Neurobehaviour MS 2008 JAN
54
NEUROBEHAVIOR (BEHAVIORAL NEUROLOGY)
description
neurooo
Transcript of Neurobehaviour MS 2008 JAN

NEUROBEHAVIOR (BEHAVIORAL NEUROLOGY)

The Division of Cognitive and Behavioral Neurology :provides a comprehensive, multidisciplinary approach to the diagnosis and management of patients who have problems with memory, executive functions, attention, language, emotion, or behavior due to disease, injury, or developmental disorders of the central nervous system. Patients receive the highest standard of neurologic, psychiatric, and social work care for the treatment of their conditions.

in the assessment and treatment of diverse clinical problems including:
- Dementia (e.g., Alzheimer’s disease and related degenerative disorders, vascular dementia, frontotemporal dementia, dementia with -parkinsonism) - Cognitive, Emotional, or Behavioral Problems due
to Diverse Conditions (e.g., epilepsy, multiple sclerosis, stroke, traumatic brain injury, brain tumor, systemic diseases with central nervous system manifestations)
- Developmental Disorders in Adults (e.g., Attention deficit disorder, learning disabilities, mental
retardation,autism)

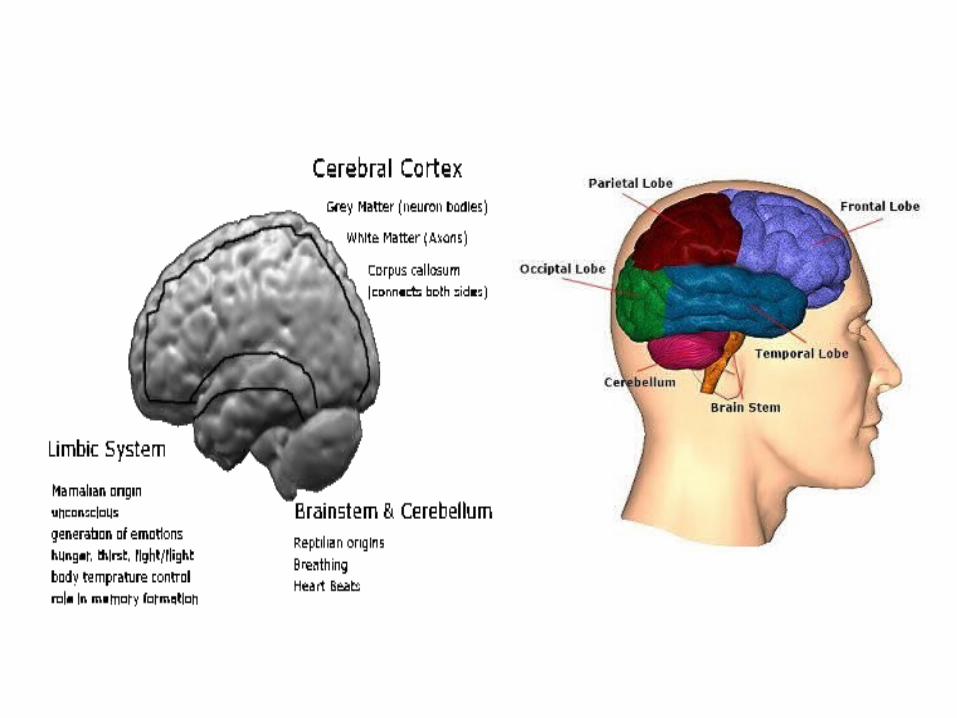
Basic brain biologyA simplified model of the human brain consists of many parts:- Brain stem, hind brain, mid brain & cerebellum -
the most ancient parts, connected to the spine, controls movement, breathing and heartbeats.
- Limbic system - consisting of many specialist organs including the Hypothalamus,
hippocampus -developed in mammals. Some memory functions and generation of emotional responses. - Cerebral cortex - the distinguishing feature of
human brains

• Each hemisphere of the cortex can further be divided into four lobes:
• Occipital - visual processing
• Parietal - movement, orientation, calculation, recognition
• Temporal - sound and speech processing, aspects of memory
• Frontal - thinking, conceptualisation, planning.

Some specific differences between the two hemispheres resulted from this and subsequent research. The right-brain is better at:
Right HemisphereLeft Hemisphere
Specialities•Copying of designs, •Discrimination of shapes e.g. picking out a camouflaged object, •Understanding geometric properties, •Reading faces, •Music, •Global holistic processing, •Understanding of metaphors, •Expressing emotions, •Reading emotions.
•Language skills, •Skilled movement, •Analytical time sequence processing.
Shared•Sensations on both side of face, •Sound perceived by both ears, •Pain, •Hunger, •Position.
Emotions Negative emotions (fearful mournful feelings), Positive emotions
neurotransmitters Higher levels of norepinephrine Higher levels of dopamine
Grey Matter White Maatter ratio
More white-matter (longer axons) on rightmore grey-matter (cell bodies) on the left

SIRKUIT AMIGDALASIRKUIT AMIGDALA ( LINTASAN EMOSI )( LINTASAN EMOSI )
dengan bagian Otak laindengan bagian Otak lain
Striatum ventral, nukleus dorsomedial thalamus
Hipokampus
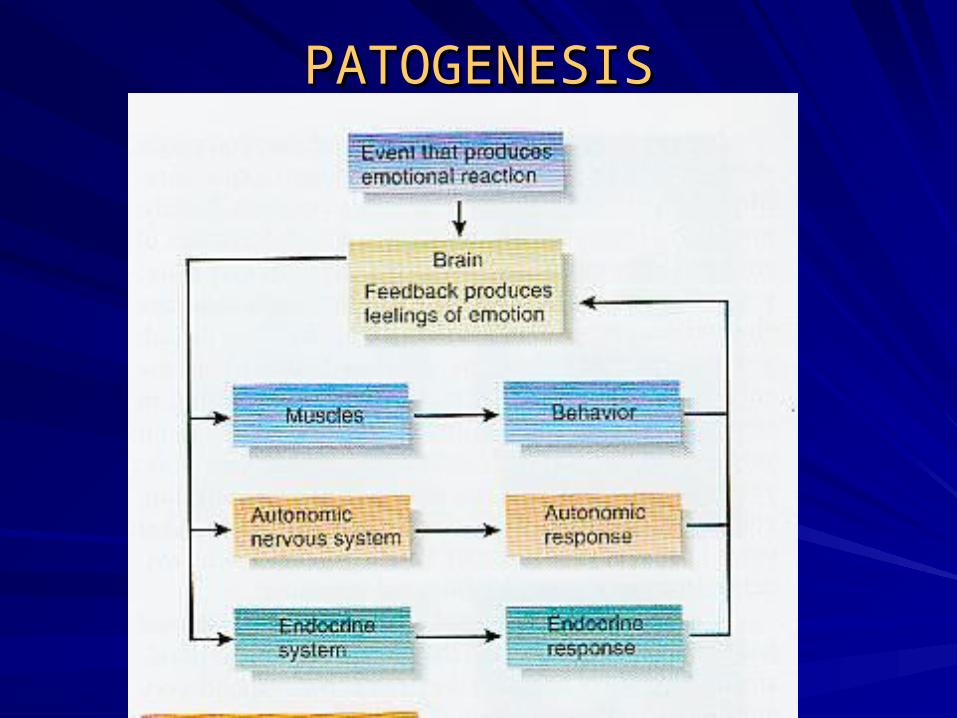
PATOGENESISPATOGENESIS

RESPON TERHADAP EMOSI RESPON TERHADAP EMOSI DARI BAGIAN-BAGIAN OTAK DARI BAGIAN-BAGIAN OTAK AKIBAT STIMULUS NUKLEUS AKIBAT STIMULUS NUKLEUS SENTRALIS AMIGDALASENTRALIS AMIGDALA

GAMBARAN fMRI pasien depresi :GAMBARAN fMRI pasien depresi :
penurunan aktifitas metabolik daerah prefrontalpenurunan aktifitas metabolik daerah prefrontal

GAMBARAN PET Scan : Peningkatan aktifitas amigdala pada orang yang melihat kata-kata ancaman

DEMENTIADEMENTIA
DEFINITION:DEFINITION:– Group of symptoms that can be caused by Group of symptoms that can be caused by
over 60-70 disorders.over 60-70 disorders.– Syndrome which refers to progressive Syndrome which refers to progressive
decline in intellectual functioning severe decline in intellectual functioning severe enough to interfere with person’s normal daily enough to interfere with person’s normal daily activities and social relationships. (activities and social relationships. (National National Institute on Aging-1995 No. 95-3782)Institute on Aging-1995 No. 95-3782)
DementiaDementia– Marked by progressive, irreversible Marked by progressive, irreversible
declines in declines in memory. memory.
visual-spatial relationshipsvisual-spatial relationships
performance of routine tasksperformance of routine tasks
language and communication skillslanguage and communication skills
abstract thinkingabstract thinking
ability to learn and carry out mathematical ability to learn and carry out mathematical calculations.calculations.
DementiaDementiaTwo Types:Two Types:– ReversibleReversible– IrreversibleIrreversible
Individuals must have intensive medical Individuals must have intensive medical physical to rule out reversible types of physical to rule out reversible types of dementia.dementia.

DementiaDementia
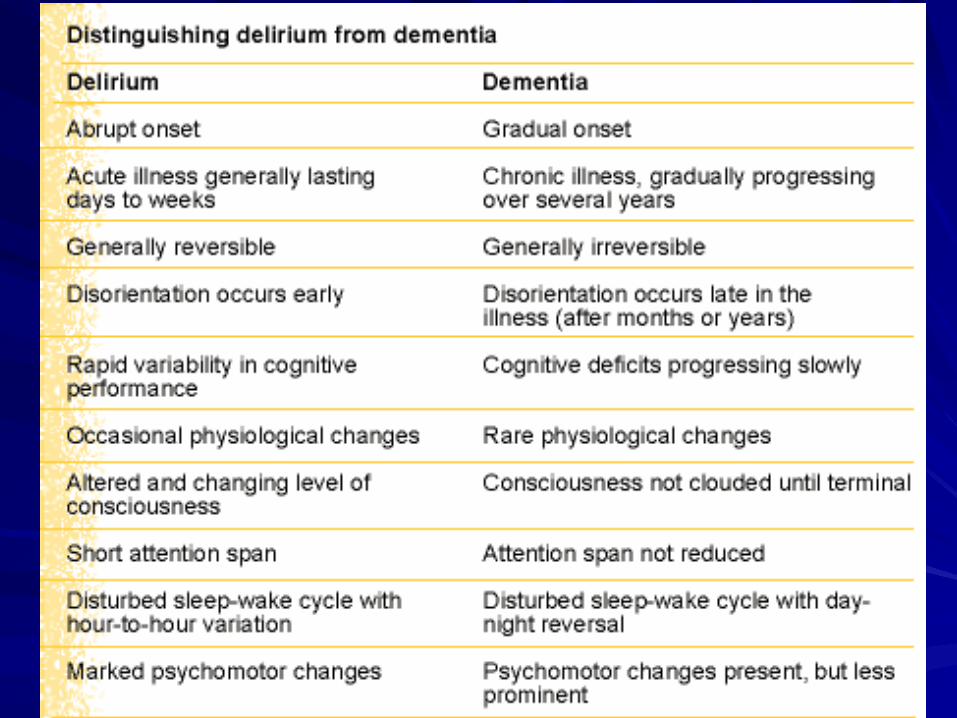
Reversible:Reversible:– D= D= Drugs, DeliriumDrugs, Delirium– E=E= Emotions (such as depression) and Emotions (such as depression) and
Endocrine DisordersEndocrine Disorders– M=M= Metabolic DisturbancesMetabolic Disturbances– E=E= Eye and Ear ImpairmentsEye and Ear Impairments– N=N= Nutritional DisordersNutritional Disorders– T=T= Tumors, Toxicity, Trauma to HeadTumors, Toxicity, Trauma to Head– I=I= Infectious DisordersInfectious Disorders– AA Alcohol, Arteriosclerosis Alcohol, Arteriosclerosis (Dick-Mulheke- Overview of (Dick-Mulheke- Overview of
Alzheimer's Disease)Alzheimer's Disease)

DementiaDementiaIrreversible:Irreversible:– Alzheimer’sAlzheimer’s– Lewy Body DementiaLewy Body Dementia– Pick’s Disease (Frontotemperal Dementia)Pick’s Disease (Frontotemperal Dementia)– Parkinson’sParkinson’s– Heady InjuryHeady Injury– Huntington’s DiseaseHuntington’s Disease– Jacob-Cruzefeldt DiseaseJacob-Cruzefeldt Disease
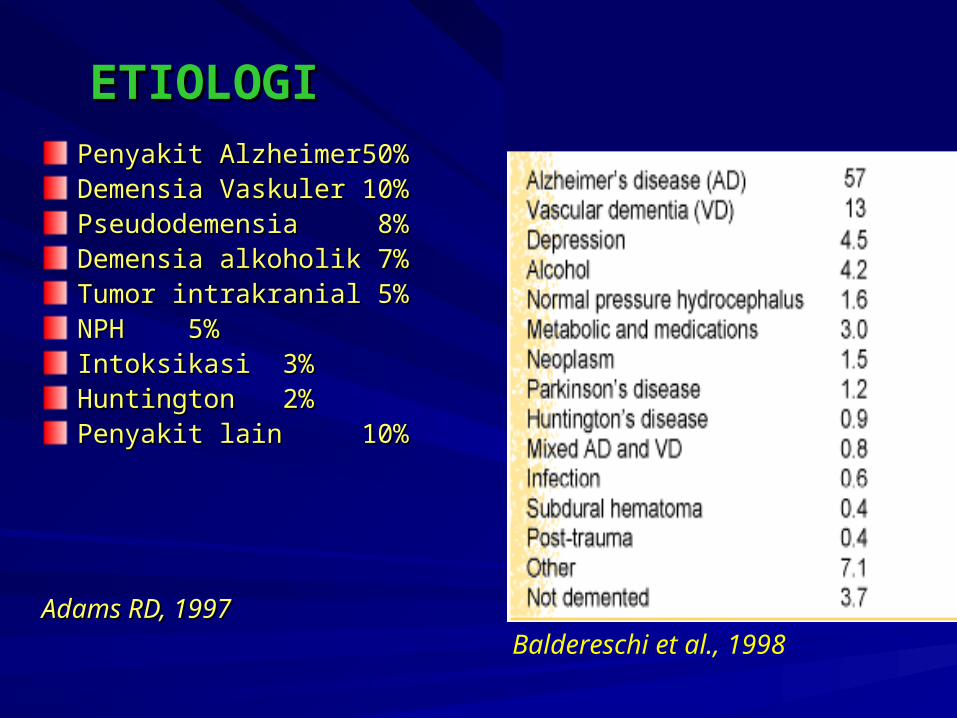
ETIOLOGIETIOLOGIPenyakit AlzheimerPenyakit Alzheimer 50%50%Demensia VaskulerDemensia Vaskuler 10%10%PseudodemensiaPseudodemensia 8% 8%Demensia alkoholikDemensia alkoholik 7% 7%Tumor intrakranialTumor intrakranial 5% 5%NPHNPH 5% 5%IntoksikasiIntoksikasi 3% 3%HuntingtonHuntington 2% 2%Penyakit lainPenyakit lain 10%10%
Adams RD, 1997Adams RD, 1997
Baldereschi et al., 1998

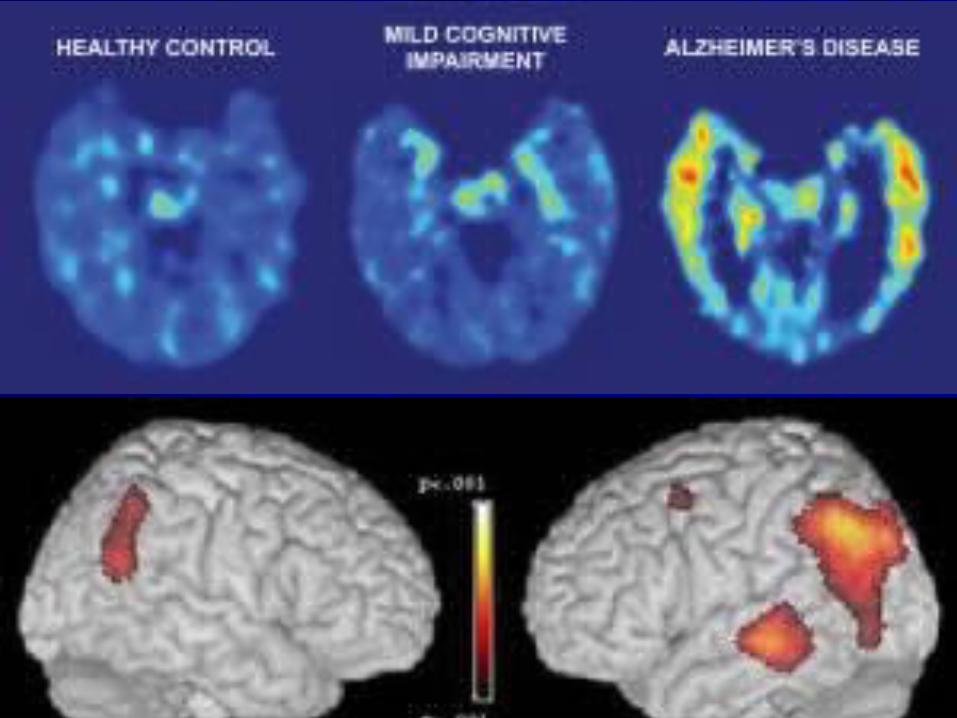
Progression of normal aging to dementiaProgression of normal aging to dementia
NormalNormal Brain AgingBrain AgingCognitionCognition
stable orstable orProdromal Prodromal reversrevers MCI MCI reversible reversibleDementiaDementia impairment impairment
otherother Alzheimer’s Alzheimer’s vascular vascularDementia dementiaDementia dementia diseasedisease dementia dementia
Golomb J,Kluger A,Ferris SH, 1999Golomb J,Kluger A,Ferris SH, 1999
MCI / VCIstable or reversible
impairment
other dementia
Alzheimerdementia
vasculardementia

•Alzheimer's DiseaseAlzheimer's Disease Estimated that 4,000,000 people in U.S. Estimated that 4,000,000 people in U.S. have Alzheimer's disease.have Alzheimer's disease.Estimated that 25-35% of people over age Estimated that 25-35% of people over age 85 have some time of dementia.85 have some time of dementia.After age 65 the percentage of affected After age 65 the percentage of affected people, doubles with every decade of life.people, doubles with every decade of life.Caring for patient with Alzheimer's disease Caring for patient with Alzheimer's disease can cost $47,000 per year can cost $47,000 per year (NIH).(NIH).

Changes Caused by Changes Caused by Alzheimer'sAlzheimer's
Diminished blood flowDiminished blood flow
Neurofibrillary TanglesNeurofibrillary Tangles
Neuritic PlaquesNeuritic Plaques
Degeneration of hippocampus, cerebral Degeneration of hippocampus, cerebral cortex, hypothalamus, and brain stemcortex, hypothalamus, and brain stem


Theories Regarding Causes of Theories Regarding Causes of Alzheimer'sAlzheimer's
Changes in NeurotransmittersChanges in NeurotransmittersAcetycholine is decreased--necessary for Acetycholine is decreased--necessary for cognitive functioning.cognitive functioning.
Changes in Protein SynthesisChanges in Protein SynthesisBeta amyloid--may be responsible for forming Beta amyloid--may be responsible for forming plaques.plaques.
Tau--major component of neurofibrillary tangles.Tau--major component of neurofibrillary tangles.
Genetic TheoriesGenetic TheoriesApoE4 on chromosone 19 linked to late-onset ApoE4 on chromosone 19 linked to late-onset Alzheimer’s Disease.Alzheimer’s Disease.

Theories Regarding Causes of Theories Regarding Causes of Alzheimer'sAlzheimer's
Genetic TheoriesGenetic TheoriesChromosome 21 --Responsible for early-onset Chromosome 21 --Responsible for early-onset Alzheimer’s Disease.Alzheimer’s Disease.
Metabolic TheoriesMetabolic TheoriesGlucose metabolism declines dramatically in Glucose metabolism declines dramatically in Alzheimer’s patients.Alzheimer’s patients.
Calcium TheoriesCalcium TheoriesToo much calcium can kill cells. Suspect that it Too much calcium can kill cells. Suspect that it may reason why neurons die in Alzheimer's may reason why neurons die in Alzheimer's patients.patients.

Theories Regarding Causes of Theories Regarding Causes of Alzheimer'sAlzheimer's
EnvironmentalEnvironmentalAluminum--Traces of metal found in brain.Aluminum--Traces of metal found in brain.
Zinc--found in brains on autopsies.Zinc--found in brains on autopsies.
Food borne poisons--amino acids found in Food borne poisons--amino acids found in legumes in Africa and India my cause neurological legumes in Africa and India my cause neurological damage.damage.
ViralViralMay be hidden in body and attack brain cells years May be hidden in body and attack brain cells years later. (later. (NIH-1995)NIH-1995)

Theories Regarding Causes of Theories Regarding Causes of Alzheimer'sAlzheimer's
Head TraumaHead Trauma– Head trauma increase the concentration of B-amyloid Head trauma increase the concentration of B-amyloid
proteinprotein
Low Level of EducationLow Level of Education– Individuals with low level of education less able to Individuals with low level of education less able to
compensate for cognitive deficitscompensate for cognitive deficits
Estrogen DeficiencyEstrogen Deficiency
Early Life Experience---have lost parent before Early Life Experience---have lost parent before age 16age 16

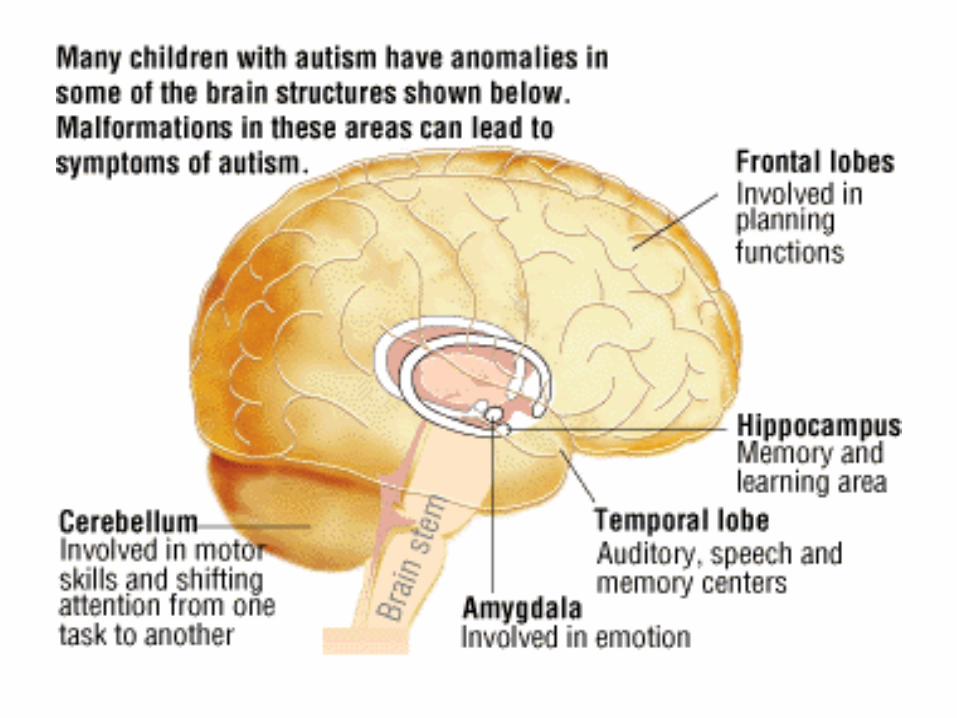
The Cholinergic HypothesisThe Cholinergic HypothesisAcetylcholine is as important neurotransmitter Acetylcholine is as important neurotransmitter in areas of the brain involved in memory in areas of the brain involved in memory formation – the hippocampus, cerebral cortex, formation – the hippocampus, cerebral cortex, and amygdala.and amygdala.
Concentrations of acetylcholine are markedly Concentrations of acetylcholine are markedly decreased in Alzheimer’s disease.decreased in Alzheimer’s disease.
Enhancement or restoration of cholinergic Enhancement or restoration of cholinergic function may significantly reduce the severity function may significantly reduce the severity of cognitive loss.of cognitive loss.
Depletion is limited to the basal forebrain Depletion is limited to the basal forebrain projection system.projection system.

Gauthier at all, 1997

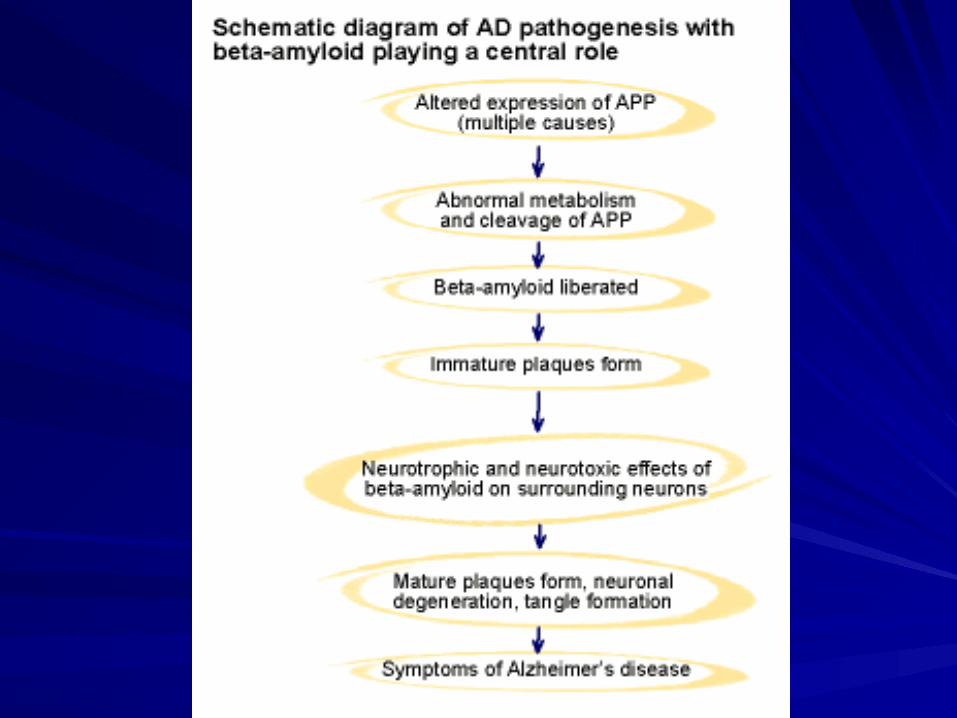
Neuronal DegenerationNeuronal Degeneration
The pathobiology of Alzheimer’s The pathobiology of Alzheimer’s disease is characterized by:disease is characterized by:
Amyloid plaquesAmyloid plaques
Neurofibrillary tanglesNeurofibrillary tangles

Neurofibrillary TanglesNeurofibrillary Tangles
Intracellular inclusion bodies consisting of Intracellular inclusion bodies consisting of paired helical filaments that appear in a paired helical filaments that appear in a characteristic double-helix shape.characteristic double-helix shape.Filaments appear to be composed of a Filaments appear to be composed of a hyperphosphorylated microtubule-hyperphosphorylated microtubule-associated protein called associated protein called tautau. . Remains of damaged neuronal Remains of damaged neuronal microtubules.microtubules.

Amyloid PlaquesAmyloid Plaques
Plaques are extracellular structures that are Plaques are extracellular structures that are more prevalent in the Alzheimer’s patient’s more prevalent in the Alzheimer’s patient’s brain, particularly in the hippocampus and brain, particularly in the hippocampus and neocortex.neocortex.
Amyloid (neuritic) plaques in Alzheimer’s Amyloid (neuritic) plaques in Alzheimer’s disease are dense and insoluble structures.disease are dense and insoluble structures.
Plaques consist of a central core of beta-Plaques consist of a central core of beta-amyloid protein surrounded by abnormal amyloid protein surrounded by abnormal axons and dendrites.axons and dendrites.



Diagnosis of Dementia Due to Diagnosis of Dementia Due to Alzheimer’sAlzheimer’s
Memory ImpairmentMemory Impairment
Multiple cognitive deficits with at least one Multiple cognitive deficits with at least one disturbance in the following areas:disturbance in the following areas:– Aphasia—loss of the ability to use symbols to Aphasia—loss of the ability to use symbols to
communicate orally or in writingcommunicate orally or in writingTwo Types:Two Types:
– Expressive—inability to form wordsExpressive—inability to form words– Receptive—decreased ability to understand spoken or Receptive—decreased ability to understand spoken or
written languagewritten language
– Apraxia—inability to initiate complex learned motor Apraxia—inability to initiate complex learned motor movement or unable to perform activity on movement or unable to perform activity on command command
– Agnosia---inability to recognize familiar objects by Agnosia---inability to recognize familiar objects by sight, touch, taste, smell or soundsight, touch, taste, smell or sound

Diagnostic TestsDiagnostic Tests
Neurological ExamNeurological Exam
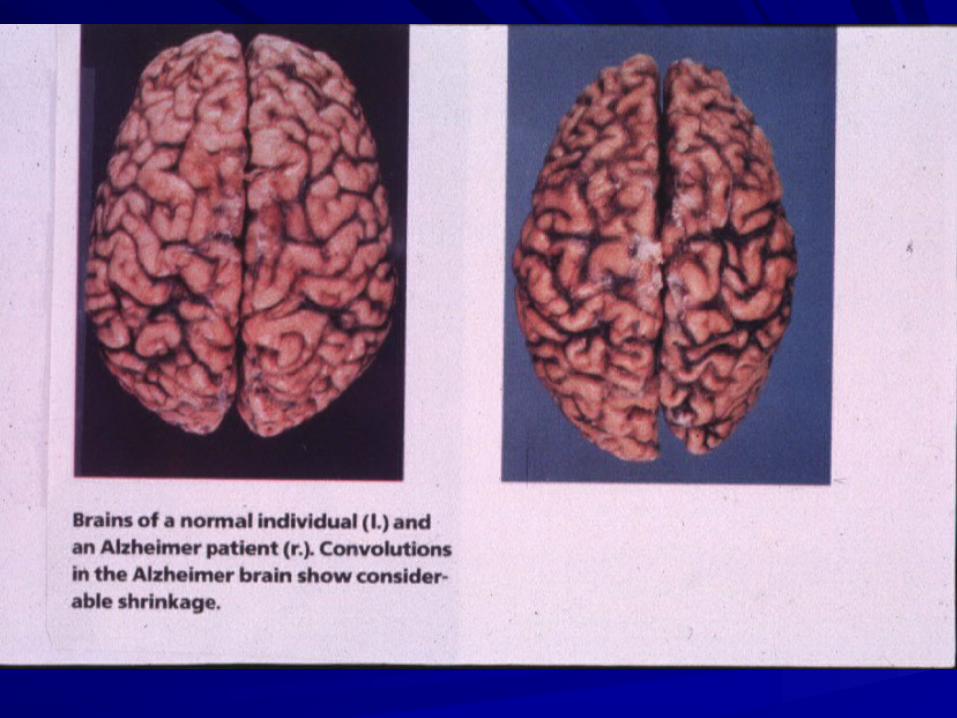
Brain Imaging—shrinkage, atrophy of Brain Imaging—shrinkage, atrophy of brain (CT or MRI)brain (CT or MRI)
Blood WorkBlood Work
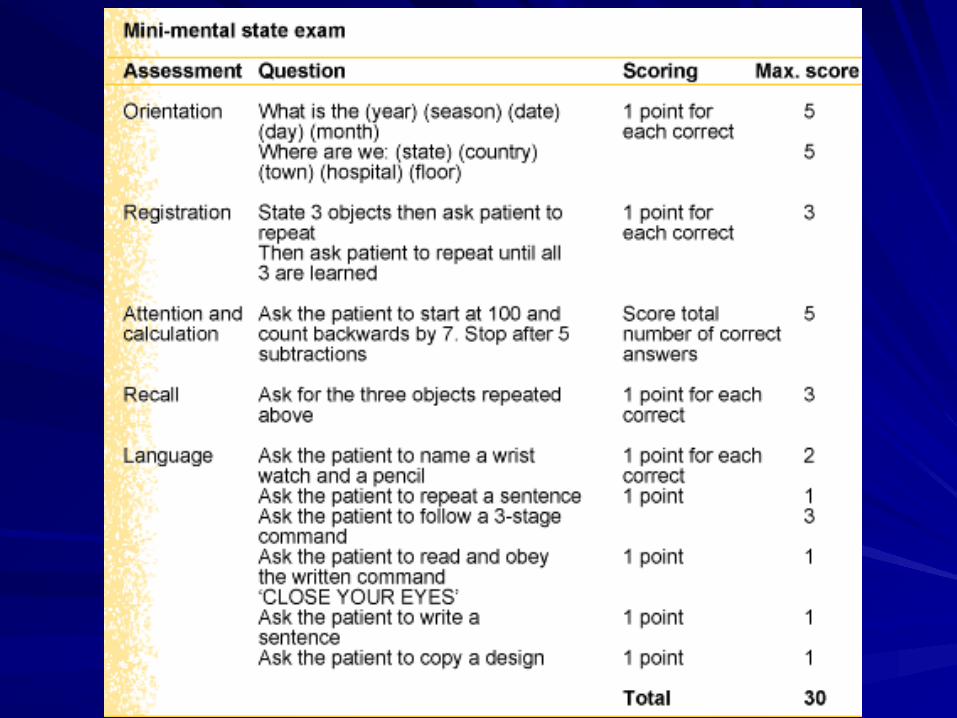

Median Scores on Mini-Mental State ExaminationMedian Scores on Mini-Mental State Examination by Age and Educational Levelby Age and Educational Level
Age (years)Age (years)Educational levelEducational level
44thth grade grade 88thth grade grade High schoolHigh school CollegeCollege
18 to 2418 to 24 2222 2727 2929 2929
25 to 2925 to 29 2525 2727 2929 2929
30 to 3430 to 34 2525 2626 2929 2929
35 to 3935 to 39 2323 2626 2828 2929
40 to 4440 to 44 2323 2727 2828 2929
45 to 4945 to 49 2323 2626 2828 2929
50 to 5450 to 54 2323 2727 2828 2929
55 to 5955 to 59 2323 2626 2828 2929
60 to 6460 to 64 2323 2626 2828 2929
65 to 6965 to 69 2222 2626 2828 2929
70 to 7470 to 74 2222 2525 2727 2828
75 to 7975 to 79 2121 2525 2727 2828
80 to 8480 to 84 2020 2525 2525 2727
8484 1919 2323 2626 2727
Reprinted with permisssion from Crum RM, Anthony JC, Basset SS, Folstein MF. Population-based norms for the mini-mental state examination by age and educational level. JAMA 1993 ; 18 : 2386-91




Stages of Alzheimer’s DiseaseStages of Alzheimer’s Disease
Mild StageMild Stage– Memory LossMemory Loss– Symptoms:Symptoms:
Confusion About PlaceConfusion About Place
Loss of SpontaneityLoss of Spontaneity
Loss of InitiativeLoss of Initiative
Mood/Personality ChangesMood/Personality Changes
Poor JudgmentPoor Judgment
Takes Longer to Perform Routine choresTakes Longer to Perform Routine chores
Trouble Handling Money, Paying BillsTrouble Handling Money, Paying Bills
Stages of Alzheimer’s DiseaseStages of Alzheimer’s Disease
Moderate StageModerate StageImpairments in:Impairments in:
languagelanguage
motor abilitymotor ability
object recognitionobject recognition
increasing memory loss and confusionincreasing memory loss and confusion
Stages of Alzheimer’s DiseaseStages of Alzheimer’s DiseaseModerate StageModerate Stage– Symptoms:Symptoms:
PProblems recognizing family members, close friends.roblems recognizing family members, close friends.
Repetitive statements and/or movements.Repetitive statements and/or movements.
Restless, especially in late afternoon and at night.Restless, especially in late afternoon and at night.
Occasional muscle twitches or jerking.Occasional muscle twitches or jerking.
Perceptual motor problems.Perceptual motor problems.
Problems organizing thoughts, thinking logically.Problems organizing thoughts, thinking logically.
Can’t find right words, makes up stories.Can’t find right words, makes up stories.
Problems reading and writing.Problems reading and writing.
May be suspicious, irritable, fidgety, teary or silly.May be suspicious, irritable, fidgety, teary or silly.
Stages of Alzheimer’s DiseaseStages of Alzheimer’s Disease
Severe StageSevere Stage– Symptoms:Symptoms:
Loses weight even with good diet.Loses weight even with good diet.
Little capacity for self-care.Little capacity for self-care.
Can’t communicate with words.Can’t communicate with words.
May put everything in mouth or touch everything.May put everything in mouth or touch everything.
Can’t control bladder or bowel.Can’t control bladder or bowel.
May have difficult with seizures, swallowing, skin May have difficult with seizures, swallowing, skin breakdown, infections.breakdown, infections.

Stages of Alzheimer’s DiseaseStages of Alzheimer’s DiseaseTerminal StageTerminal Stage– Symptoms:Symptoms:
Loss of ability to ambulate.Loss of ability to ambulate.
Loss of ability to sit.Loss of ability to sit.
Loss of ability to smile.Loss of ability to smile.
Loss of ability to hold up head.Loss of ability to hold up head.
Loss of ability to swallow. Loss of ability to swallow.

Stages of Alzheimer’s DiseaseStages of Alzheimer’s DiseaseStage IV--Terminal StageStage IV--Terminal Stage– Symptoms:Symptoms:
Loss of ability to ambulate.Loss of ability to ambulate.Loss of ability to sit.Loss of ability to sit.Loss of ability to smile.Loss of ability to smile.Loss of ability to hold up head.Loss of ability to hold up head.Loss of ability to swallow. Loss of ability to swallow.
Management of Challenging Behaviors in Dementia—Mahoney, Volicer, Hurley. Management of Challenging Behaviors in Dementia—Mahoney, Volicer, Hurley.
Health Professionals Press:2000. Baltimore, MdHealth Professionals Press:2000. Baltimore, Md..
Potential agents that can be of Potential agents that can be of benefit for Alzheimer’s diseasebenefit for Alzheimer’s disease
Reversible inhibitors of the enzyme Reversible inhibitors of the enzyme acetylcholinesterase (donepezil, tacrine, acetylcholinesterase (donepezil, tacrine, rivastigmine)rivastigmine)?Vitamin E 2000 IU units per day - 6 ?Vitamin E 2000 IU units per day - 6 month delay in disease progressionmonth delay in disease progression?Selegiline 5 mg twice a day - 4 month ?Selegiline 5 mg twice a day - 4 month delay in disease progressiondelay in disease progression?Gingko biloba – 40 mg tid?Gingko biloba – 40 mg tid