddenly
developed flaccid tetraparesis
with respiratory insufficiency and
refractory hiccups MRI showed
Longitudial extensive transverse
myelitis (LETM)in the anterior part
of the cord CSF was normal
biochemical parameters and
immunological work up were
unremarkable After corticosteroid
treatment and plasmapheresis he
was better there was no more
need for ventilation and he was
partially able to move his
extremities
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery Volume 110 Issue 9 November 2008 Pages 919ndash927
Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Managementbull No randomized double-blinded controlled treatment trials
bull Corticosteroids
bull Plasmapharesis or Plasma exchange (PLEX)
bull Immunomodulators
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
Prognosisbull Recovery usually begins within one to three months
bull Some degree of persistent disability in 40
bull Significant recovery is unlikely if there is no improvement
by three months
bull Worse outcome if rapid progression spinal shock cervical
spine involvement denervation back pain
Defresne P Hollenberg H Husson B et al Acute transverse myelitis in children clinical course and prognostic factors J Child Neurol 2003 18401
Bruna J Martiacutenez-Yeacutelamos S Martiacutenez-Yeacutelamos A et al Idiopathic acute transverse myelitis a clinical study and prognostic markers in 45 cases Mult Scler 2006 12169
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you
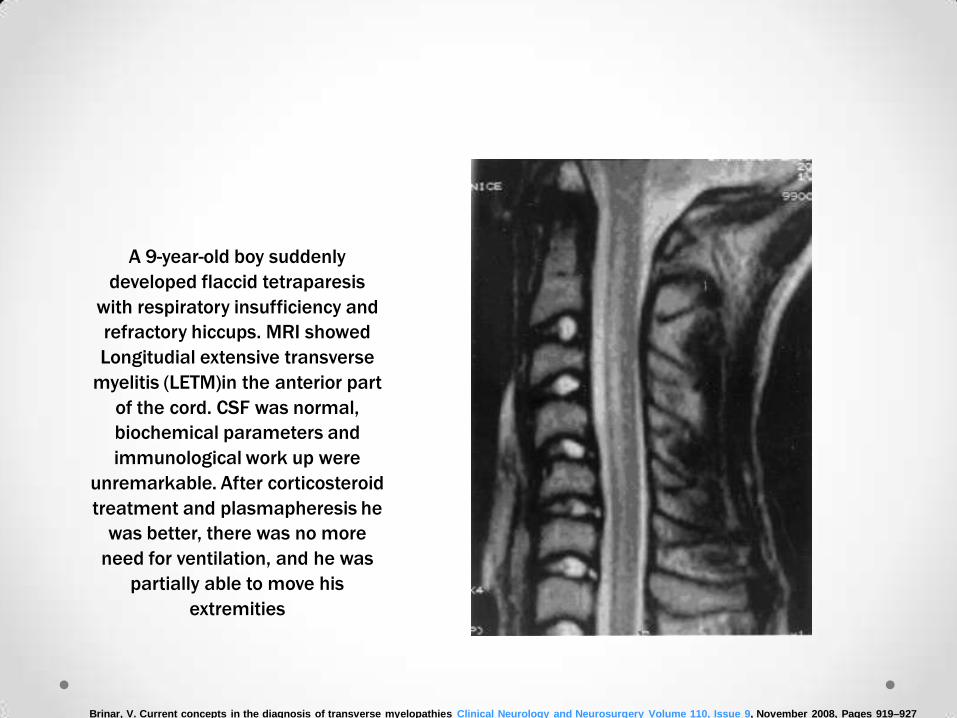
Metabolic Myelopathiesbull Vitamin B12 Deficiency
o Relative sudden onset spastic paraparesis
o Impaired perception of joint position and vibration
o Neurological symptoms may be the earliest and only sign
bull Copper Deficiencyo Malabsorption gastric surgery excessive zinc
o Subacute symptoms similar to B12
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Vascular Myelopathiesbull Vasculitis
o Polyarteritis nodosa Behcet giant cell arteritis
bull Systemic Hypoperfusiono Arrest aortic rupture aortic dissection
bull Infectiouso Syphylitic arteritis bacterial meningitis
bull Arise from hemorrhage ldquostealrdquo syndrome venous
congestion embolism
Brinar V Current concepts in the diagnosis of transverse myelopathies Clinical Neurology and Neurosurgery 110 (2008) 919ndash927
Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Summarybull Many neuromuscular diseases present with distinct
features that can be found on a thorough history and
physical examination
bull The most important theme of these diseases are early
diagnosis and admission
Thank you

Thank you