
Neurocognitive Deficit in Schizophrenia: A Quantitative ... · (De Renzi & Vignolo, 1962); Peabody...
20
Neuropsychology 1998, Vol. 12, No. 3,426-445 Copyright 1998 by the American Psychological Association, Inc. 0894-4105/98/$3.00 Neurocognitive Deficit in Schizophrenia: A Quantitative Review of the Evidence R. Walter Heinrichs and Konstantine K. Zakzanis York University The neurocognitive literature on test performance in schizophrenia is reviewed quantitatively. The authors report 22 mean effect sizes from 204 studies to index schizophrenia versus control differences in global and selective verbal memory, nonverbal memory, bilateral and unilateral motor performance, visual and auditory attention, general intelligence, spatial ability, executive function, language, and interhemispheric tactile-transfer test performance. Moder- ate to large raw effect sizes (d > .60) were obtained for all 22 neurocognitive test variables, and none of the associated confidence intervals included zero. The results indicate that schizophrenia is characterized by a broadly based cognitive impairment, with varying degrees of deficit in all ability domains measured by standard clinical tests. It is expected that schizophrenia will be understood in the near future as a kind of brain disease. Substantive and technical advances in the neurosciences are being brought to bear on the problem of tracking the disordered cognition and behavior of schizophrenia to dysfunctional brain structures and systems. Evidence from neuropsychological, neuropatho- logical, and neuroimaging studies has revived interest in schizophrenia as a neuropsychiatric disease with a putatively identifiable neuropathophysiology (Andreasen et al., 1994; Heinrichs, 1993; Levin, Yurgelun-Todd, & Craft, 1989; Randolph, Goldberg, & Weinberger, 1993). From a behavioral perspective there is broad agreement that schizophrenia produces impairment of neuropsychologi- cal function. Individuals with the illness are likely to exhibit impairment on a wide assortment of neuropsychological tasks (Blanchard & Neale, 1994). Recent findings include deficits in attention (Braff, 1993; Cornblatt & Keilp, 1994), executive function (Gruzelier, Seymour, Wilson, Jolley, & Hirsch, 1988; Heinrichs, 1990; Van der Does & Van den Bosch, 1992; Weinberger, Wagner, & Wyatt, 1986), motor and tactile dexterity (Goldstein & Zubin, 1990; Schwartz, Carr, Munich, & Bartuch, 1990), spatial abilities (Green & Walker, 1985; Raine, 1992; Stuss et al., 1983), affect recognition (Andreasen & Ehrhardt, 1982; Ennis & Whelton, 1994), intellectual ability (Goldberg, Gold, Greenberg, & Griffin, 1993), language functions (Crawford, Obonsawin, & Bremner, 1993), and memory (Paulsen et al., 1995; Randolph et al., 1994; Saykin et al., 1991). Although a number of narrative reviews have described R. Walter Heinrichs and Konstantine K. Zakzanis, Department of Psychology, York University, Toronto, Ontario, Canada. An earlier version of this research was presented at the American Psychological Association Annual Convention, Toronto, Canada, August 1996 and at the International Congress of Psychology, Montreal, Canada, August 1996. Correspondence concerning this article should be addressed to R. Walter Heinrichs, Department of Psychology, York University, 4700 Keele Street, Toronto, Ontario, Canada, M3J 1P3. Electronic mail may be sent to [email protected]. and integrated neurocognitive findings on schizophrenia (e.g., Heaton & Crowley, 1981; Heinrichs, 1993; Levin et al., 1989; Randolph et al., 1993), there has been no comprehensive quantitative evaluation of this literature. In view of the increasing use of neurocognitive measures in schizophrenia research and the accumulation of empirical evidence, we undertook such an evaluation. A number of questions were formulated to guide our review: 1. Does neurocognitive testing provide reliable evidence of impairment in schizophrenia and what is the average magnitude of difference between patients and healthy con- trols? 2. Do tests of specific neurocognitive functions (e.g., memory, language, attention) reveal similar magnitudes of difference between patients and controls or are some aspects of neurocognitive performance spared in the illness? 3. Are there relationships between neurocognitive impair- ment and clinical and demographic attributes of patients and controls? 4. Are there relationships between specific neurocognitive functions and more general tests of ability (e.g., IQ)? Accordingly, the goal of our research was to estimate the consistency, strength, and selectivity of neurocognitive deficits in schizophrenia. To accomplish this goal we compiled the results of multiple studies using meta-analytic techniques. In addition to solving potential problems with traditional literature reviews (see Wolf, 1986), meta-analysis provides tools for the analysis of magnitude and consistency of evidence (i.e., effect size d, distribution nonoverlap percentage, confidence intervals) as well as tools to assess variables that may mediate the magnitude and consistency of evidence (i.e., moderator variable analysis). The effect size estimate d measures the degree to which the phenomenon is present in the population (Cohen, 1988). In mathematical terms, d is the difference between patient and control means on a variable of interest calibrated in pooled standard deviation units. Effect size analysis allows the pitfalls of null hypothesis-statistical significance testing to be avoided, including faulty conclusions about a hypothesis that are 426 This document is copyrighted by the American Psychological Association or one of its allied publishers. This article is intended solely for the personal use of the individual user and is not to be disseminated broadly.
Transcript of Neurocognitive Deficit in Schizophrenia: A Quantitative ... · (De Renzi & Vignolo, 1962); Peabody...

Neuropsychology1998, Vol. 12, No. 3,426-445
Copyright 1998 by the American Psychological Association, Inc.0894-4105/98/$3.00
Neurocognitive Deficit in Schizophrenia:A Quantitative Review of the Evidence
R. Walter Heinrichs and Konstantine K. ZakzanisYork University
The neurocognitive literature on test performance in schizophrenia is reviewed quantitatively.
The authors report 22 mean effect sizes from 204 studies to index schizophrenia versus control
differences in global and selective verbal memory, nonverbal memory, bilateral and unilateral
motor performance, visual and auditory attention, general intelligence, spatial ability,
executive function, language, and interhemispheric tactile-transfer test performance. Moder-
ate to large raw effect sizes (d > .60) were obtained for all 22 neurocognitive test variables,
and none of the associated confidence intervals included zero. The results indicate that
schizophrenia is characterized by a broadly based cognitive impairment, with varying degrees
of deficit in all ability domains measured by standard clinical tests.
It is expected that schizophrenia will be understood in thenear future as a kind of brain disease. Substantive andtechnical advances in the neurosciences are being brought tobear on the problem of tracking the disordered cognition andbehavior of schizophrenia to dysfunctional brain structures
and systems. Evidence from neuropsychological, neuropatho-logical, and neuroimaging studies has revived interest inschizophrenia as a neuropsychiatric disease with a putativelyidentifiable neuropathophysiology (Andreasen et al., 1994;Heinrichs, 1993; Levin, Yurgelun-Todd, & Craft, 1989;Randolph, Goldberg, & Weinberger, 1993).
From a behavioral perspective there is broad agreementthat schizophrenia produces impairment of neuropsychologi-cal function. Individuals with the illness are likely to exhibitimpairment on a wide assortment of neuropsychologicaltasks (Blanchard & Neale, 1994). Recent findings includedeficits in attention (Braff, 1993; Cornblatt & Keilp, 1994),executive function (Gruzelier, Seymour, Wilson, Jolley, &Hirsch, 1988; Heinrichs, 1990; Van der Does & Van denBosch, 1992; Weinberger, Wagner, & Wyatt, 1986), motor
and tactile dexterity (Goldstein & Zubin, 1990; Schwartz,Carr, Munich, & Bartuch, 1990), spatial abilities (Green &Walker, 1985; Raine, 1992; Stuss et al., 1983), affectrecognition (Andreasen & Ehrhardt, 1982; Ennis & Whelton,1994), intellectual ability (Goldberg, Gold, Greenberg, &Griffin, 1993), language functions (Crawford, Obonsawin,& Bremner, 1993), and memory (Paulsen et al., 1995;Randolph et al., 1994; Saykin et al., 1991).
Although a number of narrative reviews have described
R. Walter Heinrichs and Konstantine K. Zakzanis, Departmentof Psychology, York University, Toronto, Ontario, Canada.
An earlier version of this research was presented at the AmericanPsychological Association Annual Convention, Toronto, Canada,August 1996 and at the International Congress of Psychology,Montreal, Canada, August 1996.
Correspondence concerning this article should be addressed toR. Walter Heinrichs, Department of Psychology, York University,4700 Keele Street, Toronto, Ontario, Canada, M3J 1P3. Electronicmail may be sent to [email protected].
and integrated neurocognitive findings on schizophrenia(e.g., Heaton & Crowley, 1981; Heinrichs, 1993; Levin etal., 1989; Randolph et al., 1993), there has been no
comprehensive quantitative evaluation of this literature. Inview of the increasing use of neurocognitive measures in
schizophrenia research and the accumulation of empiricalevidence, we undertook such an evaluation. A number of
questions were formulated to guide our review:
1. Does neurocognitive testing provide reliable evidenceof impairment in schizophrenia and what is the average
magnitude of difference between patients and healthy con-trols?
2. Do tests of specific neurocognitive functions (e.g.,memory, language, attention) reveal similar magnitudes ofdifference between patients and controls or are some aspects
of neurocognitive performance spared in the illness?3. Are there relationships between neurocognitive impair-
ment and clinical and demographic attributes of patients andcontrols?
4. Are there relationships between specific neurocognitivefunctions and more general tests of ability (e.g., IQ)?
Accordingly, the goal of our research was to estimate the
consistency, strength, and selectivity of neurocognitive
deficits in schizophrenia. To accomplish this goal wecompiled the results of multiple studies using meta-analytic
techniques. In addition to solving potential problems withtraditional literature reviews (see Wolf, 1986), meta-analysisprovides tools for the analysis of magnitude and consistency
of evidence (i.e., effect size d, distribution nonoverlappercentage, confidence intervals) as well as tools to assessvariables that may mediate the magnitude and consistency ofevidence (i.e., moderator variable analysis). The effect sizeestimate d measures the degree to which the phenomenon ispresent in the population (Cohen, 1988). In mathematicalterms, d is the difference between patient and control meanson a variable of interest calibrated in pooled standarddeviation units. Effect size analysis allows the pitfalls of nullhypothesis-statistical significance testing to be avoided,including faulty conclusions about a hypothesis that are
426
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

NEUROCOGNITIVE DEFICIT IN SCHIZOPHRENIA 427
based on a count of significant and nonsignificant studies
(see Bakan, 1966; Cohen, 1994; Schmidt, 1996). Variability
of effect sizes across studies can be indexed by common
statistics like standard deviations and confidence intervals
but also by formal tests of homogeneity (see Hedges, 1994;
Hedges & Olkin, 1985; Rosenthal, 1991, 1995). This
variability in effects can be explored and articulated through
moderator variable analysis if it is due to study differences in
sample or design features.
With these considerations in mind we organized 22 neurocog-
nitive test variables into meta-analyses to summarize the
magnitude of schizophrenia-control discrimination hi the
published literature (see Table 1). These variables reflected
memory, motor, attention, intelligence, spatial function, execu-
tive ability, language, and interhemispheric transfer processes.
Effect sizes were calculated for each of the individual
dependent variables. Attribute variables (e.g., age, education,
hospitalizations, etc.) were recorded and, when numbers
warranted, were correlated with neurocognitive effect sizes
to explore the contribution of moderators to effect size variation.
Table 1
Neurocognitive Categories and Tests Used in Meta-Analyses
Construct Recorded test variables
Global Verbal Memory
Selective Verbal Memory
Nonverbal Memory
Motor
Attention
General Intelligence
Spatial Ability
Executive Function
Language Function
Tactile-Transfer
CVLT: Trials I-V recallRAVLT: Trials I-V recallPortland Paragraph: immediate recallSelective Reminding Test: sum recallLNNB: memory indexWMS: logical memory scoreWMS-R: verbal memory indexCVLT: long-delay free recall, percentage words retained,
number of intrusions, recognition trial hitsWMS-R: logical memory IIRAVLT: recognition trial hitsRMT: memory for wordsROCFT: recall trials scoreWMS, WMS-R: visual reproduction trialsBVRT: recall trialsRMT: memory for facesPurdue Pegboard: dominant hand score, bilateral scoreGrooved Pegboard: dominant hand scoreFinger Tapping Test: dominant hand scoreWAIS-R: Digit SpanTrail Making Test: Parts A and BCPT: hits, discrimination scoreStroop Test: interference scoresWAIS-R: Full Scale, Verbal, and Performance IQNon-WAIS-R: NART IQ, ILS, Quick Test, Mill Hill
Verbal IQ, and Wonderlic Personnel TestBenton Line Orientation Test: number correctBenton Facial Recognition Test: corrected scoreWAIS-R: block design scoreWCST: categories achieved, number of perseverative responses,
number of perseverative errors, percent perseverative errorsWord Fluency: COWAT, Chicago WFTToken Test: adjusted score, correct responsesVocabulary: WAIS-R vocabulary, Mill Hill, ILS,
Peabody Picture VocabularyContralateral finger localization, tactile recognition scores
Note. CVLT = California Verbal Learning Test (Delis et al., 1987); RAVLT = Rey Auditory VerbalLearning Test (Lezak, 1995, pp. 438^42); Portland Paragraph (Lezak, 1995, p. 462); SelectiveReminding Test (Buschke & Fuld, 1974); LNNB = Luria-Nebraska Neuropsychological Battery(Golden et al., 1985); WMS = Wechsler Memory Scale (Wechsler, 1945); WMS-R = WechslerMemory Scale—Revised (Wechsler, 1987); RMT = Recognition Memory Test (Warrington, 1984);ROCFT = Rey-Osterrieth Complex Figure Test (Lezak, 1995, pp. 475^80); BVRT = Benton VisualRetention Test (Benton, 1974); Purdue Pegboard (Tiffin, 1968); Grooved Pegboard (Klove, 1963);Finger Tapping Test (Reitan & Wolfson, 1993); WAIS-R = Wechsler Adult Intelligence Scale-Revised (Wechsler, 1981); Trail Making Test (Reitan, 1958); CPT = Continuous Performance Test(Nuechterlein & Dawson, 1984); Stroop Test (Golden, 1978; Stroop, 1935); NART = National AdultReading Test (Nelson, 1982); ILS = Institute of Living Scale (Shipley, 1946); Quick Test (Ammons& Ammons, 1962); Mill Hill Scale (Raven, 1982); Wonderlic Personnel Test (Wonderlic, 1978);Benton Line Orientation and Facial Recognition Tests (Benton et al., 1994); WCST = WisconsinCard Sorting Test (Heaton et al., 1993); COWAT = Controlled Oral Word Association Test (Benton& Hamsher, 1983); Chicago WFT = Chicago Word Fluency Test (Milner, 1964); Token Test(De Renzi & Vignolo, 1962); Peabody Picture Vocabulary Test (Dunn & Dunn, 1981).
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

428 HEINRICHS AND ZAKZANIS
Method
Literature Search
The PsycINFO and Medline databases were used to find studies for
inclusion in the meta-analyses. The key words used are included in the
Appendix. The articles located by die computer search were limited to
published English language articles. According to Green and Hall
(1984), meta-analysts doing a literature search should also page through
the volumes of pertinent journals for a topic year by year. This was done
with every issue for the two relevant specialty journals, Schizophrenia
Research and Schizophrenia Bulletin, as well as for six psychiatric and
psychological journals that publish a high volume of studies on
schizophrenia (American Journal of Psychiatry, Archives of General
Psychiatry, Biological Psychiatry, British Journal of Psychiatry, Jour-
nal of Abnormal Psychology, and Journal of Nervous and Mental
Disease) and five journals in neuroscience and behavior that publish
schizophrenia research but at a lower frequency than the psychiatric
journals (Brain, Journal of the International Neuropsychological Soci-
ety, Neuropsychologf, Neuroscience, and Neuropsychopharmacology).
This proved to be an effective supplementary way to search for articles,
given the small and focused set of key words in any particular abstract or
title that a computer database uses to search for key words. Despite its
apparent cost in time, (he reasoning behind using the individual journal
technique was to avoid missing a useful article that lies outside the
database's regular purview. Although absolute coverage of the entire
relevant literature is hard to achieve, this serves to reduce the likelihood
that bias was involved in the search outcome (White, 1994).
In the course of the literature search, the frequency with which
any given neurocognitive variable was reported across studies
dictated suitability for meta-analytic synthesis. If the variable was
reported in two or more primary studies, the variable was tracked
for meta-analytic synthesis. In this way, studies were compiled for
22 meta-analyses of different neurocognitive test measures.
Criteria for Inclusion
Articles were included if they met the following criteria: (a)
publication between 1980 and 1997, (b) research designs with a
control group comprising healthy participants, and (c) study
statistics convertible to effect size d (e.g., means, standard devia-
tions, F, t, x2; see Wolf, 1986). Studies reporting only significancelevels with no descriptive or inferential statistics were excluded.
The year 1980 was chosen as a year of publication criterion
because it corresponded roughly to the introduction and use of
more systematic and reliable diagnostic criteria for schizophrenia,
such as the Diagnostic and Statistical Manual of Mental Disorders
(3rd ed.; DSM-lll; American Psychiatric Association, 1987). The
year 1997 was chosen as an upper year limit to ensure maximal
coverage of the literature by the computer-based journal databases.
However, there is typically a delay of a few months between
journal publication and availability in the database, and our article
search took place in mid-1997. Therefore, coverage of 1997 articles
was incomplete.If these criteria were met, the article was then assessed for two
additional criteria. First, schizophrenic patients must have met diagnos-
tic criteria for either the DSM-lll (or later) or the International
Classification of Diseases (ICD-9 or 10) classification systems and have
satisfied these criteria on the basis of a structured clinical interview.
Second, neurocognitive tests must have been administered by an
examiner trained in standardized testing procedures and supervised by a
psychologist This was important to track in order to ensure that thequality of the neurocognitive assessment administered in each study was
held relatively constant and did not influence the findings, hi the case of
neurocognitive data published in drug trials, only studies reporting
pretreatnient baseline data were included.
If the research article met the above criteria, its content
variable(s) was included in one (or more) of the meta-analyses. In
the case of separately published studies that used the same
participant samples, the decision rule was adopted to treat these
studies as a single study with multiple independent variables
(Hedges & Olkin, 1985). The d statistic (Cohen, 1988) was
calculated for each comparison as the difference between schizo-
phrenia and control group means normalized by the pooled
standard deviation. Whenever means and standard deviations were
reported, these were used to derive effects. When inferential
statistics were reported without central tendency and dispersion
data, the effects were calculated from these statistics based on
formulas provided by Wolf (1986).
Recorded Variables
Recorded variables for every article used in each of the
meta-analyses included the journal name, title, author(s), and date
of publication of the article. Recorded potential moderator vari-
ables of interest included mean age and education in control and
patient samples; for the patient samples, the chlorpromazine-
equivalent medication dose (equivalent neuroleptic daily dosage in
mg), percentage of male participants, onset age (defined as the age
at first psychiatric admission) and duration of illness, percentage of
patients on medication, and number of psychiatric hospitalizations
were recorded. These study characteristics were used to describe
the study set retrieved and for moderator variable analysis.
Organizing the myriad of neurocognitive test variables reported
in the literature into a coherent classification was a major chal-
lenge. Several strategies exist in the literature for organizing
diverse tests into categories of neurocognitive function, and each of
these strategies has advantages and disadvantages. First, there are a
priori approaches such as Lezak's (1995) classification, which are
influenced by theoretical and practice-related considerations about
the test measures and their putative underlying processes. For
example, Lezak includes motor and executive ability tasks in the
same chapter, presumably on the basis of a common substrate in the
frontal brain or some other assumed link. Such classifications have
no quantitative statistical underpinning, and even advocates of this
approach admit to an element of arbitrariness in test organization
(see Lezak, pp. 333-334). A second approach is based on factor-
analytic studies of neuropsychological test batteries (see Goldstein,
1984, pp. 184-210). Factor analysis provides a quantitative descrip-
tion that relates different tests to a smaller number of underlying
abilities. However, the validity of this approach as a general
strategy for organizing tests in a meta-analysis depends in part on
the availability of factor analyses that include all of the tests in the
literature on neuropsychology and schizophrenia. In practice it is
the standard test batteries like the Halstead-Reitan (e.g., Ernst,
Warner, Hochberg &, Townes, 1988) and Luria-Nebraska (e.g.,
McKay & Golden, 1981) that tend to be studied factor analytically.In the present case, we were unable to find factor-analytic studies of
schizophrenic samples that included all, or even most, of theneurocognitive test variables reported in the literature. Finally, it is
possible to avoid constructs altogether and simply compile effects
for individual tests. This approach incorporates the fewest assump-
tions about the data; however, it is unwieldy in view of the dozens
of tests in common use and the inconsistency with which different
scores from the same test are reported in the literature (e.g.,categories vs. perseverative errors, Wisconsin Card Sorting Test;
see Heaton, Chelune, Talley, Kay, & Curtiss, 1993).A further consideration is that regardless of classification method,
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

NEUROCOGNITIVE DEFICIT IN SCHIZOPHRENIA 429
many neurocognitive tests are probably influenced by several compo-
nent processes. Thus, scores on the Vocabulary subtest of the Wechsler
Adult Intelligence Scale—Revised (WAIS-R; Wechsler, 1981) may
reflect both basic language abilities and general intelligence; scores on
the Trail Making Test (Reitan, 1958) may reflect visual scanning and
perception but also motor speed, hand-eye coordination, and attention
(Lezak, 1995, pp. 382-384). Hence it may be misleading to categorize
tests on the basis of a faulty assumption that test performance is
determined by only one process.
Accordingly, whenever possible we tried to avoid aggregating
different tests and their effect sizes into hypothetical categories and
adopted a strategy, presented in Table 1, whereby effect sizes were
calculated and reported on individual tests, to most cases effect sizes
were grouped into a priori categories for presentation only and not for
statistical purposes. However, this was not feasible for memory test
variables because of the diversity of tests and related variables reported
in the literature. Hence memory test variables were selected and
aggregated into three effect size categories: global verbal, selective
verbal, and nonverbal. The global verbal memory category included
summary indexes of performance like total words recalled across
learning trials and verbal memory quotients. Selective memory vari-
ables included delayed-recall scores, savings over time, and intrusion
error rates. These selective variables are believed to be more sensitive
than global scores to memory disorders involving the medial temporal-
diencephalic system (see Delis, Kramer, Kaplan & Ober, 1987, pp. 2-3;
Lezak, 1995, pp. 147-150). Non-verbal memory variables included
recall scores for visual stimuli such as shapes and patterns that did not
involve language. The distinction between verbal and nonverbal memory
has a long history in neuropsychology and reflects the existence ofdistinct, or "material-specific," memory disorders in neurological
patients (Calev, Edelist, Kugelmass, & Lerer, 1991). Similarly, tests of
unilateral manual dexterity and finger oscillation were collapsed into a
unilateral motor category. This arrangement is supported by factor-
analytic studies showing the emergence of a distinct motor factor in
psychiatric populations (e.g., Goldstein & Shelly, 1972). These testsincluded Finger Tapping (Reitan & Wolfson, 1993), the Grooved
Pegboard (Klove, 1963), and the Purdue Pegboard (Tiffin, 1968).
The executive category comprised several test variables from the
Wisconsin Card Sorting Test (WCST; Heaton et al., 1993). This is by far
the most widely used test of executive ability in schizophrenia studies
(see Van der Does & Van den Bosch, 1992). Like Saykin et aL (1991),we combined perseveration (including perseverative responses, errors,
and percentage of perseverative errors) and categories scores into an
overall index of WCST performance. In the event that studies reporteddata on attempts to teach schizophrenia patients how to do the test, only
preinstruction baseline data were used.
Attention is a basic neurocognitive function involved to some
degree in all test performances. Nonetheless, several tests make
relatively modest demands on higher-level cognition and are
regarded primarily as measures of attention, selection, concentra-tion, and vigilance. They include two forms of digit span tasks: one
with concurrent distraction (Oltmanns, 1978) and one without
(WAIS-R, Digit Span subtest; Wechsler, 1981). Digit Span meta-
analysis was composed of test scores from both of these paradigms.
In addition, the Continuous Performance Test (CPT) is a class of
attentional tasks that all involve a requirement to respond to target
and ignore nontarget stimuli over a period of time. Scores like
target "hits," errors, and sensitivity measures ("d") based on
signal detection theory are available for the test. In their analysis of
the CPT, Van den Bosch, Rombouts, and van Asma (1996)
concluded that motor speed along with attentional mechanisms
contribute to successful performance. The same almost certainlyapplies to the Trail Making Test (Reitan, 1958), which Lezak
(1995, pp. 382-384) considers an attentional task with perceptual
and motor components. In addition, the Trail Making Test has two
forms that differ in complexity, namely, Part A and Part B. In
contrast, the Stroop Test (Golden, 1978; Stroop, 1935) does not
require a manual response. The strength of the interference trial
effect, where participants have to name perceptually incongruent
color words, has long been regarded as a measure of selective
attention in both clinical and experimental psychology. Completion
time or errors were coded for Part A and Part B of the Trail Making
Test. Continuous Performance Test scores included hits, "d," and
errors. Interference scores, error, or reaction time in the incongru-
ent color-word condition were collected for the Stroop Test.
Full-scale IQ scores were indexed from articles using the
WAIS-R, the Quick Test, the National Adult Reading Test (NART),
the Wonderlic Personnel Test (Wonderlic, 1978), and the Peabody
Picture Vocabulary Test (see Table 1). Intelligence quotients
derived from the WAIS-R were treated separately from those
derived from alternative tests like the NART. Only WAIS-R
performance IQs were gathered for the performance IQ meta-
analytic synthesis. The verbal IQ meta-analysis also included testscores from the WAIS-R only.
Spatial abilities were assessed with the Block Design subtest
(WAIS-R), and two tests from Benton's (Benton, Sivan, Hamsher,
Varney, & Spreen, 1994) laboratory, Facial Recognition and Line
Orientation (see Table 1).
In the domain of language, word fluency test scores collected
included data from the Chicago Word Fluency Test (Milner, 1964)
and the Controlled Oral Word Association Test (Benton & Ham-
sher, 1983), as well as from generically named word fluency tasks.
Recorded vocabulary scores were taken from the WAIS-R, Shipley,
and Mill Hill scales (see Table 1). The Token Test (De Renzi &
Vignolo, 1962) was used to index receptive language.
Finally, the interhemispheric transfer-task meta-analysis was
made up of scores from finger localization tests and transfer-task
test scores (see Bellini et al., 1991; Carr, 1980; Ditchfield &
Hemsley, 1990; Straube & Oades, 1992, pp. 339-341).
Results and Discussion
Data from each primary study were entered into theStatistical Package for the Social Sciences (SPSS, 1990) andthe Software for the Meta-Analytic Review of ResearchLiterature (DSTAT; Johnson, 1989) statistical software pack-ages to produce the descriptive and inferential meta-analyticresults. Descriptive data for the published studies arepresented first, followed by mean effect size summaries andrelated statistical analyses.
Descriptive Data
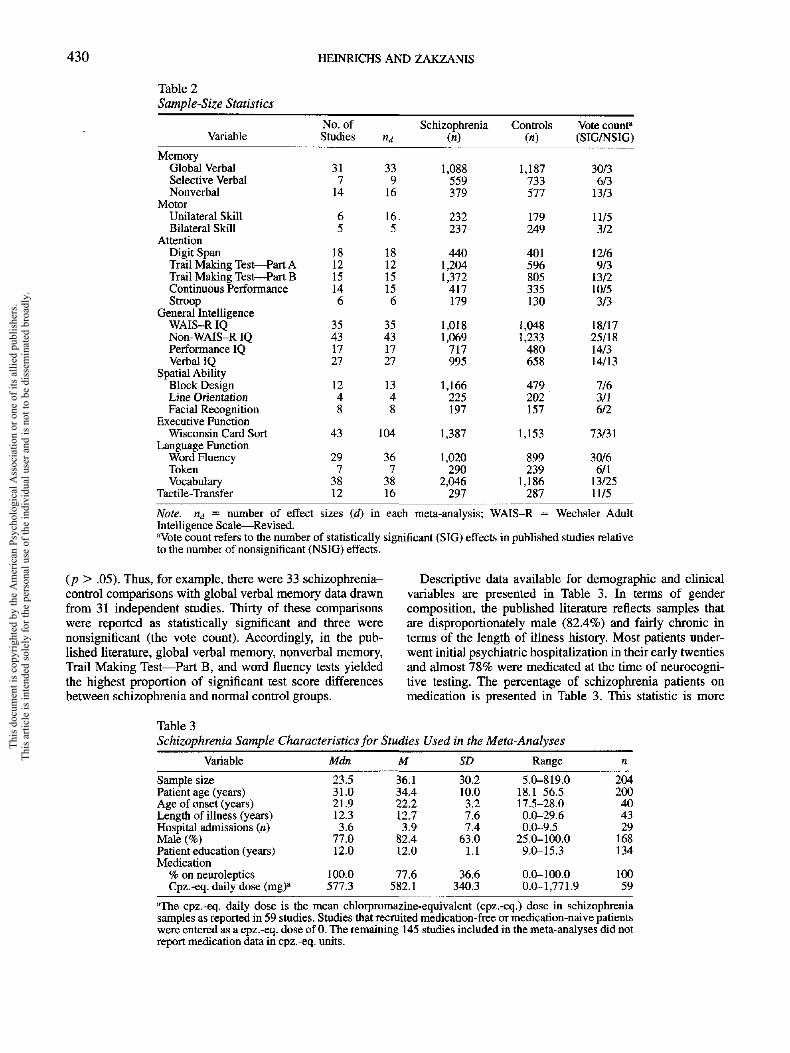
Two hundred and four studies published between 1980and mid-1997, yielding 509 effect sizes, met criteria forinclusion in the present analysis. Descriptive statistics forthe study set are shown in Table 2. The table shows howmany studies were used in each of the 22 meta-analyses, aswell as the number of individual effect sizes that wereincorporated into each mean effect size. The number ofschizophrenia patients and normal controls for each meta-analysis is also included. In total, neurocognitive test resultsfrom 7,420 schizophrenia patients and 5,865 normal healthycontrols were recorded across meta-analyses.
Table 2 also includes a "vote count" statistic in which theschizophrenia-control comparison from each primary studywas tallied as significant (p < .05) or nonsignificant
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
430 HEINRICHS AND ZAKZANIS
Table 2
Sample-Size Statistics
Variable
MemoryGlobal VerbalSelective VerbalNonverbal
MotorUnilateral SkillBilateral Skill
AttentionDigit SpanTrail Making Test — Part ATrail Making Test — Part BContinuous PerformanceStroop
General IntelligenceWAIS-R IQNon-WAlS-R IQPerformance IQVerbal IQ
Spatial AbilityBlock DesignLine OrientationFacial Recognition
Executive FunctionWisconsin Card Sort
Language FunctionWord FluencyTokenVocabulary
Tactile-Transfer
No. ofStudies
317
14
65
181215146
35431727
1248
43
297
3812
"d
339
16
165
181215156
35431727
1348
104
367
3816
Schizophrenia(n)
1,088559379
232237
4401,2041,372
417179
1,0181,069
717995
1,166225197
1,387
1,020290
2,046297
Controls
(«)
1,187733577
179249
401596805335130
1,0481,233
480658
479202157
1,153
899239
1,186287
Vote count8
(SIG/NSIG)
30/36/3
13/3
11/53/2
12/69/3
13/210/53/3
18/1725/1814/314/13
7/63/16/2
73/31
30/66/1
13/2511/5
Note. nd = number of effect sizes (d) in each meta-analysis; WAIS-R = Wechsler AdultIntelligence Scale—Revised."Vote count refers to the number of statistically significant (SIG) effects in published studies relativeto the number of nonsignificant (NS1G) effects.
(p > .05). Thus, for example, there were 33 schizophrenia-
control comparisons with global verbal memory data drawn
from 31 independent studies. Thirty of these comparisons
were reported as statistically significant and three were
nonsignificant (the vote count). Accordingly, in the pub-
lished literature, global verbal memory, nonverbal memory,
Trail Making Test—Part B, and word fluency tests yielded
the highest proportion of significant test score differences
between schizophrenia and normal control groups.
Descriptive data available for demographic and clinical
variables are presented in Table 3. In terms of gender
composition, the published literature reflects samples that
are disproportionately male (82.4%) and fairly chronic in
terms of the length of illness history. Most patients under-
went initial psychiatric hospitalization in their early twenties
and almost 78% were medicated at the time of neurocogni-
tive testing. The percentage of schizophrenia patients on
medication is presented in Table 3. This statistic is more
Table 3
Schizophrenia Sample Characteristics for Studies Used in the Meta-Analyses
Variable
Sample sizePatient age (years)Age of onset (years)Length of illness (years)Hospital admissions (n)Male (%)Patient education (years)Medication
% on neurolepticsCpz.-eq. daily dose (mg)a
Mdn
23.531.021.912.33.6
77.012.0
100.0577.3
M
36.134.422.212.73.9
82.412.0
77.6582.1
SD
30.210.03.27.67.4
63.01.1
36.6340.3
Range
5.0-819.018.1-56.517.5-28.00.0-29.60.0-9.5
25.0-100.09.0-15.3
0.0-100.00.0-1,771.9
n
204200404329
168134
10059
"The cpz.-eq. daily dose is the mean chlorpromazine-equivalent (cpz.-eq.) dose in schizophreniasamples as reported in 59 studies. Studies that recruited medication-free or medication-naive patientswere entered as a cpz.-eq. dose of 0. The remaining 145 studies included in the meta-analyses did notreport medication data in cpz.-eq. units.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
NEUROCOGNITIVE DEFICIT IN SCHIZOPHRENIA 431
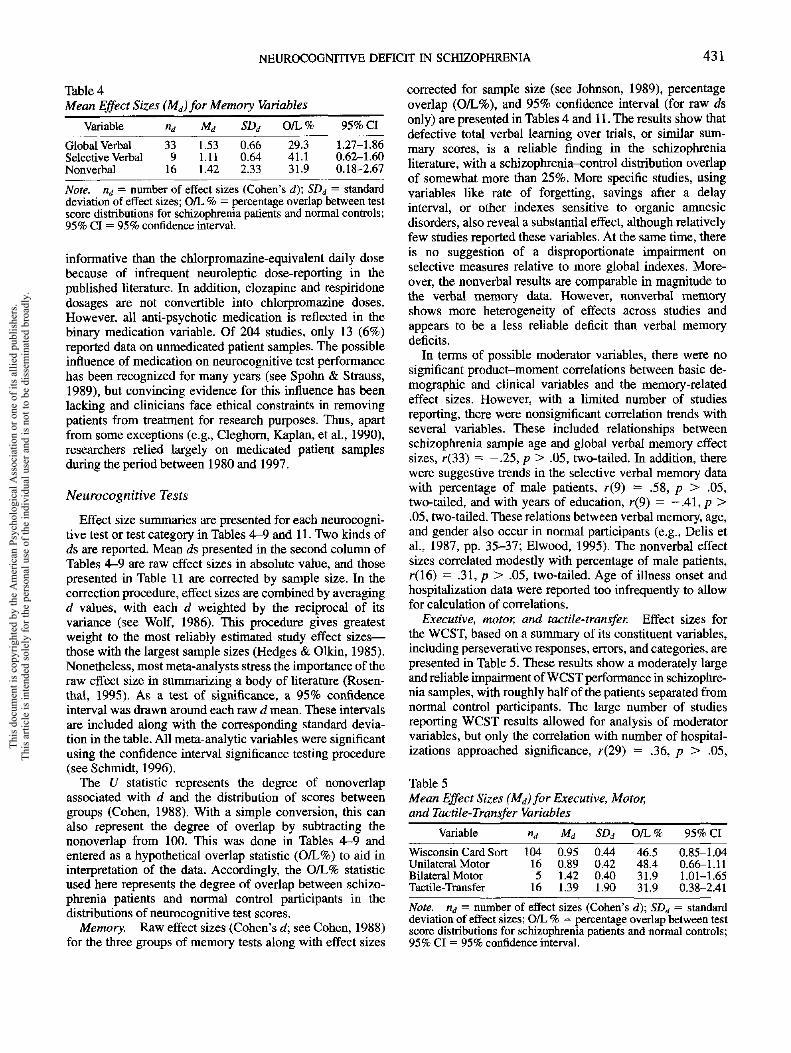
Table 4Mean Effect Sizes (Md) for Memory Variables
Variable
Global VerbalSelective VerbalNonverbal
nd
339
16
Md
1.531.111.42
SDd
0.660.642.33
0/L%
29.341.131.9
95% CI
1.27-1.860.62-1.600.18-2.67
Note, rid — number of effect sizes (Cohen's d}\ SDj = standarddeviation of effect sizes; O/L % = percentage overlap between testscore distributions for schizophrenia patients and normal controls;95% CI = 95% confidence interval.
informative than the chlorpiomazine-equivalent daily dosebecause of infrequent neuroleptic dose-reporting in thepublished literature. In addition, clozapine and respiridonedosages are not convertible into chlorpromazine doses.However, all anti-psychotic medication is reflected in thebinary medication variable. Of 204 studies, only 13 (6%)reported data on unmedicated patient samples. The possibleinfluence of medication on neurocognitive test performancehas been recognized for many years (see Spohn & Strauss,1989), but convincing evidence for this influence has beenlacking and clinicians face ethical constraints in removingpatients from treatment for research purposes. Thus, apartfrom some exceptions (e.g., Cleghorn, Kaplan, et al., 1990),researchers relied largely on medicated patient samplesduring the period between 1980 and 1997.
Neurocognitive Tests
Effect size summaries are presented for each neurocogni-tive test or test category in Tables 4—9 and 11. Two kinds ofds are reported. Mean ds presented in the second column ofTables 4-9 are raw effect sizes in absolute value, and thosepresented in Table 11 are corrected by sample size. In thecorrection procedure, effect sizes are combined by averagingd values, with each d weighted by the reciprocal of itsvariance (see Wolf, 1986). This procedure gives greatestweight to the most reliably estimated study effect sizes—those with the largest sample sizes (Hedges & Olkin, 1985).Nonetheless, most meta-analysts stress the importance of theraw effect size in summarizing a body of literature (Rosen-thai, 1995). As a test of significance, a 95% confidenceinterval was drawn around each raw d mean. These intervalsare included along with the corresponding standard devia-tion in the table. All meta-analytic variables were significantusing the confidence interval significance testing procedure(see Schmidt, 1996).
The U statistic represents the degree of nonoverlapassociated with d and the distribution of scores betweengroups (Cohen, 1988). With a simple conversion, this canalso represent the degree of overlap by subtracting thenonoverlap from 100. This was done in Tables 4—9 andentered as a hypothetical overlap statistic (O/L%) to aid ininterpretation of the data. Accordingly, the O/L% statisticused here represents the degree of overlap between schizo-phrenia patients and normal control participants in thedistributions of neurocognitive test scores.
Memory. Raw effect sizes (Cohen's d; see Cohen, 1988)for the three groups of memory tests along with effect sizes
corrected for sample size (see Johnson, 1989), percentageoverlap (O/L%), and 95% confidence interval (for raw dsonly) are presented in Tables 4 and 11. The results show thatdefective total verbal learning over trials, or similar sum-mary scores, is a reliable finding in the schizophrenialiterature, with a schizophrenia-control distribution overlapof somewhat more than 25%. More specific studies, usingvariables like rate of forgetting, savings after a delayinterval, or other indexes sensitive to organic amnesicdisorders, also reveal a substantial effect, although relativelyfew studies reported these variables. At the same time, thereis no suggestion of a disproportionate impairment onselective measures relative to more global indexes. More-over, the nonverbal results are comparable in magnitude tothe verbal memory data. However, nonverbal memoryshows more heterogeneity of effects across studies andappears to be a less reliable deficit than verbal memorydeficits.
In terms of possible moderator variables, there were nosignificant product-moment correlations between basic de-mographic and clinical variables and the memory-relatedeffect sizes. However, with a limited number of studiesreporting, there were nonsignificant correlation trends withseveral variables. These included relationships betweenschizophrenia sample age and global verbal memory effectsizes, r(33) = -.25, p > .05, two-tailed. In addition, therewere suggestive trends in the selective verbal memory datawith percentage of male patients, r(9) = .58, p > .05,two-tailed, and with years of education, r(9) = —.41, p >.05, two-tailed. These relations between verbal memory, age,and gender also occur in normal participants (e.g., Delis etal., 1987, pp. 35-37; Elwood, 1995). The nonverbal effectsizes correlated modestly with percentage of male patients,r(16) = .31, p > .05, two-tailed. Age of illness onset andhospitalization data were reported too infrequently to allowfor calculation of correlations.
Executive, motor, and tactile-transfer. Effect sizes forthe WCST, based on a summary of its constituent variables,including perseverative responses, errors, and categories, arepresented in Table 5. These results show a moderately largeand reliable impairment of WCST performance in schizophre-nia samples, with roughly half of the patients separated fromnormal control participants. The large number of studiesreporting WCST results allowed for analysis of moderatorvariables, but only the correlation with number of hospital-izations approached significance, r(29) = -36, p > .05,
Table 5Mean Effect Sizes (Mj) for Executive, Motor,and Tactile-Transfer Variables
Variable
Wisconsin Card SortUnilateral MotorBilateral MotorTactile-Transfer
"d
104165
16
Md
0.950.891.421.39
SDd
0.440.420.401.90
O/L%
46.548.431.931.9
95% CI
0.85-1.040.66-1.111.01-1.650.38-2.41
Note. nd = number of effect sizes (Cohen's d); SDa = standarddeviation of effect sizes; O/L % = percentage overlap between testscore distributions for schizophrenia patients and normal controls;95% CI = 95% confidence interval.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

432 HEINRICHS AND ZAKZANIS
two-tailed. In addition, a large number of studies (n = 33)reported WCST results along with WAIS-R IQ results,thereby permitting an examination of possible relationshipsbetween general intellectual levels in schizophrenia samplesand the WCST effect size in the same sample. There was asignificant relationship between WCST effect size and IQscore, r(33) = -.54, p < .01, and between WCST effects
and IQ effects, r(33) = .56, p < .005. These relationshipsimply that patient samples are likely to differ from controlsamples on the WCST if they also differ in terms of IQ.Thus, impaired WCST scores in schizophrenia may be, inpart, a reflection of low general intellectual abilities.
Unilateral motor tests produced effect sizes that weresimilar in magnitude to the WCST results, especially whenthe effects were corrected for sample size (see also Table11). There was a nonsignificant association with the propor-
tion of male patients in the study sample, r(l4) = ~-36,p >.05, two-tailed. The number of studies reporting bilateralmotor results was very small, making general conclusions
difficult.Results of tests where patients identify and discriminate
tactile stimuli under conditions that require transfer ofinformation across the corpus callosum showed a large meaneffect size, even after correction for sample size. At the sametime, the results were very heterogeneous, indicating theexistence of patient samples with extensive overlap, as wellas samples with very little overlap, with control distribu-tions. There were no significant moderator correlations inthe tactile-transfer results, but there were suggestive trendswith patient sample age, r(15) = .47, p > .05, two-tailed;education, r(10) = —.68, p > .05, two-tailed; and percent-age of male patients, r(15) = .33, p > .05, two-tailed.
Attention. Results for attention variables are presentedin Table 6. The most frequently reported, attention-relatedtest variable was digit span. Eighteen studies reported data,with 3 of these reporting results with the distraction version(Oltmanns, 1978) and the rest with the WAIS-R versionwithout distraction. The average effect size for the subset ofdistraction digit spans was .81, but the number of studieswas too small to allow for a statistical comparison. Theoverall effect size of .62 represents a hypothetical overlapwith control distributions of about 60%, suggesting a fairlymodest degree of discrimination. Larger effects were ob-tained in studies using versions of the Continuous Perfor-mance Test and the Stroop Test, but the number of articlesreporting Stroop results is small. Overall, die Continuous
Table 6Mean Effect Sizes (Md) for Attention Variables
Variable ~^d ~Md ~SDd O / L % 9 5 % CI
Digit Span 18 0.62 0.51 61.8 0.35-0.96Continuous Performance 15 1.18 0.49 37.8 0.94-1.50Stroop 6 1.22 0.63 41.1 0.23-2.11Trail Making—Part A 12 0.95 0.32 48.4 0.73-1.16Trail Making—Part B 15 1.07 0.52 41.1 0.80-1.33
Note. 114 = number of effect sizes (Cohen's af); SDd = standarddeviation of effect sizes; O/L % = percentage overlap between testscore distributions for schizophrenia patients and normal controls;95% CI = 95% confidence interval.
Table 7
Mean Effect Sizes (Md)for General intelligence Variables
Variable
WAIS-R IQNon-WAIS-R IQVerbal IQPerformance IQ
nd
35432717
Md
1.240.630.981.46
SDd
0.890.600.680.89
O/L%
37.861.844.629.3
95% CI
0.88-1.560.35-0.920.70-1.201.07-1.90
Note. nd — number of effect sizes (Cohen's d); SDd = standarddeviation of effect sizes; O/L % = percentage overlap between testscore distributions for schizophrenia patients and normal controls;95% CI = 95% confidence interval; WAIS-R = Wechsler AdultIntelligence Scale—Revised.
Performance and Trail Making tests seem to be about
equally sensitive to schizophrenia, yielding large effect sizesthat separate more than half of the patient and controldistributions. Nevertheless, Trail Making Test results arebased on smaller sample sizes, which causes shrinkage in thecorrected effect size compared with the Continuous Perfor-mance data (see Table 11 presented later).
The two effect sizes for the Trail Making Test are alsoinformative because they represent a situation where asimple and a more complex and demanding version of aneurocognitive task can be studied. If task difficulty and taskcomplexity, rather than specific neurocognitive functionslike visual scanning and sequencing, contribute to schizophre-nia-control differences, more demanding versions of thesame basic test should yield significantly larger effect sizesthan less demanding versions. Thus Part B of the TrailMaking Test should produce a larger effect size than Part Awhen applied to the same sample of patients and controls.
Part A requires rapid sequential connection of numbers in apaper-and-pencil format, whereas Part B requires alternationbetween alphabetic and numeric sequences. Possum, Holm-berg, and Reinvang (1992) have shown that the spatialarrangement and dual symbol systems of Part B underlie theslower Part B completion times.
Accordingly, we carried out a paired-difference t testcomparing effect sizes from the two forms. There was nosignificant difference between the two parts of the TrailMaking Test, f(25) = -1.3, p > .05, two-tailed. Hence, itappears likely that task difficulty and complexity are lessimportant than the more specific attention and scanning-related neurocognitive processes elicited by this particulartest. Alternatively, because both alphabetic and numericsequences are probably overlearned information, the differ-ences in processing demands between Parts A and B of theTrail Making Test may be minimal.
General intellectual ability. Effect sizes for intelligencetest results are presented in Table 7. Full scale IQ estimateswere obtained from a variety of intelligence tests in additionto the WAIS-R (see Table 1). To assess whether WAIS-Rand non-WAIS-R-derived IQs differed in terms of theirability to separate schizophrenia and control distributions,we calculated a t test on the respective mean d values. Thiscalculation indicated substantially larger average effect sizesin patient-control comparisons that used the WAIS-R,f (76) = 2.81, p < .01, two-tailed. Whether this indicates thatthe WAIS-R is more difficult for patients to complete than
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

NEUROCOGNITIVE DEFICIT IN SCHIZOPHRENIA 433
Table 8Mean Effect Sizes (Md) for Spatial Ability Variables
Variable
Line OrientationBlock DesignFacial Recognition
"j
4138
Md
1.100.730.88
SDd
0.620.610.44
O/L%
41.157.048.4
95% CI
0.12-2.00.29-1.190.44-1.19
Note, nd — number of effect sizes (Cohen's d); SDd = standarddeviation of effect sizes; O/L % = percentage overlap between testscore distributions for schizophrenia patients and normal controls;95% CI = 95% confidence interval.
measures like the Shipley, Quick, and NART is unclear. Thenon-WAIS-R measures tend to be briefer and less compre-hensive in scope than the WAIS-R. At the same time, some
of these alternative measures, like the NART, are regarded asmeasures of premorbid rather than morbid intelligence. Weextracted the NART data from the study set and found amean d of .42 (SD = .68) for 19 studies. Hence, smaller
differences between patients and controls on such tests mayreflect a robustness of performance in the presence ofschizophrenic illness. However, there is a considerable
degree of dispersion around the NART mean, and individualstudy effects ranged from -1.85 to +0.91, which raisesquestions of reliability in the use of this measure to indexpremorbid ability levels. In any case, the data suggest thatputative tests of general intellectual function are not inter-changeable and can be expected to vary in sensitivity toschizophrenic illness.
Intelligence measured with the WAIS-R yields largeeffect sizes in schizophrenia-control comparisons, withdistribution overlaps that are well below 50%. In addition,intellectual differences are reliable, with none of the confi-dence intervals including zero. Finally, no significant relation-ships were found between IQ effect sizes and potentialmoderators including age, education, neuroleptic dose, sam-ple gender composition, or age of illness onset.
Spatial ability. Results pertaining to the relatively smallnumber of patient-control comparisons that used tests ofvisuospatial skill are presented in Table 8. These tests are notused frequently in the schizophrenia literature, but theavailable data suggest there are moderately large effect sizes,with less man 50% overlap between schizophrenia andcontrol distributions. However, the d values shrink consider-ably when corrected for sample size (see Table 11 presentedlater), indicating that most studies using spatial ability testsare based on small samples of patients and controls. Withthis correction the effect sizes correspond to more moderatehypothetical overlap values, suggesting that perhaps twothirds of the patients and controls are indistinguishable interms of spatial skill.
Language. The effect size summary for language-related tests is presented in Table 9. This shows large effectsfor tests of word generation such as the Controlled OralWord Association Test and the Token Test (the latter isprimarily an auditory comprehension measure; see Table 1).In both cases, these-effect sizes represent only aboutone-third overlap between schizophrenia and control distri-butions. However, this evidence is qualified by a relativelysmall number of contributing studies in the case of the Token
Test. In addition, the relatively large standard deviations
imply considerable dispersion and hence heterogeneity ofeffect sizes in both the fluency and Token Test data.
In contrast, a more moderate average effect size wasobtained for vocabulary tests. This is another aggregate of
measures, with some derived from the WAIS-R Vocabularysubtest and others based on scales such as the Mill Hill andShipley scales (see Table 1). Nonetheless, there was no
significant difference between the average effect size gener-ated by WAIS-R and non-WAIS-R-based vocabulary tests,
r(36) = 1.71,p> .05.Overall, expressive and receptive language tests appear to
be fairly powerful and moderately reliable discriminators ofschizophrenia and control populations. None of the effectsizes correlated significantly with potential demographic orclinical moderators. However, with 13 studies reporting bothfluency and chlorpromazine dose data, there was a strongtrend for highly medicated samples to yield smaller word
fluency differences relative to control samples, r(13) =-.75,p>.05.
Inferential data. It is unlikely that a literature reviewwill uncover every study of a hypothesis that has beenconducted. Rosenthal (1979) has called this the "file drawerproblem" because of the tendency for studies of nonsignifi-cant results to remain unpublished, perhaps languishing inforgotten file drawers (see also Wolf, 1986, p. 37). Kraemerand Andrews (1982) note that "published research studiestend to be biased toward positive findings. A study is oftenabandoned if it is apparent that statistically significantfindings will not be forthcoming. Reports of nonsignificantfindings are generally unpublishable even when they arereplications of earlier studies reporting significant results"(p. 405). To deal with the file drawer problem in the presentset of meta-analyses, Orwin's (1983) fail-safe N procedurewas carried out. Table 10 shows the estimated number ofunpublished or unretrieved studies, each with a trivial effectsize of d — 0.1 (92% distribution overlap), needed to reducethe effect sizes reported in Tables 4-9 to 0.1 or smaller.Although the actual existence of such countervailing evi-dence cannot be entirely ruled out, it seems unlikely thatsuch large numbers of studies are actually present inneglected file drawers.
Summary and Conclusions
In our quantitative review, we found neurocognitivedeficit to be a reliable finding in schizophrenia. In addition, itis clear that the deficit exists in relation to most neurocogni-
Table 9Mean Effect Sizes (Mj)for Language Function Variables
Variable
Word FluencyVocabularyToken Test
"d
36387
Md
1.390.691.35
SDd
1.200.480.94
O/L%
31.957.034.7
95% CI
0.91-1.800.50-0.860.98-1.70
Note, rij = number of effect sizes (Cohen's d); SDd = standarddeviation of effect sizes; O/L % = percentage overlap between testscore distributions for schizophrenia patients and normal controls;95% CI = 95% confidence interval.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
434 HEINRICHS AND ZAKZANIS
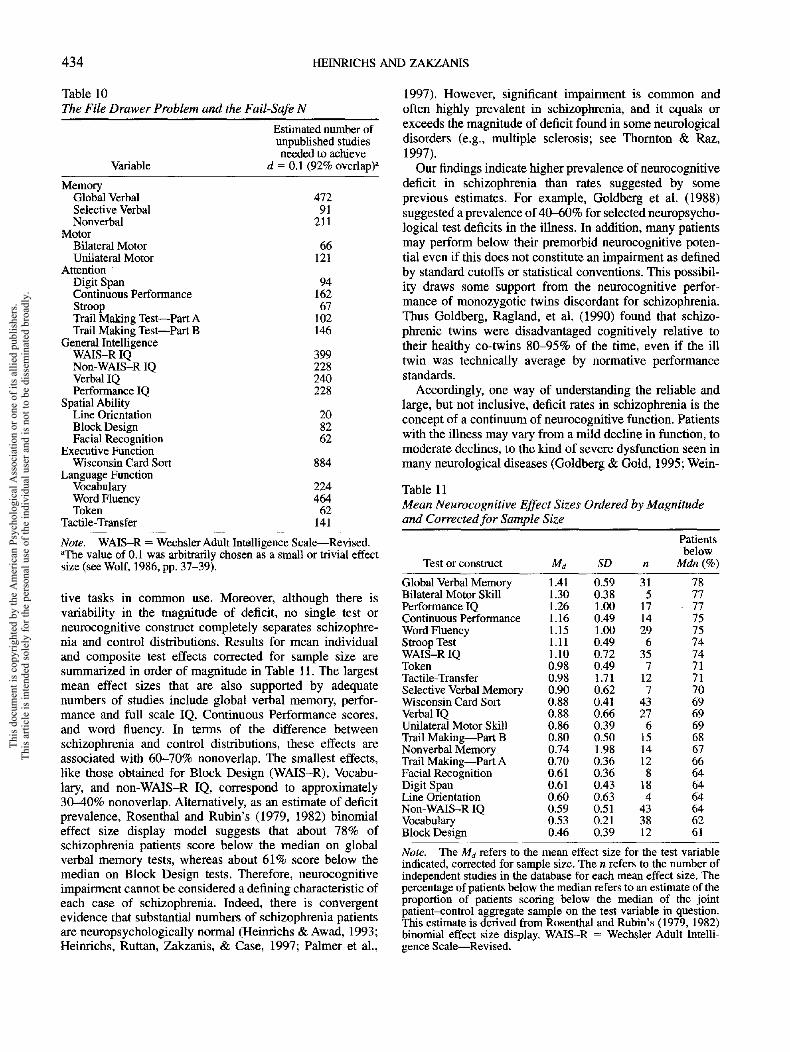
Table 10The File Drawer Problem and the Fail
Variable
MemoryGlobal VerbalSelective VerbalNonverbal
MotorBilateral MotorUnilateral Motor
AttentionDigit SpanContinuous PerformanceStroopTrail Making Test— Part ATrail Making Test— Part B
General IntelligenceWAIS-R IQNon-WAIS-R IQVerbal IQPerformance IQ
Spatial AbilityLine OrientationBlock DesignFacial Recognition
Executive FunctionWisconsin Card Sort
Language FunctionVocabularyWord FluencyToken
Tactile-Transfer
-SafeN
Estimated number ofunpublished studiesneeded to achieve
d = Q.\ (92% overlap)8
47291
211
66121
9416267
102146
399228240228
208262
884
22446462
141
Note. WAIS-R = Wechsler Adult Intelligence Scale—Revised."The value of 0.1 was arbitrarily chosen as a small or trivial effectsize (see Wolf, 1986, pp. 37-39).
live tasks in common use. Moreover, although there isvariability in the magnitude of deficit, no single test orneurocognitive construct completely separates schizophre-nia and control distributions. Results for mean individualand composite test effects corrected for sample size aresummarized in order of magnitude in Table 11. The largestmean effect sizes that are also supported by adequatenumbers of studies include global verbal memory, perfor-mance and full scale IQ, Continuous Performance scores,and word fluency. In terms of the difference betweenschizophrenia and control distributions, these effects areassociated with 60-70% nonoverlap. The smallest effects,like those obtained for Block Design (WAIS-R), Vocabu-lary, and non-WAJS-R IQ, correspond to approximately30-40% nonoverlap. Alternatively, as an estimate of deficitprevalence, Rosenthal and Rubin's (1979, 1982) binomialeffect size display model suggests that about 78% ofschizophrenia patients score below the median on globalverbal memory tests, whereas about 61% score below themedian on Block Design tests. Therefore, neurocognitiveimpairment cannot be considered a denning characteristic ofeach case of schizophrenia. Indeed, there is convergentevidence that substantial numbers of schizophrenia patientsare neuropsychologically normal (Heinrichs & Awad, 1993;Heinrichs, Ruttan, Zakzanis, & Case, 1997; Palmer et al.,
1997). However, significant impairment is common andoften highly prevalent in schizophrenia, and it equals orexceeds the magnitude of deficit found in some neurologicaldisorders (e.g., multiple sclerosis; see Thornton & Raz,1997).
Our findings indicate higher prevalence of neurocognitivedeficit in schizophrenia than rates suggested by someprevious estimates. For example, Goldberg et al. (1988)suggested a prevalence of 40-60% for selected neuropsycho-logical test deficits in the illness. In addition, many patientsmay perform below their premorbid neurocognitive poten-tial even if this does not constitute an impairment as definedby standard cutoffs or statistical conventions. This possibil-ity draws some support from the neurocognitive perfor-mance of monozygotic twins discordant for schizophrenia.Thus Goldberg, Ragland, et al. (1990) found that schizo-phrenic twins were disadvantaged cognitively relative totheir healthy co-twins 80-95% of the time, even if the illtwin was technically average by normative performancestandards.
Accordingly, one way of understanding the reliable andlarge, but not inclusive, deficit rates in schizophrenia is theconcept of a continuum of neurocognitive function. Patientswith the illness may vary from a mild decline in function, tomoderate declines, to the kind of severe dysfunction seen inmany neurological diseases (Goldberg & Gold, 1995; Wein-
Table 11Mean Neurocognitive Effect Sizes Ordered by Magnitudeand Corrected for Sample Size
Test or construct
Global Verbal MemoryBilateral Motor SkillPerformance IQContinuous PerformanceWord FluencyStroop TestWAIS-R IQTokenTactile-TransferSelective Verbal MemoryWisconsin Card SortVerbal IQUnilateral Motor SkillTrail Making — Part BNonverbal MemoryTrail Making — Part AFacial RecognitionDigit SpanLine OrientationNon-WAIS-R IQVocabularyBlock Design
Ma
1.411.301.261.161.151.111.100.980.980.900.880.880.860.800.740.700.610.610.600.590.530.46
SD
0.590.381.000.491.000.490.720.491.710.620.410.660.390.501.980.360.360.430.630.510.210.39
n
315
171429
6357
127
43276
1514128
184
433812
Patientsbelow
Mdn(%)
7877
- 7775757474717170696969686766646464646261
Note. The Md refers to the mean effect size for the test variableindicated, corrected for sample size. The n refers to the number ofindependent studies in the database for each mean effect size. Thepercentage of patients below the median refers to an estimate of theproportion of patients scoring below the median of the jointpatient-control aggregate sample on the test variable in question.This estimate is derived from Rosenthal and Rubin's (1979, 1982)binomial effect size display. WAIS-R = Wechsler Adult Intelli-gence Scale—Revised.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

NEUROCOGNTTIVE DEFICIT IN SCHIZOPHRENIA 435
berger, 1995). At the mild end, a patient's neurocognitivedysfunction is relative to his or her own potential and may
overlap with levels of function obtained by many healthy
individuals. At the severe extreme, a patient may havecognitive and neurological abnormalities that are completely
distinguished from normal control values.The limitations of this kind of explanation include its
testability. There are practical difficulties involved in accu-
rately assessing premorbid neurocognitive potential in largenumbers of schizophrenia patients. Moreover, the con-tinuum argument must assume that patients who show
average neurocognitive function—roughly half of thosewith the illness—have nevertheless undergone a relativedecline. Therefore, the same proportion of patients must
have been slightly above average by normative performancestandards before illness onset. This seems a rather difficultprediction to test. Finally, although discordant monozygotictwins provide an important perspective on schizophrenia,
they cannot be regarded as representative of either thehealthy or patient populations as a whole.
Another explanation for the 61—78% neurocognitive defi-
cit rate in our quantitative review is that such deficit issecondary, peripheral rather than central to the illness. Mostdiseases have peripheral features that are tied only modestly
and indirectly to the primary pathology. For example,overall brain volume reductions are less prevalent in Alzhei-mer's disease than volume reductions in a specific structure,the hippocampus (Seab et al., 1988). Presumably, thisreflects the primary locus of pathology in the hippocampusand other specific structures and the less direct relation ofthis focal pathology to general changes in brain volume. Thefunctions measured by standard neurocognitive tests inschizophrenia patients may also be relatively peripheral tothe still unknown primary dysfunction.
At the same time, it may not be reasonable to expectextremely high rates of control—patient discrimination giventhe vagaries inherent in psychological measurement. For acomparison, consider the normative data on the WCSTprovided by Heaton et al. (1993). The effect size forcategories achieved on the WCST is -1.04 SD units whenneurological patients with focal frontal lesions are comparedwith healthy controls. When "categories" is extracted as aseparate score from our own meta-analytic data on schizo-phrenia, the mean effect size is - ] .05. Given the traditionaldifficulty of discriminating schizophrenia from more conven-tional neurobehavioral disorders, it may well be that at leastsome neurocognitive tests are as sensitive to schizophreniaas they are to neurological conditions in general (Heaton etal., 1994). Moreover, the sensitivity of neurocognitive teststo schizophrenia compares favorably with structural andfunctional neuroimaging methods, which tend to yield effectsizes less than 1.0 (Raz and Raz, 1990; Zakzanis &Heinrichs, 1997).
Of equal theoretical interest for understanding schizophre-nia is the vexed question of heterogeneity and whethersubstantial but not absolute (e.g., d > 4.0, nonover-lap = 97%) effect sizes reflect the existence of cognitivelyintact and impaired subpopulations of patients. In addition,several tests and constructs are characterized by large
dispersion of individual effects around their means (e.g.,
Performance IQ, word fluency, tactile-transfer tests, nonver-
bal memory tests; see Table 11). Such dispersion alsoimplies the existence of impaired and normal subgroups ofpatients. This is inimical to the continuum view of neurocog-nitive deficit, which argues for a single disease process with
variable expression. In contrast, a strong form of theheterogeneity argument is the contention that multipledisease processes underpin schizophrenia (see Carpenter,
Buchanan, Kirkpatrick, & Tamminga, 1993; Heinrichs,1993; Liddle & Barnes, 1990). Advocates of the singledisease-continuum model can point to brain features like
ventricle size to show that schizophrenia patients are nor-mally distributed on such measures, with little evidence ofthe kind of bimodality that might indicate subpopulations
(David, Goldberg, Gibbon, & Weinberger, 1991). On theother hand, there is clear evidence of bimodal distributionsin schizophrenia on some psychophysiological measures,
like smooth-pursuit eye movements (Clementz, Grove,lacono, & Sweeney, 1992; lacono, Moreau, Beiser, Heming,& Liu, 1992). Our meta-analytic evidence cannot resolve
this debate, but it forcefully underscores the need to developtestable illness models that take heterogeneity into accountand extend the search for evidence of multiple disease
processes.Despite the fact that all tests and neurocognitive catego-
ries yielded at least moderate and often large effects, sometests appear to produce greater differences between patientsand controls than other tests. The order of effect magnitudesin Table 11 bears a very rough similarity to Saykin et al.'s(1991) study of a schizophrenia sample that showed thegreatest difference from controls on a group of memoryfunctions, followed by differences in motor-attentional andlanguage functions. In addition, a recent meta-analysis byWoodruff, McManus, and David (1995) supports the ideathat corpus callosum abnormalities exist in schizophrenia.This is consistent with defective recognition of tactileinformation on interhemispheric transfer tasks. Neverthe-less, our meta-analysis, based on 204 studies, 7,420 schizo-phrenia patients, and 5,865 normal controls, confirms previ-ous suggestions that any selectivity of deficit in schizophreniaoccurs in the context of a background of a very generalimpairment. Even the less-sensitive tasks yielded effect sizesbetween 0.5 and 1.0 on average, suggesting that anydifferential sensitivity of specific tests is relatively mild andcoexists with a more broadly based impairment in cognitivebrain function. Moreover, it is not known to what extentdifferences in task complexity, difficulty, floor or ceilingeffects, and other psychometric properties may have contrib-uted to the appearance of more or less powerful effect sizesacross selected neurocognitive measures (see Chapman &Chapman, 1973, 1978). Data from the Trail Making Testsuggest that more complex tests do not necessarily increasethe disadvantage patients show relative to controls oncognitive tasks. However, a comparison of WAIS—R- andnon-WAIS-R-derived IQ estimates showed that differentmeasures of the same cognitive function may yield markedlydifferent degrees of separation between schizophrenia andcontrol samples.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
436 HEINRICHS AND ZAKZANIS
Hence, a cautious interpretation of our meta-analytic datawould be that all areas of neurocognitive function arecompromised in a large proportion of schizophrenia pa-
tients. Long-standing arguments concerning "core" or selec-tive deficits against a background of general impairment areunlikely to be resolved until researchers routinely calibrate
the difficulty and complexity levels of their tests beforeapplying them to clinical populations.
Moderator variable analysis is an essential part of meta-
analytic investigation because it assesses the contribution ofstudy differences in sample attributes, design, and instru-ment features to effect size heterogeneity and replication.However, moderator analysis is dependent on the individual
reporting practices of investigators and presumably theexpectations of journal editors and reviewers. In terms ofmoderator variables, the published literature on neurocogni-
tion in schizophrenia is surprisingly limited and ofteninadequate. We found that even basic participant attributes,such as age, education, and gender composition, were notreported by all studies. Clinical variables of special rel-evance to schizophrenia, like neuroleptic medication dose,age of illness onset, duration of illness, and frequency ofhospitalization were so underreported that we were able toconduct only a limited correlational study of potentialmoderators, with many correlations missing statistical signifi-cance because of inadequate power.
In the moderator variable analysis there were nonsignifi-cant trends that imply possible links between neurocognitive
deficits and some demographic and clinical aspects of thepatient samples. Thus, higher neuroleptic doses associatewith smaller differences between patients and controls onexpressive language tests (see Spohn & Strauss, 1989). Witha very limited number of studies available for analysis, thereis little to suggest an association between chronicity ofillness and neurocognitive deficit. A moderate, non-significant trend is suggested between frequent hospitaliza-tion and executive deficits measured by the WCST. Moreconsistent reporting of these sample attributes by researchersin individual studies will increase statistical power formeta-analytic purposes and facilitate future efforts at under-standing how neurocognitive and clinical variables are
related in the published literature.Although many studies did not report IQ along with other
neurocognitive variables of interest, there is evidence that atleast one commonly used neurocognitive measure in schizo-phrenia research is tied to general intellectual ability.Differences between patients and controls in terms of WCSTperformance were correlated with differences in IQ scoresand in IQ effect sizes, which is consistent with earlier studiessuggesting a relationship between intelligence and WCSTperformance in neuropsychiatric patients (e.g., Heinrichs,
1990).The finding that patient samples that differ in general
intelligence from their control samples are also likely todiffer in WCST performance reinforces the question ofwhether general ability factors underpin apparently selectiveneurocognitive deficits in schizophrenia. In other words, theillness may bring with it a generalized cognitive deficit thatmanifests itself in putatively different tests that nonetheless
depend heavily on general ability for successful perfor-mance. Although defective WCST scores may coexist withaverage IQs in many neurological disorders, this does not
appear to be the case in schizophrenia (see Heaton et al.,1993).
It is also possible that functions other than intelligence
contribute to patient performance on a broad variety of tasks.Neurocognitive tests probably measure several componentprocesses at the same time. These processes may be
weighted differentially in terms of particular task demands.Hence, the final score or performance value may reflect thiscomplexity rather than just the preservation or impairmentof a supposedly "pure" function. For example, verbal
memory tasks, such as the California Verbal Learning Test(Delis et al., 1987), require not only intact verbal memoryfor success but also basic language comprehension, auditory
attention, and expressive language. Similarly, many tasks inaddition to those subsumed under the label of "attention"require attention-related skills. It is not known to what extent
shared functions contribute to neurocognitive test perfor-mance and give rise to spurious impressions of selectiveimpairment. However, concurrent reporting of general andmore specific neurocognitive test scores, along with data ontask difficulty, will make it easier to assess the credibility ofputatively selective deficits (Chapman & Chapman, 1978,1989).
Neuropsychological research has traditionally used match-ing strategies to demonstrate selectivity of deficit. In thisway, a lesion group and a control group are matched in termsof general intellectual ability, education, and other attributesthat may confound the demonstration of specific deficit. Inthe case of schizophrenia, however, the nature of the illnessand its onset in late adolescence or early adulthood prema-turely curtail academic achievement. Hence, the use ofeducational attainment or IQ for matching purposes can leadto spuriously low estimates of general ability in schizophre-nia populations. With this problem in mind, some investiga-tors have argued for the use of measures for matchingpurposes, such as oral reading or spelling tests, that are lesssensitive to the illness (Kremen et al., 1996). This is anexcellent suggestion for future research on neurocognitiveaspects of schizophrenia. In our review we found that theoverwhelming majority of studies matched patients andcontrols on age (98%) and gender composition (82%). Only19 studies even reported data from the NART, a measure ofputative premorbid intellectual ability that may lend itself tomatching purposes. Such tasks are clearly not representedwidely in matching paradigms in the published literature.This relative neglect of matching issues from a neuropsycho-logical standpoint may reflect the fact that most studiesemploy neurocognitive measures within a framework thatincludes neuroimaging techniques, symptom scales, andpsychophysiological measures. The psychometric require-ments of a valid patient-control comparison in neurocogni-tive terms may be overlooked in the concern for the needs ofa valid neurobiological comparison. Nevertheless, futureresearch on the neuropsychology of schizophrenia will bemore informative to the extent that the vagaries of Meehl's(1970) "matching fallacy" are addressed.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

NEUROCOGNITIVE DEFICIT IN SCHIZOPHRENIA 437
In conclusion, we addressed the strength and consistency
of neurocognitive findings in schizophrenia in our quantita-
tive review. This literature has accumulated in tandem with
the view that schizophrenia is a neurological disorder that
manifests itself in behavior. Our quantitative synthesis
confirms that a large proportion of this patient population is
impaired on standard neurocognitive tests, and the evidence
suggests that any selective deficits in functions like verbal
memory are relative and exist against a background of
general dysfunction. This picture is complicated by issues of
test equivalence within and between neurocognitive func-
tions, by the need to improve reporting of potential modera-
tor variables, and by the need to develop testable illness
models that can account for why substantial numbers of
patients are indistinguishable from controls on many tests.
References
References marked with an asterisk indicate studies included in thethe meta-analyses.
* Alien, H. A., Liddle, P. F., & Frith, C. f. (1993). Negative features,retrieval processes, and verbal fluency in schizophrenia. BritishJournal of Psychiatry, 163, 769-775.
*Aloia, M. S., Gourovitch, M. L., Weinberger, D. R., & Goldberg,T. E. (1996). An investigation of semantic space in patients withschizophrenia. Journal of the International NeuropsychologicalSociety, 2, 267-273.
American Psychiatric Association. (1987). Diagnostic and statisti-cal manual of mental disorders (3rd ed.). Washington, DC:Author.
Ammons, R. B., & Ammons, C. H. (1962). The Quick Test (QT):Provisional manual. Psychological Reports (Monograph supple-ment 1-VIl), 111-161.
Andreasen, N. C., Arndt, S., Swayze, V., Cizaldo, T., Flaum, M.,O'Leary, D., Ehrhardt, J. C., & Yuh, W. T. C. (1994). Thalamicabnormalities in schizophrenia visualized through magneticresonance image averaging. Science, 266, 294—298.
Andreasen, N. C., & Ehrhardt, 3. C. (1982). Ventricular enlarge-ment in schizophrenia: Relationship to positive and negativesymptoms. American Journal of Psychiatry, 139, 297-302.
*Archer, J., Hay, D. C., & Young, A. W. (1992). Face processing inpsychiatric conditions. British Journal of Clinical Psychology,31, 45-61.
*Axelrod, B. N., Goldman, R. S., Tompkins, L. M., & Jiron, C. C.(1994). Poor differential performance on the Wisconsin CardSorting Test in schizophrenia, mood disorders, and traumaticbrain injury. Neuropsychiatry, Neuropsychology, and BehavioralNeurology, 7, 20-24.
Bakan, D. (1966). The test of significance in psychologicalresearch. Psychological Bulletin, 66, 1-29.
*Bartfai, A., Wirson, A., Levander, S., & Schalling, D. (1989).Smooth pursuit eye tracking and neuropsychological perfor-mance in healthy volunteers. Acta Psychiatrica Scandinavica,80, 479^(86.
*Beatty, W. W., Jocic, Z., Monson, N., & Katzung, V. M. (1994).Problem solving by schizophrenic and schizoaffective patientson the Wisconsin and California card sorting tests. Neuropsychol-ogy, 8, 49-54.
*Beatty, W. W., Jocic, Z., Monson, N., & Staton, D. (1993).Memory and frontal lobe dysfunction in schizophrenia andschizoaffective disorder. The Journal of Nervous and MentalDisease, 181, 448^153.
*Bellini, L., Abbruzzese, M., Gambini, O., Rossi, A., Stratta, P., &Scarone, S. (1991). Frontal and callosal neuropsychologicalperformances in schizophrenia: Further evidence of possibleattention and mnesic dysfunctions. Schizophrenia Research, 5,115-121.
Benton, A. L. (1974). Revised Visual Retention Test (4th ed.). NewYork: Psychological Corporation.
Benton, A. L., & Hamsher, K. (1983). Multilingual AphasiaExamination. Iowa City: AJA Associates.
Benton, A. L., Sivan, A. B., Hamsher, K., Varney, N., & Spreen, O.(1994). Contributions to neuropsychological assessment (2nded.). New York: Oxford University Press.
*Berman, K. F., Illowsky, B. P., & Weinberger, D. R. (1988).Physiological dysfunction of dorsolateral prefrontal cortex inschizophrenia IV: Further evidence for regional and behavioralspecificity. Archives of General Psychiatry, 45, 616-622.
*Bilder, R. M., Lipschutz-Broch, L., Reiter, G., Geisler, S. H.,Mayeroff, D. L, & Liberman, J. A. (1992). Intellectual deficits infirst-episode schizophrenia: Evidence for progressive deteriora-tion. Schizophrenia Bulletin, 18, 437-448.
*Blanchard, J. J., & Neale, J. M. (1994). The neuropsychologicalsignature of schizophrenia: Generalized or differential deficit?American Journal of Psychiatry, 151, 40-48.
*Bornstein, R. A., Nasrallah, H. A., Olson, S. C., Coffman, J. A.,Torello, M., & Schwarzkopf, S. B. (1990). Neuropsychologicaldeficit in schizophrenic subtypes: Paranoid, nonparanoid, andschizoaffective subgroups. Psychiatry Research, 31, 15-24.
*Borod, J. C., Martin, C. C., Alpert, M., Brozgold, A., &Welkowitz, J. (1993). Perception of facial emotion in schizo-phrenic and right brain-damaged patients. The Journal ofNervous and Mental Disease, 181, 494—502.
Braff, D. L. (1993). Information processing and attention dysfunc-tions in schizophrenia. Schizophrenia Bulletin, 19, 233-259.
*Braff, D. L., Glick, I. D., Johnson, M. H., & Zisook, S. (1988).The clinical significance of thought disorder across time inpsychiatric patients. The Journal of Nervous and Mental Dis-ease, 176, 213-220.
*Braff, D. L., Heaton, R., Kuck, J., Cullum, M., Moranville, J.,Grant, L, & Zisook, S. (1991). The generalized pattern ofneuropsychological deficits in outpatients with chronic schizo-phrenia with heterogeneous Wisconsin Card Sorting Test results.Archives of General Psychiatry, 48, 891-898.
*Brown, K. W., White, T., & Palmer, D. (1992). Movementdisorders and psychological tests of frontal lobe function inschizophrenic patients. Psychological Medicine, 22, 69-77.
*Buchanan, R. W., Strauss, M. E., Breier, A., Kirkpatrick, B., &Carpenter, W. T. (1997). Attentional impairments in deficit andnondeficit forms of schizophrenia. American Journal of Psychia-try, 154, 363-370.
Buschke, H., & Fuld, P. A. (1974). Evaluating storage, retention,and retrieval in disordered memory and learning. Neurology, 24,1019-1025.
*Butler, R. W., Jenkins, M. A., Sprock, J., & Braff, D. L. (1992).Wisconsin Card Sorting Test deficits in chronic paranoid schizo-phrenia: Evidence for a relatively discrete subgroup? Schizophre-nia Research, 7, 169-176.
*Calev, A. (1984). Recall and recognition in mildly disturbedschizophrenics: The use of matched tasks. Psychological Medi-cine, 14, 425-429.
*Calev, A., Edelist, S., Kugelmass, S., & Lerer, B. (1991).Performance of long-stay schizophrenics on matched verbal andvisuospatial recall tasks. Psychological Medicine, 21, 655-660.
*Calev, A., Venables, P. H., & Monk, A. F. (1983). Evidence fordistinct verbal memory pathologies in severely and mildlydisturbed schizophrenics. Schizophrenia Bulletin, 9, 247-264.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
438 HEINRICHS AND ZAKZANIS
*Caplan, R., & Guthrie, D. (1994). Blink rate in childhoodschizophrenia spectrum disorder. Biological Psychiatry, 35,228-234.
Carpenter, W. T., Buchanan, R. W., Kirkpatrick, B., & Tamminga,
C. (1993). Strong inference, theory testing, and the neuro-anatomy of schizophrenia. Archives of General Psychiatry, 50,
825-831.*Carr, S. A. (1980). Interhemispheric transfer of stereognostic
information in chronic schizophrenics. British Journal of Psychia-try, 136, 53-58.
*Carrigan, P. W., & Green, M. F. (1991). Signal detection analysisof short-term recall in schizophrenia. The Journal of Nervous
and Mental Disease, 179, 495^198.*Carter, C. S., Robertson, L. C, & Nordahl, T. E. (1992). Abnormal
processing of irrelevant information in chronic schizophrenia:Selective enhancement of Stroop facilitation. Psychiatry Re-search, 41, 137-146.
Chapman, L. J., & Chapman, J. P. (1973). Problems in themeasurement of cognitive deficit. Psychological Bulletin, 79,380-385.
Chapman, L. J., & Chapman, J. P. (1978). When should schizo-phrenic and normal groups be compared? Journal of PsychiatricResearch, 14, 321-325.
Chapman, L. J., & Chapman, J. P. (1989). Strategies for resolvingthe heterogeneity of schizophrenics and their relatives usingcognitive measures. Journal of Abnormal Psychology, 98, 357-366.
*Clare, L., McKenna, P. J., Mortimer, A. M., & Baddeley, A. D.(1993). Memory in schizophrenia: What is impaired and what ispreserved. Neumpsychologia, 31, 1225-1241.
*Cleghorn, J. M. (1989). Increased frontal and reduced parietalglucose metabolism in acute untreated schizophrenia. PsychiatryResearch, 28, 119-133.
*Cleghorn, J. M., Garnett, E. S., Nahmias, C., Brown, G. M.,Kaplan, R. D., Szechtman, H., Szechtman, B., Franco, S.,Deimer, S. W, & Cook, P. (1990). Regional brain metabolismduring auditory hallucinations in chronic schizophrenia. BritishJournal of Psychiatry, 157, 562-570.
Cleghorn, J. M., Kaplan, R. D., Szechtman, B., Szechtman, H., &Brown, G. M. (1990). Neuroleptic drag effects on cognitivefunction in schizophrenia. Schizophrenia Research, 3, 211-219.
Clementz, B. A., Grove, W. W, lacono, W. G., & Sweeney, J. A.(1992). Smooth-pursuit eye movement dysfunction and liabilityfor schizophrenia: Implications for genetic modeling. Journal ofAbnormal Psychology, 101, 117-129.
Cohen, J. (1988). Statistical power analysis for the behavioralsciences (2nd ed.). New York: Academic Press.
Cohen, J. (1994). The earth is round (p < .05). American Psycholo-gist, 49, 997-1003.
*Condray, R., Steinhauer, S. R., & Goldstein, G. (1992). Languagecomprehension in schizophrenics and their brothers. BiologicalPsychiatry, 32, 790-802.
"Condray, R., Steinhauer, S. R., Van Kammen, D. P., & Kasparek,A. (1996). Working memory capacity predicts language compre-hension in schizophrenic patients. Schizophrenia Research, 20,1-13.
"Corcoran, R., Mercer, G., & Frith, C. D. (1995). Schizophrenia,symptomatology and social inference: Investigating "theory ofmind" in people with schizophrenia. Schizophrenia Research,17, 5-13.
Cornblatt, B. A., & Keilp, J. G. (1994). Impaired attention,genetics, and the pathophysiology of schizophrenia. Schizophre-nia Bulletin, 20, 31-46.
*Cornblatt, B. A., Lenzenwger, M. F., & Kimling, L. E. (1989). Thecontinuous performance test; Identical pairs version II: Contrast-
ing attentional profiles in schizophrenic and depressed patients.Psychiatry Research, 29, 65-85.
*Craft, S., Willerman, L., & Bigler, E. D. (1987). Callosaldysfunction in schizophrenia and schizo-affective disorder. Jour-nal of Abnormal Psychology, 96, 205-213.
*Crawford, J. R., Besson, J. A. O., Bremmer, M., Ebmeier, K. P.,
Cochrane, R. H. B., & Kirkwood, K. (1992). Estimation ofpremorbid intelligence in schizophrenia. British Journal ofPsychiatry, 161, 69-74.
*Crawford, J. R., Obonsawin, M. C., & Bremner, M. (1993).
Frontal lobe impairment in schizophrenia: Relationship to intel-lectual functioning. Psychological Medicine, 23, 787-790.
*Cullum, C. M., Harris, J. G., Waldo, M. C., Smernoff, E.,Madison, A., Nagamato, H. T., Griffith, J., Adler, L. E., &
Freedman, R. (1993). Neurophysiological and neuropsychologi-cal evidence for attentional dysfunction in schizophrenia. Schizo-phrenia Research, 10, 131—141.
*Culver, C. L., Kunen, S., & Zinkgraf, S. A. (1986). Patterns ofrecall in schizophrenics and normal subjects. The Journal ofNervous and Mental Disease, 174, 620-623.
*Cutmore, T. R. H., & Beninger, R. J. (1990). Do neurolepticsimpair learning in schizophrenic patients? Schizophrenia Re-search, 3, 173-186.
*Dabson, D. J. G., & Neufeld, R. W. J. (1987). Span of apprehen-sion among remitted schizophrenics using small visual angles.The Journal of Nervous and Mental Disease, 175, 362-370.
*Dalby, J. T., & Williams, R. (1986). Preserved reading andspelling ability in psychotic disorders. Psychological Medicine,16, 171-175.
*David, A. S. (1993). Callosal transfer in schizophrenia: Too muchor too little. Journal of Abnormal Psychology, 102, 573-579.
*David, A. S. (1993). Spatial and selective attention in the cerebralhemispheres in depression, mania, and schizophrenia. Brain &Cognition, 23, 166-180.
*David, A. S., & Cutting, J. C. (1992). Visual imagery and visualsemantics in the cerebral hemispheres in schizophrenia. Schizo-phrenia Research, S, 263-271.
David, D. G., Goldberg, T. E., Gibbon, R., & Weinberger, D. R.(1991). Lack of a bimodal distribution of ventricular size inschizophrenia: A Gaussian mixture analysis of 1056 cases andcontrols. Biological Psychiatry, 30, 887-903.
*Dean, R. S., Gray, J. W., & Seretny, M. L. (1987). Cognitiveaspects of schizophrenia and primary affective depression.International Journal of Clinical Psychology, 9, 33-36.
*de Bonis, M., de Boeck, P., Lida-Pulik, H., & Feline, A. (1995).Identity disturbances and self-other differentiation in schizo-phrenics, borderlines, and normal controls. Comprehensive Psy-chiatry, 36, 362-366.
Delis, D. C., Kramer, J. H., Kaplan, E., & Ober, B. A. (1987).California Verbal Learning Test. San Antonio, TX: The Psycho-logical Corporation.
*DeMyer, M. K., Gilmor, R. L., Hendrie, H. C., DeMyer, W. E.,Augustyn, G. T., & lackson, R. K. (1988). Magnetic resonancebrain images in schizophrenic and normal subjects: Influence ofdiagnosis and education. Schizophrenia Bulletin, 14, 21-37.
De Renzi, E., & Vignolo, L. (1962). The Token Test: A sensitive testto detect receptive disturbances in aphasics. Brain, 85, 665-678.
*Dieci, M., Vita, A., Silenzi, C., Caputo, A., Comazzi, M., Ferrari,L., Ghiringhelli, L., Mezzetti, M., Tenconi, F., & Invernizzi, G.(1997). Non-selective impairment of Wisconsin Card SortingTest performance in patients with schizophrenia. SchizophreniaResearch, 25, 33^42.
*Ditchfield, H., & Hemsley, D. R. (1990). Interhemispherictransfer of information and schizophrenia. European Archives ofPsychiatry and Neurological Sciences, 239, 309-313.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
NEUROCOGNITIVE DEFICIT IN SCHIZOPHRENIA 439
Dunn, L. M., & Dunn, L. M. (1981). Peabody Picture Vocabulary
Test—revised manual. Circle Pines, MN: American GuidanceService.
*Earle-Boyer, E. A., Serper, M. R., Davidson, M., & Harvey, P. D.(1991). Continuous performance tests in schizophrenic patients:Stimulus and medication effects on performance. PsychiatryResearch, 37, 47-56.
*Eikmeier, G., Lodemann, E., Zerbin, D., & Gastpar, M. (1992).P300, clinical symptoms, and neuropsychological parameters inacute and remitted schizophrenia: A preliminary report. Biologi-
cal Psychiatry, 31, 1065-1069.Elwood, R. W. (1995). The California Verbal Learning Test:
Psychometric characteristics and clinical application. Neuropsy-chology Review, 5, 173-201.
Ennis, J. H., & Whelton, C. (1994). The relationship between face
recognition, facial affect recognition, and social skills in schizo-phrenia. Canadian Journal of Psychiatry, 39, 58-66.
Ernst, J., Warner, M. H., Hoehberg, M. T., & Townes, B. (1988).Factor analysis of the Halstead-Reitan Neuropsychological Bat-tery including the WAIS and replications using the WAIS-R.
International Journal of Neuropsychology, 10, 103-105.*Fautsman, W. O., Moses, J. A., Ringo, D. L., & Newccomer, J. W.
(1991). Left-handedness in male schizophrenic patients is associ-ated with increased impairment on the Luria-Nebraska Neuropsy-chological Battery. Biological Psychiatry, 30, 326-334.
Possum, B., Holmberg, H., & Reinvang, I. (1992). Spatial and
symbolic factors in performance on the Trail Making Test.Neuropsychology, 6, 71-75.
*Frame, C. L., & Oltmanns, T. F. (1982). Serial recall byschizophrenic and affective patients during and after psychotic
episodes. Journal of Abnormal Psychology, 91, 311-318.*Franke, P., Maier, W., Hain, C., & Klinger, T. (1992). Wisconsin
Card Sorting Test: An indicator of vulnerability to schizophre-nia? Schizophrenia Research, 6, 243-249.
*Franke, P., Maier, W., Hardt, J., Frieboes, R., Lichtermann, D., &Hain, C. (1993). Assessment of frontal lobe functioning inschizophrenia and unipolar major depression. Psychopathology,26, 76-84.
*Franke, P., Maier, W., Hardt, J., & Hain, C. (1993). Cognitivefunctioning and anhedonia in subjects at risk for schizophrenia.Schizophrenia Research, 10, 77—84.
*Fraser, W. L, King, K. M., Thomas, P., & Kendell, R. E. (1986).The diagnosis of schizophrenia by language analysis. BritishJournal of Psychiatry, 148, 275-278.
*Frith, C. D., Friston, K. J., Herald, S., Silberweig, D., Fletcher, P.,Camila, C., Dolan, R. J., Frackowiak, F. S. J., & Liddle, P. F.(1995). Regional brain activity in chronic schizophrenic patientsduring the performance of a verbal fluency task. British Journalof Psychiatry, 167, 343-349.
*Galynker, I. I., & Harvey, P. D. (1992). Neuropsychologicalscreening in the psychiatric emergency room. ComprehensivePsychiatry, 33, 291-295.
*Garety, P. A., Phil, M., Hemsley, D. R., & Wessely, S. (1991).Reasoning in deluded schizophrenic and paranoid patients. TheJournal of Nervous and Mental Disease, 179, 194-201.
*Gold, J. M., Herman, B. P., Randolph, C., Wyler, A. R., Goldberg,T. E., & Weinberger, D. R. (1994). Schizophrenia and temporallobe epilepsy: A neuropsychological analysis. Archives ofGenreral Psychiatry, 51, 265-272.
*Gold, J. M., Randolph, C., Carpenter, C. J., Goldberg, T. E., &Weinberger, D. R. (1992). Forms of memory failure in schizophre-nia. Journal of Abnormal Psychology, 101, 487-494.
Goldberg, T. E., & Gold, J. M. (1995). Neurocognitive deficits inschizophrenia. In S. R. Hirsch & D. R. Weinberger (Eds.),
Schizophrenia (pp. 146-162). Oxford, England: Blackwell
Science.Goldberg, T. E., Gold, J. M., Greenberg, R., & Griffin, S. (1993).
Contrasts between patients with affective disorders and patientswith schizophrenia on a neuropsychological test battery. Ameri-can Journal of Psychiatry, 150, 1355-1362.
Goldberg, T. E., Kelsoe, J. R., Weinberger, D. R., Pliskin, N. H.,Kirwin, P. D., & Berman, K. F. (1988). Performance ofschizophrenia patients on putative neuropsychological tests offrontal lobe function. International Journal ofNeuroscience, 42,51-58.
*Goldberg, T. E., Ragland, D. R., Gold, J. M., Bigelow, L. B.,Torrey, E. F., & Weinberger, D. R. (1990). Neuropsychologicalassessment of monozygotic twins disconcordant for schizophre-nia. Archives of General Psychiatry, 47, 1066-1072.
*Goldberg, T. E., Saint-Cyr, J. A., & Weinberger, D. R. (1990).Assessment of procedural learning and problem solving inschizophrenic patients by tower of Hanoi type tasks. Journal ofNeuropsychiatry and Clinical Neurosciences, 2, 165-173.
*Goldberg, T. E., Weinberger, D. R., Pliskin, N. H., Berman, K. F,& Plodd, M. H. (1989). Recall memory deficit in schizophrenia:A possible manifestation of prefrontal dysfunction. Schizophre-nia Research, 2, 251-257.
Golden, C. J. (1978). Stroop Color and Word Test. Chicago:Stoelting.
Golden, C. J., Purisch, A. D., & Hammeke, T. A. (1985).Luria-Nebraska Neuropsychological Battery: Forms I and II.Los Angeles: Western Psychological Services.
Goldstein, G. (1984). Comprehensive neuropsychological assess-ment batteries. In G. Goldstein & M. Hersen (Eds.), Handbookof psychological assessment (pp. 181-210). New York: Per-gamon Press.
Goldstein, G., & Shelly, C. (1972). Statistical and normativestudies of the Halstead Neuropsychological Test Battery relevantto a neuropsychiatric hospital setting. Perceptual and MotorSkills, 34, 603-620.
*Goldstein, G., & Zubin, J. (1990). Neuropsychological differ-ences between young and old schizophrenics with and withoutassociated neurological dysfunction. Schizophrenia Research, 3,117-126.
*Goldstein, P. C., Rosenbaum, G., & Taylor, M. A. (1997).Assessment of differential attention mechanisms in seizuredisorders and schizophrenia. Neuropsychology, 11, 309-317.
*Gourovitch, M. L., Goldberg, T. E., & Weinberger, D. R. (1996).Verbal fluency deficits in patients with schizophrenia: Semanticfluency is differentially impaired as compared with phonologicfluency. Neuropsychology, 10, 573-577.
Green, B. F, & Hall, J. A. (1984). Quantitative methods forliterature reviews. Annual Review of Psychology, 35, 37-53.
*Green, M., & Walker, E. (1985). Neuropsychological perfor-mance and positive and negative symptoms in schizophrenia.Journal of Abnormal Psychology, 94, 460-469.
*Green, M., & Walker, E. (1986). Attentional performance inpositive and negative symptom schizophrenia. The Journal ofNervous and Mental Disease, 174, 208-213.
*Greiffenstein, M., Milberg, W., Lewis, R., & Rosenbaum, G.(1981). Temporal lobe epilepsy and schizophrenia: Comparisonof reaction time deficits. Journal of Abnormal Psychology, 90,105-112.
*Gruzelier, J., Liddiard, D., Davis, L., & Wilson, L. (1990).Topographical EEG differences between schizophrenic patientsand controls during neuropsychological functional activation.International Journal of Psychophysiology, S, 275-282.
*Gruzelier, J., Seymour, K., Wilson, L., Jolley, A., & Hirsch, S.(1988). Impairments on neuropsychological tests of temporo-
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
440 HEINRICHS AND ZAKZANIS
hippocampal and frontohippocampal functions and word fluencyin remitting schizophrenia and affective disorders. Archives of
General Psychiatry, 45, 623-629.*Guich, S. M., Buchsbaum, M. S., Burgwald, L., Wu, J., Haier, R.,
Asarnow, R., Nuechterlein, K., & Patkin, S. (1989). Effect ofattention on frontal distribution of delta activity and cerebral
metabolic rate in schizophrenia. Schizophrenia Research, 2,
439-448.*Hagger, C, Buckley, P., Kenny, J. T., Friedman, L., Ubogy, D., &
Meltzer, H. Y. (1993). Improvement in cognitive functions andpsychiatric symptoms in treating refractory schizophrenic pa-
tients receiving clozapine. Biological Psychiatry, 34, 702-712.*Hain, C., Maier, W., Klinger, T., & Frankle, P. (1993). Positive/
negative symptomatology and experimental measures of atten-tion in schizophrenic patients. Psychopathology, 26, 62-69.
*Hanes, K. R., Andrewes, D. G., & Pantelis, C. (1995). Cognitiveflexibility and complex integration in Parkinson's disease,Huntington's disease, and schizophrenia. Journal of the Interna-
tional Neuropsychological Society, 1, 545-553.*Harris, J. G., Adler, L. E., Young, D. A., Cullum, C. M., Rilling,
L. M., Cicerello, A., Intermann, P. M., & Freedman, R. (1996).Neuropsychological dysfunction in parents of schizophrenics.
Schizophrenia Research, 20, 253-260.*Harvey, P. D. (1983). Speech competence in manic and schizo-
phrenic psychoses: The association between clinically ratedthought disorder and cohesion and reference performance.
Journal of Abnormal Psychology, 92, 368-377.*Harvey, P. D., Earle-Boyer, E. A., Wielgus, M. S., & Levinson,
J. C. (1986). Encoding, memory, and thought disorder inschizophrenia and mania. Schizophrenia Bulletin, 12, 252-261.
"Harvey, P. D., Keefe, R. S. E., Moskowitz, J., Putrram, K. M.,Mohs, R. C., & Davis, K. L. (1990). Attentional markers ofvulnerability to schizophrenia: Performance of medicated andunmedicated patients and normals. Psychiatry Research, 33,
179-188.*Harvey, S. A., Nelson, E., Haller, J. W., & Early, T. S. (1993).
Lateralized attentional abnormality in schizophrenia is corre-lated with severity of symptoms. Biological Psychiatry, 33,
93-99.Heaton, R. K., Chelune, G. J., Talley, J., Kay, G. G., & Curtiss, G.
(1993). Wisconsin Card Sorting Test manual—revised andexpanded. Odessa, FL: Psychological Assessment Resources.
Heaton, R. K., & Crowley, T. J. (1981). Effects of psychiatricdisorders and their somatic treatments on neuropsychologicaltest results. In S. B. Filskov & T. J. Boll (Eds.), Handbook ofclinical neuropsychology (pp. 481-525). New York: Wiley.
Heaton, R. K., Paulsen, J. S., McAdams, L. A., Kuck, J., Zisook, S.,Braff, D., Harris, J., & Jeste, D. V. (1994). Neuropsychologicaldeficits in schizophrenics: Relationship to age, chronicity, anddementia. Archives of General Psychiatry, SI, 469-476.
Hedges, L. V. (1994). Fixed effect models. In H. Cooper & L. V.Hedges (Eds.), The handbook of research synthesis (pp. 285-299). New York: Russell Sage Foundation.
Hedges, L. V., & Olkin, I. (1985). Statistical methods for meta-analysis. New York: Academic Press.
Heinrichs, R. W. (1990). Variables associated with Wisconsin CardSorting Test performance in neuropsychiatric patients referredfor assessment. Neuropsychiatry, Neuropsychology, and Behav-ioral Neurology, 3, 107-112.
Heinrichs, R. W. (1993). Schizophrenia and the brain: Conditionsfor a neuropsychology of madness. American Psychologist, 48,221-233.
Heinrichs, R. W., & Awad, A. G. (1993). Neurocognitive subtypesof chronic schizophrenia. Schizophrenia Research, 9, 49-58.
Heinrichs, R. W., Ruttan, L. A., Zakzanis, K. K., & Case, D. (1997).Parsing schizophrenia with neurocognitive tests: Evidence ofstability and validity. Brain and Cognition, 35, 207-224.
*Highgate-Maynard, S., & Neufeld, R. W. J. (1986). Schizophrenicmemory-search performance involving nonverbal stimulus prop-
erties. Journal of Abnormal Psychology, 95, 67-73.*Holzman, P. S., Shenton, M. E., & Solovay, M. R. (1986). Quality
of thought disorder in differential diagnosis. SchizophreniaBulletin, 12, 360-372.
lacono, W. G., Moreau, M., Beiser, M., Heming, J. A. E., & Liu,T. Y. (1992). Smooth-pursuit eye tracking in first-episode
psychotic patients and their relatives. Journal of AbnormalPsychology, 101, 104-116.
*Javitt, D. C., Doneshka, P., Zylberman, I., Ritter, W., Vaughan,H. G., Jr. (1993). Impairment of early cortical processing inschizophrenia: An event-related potential confirmation study.Biological Psychiatry, 33, 513-519.
Johnson, B. T. (1989). DSTAT: Software for the meta-analyticreview of research literatures. Hillsdale, NJ: Erlbaum.
*Johnson, O., & Crockett, D. (1982). Changes in perceptualasymmetries with clinical improvement of depression and schizo-phrenia. Journal of Abnormal Psychology, 91, 45-54.
*Jones, S. H., Gray, J. A., & Hemsley, D. R. (1992). Loss of thekamin blocking effect in acute but not chronic schizophrenics.Biological Psychiatry, 32, 739-755.
*Jones, S. H., Hemsley, D. R., & Gray, J. A. (1991). Contextualeffects on choice reaction time and accuracy in acute and chronicschizophrenics: Impairment in selective attention or in theinference of prior learning? British Journal of Psychiatry, 159,415-421.
"Joyce, E. M., Collinson, S. L., & Crichton, P. (1996). Verbalfluency in schizophrenia: Relationship with executive function,semantic memory and clinical alogia. Psychological Medicine,26, 39-49.
*Kahn, E. M., Weiner, R. D., Coppola, R., Kudler, H. S., & Schultz,K. (1993). Spectral and topographic analysis of EEC in schizo-phrenic patients. Biological Psychiatry, 33, 284—290.
*Kareken, D. A., Our, R. C., Mozley, P. D., Mozley, L. H., Saykin,A. J., Stasel, D. L. & Gur, R. E. (1995). Cognitive functioningand neuroanatomic volume measures in schizophrenia. Neuropsy-
chology, 9, 211-219.*Kareken, D. A., Moberg, P. J., & Gur, R. C. (1996). Proactive
inhibition and semantic organization: Relationship with verbalmemory in patients with schizophrenia. Journal of the Interna-tional Neuropsychological Society, 2, 486-493.
"Katsanis, J., lacono, W. G., & Beiser, M. (1990). Anhedonia andperceptual aberration in first-episode psychotic patients and theirrelatives. Journal of Abnormal Psychology, 99, 202-206.
"Kawasaki, Y, Maeda, Y, Suzuki, M., Urato, K., Higashima, M.,Kiba, K., Yamaguchi, N., Matsuda, H., & Hisada, K. (1993).SPECT analysis of regional cerebral blood flow changes inpatients with schizophrenia during the Wisconsin Card SortingTest. Schizophrenia Research, 10, 109-116.
*Keefe, J. A., & Magaro, P. A. (1980). Creativity and schizophre-nia: An equivalence of cognitive processing. Journal of Abnor-mal Psychology, 89, 390-398.
*Keefe, R. S. E., Lees Roitman, S. E., Harvey, P. D., Blum, C. S.,DuPre, R. L., Prieto, P. M., Davidson, M., & Davis, K. L. (1995).A pen-and-paper human analogue of a monkey prefrontal cortexactivation task: Spatial working memory in patients with schizo-phrenia. Schizophrenia Research, 17, 25-33.
*Kerr, S. L., & Neale, J. M. (1993). Emotion perception inschizophrenia: Specific deficit or further evidence of generalizedpoor performance. Journal of Abnormal Psychology, 102, 312-318.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
NEUROCOGNiriVE DEFICIT IN SCHIZOPHRENIA 441
*Killian, G. A., Holzman, P. S., Davis, J. M., & Gibbons, R. (1984).
Effects of psychotropic medication on selected cognitive and
perceptual measures. Journal of Abnormal Psychology, 93,
58-70.
Klove, H. (1963). Clinical neuropsychology. In F. M. Forster (Ed.),
The medical clinics of North America (pp. 1647-1658). New
York: Saunders.
*Knight, R. A., Elliot, D. S., & Freedman, E. G. (1985). Short-term
visual memory in schizophrenics. Journal of Abnormal Psychol-
ogy, 94, 427-442.
*Knight, R. A., Youard, P. J., & Wooles, I. M. (1985). Visual
information-processing deficits in chronic schizophrenic sub-
jects using tasks matched for discriminating power. Journal of
Abnormal Psychology, 94, 454-459.
*Kolb, B., & Whishaw, I. Q. (1983). Performance of schizophrenic
patients on tests sensitive to left or right frontal, temporal, or
parietal function in neurological patients. The Journal of Ner-
vous and Mental Disease, 171, 435-443.
*Krakowski, M. I., Convit, A., Jaeger, J., Lin, S., & Volavka, J.
(1989). Neurological impairment in violent schizophrenic inpa-
tients. American Journal of Psychiatry, 146, 849-853.
Kraemer, H. C., & Andrews, G. (1982). A nonparametric technique
for meta-analysis effect size calculation. Psychological Bulletin,
91, 404-412.
*Kremen, W. S., Seidman, L. S., Faraone, S. V., Pepple, J. R.,
Lyons, M. J., & Tsuang, M. T. (1996). The "3Rs" and
neuropsychological function in schizophrenia: An empirical test
of the matching fallacy. Neuropsychology, 10, 22-31.
*Kwapil, T. R., Chapman, L. J., & Chapman, J. P. (1992). Monaural
and binaural story recall by schizophrenic subjects. Journal of
Abnormal Psychology, 101, 709-716.
*Kwapil, T. R., Hegley, D. C., Chapman, L. J., & Chapman, J. P.
(1990). Facilitation of word recognition by semantic priming in
schizophrenia. Journal of Abnormal Psychology, 99, 215-221.
*Landro, N. I., Orbeck, A. L., & Rund, B. R. (1993). Memory
functioning in chronic and non-chronic schizophrenics, affec-
tively disturbed patients and normal controls. Schizophrenia
Research, 10, 85-92.
*Laplaute, L., Everett, J., & Thomas, J. (1992). Inhibition through
negative priming with Stroop stimuli in schizophrenia. British
Journal of Clinical Psychology, 31, 307-326.
*Lawrie, S. M., Abukmeil, S. S., Chiswick, A., Egan, V., Santosh,
C. G., & Best, J. J. K. (1997). Qualitative cerebral morphology in
schizophrenia: A magnetic resonance imaging study and system-
atic literature review. Schizophrenia Research, 25, 155—166.
"Levander, S. E., Bartfai, A., & Schalling, D. (1985). Regional
cortical dysfunction in schizophrenic patients studied by comput-
erized neuropsychological methods. Perceptual and Motor Skills,61, 479-495.
*Levin, S., Hall, J. A., Knight, R. A., & Alpert, M. (1985). Verbaland nonverbal expression of affect in speech of schizophrenic
and depressed patients. Journal of Abnormal Psychology, 94,
487-497.
Levin, S., Yurgelun-Todd, D., & Craft, S. (1989). Contributions of
clinical neuropsychology to the study of schizophrenia. Journal
of Abnormal Psychology, 98, 341-356.
*Lewis, S. W., Ford, R. A., Syed, G. M., Reveley, A. M., Toone,
B. K. (1992). A controlled study of 99mTc-HMPAO single-
photon emission imaging in chronic schizophrenia. Psychologi-
cal Medicine, 22,27-35.
Lezak, M. D. (1995). Neuropsychological assessment (3rd ed.).
New York: Oxford University Press.
Liddle, P. F., & Barnes, T. R. E. (1990). Syndromes of chronic
schizophrenia. British Journal of Psychiatry, 157, 558-561.
*Lim, K. O., Sullivan, E. V, Zipursky, R. B., & Pfefferbaum, A.
(1996). Cortical gray matter volume deficits in schizophrenia: A
replication. Schizophrenia Research, 20, 157-164.
*Maler, W., Franke, P., Hain, C., Kopp, B., & Rist, F. (1992).
Neuropsychological indicators of the vulnerability to schizophre-
nia. Progress in Neuro-Psychopharmacology and Biological
Psychiatry, 16, 703-715.
*Mandal, M. K., & Rai, A. (1987). Responses to facial emotion and
psychopathology. Psychiatry Research, 20, 317-323.
*Marsh, L., Suddath, R. L., Higgins, N., & Weinberger, D. R.
(1994). Medial temporal lobe structures in schizophrenia: Rela-
tionship of size to duration of illness. Schizophrenia Research,
II, 225-238.
*Mather, J. A., Neufeld, R. W. J., Merskey, H., & Russel, N. C.
(1992). Disruption of saccade production during oculomotor
tracking in schizophrenia and the use of its changes across target
velocity as a discriminator of the disorder. Psychiatry Research,
43, 93-109.
*Mattes, R., Cohen, R., Berg, P., Canavan, A. G. M., & Hopmann,
G. (1991). Slow-cortical potentials (SCPS) in schizophrenic
patients during performance of the Wisconsin Card Sorting Test
(WCST). Neumpsychologia, 29, 195-205.
*McCarley, R. W., Faux, S. F., Shenton, M., LeMay, M., Cane, M.,
Ballinger, R., & Duffy, F. H. (1989). CT abnormalities in
schizophrenia: A preliminary study of their correlations with
P300/P200 electrophysiological features and positive/negative
symptoms. Archives of General Psychiatry, 46, 698-708.
*McGuire, P. K., Silbersweig, D. A., Wright, 1, Murray, R. M.,
Frackowiak, R. S. J., & Frith, C. D. (1996). The neural correlates
of inner speech and auditory verbal imagery in schizophrenia:
Relationship to auditory verbal hallucinations. British Journal of
Psychiatry, 169,148-159.
McKay, S. E., & Golden, C. J. (1981). The assessment of specific
neuropsychological skills using scales derived from factor
analysis of the Luria-Nebraska Neuropsychological Battery.
International Journal of Neuroscience, 14, 189-204.
*McKay, S. E., McKenna, P. J., Bentham, P., Mortimer, A. M.,
Holbery, A., & Hodges, J. R. (1996). Semantic memory is
impaired in schizophrenia. Biological Psychiatry, 39, 929-937.
Meehl, P. E. (1970). Nuisance variables and the ex post facto
design. In M. Radner & S. Winokur (Eds.), Minnesota studies in
the philosophy of science (pp. 373-402). Minneapolis, MM:
University of Minnesota Press.
*Michie, P. T., Fox, A. M., Warp, P. B., Catts, S. V, & McConaghy,
N. (1990). Event-related potential indices of selective attention
and cortical lateralization in schizophrenia. Psychophysiology, 8,
234-244.
Milner, B. (1964). Some effects of frontal lobectomy in man. In
J. M. Warren & K. Akert (Eds.), The frontal granular cortex and
behavior(pp. 313-334). New York: McGraw-Hill.
*Min, S. K., & On, B. H. (1992). Hemispheric asymmetry in visual
recognition of words and motor response in schizophrenic and
depressive patients. Biological Psychiatry, 31, 255-262.
*Mirsky, A. F, Ingraham, L. J., & Kugelmass, S. (1995). Neuropsy-
chological assessment of attention and its pathology in the Israeli
cohort. Schizophrenia Bulletin, 21, 193-204.
*Morice, R. (1990). Cognitive inflexibility and pre-frontal dysfunc-
tion in schizophrenia and mania. British Journal of Psychiatry,157, 50-54.
*Morice, R., & Delahunty, A. (1996). Frontal/executive impair-
ments in schizophrenia. Schizophrenia Bulletin, 22, 125-137.*Morice, R., & McNicol, D. (1986). Language changes in schizo-
phrenia: A limited replication. Schizophrenia Bulletin, 12, 239-
251.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
442 HEINRICHS AND ZAKZANIS
*Morrison-Stewart, S. L., Williamson, P. C., Corning, W. C.,
Kutcher, S. P., Snow, W. G., & Merskey, H. (1992). Frontal and
non-frontal lobe neuropsychological test performance and clini-
cal symptomatology in schizophrenia. Psychological Medicine,
22, 353-359.*Mueser, K. T., Bellack, A. S., Morrison, R. L., & Wade, J. H.
(1990). Gender, social competence, and symptomatology in
schizophrenia: A longitudinal analysis. Journal of Abnormal
Psychology, 99, 138-147.
*Nathaniel-James, D. A., Brown, R., & Ron, M. A. (1996).
Memory impairment in schizophrenia: Its relationship to execu-tive function. Schizophrenia Research, 21, 85-96.
*Nathaniel-James, D. A., & Frith, C. D. (1996). Confabulation inschizophrenia: Evidence of a new form? Psychological Medi-
cine, 26, 391-399.Nelson, H. E. (1982). The National Adult Reading Test (NART) test
manual. Windsor, England: NFER-Nelson.
*Nelson, H. E., Pantelis, C., Carruthers, K., Speller, J., Baxendale,S., & Barnes, T. R. E. (1990). Cognitive functioning and
symptomatology in chronic schizophrenia. Psychological Medi-cine, 20, 357-365.
*Nestor, P. G., Faux, S. F., McCarley, R. W, Shenton, M. E., &Sands, S. F. (1990). Measurement of visual sustained attention in
schizophrenia using signal detection analysis and a newlydeveloped computerized CPT task. Schizophrenia Research, 3,
329-332.Nuechterlein, K. H., & Dawson, M. E. (1984). Information
processing and attentional functioning in the developmental
course of schizophrenic disorders. Schizophrenia Bulletin, 10,
160-203.*Obiols, J. E., Clos, M., Corbero, E., Domingo, M., Trincheria, I.,
& Domench, E. (1992). Sustained attention deficit in youngschizophrenic and schizotypic men. Psychological Reports, 71,
1131-1136.*Obiols, J. E., Marcos, T., & Salamero, M. (1987). Ventricular
enlargement and neuropsychological testing in schizophrenia.Acta Psychiatrica Scandinavica, 76, 199-202.
"O'Carrol, R. (1992). Selecting controls for schizophrenia research
studies: The use of the National Adult Reading Test (NART) is ameasure of premorbid ability. Schizophrenia Research, 8, 137-141.
*O'Donnell, B. F, Shenton, M. E., McCarley, R. W., Faux, S. F.,Smith, R. S., Salisbury, D. F, Nestor, P. G., Pollack, S. D.,
Kikinis, R., & Jolesz, F. A. (1993). The auditory N2 componentin schizophrenia: Relationship to MRI temporal lobe gray matterand to other ERP abnormalities. Biological Psychiatry, 34,
26-40.Oltmanns, T. F. (1978). Selective attention in schizophrenia and
manic psychoses: The effect of distraction on informationprocessing. Journal of Abnormal Psychology, 87, 212—225.
*Oltmanns, T. F., Murphy, R., Berenbaum, H., & Dunlop, S. R.(1985). Rating verbal communication impairment in schizophre-nia and affective disorders. Schizophrenia Bulletin, 11, 292-299.
Orwin, R. G. (1983). A fail-safe N for effect size. Journal of
Educational Statistics, 8, 157-159.*Palmer, B. W, Heaton, R. K., Paulsen, J. S., Kuck, J., Braff, D.,
Harris, M. J., Hsook, S., & Jeste, D. V. (1997). Is it possible to beschizophrenic yet neuropsychologically normal? Neuropsychol-
ogy, 11, 437^(46.*Park, S., & Holzman, P. S. (1993). Association of working
memory deficit and eye tracking dysfunction in schizophrenia.Schizophrenia Research, 11, 55-61.
*Paulsen, J. S., Heaton, R. K., Sadek, J. R., Perry, W., Delis, D. C.,
Braff, D., Kuck, J., Zisook, S., & Jeste, D. V. (1995). The nature
of learning and memory impairments in schizophrenia. Journal
of the International Neuropsychological Society, 1, 88—99.
*Paus, T. (1991). Two modes of central gaze fixation maintenance
and oculomotor distractibility in schizophrenics. Schizophrenia
Research, 5, 145-152.
*Paus, T. (1989). Oculomotor and electrophysiological signs of
distractibility in schizophrenics. Activitas Nervosa Superior, 32,
147-148.
*Phillips, M. L., Woodruff, P. W. R., & David, A. S. (1996). Stroop
interference and facilitation in the cerebral hemispheres in
schizophrenia. Schizophrenia Research, 20, 57-68.
*Pishkin, V., & Bourne Jr., L. E. (1981). Abstraction and the use of
available information by schizophrenic and normal individuals.
Journal of Abnormal Psychology, 90, 197-203.
*Pishkin, V., & Williams, W. V. (1983). Cognitive deficit in
schizophrenia: Subvocal mediation, rigidity, and complexity
parameters. The Journal of Nervous and Mental Disease, 171,
24-29.*Pishkin, V., & Williams, W. V. (1984). Redundancy and complex-
ity of information in cognitive performances of schizophrenic
and normal individuals. Journal of Clinical Psychology, 40,
648-654.
*Pogue-Geile, M. F, & Oltmanns, T. F. (1980). Sentence percep-
tion and distractibility in schizophrenic, manic, and depressed
patients. Journal of Abnormal Psychology, 89, 115-124.*Ragin, A. B., & Oltmanns, T. F. (1986). Lexical cohesion and
formal thought disorder during and after psychotic episodes.
Journal of Abnormal Psychology, 95, 181-183.
Raine, A. (1992). An evaluation of structural and functional
prefrontal deficits in schizophrenia: MRI and neuropsychologi-
cal measures. Psychiatry Research, 45, 123-137.
*Raine, A., Andrews, H., Sheard, C., Walder, C., & Manders, D.
(1989). Interhemispheric transfer in schizophrenics, depressives,
and normals with schizoid tendencies. Journal of Abnormal
Psychology, 95,35-41.
*Raine, A., Harrison, G. N., Reynolds, G. P., Sheard, C., Cooper,
J. E., & Medley, I. (1990). Structural and functional characteris-tics of the corpus callosum in schizophrenics, psychiatric
controls, and normal controls: A Magnetic resonance imaging
and neuropsychological evaluation. Archives of General Psychia-
try, 47, 1060-1064.'Randolph, C., Gold, J. M., Kozora, E., Cullum, C. M., Herman,
B. P., & Wyler, A. R. (1994). Estimating memory function:
Disparity of Wechsler Memory Scale—Revised and CaliforniaVerbal Learning Test indices in clinical and normal samples.
Clinical Neuropsychologist, 8, 99-108.
Randolph, C., Goldberg, T. E., & Weinberger, D. R. (1993). The
neuropsychology of schizophrenia. In K. M. Hielman & E.Valenstein (Eds.), Clinical neuropsychology (3rd ed.). (pp.
499-522). New York: Oxford University Press.Raven, J. C. (1982). Revised manual for Raven's Progressive
Matrices and Vocabulary Scale. Windsor, England: NFER-
Nelson.Raz, S., & Raz, N. (1990). Structural brain abnormalities in the
major psychoses: A quantitative review of the evidence fromcomputerized imaging. Psychological Bulletin, 108, 93-108.
Reitan, R. (1958). Validity of the Trailmaking Test as an indicatorof organic brain damage. Perceptual and Motor Skills, 8,
271-276.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
NEUROCOGNIT1VE DEFICIT IN SCHIZOPHRENIA 443
Reitan, R., & Wolfson, D. (1993). The Halstead-Reitan Neuropsy-chological Test Battery: Theory and clinical interpretation.
Tucson, AZ: Neuropsychology Press.*Rist, P., & Thurm, I. (1984). Effects of intramodal and crossmodal
stimulus diversity on the reaction time of chronic schizophren-ics. Journal of Abnormal Psychology, 93, 331-338.
*Rizzo, L., Danion, J. M., Van Der Linden, M., & Grange, D.(1996). Patients with schizophrenia remember that an event hasoccurred, but not when. British Journal of Psychiatry, 168,
427-431.*Rizzo, L., Danion, J. M., Van Der Linden, M., Grange, D., &
Rohmer, J. G. (1996). Impairment of memory for spatial context
in schizophrenia. Neuropsychology, 10, 376-384.*Robertson, G., & Taylor, P. J. (1985). Some cognitive correlates of
schizophrenic illness. Psychological Medicine, 15, 81-98.*Rosenbaum, G., Chapin, K., & Shore, D. L. (1988). Attention
deficit in schizophrenia and schizotypy: Marker versus symptom
variables. Journal of Abnormal Psychology, 97, 41-47.Rosenthal, R. (1979). The file drawer problem and tolerance for
null results. Psychological Bulletin, 86, 638-641.Rosenthal, R. (1991). Meta-analytic procedures for social re-
search. Beverly Hills, CA: Sage.
Rosenthal, R. (1995). Writing meta-analytic reviews. Psychologi-cal Bulletin, 118, 183-192.
Rosenthal, R., & Rubin, D. B. (1979). A note on percent varianceexplained as a measure of the importance of effects. Journal ofApplied Social Psychology, 9, 395-396.
Rosenthal, R., & Rubin, D. B. (1982). A simple general purposedisplay of magnitude of experimental effect. Journal of Educa-tional Psychology, 74, 166-169.
*Rdxborough, H., Muir, W. J., Blackwood, D. H. R., Walker, M. T.,& Blackburn, I. M. (1993). Neuropsychological and P300abnormalities in schizophrenics and their relatives. Psychologi-cal Medicine, 23, 305-314.
*Rund, B. R. (1982). The effect of distraction on focal attention inparanoid and non-paranoid schizophrenic patients compared tonormals and non-psychotic psychiatric patients. Journal ofPsychiatric Research, 17, 241-250.
*Rund, B. R. (1989). Distractibility and recall capability inschizophrenics: A 4-year longitudinal study of stability incognitive performance. Schizophrenia Research, 2, 265—275.
*Rund, B. R., Landro, N. I., & Orbeck, A. L. (1993). Stability inbackward masking performance in schizophrenics, affectivelydisturbed patients, and normal controls. Journal of Nervous andMental Disease, 181, 233-237.
*Rund, B. R., Orbeck, A. L., & Landro, N. I. (1992). Vigilancedeficits in schizophrenics and affectively disturbed patients. ActaPsychiatrica Scandinavica, 86, 207-212.
*Russell, A. J., Cullum, C. M., Jones, P. B., Hemsely, D. R., &Murray, R. M. (1997). Schizophrenia and the myth of intellectualdecline. American Journal of Psychiatry, 154, 635-639.
*Russell, P. N., Consedine, C. E., & Knight, R. G. (1980). Visualand memory search by process schizophrenics. Journal ofAbnormal Psychology, 89, 109-114.
*Saccuzzo, D. P., & Braff, D. L. (1980). Associative cognitivedysfunction in schizophrenia and old age. The Journal ofNervous and Mental Disease, 168, 41—45.
*Sagawa, K., Kawakatsu, S., Komatani, A., & Totsuka, S. (1990).Frontality, laterality, and cortical-subcortical gradient of cerebralblood flow in schizophrenia: Relationship to symptoms andneuropsychological functions. Neuropsychobiology, 24, 1-7.
*Salovay, M. R., Shenton, M. E., & Holzman, P. S. (1987).
Comparative studies of thought disorders in mania and schizo-phrenia. Archives of General Psychiatry, 44, 13—20.
*Sasi, P. T., & Srivastava, A. (1992). Neurocognitive impairment inpositive and negative schizophrenia. Psychological Studies, 37,
47-56.*Saykin, A. J., Gur, R. C., Gur, R. E., Mozley, P. D., Mozley, L. H.,
Resnick, S. M., Kester, D. B., & Stafiniak, P. (1991). Neuropsycho-logical function in schizophrenia: Selective impairment in memoryand learning. Archivesof General Psychiatry, 48, 618-624.
*Saykin, A. J., Shtasel, D. L., Gur, R. E., Kester, B., Mozley, L. H.,Stafiniak, P., & Gur, R. C. (1994). Neuropsychological deficits inneuroleptic naive patients with first-episode schizophrenia. Ar-chives of General Psychiatry, 51, 124-131.
*Scarone, S., Abbruzzese, M., & Gambini, O. (1993). The Wiscon-sin Card Sorting Test discriminates schizophrenic patients andtheir siblings. Schizophrenia Research, 10, 103-107.
*Schmand, B., Brand, N., & Kuipers, T. (1992). Procedurallearning of cognitive and motor skills in psychotic patients.Schizophrenia Research, 8, 157-170.
Schmidt, F. L. (1996). Statistical significance testing and cumula-
tive knowledge in psychology: Implications for training ofresearchers. Psychological Methods, 1, 115—129.
*Schneider, S. G., & Asarnow, R. F. (1987). A comparison ofcognitive/neuropsychological impairments of nonretarded autis-tic and schizophrenic children. Journal of Abnormal ChildPsychology, 15, 29^6.
*Schwartz, B., Deutsch, L. H., Cohen, C., Warden, D., Deutsch,S. I. (1991). Memory for temporal order in schizophrenia.Biological Psychiatry, 29, 329-339.
*Schwartz, B., Rosse, R. B., Veazey, C., & Deutsch, S. I. (1996).
Impaired motor skill learning in schizophrenia: Implications forcoru'costrialal dysfunction. Comprehensive Psychiatry, 39, 241-248.
*Schwartz, B., Winstead, D. K., & Adinoff, B. (1983). Temporal
integration deficit in visual information processing by chronicschizophrenics. Biological Psychiatry, 18, 1311-1320.
Schwartz, F, Carr, A., Munich, R. L., & Bartuch, E. (1990).
Voluntary motor performance in psychotic disorders. Psychologi-cal Reports, 66, 1223-1234.
Scab, J. P., Jagust, W. J., Wong, S. T., Roos, M. S., Reed, B. R., &Budinger, T. F. (1988). Quantitative NMR measurement ofhippocampal atrophy in Alzheimer's disease. Magnetic Reso-nance in Medicine, 8, 200-208.
*Seidman, L. J., Oscar-Berman, M., Kalinowski, A. G., Ajilore, O.,Kremen, W. S., Faraone, S. V., & Tsuang, M. T. (1995).
Experimental and clinical neuropsychological measures of pre-frontal dysfunction in schizophrenia. Neuropsychology, 9, 481-490.
*Seidman, L. J., Pepple, J. R., Faraone, S. V., Kremen, W. S.,
Green, A. L, Brown, W. A., & Tsuang, M. T. (1993). Neuropsy-chological performance in chronic schizophrenia in response toneuroleptic dose reduction. Biological Psychiatry, 33, 575-584.
*Seidman, L. J., Talbat, N. L., Kalinowski, A. G., McCarley, R. W.,Faraone, S. V, Kremen, W. S., Pepple, J. R., & Tsuang, M. T.(1992). Neuropsychological probes of fronto-limbic systemdysfunction in schizophrenia: Olfactory identification and Wis-consin Card Sorting performance. Schizophrenia Research, 6,55-65.
*Sengal, R. A., & Lovallo, W. R. (1983). Effects of cueing onimmediate and recent memory in schizophrenia. The Journal ofNervous and Mental Disease, 171, 426-430.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.

444 HEINRICHS AND ZAKZANIS
*Sereno, A. B., & Holzman, P. S. (1996). Spatial selective attention
in schizophrenic, affective disorder, and normal subjects. Schizo-
phrenia Research, 20, 33-50.
*Shenton, M. E., Kikinis, R., McCarley, R. W., Metcalf, D.,
Tieman, J., & Jalesz, F. A. (1991). Application of automated
MRI volumetric measurement techniques to the ventricular
system in schizophrenics and normal controls. Schizophrenia
Research, 5, 103-113.
Shipley, W. C. (1946). Institute of Living Scale. Los Angeles:
Western Psychological Services.
*Shoqeirat, M. A., & Mayes, A. R. (1988). Spatiotemporal memory
and rate of forgetting in acute schizophrenics. Psychological
Medicine, 18, 843-853.
*Solomon, C. M., Holyman, P. S., Levin, S., & Gale, H. J. (1987).
The association between eye-tracking dysfunction and thought
disorder in psychosis. Archives of General Psychiatry, 44,
31-35.
*Slaghuis, W. L., & Bakker, V. J. (1995). Forward and backward
visual masking of contour by light in positive and negative symptom
schizophrenia. Journal of Abnormal Psychology, 104,41-54.
*Sonobe, N. (1993). Eye movements, verbal material recall and
negative symptoms in chronic schizophrenia. International
Journal of Psychophysiology, 15, 73-78.
•Souza, V. B. N., Muir, W. i., Walker, M. T., Glabus, M. F.,
Roxborough, H. M., Sharp, C. W., Dunan, J. R., & Blackwood,
D. H. R. (1995). Auditory P300 event-related potentials and
neuropsychological performance in schizophrenia and bipolar
affective disorder. Biological Psychiatry, 37, 300-310.
Spohn, H. E., & Strauss, M. E. (1989). Relation of neuroloeptic and
anticholinergic medication to cognitive functions in schizophre-
nia. Journal of Abnormal Psychology, 98, 367-380.
SPSS, Inc. (1990). SPSS reference guide. Chicago: Author.
*Stirling, J. D., Helkwell, J. S. E., & Hewitt, J. (1997). Verbal
memory impairment in schizophrenia: No sparing of short term
recall. Schizophrenia Research, 25, 85-95.
*Strandburg, R. 1, Marsh, J. T., Brown, W. S., Asarnow, R. F.,
Guthrie, D., & Higa, J. (1990). Event-related potential correlates
of impaired attention in schizophrenic children. Biological
Psychiatry, 27, 1103-1115.
Straube, E. R., & Oades, R. D. (1992). Schizophrenia: Empirical
research and findings. San Diego, CA: Academic Press.
Stroop, J. R. (1935). Studies of interference in serial verbal
reactions. Journal of Experimental Psychology, IS, 643-662.
*Stuss, D. T., Benson, D. F., Kaplan, E. E, Weir, W. S., Naeser,
M. A., Liberman, I., & Ferrill, D. (1983). The involvement of
orbitofrontal cerebrum in cognitive tasks. Neuropsychologia, 21,
235-248.*Sullivan, E. V, Mathalon, D. H., Ha, C. N., Zipursky, R. B., &
Pfefferbaum, A. (1992). The contribution of constructional
accuracy and organizational strategy to nonverbal recall in
schizophrenia and chronic alcoholism. Biological Psychiatry,
32, 312-333.*Sullivan, E. V., Mathalon, D. H., Zipursky, R. B., Kersteen-
Tucker, Z., Knight, R. T., & Pfefferbaum, A. (1993). Factors of
the Wisconsin Card Sorting Test as measures of frontal-lobe
function in schizophrenia and in chronic alcoholism. Psychiatry
Research, 46, 175-199.
•Sullivan, E. V., Shear, P. K., Lim, K. O., Zipursky, R. B., &
Pfefferbaum, A. (1996). Cognitive and motor impairments are
related to gray matter volume deficits in schizophrenia. Compre-
hensive Psychiatry, 39, 234-240.*Sullivan, E. V., Shear, P. K., Zipursky, R. B., Sagar, H. J., &
Pfefferbaum, A. (1997). Patterns of content, contextual, and
working memory impairments in schizophrenia and non amnesic
alcoholism. Neuropsychology, 11, 195-206.
Thornton, A. E., & Raz, N. (1997). Memory impairment in multiple
sclerosis: A quantitative review. Neuropsychology, 11, 357-366.
Tiffin, J. (1968). Purdue Pegboard examiner's manual. Rosemont,
IL: London House.
"Van den Bosch, R. J. (1984). Eye tracking impairment: Atten-
tional and psychometric correlates in psychiatric patients. Jour-
nal of Psychiatric Research, 18, 277-286.
*Van den Bosch, R. J., Rombouts, R. P., & van Asma, M. J. O.
(1996). What determines continuous performance task perfor-
mance? Schizophrenia Bulletin, 22, 643-651.
*Van den Bosch, R. J., van Asma, M. J. O., Rombouts, R., &
Lauwerlens, J. W. (1992). Coping style and cognitive dysfunc-
tion in schizophrenic patients. British Journal of Psychiatry, 161
(suppl. 18), 123-128.
Van der Does, A. W., & Van den Bosch, R. J. (1992). What
determines Wisconsin Card Sorting performance in schizophre-
nia? Clinical Psychology Review, 12, 567-583.
*Walker, E., & Marwit, S. J. (1980). A cross-sectional study of
emotion recognition in schizophrenics. Journal of Abnormal
Psychology, 89, 428^136.
Warrington, E. K. (1984). Recognition Memory Test, Windsor,
England: NFER-Nelson.
Wechsler, D. (1945). A standardized memory scale for clinical use.
Journal of Psychology, 19, 87-95.
Wechsler, D. (1981). Wechsler Adult Intelligence Scale—Revised
[Manual]. New York: The Psychological Corporation.
Wechsler, D. (1987). Wechsler Memory Scale manual. San Anto-
nio, TX: The Psychological Corporation.
Weinberger, D. R. (1995). The neurodevelopmental hypothesis of
schizophrenia. In S. R. Hirsch & D. R. Weinberger (Eds.),
Schizophrenia (pp. 293-323). Oxford, England: Blackwell Scien-
tific Publications.Weinberger, D. R., Wagner, R. L., & Wyatt, R. J. (1986).
Physiological dysfunction of dorsolateral prefrontal cortex in
schizophrenia I. Archives of General Psychiatry, 43, 114.
*Weiner, R. U., Opler, L. A., Kay, S. R., Merriam, A. E., &
Papouchis, N. (1990). Visual information processing in positive,
mixed, and negative schizophrenic syndromes. Journal of Ner-
vous and Mental Disease, 178, 616-626.
*Weiss, K. M., Chapman, H. A., Strauss, M. E., & Gilmore, G. C.
(1992). Visual information decoding deficits in schizophrenia.
Psychiatry Research, 44, 203-216.*Weiss, K. M., Vortunski, P. B., & Simpson, D. M. (1988).
Information overload disrupts digit recall performance in schizo-
phrenics. Schizophrenia Research, 1, 299-303.
*Wells, D. S., & Leventhal, D. (1984). Perceptual grouping in
schizophrenia: Replication of Place and Gilmore. Journal of
Abnormal Psychology, 93, 231-234.
White, H. D. (1994). Scientific communication and literature
retrieval. In H. Cooper & L. V. Hedges (Eds.), The handbook of
research synthesis. New York: Russell Sage Foundation.
*Williamson, P. C. (1989). Psychological, topographic EEG, and
CT scan correlates of frontal lobe function in schizophrenia.
Psychiatry Research, 29, 137-149.
Wolf, F. M. (1986). Meta-analysis: Quantitative methods for
research synthesis. Newbury Park, CA: Sage.
Wonderlic, E. F. (1978). Wonderlic Personnel Test manual. North-
field, IL: E. F. Wonderlic & Associates.
*Wood, F. B., & Flowers, D. L. (1990). Hypofrontal versus
hypo-sylvian blood flow in schizophrenia. Schizophrenia Bulle-
tin, 16, 413^24.
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.
NEUROCOGNmVE DEFICIT IN SCHIZOPHRENIA 445
Woodruff, P. W. R., McManus, I. C., & David, A. S. (1995).
Meta-analysis of corpus callosum size in schizophrenia. Journal
of Neurology, Neurosurgery and Psychiatry, 58, 457—461.
*Yates, W. R., Swaze, V. W., H, & Andreasen, N. C. (1990).
Neuropsychological effect of global and focal cerebral atrophy
in schizophrenia. Neuropsychiatry, Neuropsychology, and Behav-
ioral Neurology, 3, 98-106.
*Young, A. H., Blackwood, D. H. R., Roxborough, H., McQueen,
J. K.. Martin, M. J., & Kean, D. (1991). A magnetic resonance
imaging study of schizophrenia: Brain structure and clinical
symptoms. British Journal of Psychiatry, JS8, 158-164.
*Yurgelun-Todd, D. A., & Kinney, D. K. (1993). Patterns ofneuropsychological deficits that discriminate schizophrenic indi-viduals from siblings and control subjects. Journal ofNeuropsy-chiatry and Clinical Neurosciences, 5, 294-300.
Zakzanis, K. K., & Heinrichs, R. W. (1997). The frontal-executivehypothesis in schizophrenia: Cognitive and neuroimaging evi-dence. The Clinical Neuropsychologist, 11, 33.
*Zipursky, R. B., Marsh, L., Lim, K. O., DeMent, S., Shear, P. K.,Sullivan, E. V., Murphy, G. M., Csernansky, J. G., & Pfeffer-baum, A. (1994). Volumetric MRI assessment of temporallobe structures in schizophrenia. Biological Psychiatry, 35,502-516.
Appendix
Key Words Used in Computer Database Search
Schizophrenia MemorySchizophrenia California Verbal LearningSchizophrenia WechslerSchizophrenia Nonverbal MemorySchizophrenia Selective MemorySchizophrenia Global MemorySchizophrenia Verbal MemorySchizophrenia Complex FigureSchizophrenia Face RecognitionSchizophrenia Spatial PerceptionSchizophrenia Line Orientation
Schizophrenia TransferSchizophrenia PurdueSchizophrenia Motor DexteritySchizophrenia Finger TappingSchizophrenia Motor DisorderSchizophrenia StroopSchizophrenia Digit SpanSchizophrenia Continuous PerformanceSchizophrenia Backward MaskingSchizophrenia TrailsSchizophrenia Trail Making
Schizophrenia Wisconsin Card Sorting TestSchizophrenia IQSchizophrenia Verbal IQSchizophrenia Performance IQSchizophrenia VocabularySchizophrenia Block DesignSchizophrenia Word FluencySchizophrenia TokenSchizophrenia ComprehensionSchizophrenia Affect RecognitionSchizophrenia Dichotic Listening
Received May 5, 1997
Revision received October 15, 1997
Accepted October 20, 1997 i
This
doc
umen
t is c
opyr
ight
ed b
y th
e A
mer
ican
Psy
chol
ogic
al A
ssoc
iatio
n or
one
of i
ts a
llied
pub
lishe
rs.
This
arti
cle
is in
tend
ed so
lely
for t
he p
erso
nal u
se o
f the
indi
vidu
al u
ser a
nd is
not
to b
e di
ssem
inat
ed b
road
ly.


















