Neurological Study of Radial Nerve Conduction During...
3
*Corresponding author: Gianluigi Bisleri, Cardiochirurgia SSVD – Spedali Civili, P.le Spedali Civili, 1, 25123 Brescia (Italy). Tel: +390303996401 ; Fax: +390303996096 ; Email: [email protected] © 2014 mums.ac.ir All rights reserved. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Neurological Study of Radial Nerve Conduction During Endoscopic Radial Artery Harvesting:An Intra‐Operative Evaluation Gianluigi Bisleri 1 *, Laura Giroletti 1 , Roberto Stefini 2 , Bruno Guarneri 3 , Claudio Muneretto 1 1 Division of Cardiac Surgery, University of Brescia Medical School, Brescia, Italy 2 Division of Neurosurgery, Spedali Civili, Brescia, Italy 3 Section of Neurophysiopathology, Spedali Civili, Brescia, Italy ARTICLE INFO ABSTRACT Article type: Case report Endoscopic radial artery harvesting (ERAH) is a feasible and attractive minimally invasive approach for conduit procurement, however there have been concerns about a potential neurological damage occurring at the harvest limb site secondary to injury of the radial nerve during endoscopic harvesting. We present a case of ERAH in which we evaluated intraoperatively the characteristics of radial nerve conduction by means of electroneuromyography (ENM) during harvesting. No pathological changes of nerve conduction were detected at the harvest limb site during surgery and postoperatively, thereby supporting the benefits of the endoscopic approach in terms of neurological outcomes following radial artery procurements with a less invasive approach. Article history: Received: 21 March 2014 Revised: 10 April 2014 Accepted: 15 Jul 2014 Keywords: Endoscopic Harvesting Nerve Conduction Radial Artery Radial Nerve ►Please cite this paper as: Bisleri G, Giroletti L, Stefini R, Guarneri B, Muneretto C. Neurological Study of Radial Nerve Conduction During Endoscopic Radial Artery Harvesting:An Intra‐Operative Evaluation. J Cardiothorac Med. 2014; 2(3): 207‐209. Introduction Endoscopic radial artery harvesting (ERAH) has emerged in recent years as an attractive alternative approach to conventional open harvesting technique and several reports previously demonstrated the feasibility and safety of this novel approach for radial artery procurement (1,2). Despite the obvious advantages related to the use of a minimally invasive approach, such as a reduced incidence of wound complications and improved cosmetics, there have been controversial results about the persistence of potential impairment at the harvest limb site during endoscopic radial artery harvesting, mostly in relation with a damage occurring at the radial nerve (3). We therefore sought to evaluate the potential alterations occurring in terms of radial nerve conduction intraoperatively during ERAH by means of electroneuromiography (ENM). Case Presentation A 51‐year‐old woman was diagnosed with intracranial meningioma and admitted to Division of Cardiac Surgery, University of Brescia Medical School, Brescia, Italy in order to undergo an extra‐intracranial high‐flow bypass with the use of a radial artery as the conduit of choice. The patient signed an informed consent for the procedure. Following confirmation of a negative Allen test at the non‐dominant arm, endoscopic radial artery harvesting was performed by means of a non‐sealed system combining a reusable stainless steel retractor (Karl Storz, Tuttlingen, Germany) and a disposable vessel sealing system (Ligasure, Covidien, Boulder, CO): as previously described (4), a 2 cm longitudinal incision was performed on the volar surface of the forearm, at the level of the radial styloid prominence. Once the radial artery has been separated as a pedicled conduit
Transcript of Neurological Study of Radial Nerve Conduction During...

*Corresponding author: Gianluigi Bisleri, Cardiochirurgia SSVD – Spedali Civili, P.le Spedali Civili, 1, 25123 Brescia (Italy). Tel: +390303996401 ; Fax: +390303996096 ; Email: [email protected] © 2014 mums.ac.ir All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Neurological Study of Radial Nerve Conduction DuringEndoscopic Radial Artery Harvesting:An Intra‐OperativeEvaluationGianluigi Bisleri1*, Laura Giroletti1, Roberto Stefini2, Bruno Guarneri3,ClaudioMuneretto11 DivisionofCardiacSurgery,UniversityofBresciaMedicalSchool,Brescia,Italy2 DivisionofNeurosurgery,SpedaliCivili,Brescia,Italy3 SectionofNeurophysiopathology,SpedaliCivili,Brescia,Italy
ARTICLEINFO ABSTRACT
Articletype:Casereport
Endoscopic radial artery harvesting (ERAH) is a feasible and attractive minimallyinvasiveapproachforconduitprocurement,howevertherehavebeenconcernsaboutapotentialneurologicaldamageoccurringattheharvestlimbsitesecondarytoinjuryoftheradialnerveduringendoscopicharvesting.WepresentacaseofERAHinwhichweevaluatedintraoperativelythecharacteristicsofradialnerveconductionbymeansof electroneuromyography (ENM) during harvesting. No pathological changes ofnerve conduction were detected at the harvest limb site during surgery andpostoperatively,therebysupportingthebenefitsoftheendoscopicapproachintermsof neurological outcomes following radial artery procurementswith a less invasiveapproach.
Articlehistory:Received:21March2014Revised:10April2014Accepted:15Jul2014
Keywords:EndoscopicHarvestingNerveConductionRadialArteryRadialNerve
►Please cite this paper as: Bisleri G, Giroletti L, Stefini R, Guarneri B, Muneretto C. Neurological Study of Radial Nerve Conduction DuringEndoscopicRadialArteryHarvesting:AnIntra‐OperativeEvaluation.JCardiothoracMed.2014;2(3):207‐209.
IntroductionEndoscopic radial artery harvesting (ERAH)
has emerged in recent years as an attractivealternative approach to conventional openharvesting technique and several reportspreviously demonstrated the feasibility andsafety of this novel approach for radial arteryprocurement (1,2). Despite the obviousadvantages related to the use of a minimallyinvasiveapproach,suchasareducedincidenceofwound complications and improved cosmetics,there have been controversial results about thepersistence of potential impairment at theharvestlimbsiteduringendoscopicradialarteryharvesting, mostly in relation with a damageoccurringattheradialnerve(3).
Wethereforesoughttoevaluatethepotentialalterations occurring in terms of radial nerveconduction intraoperatively during ERAH bymeansofelectroneuromiography(ENM).
CasePresentationA 51‐year‐old woman was diagnosed with
intracranial meningioma and admitted toDivisionofCardiacSurgery,UniversityofBresciaMedicalSchool,Brescia,Italyinordertoundergoan extra‐intracranial high‐flow bypass with theuseofaradialarteryastheconduitofchoice.Thepatient signed an informed consent for theprocedure.
Following confirmation of a negative Allentest at thenon‐dominantarm, endoscopic radialartery harvestingwas performed bymeans of anon‐sealedsystemcombiningareusablestainlesssteel retractor (Karl Storz,Tuttlingen,Germany)andadisposablevesselsealingsystem(Ligasure,Covidien, Boulder, CO): as previously described(4), a 2 cm longitudinal incisionwas performedonthevolarsurfaceoftheforearm,atthelevelofthe radial styloid prominence. Once the radialarteryhas been separated as a pedicled conduit

Bisleri G et a
208
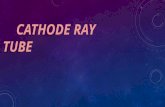
Figure1.(andcathodfrom thvision, tand endfascia bcarpimuoftherafossa); ttheflexooftheensystem.
Throunder dphase) alimbsitelatency(SNAPs)electrod(SpesMethecourthe forelectrodrespectivaroundfinally aItaly) wpacing sreducep
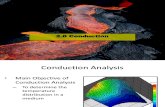
A sinfrequencvolar suTable 1. AduringERAStimulus(T
T0:T1:T2:T3:T4:T5:T6:1.SNAPs:
al
(A)Pacingelectrde),placedaroun
e surroundithe endoscopdoscopic habetween theusclewasdivadialartery(athen, the braorcarpisidewndoscopicret
ughout thehdirect visionan ENM wase inorder toof sensory of the radieswereutiliedica, Genovarseoftheradrearm (Figues (SpesMvely anodethe thumb ground elecwas positionesite and thepotentialsignngle pacing ocyof1Hz,larface of fore
Amplitude andAHTime) Late
sensorynervea
rodeappliedalondthethumbof
ng structurepic retractorrvesting stabrachioradi
videduptothatthelevelofachioradialisweredissectetractorandth
harvestingpror during
s performedevaluate they nerve acal nerve. Difzed: first,apa, Italy) wasdialnerve,ature 1 A);Medica, Geand cathodof the ipsilactrode (SpesMed on the parecording s
nalinterferenof mean ampsting0,1ms,earm about 2
latency of SNA
encyofSNAPs1(m/s)2.82.82.82.72.62.82.9
actionpotentials
ngthecourseoff theipsilateralli
es under dirr was advanarted: first,ialis and fleheproximalftheantecubside and finedjustbymehevesselseal
rocedure (eitthe endosco at the harveamplitudeaction potentfferent kindspacingelectrs applied althemid‐levetwo recordenova, Itae, were plaateral limbMedica, Genolm betweensite in orderce(Figure1Bplitude 170 V,wasapplied2‐3 cm after
APs1 of radial n
AmplitudeofSNAPs1(µV)
5555655
ftheradialnerveimb;groundelec
rectncedtheexorendbitalallyeansling
theropicvestandtialss ofodeongelofdingaly),acedandova,ther toB).V atdonthe
nerve
f)
inccouatt(T1phadifTab3.06.2
abncontheparsite
Di
tiorepthanercaninttraappinjuwhtecrepincenddiffprocomtecandadvwereusys
Neurological
eduringERAHpctrodepositione
cision on thurse,beforetthefirststep1) and abouases of endofferenttimepble1.Norma0msec,while2µV.Asshowninnormal valunduction dure radial artresthesiaoriewasreporte
iscussionNeurologicalnalradialartportedtooccuat is, from 0rvous injurynbemultifacttheforearm,action. A releproach is reurytothelathich insteadchnique. Howported in litecidence of nedoscopicradifferent techocurement mmplications,chnologiesalldlimitednervvantages. Inellasinthecuusable retracstem with bip
Study During Endo
J Cardio
procedure;(B)Redonthepalmb
e wrist, alothestartofEsofharvestinut every fiveoscopic harvpointsofrecoalrangeforlae for amplitu
nTable1,ENues in termring the endotery. At clinimpairedsenedduringthe
l disturbanceeryharvestinurwithinanto 86% (3)following ratorial:directtheuseofcaevant advantaelated to theteralcutaneoucan be inj
wever, there aerature to dateurological dialarteryharvhniques formay impact tin particulalowingforrevousirritatioour routine currentclinicalctor along wpolar radiofr
oscopic Radial Arte
othorac Med. 2014;
Recordingelectroetweenthepaci
ong the radiERAHprocedngunderdiree minutes duvesting (T2‐TordingareouatencyofSNAude of SNAPs
NMdidnotdms of radiaoscopic harvnical evaluansibilityatthepostoperati
es followingngapproachhextremelywi). The mechadial artery hdamagetothauteryandmage of an ene possibilityusantebrachured with tare conflictintewith respedisturbancesvesting(3).Tendoscopic
the incidencear the useducedthermncouldyieldclinical experlreport)wecwith a vesserequency and
ry Harvesting
; 2(3):207-209.
odes(anodengsite
ial nervedure(T0),ectvisionuring theT6) . TheutlinedinAPsare<s are 4.6‐
epictanyal nervevesting ofation, noeharvestvestay.
conven‐havebeeniderange,anisms ofharvestinghenervesmechanicalndoscopicto avoid
hialnerve,the openng resultsect to thefollowingTheuseofc radiale of suchof novelalspreadpotentialrience (ascombineael sealingd a tissue

Neurological Study During Endoscopic Radial Artery Harvesting Bisleri G et al
J Cardiothorac Med. 2014; 2(3):207-209. 209
impedance algorithmwhich allows for a tailoredenergy delivery and adjustment with minimalthermal spread. The possibility to monitorintraoperatively the radial nerve conduction viaENM provided us with a unique opportunity todemonstrate that endoscopic radial arteryharvesting with our current approach does notalternerveconduction.
ConclusionFurther studies on a larger series of patients
alongwithacomprehensivepostoperativeclinicalevaluationarewarranted inorder to confirm thereal impact of neurological sequelae followingendoscopicprocurementoftheradialartery,albeitthisstudydemonstratedforthefirsttimethatthisminimally invasive technique does not directlycauseradialnerveconductionabnormalities.
ConflictofInterestTheauthorsdeclarenoconflictofinterest.
References1. Connolly MW, Torrillo LD, Stauder MJ, Patel NU,
McCabe JC, Loulmet DF, et al. Endoscopic RadialArtery Harvesting: Results of First 300 Patients.AnnThoracSurg,2002;74:502–6.
2. Patel AN, Henry AC, Hunnicutt C, Cockerham CA,Willey B, Urschel HC Jr. Endoscopic radial arteryharvestingisbetterthantheopentechnique.AnnThoracSurg.2004;78(1):149‐53.
3. BisleriG,MoggiA,MunerettoC.Endoscopicvesselharvesting:goodorbad?.CurrOpinCardiol.2013;28(6):666‐70.
4. Bisleri G, Muneretto C. Endoscopic radial arteryharvesting. Multimedia Manual of CardiothoracicSurgery.2009;0907:2008.