
Neurological Institute - Cleveland Clinic · The multidisciplinary Cleveland Clinic Neurological...
42
Neurological Institute 2010 Annual Report
Transcript of Neurological Institute - Cleveland Clinic · The multidisciplinary Cleveland Clinic Neurological...

Neurological Institute
2010 Annual Report
02 Chairman’s Letter
04 Cleveland Clinic Neurological Institute Overview
08 Research and Clinical Highlights
24 Institute Review
36 Staff Achievements
38 Services for Physicians and Patients
On the cover: The evolution of the football helmet is traced in Cleveland Clinic’s Spine Research Laboratory. From the days of leather to contemporary plastic, helmet design has progressed over the decades, and the process is accelerating as researchers and clinicians seek to better protect athletes from head, neck and spine trauma.
Contents
Go green with Cleveland Clinic today!
Use your smartphone to connect to our medical professionals page and sign up to receive publications electronically from Cleveland Clinic Neurological Institute.
To “read” the Tag with your smartphone, find and download a reader from http://www.gettag.mobi.

Expert Neurological Care throughout an Integrated Hospital System
In almost five years of existence, the multidisciplinary Neurological Institute has matured to foster
collaboration among Cleveland Clinic neuroscientists who are united not only by shared interests, but
also by a commitment to provide comprehensive, patient-centered care. In this report, we document
the myriad ways we are meeting this challenge in venues across the enterprise – from our main
campus to our regional hospitals and family health centers to our remote locations – with a common
goal of driving superior patient outcomes and delivering exceptional value.

Michael T. Modic, MD, FACR
Dear Colleagues,
As the incidence of neurological disorders increases, so, too, does the public’s awareness of their
prevalence, causes and devastating consequences. The most recent example is traumatic brain
injury, which has ignited a vigorous dialogue likely to influence the care of every athlete who
sustains a concussion, as well as returning military personnel with blast-related brain injuries.
2 Chairman’s Letter

This issue runs deep, extending beyond professional
football’s Sunday afternoon hit parade to the often-
overlooked and overshadowed accidents that occur
on playgrounds and in amateur athletic venues across
America in the course of everyday life.
At Cleveland Clinic, clinicians and researchers in the
Neurological Institute, Orthopaedic & Rheumatologic
Institute, Lerner Research Institute and Children’s
Hospital are collaborating across the enterprise to
better understand and respond to concussive injuries.
This inter-institutional cooperation characterizes our
entire hospital system’s approach to dealing with
medical disorders in a multidisciplinary fashion.
Following are additional areas of topical interest and
progress/success:
• Cleveland Clinic physicians have joined together
to develop care paths incorporating standardized,
evidence-based encounters with embedded
outcomes and quality measures over the longitudi-
nal course of patient care. Under the leadership of
Irene Katzan, MD, MS, Director of Enterprise Stroke
Systems, we structured a stroke care path and
established comprehensive stroke centers at our
main campus and two regional hospitals. With the
integration of the Department of Physical Medicine
and Rehabilitation and Cleveland Clinic at Home,
we are now one multidisciplinary institute aligned to
apply standard care protocols across all venues for
stroke and other brain dysfunction patients requiring
post-acute care.
• Teamwork within and between the Neurological
and Imaging institutes is supporting the ongoing
development of Cleveland Clinic Lou Ruvo Center for
Brain Health, co-located in Cleveland and Nevada.
Technology bridges geography, enabling secure
digital transfer of patient images to subspecialty-
trained radiologists throughout our system, who
interpret brain exams performed at remote sites.
Last May, this center marked the grand opening
of its Las Vegas facility, an architectural landmark
designed with the needs of patients and caregivers
uppermost in mind. Concurrently, we invested to
significantly strengthen our brain health staff and
physical resources in Cleveland and prepared to
build out the program at Cleveland Clinic Florida.
Multiple access points are consistent with our strate-
gic response to the projected growth in the volume
of patients with neurocognitive disorders.
• Design of our new interventional MRI suite was
another collaborative effort of the Neurological
and Imaging institutes. This technology provides
intraoperative guidance for the most exacting
neurosurgical procedures, including laser ablation
of tumors, cranial biopsies, and placement of deep
brain stimulators and stereotactic EEG electrodes.
• Complementary skill sets in the Neurological
Institute and Cleveland Clinic’s Sydell and Arnold
Miller Family Heart & Vascular Institute are the
foundation of a partnership that created the Center
for Syncope and Autonomic Disorders. This
innovative treatment model, headed by a neurologist
and a cardiologist, provides complete care for
patients with autonomic nervous system disorders,
including safe, noninvasive testing.
• Our neurological nursing staff is actively involved with
interdepartmental teams seeking to effect meaningful
change in the priority area of patient satisfaction.
Nurses have availed themselves of educational
opportunities in pain management, in the belief that
those who become adept at assessing and managing
pain and setting expectations of pain relief will
significantly enhance the patient experience.
These and other initiatives described in these pages
reflect the continuing evolution of the Neurological
Institute. We appreciate the opportunity to report
on our progress and we welcome your comments.
Michael T. Modic, MD, FACR
Chairman, Cleveland Clinic Neurological Institute
Cleveland Clinic Neurological Institute Annual Report 3

Cleveland Clinic Neurological Institute Overview
The institute is anchored by specialized, disease-
specific centers. Each center incorporates the
expertise of physicians and allied health professionals
from all medical and surgical specialties related to
the diagnosis and management of that disease or
group of diseases, thus fostering collaboration and
improved patient access.
The institute also comprises four departments –
Neurology, Neurological Surgery, Psychiatry and
Psychology, and Physical Medicine and Rehabilitation
– that integrate resident training, academics
and research. The latter department, formerly
the Rehabilitation Institute, was merged into the
Neurological Institute in 2009. Its addition, and
the subsequent formation of Cleveland Clinic
at Home, enables seamless delivery of a continuum
of healthcare services from hospital to home.
U.S.News & World Report’s “America’s Best
Hospitals” survey has consistently ranked our
neurology and neurosurgery programs among the
top 10 in the nation. We also hold top rankings in
Ohio for neurology, neurosurgery, pediatric
neurology/neurosurgery and psychiatry.
Expert, Specialized Diagnosis
Neurological Institute physicians draw on advanced
diagnostic capabilities and experience. Our imaging
services include structural and functional MRI,
CT, PET, myelography, diagnostic cerebral/spinal
angiography, interventional neuroradiology, and
carotid and transcranial Doppler ultrasound. Our
neuroimaging staff subspecializes in disease enti-
ties such as epilepsy and cerebrovascular disease,
ensuring accurate, in-depth interpretations.
Overview4
The multidisciplinary Cleveland Clinic Neurological Institute includes more than 300 medical, surgical and
research specialists dedicated to the diagnosis, treatment and rehabilitation of adult and pediatric patients
with disorders of the central nervous system.
Neurological Institute Centers
• Center for Behavioral Health
• Lou Ruvo Center for Brain Health
• Brain Tumor and Neuro-Oncology Center
• Cerebrovascular Center
• Cleveland Clinic at Home
• Epilepsy Center
• Mellen Center for Multiple Sclerosis Treatment and Research
• Center for Neuroimaging
• Neurological Center for Pain
• Center for Neurological Restoration
• Neuromuscular Center
• Center for Pediatric Neurology and Neurosurgery
• Center for Regional Neurosciences
• Sleep Disorders Center
• Center for Spine Health
Cleveland Clinic Neurological Institute Annual Report 5
Additional diagnostic tools are found in our epilepsy
monitoring units, sleep laboratories, neuropsychologi-
cal testing facilities, electromyography laboratory,
autonomic laboratory and cutaneous nerve laboratory.
The Latest Treatment Modalities
Patients find leading-edge treatment options at the
Neurological Institute, where we continue to advance
such innovations as deep brain stimulation, laser
interstitial thermal therapy for brain tumors, epilepsy
surgery, stereotactic spine radiosurgery, endovascular
treatment of cerebral aneurysms and vascular mal-
formations, and neuroendoscopy. Joint Commission
certification as a Primary Stroke Center and accredita-
tion by the American Academy of Sleep Medicine are
just two reflections of our commitment to provide the
most advanced, highest-quality care to our patients.
Relevant Research
We conduct research directly related to conditions
experienced by our patients, including translational
research and clinical trials of drug and device inter-
ventions. In 2009, more than 220 clinical research
trials involving almost 1,800 patients were under
way in the Neurological Institute. Neurologically
based research grants and contract awards totaled
more than $21 million.
In June 2010, the institute announced an alliance
with Numoda Corporation to accelerate the process
by which neuroscience research discoveries are
moved from the laboratory to the patient.
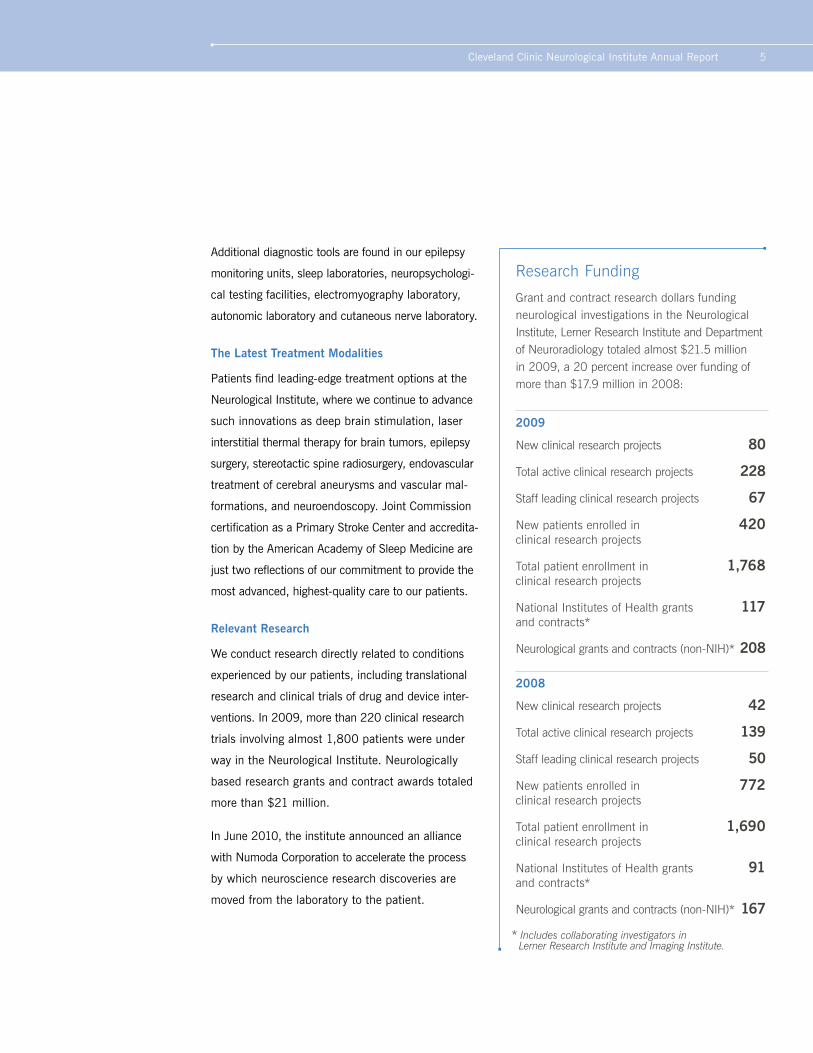
Research Funding
Grant and contract research dollars funding neurological investigations in the Neurological Institute, Lerner Research Institute and Department of Neuroradiology totaled almost $21.5 million in 2009, a 20 percent increase over funding of more than $17.9 million in 2008:
2009
New clinical research projects 80
Total active clinical research projects 228
Staff leading clinical research projects 67
New patients enrolled in 420 clinical research projects
Total patient enrollment in 1,768 clinical research projects
National Institutes of Health grants 117 and contracts*
Neurological grants and contracts (non-NIH)* 208
2008
New clinical research projects 42
Total active clinical research projects 139
Staff leading clinical research projects 50
New patients enrolled in 772 clinical research projects
Total patient enrollment in 1,690 clinical research projects
National Institutes of Health grants 91 and contracts*
Neurological grants and contracts (non-NIH)* 167
* Includes collaborating investigators in Lerner Research Institute and Imaging Institute.
Overview6
Convenient Care in the Community
We are committed to making access to world-
class care convenient for all patients. Neurological
Institute services are available at Cleveland Clinic
health system regional hospitals and family health
centers throughout northeast Ohio. As a result,
patients can easily access specialists who treat
the most complex neurological conditions. This
approach is predicated on the notion that those we
serve are entitled to a uniformly high level of care,
and location should never be an issue.
Key components in our regional network include:
• Cleveland Clinic Neurological Institute at Lakewood
Hospital, which provides comprehensive services
to Cleveland’s West Side and western suburbs
• More than 100 acute inpatient rehabilitation
beds at facilities across northeast Ohio
• More than 45 inpatient and outpatient sites, where
675-plus physical and occupational therapists
offer physical medicine and rehabilitation services
• Cleveland Clinic at Home, which brings in-home
and distance healthcare to individuals in an
expansive area encompassing 14 Ohio counties
and provides home infusion/pharmacy services
in eight states
Neurological Institute Volume, 2009
Patients
Total outpatient visits 143,401
Admissions 17,060
Inpatient days 113,895
Procedures
Surgical/interventional 8,016
Neuroimaging studies 63,514
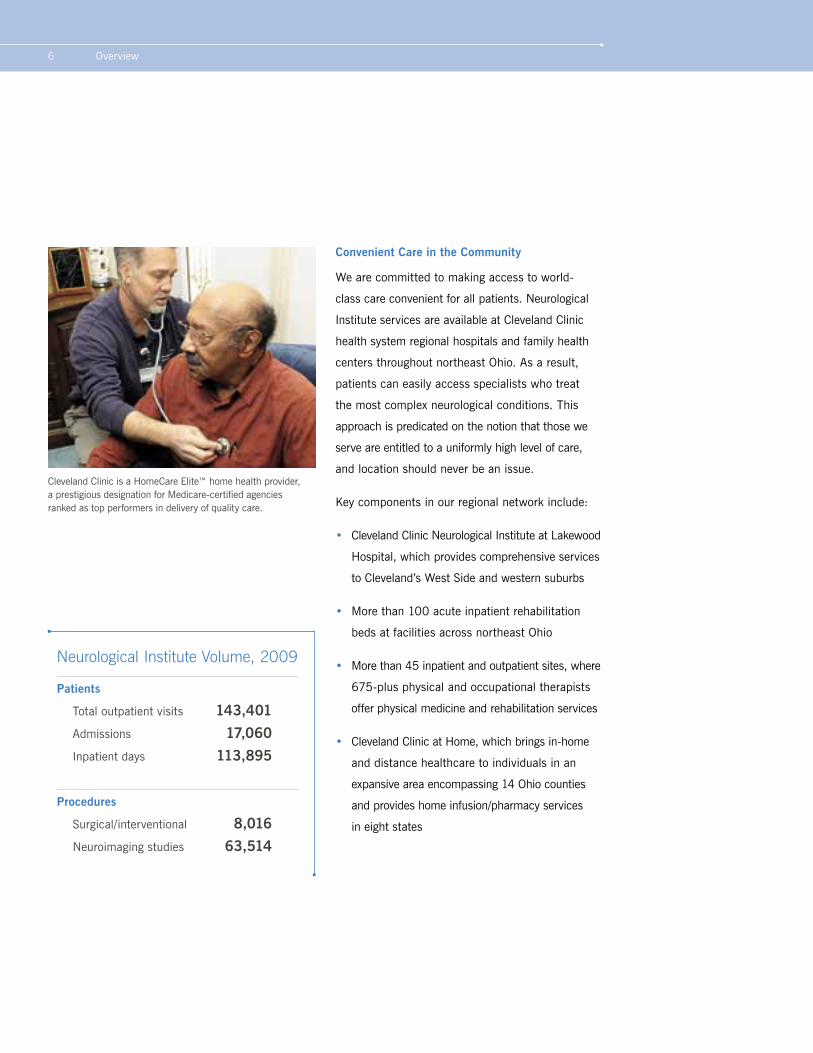
Cleveland Clinic is a HomeCare Elite™ home health provider, a prestigious designation for Medicare-certified agencies ranked as top performers in delivery of quality care.

Cleveland Clinic Neurological Institute Annual Report 7
Integrated Nursing
Nurses in the Neurological Institute rank as
respected members of the care team. As such, they
are encouraged to offer their input to physicians and
administrators and to engage in problem solving and
process improvement. Patients benefit from this
integration through improved coordination of care
and commonly held provider goals.
Opportunities for further education and career advance-
ment are readily available to institute nurses. Their
participation is welcomed in all continuing education
programs, and those with at least two years’ experience
in the institute can aspire to certification in neurosci-
ence nursing. These subspecialists staff areas such as
the Neurological Intensive Care Unit and neurological
stepdown units that treat the most complex patients.
Each November, Cleveland Clinic’s “Innovations in
Neuroscience” conference convenes in Cleveland.
This meeting, originally limited to nurses, broadened
its reach in 2009 to include physician assistants and
medical assistants as organizers continued to work
toward increased provider collaboration.
Pioneering the Collection of Data and Outcomes
Now in its third year, the Neurological Institute’s
Knowledge Program© has captured data from more
than 1 million self-administered patient question-
naires. One of the world’s first interactive clinical
patient databases, the Knowledge Program is dem-
onstrating its value as it evolves, with collection
and correlation of electronic information on patient
health status, quality of life and outcomes.
We are aggregating this patient-generated data with
information from other sources, such as imaging
results and information collected during patient
encounters, to optimize clinical decision making,
quality improvement and research opportunities.
All these data are accessible to physicians through
an interface with the patient’s electronic medical
record. The Knowledge Program is proving to be
among our most constructive tools for delivering
individualized care to improve outcomes and qual-
ity of life, in line with Cleveland Clinic’s guiding
principle: Patients First.
Neurological Institute nurses are encouraged to offer their input and to subspecialize in neuroscience nursing, which qualifies them to care for the most complex patients.

Research and Clinical Highlights8
Cleveland Clinic Neurological Institute Annual Report 9
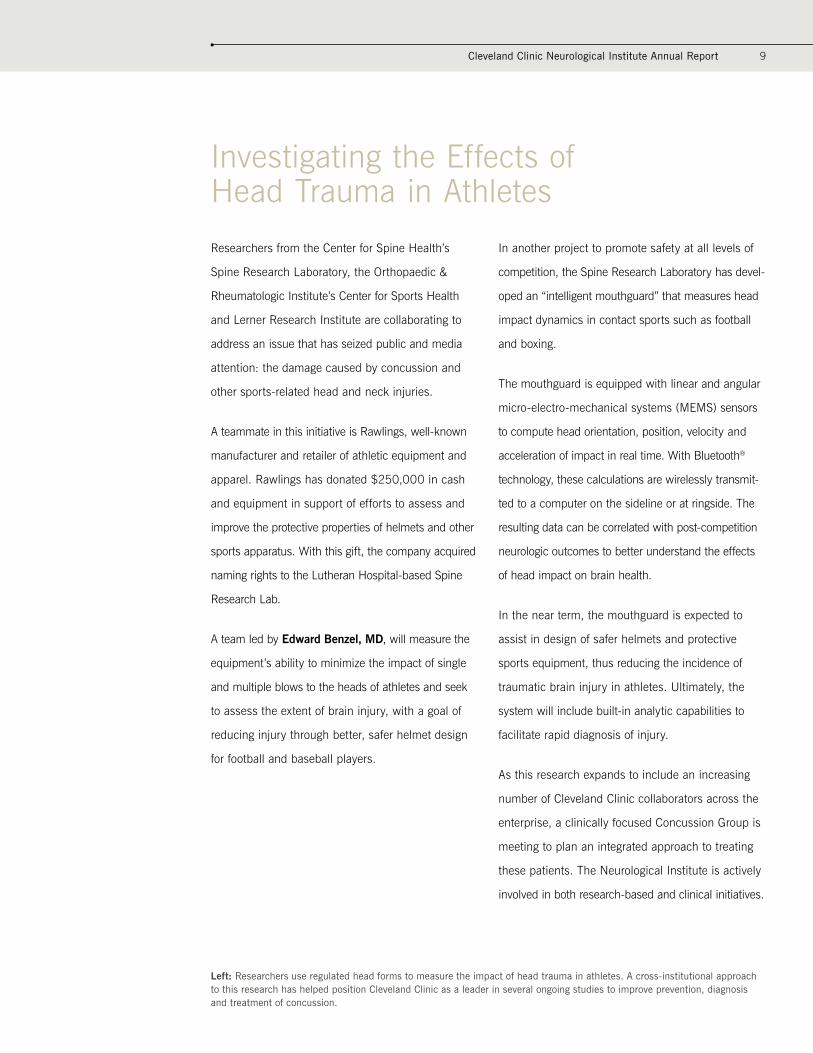
Investigating the Effects of Head Trauma in Athletes
Researchers from the Center for Spine Health’s
Spine Research Laboratory, the Orthopaedic &
Rheumatologic Institute’s Center for Sports Health
and Lerner Research Institute are collaborating to
address an issue that has seized public and media
attention: the damage caused by concussion and
other sports-related head and neck injuries.
A teammate in this initiative is Rawlings, well-known
manufacturer and retailer of athletic equipment and
apparel. Rawlings has donated $250,000 in cash
and equipment in support of efforts to assess and
improve the protective properties of helmets and other
sports apparatus. With this gift, the company acquired
naming rights to the Lutheran Hospital-based Spine
Research Lab.
A team led by Edward Benzel, MD, will measure the
equipment’s ability to minimize the impact of single
and multiple blows to the heads of athletes and seek
to assess the extent of brain injury, with a goal of
reducing injury through better, safer helmet design
for football and baseball players.
In another project to promote safety at all levels of
competition, the Spine Research Laboratory has devel-
oped an “intelligent mouthguard” that measures head
impact dynamics in contact sports such as football
and boxing.
The mouthguard is equipped with linear and angular
micro-electro-mechanical systems (MEMS) sensors
to compute head orientation, position, velocity and
acceleration of impact in real time. With Bluetooth®
technology, these calculations are wirelessly transmit-
ted to a computer on the sideline or at ringside. The
resulting data can be correlated with post-competition
neurologic outcomes to better understand the effects
of head impact on brain health.
In the near term, the mouthguard is expected to
assist in design of safer helmets and protective
sports equipment, thus reducing the incidence of
traumatic brain injury in athletes. Ultimately, the
system will include built-in analytic capabilities to
facilitate rapid diagnosis of injury.
As this research expands to include an increasing
number of Cleveland Clinic collaborators across the
enterprise, a clinically focused Concussion Group is
meeting to plan an integrated approach to treating
these patients. The Neurological Institute is actively
involved in both research-based and clinical initiatives.
Left: Researchers use regulated head forms to measure the impact of head trauma in athletes. A cross-institutional approach to this research has helped position Cleveland Clinic as a leader in several ongoing studies to improve prevention, diagnosis and treatment of concussion.

Cleveland Clinic Neurological Institute Annual Report 11
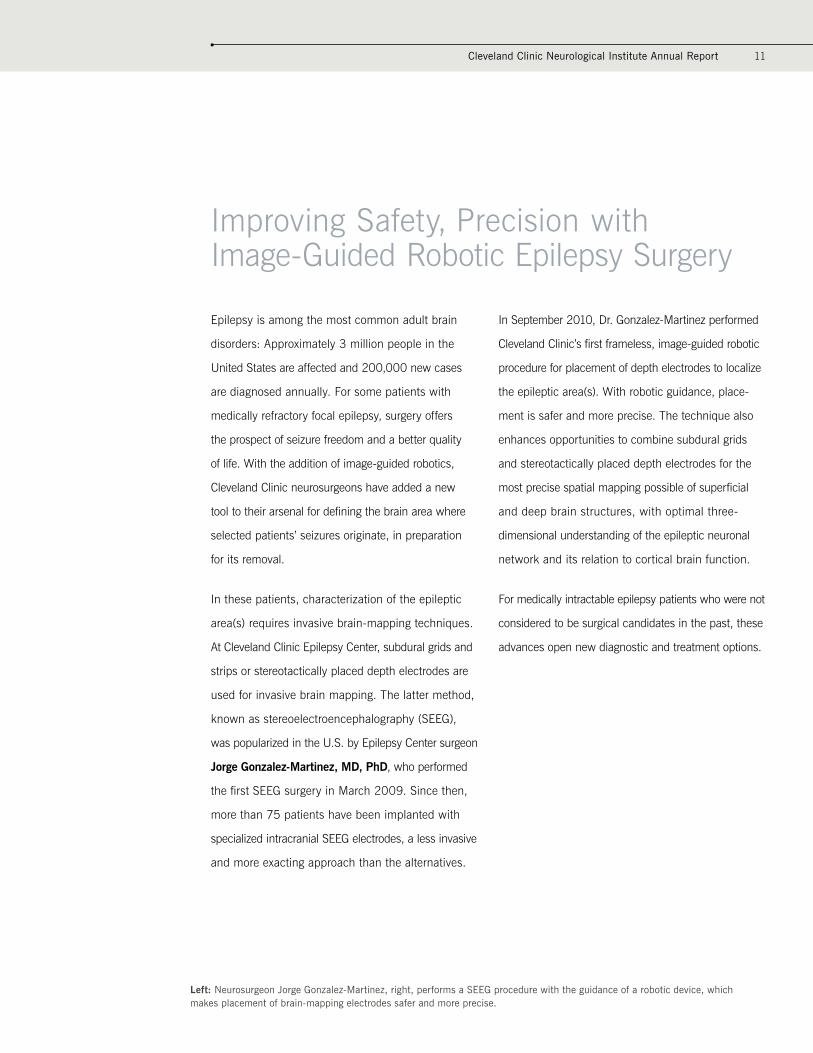
Improving Safety, Precision with Image-Guided Robotic Epilepsy Surgery
Epilepsy is among the most common adult brain
disorders: Approximately 3 million people in the
United States are affected and 200,000 new cases
are diagnosed annually. For some patients with
medically refractory focal epilepsy, surgery offers
the prospect of seizure freedom and a better quality
of life. With the addition of image-guided robotics,
Cleveland Clinic neurosurgeons have added a new
tool to their arsenal for defining the brain area where
selected patients’ seizures originate, in preparation
for its removal.
In these patients, characterization of the epileptic
area(s) requires invasive brain-mapping techniques.
At Cleveland Clinic Epilepsy Center, subdural grids and
strips or stereotactically placed depth electrodes are
used for invasive brain mapping. The latter method,
known as stereoelectroencephalography (SEEG),
was popularized in the U.S. by Epilepsy Center surgeon
Jorge Gonzalez-Martinez, MD, PhD, who performed
the first SEEG surgery in March 2009. Since then,
more than 75 patients have been implanted with
specialized intracranial SEEG electrodes, a less invasive
and more exacting approach than the alternatives.
In September 2010, Dr. Gonzalez-Martinez performed
Cleveland Clinic’s first frameless, image-guided robotic
procedure for placement of depth electrodes to localize
the epileptic area(s). With robotic guidance, place-
ment is safer and more precise. The technique also
enhances opportunities to combine subdural grids
and stereotactically placed depth electrodes for the
most precise spatial mapping possible of superficial
and deep brain structures, with optimal three-
dimensional understanding of the epileptic neuronal
network and its relation to cortical brain function.
For medically intractable epilepsy patients who were not
considered to be surgical candidates in the past, these
advances open new diagnostic and treatment options.
Left: Neurosurgeon Jorge Gonzalez-Martinez, right, performs a SEEG procedure with the guidance of a robotic device, which makes placement of brain-mapping electrodes safer and more precise.

Cleveland Clinic Neurological Institute Annual Report 13
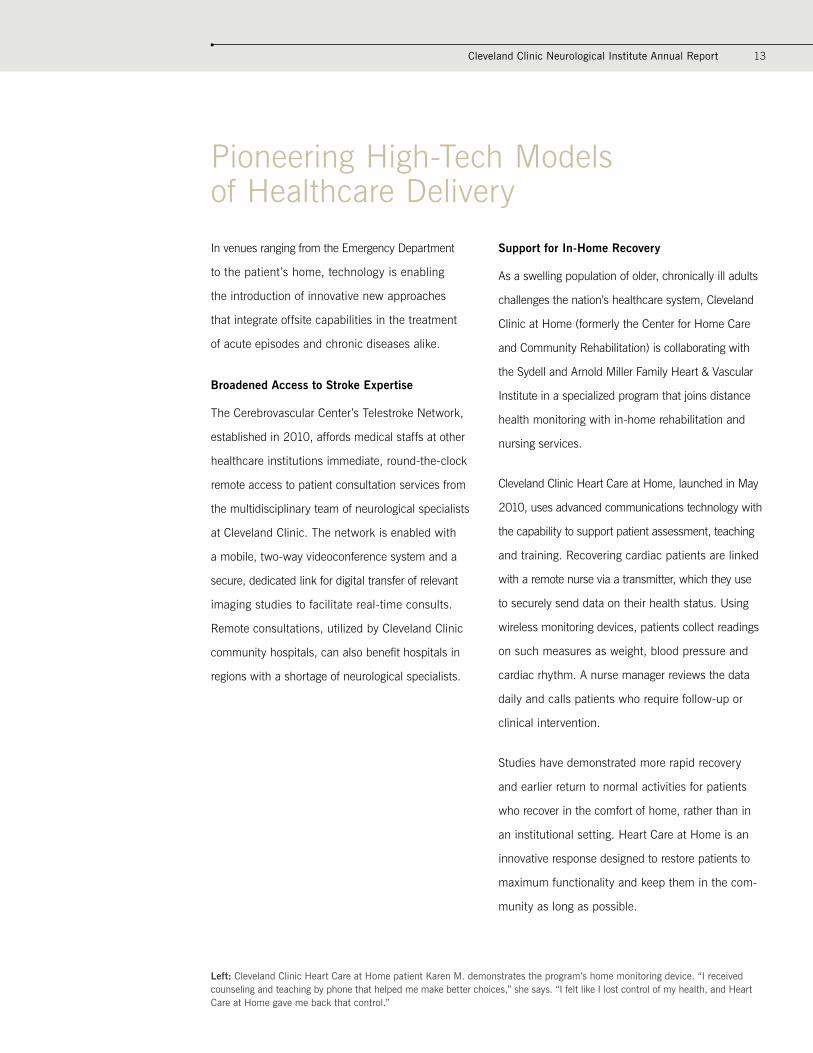
Pioneering High-Tech Models of Healthcare Delivery
In venues ranging from the Emergency Department
to the patient’s home, technology is enabling
the introduction of innovative new approaches
that integrate offsite capabilities in the treatment
of acute episodes and chronic diseases alike.
Broadened Access to Stroke Expertise
The Cerebrovascular Center’s Telestroke Network,
established in 2010, affords medical staffs at other
healthcare institutions immediate, round-the-clock
remote access to patient consultation services from
the multidisciplinary team of neurological specialists
at Cleveland Clinic. The network is enabled with
a mobile, two-way videoconference system and a
secure, dedicated link for digital transfer of relevant
imaging studies to facilitate real-time consults.
Remote consultations, utilized by Cleveland Clinic
community hospitals, can also benefit hospitals in
regions with a shortage of neurological specialists.
Support for In-Home Recovery
As a swelling population of older, chronically ill adults
challenges the nation’s healthcare system, Cleveland
Clinic at Home (formerly the Center for Home Care
and Community Rehabilitation) is collaborating with
the Sydell and Arnold Miller Family Heart & Vascular
Institute in a specialized program that joins distance
health monitoring with in-home rehabilitation and
nursing services.
Cleveland Clinic Heart Care at Home, launched in May
2010, uses advanced communications technology with
the capability to support patient assessment, teaching
and training. Recovering cardiac patients are linked
with a remote nurse via a transmitter, which they use
to securely send data on their health status. Using
wireless monitoring devices, patients collect readings
on such measures as weight, blood pressure and
cardiac rhythm. A nurse manager reviews the data
daily and calls patients who require follow-up or
clinical intervention.
Studies have demonstrated more rapid recovery
and earlier return to normal activities for patients
who recover in the comfort of home, rather than in
an institutional setting. Heart Care at Home is an
innovative response designed to restore patients to
maximum functionality and keep them in the com-
munity as long as possible.
Left: Cleveland Clinic Heart Care at Home patient Karen M. demonstrates the program’s home monitoring device. “I received counseling and teaching by phone that helped me make better choices,” she says. “I felt like I lost control of my health, and Heart Care at Home gave me back that control.”

Cleveland Clinic Neurological Institute Annual Report 15
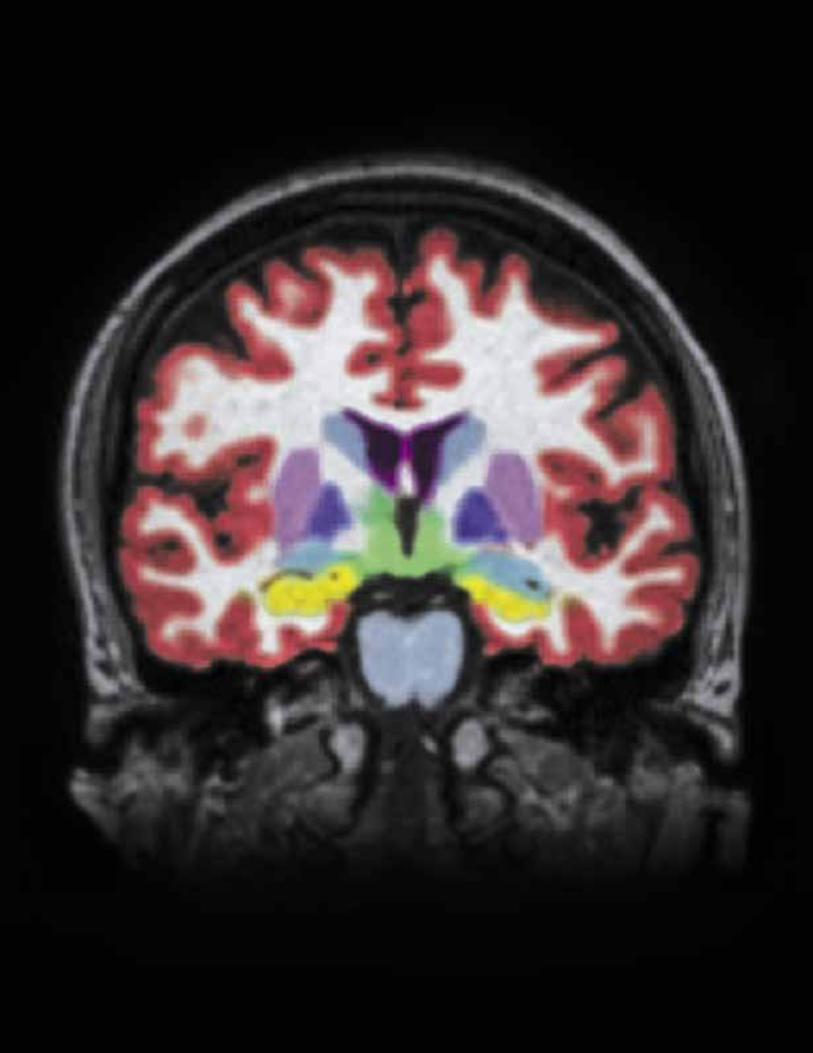
Meeting the Challenge of the Impaired Brain
“Neurological disorders affect millions of people
around the world and represent a vast and growing
need for new and improved treatment options,” notes
Michael T. Modic, MD, FACR, who chairs Cleveland
Clinic Neurological Institute.
More than 5 million Americans are living with
Alzheimer’s disease. For those who suffer and those
who love them, Cleveland Clinic Lou Ruvo Center for
Brain Health pursues a dual mission to advance early
diagnosis, treatment and research of neurocognitive
disorders while providing intensive support and
education for patients’ caregivers.
The year 2010 marked rapid progress in the evolution
of the center, co-located in Ohio, Nevada and Florida.
In May, a grand opening celebration showcased the
center’s Las Vegas home, a striking $80 million facility
designed by Frank Gehry. In July, the center observed
its first anniversary of treating patients and welcomed a
new leadership team headed by Jeffrey L. Cummings,
MD, a world-renowned innovator in the research
of neurodegenerative disorders and an expert on
Alzheimer’s disease.
The center offers patients and families a continuum of
care, with outpatient services that include physician
evaluation, memory testing, neuroimaging, treatment
and caregiver support. Under Dr. Cummings’ direction,
a robust clinical trials program has been launched.
Left: A segmented image of the brain, used to measure brain volume and hippocampal volume changes in Alzheimer’s disease.
Above: Dramatic shapes and light-filled spaces distinguish Cleveland Clinic’s Lou Ruvo Center for Brain Health in Las Vegas. The facility is part of a comprehensive approach to the prevention, diagnosis and management of brain health disorders, with complementary services in Cleveland and in Weston, Florida.

17Cleveland Clinic Neurological Institute Annual Report
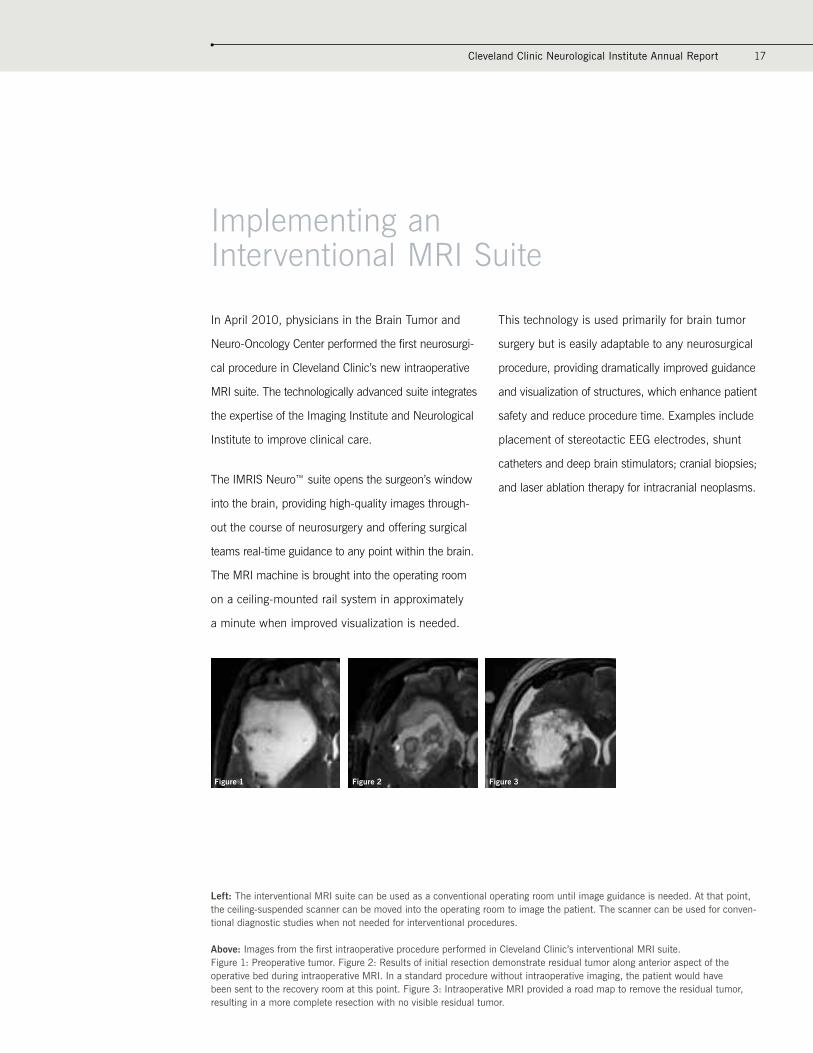
Implementing an Interventional MRI Suite
In April 2010, physicians in the Brain Tumor and
Neuro-Oncology Center performed the first neurosurgi-
cal procedure in Cleveland Clinic’s new intraoperative
MRI suite. The technologically advanced suite integrates
the expertise of the Imaging Institute and Neurological
Institute to improve clinical care.
The IMRIS Neuro™ suite opens the surgeon’s window
into the brain, providing high-quality images through-
out the course of neurosurgery and offering surgical
teams real-time guidance to any point within the brain.
The MRI machine is brought into the operating room
on a ceiling-mounted rail system in approximately
a minute when improved visualization is needed.
This technology is used primarily for brain tumor
surgery but is easily adaptable to any neurosurgical
procedure, providing dramatically improved guidance
and visualization of structures, which enhance patient
safety and reduce procedure time. Examples include
placement of stereotactic EEG electrodes, shunt
catheters and deep brain stimulators; cranial biopsies;
and laser ablation therapy for intracranial neoplasms.
Left: The interventional MRI suite can be used as a conventional operating room until image guidance is needed. At that point, the ceiling-suspended scanner can be moved into the operating room to image the patient. The scanner can be used for conven-tional diagnostic studies when not needed for interventional procedures.
Above: Images from the first intraoperative procedure performed in Cleveland Clinic’s interventional MRI suite. Figure 1: Preoperative tumor. Figure 2: Results of initial resection demonstrate residual tumor along anterior aspect of the operative bed during intraoperative MRI. In a standard procedure without intraoperative imaging, the patient would have been sent to the recovery room at this point. Figure 3: Intraoperative MRI provided a road map to remove the residual tumor, resulting in a more complete resection with no visible residual tumor.
Figure 1 Figure 2 Figure 3


Cleveland Clinic Neurological Institute Annual Report 19
Investigating Neurorepair in MS through Stem Cell Transplantation
With a $2.75 million grant from the U.S. Department
of Defense and a $1 million grant from the National
Institutes of Health, Jeffrey Cohen, MD, is studying
mesenchymal stem cell (MSC) transplantation as
a potential neuroprotective treatment for multiple
sclerosis (MS). No formal trials of this therapy in
MS patients have been published.
The primary objective of this Phase I study, con-
ducted in collaboration with the National Center for
Regenerative Medicine and the Montreal Neurological
Institute, is to evaluate the safety and tolerability of
a single infusion of autologous MSC transplantation
in patients with relapsing forms of MS. These cells
have immunomodulatory actions that may be benefi-
cial. In addition, the ability of MSCs to replace neural
cells through transdifferentiation or, more likely, by
augmentation of intrinsic tissue repair mechanisms,
has focused substantial attention on transplantation
as an approach to neurorepair in MS.
Left: Figure denotes the characteristic morphology of mesenchymal stem cells in culture.
Above: Typical MRI findings in multiple sclerosis are shown here. In the MSC trial, routine and advanced MRI techniques will be used to monitor MS disease activity and changes in the extent of brain tissue damage.

Cleveland Clinic Neurological Institute Annual Report 21
Treating Chronic Central Pain with Deep Brain Stimulation
Andre Machado, MD, PhD, Director of Cleveland Clinic
Center for Neurological Restoration, received an NIH
New Innovator Award and a five-year, $1.5 million
grant to fund investigation of a novel approach
for managing patients with central thalamic pain
syndrome, a particularly severe form of pain.
In this pilot study, Dr. Machado will utilize deep brain
stimulation (DBS) of the ventral capsular/ventral
striatal (VC/VS) area, the goal being to modulate the
affective component in patients with refractory pain
and, consequently, to reduce pain-related disability.
This approach departs from the traditional practice
of intervening in the sensory-discriminative neural
pathways of pain transmission to produce analgesia.
The research marks the first use of DBS of the VC/
VS for management of central pain. It builds upon the
work of a multicenter collaborative, including Cleveland
Clinic, that has evaluated stimulation of the VC/VS
for treatment of disabling depression and obsessive-
compulsive disorders.
Left: Neurosurgeon Andre Machado, MD, PhD, performs deep brain stimulation (DBS). Dr. Machado, who directs the Center for Neurological Restoration, is investigating a new application of DBS for management of intractable thalamic pain syndrome, which has shown inconsistent response to other surgical approaches.

Cleveland Clinic Neurological Institute Annual Report 23
Exploring the Potential of Forced Exercise for Parkinson’s Patients
It was a surprising discovery that Jay Alberts, PhD,
made during a bicycle trip across Iowa: A patient with
Parkinson’s disease, pushed to pedal a tandem bike
at an accelerated rate, experienced improved motor
function even in her non-exercised upper extremi-
ties, which suggests the occurrence of neurochemical
changes with disease-modifying impact. This insight
led to research and to a place among the top 10
medical innovations of 2009. This prestigious list is
unveiled each year at the Cleveland Clinic Medical
Innovation Summit.
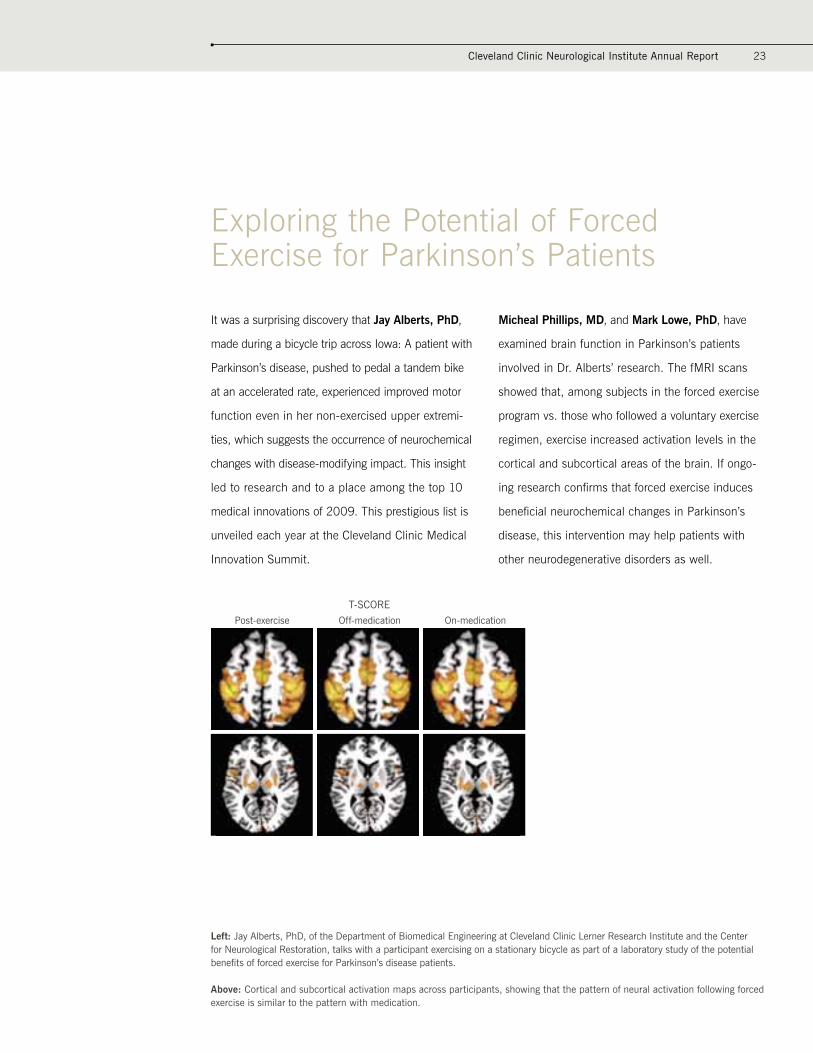
Micheal Phillips, MD, and Mark Lowe, PhD, have
examined brain function in Parkinson’s patients
involved in Dr. Alberts’ research. The fMRI scans
showed that, among subjects in the forced exercise
program vs. those who followed a voluntary exercise
regimen, exercise increased activation levels in the
cortical and subcortical areas of the brain. If ongo-
ing research confirms that forced exercise induces
beneficial neurochemical changes in Parkinson’s
disease, this intervention may help patients with
other neurodegenerative disorders as well.
T-SCOREPost-exercise Off-medication On-medication
Left: Jay Alberts, PhD, of the Department of Biomedical Engineering at Cleveland Clinic Lerner Research Institute and the Center for Neurological Restoration, talks with a participant exercising on a stationary bicycle as part of a laboratory study of the potential benefits of forced exercise for Parkinson’s disease patients.
Above: Cortical and subcortical activation maps across participants, showing that the pattern of neural activation following forced exercise is similar to the pattern with medication.
Institute Review24
Research and Innovation
Examining Treatment Success through Patients’ Eyes
With the only ethics award granted by the National
Institute of Neurological Disorders and Stroke through
the American Recovery and Reinvestment Act,
neuropsychologist Cynthia Kubu, PhD, and
bioethicist Paul Ford, PhD, are studying the ethics
of control and consent in deep brain stimulation
(DBS) for Parkinson’s disease.
Conventional wisdom holds that to patients, a
significant reduction in symptoms equates to
treatment success, but data hint that individual
perspectives may be more complex, incorporating
values, resumption of specific activities/goals, and
underlying cognitive and personality attributes. This
study focuses on defining a more patient-centered
metric than mere symptom-specific measures to
evaluate and better understand treatment success.
With a second grant awarded by the Greenwall
Foundation, Dr. Ford and Dr. Kubu are addressing
similar issues in a population of patients undergoing
epilepsy surgery. Findings from both studies may
have implications for the informed consent process
and for other neurosurgical populations.
Controlling Pseudobulbar Affect in ALS and MS Patients
Erik Pioro, MD, PhD, Director of the Section of
Amyotrophic Lateral Sclerosis (ALS) and Related
Disorders, and Jeffrey L. Cummings, MD, Director
of Cleveland Clinic Lou Ruvo Center for Brain Health,
co-authored a study reporting that an experimental
drug reduces involuntary bouts of laughing and/or
crying in ALS and multiple sclerosis (MS) patients.
“These outbursts are socially debilitating because they
are so unpredictable, are uncontrollable and can be
very embarrassing,” said Dr. Pioro, the lead author.
A 12-week, double-blind, placebo-controlled study
of 326 patients tested the effectiveness of dextro-
methorphan plus low-dose quinidine (DMq). The
drug reduced the frequency of uncontrolled out-
bursts, known as pseudobulbar affect, almost
50 percent. The study was featured in the June
2010 issue of Neurology Reviews and online in
Annals of Neurology. The drug, with the brand
name Nudexta™, was subsequently approved by
the Food and Drug Administration.
Postoperative X-ray shows bilateral deep brain stimulation leads and electrodes in a patient with Parkinson’s disease.

Cleveland Clinic Neurological Institute Annual Report 25
Reducing Procedure Time in Spine Surgery
Digital radiography is significantly faster than conven-
tional radiography (100 seconds vs. 823 seconds)
in localizing the cervical spine level during surgery,
according to a study by Michael Steinmetz, MD, and
colleagues that appeared in the December 2009 issue
of The Spine Journal.
Of 18 patients undergoing single-level anterior cervical
discectomy and fusion with plate and allograft,
10 underwent cervical spine level localization with
conventional radiography and eight underwent
localization with digital imaging. The authors reported
that the latter technique decreased the cycle time for
data acquisition, provided accurate information and
increased operational efficiency, which may reduce
costs and improve patient safety.
Partnering to Bring Research Discoveries to Patients
In May 2009, the Neurological Institute finalized a joint
venture agreement with Numoda Corporation to collabo-
rate in providing physicians and researchers with
systems and tools to improve clinical research manage-
ment. Numoda’s integrated technology platforms offer
rapid data validation and analysis, helping to ensure
on-time, efficiently run projects for pharma, biotech,
medical device and diagnostic companies, and contract
research organizations. The combination of academic
medical center expertise and industry best practices is
expected to hasten development of novel therapies and
treatments for neurological disorders.
Spine surgeons are skilled in minimally invasive techniques and in the most complex procedures. Surgery may be indicated when nonoperative treatments fail.

26
Research and Innovation (continued)
Targeting Metabolism in Brain Tumors
Glioblastoma multiforme is among the most virulent
cancers; most patients succumb within 12 months.
With a $50,000 grant from the Musella Foundation
for Brain Tumor Research & Information, researchers
in the Brain Tumor and Neuro-Oncology Center will
investigate the link between metabolism of glucose
and an oncogene that is necessary for tumor growth
and survival.
This work is based on the theory that malignant
gliomas will stop spreading if they are deprived of the
ability to fuel themselves through glycolysis. The study
will also explore the mechanism by which normal
brain cells, in the absence of glucose, generate energy
from ketone bodies – an ability that some or most
fast-growing, invasive cancers appear to lack.
Tumor Board Cases
Both the Brain Tumor and Neuro-Oncology
Center and the Center for Spine Health
use a multidisciplinary team approach to
evaluate and treat patients with complex
brain or spine tumors. The volume of cases
has multiplied since these two groups
began meeting.
Brain Tumor Board
2010 cases (through mid-December): 1,554
Total number of cases since board’s inception in 2000: 17,019
Spine Tumor Board
2010 cases (through mid-December): 283
Total number of cases since board’s inception in 2006: 1,313
Institute Review
Cleveland Clinic Neurological Institute Annual Report 27
Enhanced Clinical Care
Sweating Out a Diagnosis
The Center for Syncope and Autonomic Disorders, a
collaborative effort of the Neuromuscular Center and
the Department of Cardiovascular Medicine, diagno-
ses and treats autonomic nervous system disorders.
Often, special testing is required to reach a diagnosis.
The newest offering is the thermoregulatory sweat
test, which employs a sweat-reactive powder and a
heating cabinet.
The powder is dusted on the patient’s body, and
the heat and humidity in the cabinet are adjusted to
raise the patient’s body temperature approximately
one degree Centigrade, which produces generalized
sweating. The resulting sweat patterns are helpful in
the diagnosis of a wide array of peripheral and central
autonomic and neurological disorders.
This sensitive test is part of a complete panel of
cardiovascular and sudomotor tests that the Center
for Syncope and Autonomic Disorders administers to
assess the full spectrum of autonomic disorders.
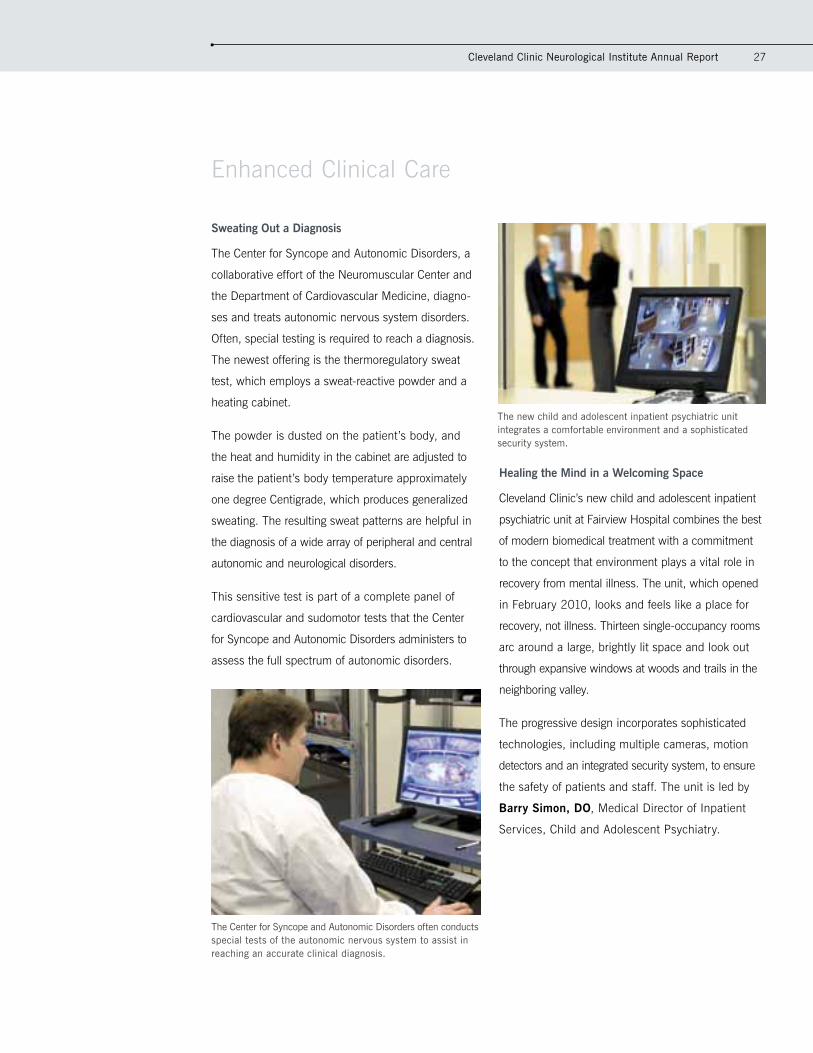
Healing the Mind in a Welcoming Space
Cleveland Clinic’s new child and adolescent inpatient
psychiatric unit at Fairview Hospital combines the best
of modern biomedical treatment with a commitment
to the concept that environment plays a vital role in
recovery from mental illness. The unit, which opened
in February 2010, looks and feels like a place for
recovery, not illness. Thirteen single-occupancy rooms
arc around a large, brightly lit space and look out
through expansive windows at woods and trails in the
neighboring valley.
The progressive design incorporates sophisticated
technologies, including multiple cameras, motion
detectors and an integrated security system, to ensure
the safety of patients and staff. The unit is led by
Barry Simon, DO, Medical Director of Inpatient
Services, Child and Adolescent Psychiatry.
The new child and adolescent inpatient psychiatric unit integrates a comfortable environment and a sophisticated security system.
The Center for Syncope and Autonomic Disorders often conducts special tests of the autonomic nervous system to assist in reaching an accurate clinical diagnosis.

28
Promoting Early Detection of Brain Metastases
Approximately one-quarter of all cancer patients
develop metastatic brain tumors in the course of their
illness when a primary cancer spreads to the brain.
To educate cancer patients on risk factors, symptoms
and available treatment options, the Brain Tumor
and Neuro-Oncology Center launched its B-AwareSM
initiative in 2010.
Under the auspices of the B-Aware campaign, the
center joined with Cleveland Clinic Taussig Cancer
Institute and the American Cancer Society to pre sent
a free informational program for patients, their
families and friends. In addition, the center created
educational materials to disseminate the message
that brain metastases are potentially life threatening
but treatable, and prompt diagnosis is critical.
Performing to a Higher Stroke Care Standard
The Cerebrovascular Center’s commitment to treating
stroke patients according to evidence-based guide-
lines was underscored in 2010 with the center’s
receipt of the American Heart Association/American
Stroke Association’s Get With The Guidelines®
– Stroke Gold Plus Performance Achievement Award.
The designation signifies full compliance with seven
stroke performance achievement indicators.
In addition, The Joint Commission recertified Cleveland
Clinic as a Primary Stroke Center. With regional
expansion and the development of a comprehensive
stroke care path, Cleveland Clinic hospital system now
has five Primary Stroke Centers offering patients in
northeast Ohio convenient access to top-quality care.
The Cerebrovascular Center has one of the highest
stroke-related patient volumes in North America and a
case severity index ranked among the top 2.2 percent
in the nation.
Cranial Radiosurgery Milestone
The Brain Tumor and Neuro-Oncology Center performed its 3,000th Gamma Knife® procedure in
January 2010, solidifying its reputation for technical leadership, experience and clinical expertise.
Cleveland Clinic Gamma Knife Center® opened in 1997, offering patients a nonsurgical treatment option
for certain malignant and noncancerous brain disorders, including brain metastases, pituitary tumors
and arteriovenous malformations.
Institute Review
Enhanced Clinical Care (continued)
A patient diagnosed with multiple brain metastases and treated with cranial radiosurgery.

Brain Tumor Board
2010 cases (through mid-August): 1,155
Total number of cases since board’s inception in 2000: 16,620
Spine Tumor Board
2010 cases (through mid-August): 218
Total number of cases since board’s inception in 2006: 1,249
Cleveland Clinic Neurological Institute Annual Report 29
Accelerating Epilepsy Diagnosis and Care
Cleveland Clinic Epilepsy Center, an international leader
in epilepsy diagnosis and treatment, expanded its
epilepsy monitoring units to improve patient access:
• Adult Epilepsy Monitoring Unit: from 10 to 14 beds
• Pediatric Epilepsy Monitoring Unit: from eight to nine
beds, plus the addition of a playroom for patients and
their siblings
The expansions enable patient consultations within
24 to 48 hours and expedited admission to the
appropriate monitoring unit to accurately diagnose
seizure problems and design the best possible
treatment plan.
Each year, the epilepsy team monitors more than
600 adults and 500 children. Both monitoring units
operate around the clock, staffed with dedicated
nursing and technical personnel and equipped with
the latest, most innovative technology.
Shaping a Supportive NeuroEthics Program
2010 saw the emergence of an active, viable
NeuroEthics program – a partnership between
the Neurological Institute and the Department of
Bioethics, with faculty from both areas. The program
was conceived to address the many ethical chal-
lenges posed for patients, families, caregivers,
researchers and clinicians by the rising incidence
of brain-based diseases and the attendant suffering.
The core faculty includes Paul Ford, PhD, Director;
Cynthia Kubu, PhD, Associate Director of
Neuroethics Research; and Adrienne Boissy, MD,
Associate Director of Clinical Neuroethics.
In its first full year, the program’s ambitious agenda
comprised:
• An inaugural distinguished neuroethics lecture,
delivered in June by Roberta Bondar, MD, nation-
ally recognized astronaut and neurologist
• A one-day symposium on the ethics of invasive
brain testing, presented in October through a
collaboration between the Epilepsy Center and
the Department of Bioethics
• A burgeoning research component, including two
ongoing grants with a combined budget of almost
$1 million (see details on page 24)
• Development of a robust ethics education program
In addition, the faculty provided continuing clinical
consultations. Ethicists participate in specialized patient
management conferences where difficult patient
selection and care issues are aired. They also are called
upon to consult on specific neurosurgical issues.
The Adult Epilepsy Monitoring Unit has undergone a significant expansion to expedite admission for diagnosis of seizure disorders.

30
Patient Experience
Creating a Calming Environment for Families
The task: Design a space to accommodate people
overwhelmed by grief, anxiety, exhaustion, relief
and a range of other powerful emotions as they
cope with a loved one’s health crisis. That responsi-
bility fell to patients and family members on the
Neurological Institute Patient Advisory Council,
working with a diverse Cleveland Clinic care team.
Led by Adrienne Boissy, MD, who chairs the
council, the team consulted with designers, the
Office of Patient Experience, IT and art curators on
appropriate carpeting, lighting, artwork and restroom
options to convey a sense of peace and hope to
patients’ families.
After nine months of collaboration, the Neuro-ICU
Family Comfort Area opened with a celebratory
ribbon-cutting. The comfort area, which seats
approximately 15 people, represents the vision and
partnership of patients, staff and employees. Not
content to rest on its laurels, the council went to work
on an admission brochure for neurological inpatients.
Celebrating the Defiance of Chronic Pain
Few chronic pain programs endure to mark three
decades of service to people who are emotionally and
physically devastated by pain. The Neurological Center
for Pain’s Chronic Pain Rehabilitation Program (CPRP)
is a rare exception. To commemorate its long legacy of
care, the CPRP invited all current and former patients
nationwide to attend an October 2009 reunion. Some
90 individuals turned out, many with family members,
to connect with other CPRP alumni and honor their
collective achievement in learning to manage their pain
and refusing to let it define them.
CPRP Program Director Judith Scheman, PhD,
welcomed the guests and former patients Penny Cowan
and Jim Ryser spoke of how they overcame their pain
and developed programs to help others. Edward
Covington, MD, Director of the Neurological Center for
Pain, was recognized for his dedication to the field.
Institute Review
The Neuro-ICU Family Comfort Area is an island of serenity for main campus visitors dealing with the severe illness of a loved one.
Brain Tumor Board
2010 cases (through mid-August): 1,155
Total number of cases since board’s inception in 2000: 16,620
Spine Tumor Board
2010 cases (through mid-August): 218
Total number of cases since board’s inception in 2006: 1,249
Cleveland Clinic Neurological Institute Annual Report 31
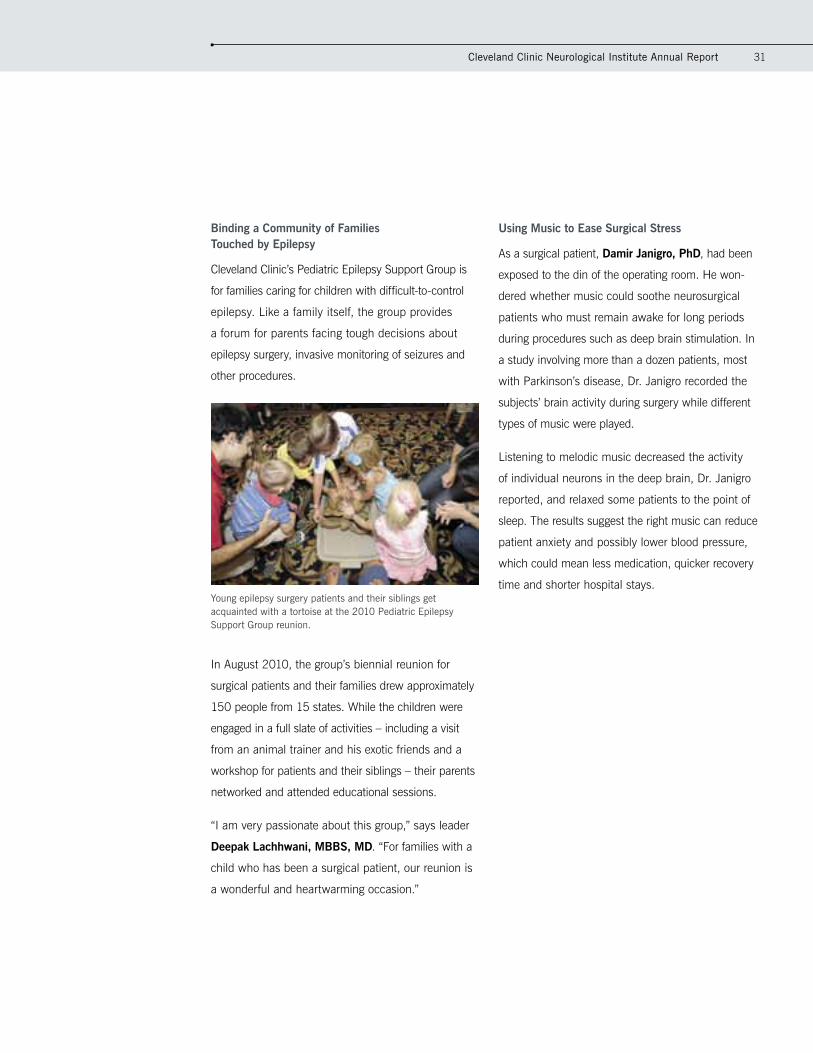
Binding a Community of Families Touched by Epilepsy
Cleveland Clinic’s Pediatric Epilepsy Support Group is
for families caring for children with difficult-to-control
epilepsy. Like a family itself, the group provides
a forum for parents facing tough decisions about
epilepsy surgery, invasive monitoring of seizures and
other procedures.
In August 2010, the group’s biennial reunion for
surgical patients and their families drew approximately
150 people from 15 states. While the children were
engaged in a full slate of activities – including a visit
from an animal trainer and his exotic friends and a
workshop for patients and their siblings – their parents
networked and attended educational sessions.
“I am very passionate about this group,” says leader
Deepak Lachhwani, MBBS, MD. “For families with a
child who has been a surgical patient, our reunion is
a wonderful and heartwarming occasion.”
Using Music to Ease Surgical Stress
As a surgical patient, Damir Janigro, PhD, had been
exposed to the din of the operating room. He won-
dered whether music could soothe neurosurgical
patients who must remain awake for long periods
during procedures such as deep brain stimulation. In
a study involving more than a dozen patients, most
with Parkinson’s disease, Dr. Janigro recorded the
subjects’ brain activity during surgery while different
types of music were played.
Listening to melodic music decreased the activity
of individual neurons in the deep brain, Dr. Janigro
reported, and relaxed some patients to the point of
sleep. The results suggest the right music can reduce
patient anxiety and possibly lower blood pressure,
which could mean less medication, quicker recovery
time and shorter hospital stays.Young epilepsy surgery patients and their siblings get acquainted with a tortoise at the 2010 Pediatric Epilepsy Support Group reunion.
32
Integrating World-Class Care Regionwide
The Neurological Institute’s Center for Regional Neurosciences combines physicians and other healthcare
providers in neurology, neurosurgery, neuroradiology and behavioral sciences, who see adult and pediatric
patients at Cleveland Clinic locations throughout northeast Ohio. Regional facilities extend advanced treat-
ments, technologies and the expertise of Cleveland Clinic into surrounding communities, making it easier for
patients to access specialists who treat the most complex neurological conditions.
Upgrading and Expanding to Optimize Outcomes
• Lakewood Hospital, a Cleveland Clinic hospital,
received a $1 million donation from Cleveland’s
Harold C. Schott Foundation to improve neurologi-
cal and geriatric services promoting brain health.
The donation funds The Harold C. Schott Pavilion
for Geriatric Neurological Health, providing patient
education and resources, allowing the hospital to
better care for patients with age-related neurologi-
cal disorders such as dementia and Parkinson’s
disease, and helping to establish Lakewood as
a hub for regional neurological care.
The hospital will partner with Cleveland Clinic Lou
Ruvo Center for Brain Health. Under the direction
of renowned researcher Jeffrey L. Cummings, MD,
the center is expanding its management of clinical
trials. Programming at Lakewood will focus on
enrolling patients in trials of new treatment options
for Alzheimer’s disease.
Cleveland Clinic Neurological Institute at Lakewood
Hospital opened in 2008, with a multidisciplinary
staff offering treatments for even the most complex
conditions at a convenient site for residents of
Cleveland’s West Side and western suburbs.
• Recent enhancements at Cleveland Clinic’s Hillcrest
Hospital illustrate the significance the Neurological
Institute attaches to regional integration. Among
the improvements was the installation of a state-of-
the-art, flat-panel-detector biplane angiography
suite. This equipment enables the performance of
therapeutic endovascular procedures and positions
Hillcrest to be a leader in the management of
acute ischemic stroke and complex cerebrovascular
conditions. Continued expansion of neurological
services at Hillcrest is likely.
• Cleveland Clinic Sleep Disorders Center extended
its presence to two additional community hospitals
in the Cleveland Clinic system: Medina and
Hillcrest hospitals. For patient comfort and
convenience, the Sleep Disorders Center offers
overnight sleep studies at nine regional locations,
including six hotels, where sleep studies are
performed for adults and children age 12 and older.
Consultations and sleep studies for patients of all
ages are performed at our main location at Fairhill.
Institute Review

Cleveland Clinic Neurological Institute Annual Report 33
Cleveland ClinicChagrin Falls
Cleveland ClinicTwinsburg
Cleveland ClinicStrongsville
Cleveland ClinicBrunswick
Cleveland ClinicWestlake
Cleveland ClinicLorain
Cleveland Clinic
Children’sHospital,Shaker
Cleveland ClinicElyria
Cleveland ClinicAvon Lake
Cleveland ClinicBroadview Heights
Lake Erie
Cleveland ClinicWooster
Cleveland ClinicBeachwood
Cleveland Clinic Solon
Cleveland ClinicWilloughby Hills
LORAIN COUNTY
CUYAHOGA COUNTY
SUMMIT COUNTYMEDINA COUNTY
LAKE COUNTY
PORTAGECOUNTY
GEAUGACOUNTY
(WAYNE COUNTY)
Cleveland ClinicLakewood
Cleveland Clinic Avon
EuclidHospital
Hillcrest Hospital
Huron Hospital
Lutheran Hospital
Lakewood Hospital
Fairview Hospital
South Pointe Hospital
Medina Hospital
Marymount Hospital

34
Education
Extending CME Opportunities
Cleveland Clinic’s Center for Continuing Education
is responsible for one of the world’s largest, most
diverse CME programs. In 2009 and 2010, more
than 30,000 professionals participated in more than
500 Neurological Institute-sponsored CME programs,
ranging from weekly Grand Rounds in six depart-
ments to multi-day international symposia, regional
programs, association meetings, guest lectures and
training courses. Among the highlights:
• 2010 Neurology Update – a Comprehensive Review
for the Clinician, which brought almost 200 neurolo-
gists, internists, family practice physicians and other
providers from 35 states to Washington, D.C.
• 2010 International Symposium on Long-Term
Control of Secondary Central Nervous System
Malignancies, which attracted almost 200 indi-
viduals from around the world to Cleveland. This
event, presented by the Neurological Institute and
Taussig Cancer Institute, marked the launch of
the B-AwareSM educational campaign for cancer
patients (see page 28).
• Endovascular Therapy for Supra-Aortic Disorders
symposium. This 2009 event, a new joint venture
with Beijing Tiantan Hospital, drew more than
300 attendees to Beijing. A second symposium,
A Focus on Acute Ischemic Stroke, took place in
October 2010 in Las Vegas, Nevada.
The Center for Continuing Education’s efforts to
expand CME opportunities through nontraditional
learning were highly successful. The number of
online certificates awarded rose to 10,422 in 2010,
from 5,995 the prior year. In 2008, 2,221 online
certificates were issued.
Health Care Quality Innovation Summit
Optimizing Value and Securing a Future of Innovation and Quality
May 11-13, 2011
InterContinental Hotel and Bank of America Conference Center, Cleveland, Ohio
This multidisciplinary conference on Cleveland Clinic’s main campus is dedicated to exploring novel strategies for improving the assess-ment and delivery of quality health care. The summit brings together the major stakeholders in this process, including physicians, nurses, patients, provider institutions, public and private payers, government agencies and more. In-depth discussions will focus on the shared and sometimes competing visions through which health care quality metrics can be used to advance outcomes.
Register today! ccfcme.org/Quality11
Institute Review

Cleveland Clinic Neurological Institute Annual Report 35
Observing a Tradition: NI Research Day
The annual Neurological Institute Research Day was
created to provide an opportunity for trainees in the
institute to present their research projects to the
Cleveland Clinic neuroscience community. Patterned
after national scientific meetings with poster and
platform sessions, the event is open to residents,
fellows, medical students, PhD students and
postdoctoral fellows conducting research in the
Neurological Institute and the Department of
Neurosciences of Lerner Research Institute. Each
year, 65 or more trainees present projects, many
of which go on to national presentation and peer-
reviewed publication.
Projects are evaluated by a panel of judges from
the departments of Neurology, Neurological Surgery,
and Psychiatry and Psychology. Awardees are selected
in a number of categories, based on scientific merit,
originality, quality and relevance of the projects.
Staff attendance is encouraged and CME credits
are provided. The day ends with a reception and
an awards ceremony.
Neurological Institute Research Day showcases the research projects of physicians in training. Staff physicians judge the work and confer awards for excellence.

Staff Achievements36
Staff Achievements
Milestone
• William Bingaman, MD, Vice Chairman, Clinical
Areas, Neurological Institute, performed his 1,000th
pediatric epilepsy surgery, a tremendous achieve-
ment for any neurosurgeon in his or her lifetime.
Cleveland Clinic is one of a few centers to perform
brain surgery on epileptic patients to improve their
quality of life. Cleveland Clinic Epilepsy Center leads
the country in surgical volume, with more than
350 surgeries in children and adults each year.
Grant Awards
• The National Multiple Sclerosis Society committed
almost $305,000 to a two-year study of “Patient
Decision-Making in Multiple Sclerosis,” led by
Robert Fox, MD. The study’s goal is to assess
risk tolerance and its role in patient decision
making in the treatment of MS.
• Stephen Rao, PhD, was awarded a five-year,
$2.1 million grant by the National Institute on
Aging to examine the value of task-activated
functional MRI (fMRI) in the identification and
prediction of disease course in populations at
risk for development of Alzheimer’s disease. fMRI
will also be used as an outcome measure in a
randomized, double-blind, placebo-controlled
clinical trial involving the rivastigmine (Exelon®)
patch in patients with the amnestic form of mild
cognitive impairment.
• Tatiana Falcone, MD, received a $791,622
federal grant to improve access, knowledge and
mental health resources for children with epilepsy.
The three-year grant will also support training in
the problems children with epilepsy face and how
to help them. Partners in the project include the
Epilepsy Association of Cleveland, the Cleveland
Metropolitan School District and the National
Alliance of Mental Illness Greater Cleveland.
• J. Javier Provencio, MD, FCCM, is one of
seven recipients nationwide of a 2010 research
grant from the Brain Aneurysm Foundation.
He received $20,000 for his project, “Timing
Neutrophil Inactivation to Prevent Vasospasm
in Murine Model.”
• Imad Najm, MD, received an $846,847
Department of Defense grant to study the
mechanisms of epilepsy development following
severe head injury. This grant will enable the
study of imaging and neurophysiologic predictors
of epilepsy development after traumatic brain
injury (TBI) and assessment of the effect
of deep brain stimulation on the treatment of
TBI-induced epilepsy.

Cleveland Clinic Neurological Institute Annual Report 37
Appointments
• Neurological Institute Chairman Michael T.
Modic, MD, FACR, was appointed to the newly
created post of Cleveland Clinic Chief Emerging
Business Officer. Dr. Modic works with executive
leadership to review emerging business strategy,
capitalize on strategic thinking and assess new
ideas to expand opportunities. He continues as
Chairman of the Neurological Institute and works
closely with other institutes to identify ways to
take advantage of existing opportunities.
• Donald A. Malone Jr., MD, was appointed
Chairman of the Department of Psychiatry and
Psychology. He also serves as Director of the
Center for Behavioral Health. Dr. Malone succeeds
George Tesar, MD, who held the department
chairmanship for 16 years and continues as
Director of the General Psychiatry Residency
Training Program.
• Robert Weil, MD, was named to fill the newly
created position of Director of Neurological Institute
Surgical Operations. His responsibilities include
improving operational efficiency and enhancing the
institute’s ability to achieve and maintain excellence
in patient care, safety, satisfaction and outcomes.
Recognition
• Steven Landers, MD, MPH, Director of Cleveland
Clinic at Home, was chosen 2009 Physician of
the Year by the National Association for Home
Care & Hospice.
• Richard Ransohoff, MD, was among five
healthcare professionals inducted in 2009 into
the National Multiple Sclerosis Society’s Volunteer
Hall of Fame.
• Tatiana Falcone, MD, was chosen by the
American Academy of Child and Adolescent
Psychiatry as a mentor for its summer 2010
medical student research training program. The
prestigious designation is limited to a small
number of academy members annually.
• A textbook authored by Edward Benzel, MD;
Michael Steinmetz, MD; and Imad Najm, MD,
received the Benjamin Franklin Silver Award
for 2010 in the professional/technical category.
Their text, “Anatomic Basis of Neurologic
Diagnosis,” was the only Thieme Publishers
award recipient. The competition attracted more
than 1,300 entries, which were judged for
editorial and design excellence.
• “The Kindness of Cleveland” was the title of
a February 2010 blog posting by Scott Simon
extolling the skill and wisdom of Edward Benzel,
MD, who performed cervical spine surgery on the
popular National Public Radio host. Dr. Benzel was
not the only one who earned Mr. Simon’s praise:
“From shuttle drivers to nurses and surgeons, the
staff at the Cleveland Clinic filled an anxious time
for our family with warmth, and even laughter.”
Mr. Simon returned to Cleveland Clinic in May
2010 to deliver the keynote address at the first
Patient Experience Summit.
Services for Physicians and Patients38
Stay Connected to Cleveland Clinic
Cleveland Clinic Information
Neurological Institute24/7 hospital transfers or physician consults
800.553.5056
Neurological Institute Contact Center
Centralized scheduling that allows patients to make appointments – including same-day appointments, if necessary – with any Neurological Institute physician at any location.
216.636.5860 or toll-free 866.588.2264
On the Web at clevelandclinic.org/neuroscience
Services for PhysiciansPhysician Directory View all Cleveland Clinic staff online at clevelandclinic.org/staff.
Referring Physician Center For help with service-related issues, information about our clinical specialists and services, details about CME opportunities and more, contact us at [email protected], or 216.448.0900 or toll-free 888.637.0568.
Critical Care Transport Worldwide Cleveland Clinic’s critical care transport team and fleet of mobile ICU vehicles, helicopters and fixed-wing aircraft serve critically ill and highly complex patients across the globe. To arrange a transfer for STEMI (ST elevated myocardial infarction), acute stroke, ICH (intracerebral hemorrhage), SAH (subarachnoid hemorrhage) or aortic syndromes, call 877.379.CODE (2633). For all other critical care transfers, call 216.444.8302 or 800.553.5056.
Request for Medical Records 216.444.2640 or toll-free 800.225.2273, ext. 42640
Track Your Patient’s Care Online DrConnect offers referring physicians secure access to their patients’ treatment progress while at Cleveland Clinic. To establish a DrConnect account, visit clevelandclinic.org/drconnect or email [email protected].
Online Medical Second Opinions from Cleveland Clinic’s MyConsult are particularly valuable for patients who wish to avoid the time and expense of travel. Visit clevelandclinic.org/myconsult, email [email protected] or call 800.223.2273, ext. 43223.
Outcomes Data View the latest clinical Outcomes book from Cleveland Clinic Neurological Institute at clevelandclinic.org/quality/outcomes.
CME Opportunities: Live and Online Cleveland Clinic’s Center for Continuing Education’s website, ccfcme.com, offers convenient, complimentary learning opportunities, from a virtual textbook of medicine (Disease Management Project) and a medical newsfeed refreshed daily, to myCME, a system for physicians to manage their CME portfolios. Many live CME courses are hosted in Cleveland, an economical option for business travel.
Services for PatientsMedical Concierge Complimentary assistance for out-of-state patients and families, 800.223.2273, ext. 55580, or email [email protected]
Global Patient Services Complimentary assistance for national and international patients and families, 001.216.444.8184 or visit clevelandclinic.org/gps

The multidisciplinary Neurological Institute, one of 26 institutes at Cleveland Clinic, is internationally
known for superior diagnosis and treatment of neurological disorders ranging from the common to
the most complex. More than 300 specialists combine clinical expertise, academic achievement and
innovative research to accelerate transfer of investigational therapies unavailable elsewhere, for the
benefit of adult and pediatric patients. The institute is committed to improving outcomes while treating
patients with compassion and respect.
Cleveland Clinic is a nonprofit, multispecialty academic medical center, consistently ranked among the
top hospitals in America by U.S.News & World Report. Founded in 1921, it is dedicated to providing
quality specialized care and includes an outpatient clinic, a hospital with more than 1,300 staffed beds,
an education institute and a research institute.
Cleveland Clinic ©2011
ART DIReCTION: Barbara Ludwig Coleman
eDITOR: Terry Pederson
MARkeTING: Colleen Burke, Sarah Delly, Jennifer Lynch, Laura Vasile
PhOTOGRAPhy: Matt Carbone Photography, Al Fuchs, Don Gerda, Neil Lantzy, Russell Lee, Willie McAllister, Tom Merce, Steve Travarca
PRINT PRODuCTION: Paul Durrant

10-NEU-018
The Cleveland Clinic Foundation9500 Euclid AvenueCleveland, Ohio 44195


















