Neurodiagnostic Tests
81
Title Neurodiagnostic Tests Module 5
Transcript of Neurodiagnostic Tests

Title
Neurodiagnostic Tests
Module 5
TitleIntroduction
Introduction, Objectives and Key Topics
▪ Introduction▪ This module will address the concepts of neurodiagnostic tests
▪ Objectives▪ Describe the major radiological studies used in the diagnosis of neurological processes▪ Describe the relations of intracranial concepts▪ Discuss cerebral blood flow hemodynamics▪ Identify normal and abnormal cerebral blood flow▪ Describe cerebral autoregulation mechanisms▪ Discuss normal cerebral metabolism▪ Identify the impact of cerebral ischemia
▪ Key Points▪ Radiological studies
▪ Intracranial pressure
▪ Cerebral blood flow
▪ Metabolism
TitleSpeaker Bio
Your Instructors
Speaker Bio
Rachel Malloy, MSN, RN, CNRN, SCRN is a native of Kansas City, Missouri. She began her nursing career 20 year ago after graduating with her Bachelor in Science in Nursing From Research College of Nursing in Kansas City, MO. The majority of her experience is in neurocritical care, diagnostic medicine and imaging and stroke. In 2011, she began working in Industry as a clinical resource and educator working with neuro programs across the nation. Rachel’s qualification include:
▪ Master of Science in Nursing with an education focus from Research College of Nursing in Kansas City, MO with a thesis focusing on Guidelines for Use of Human Patient Simulators
▪ Certified Neuroscience Registered Nurse (CNRN)▪ Stroke Certified Registered Nurse (SCRN)▪ Post-graduate Fellowship in Neurovascular Education and Training in Stroke
Management and Acute Reperfusion Therapy▪ Expertise in principles of intracranial dynamics, cerebral monitoring, imaging and
stroke
Rachel Malloy, MSN, RN, CNRN, SCRN
Rachel speaks locally, nationally and internationally on a variety of topics including cerebral dynamics, neuroimaging, traumatic brain injury, correlative assessment and stroke.
Title
Radiological Studies
Module 6, Section 1

TitlePlain X-Rays
Plain X-Ray
• X-ray studies are also known as radiographs
• X-ray beams pass through the body and are absorbed in different amounts depending on the density
• Shades of black, white and gray
• Dense material such as bone shows up white on an x-ray
• Used to identify fractures, bone defects, dislocation, vertebral compression, spinal curvatures, spinal canal stenosis, degenerative processes and calcification of bone
• Dependent on the view of the x-ray (lateral, posteroanterior, or anteroposterior) depends on the anatomical structures that will be demonstrated

TitlePlain X-ray
Plain X-Ray: Procedural Considerations
• Rule out cervical-spine injury before hyperextending the neck or head position
• Perform cervical spine radiographs on all patients with suspected head or spinal cord injuries
• No special instructions or sedation required
• No special pre- or post-procedural care required
TitleCT
Computerized Tomography (CT)
• Two dimensional (2D) radiograph constructed from a series of cross sectional images
• Can also be 3D and 4D
• Accurately depicts the size and location of pathological conditions
• Measured in density: hypo-dense, iso-dense, hyper-dense
• May require iodinated contrast to enhance areas
TitleCT - Views
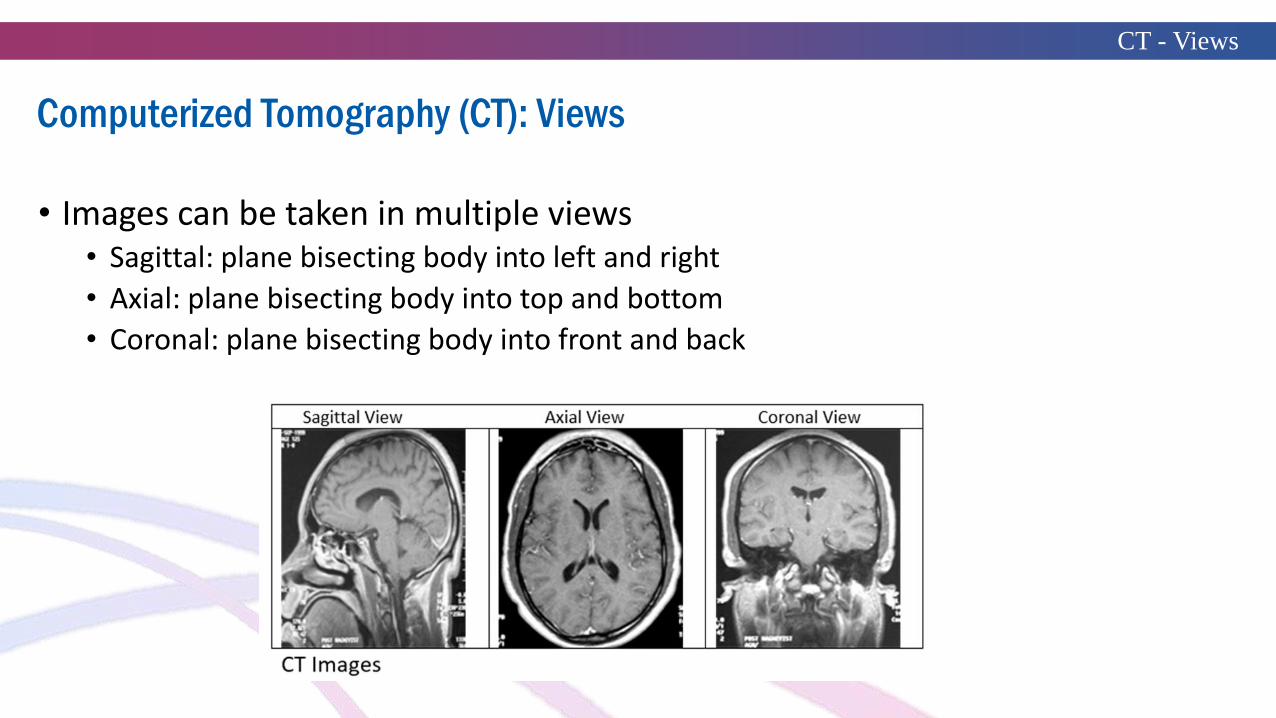
Computerized Tomography (CT): Views
• Images can be taken in multiple views• Sagittal: plane bisecting body into left and right
• Axial: plane bisecting body into top and bottom
• Coronal: plane bisecting body into front and back

TitleCT - Purpose
Computerized Tomography (CT): Purpose
• Used to detail specific areas of the head or spine
• Used to detect vascular changes with in brain tissue and spaces
• Used to detect edema, shift from midline or compartments, hydrocephalus and obliteration of gyri
TitleCT Angiography
CT Angiography (CTA)
• Noninvasive technique for imaging extracranial/intracranial vessels including vascular abnormalities
• Requires contrast bolus
• 3-D reconstruction of the data allows visualization of the arterial anatomy
TitleCT Angiography
CT Angiography (CTA): Purpose
• Can be used to assess carotid arteries for stenosis• Not operator-dependent like carotid doppler• More accurate for calcified vessels• Distinguishes trickle flow from occlusion
• Can be used for evaluation of the cerebral aneurysms• Sensitive for locating ruptured aneurysms in patients with subarachnoid hemorrhage• Good visualization for aneurysms of all sizes even small aneurysms
• Advantages over cerebral angiography:• Less expensive• Less invasive• Fewer potential complications
TitleCT Perfusion
CT Perfusion
CT Perfusion (CTP)
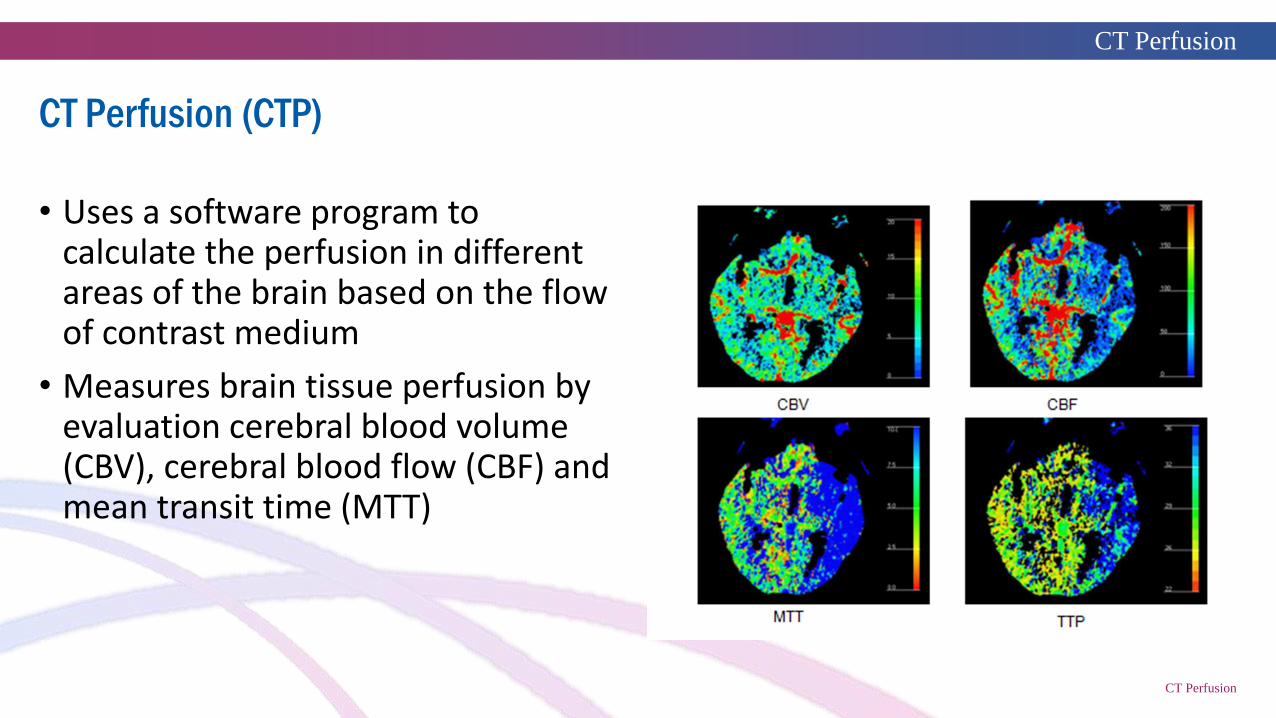
• Uses a software program to calculate the perfusion in different areas of the brain based on the flow of contrast medium
• Measures brain tissue perfusion by evaluation cerebral blood volume (CBV), cerebral blood flow (CBF) and mean transit time (MTT)

TitleCT Perfusion
CT Perfusion (CTP): Purpose
• Measures cerebral blood flow
• Demonstrates regional hypoperfusion states
• Distinguishes tissue at risk of infarction from previously infarcted tissue
Useful in identifying penumbra in acute ischemic stroke

TitleCT Fluoroscopy
CT Fluoroscopy
• Combines the benefit of CT with the advantage of real-time imaging
• Used for percutaneous interventional procedures
• Disadvantages of fluoroscopy are:• Radiation exposure
• Requires conscious sedation
TitleMagnetic Resonance
Imaging (MRI)
Magnetic Resonance Imaging (MRI)
• Uses radiofrequency waves and magnetic fields in combination to provide images of various anatomical components based on variations in tissue
• A pulse sequence is used to change the radiofrequency and magnetic field gradient pulses to produce desired images
• Does not use radiation
• Contraindicated with certain metal implants due to the presence of the magnetic fields
• Images can be taken in multiple views: sagittal, axial, and coronal

TitleMagnetic Resonance
Imaging (MRI)Magnetic Resonance Imaging (MRI)
T1 and T2 Sequences
• T1-weighted images: differentiation is caused largely by the difference in T1 of the tissues. • In T1-weighted images, dark represents
water, CSF, edema, or calcium, whereas bright represents lipid or gadolinium
• Similarly, T2-weighted images: differentiation is caused by difference in T2 of the tissues. • In T2-weighted images, dark represents
calcium and bone, whereas brightrepresents CSF, water, or edema
TitleMagnetic Resonance
Imaging (MRI)Magnetic Resonance Imaging (MRI)
DWI and GRE Sequences
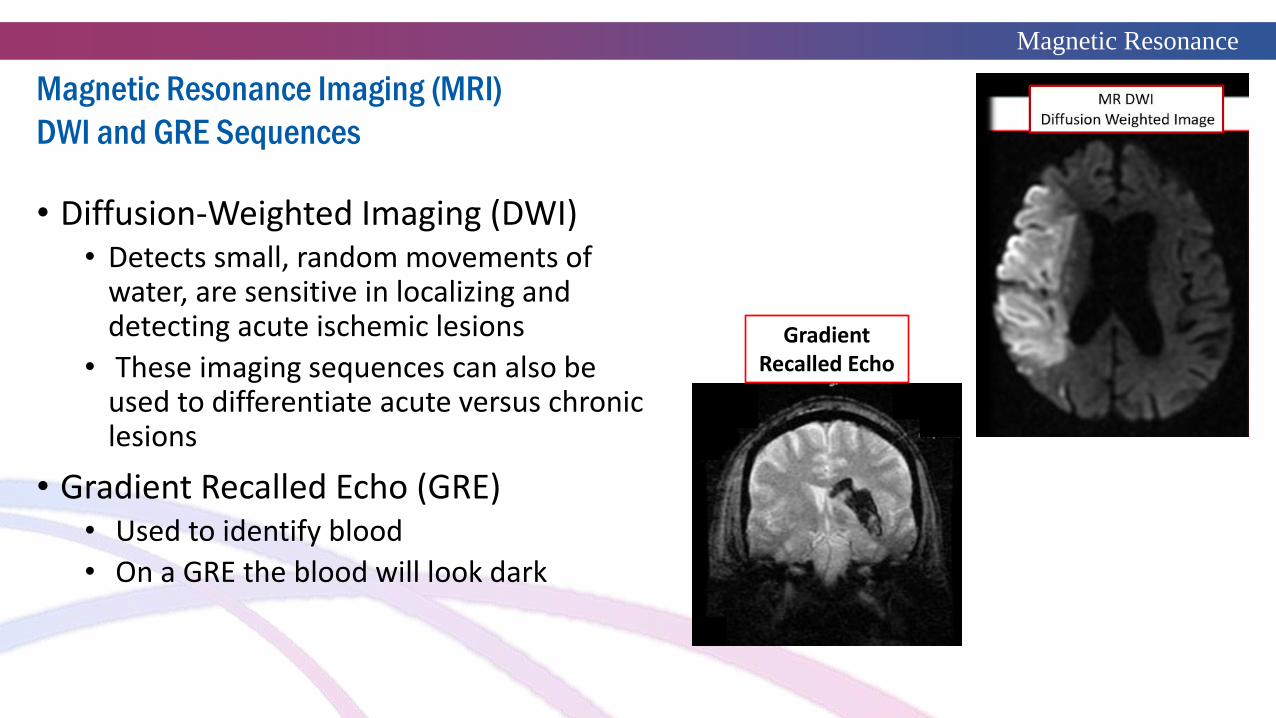
• Diffusion-Weighted Imaging (DWI)• Detects small, random movements of
water, are sensitive in localizing and detecting acute ischemic lesions
• These imaging sequences can also be used to differentiate acute versus chronic lesions
• Gradient Recalled Echo (GRE)• Used to identify blood
• On a GRE the blood will look dark
Gradient Recalled Echo

TitleMagnetic Resonance
Imaging (MRI)
Magnetic Resonance Imaging (MRI): Purpose
• Diagnose structural and biochemical abnormalities of brain and nervous system
• Detect necrotic tissue, oxygen-deprived tissue, and degenerative diseases of CNS
• Demonstrate white-matter changes as seen in multiple sclerosis
• Better visualization of brain stem and posterior fossa structures, especially structures adjacent to bone

TitleMR Angiogram
MR Angiogram (MRA)
• Quality noninvasive imaging of the cerebral vasculature and vessels of the neck
• Detection of vascular abnormalities such as cerebral aneurysms, arteriovenous malformations, fistulas, and narrowing of vessels
• Useful in some cases (e.g., “thunderclap” headaches with normal CT scan and CSF examinations) when a patient declines an arteriogram
• Can detect saccular aneurysms not seen on cerebral angiography

TitleMR Perfusion
MR Perfusion
• A metabolic parameter imaging technique that measures cerebral blood volume, cerebral blood flow, and mean transit time
• Used for:• Noninvasive histologic assessment of tumors
• Evaluating neurodegenerative conditions such as Alzheimer's disease
• Evaluating tissue at risk after acute ischemic stroke
• Compared to MR diffusion weighted images to identify a tissue mismatch

TitleMR Spectroscopy
Slide 22
MR Spectroscopy
• A noninvasive technique for evaluating proton-containing compounds within the brain tissue; particularly tumors
• Provides neurochemical data about normal or morphologically altered tissues by analyzing molecules such as hydrogen ions or protons
• Monitors changes in chemical composition of a lesion or region during treatment
• MR spectroscopy can be used to determine tumor type and aggressiveness, and distinguish between tumor recurrence and radiation necrosis

TitleFunctional MRI
Functional MRI (fMRI)
• A type of MRI that allows study of brain metabolism and blood flow as well as mapping of functional cortical activity during the performance of cognitive and motor activities
• Not a direct reflection of neuronal activation, but rather reflects secondary changes in CBF and oxygenation in brain tissues during activation versus nonactivation
• Used for mapping brain activity pathways
• Used to identify the motor cortex, giving functional information in addition to structural data for pre-surgical mapping
• Used for neurological and psychiatric conditions

TitleMRI
MRI: Advantages and Disadvantages
• Advantages• View of anatomic detail is better with MRI than CT, especially in the brain stem and
cerebellum regions
• MRI has greater sensitivity and specificity for extracerebral lesions compared with CT
• MRI is more sensitive for contusions, hematomas, intraparenchymal injury, and edema
• MRI IV contrast agent is gadolinium, which has a low incidence of allergic reaction and is metabolized by the liver
• Disadvantages• Long scan times may be necessary
• MRI is more sensitive to motion
• Claustrophobic patients may require oral sedation and, rarely, conscious sedation
• Certain medical equipment and implantable devices can be problematic
TitleMRI
MRI – Procedural Considerations
• All patients should complete a safety screening questionnaire
• Patients should be screened for possible claustrophobia
• Patients must be instructed on the MRI scanners sensitivity to motion
• Patients requiring conscious sedation must be monitored according to institutional guidelines
TitlePositron Emission tomography (PET)
Positron Emission Tomography (PET)
• Imaging technique using positron-emitting radioactive isotopes that provides a functional scan
• Maps brain biochemistry and physiology
• Complements but does not replace other imaging studies that provide anatomical information
• Can assist in differentiating between a tumor and post-radiation necrosis
• Useful in studying dementia and its effect on cerebral metabolism
• PET is also an important research tool to map normal human brain

Title
PET: Procedural Considerations
• Patient should fast for 4-6 hours prior to the scan. • Water should be encouraged during this time of fasting
• No strenuous exercise the day before, or day of the scan
• Remove dentures, glasses, jewelry to eliminate artifact
• Twenty-two gauge or larger-bore IV should be placed
• Obtain blood glucose (BG) level and follow institution guidelines for accepted BG level
• Patient should be able to return to normal activities after the test is completed

TitleSingle Photon Emissions
computed tomography (SPECT)
Single Photon Emissions Computed Tomography (SPECT)
• Based on the same principles as PET technology, but the decay of the radioactive “tags” emits only a single photon and requires a rotating gamma camera
• Multi-slice imaging technique uses radionuclides for physiological imaging that measures regional cerebral blood flow and perfusion
• Used to detect changes in cerebral perfusion and is especially useful in acute ischemic events such as stroke, seizures, tumors, and dementia
• Useful in understanding impact on cerebral perfusion as a result of psychiatric disorders and depression

TitleCerebral Angiography
Cerebral Angiography
• Imaging is produced by fluoroscopy, a technique to obtain real-time moving images
• This exam is performed in interventional radiology
• Radiopaque contrast is injected into the carotid or vertebral arteries via catheter placement into the femoral or brachial artery
• Provides radiographs of the cerebral vasculature
• Most accurate and sensitive way to look at the cerebral vasculature
• The terms angiography or arteriography are used to describe both arteriograms and venograms
TitleAngiography: Purpose
Cerebral Angiography: Purpose
• Extracranial and carotid arteries are examined to detect the following:• Atherosclerotic disease• Dissections• Intimal tears due to trauma• Carotid body tumors• Angiofibromas as a prelude to embolization
• Intracranial circulation is examined to detect to detect the following:• Atherosclerotic disease• Aneurysms• Arteriovenous malformations (AVMs)• Arteriovenous fistulas (carotid cavernous fistulas [CCF])• Vasospasm• Arteritis• Intracranial tumor vascularity, in some instances

TitleAngiography
Cerebral Angiography: Advantages and Disadvantages
• Advantage• Gold standard for diagnosis of cerebral aneurysms, arteriovenous malformation,
arteriovenous fistula, or other vascular abnormalities
• Allows for diagnosis and treatment
• Disadvantage• Invasive with risk of serious complications including:
• Emboli dislodged from atherosclerotic plaque
• Thrombus formation on a catheter or guidewire
• Catheter causing dissection leading to occlusion of the vessel
TitleAngiography
Cerebral Angiography: Procedural Considerations
• Collect baseline neurological and vital signs
• Review laboratory reports for abnormal results
• Review history of allergies
• Establish IV access
• After the procedure, lie the patient flat with leg extended for 6 hours
• Monitor puncture site periodically for bleeding
• Monitor neurological and vital signs for evidence of complications
• Monitor pedal pulses of catheterized leg for evidence of impaired circulation

TitleMyelogram
Myelogram
• Fluoroscopic images are produced from injection of nonionic water-based contrast media into the subarachnoid space via lumbar puncture
• Radiographs are taken to provide visualization of the spinal cord and adjacent anatomical structures such as the intervertebral disk and nerve roots
• Used to identify spinal cord or nerve root lesions or compression
• Used to detect disk herniation, spinal stenosis, and arachnoiditis

TitleMyelogram
Myelogram: Procedural Considerations
• Obtain baseline neurological and vital signs
• Maintain NPO status for 4 - 6 hours before the procedure
• Establish IV access
• Anticoagulants and antiplatelets should be withheld
• Patient may require a coagulation profile before the examination
• Maintain elevation of the head at 30 - 45 degree angle for 4-6 hours post-procedure
• Observe patient for signs of complications such as headache, stiff neck, nausea, fever, seizure, paralysis, decreased consciousness and loss of bladder control
• Monitor puncture site for evidence of bleeding
• Increase fluid intake to assist with clearance of contrast

Title
Conclusion
Thank You
Neurodiagnostic Tests
Module 5

Title
Neurodiagnostic Tests:EEG, EMG, & Nerve Conduction
Module 5

TitleIntroduction
Introduction, Objectives and Key Topics
▪ Introduction
▪ This section of neurodiagnostic studies will focus on EEG, EMG, and nerve conduction studies.
▪ Objectives
▪ Understand the diagnostic capabilities of EEG, EMG, and nerve conduction studies▪ Describe the patient population that might benefit from EEG, EMG, and nerve conduction monitoring▪ Describe the nursing considerations for EEG, EMG, and Nerve conduction monitoring ▪ Describe the nursing care for a patient undergoing EEG, EMG, and nerve conduction monitoring
▪ Key Points
▪ EEG
▪ Differences between EMG and nerve conduction studies
▪ Patient care considerations

TitleInstructor
Your Instructor
Fern Cudlip MSN, FNP, CNRN, ANVP
Fern S. Cudlip MSN, FNP-BC, CNRN, NVRN-BC, ANVP-BC has been a Nurse Practitioner since 1995. She began work in neurocritical care in 2001 with building a spine and brain trauma program. Then in 2010, Fern focused her efforts in neurovascular care after completing the NETSMART AP fellowship program.
Fern has a strong clinical and administrative background in all aspects of program development and clinical management pertaining to acute and elective spine care, brain trauma, and comprehensive stroke service. In addition, she has participated in furthering stroke care through lecturing, research and publication.

TitleEEG Testing
Electroencephalography (EEG)
• An EEG is a non-invasive monitoring tool utilized to evaluate the electrical activity within the brain• Since brain cells typically communicate with each other through electrical impulses, the EEG
can be utilized to help detect potential problems associated with brain cell activity
• To monitor brain cell communication, the EEG tracks and records brain wave patterns through small electrodes that are attached to the scalp • Electrodes are connected to a computer with wires
• Electrodes are able to analyze the electrical impulses in the brain and then send these signals to a computer for an electrical recording of the results
• This can be correlated to a simultaneous video recording of the patient’s activity
• The character and morphology of the individual electrical impulses in the EEG recording allow providers to assess for abnormal patterns and irregularities that may signify seizure activity and/or other brain disorders

Title
EEG Activity
How it works!
• Neurons in the brain are electrically charged from the ions that exist on either side of the cell membrane
• When the wave of these ions reaches the electrodes that have been placed on the scalp, they exert a “push” or a “pull” on the metal of the electrode
• This “push” and/or “pull” difference is measured as a voltage across time on the EEG
EEG Testing

TitleEEG Testing
EEG: Applied Purposes
EEG is used in several ways:
• Investigate epilepsy, locate a seizure origin, and test epilepsy drugs
• Brain lesions: Tumors or stroke, may have unusually slow EEG waves, depending
on the size and the location of the lesion
• Diagnostic tool for other disorders that influence brain activity: Alzheimer's
disease, certain psychoses, and a sleep disorders
• Determine the overall electrical activity of the brain:
• Evaluation of trauma, drug intoxication, or extent of brain damage in comatose patients
• Controlling depth of anesthesia
• Monitoring of blood flow in the brain during surgical procedures
TitleEEG Testing
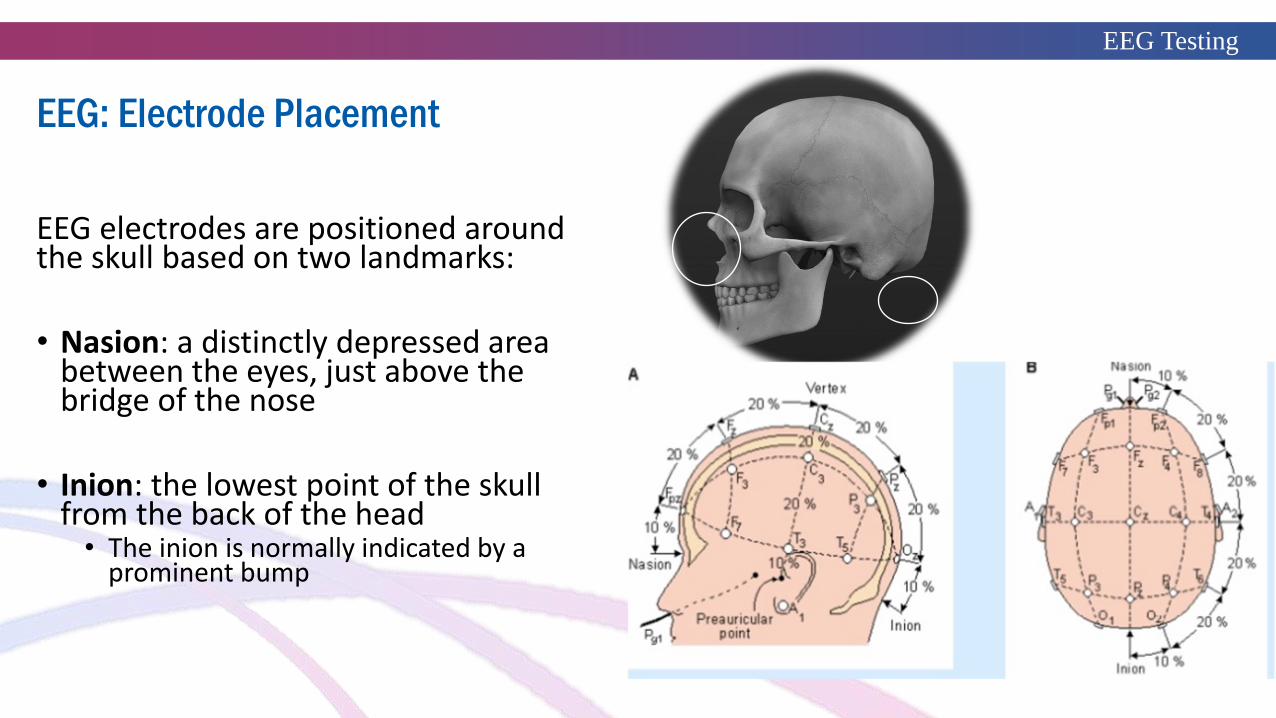
EEG electrodes are positioned around the skull based on two landmarks:
• Nasion: a distinctly depressed area between the eyes, just above the bridge of the nose
• Inion: the lowest point of the skull from the back of the head• The inion is normally indicated by a
prominent bump
EEG: Electrode Placement

TitleEEG Testing
• Electrodes may be placed separately on the scalp or mounted on a special cap or band on the head
• The placement of electrodes is standardized by the International 10–20 system:
• An internationally recognized electrode placement method that ensures standardized reproducibility
• Allows a subject’s EEG study to be compared over time
• The system is based on the relationship between the location of an electrode and the underlying area of cerebral cortex
• The “10” and “20” refer to the distances between adjacent electrodes
• 10% or 20% of the total front–back or right–left distance of the skull
Each site letter/number identifies the lobe and hemisphere location.
• The letters F, T, C, P and O stand for frontal, temporal, central, parietal, and occipital lobes, respectively
EEG: Electrode Placement
Fisher RS, Acevedo C, Arzimanoglou A, et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia 2014; 55:475.
TitleEEG Testing
EEG: Evoked Potentials
• Evoked potential are the electrical responses that are recorded on the EEG in response to
a stimulus
• These evoked responses may be recorded from different areas of the cerebral cortex and brain stem
• There are three kinds of evoked potentials in clinical use:
• Auditory evoked potentials are responses that may be elicited by a click or tone stimulus presented
through earphones:
• Measures responses of the brain stem to stimulation of the eighth cranial nerve
• Visual evoked potentials are responses elicited by a flashing light or changing pattern on a monitor:
• Can diagnose visual stimuli problems in the optic nerve tracts of the occipital lobe.
• Somatosensory evoked potentials are responses elicited by electrical stimulation of peripheral nerve:
• Can detect problems with the brain and spinal cord from stimulation of peripheral nerves

TitleEEG Testing
EEG Waveforms
• Normal EEG waveforms are defined and described by their frequency, amplitude, and location • The EEG frequency is measured in Hertz (Hz)
• EEG waveforms are also viewed in the context of frequency for age and state of alertness
• The waveform may be assessed as abnormal if:• The waveform occurs at an inappropriate scalp location• The waveform demonstrates irregularities in rhythmicity or amplitude
• Most waves of frequencies of 8 Hz or higher are normal findings in the EEG of an awake adult
• Waves with a frequency of < 7 Hz are often classified as abnormal in awake adults (but are normal in children or in adults who are asleep)

TitleEEG Testing
Roy Sucholeiki, MD Director, Comprehensive Seizure and Epilepsy Program, The Neurosciences Institute at Central DuPage Hospital
EEG Waveform Frequency
• The frequencies of most brain waves range from are 0.5-500 Hz
• The categories, most clinically relevant, are as follows:▪ Alpha waves - 8-13 Hz
▪ Beta waves - Greater than 13 Hz
▪ Theta waves - 3.5-7.5 Hz
▪ Delta waves - 3 Hz or less
• Alpha waves generally represent attention and awareness and are seen in all age groups
• More common in adults and occur rhythmically on both sides of the head, with a slightly higher amplitude on the non-dominant side
• Beta waves are observed in all age groups and represent cortical processing and tend to be symmetric, small in amplitude, and more
evident anteriorly
• Drugs, such as barbiturates and benzodiazepines, may augment beta waves
• Theta waves represent memory and emotions of the limbic system; are normally seen during sleep at any age
• In the awake adult, theta waves are abnormal if they occur in excess. Theta and delta waves are known collectively as slow waves
• Delta waves are slow waves with a frequency of 3 Hz or less; are normally seen in deep sleep in adults, infants and children, but are
abnormal in the awake adult
• Delta waves may have the largest amplitude of all waves
• Delta waves can indicate focal or diffuse dysfunction

TitleEEG Testing
EEG Preparation: Before the Exam
• If the patient routinely takes seizure medication, antidepressants, or stimulants, he or she may be asked to stop taking these medications 1 to 2 days before the test
• The patient may be told not to consume caffeine before the test
• The patient should avoid using hair styling products (hairspray or gel) on the day of the exam
• It is prudent to have someone take the patient to the EEG location, especially if he or she has been asked to stop taking seizure medications
• If the patient is having a sleep EEG, he or she may be asked to stay awake the night before the exam
TitleEEG Testing
EEG: During the Procedure
There are 2 types of EEG monitoring:• Sleep EEG: the patient will be placed in a room that encourages relaxation in hopes of observing
the brain's electrical activity during sleep • The sleep EEG usually last about 2 to 3 hours
• Ambulatory EEG: this is a specialized ambulatory EEG where the electrodes are attached to a portable cassette recorder• The patient is then allowed to go home and resume normal activities while the EEG continuously records• The ambulatory EEG typically lasts 24 hours
General Concepts:• A standard noninvasive EEG takes about 1 hour• During this time period, the brain's electrical activity is recorded continuously • The patient may be positioned on a bed, table or chair; then an EEG technician (or other qualified
person) will attach 16 to 20 electrodes to the scalp• The technician may tell the patient to breathe slowly or quickly and may also utilize visual stimuli
such as flashing lights and then record the brain wave responses to such stimuli

TitleEEG Testing
Post EEG Instruction
• After the EEG is completed, the technician will remove the electrodes • Generally, there is no added required recovery time • The patient will be instructed on when to resume any medications• Remember, if the patient has been off their seizure medications, they may be at risk for a
seizure • Thus, the patient should not drive
• Until seizure medications are resumed, the patient should also avoid activities that may harm them if a seizure occurs

Title
EMG

TitleEMG
Bhimani. Anderson, Henly, & Stoddard, 2011, p.108
Electromyography (EMG)
Electromyography (EMG) is the clinical study of the electrical activity of muscle fibers individually and collectively:
• An electromyography detects the electric potential generated by muscle cells when these cells are electrically activated
• The signals are then analyzed for abnormalities during rest, with slight contraction, and forceful contraction• The EMG is often performed along side the nerve conduction study for similar reasons during the evaluation
of nerve functionality
EMG can be useful in the following ways:• As a diagnostics tool for identifying neuromuscular diseases (Ex: myasthenia gravis)• Assessment of nerve compression or injury (Ex: carpal tunnel, polymyositis, or sciatica from low back pain)• Assessment of disorders of motor control (Ex: muscular dystrophy)• Assessment of disorders that affect the motor neurons in the brain and spinal chord, such as amyotrophic
lateral sclerosis or polio• As a guide for neuromuscular blocking medications (botulinum toxin or phenol injections)• As a control signal for prosthetic devices such as prosthetic hands, arms, and lower limbs

TitleEMG
EMG Procedure
• The patient is positioned on an examination table and the skin is cleaned of oils
• A specialist inserts one or more small electrode needles through the skin into the muscle• The needles are placed at targeted areas being tested
• During the study, the surface electrodes will transmit a tiny electrical current that might be felt as a twinge or spasm • The needle electrode may cause discomfort or pain that usually ends shortly after the needle is removed
• The provider will also instruction the patient on when to rest and/or contract a muscle• Depending on what muscles and nerves the examiner testing, the patient may also be asked to change
positions during the exam
• Advantage/Disadvantage:
• Surface electrodes are sensitive and have minimal discomfort• Disadvantage is that the surface electrodes receive information from a large area, causing greater potential
for crosstalk interference from other adjacent muscles.• Disadvantage is that the fine needle insertion causes discomfort
• This can cause cramping due to increased tightness & spasticity in the muscle• When cramping occurs, the electrode have less capability to repeat
TitleEMG
EMG: Nursing Considerations
• This is an invasive procedure that produces slight discomfort
• Patients at risk for tissue injury include: thrombocytopenia, coagulopathies, and use of anticoagulant/antiplatelet
medications
• Complications are rare, but might include bleeding, infection, nerve injury, pneumothorax (if there is injury during
examination of the muscle along the chest)
• Since the EMG is conducted alongside the nerve conduction study, similar cautions must be taken regarding location
proximity to implanted devices (pacemaker, AICD, nerve stimulators etc.)
• Reasonable caution should be taken when testing in an extremity associated with lymphedema
• After the procedure, the patient may experience some temporary, minor bruising where the needle electrode were
inserted into the muscle
• This bruising should fade within several days
• Advise the patient to contact the provider if the bruising persists or worsens
• Post procedure, clarify with the provider, resumption or adjustment of pertinent patient medications (antiplatelet,
anticoagulant, steroids, and other medications used in motor/nerve disease processes)

Title
Nerve Conduction Studies

TitleNerve Conduction Study
Neurodiagnostic Testing: Nerve Conduction Study (NCS)
NCS are a commonly utilized non-invasive test purposed with evaluating the speed of conduction of an electrical impulse through a nerve in a motor and sensory pathwayThe speed of the nerve conduction is related to the diameter of the nerve and the degree of myelination:
• Theoretically, normal functioning nerves will transmit a stronger or faster signal than damaged nerves• NCS are primary utilized for evaluation of paresthesia and/or weakness of the extremities• The actual “measurement” of the nerve function is termed: nerve conduction velocity (NCV)
Indication for testing:• Evaluation of nerve damage• Differentiation between mononeuropathy vs polyneuropathy• Prognostic capability regarding the extent of nerve damage
Pathology: There are three main pathologic mechanisms affecting peripheral nerve:
• Axonal degeneration: produces a reduced amplitude in the NCS• Demyelination: when myelin is disrupted, it takes longer for the driving current to activate the next node to
threshold, resulting in slowing in internodal conduction and a reduced conduction velocity along that segment of nerve
• Conduction block: causes a conduction failure at the failure point of the axon; this can occur with acquired demyelinating nerve lesions
Evoked action potentials and conduction velocity in human sensory nerves: Buchthal F, Rosenfalck:Brain Res. 1966; 3:1.
TitleNerve Conduction Study
http://www.ncbi.nlm.nih.gov/books/NBK2 7199/#A7198
Common Disorders Diagnosed with NCS
Peripheral neuropathy• Mononeuropathy: Damage to a nerve outside the brain or spinal cord
• Carpal tunnel
• Multifocal neuropathy: Damage to two or more nerve areas• Vasculitides, rheumatoid arthritis, lupus, sarcoid, leprosy, Lyme disease, and amyloidosis
• Polyneuropathy: Simultaneous malfunction of many peripheral nerves• Diabetic neuropathy
• Myopathy• Muscular dystrophies: Group of diseases that cause progressive weakness and loss of muscle mass.• Myotonia: A neuromuscular condition in which the relaxation of a muscle is impaired.• Congenital myopathies: A broad term for any muscle disorder present at birth. This defect primarily affects skeletal muscle
fibers and causes muscular weakness and/or hypotonia.• Metabolic myopathies: Refers to a group of hereditary muscle disorders caused by specific enzymatic defects due to
defective genes
• Radiculopathy:• Nerve pain secondary to compression or inflammation of a spinal nerve. (ex: nerve compression from a herniated disc)
• Neuromuscular junction disorders• Group of disorders that result from destruction, malfunction or absence of one or more key proteins involved in
neuromuscular transmission (ex: Myasthenia gravis)

TitleNerve Conduction Study
NCS: Procedure
• Does not require anesthesia or sedation and takes roughly 30-90 minutes:
• Skin prep: Ensure the skin of the affected area of the patient is cleaned and dry
• Confirm proper grounding and functional electrodes. Ensure the electrodes are limited to the limb of interest
• Relative precaution with pacemakers: keep electrodes as far away from the heart as possible without crossing any implanted
cardiac devices
• Do not stimulate the nerve within 6 inches of pacemakers, implanted cardioverter-defibrillator, or other implanted stimulator
devices
• Avoid ipsilateral proximal stimulation sites where nerves might be bundled (Ex: axilla, Erb’s point)
• A provider will locate the nerves to be studied. The electrodes are attached to a recording electrode over the nerve with paste. In
addition, a stimulating electrode is placed at a set distance away from the recording electrode
• A small electrical stimulus is applied to affected nerve; electrodes measure the current of the stimulus along the nerve
pathway
• The nerve conduction velocity is calculated by measuring the distance between electrodes and the time it takes for the
electrical impulse to travel between the two electrodes
• Electromyogram (which measures the electrical activity of the muscle) is often performed at the same time to distinguish between
nerve vs muscle disorder
• Complications: minimal complications. The patient may experience discomfort (not typically “pain”) from the electrical current

Title
https://commons.wikimedia.org/wiki/File:Nerve_conduction_velocity.jpg
NCS
If a nerve is damaged, the current will be slower or weaker
TitleNerve Conduction Study
NCS: Nursing Considerations• NCS may be done in both inpatient and outpatient settings:
• No fasting or sedation is generally required for this procedure• Caution should be taken in the critical care settings which might predispose a patient to potential risk of electrical injury when a
patient is attached to multiple electrical devices plugged into different outlets• NCS may be performed safely in patients with implantable cardiac devices; caution should be exercised and a cardiologist
consulted before the study
• Advise the patient to stop use of lotions or oils on their skin for a few days prior to the procedure• Remove all clothing, hair pins, jewelry, eyeglasses, hearing aids or other metal items before the procedure• Maintain normal body temperature before and during the procedure:
• Low body temperature can slow nerve conduction
• After the procedure, the paste utilized to attach the electrodes will be removed • The patient may be instructed to avoid strenuous activities for the rest of the procedural day (returning to usual
activities the following day)
• Conditions that might interfere with the NCS:▪ Damaged spinal cord▪ Severe pain prior to the test▪ Changes in body temperature

TitleNerve Conduction Study
NCS: F Wave Responses
• In a routine motor and sensory nerve conduction study, an adjusted level of nerve stimulation is utilized to evaluate the nerve conduction in a segment of the limb
• F-wave studies: are late feedback analyses of the proximal portions of the motor axons (i.e., portions of nerves near the spinal cord)• The F-wave study utilizes maximal stimulation of a motor nerve to derive the conduction velocity of nerve
• In this type of NCS, the action potential travels from the site of the stimulating electrode in the limb to the spinal cord's ventral horn and then back to the limb in the same nerve that was stimulated
• Purpose: prognostication of clinical course and efficacy of treatment and diagnosis of focal and generalized peripheral nerve disorders:• Classification of nerve conduction abnormality caused by axonal degeneration, demyelination, and conduction block
• Therapeutic assessment and treatment of radiculopathy, plexopathies, and peripheral polyneuropathies (Guillain –Barre’, diabetic radiculopathies)
• Advantage/disadvantage:
• Evaluation of nerve segment innervated by the muscle being recorded
• Does not monitor the radiculopathy affecting the sensory nerve root
TitleNCS
NCS: H-Reflex Response and Repetitive Nerve Stimulation
• H-reflex study stimulates a nerve and records the reflex electrical discharge from a muscle in the limb:• Also evaluates conduction between the limb and the spinal cord, but in this case, the afferent impulses (those going
toward the spinal cord) are in sensory nerves while the efferent impulses (those coming from the spinal cord) are in motor nerves
• Repetitive nerve stimulation (RNS): during RNS, electrical stimulation is delivered to a motor nerve several times/second
• Changes in the muscle response are observed after a series of simulations. During this test, the joint is immobilized to minimize movement artifact
• Acetylcholinesterase inhibitors are discontinued before this study to prevent false negative results
• Temperature control must be maintained. Reduced temperature may result in a false negative result
• Purpose: helps differentiation between presynaptic and postsynaptic conduction in neuromuscular junction• Utilized in diagnosis of neuromuscular junction disorders: Myasthenia gravis (MG), Lambert-Eaton MG, botulism,
radiculopathy, peripheral neuropathy, polymyositis, myopathies, management of medication effects, and organophosphate poisoning
Title
Conclusion
Thank You
Neurodiagnostic Tests
EEG, EMG & Nerve Conduction
Module 5
Neurodiagnostics Conclusion

Title
Laboratory StudiesNeuropathology StudiesNeuropsychological Testing
Module 5

TitleIntroduction
2 of 19
Introduction, Objectives and Key Topics
Introduction▪ Cerebral spinal fluid (CSF) studies are conducted to determine if there is any blood or infection in the CSF as well as determining inflammatory or
demyelinating disease processes. Biopsies are indicated to determine or confirm a diagnosis. There are many neuropsychiatric assessments to
assess memory, intelligence, visuospatial, executive functioning, emotion, depression, and dementia.
Objectives▪ Describe the cerebral spinal studies used to diagnose neurological conditions.
▪ Summarize the indications for neurological biopsy procedures.
▪ Explain the components of a comprehensive neuropsychiatric assessment.
Key Points▪ Cerebral spinal fluid should be clear, colorless, with no WBCs or RBCs, glucose should be 2/3 blood glucose level, and protein level
of 14 - 45mg/100ml.
▪ Biopsy is tissue taken for histological evaluation.
▪ Neuropsychiatric assessments are conducted to assess memory, intelligence, visuospatial, executive functioning, emotion,
depression, and dementia.
TitleSpeaker Bio
Speaker Bio
• Cynthia Bautista, PhD, APRN, FNCS, FCNS
• Associate Professor, Egan School of Nursing, Fairfield University, Fairfield, CT
Cynthia Bautista, PhD, APRN, FNCS, FCNS
Title
Laboratory Studies
Module 5

TitleLaboratory Studies
4 of 19
Cerebral Spinal Fluid Studies: Cerebral Spinal Fluid (CSF)
• Gross appearance• Viscous: meningeal infection, cryptococci, metastatic mucinous adenocarcinoma
• Turbid: elevated WBC or RBC count, presence of bacteria
• Xanthochromia: presence of bilirubin, due to bleeding or elevated bilirubin
• Yellow: protein > 100 mg
• WBC count• Neutrophilic leukocytes: bacterial infection, fungal infection, chemical meningitis
• Lymphocytic cells: bacterial, viral, or fungal infection, parasitic diseases, T-cell leukemia virus, brain abscess, neoplasm, sarcoidosis, multiple sclerosis
• Eosinophils: lymphoma, helminth infection

TitleCerebral Spinal Fluid Studies
5 of 19
Normal and Abnormal Characteristics of Cerebral Spinal Fluid
Characteristic Normal Abnormal
Color Clear, colorless Cloudy, often due to presence of WBCs or bacteria
Xanthochromic due to presence of RBCs
WBCs 0–5/mm3, all mononuclear Elevated for tumor, meningitis, subarachnoid hemorrhage, infarct, or abscess
RBCs None Presence due to traumatic tap or subarachnoid hemorrhage
Chloride 120–130 mEq/L Decreased levels associated with meningeal infection and tuberculosis meningitis.
Glucose 50–75 mg/100 ml Decreased level associated with presence of bacteria
Pressure 70–180 mm H2O Low: inaccurate placement of needle, dehydration, or block along SAS or at foramen magnumElevated: benign intracranial hypertension; cerebral edema; CNS tumor, abscess, or cyst; hydrocephalus; muscle tension or abdominal compression; or subdural hematoma
Protein 14–45 mg/100 ml Elevated: demyelinating/degenerative disease, Guillain-Barré syndrome, hemorrhage infection, and spinal block tumor

TitleCerebral Spinal Fluid Studies
6 of 19
Cerebral Spinal Fluid Studies: Microbiology and Serology
• Positive CSF culture has a 92% sensitivity and 95% specificity• Gold standard for diagnosing bacterial meningitis
• CSF Serology preferred for syphilis, brucellosis, and Lyme disease
TitleCerebral Spinal Fluid Studies
7 of 19
Cerebral Spinal Fluid Studies: CSF Chemistries
• Glucose: deceased with bacteria
• Protein: elevated with bacterial meningitis
• Lactate: elevated with bacterial meningitis, non-Hodgkin lymphoma, head injury, anoxia
• Chloride: decrease of 25% in tuberculous meningitis
• Glutamate: greater than 35mg/dl associated with hepatic encephalopathy

TitleLaboratory Studies
8 of 19
Tumor Markers
• Metastatic carcinoma (from breast, lung, bowel) with negative cytology• Elevated CSF carcinoembryonic antigen
• Metastatic leptomeningeal adenocarcinoma and acute myeloblastic leukemia • Elevated beta glucuronidase
• Various CNS tumors, especially myeloid and mycotic leukemias • Elevated lysozyme (i.e., muramidase)

Title
Neuropathology Studies
Module 5
TitleNeuropathology Studies
10 of 19
Biopsy
• Tissue taken for histological evaluation
• Performed at site of suspected lesion within the central or peripheral nervous system
• Indicated to determine or confirm a diagnosis
• Brain biopsy is most often done using stereotactic methods• Complications include hemorrhage, infection, and neurological deficits

Title
Neuropsychological Testing
Module 5

TitleNeuropsychological Testing
12 of 19
Memory
Test Purpose Procedure Timing
Wechsler Memory Scale Memory function 1. Memory span 2. Mental control 3. Current Information 4. Orientation 5. Logical memory6. Visual reproduction
20 – 25 minutes
California Verbal Learning Test Verbal memory 1. 16 common words2. Second list is given3. Recall the first list
20 minutes
Brief Visuospatial Memory Test - Revised Nonverbal memory 1. Geometric designs 2. Repeat the exercise
45 minutes
TitleNeuropsychological Testing
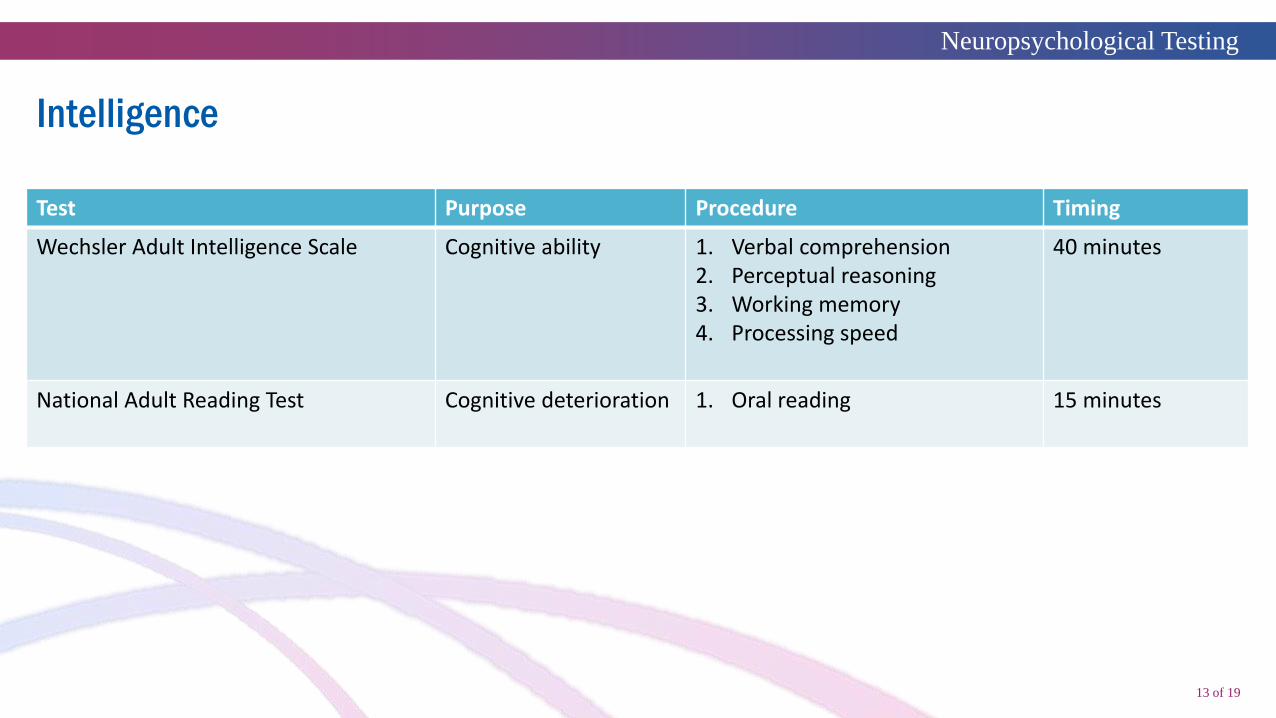
13 of 19
Intelligence
Test Purpose Procedure Timing
Wechsler Adult Intelligence Scale Cognitive ability 1. Verbal comprehension2. Perceptual reasoning3. Working memory4. Processing speed
40 minutes
National Adult Reading Test Cognitive deterioration 1. Oral reading 15 minutes

TitleNeuropsychological Testing
14 of 19
Visuospatial
Test Purpose Procedure Timing
Rey-Osterrieth Complex VisuospatialMemoryAttentionPlanningExecutive
1. Copy is placed in front of subject, who is asked to replicate it
2. After short time, asked to replicate from memory
3. After 20 min, asked to replicate from memory
30 minutes
Clock Test VisuospatialConstructional disabilities
1. Make simple free-hand drawings of a clock face, a daisy, a house, a person, and a bicycle
5 minutes
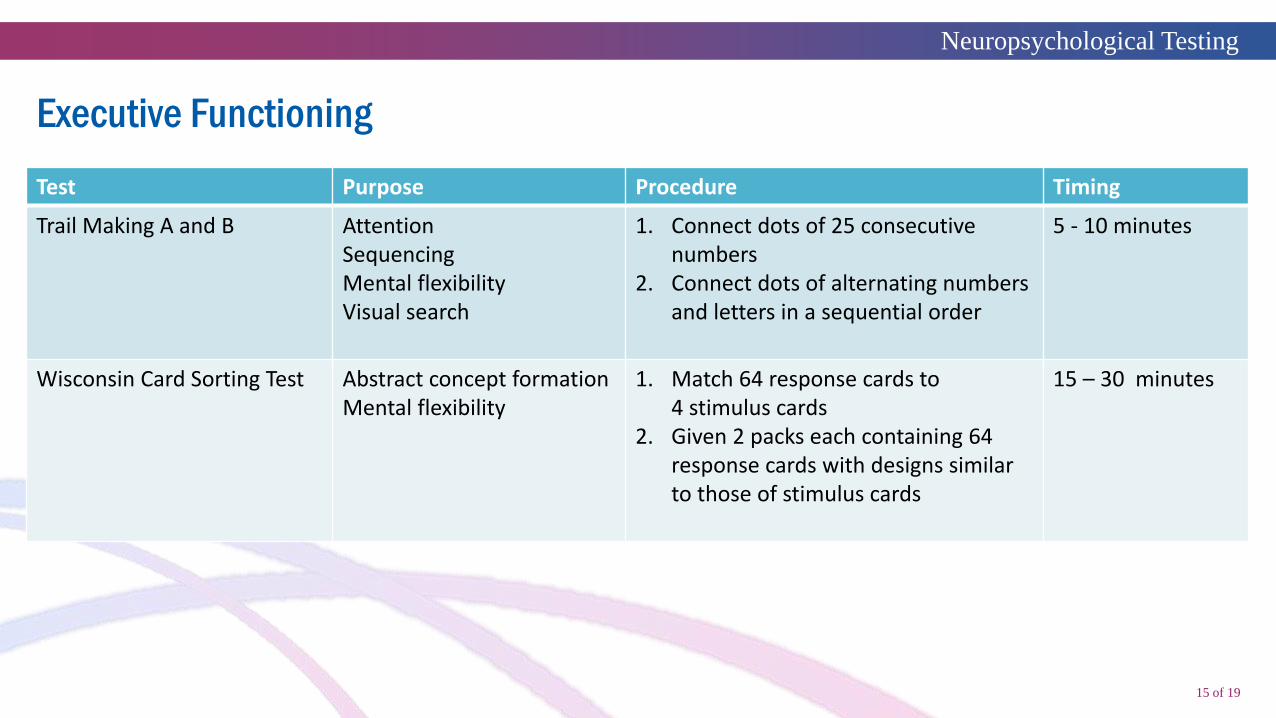
TitleNeuropsychological Testing
15 of 19
Executive Functioning
Test Purpose Procedure Timing
Trail Making A and B AttentionSequencingMental flexibilityVisual search
1. Connect dots of 25 consecutive numbers
2. Connect dots of alternating numbers and letters in a sequential order
5 - 10 minutes
Wisconsin Card Sorting Test Abstract concept formationMental flexibility
1. Match 64 response cards to 4 stimulus cards
2. Given 2 packs each containing 64 response cards with designs similar to those of stimulus cards
15 – 30 minutes
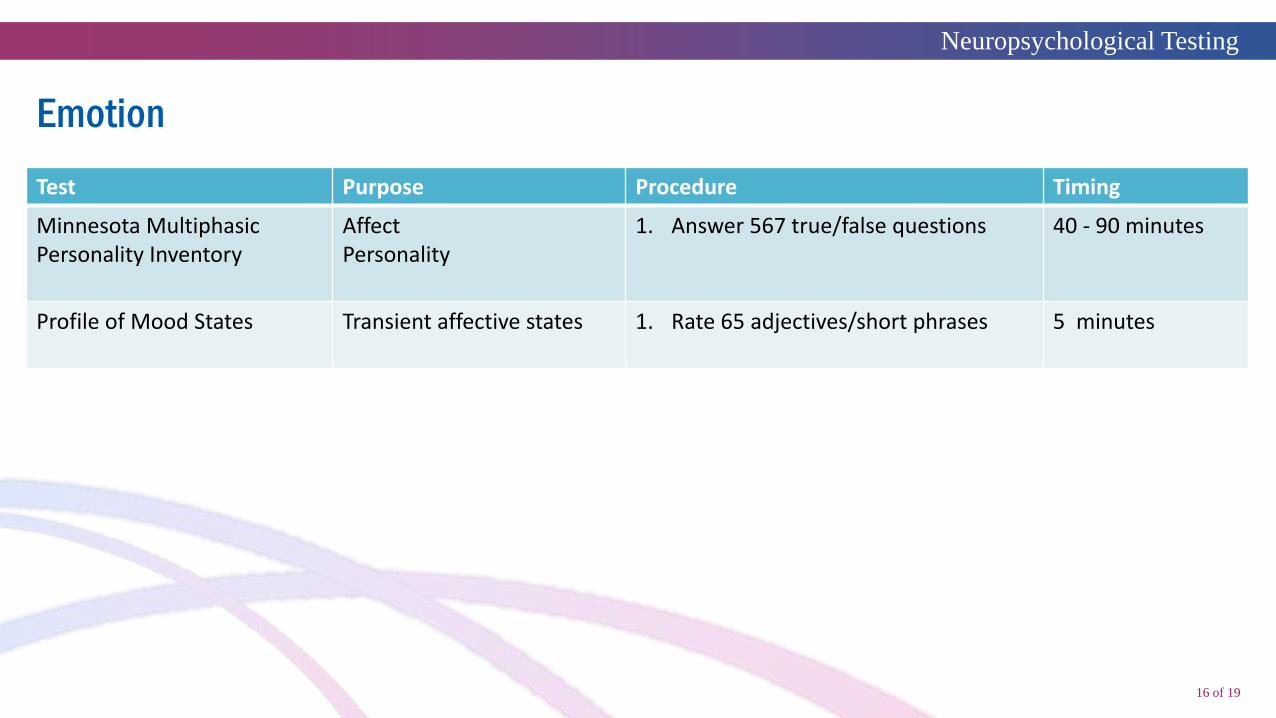
TitleNeuropsychological Testing
16 of 19
Emotion
Test Purpose Procedure Timing
Minnesota Multiphasic Personality Inventory
AffectPersonality
1. Answer 567 true/false questions 40 - 90 minutes
Profile of Mood States Transient affective states 1. Rate 65 adjectives/short phrases 5 minutes

TitleNeuropsychological Testing
17 of 19
Depression Screening
Test Purpose Procedure Timing
Hamilton Depression Rating Scale Severity of depression 1. Answer 21 questions 10 minutes
Beck Depression Inventory Severity of depression 1. Answer 21 questions 10 minutes
Patient Health Questionnaire Screens for depression 1. Answer 9 questions 5 – 10 minutes
Major Depression Inventory Generates diagnosisEstimates severity
1. Answer 12 questions 10 minutes
Geriatric Depression Scale Assess depression in older adults
1. Answer 30 questions 10 minutes

TitleNeuropsychological Testing
18 of 19
Dementia
Test Purpose Procedure Timing
Mini-Mental State Exam Severity of dementia 1. Answer 30 questions 5 - 10 minutes
Clock Drawing Screens for dementia 1. Make a free-hand drawing of a clock face
5 minutes
Montreal Cognitive Assessment Screens for dementia 1. Answer 30 questions 10 minutes
Saint Louis UniversityMental State Exam
Screens for dementia 1. Answer 11 questions 10 minutes

Title
Conclusion
Thank You
Neurodiagnostic Test
Module 5
Conslusion