Neubrander ASD03-Web Copy

of 11
-
Upload
jumabarrientos -
Category
Documents
-
view
215 -
download
0
Transcript of Neubrander ASD03-Web Copy
-
7/28/2019 Neubrander ASD03-Web Copy
1/11
-
7/28/2019 Neubrander ASD03-Web Copy
2/11
Qeeg-guidedneurofeedBAck:
new BrAin-BAsedindividuAlized evAluAtionAnd treAtment for Autism
By JaMES NEuBRaNdER, Md,1 MIChaEl lINdEN, Phd,2
Jay guNkElMaN, QEEgd,3,4 aNd CyNhIa kERSON, Phd 3,5,6
Afiai:1 Road to Recovery Clinic, Iselin, NJ. 2 Attention Learning Center, San Juan Capistrano, CA. 3 Brain ScienceInternational, Pleasanton, CA. 4 Behavioral Medicine Research and Training Foundation, Port Angeles, WA.5 Marin Biofeedback, San Rafael, CA. 6 ISNR Research Foundation, San Rafael, CA.
QEEG-guided neuroeedback is based on normalizing dysregulated brain regions that relate to specifc clinical presentation. With ASD, thismeans that the approach is specifc to each individuals QEEG subtype patterns and presentation. The goal o neuroeedback with ASD is to
correct amplitude abnormalities and balance brain unctioning, while coherence neuroeedback aims to improve the connectivity and plasticitybetween brain regions. This tailored approach has implications that should not be underestimated. . . . Clinicians, including the authors, havehad amazing results with ASD, including signifcant speech and communication improvements, calmer and less aggressive behavior, increasedattention, better eye contact, and improved socialization. Many of our patients have been able to reduce or eliminate their medications aftercompletion o QEEG-guided neuroeedback.
prEfAcE
Prents o ciren wit tism now me ( JN) s psicin wo ses rios biomeic tretmentsto ep ciren moe towr recoer. Seerers o, I ws introce to te power
moit o QEEg-ie neroeebc. Tistretment ses EEg bioeebc, so nowns neroeebc, ie b te Q EEg, orqntittie eectroenceporm. Neroeebcs since become n importnt ition to mprctice becse it oers terpetic options tt renot possibe tro biomeic tretments one.
o te, I e obtine QEEgs on nres
o ciren wit tism n e wtce teneroeebc process ep tem te one or moresteps orwr on teir ros to recoer. Tt is wit peses me to e been se bAutism ScienceDigestto write tis rtice to introce QEEg n
QEEg-ie neroeebc or ciren wittism s one more importnt tretment option orprents to consier.
ato I e prescribe mn neroeebcsessions or m cients, I cnnot cim to be nexpert in QEEg interprettion. In tt rer,I eer to tose wo ete m ptients EEgtrcins n sbseqent recommen pproprite
neroeebc protocos tt m neroeebctecnicins ten impement. M cotors (Ml, Jn Ck), wose biorpies spe or temseesre some o te most respecte nmes in te eo QEEg n QEEg-ie neroeebc.
In tis pper, te proie n oeriew o tescience bein te process, teoretic ptorm,n n otine o te benets t is tretment cnoer to te mn ciren w o e ttention-ecit or ttention-ecit/perctiit isorer(add/adhd), asperers snrome, per sieeeopment isorer-not oterwise specie(Pdd-NOS), or tism spectrm isorer (aSd
I e obtine QEEgs on nres o ciren wit tism n e wtce te
neroeebc process ep tem te one or more steps orwr on teir ros to recoerwww.autsmone.org REPRINTED WITH PERMISSION AUTISM SCIENCE DIGEST: THE JOURNAL OF AUTISMONE ISSU
-
7/28/2019 Neubrander ASD03-Web Copy
3/11
-
7/28/2019 Neubrander ASD03-Web Copy
4/11
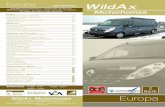
tabe 1. eeG frquncy bnds
Band Frequency Normal occurence Signifcance
Delta 0.5-3.5 Hz Deep sleep and inants Sign o signifcant brain dysunction, lethargy,
drowsiness, or cognitive impairment
Theta 3.5-7.5 Hz Young children, drowsiness, some
aspects o learning
Slowing oten related to attention/cognitive
impairments, internal ocus
Alpha 7.5-13 Hz Eyes closed, relaxat ion,
sel-awareness
Excessive alpha during demand states can be a sign
o learning difculties, emotional stability, or relating to
the environment or others
Beta 13-30 Hz Fast activity, associated with
alertness and activity
Excessive beta is oten associated with anxiety,
irritability, and poor integration
Gamma 30+ Hz Higher mental activity and
consolidation o inormation, possibly
with higher states o meditation
Possible cognitive decline
Sources: Demos JN. Getting Started with Neurofeedback. New York, NY: WW Norton, 2005; and Thompson M, Thompson L. The Neurofeedback Book. Wheatridge, CO:Association or Applied Psychophysiology and Bioeedback, 2003.
in ttention, impsiit, n perctiit ofenoccrre (linen et ., 1996). lbrs resercin te 1980s n 1990s rter inicte tt IQn continos perormnce test (CP) scoresincrese s rest o te neroeebc trinin(lbr et ., 1995). Moreoer, in 1995 lbr ncoees pbise onitin oow-pst tt inicte tt te positie rests romneroeebc were sti sinicnt or 15 ot o 16beiors fer 10 ers.
In 1996, linen n coees pbisete rst rnomize controe sty oneroeebc wit stents wit adhd.Teir rests spporte lbrs previos boy oreserc n i ite sinicnt improvementsin ttention n IQ scores compre wit wit is t contro rop. Oter rese rcers veon tt te eects o neroeebc onadhd re simir to te eects o stimntmeiction rin tretment bt persist fertretment is iscontine. or exmpe, Monstrn coees (2002) compre stimnt
meiction reime to neroeebc, wie soproviin prent trinin. Teir rests spportete sinicnt eects o neroeebc witadhd ciren n itiony sowe ttte eects were on-stin s compre witte temporry eects o meiction. cs ncoees (2003) concte simir comprison
bt se QEEg pttern nysis to eveop morespecic neroeebc protocos, incininibitin i bet (18-30 hz) ctivity. Teirneroeebc pproc te sme positiveeects s metypenite, wit simir sinicnteects on mtipe mesres; once in, owever,te meiction eects were ony temporry.
Mny o te more tn 30 ery stieson neroeebc n adhd ve beencriticize or cin eqte contros or vin
nsopisticte reserc esins. Recenty,owever, eccy or neroeebc tretmentws est bise concsi vey in met-n ysis ttsows tt neroeebc or adhd is boteccios n specic (arns et ., 2009).
quAntItAtIvE
ElEctroEncEphAlogrAm (qEEg)
Te EEg cn be mesre qntittivey. Tismens tt te brins ctivities cn be stiener ierent tss n evte rom more compreensive perspective. Te QEEg
tecniqes re qite sopisticte, invovinmeic evice mpiers n tbses osttistic iverences. accorin to Jonstonen gnemn (2003), QEEg nysis reers tosin processin n extrction o etres romte EEg sin (see ire 1, section 2). afer teeectric inormtion is processe, it is compre
to tbse o norm sbjects. Tese tbsesrey on sbjects wo ve been etermine normbse on stnr screenin toos or meic,psycooic, n bevior istory. Teseince interview n psycooic tests sc ste Minnesot Mtipsic Personity Inventor(MMPI), te lri-Nebrs NeropsycooiBttery (lNNB), te Wecser Inteience Scor Ciren (WISC), n oters.
acqirin te EEg sy t es bot one
to one n ors. Becse some aSdciren ve sensitivity isses, noweebeprctitioners vise prents to brin te ci tote cinic in vnce o te session to miirizeim or er wit te settin n c inicins. Teptient is instrcte to ws is or er ir priorto te cqisition (min sre tt it is r y by ttime o te procere) n to voi sin ny emosses, or sprys. drin te EEg recorin, 1cnnes wit es re set onto te ptients scwit conct ive pste. Norm y, te ptientsEEg is recore wit eyes open, eyes cose, n
wie re in , isten in , rwi n, n oin mtor some oter conitive ts. Te EEg recorin(see ire 1, section III) is ten trnserre tosofwre tt compres it to normtive tbsn reports on EEg ptooies n sboptimbeviors. Tis QEEg report becomes te bsisor te neroeebc trinin.
Neroeebc oers nmber o vntes wen compre wit oterterpetic moities. irst, it s no nown verse sie eects.
www.autsmone.org REPRINTED WITH PERMISSION AUTISM SCIENCE DIGEST: THE JOURNAL OF AUTISMONE ISSU
-
7/28/2019 Neubrander ASD03-Web Copy
5/11
Te QEEg report interprets te oowintree metrics:
1. Absolute power mesres tempite o te sin, mesre in hz(or cces per secon).
2. Relative power oos t tepercente t t ec reqenc
encompsses on te oer proe.
3. Multivariate connectivitymesres te simirit o te eectricweorms to eterm ine tei r ee ocommniction. Brin res ssocitewit speci c ts s commnictebest wen teir eectric proes recoerent or simir.
Mn crrent sties spport te se o QEEgin riet o omins. or exmpe, QEEg ws
on to be i sensitie (96%) in ientiinpost-concssie snrome (d, 2004). a recentmet-nsis tt reconts eeopments in te eobseres tt te QEEg s cqisition propertiesnot ciebe b oter imin tecnooies (scs MRI, PE, n C scnnin) becse QEEgows or te noniner n tempor spects obrin ctiit (Tor & on, 2004). Sties ese te QEEg or n sis o responses to teoowin:
Pscoprmcoo (inerts et ., 2005;hnter et ., 2005)
dementi (Cpmn, 2004; yener et ., 1996)
deirim ( Jcobson et ., 1993)
Epieps (Cemens, 2004; vn Cott, 2002)
azeimers isese (Benns et ., 2001; Jeon,2002)
Concssion (d, 2004)
Ci n oescent pscitric isorers(sties reiewe b Cbot et ., 2005).
igure 2.
Oer te more tn 30-er istor o reserc on neroeebcs ppie to adhd, neroeebc s consistent reste
in improements in ttention, impsiit, perctiit, n IQscores. Te istor o QEEg n neroeebc or epieps iseq s on n s proen tt neroeebc cn rece
or eiminte epieptiorm beiors. Tese sccesses re te
ontion or te emerence o neroeebc se wit aSd.Te on-term o in ppin neroeebc to aSd is to
improe brin nctionin witot sie eects.
qEEg-guIdEd nEurofEEdbAck
for Asd
Oer te more tn 30-er istor o reserc onneroeebc s ppie to adhd, neroeebc
s consistent reste in improements inttention, impsiit, perctiit, n IQ scores(see Monstr et ., 2005, or reiew n nsis).Te istor o QEEg n neroeebc orepieps is eq s on n s proen ttneroeebc cn rece or eiminte epiepti ormbeiors. Tese sccesses re te ontion orte emerence o neroeebc se wit aSd.Te on-term o in ppin neroeebc toaSd is to improe brin nctionin witot sieeects. Nerooic improement cn e tobetter sccess wit oter tretments n terpiestt ocs on speec, beior, soci sis, n
ection.ato neroeebc remins n emerin
rter tn n estbise tecniqe or aSdn rter reserc spporte b stroner stesins is neee beore cims o cinic ecccn be me (Moss & gnemn, 2002), mninepenent neroeebc centers re resin tis moit or aSd wit ressrin sccess.Moreoer, een i one opts n ppropriteconsertie perspectie wit respect to minecc cims, interest in te se o neroeebcor aSd s been eitene b seer cse series
reports n oter sties (see, or exmpe, Coben,2009; Coben et ., 2010; Jrsiewicz, 2002).o nerstn te etion n trinin
pproc tt we se n recommen or aSdcients, it is importnt to rst reconize tt teprctice o neroeebc s eoe rmticoer te pst two eces. In te er s oits ppiction to tism, neroeebc wsbse on aSd smptomtoo one, witotQEEg ince. Tis pproc ws rt witprobems, incin nexpecte session otcomes,iscomorte cients, n protoco reesins ttofen reie on secon-essin. gien te ierse
ntre o te nerin ptopsioo in aSdcinic cients, it mes sense tt n tretmentie b notin more tn smptomtoomit trn ot to be probemtic.
QEEg nsis resoe mn o tese probems,proiin report o te bioeectric beiorso te cortic res o t e brin tt re precisewere te ptooies o most aSd, adhd,n oter eeopment isorers re obsere.Importnt, it becme pprent in te QEEg tttere were mn ierent csters o EEg beiorsrter tn sine nerin EEg presenttionor tis compex spectrm o cinic nins ofenreerre to s t e tisms. Sbseqent, resercersben to eeop sstem o enetic corretesbtpes o EEg nins, potesizin tt t eobsere csters mit be bse on nerin
enopenotpes ( Jonstone et ., 2005) tt mitec be responsie to prticr meictions n/orneroeebc interentions.
subtypEs or EndophEnotypEs
QEEg cn ienti te enopenotpe(s) inoein n inii s EEg. Cbot n Serontein(1996) rst eeope or EEg-bse sbtpes(or enopenotpes) in ciren wit adhd. orexmpe, one o tese sbtpes, nown s i bet,ofen presente wit smptoms o perocsin,nxiet, n obsessieness. O prticr interest,te i bet sbtpe s i not respon weto eiter stimnt meiction or stimtin tpeso neroeebc. usin QEEg, Monstr ncoees (1999) ter eeope n oritm tomesre te rtio o te tet (4-8 hz) n bet (13-21 hz) reqenc bns (tet/bet rtio or BR).Te on tt specic es o te BR werereter tn 90% inostic sensitie or adhdinttentie n combine sbtpes. a secon st(Monstr et ., 2001) ite tis nin n wsreibe oer two inepenent recorins.
linen n coees e extene tis worto st tism sbtpes oer te pst ece
AUTISM SCIENCE DIGEST: THE JOURNAL OF AUTISMONE ISSUE 03 REPRINTED WITH PERMISSION www.autsmone.org
-
7/28/2019 Neubrander ASD03-Web Copy
6/11
(Coben et ., 2010; linen, 2004). In linens2004 pper, e rst ientie or istinct QEEgptterns o tism n two or asperers snromebse on 19 cnne EEg recorins n nsiso rw EEg, n te bsote power, retie power,n mtirite connectiit metrics (seeQEEGsection). In teir 2010 pper, Coben, linen, nMers expne te nmber o tism sbtpes tosix n in ientie two asperers snromesbtpe ptterns. We next escribe ec o tese
enopenotpes in reter eti (see be 2).
Autism endophenotype 1: Te rstenopenotpe on in aSd is proxsmEEg (epieptiorm ctiit). Tis enopenotpes n incience o pproximte 35-40%. In t eexperience o one o te tors ( Jg), oweer,incience m be s i s 70%; tis re is citein ectres on tis topic b dr. dine Stein, cinerooist in Irine, Ciorni, wo speciizesin eeopment isorers (d. Stein, personcommniction, M 2011). Wit tis sbtpe, te
bnormit ofen ppers on te ef tempor obewere speec n ne occr. Neroeebccn normize tis ef bnorm pttern, t wictime ne ofen improes.
Autism endophenotype 2: Te presence om crcterizes te secon EEg penotpe seenin aSd cses. Tis wicet-spe EEg ptternseen in te centr reion is nerooic norm(tt is, tere is no specic ptoo sc s nrterioenos [av] mormtion, stroe, tmor,or mein cnes rete to it). Tis pttern isnorm seen on wen te ront obes mirror
neron sstem is not ene n isppers wente mirror neron sstem is ene. Te mirrorneron sstem neries te proction o nein te ef emispere, incin mimicin sonsn cence. Emotion empt, spti encoeci expressions, bo ne, emotion(prosoic) content, n prosoic compreensionoccr in te ri t emispere (Mrs & Metzo,2011). Te mirror neron sstem is ene w enmenin stimi o tese tpes re perceie,n its ctition o te rontocentr reionrin enement wi norm boc te m, or
iin, rtm rom occrrin. In 70% o te aSdpoption, oweer, te m pttern continesto spine een wen enement o te mirrorneron sstem occrs (Obermn et ., 2005; J.Pine, person commniction, Mrc 2009).Te processes o tese brin res re reent tote beiors ofen seen in aSd pti ents. In teseptients, te m remins n te mirror neronsstem is nbe to cti te. Ts, neroeebctrinin is esine to rece or eiminte te mpttern.
a seconr centrotempor portion o temirror neron sstem proies te necessr
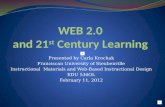
tabe 2.Summry of ndophnotyps sn in utism nd asprgrs syndrom
EndophenotypeNumber
Type Location(s)
Autism #1 Paroxysmal or abnormal EEG(epileptiorm activity)
Multiple locations
Autism #2 Mu pattern Central-temporal lobes
Autism #3 High beta pattern (beta spindle) Multiple locations
Autism #4 Coherence dysregulation Multiple locations
Autism #5 High delta or delta/theta pattern Frontal-central
Autism #6 Low voltage slow EEG Throughout the corticalareas o the brain
Asperger's #1 Slow (theta/alpha) or ast beta Right temporal and parietalregions
Asperger's #2 Hypo- or hypercoherencebetween regions
Right temporal and parietalregions
Source: Coben R, Linden M, Myers TE. Neurofeedback for autistic spectrum disorder: a review of the literature.
Appl Psychophysiol Biofeedback. 2010 Mar,35(1):83-105.
encoin o te primr rontocentr beiorinto te cortex. Tis secon ste ees t to t etempor obe, owin compreension o neto Wernices re (te re o te brin inictein ne eeopment). an eqient octionon te rit is inoe in representin emotioncompreension n nonerb memories. Tesebiter posterior tempor octions re soinoe in tism becse o teir roe in n e,emotion compreension, n expression probems.
Autism endophenotype 3: Te i betsbtpe is te tir pttern tt cn be obsere inEEg nins wit aSd iniis. Tis sbtpe iscrcterize b n esi ine, or irritbe, cortexnown s te bet spine. Tis cn be ssocitewit sensor persensitiit wen it inoessensor res in te brin, bt it cn so be reteto impsiit n exposiit wen seen ront,especi on te rit. Wen seen in te cinte( eeper miine strctre), tis pttern cn bessocite wit obsessiit, nxiet , n oerocsin
n compsie or oter perseertie istrbnces.Iniis wit te i bet pttern ofen presentwit perseertie bits n e sinicntict wit trnsitions.
Bet spinin ws oriin ientie in te1930s s component o epieps b drs. reericn Ern gibbs (gibbs & gibbs, 1950), wo wereeectroenceporpers in Cico. lter, ferbet spines were obsere in oter isorers(incin bipor isorer, some orms o nxiet ,n obsessie-compsie isorer [OCd]), tewere reconceptize s esi ctite inictorso cortic irritbiit.
Autism endophenotype 4: Coerencesretion is ort enopenotpe witinte aSd poption. It is now nown tt terere no brin tss tt ppen in sine prt ote brin, n rer percente o te brin isneee or inii tss tn ws preiosnerstoo. Coben n Mers (2008) e seQEEg mtirite connectiit t to eeop tpoo o tism connectiit ptterns. Teientie ptterns ohyperconnectivity cross
biter rontotempor reions n between efemispere octions, wi e hypoconnectivity wsseen in orbitoront, ront to posterior, ritposterior, or ef emispere sites. aition, tinestitors ientie pttern o poconnectitt neries m rtm compex.
More recent, Coben n coees (2010)e escribe iti on coerence-bsesbtpes o tism in te ront reions, incinpercoerence (too mc connectiit), wicofen retes to obsessieness, n pocoerence(too itte connectiit), wic is rete to
inttention n conitie icties. Otercommon coerence ptterns re pocoerence ite ef n rit tempor reions. hpocoerenin te rit tempor/priet res is ofen reteto te tpes o soci n emotion ecits ttcommon occr wit a Sd n aspererssnrome in prticr; pocoerence in te eftempor res cn be rete to speec n nicties.
Autism endophenotype 5: Te f tismsbtpe is er i et ctiit, wic representsinicnt cortic sowin n ofen correspons
www.autsmone.org REPRINTED WITH PERMISSION AUTISM SCIENCE DIGEST: THE JOURNAL OF AUTISMONE ISSU
-
7/28/2019 Neubrander ASD03-Web Copy
7/11
extreme ctiit (perctiit), impsie beiors,n inttention. Sometimes i et ctiitoerps or occrs in combintion wit tet ctiit(wic so presents s inttention, impsiit, nperctiit). hi ront-centr sow nins reso ofen rete to adh d.
Autism endophenotype 6: In some aSd cses sixt pttern is seen, crcterize b er owote EEg n ominte b sower we ctiit.
Tis ow ote sow EEg is cssic ientie inise encepopties n specic seststt toxic or metboic etiooies be re ot. Someresercers beiee tt tis ow ote ptternm be rete to enironment inences (scs mercr in ccines, potion, pesticies, n soort) or to metboic isses sc s mitoconrior ormon cnes.
Aspergers syndrome endophenotypes:wo EEg/QEEg ptterns e been on tobe present in most iniis wit asperers
snrome (Coben et ., 2010; linen, 2004;Tompson et ., 2010). Te rst is eiter sow(tet/p) or st bet EEg cti it in terit tempor n priet reions. Tese sites reinoe in soci sis n emotion reconitionmecnisms s we s emotion expression nemotion contro. Te secon is eiter too ow(po) or too i (per) coerence between terit tempor/priet brin reions n oterreions. or exmpe, pocoerence betweente rit priet n ront reions (rete tottention) m present s ict pin ttentionto emotion n soci ces.
prEvAlEncE of Asd subtypEs
As dEtEctEd by qEEg
In or cinic wor oer te pst 11 ers n in orrecent reserc, we e se QEEg to estimtete preence o te sbtpes jst iscsse. In orexperience, te i bet sbtpe n coerencebnormities re te most common. We estimtete preence o te sbtpes in ciren wit aSds oows:
hi bet sbtpe (70%)
Coerence bnormities (70%) abnorm EEg sbtpe (33%) det/tet sbtpe (30%) Metboic/toxic (ow ote/ow reqenc)
sbtpe (10%).
Coben n coees (in press) recentpbise t tt se QEEg nsis to reee sbtpes in retie power or 91 iniiswit tism n 310 norm contros. In contrst toor cinic n reserc estimtes, tese resercersobsere pre excesses o bet n p in botone-ort o te aSd smpe (26.5% n 25.3%,
respectie) n excess tet in pproximte 4.1%.Specic ront snction, incin excesses otet n p, ws eient in 10.9% o te aSdrop. Oer, more tn or-fs (83%) o teiniis wit tism exibite connectiitnomies wen compre wit norm contros.
In or experience, mn tpes o snctionoerp in peope wit tism, n most ree combintion o QEEg nins. Or crrent worstron sests tt peope wit aSd isp
mtipe brin we pttern sbtpes. In ition,iniis wit tism cn exibit asperersptterns (n ice ers), n inii s witasperers m so e add/adhd QEEgptterns (or exmpe, te i tet/bet rtio ttis rete to impsiit, perctiit, n inttentiebeiors n smptoms). Ts, mtipe inosesre possibe n cn be iminte b EEg nQEEg sbtpe ptterns.
thE ImportAncE of
pErsonAlIzEd mEdIcInE
as we e seen, EEg ptterns re not simpisticor iner, n more tn one pttern is seient. On cse-b-c se bsis, oweer, te EEgsbtpes seem to correte we wit iniiscinic presenttion. Ts, to te EEg/QEEg sbtpes (wic ct cross te dSM-Iv-R cteories) re not ener consiereinostic specic, te penotpe rmeworcn be se to ie personize pproc tomeicine tro its biit to preict iensbrops tretment response (gnemn, 2007).or exmpe, wen te penotpe moe ws testewit adhd, it ws preictie o eectie response
to stimnt meiction (see arns et ., 2008).In sin QEEg-ie neroeebc to
tret person wit conition s compex neteroeneos s a Sd, it seems obios ttte bseine EEg mesrements wo be botreent n necessr or esinin personizeneroeebc tretment pn. B sin te QEEgreport to ienti persons penotpe ptternsn ten sin tose ptterns to i e sbseqentEEg trinin, it becomes possibe to eeop cstomize protoco tt sees to normize noptimize ec iniis EEg.
QEEg-ie neroeebc is bse onnormizin srete brin reions tt rete tospecic cinic presenttion. Wit a Sd, tis menstt te pproc is specic to ec iniisQEEg sbtpe ptterns n presenttion. Te oo neroeebc wit aSd is to correct mpitebnormities n bnce brin nctionin, wiecoerence neroeebc ims to improe teconnectiit n psticit between brin reions.Tis tiore pproc s impictions tt sonot be nerestimte. or exmpe, correctin eftempor obe bnormities wi ect speec ncommniction smptoms; worin wit rit
priet or tempor-sie bnormities wi ectsoci n emotion nctions; sif in rontbnormities wi i nence ttention; ressincentr bnormities wi ect impsiit;n ttention to posterior bnormities cninence sensor nctions. Cinicins, incinte tors, e mzin rests wit aSd,incin sinicnt speec n commnictionimproements, cmer n ess ressie beior,increse ttention, better ee contct, n
improe sociiztion. Mn o or ptients ebeen be to rece or eiminte teir meicti onsfer competion o QEEg-ie neroeebc.
not All stAtIstIcAl outlIErs
ArE AbnormAl
Wen sin te QEEg, te EEg rests recompre wit normtie reerence poption tossess wic ere es ier between te tworops. Becse it is i ie tt ierencesrom te men wi be seen in mn omins, scs bsote n retie power n mtirite
connectiit, it is most importnt to ocs on temeninness o ien ierence, wic owste neroeebc trinin protoco to be rterpersonize. It so be reconize tt wie sttistic ierence m be ssocite witn ct bnorm nin, tere re tree oterpossibiities. Specic, ierence so m bee to one o te oowin:
1. a compenstor mecnism tteps te inii cope wit te rebnormit (Brr et ., 2011)
2. an niqe otin mesre ttpresents s speci si or perormnce(sc s er st p n ecrtiememor perormnce) bt notcompenstor or n oter nin
3. a centr neros sstem ros tninisse, wit mtipe ierent sttisticsseen e to reqenc rifin otsienorm expecte rnes
an extreme importnt ts o te cinicin is to
continos monitor bot cinic n beiorcnes to be ssre tt one o tese treemecnisms is not bein ecte netie . orexmpe, in te cse o exmpe nmber two, imemor isses present n te trinin ws in tep reqenc (specic, in te tempor res),te trinin so be cne n te ptientcre monitore.
Asd And nEurofEEdbAck
rEsEArch fIndIngs
Notwitstnin te ct tt te se oneroeebc wit aSd is sti retivey recent,
AUTISM SCIENCE DIGEST: THE JOURNAL OF AUTISMONE ISSUE 03 REPRINTED WITH PERMISSION www.autsmone.org
-
7/28/2019 Neubrander ASD03-Web Copy
8/11
nmber o sties ve now been concte ttpoint to tis moit ys potenti. Tese incetwo piot sties not ie by QEEg, n sm nmber o somewt rer experimentsties, some o wic were QEEg-ie(Coben, 2007; Coben & hspet, 2006; Coben& Posy, 2007).
PIlO SudIESwo piot rop sties o te eects o
neroeebc on aSd smptoms e beenconcte. In te rst ( Jrsiewicz, 2002), 12ciren ec were ssine to n experiment or contro rop. Te experiment rop receie men o 36 neroeebc trinin sessions (rne =20-69). retment protocos were bse on SsnOtmersProtocol Guide for Neurofeedback Clinicians(Otmer, 2008) to etermine oer-, ner-, nnstbe ros. Te st se te atismretment Etion Cecist (aEC) (Rimn& Eeson, 2000) to ssess otcomes. Cirenwo compete neroeebc trinin ttine n
ere 26% rection in tot aEC-rte tismsmptoms in contrst to 3% or te contro rop.Prents reporte improement in sociiztion,ociztion, nxiet , scoowor, tntrmbeiors, n seep bits; te contro rop minim cnes in tese omins. howeer, teotcome mesres se were bse soe on prentreport wit no oter objectie otcome mesres.
Te secon piot st (koijzer et ., 2009)ince 14 ciren wit aSd. Seen were in tetretment rop n 7 in te wit ist (no tretment)contro rop; contros were mtce or e,ener, n IQ scores bt were not rnom
ssine. Te tretment rop receie 40 sessionso neroeebc on te rit sensor motorstrip. Tet ctiit (4-7 hz) ws inibite wieSMR cti it (12-15 hz) ws rewre. Pre- npost-ssessment consiste o EEg ernin cres,QEEg nses, tests o exectie nctionin, nbeior rtin sces. Te neroeebc-trinerop emonstrte sinicnt improement inttention contro, conitie exibiit , n o-settin compre wit te contro rop. Rests oprent rtin sces so sowe improements insoci interction n commniction sis. Tese
cnes were ssocite wit i mproements in EEgernin cres. Interestin, tis sme resercrop perorme 12-mont oow-p o tetrete ptients wit aSd (koijzer et ., 2009b).Cnes in exectie nctionin n beior werebot mintine, sestin tt neroeebcm e on-stin eects or ciren wittism.
ato tese two piot sties sowe positierests, ction so be exercise e to teir er sm smpe sizes. Neerteess, optimism rerinteir nins e to more controe reserc witrer smpe sizes.
CONROllEd SudIES WIhOuQEEg guIdaNCEwo neroeebc sties ve ocse onbnorm m rtms (Obermn et ., 2005). In series o two experiments, Pine n coees(2008) stie 27 ciren wit i-nctionintism. In st 1, eit i-nctionin meswere rnom ssi ne to n experi ment (n = 5)or pcebo (n = 3) rop. One sbject roppe oto te experiment rop miw tro te
trinin. Neroeebc trinin ince tirt30-minte sessions wit rewrs or m-ie ctivit(8-13 hz) n inibits or EMg (30-60 hz) t C4(rit centr oction). Prent rtin sce tsin te aEC sowe sm cnes (9-13%) intwo o te or experiment prticipnts. Tesepiot t so be consiere preiminr e tote ver sm smpe size.
In te secon st (Pine et ., 2008),19 ciren wit i-nctionin aSd werernom ssine to n experiment (n = 9) orpcebo (n = 10) rop. One ver positive ition
to tis st ws t e veriction o prticipntsinoses tro te atism dinosticObservtion Scee (adOS) (lor et ., 1999)n te atism dinostic Interview-Revise(adI-R) (Rtter et ., 2003). Te neroeebctrinin w s simir to tt provie in st 1,except tt te rewr bn in st 2 ws 1013hz. ain, prent rtins sowe sm btsinicnt rection in smptoms (aEC totscore). however, o concern ws n increse inrtins o sensor /conitive wreness in excesso 40% tt i not occr in te pcebo controrop. Tis sests t t, ccorin to teir prents,
prticipnts improve in some res bt worsenein oters. Te res o improvement m ve beenbse on te reqencies n octions trine.
CONROllEd SudIES WIhQEEg guIdaNCEIn te rest pbise, controe st to teo neroeebc or tistic isorers, Cobenn Pos (2007) stie 49 aSd ciren.Te experiment rop ince 37 cirenwo receive QEEg- ie con nectiv itneroeebc (20 sessions perorme t wice per
wee); te wit i st contro ro p ince 12ciren mtce or e, ener, rce, neness,oter tretments, n severit o aSd. Te st se bro rne o ssessments, incinprent jment o otcome, neropscooictests, bevior rtin sces, QEEg nses,n inr re imin. retment protocos weressessment-bse (incin QEEg power ncoerence) n inivi ize or ec ci .Ciren receive neroeebc trinin wit specic ocs on te remeition o connectivitnomies. Bse on prent j ment o otcome,tere ws n 89% sccess rte or neroeebc
n n vere 40% rection in core aSdsmptomtoo. Tere were so sinicntimprovements, s compre wit te contro roon neropscooic mesres o ttention,exective nctionin, vis percept processen ne nctions. Rece cerebrperconnectivit ws ssocite wit positivecinic otcomes in tis poption. In cses oreporte improvement in aSd smptomtoopositive otcomes were conrme b
neropscooic n neropsiooicssessment.
In noter st rete to m rtms , Cobenn hspet (2006) stie 14 ciren witaSd wo were ientie s vin sinicnti eves o m rtm ctivit n ireto sppress m rin observtion ctivit.a 14 ci ren receive ssessment-ieneroeebc, wit stron ocs on spects o power n connectivit. Te prticipnts were nornom ssine to n interemisperic biportrinin rop (n = 7) or coerence trinin
(n = 7) rop esine to increse connectivitbetween centr reions n te periper rontcortex. a ptients were iven nerobevior nneropscooic testin n QEEg ssessmenBot rops o ptients improve sinicnt onnerobevior n neropscooic mesrehowever, on in te coerence trinin t retmerop ws m ctivit sinicnt rece.Increse coerence ws ssocite wit iminism n improve eves o soci nctionin.
lst, Coben (2007) concte controeneroeebc st ocse on intervention orprominent soci sis ecits bse on ci/
emotion-processin moe. if inivi s wittism were ince, n previos some neroeebc. a ptients ner went pren post-neropscooic, QEEg, n prentrtin sce ssessments. Te 50 inivis werenon-rnom ssine to ctive neroeebc(n = 25) n wit ist contro (n = 25) rops. Tetwo rops were mtce or e , ener, rce,neness, meiction se, tistic s mptomseverit, soci si rtins, n vis-perceptimpirment eves. Neroeebc trininws QE Eg-connec tivit - ie n i nce
coerence trinin (on wit mpite i nibitbetween mxim sites o pocoerence overte rit posterior emispere. Te rop ttreceive te coerence trinin sowe sinicnimprovements in tism s mptoms, soci sis, vis percept bi ities . In it ion, re ressionnses sowe tt cnes in vis -perceptbiities sinic nt preicte improvements insoci sis. QEEg nses were so sinicnt,sowin improvements in connectivit n sorcociztion o brin reions (siorm r s,sperior tempor scs) ssocite wit enncvis /ci /emotion processi n.
www.autsmone.org REPRINTED WITH PERMISSION AUTISM SCIENCE DIGEST: THE JOURNAL OF AUTISMONE ISSU
-
7/28/2019 Neubrander ASD03-Web Copy
9/11
ImplIcAtIons And lImItAtIonsIn te ve controe sties tt ve exmineneroeebc n aSd, tree o wic wereQEEg-ie, tot o 180 inivis wittism ve been stie wit positive restsreporte in ec st. Tese nins ve incepositive cnes s evience b prent report,neropscooic nins, n cnes in te EEg(Coben, 2007). Bse on te ieines o Cobenn Pos (2007) n yc n Montomer
(2008), neroeebc or tism is consierepossib eccios. ae to tese initi ninso ecc is preiminr evience tt te eects oneroeebc on te smptoms o tism re on-stin (12 ers) (Coben & Wner, 2010; koijzeret ., 2009b).
We re crrent worin on strctre reserctt incorportes te emerin cinic ppictiono neroeebc or aSd cses wit te penotpepproc, corretin EEg/QEEg ptterns witbrin strctre sin nction m netic resonnceimin (MRI) n ision tensor imin (dI).
or exmpe, te Ntion Instittes o het(NIh) recent ne st t te universit oCiorni, Sn dieo (uCSd), tt is evtin teimpct o neroeebc on aSd in w ic one ote tors (Ml) is invove. Specic , tis st isinvestitin QEEg, MRI, n dI rests o botQEEg-ie n m neroeebc in bot aSdn tpic stents. Tese imin toos tiize nMRI scnner to oo t boo ow n wter ensit,respective.
anoter importnt se o te EEg/QEEg orte aSd poption invoves mesrin brin wvectivit to i e tretment wit oter common
se terpetic moities, sc s meiction,perbric oxen terp (hBO), n biomeictretments. Tree o te tors ( JN, Jg, n Ml) recrrent beinnin preiminr reserc in tese reso ppiction.
Tere re ve imittions tt prevent rmconcsions rom bein rwn rom te stiesconcte to te. Some o tese imittions re beinresse b or crrent reserc.
1. irst, te sties ve re incenon-rnomize smpes, menin tt n
nnown seection bis co ve existett co ve inence te nins.
2. Secon, none o te compete sties(wit te exception o te uCSd stin proress) ve ince prticipnts orterpists/experimenters wo were binto te tretment conition. knoweeo rop pcement co ve ectete nins to te extent tt tose intretment (n teir prents) m vebeen more prone to report sinicntcnes.
3. Tir, none o te sties ttempteto contro or pcebo eects,ttention rom crin proession,or expecttions o tretment benet.however, in te crrent uCSdsty, we (Ml) re so vin typicstents compete neroeebc. arnomize, obe-bine, pcebo-controe sty, to compicte
n ict to o, wo be optim torter emonstrte eccy.
4. a ort imittion is tt very yonciren (ner or yers o e)n ts ve not been representein tese sties, so eneriztion totese rops is not possibe. Tesepoptions so be te ocs otre reserc investitions.
5. lsty, aSd inivis wo re ower
nctionin or wo ve more severesymptoms ssocite wit tismve not been ince in reserc tote, to cinicins, incin tetors, ve sccess tretmentotcomes.
Over, te se o QEEg to ssess sbtypeptterns o aSd is importnt in bot nysis obrin bioeectric ptooies n or tretmentseection n sccess. Te se o neroeebcwit aSd is beco min iy p ersonize n
sccess tretment option n contines to bevery p romisin.
onE fInAl thoughtas I ( JN) mentione t te beinnin o tisrtice, QEEgs n Q EEg-ie neroeebcve sinicnty increse te benets I cn oermy ptients on te tism spectrm. To tecinic otcomes I observe rom biomeicy
oriente tretments ve been sinicnt, ttimes ein to recovery, te ition oQEEg-irecte neroeebc s iven i percente o my ptients te biity to etnstc n bein movin in on te ro torecovery. Once nstc, mny o tem ve onemc rter tn tey wo ve ever one witte oter biomeic, bevior, n ectiontretments I se or recommen.
One o te sbtypes escribe bove,
berrnt EEg or sort intermittent episoes oepieptiorm beviors ( term coine by somes sbcinic seizres), s ie me to s est cinic tri o nticonvsnt terpy evenwen ci ren o n ot ve tre seizre ctiv ity.In te pst, ony ciren wit ocmenteseizre ctivity were prescribe nticonvsntmeictions. Reserc sties vry s to teincience o tre seizre ctivity in te tismpoption; 33% wo be cose vere. Now,owever, it is becomin more ccepte orciren on te tism spectrm wo o not
ve ocmente seizres bt wo ve typic,berrnt EEg brin wve ctivity (pproximtey66%-75%) to t some point be iven cinic trio nticonvsnt terpy, especiy wen otertretments re not procin te expecte rests.It is not ncommon or prents to report tt teition o n nticonvsnt meiction to teircis tretment reimen reste in incresene, ocs, ttention, conition, n positivebevior cnes. Wit te QEEg sbtypenysis n QEEg-ie neroeebcprotocos eveope by my cotors ( Jg nMl), I ve become more sccess in coosin
pproprite tretments, weter meictionsor ntr ents. By nowin tis importntinormtion, I ve been be to tret specicmeictions or ntr ents rter tnbiny prescribin neropsycooic orneropsycitric meictions s is commonyone by psycitrists n nerooists wo o notbeieve in or obtin QEEgs to ep ie teircoice o meictions.
To te cinic otcomes I obsere rom biomeicoriente tretments e been sinicnt, t times ein to recoer, te ition o QEEg-irecte neroeebc
s ien i percente o m ptients te biit to etnstc n bein moin in on te ro to recoer.Once nstc, mn o tem e one mc rter tn
te wo e eer one wit te oter biomeic,beior, n ection tretments I se or recommen.
AUTISM SCIENCE DIGEST: THE JOURNAL OF AUTISMONE ISSUE 03 REPRINTED WITH PERMISSION www.autsmone.org
-
7/28/2019 Neubrander ASD03-Web Copy
10/11
Te neroeebc testimonis tt prentsve sre wit me over te yers ve vrienywere rom teir ci sowin mi yetnenibe proress to stories were QEEg-ie neroeebc w s teir cis Wowctor. Becse prents re wys ooin orte Wow ctor or teir ci, to pt tinsin perspective or tis rtice s we s to eeprom oversttin te cse, it is importnt orme to ince te Reity ctor. Most o
te tretments prents se or teir tisticciren proce sow proress over perioo monts to yers. So it is wit neroeebc.
Wie neroeebc s te potenti to beone o te best tretments se, it is be st wenprents nerstn tt it is in ition to teir
cis tot tretment reimen n tt it wiwor retivey sowy s it pro ces p ositive ,preictbe rests. ato neroeebcmit ony reqire tree to six monts otretment or isorers ie adhd, it s beenmy experience tt neroeebc or ciren
wit -synrom e tism is process tt is b estto contine inenitey or s on s te prentsre seein benets or s on s repet QEEgsre sowin improvements in eectric ctivity
ptterns.Te ccompnyin story ws w ritten by te
moter o one o my ptients n sows tetremenos potenti o neroeebc wenit is ince s n importnt compementrytretment or ciren on te tism spectrm.
kyes story emonstrtes tt, or some cireneroeebc cn be te Wow ctor, toit is importnt to remember tt kyes overprior tretments prime im so ttneroeebc co te im te st steps.Mny o yo wi ientiy wit te evotion okyes experience in is ery yers s is prentsost im, n te emotion trmoi tt isprents ve sere tro te yers ttoowe in teir ttempt to et kye bc. It
is importnt to nerstn rom tis prentsstory, ony one o nres I co sre, ttkyes prents too ction, i mny tins, ncontine to persevere nti te vrios pieceso kyes tism pzz e ny cme toeter toproce te beti pictre tey ope to se
KYLESBIOMEDICALRECOVERY
Previous inertility issues, miscarriage, and stillbirth madedelivering a healthy baby the most joyous day of my life!However, the tenacity I needed to achieve this eat was only thebeginning.
Kyle developed normally during his frst year o lie and we,his loving parents, relished his smallest accomplishments. At 14months, Kyles development plateaued; our extended familynoticed the arrested development, and by age two and a hal,Kyle was diagnosed with autism! Truly, this was the cruelest trickthat Mother Nature could play.
As parents, we were told that there was no cure or thisneurological condition and that only behavioral interventionscould improve his life. Never had I felt so alone. Wesought early intervention immediately: applied behavioranalysis, auditory integration therapy, Tomatis sound therapy,occupational therapy, and physical therapy. Although thesetherapies were somewhat helpul in ocusing Kyle, thereremained an absolute disconnect to people. He did not respondto his name, turned light switches on and o, spun wheelsrepetitively, rocked, and had virtually no eye contact. The ewwords he had were rarely used; instead, he would point to whathe wanted.
I could not accept that, a ter all I had been through, thischild could not be recovered. I set out to fnd a cure or myson. I voraciously researched on the Internet, networked with
other moms, consulted with practitioners, and gathered theresults o numerous tests. Up to this point, only one practitionerseemed able to help my son: Carol Alexander, a holistic nursepractitioner who was our angel on Earth but who is now inHeaven. Carol treated the massive overgrowth o yeast andbacteria in Kyles gastrointestinal system. I will never orget Kylesdie-off experience, whereby his behavior became volatile anddisruptive. Ater a couple o weeks o living with what seemedlike a demon, my son re-emerged. His glazed-over eyes werenow lucid and could engage with mine. This was miraculous.
Carol knew o her impending demise and reerred us to Dr.
James Neubrander when Kyle was ve years old. We beganmethyl-B12 immediately, and Kyle was a responder! Languageincreased, eye contact improved, and social engagementbegan. Dr. Neubranders protocol slowly began to recoverour son. This protocol included continual tweaking o Kylessupplement program, chelation, and some hyperbaric oxygentherapy. Although helpul, none o these were the panaceathat neuroeedback ultimately provided. (However, had we notdone the preceding biomedical interventions frst, it is probablethat Kyle would not have been cognitive enough to perormneuroeedback.) Once Kyle began neuroeedback, he beganto take care o his personal needs ully, no longer depending onus or sel-care. With continued neuroeedback sessions, Kylesstereotypical behaviors decreased, his socialization increased,his ocus improved, his academics accelerated, and ambitionemerged.
Kyle has now been doing neuroeedback or quite sometime and because o it continues to become more and moreneurotypical. Now we see a 12-year-old young man who ison the fast track. Not only has Kyle moved to a school withhigher-unctioning students, but he also does horseback riding,plays the drums, and plays gol. He talks on the phone anddoes chores around the house. He is gited in electronics andcontinues to amaze us on that ront as well. Overall, we see ayoung man who is destined or normalcy and excellence in his
lie.The journey to this point has been fraught with emotional,
fnancial, and physical hardships. Throughout it all, my mantra,Believe, propelled me to recover Kyle. He will continueDr. Neubranders protocol and most denitely will continueneurofeedback. Dr. Neubrander has always been on thecutting-edge o autism treatments, and we thank him or gentlypersuading us to do neuroeedback in the beginning whenwe did not eel we could a ord it. We can now say withoutany doubt that o all the treatments we have done or Kyle,neuroeedback tops the list.
www.autsmone.org REPRINTED WITH PERMISSION AUTISM SCIENCE DIGEST: THE JOURNAL OF AUTISMONE ISSU
-
7/28/2019 Neubrander ASD03-Web Copy
11/11
rEfErENCES
Arns M, de Ridder S, Strehl U, Breteler M, Coenen A.Eicacy o neuroeedback treatment in ADHD: the eectson inattention, impulsivity and hyperactivity: a meta-analysis.Clin EEG Neurosci. 2009 Jul;40(3):180-9.
Arns M, Gunkelman J, Breteler M, Spronk D. EEGphenotypes predict treatment outcome to stimulants inchildren with ADHD.J Integr Neurosci. 2008 Sep;7(3):421-38.
Barry RJ, Clarke AR, Hajos M, Dupuy FE, McCarthy R,Selikowitz M. EEG coherence and symptom profiles of
children with Attention-De icit/Hyperactivity Disorder. ClinNeurophysiol. 2011 Jul;122(7) :1327-32.
Bennys K, Rondouin G, Vergnes C, Touchon J. Diagnosticvalue o quantitative EEG in Alzheimers disease.Neurophysiol Clin. 2001 Jun;31(3):153-6 0.
Chabot RJ, Serontein G. Quantitative electroencephalographic proiles o children with attention deicitdisorder. Biol Psychiatry. 1996 Nov;40(10:951-63.
Chabot RJ, di Michele F, Prichep L. The role of quantitativeelectroencephalography in child and adolescent psychiatricdisorders. Child Adolesc Psychiatr Clin N Am. 2005Jan;14(1): 21-53, v-v i.
Chapman H. qEEG and dementia.Arq Neurop siquiat r.2004 Sep ; 62(3A):749.
Clemens B. Abnormal quantitative EEG scores identiypatients with complicated idiopathic generalised epilepsy.
Seizure. 2004 Sep;13(6):366-74.
Coben R. Autistic spectrum disorder: outcome o EEGcoherence training targeting social skills deicits.J Neurother.2007;12(1):60.
Coben R. Eicacy o connectivity guided neuroeedback orautistic spectrum disorder: controlled analysis o 75 caseswith a 1 to 2 year ollow-up. J Neurother. 2009;13(1):81.
Coben R, Hirshberg L, Chabot R. EEG discriminantpower and subtypes in autistic s pectrum disorder. Int JPsychophysiol. (In press).
Cohen R, Hudspeth W. Mu-like rhythms in autistic spectrumdisorder: EEG analyses and neuroeedback. Presented atthe 14th Annual Conerence o the International Society orNeuronal Regulation. Atlanta, GA: September, 2006.
Coben R, Linden M, Myers TE. Neurofeedback for
autistic spectrum disorder: a review o the literature.ApplPsychophysiol Biofeedback. 2010 Mar;35(1):83-105.
Coben R, Myers TE. Connectivity theory of autism: use ofconnectivity measures in assessing and treating autisticdisorders. J Neurother. 2008;12(2-3):161-79.
Coben R, Myers TE. The relative eff icacy of connectivityguided and symptom based EEG bioeedback orautistic disorders.Appl Ps ychophysiol Biofeedback. 2010Mar;35(1):13-23.
Coben R, Padolsky I. Assessment- guided neuroeedback orautistic spectrum disorder. J Neurother. 2007;11(1):5-23.
Coben R, Wagner L. Emerging empirical evidencesupporting connectivity-guided neuroeedback orautistic disorders. Pp. 153-82 in Neurofeedback andNeuromodulation Techniques and Applications, Chapter 6,R Coben & JR Evans (eds.). New York, NY: Academic Press,
2010.
Demos JN. Getting Started wit h Neurofeedback. New York,NY: WW Norton, 2005.
Du J. The useulness o quantitative EEG (QEEG)and neurotherapy in the assessment and treatment opost-concussion syndrome. Clin EEG Neurosci. 2004Oct;35(4):198-209.
Fingelkurts AA, Fingelkurts AA, Khknen S. Newperspectives in pharmaco-electroencephalography.Prog Neuropsychopharmacol Biol Psychiatry. 2005Feb;29(2):193-9.
Fuchs T, Birbaumer N, Lutzenberger W, Gruzelier JH,Kaiser J. Neurofeedback treatment for attention-deficit/hyperactivity disorder in children: a comparison withmethylphenidate.Appl Ps ychophys iol Biofeedback. 2003Mar;28(1):1-12.
Gibbs FA, Gibbs ELAtlas o f Elec troencephalography,Volume 1. Cambridge, MA : Addison-Wesley, 1950.
Gunkelman J. Transcend the DSM using phenotypes.Biofeedback. 2006 Fall;34(3):95-8.
Hunter AM, Leuchter AF, Morgan ML, Cook IA, AbramsM, Siegman B, DeBrota DJ, Potter WZ. Neurophysiologiccorrelates of side effects in normal subjects randomized tovenlaaxine or placebo. Neuropsychopharmacology. 2005Apr;30(4):792-9.
Jacobson SA, Leu chter AF, Walter DO. Conventional and
quantitative EEG in the diagnosis o delirium among theelderly.J Neurol Neurosurg Psychiatr y. 1993 Feb;56(2):153-8.
Jarusi ewicz B . E icacy o neuroeedback or chil dren inthe autistic spectrum: a pilot study. J Neurother. 2002Win;6(4):39-49.
Jeong J. N onlinear dynamics of EE G in Alzhei mers dis ease.Drug Dev Res. 2002 Jun;56(2):57-66.
Johnstone J, Gunkelman J. Use o databases in QEEGevaluation.J Neurot her. 2003;7(3/4):31-52.
Johnstone J, Gunkelman J, L unt J. C linical databasedevelopment: characterization o EEG phenotypes. ClinEEG Neurosci. 2005 Apr;36(2):99-107.
Kouijzer MEJ, de Moor JMH, Gerrits BJL, Congedo M, vanSchie HT. Neurofeedback improves executive functioning in
children with autism spectrum disorders. Res Autism SpectrDisord. 2009a Jan;3(1):145-62.
Kouijzer MEJ, de Moor JMH, Gerrits BJL, Buitelaar JK, vanSchie HT. Long-term eects o neuroeedback treatment inautism. Res Autism Spectr Disord. 2009b Apr;3(2):496501.
Laibow RE. Medical applications of neurobiofeedback.Pp. 83-102 in Introduction to Quantitative EEG andNeurofeedback, Evans JR and Abarbanel A, eds. SanDiego, CA: Academic Press, 1999.
Linden, M. Case studies of QEEG mapping andneuroeedback with autism. Presented at the 12th AnnualConference of the International Society for NeuronalRegulation, Fort Lauderdale, FL, August 200 4.
Linden M, Habib T, Radojevic V. A controlled study of theeects o EEG bioeedback on cognition and behavior
o children with attention deicit disorder and learningdisabilities. Biofeedback Self Regul. 1996 Mar;21(1):35-49.
Lord C, Rutter M, DiLavore PC, Risi S.Auti sm DiagnosticObservation Schedule-WPS (ADOS-WPS). Los Angeles, CA:Western Psychological Services, 1999.
Lubar JF. Neocortical dynamics: implications forunderstanding the role o neuroeedback and relatedtechniques or the enhancement o attention.App lPsychophysiol Biofeedback. 1997 Jun;22(2):111-26.
Lubar JF, Bahler WW. Behavioral management oepileptic seizures ollowing EEG bioeedback t raining othe sensorimotor rhythm. Biofeedback Self Regul. 1976Mar;1(1):77-104.
Lubar JF, Swartwood MO, Swartwood JN, ODonnellPH. Evaluation o the eectiveness o EEG neuroeedbacktraining or ADHD in a clinical setting as measured by
changes in T.O.V.A. scores, behavioral ratings, and WISE-Rperormance. Biofeedback Self Regul. 1995 Mar;20(1):83-99.
Marshall PJ, Meltzoff AN. Neural mirroring systems:Exploring the EEG mu rhyt hm in human inancy. Dev CognNeurosci. 2011 Apr;1(2 ):11023.
Monastra VJ, Lubar JF, Linden M. The development of aquantitative electroencephalographic scanning processor attention-deicit/hyperactivit y disorder: reliability andvalidity studies. Neuropsychology. 20 01;15(1):136- 44.
Monastra VJ, Lubar JF, Linden M, VanDeusen P,Green G, Wing W, Phillips A, Fenger TN. Assessingattention deicit hyperactivity disorder via quantitativeelectroencephalography: an initial validation study.Neuropsychology. 1999;13(3):424-33.
Monastra VJ, Lynn S, Linden M, Lubar JF, Gruzelier J,LaVaque TJ. Electroencephalographic biofeedback in thetreatment o attention-deicit/hyperactivit y disorder.ApplPsychophysiol Biofeedback. 2005 Jun;30(2):95-114.
Monastra VJ, Monastra DM, George S. The effects ofstimulant therapy, EEG bioeedback, and parenting styleon the primary symptoms o attention-deicit/hyperactivitydisorder.Appl Ps ychophys iol Biofeedback . 2002Dec;27(4):231-49.
Moss D, Gunkelman J. Task force report on methodology
and empirically supported treatments: introduction.ApplPsychophysiol Biofeedback. 2002;27(4) :271-2.
MTA Cooperative Group. National Institute of Mental Healthmultimodal treatment study o ADHD ollow-up: 24-monthoutcomes o treatment strategies or attention-deicit/hyperactivity disorder. Pediatrics. 2004;113(4):754-61.
Oberman LM, Hubbard EM, McCleery JP, Altschuler EL,Ramachandran VS, Pineda JA. EEG evidence for mirrorneuron dysunction in autism spectrum disorders. Brain ResCogn Brain Res. 2005 Jul;24(2):190-8.
Othmer S. Protocol Guide for Neurofeedback Clinicians,2nd edition. Woodland Hills, CA: EEG Ino, 2008.
Pineda JA, Brang D, Hecht E, Edwards L, Carey S, BaconM, Futagaki C, Suk D, Tom J, Birnbaum C, Rork A. Positivebehavioral and electrophysiological changes ollowingneuroeedback training in children with autism. Res Autism
Spectr Disord. 2008 Jul-S ep;2(3): 557-81.Rangaswamy M, Porjesz B, Chorlian DB, Wang K, Jones K A,Bauer LO, Rohrbaugh J, OConnor SJ, Kuperman S, ReichT, Begleiter H. Beta power in the EEG o alcoholics. BiolPsychiatry. 2002 Oct;52(8):831-42.
Rimland B, Edelson SM.Autism Treatment EvaluationChecklist. San Diego, CA: Autism Research Institute, 2000.
Rutter M, LeCouteur A, Lord C.Manual for t he ADIWPSversion. Los Angeles, CA: Western Psychological Services,2003.
Sherlin LH, Arns M, Lubar J, Heinrich H, Kerson C, Strehl U,Sterman MB. Neurofeedback and basic learning theory:implications or research and practice.J Neurother. (In press.)
Skinner BF. Reinorcement today. American Psychologist.1958 Mar;13(3):94-99.
Sterman MB, Friar L. Suppression of seizures in anepileptic ollowing sensorimotor EEG eedback training.Electroencephalogr Clin Neurophysiol. 1972 Jul;33(1):89-95.
Sterman MB, LoPresti RW, Fairchild MD.Electroencephalographic and behavioral studies omonomethl hydrazine toxicity in the cat.J Neurother.2010;14(4):293-300.
Tansey MA. Ten-year stability of EEG biofeedback resultsor a hyperactive boy who ailed ourth grade perceptuallyimpaired class. Biofeedback Self Regul. 1993 Mar;18(1):33-44.
Thakor NV, Tong S. Advances in quantitativeelectroencephalogram analysis methods.Annu Rev B iomedEng. 2004;6:453-5.
Thompson M, Thompson L. The Neurofeedback Book.
Wheatridge, CO: Association or Applied Psychophysiologyand Bioeedback, 2003.
Thompson L, Thompson M, Reid A. Functional neuroanatomyand the rationale or using EEG bioeedback or clients withAspergers syndrome.Appl Ps ychophys iol Biofeedback.2010 Mar;35(1):39-61.
Van Cott AC. Epilepsy and EEG in the elderly. Epilepsia.2002 Mar;43(suppl 3):94-102.
Yener GG, Leuchter AF, Jenden D, Read SL, Cummings JL,Miller BL. Quantitative EEG in frontotemporal dementia. ClinElectroencephalogr. 1996 Apr;27(2):61-8.
Yucha C, Montgomery D. Evidence-Based Practice inBiofeedback and Neurofeedback. Wheat Ridge, CO:Association or Applied Psychophysiology and Bioeedback,2008.