Neurology CNS Hemorrhage for OSPE
29
OSPE-Learn CNS hemorrhage O Great St. Joseph of Cupertino who while on earth did obtain from God the grace to be asked at your examination only the questions you knew, obtain for me a like favors in the examinations for which I am now preparing. In return I promise to make you known and cause you to be invoked. Through Christ our Lord. St. Joseph of Cupertino, Pray for us. Amen.
-
Upload
kavindya-fernando -
Category
Health & Medicine
-
view
456 -
download
2
Transcript of Neurology CNS Hemorrhage for OSPE

OSPE-Learn CNS hemorrhage
O Great St. Joseph of Cupertino who while on earth did obtain from God the grace to be asked at
your examination only the questions you knew, obtain for me a like favors in the examinations for
which I am now preparing. In return I promise to make you known and cause you to be invoked.
Through Christ our Lord.
St. Joseph of Cupertino, Pray for us.
Amen.

This is intraventricular hemorrhage (IVH) which arose in the subependymal region (germinal matrix) of a 28 week gestational age newborn. The germinal matrix region is very susceptible to such lesions at this period of development, leading to IVH as a complication of prematurity.
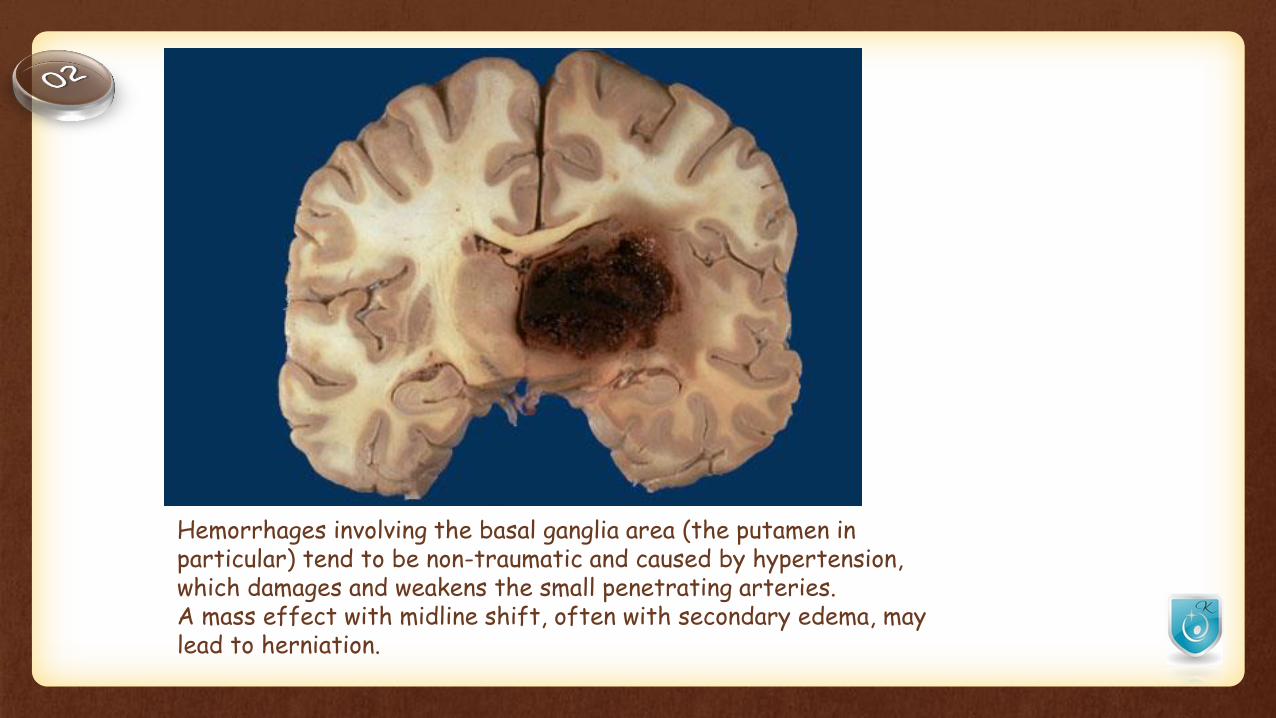
Hemorrhages involving the basal ganglia area (the putamen in particular) tend to be non-traumatic and caused by hypertension, which damages and weakens the small penetrating arteries. A mass effect with midline shift, often with secondary edema, may lead to herniation.

This is a computed tomographic (CT) scan demonstrating a hypertensive hemorrhage in the right thalamus that has extended into the ventricular system. Hemorrhages in this location are not amenable to surgical intervention with removal of the blood.

The large hemorrhage in this adult brain arose in the basal ganglia region of a patient with hypertension. This is one cause for a "stroke"

This computed tomographic (CT) scan of the head in transverse view demonstrates an area of hemorrhage in a patient with a history of hypertension.

A blood clot is seen over the external surface of the durawithin the cranial cavity after removing the top of the skull at autopsy.
Thus, this is an epidural hematoma.
Such a location for hemorrhage is virtually always the result of trauma.
The most likely source of bleeding is a tear in the middle meningeal artery.
The arterial source means that the bleeding is brisk and blood collects quickly, leading to neurologic signs and symptoms within minutes to hours.
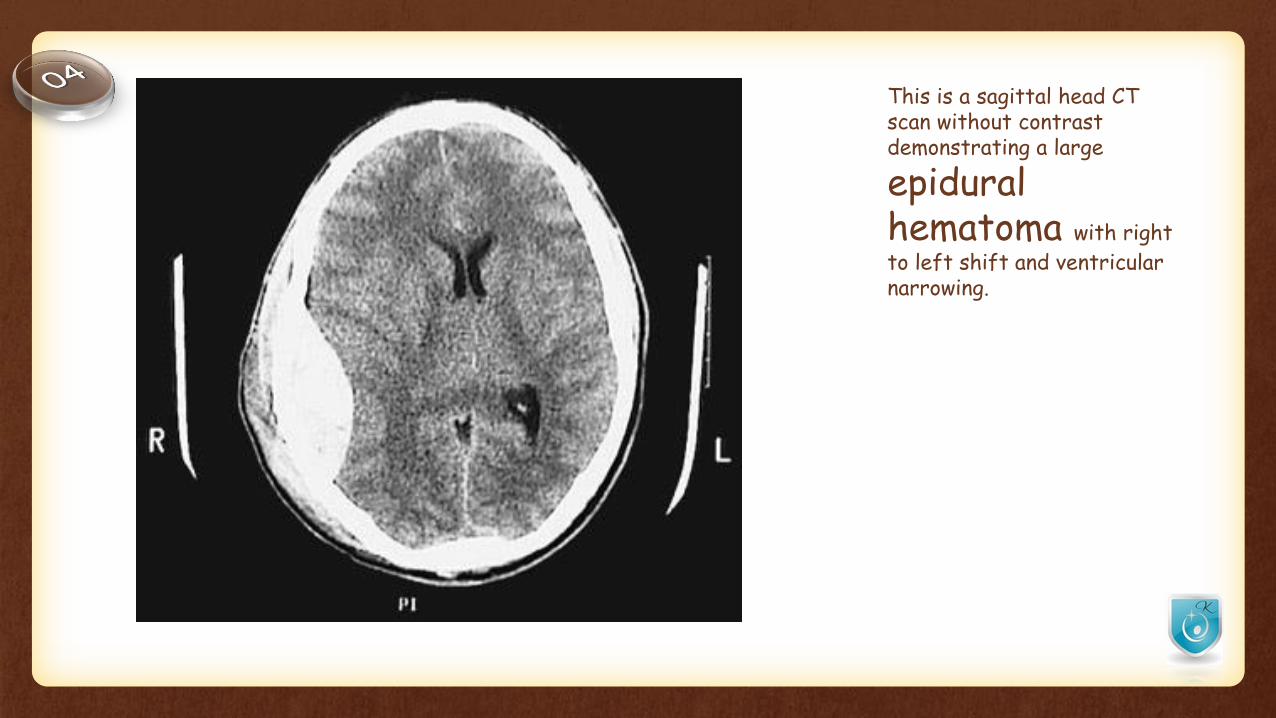
This is a sagittal head CT scan without contrast demonstrating a large
epidural hematoma with right
to left shift and ventricular narrowing.
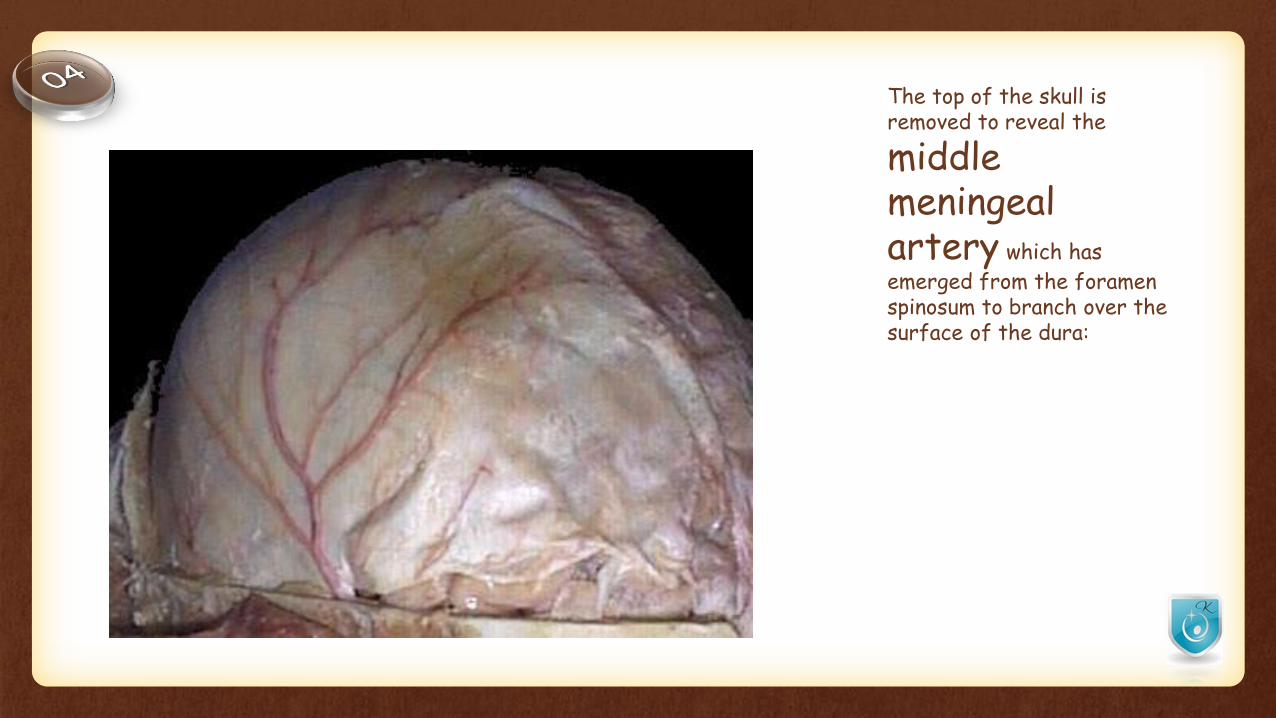
The top of the skull is removed to reveal the
middle meningeal artery which has
emerged from the foramen spinosum to branch over the surface of the dura:

The dura has been reflected back (with a small portion visible at the lower right) to reveal a subdural hematoma.
Such a blood clot is usually the result of trauma with tearing of the cerebral bridging veins at the vertex.
The venous source means that the bleeding may be slow and blood collects over a variable length of time, leading to neurologic signs and symptoms within hours to days or even weeks.
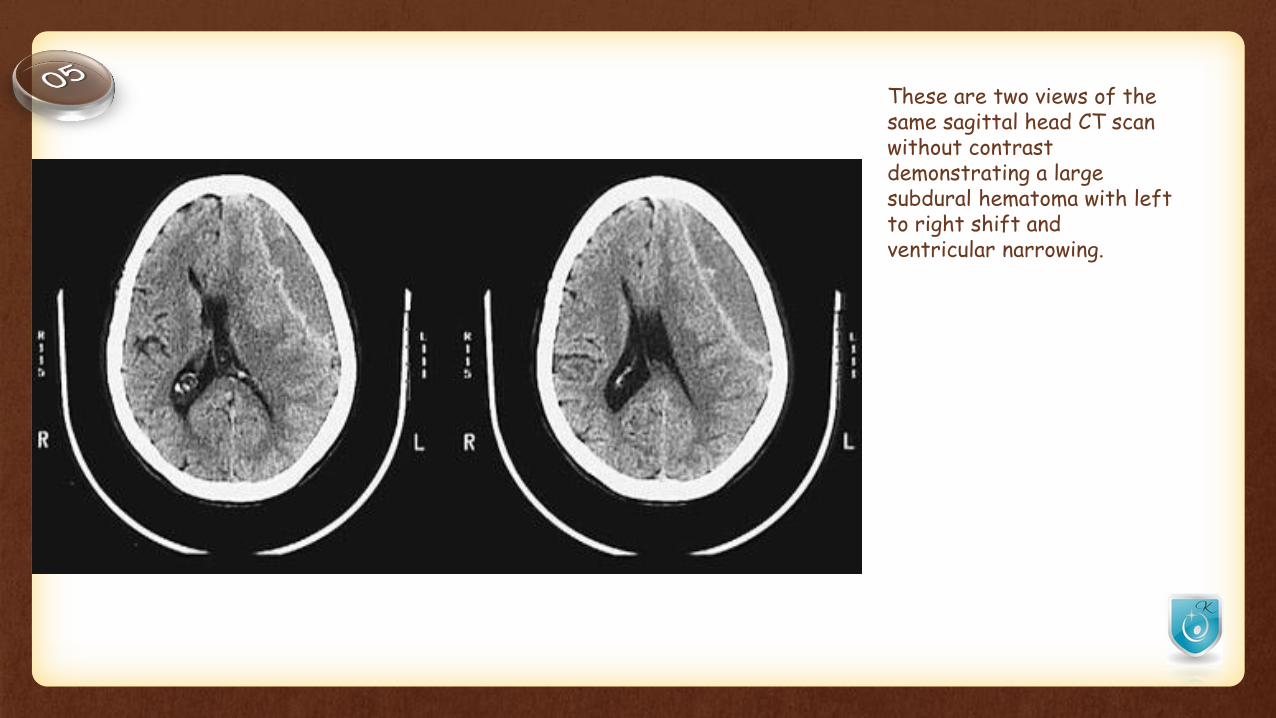
These are two views of the same sagittal head CT scan without contrast demonstrating a large subdural hematoma with left to right shift and ventricular narrowing.

The dura has been reflected above to reveal the bridging veins that extend across to the superior aspect of the cerebral hemispheres.
These cerebral veins can be torn with trauma, particularly if there is significant cerebral atrophy (as with aging) that exposes these veins even more.

Here is a bilateral chronic subdural hematoma.
The blood clots are brown to tan because of organization.
Since the bleeding is venous, subdurals can form more slowly and insidiously than clots from arterial hemorrhages.
Subdurals are most common in the very young and the elderly.

This is a sagittal head CT scan without contrast demonstrating bilateral subdural hematomas, the right greater in size than the left.

The cerebral arterial circulation at the base of the brain is diagrammed here.
A berry aneurysm is diagrammed at the final bifurcation of the right internal carotid artery.
The most common locations for berry aneurysms are in the region of the anterior communicating and anterior cerebral, at the trifurcation of the middle cerebral, and at the bifurcation of internal carotid with posterior communicating. Vertebral-basilar aneurysms comprise <10% of cases. Multiple aneurysms occur in about 20 to 30% of cases

Abbr Name of Artery Distribution
ACA Anterior Cerebral ArterySupplies most medial portions of frontal lobes and superior medial parietal lobes
AComAAnterior Communicating Artery
Connects the anterior cerebral arteries at their closest juncture
ICA Internal Carotid ArteryAscends through base of skull to give rise to the anterior and middle cerebral arteries, and connect with posterior half of circle of Willis via posterior communicating artery
MCA Middle Cerebral ArteryTrifurcates into temporal, frontal, and parietal branches that supply most of the parenchyma of these lobes
PComAPosterior Communicating Artery
Connects the anterior circle of Willis with the posterior cerebral artery of vertebral-basilar circulation posteriorly
PCA Posterior Cerebral ArterySupplies the occipital lobe and the inferior portion of temporal lobe. A branch supplies the choroid plexus.
SCA Superior Cerebellar Artery Supplies the dorsal cerebellum, pons, and midbrain
BA Basilar ArteryFormed by the junction of the two vertebral arteries, it terminates as a bifurcation into the posterior cerebral arteries
AICAAnterior Inferior Cerebellar Artery
Supplies the inferior cerebellum and portions of pons and medulla
VA Vertebral ArteryThe vertebrals emerge from the posterior base of skull and merge to form the basilar artery
PICAPosterior Inferior Cerebellar Artery
Supplies the posterior cerebellum, choroid plexus in 4th ventricle, and portions of medulla
ASA Anterior Spinal Artery Descends along the anterior (ventral) aspect of the spinal co

The white arrow on the black card marks the site of a ruptured berry aneurysm in the circle of Willis.
This is a major cause for subarachnoid hemorrhage

The circle of Willis has been dissected, and three berry aneurysms are seen.
Multiple aneurysms are seen in about 20-30% of cases of berry aneurysm. Such aneurysms are "congenital" in the sense that the defect in the arterial wall is present from birth, but the actual aneurysm takes years to develop, so that rupture is most likely to occur in young to middle age adults.

The subarachnoid hemorrhage from a ruptured aneurysm shown here at the base of the brain is more of an irritant producing vasospasm than a mass lesion. However, a large aneurysm could act like a mass and press on the brainstem or cranial nerve.

Another cause for intracranial hemorrhage, particularly in persons aged 10 to 30, is a vascular malformation.
The dura has been removed, and seen here is a mass of irregular, tortuous vessels over the left posterior parietal region.

This angiogram demonstrates a tortuous collection of irregular small vessels in the temporal region of the brain.

The intraventricular and intracerebral hemorrhage seen here resulted from a ruptured vascular malformation.
The hemorrhage from such a lesion (which is most often histologically an arteriovenous malformation--AVM) can be intracerebral or extend into ventricles or subarachnoid space.

A coronal section through the frontal lobes reveals extensive contusions involving the inferior gyri.
This was a contracoup injury from a fall in the bathtub by an elderly person.

The characteristic location of the dark red-black hemorrhage over the anterior inferior surface of this brain is consistent with a fall backwards resulting in a contracoup injury to the inferior frontal and temporal lobes.
This has resulted in extensive contusions and subarachnoid hemorrhage.

The orange-brown, scalloped appearance of these lesions is consistent with old contusions.
The resolution left behind hemosiderin from the hemorrhage that produces the orange-brown staining.

The so-called Duret hemorrhages seen here in the pons are secondary to downward compression from herniation of the medial temporal lobe that leads to stretching and ischemia of perforating arterioles.
The compression can result from a variety of lesions with mass effect producing herniation--hemorrhages, edema, inflammation, neoplasms.

The extensive white matter pinpoint red petechial hemorrhages seen here are typical for fat embolism syndrome.
Interestingly, neurologic signs and symptoms usually appear about a week after the initiating event, such as long bone fractures in a vehicular accident.


Thank You!