Nerve & Joint Blocks
15
NERVE & JOINT BLOCKS IN LARGE ANIMALS Dane M. Tatarniuk, DVM September 3rd, 2013 Nerve & Joint Blocks Overview : - Nerve and joint blocks are useful tools utilized by veterinarians to aide in the diagnosis of lameness or to provide analgesia to facilitate surgical procedures. Resource : - One of the best resources I have encountered for nerve and joint blocks is “Equine Joint Injection and Regional Anesthesia ” by William Moyer, Jim Schumacher, John Schumacher. Published by Academic Veterinary Solutions, most recent edition is from 2011. Terminology : - Nerve block = Perineural Anesthesia - Joint block = Intra-articular Anesthesia Neurophysiology : - Mechanism: o Nerves require Na+ influx across the peripheral nerve membrane (from extracellular to intracellular) to initiate depolarization and create an action potential o Local anesthetics bind and block Na+ channels on the membrane Prevents influx of Na+ = no depolarization - Anesthetics are often coupled with epinephrine for vasoconstriction o Longer anesthetic time via delayed reabsorption o Less bleeding Drugs : 1
-
Upload
dane-tatarniuk -
Category
Health & Medicine
-
view
1.988 -
download
4
description
Review of common nerve & joint blocks used in horses. Prepared for 3rd year veterinary students.
Transcript of Nerve & Joint Blocks

NERVE & JOINT BLOCKS IN LARGE ANIMALS
Dane M. Tatarniuk, DVMSeptember 3rd, 2013
Nerve & Joint Blocks Overview :- Nerve and joint blocks are useful tools utilized by
veterinarians to aide in the diagnosis of lameness or to provide analgesia to facilitate surgical procedures.
Resource: - One of the best resources I have encountered for nerve and joint
blocks is “Equine Joint Injection and Regional Anesthesia” by William Moyer, Jim Schumacher, John Schumacher. Published by Academic Veterinary Solutions, most recent edition is from 2011.
Terminology:- Nerve block = Perineural Anesthesia- Joint block = Intra-articular Anesthesia
Neurophysiology:- Mechanism:
o Nerves require Na+ influx across the peripheral nerve membrane (from extracellular to intracellular) to initiate depolarization and create an action potential
o Local anesthetics bind and block Na+ channels on the membrane
Prevents influx of Na+ = no depolarization- Anesthetics are often coupled with epinephrine for
vasoconstrictiono Longer anesthetic time via delayed reabsorptiono Less bleeding
Drugs:
1
Drug Onset DurationLidocaine Fast 1 – 2
hoursMepivicaine(Carbocaine
®)
Fast 2 – 3 hours
Bupivicaine Intermediate
3 – 6 hours

- Mepivicaine considered less tissue irritating compared to lidocaine
- Bupivicaine is the longest acting, useful when long analgesic duration is required
Anatomical Considerations:- What structures are innervated at varying levels of the limb?
o ie, a palmar digital nerve block will block sensation to the navicular bone
- Where do nerves branch?o ie, an abaxial nerve block is higher than the dorsal
branch of the palmar digital nerve, thus sensation to the entire foot is blocked
- Are joints separate or do they communicate with other joints?o ie, intra-articular block of the middle carpal joint will
also block the carpal-metacarpal joint as they communicate together
- Are synovial structures in close proximity to the nerves?o ie, perform low-four point nerve block and
inadvertently inject and desensitize the flexor tendon sheath
Lameness Exam Considerations:- Is the lameness ‘blockable’?
o First need to identify and feel confident in which of the four limbs is the lame leg.
o After identifying the lame leg, determine whether the lameness can be consistently seen
o Often requires a grade 2/5 or higher lameness (AAEP scale)
- Is the horse amendable to blocking?o Cannot sedate with alpha-2 agonists
Sedation provides low grade analgesia Sedation changes balance and gait of horse
o Can tranquilize with acepromazine, as it has no analgesic properties
o Can apply nose twitch, if necessaryo Forelimbs are easier to block than hindlimbso With good horsemanship and proper positioning, most
horses can be safely blocked.- Distal-to-Proximal Nerve Block Sequence
o Nerve blocks will desensitize the tissue that is distal and deep to the site of injection
2

o The lower you begin your nerve blocks, the more sensitive your examination will be
Start low and move proximal with subsequent nerve blocks
o This rule only applies for nerve blocks, not joint blocks Joint blocks only anesthetize the joint Following a joint block, you can move back down
distally in the limb and perform another joint or nerve block below your first joint block
ie, you can perform a radial-carpal joint block first, and then move downwards to perform a palmar digital nerve block
ie, you cannot perform a four-point nerve block first, and then move downwards to perform a palmar digital nerve block….because that region is already desensitized!
- Did the block work?o Takes approximately 5 – 10 minutes after injection for
block to worko The easiest method of determining whether your block
worked is to test for skin sensitivity in the region that should be numb
o This is often achieved by ‘poking’ the horse with a pen, hemostat, etc.
o Horses can visualize your movements and react in response to what they see (vs. what they feel) so it helps to have handler cover the eye on the ipsilateral side
o For foot sensitivity, if the foot was previously positive you can reapply hoof testers to determine if the foot is now negative
o Stoic horses will fail to show response to skin stimulation, even when skin remains innervated
Compare to the other limb to look for differing response
o If the block did not work, re-inject again (“top-off the block”)
Preparation of Injection Site:- Nerve blocks
o Ensure that the skin is cleano Often only takes 1-5 minutes of alternating
chlorhexidine or betadine with alcohol wipes
3

o If the site of nerve block is close to a synovial structure, there exists a potential for inadvertent injection into the synovial structure
Consider preparing the skin aseptically (as you would for a joint block)
- Joint blockso Intra-articular placement of the needleo Require (minimum of) 10 minute aseptic surgical scrub
of skin at the location of needle placemento Betadine or chlorhexidine scrub, alternating with
alcohol o Sterile technique
Sterile gloves, sterile syringe, sterile needles – don’t break sterile technique
New bottle of local anesthetic solution
Side Effects:- Cellulitis
o Bacterial infection of the subcutaneous tissueso Heat, swelling, pain on palpation – localized over
injection site- Hematoma
o Often artery/vein run in close proximity to nerve- Synovitis
o Non-septic (“joint flair”)o Septic
No bueno, treat as an orthopedic emergency (refer)
- Toxicity of local anesthetico Lidocaine toxicity is ~10mg/kg
Maximum dose in 500kg horse is 300ml of 2% lidocaine
Outcome:- Improvement in original lameness
o Often the lameness is not completely gone, but substantial improvement is attained (“subjectively 70-80% improved”)
- Lameness switches to another limbo Often indicates that there is a bilateral lameness
present- No improvement in lameness
o Can wait longer to see if further time allows for the block to better desensitize region
4

o Move to the next block proximally in the limb, or consider other diagnostics
- Failure to respond to a block (“False Negative”)o Mechanical lameness (not originating from pain)o Chronic, deep pain (ie, laminitis or bad foot abscess)o Learned behavior (horse anticipates limb to hurt so still
attempts to guard the limb while moving)
5

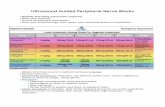
NERVE BLOCKS
- These are the most common nerve blocks, in order of distal to proximal, used for the diagnosis of lameness.
1) Palmar / Plantar Digital Nerve Block- Volume: 1 – 2 cc- Needle: 25 gauge, ¾ inch- Technique: Palpate the lateral and the medial palmar/plantar digital neurovascular bundle. Place needle axial to the collateral cartilage, as low in the foot as possible. Can perform with the limb held up or with the horse standing on the limb.- Structures Blocked: Desensitizes the palmar/plantar third of the foot, as well as the sole. Anatomical structures in this area include the digital cushion, navicular bone, navicular bursa, distal aspect of deep digital flexor tendon, wings of the third phalanx, bars/sole/frog of the foot, and on occasion the coffin joint.
2) Abaxial Sesamoid Nerve Block (also known as ‘basi-sesamoid’)- Volume: 1 – 2 cc- Needle: 25 gauge, ¾ inch- Technique: Palpate the lateral and medial palmar/plantar digital neurovascular bundle on the abaxial aspects of the sesamoid bones. Insert needle along the length of each nerve. Nerves are at the palmar/plantar aspect of the bundle (cranial->“V.A.N.”->caudal)- Structures Blocked: Desensitizes the limb from below the level of the fetlock. Anatomical structures in this area include the entire foot, coffin joint, pastern joint, P1/P2/P3, distal sesamoidean ligaments, distal common digital extensor tendon, distal deep digital flexor tendon, etc.
3) Low Four Point Nerve Block (forelimb)- Volume: 2 – 3cc- Needle: 1 inch, 22 gauge- Technique: Four point nerve block requires injection of anesthetic along the both the lateral & medial palmar nerves, as well as the lateral & medial palmar metacarpal nerves. The lateral & medial palmar nerves can be blocked via injecting in between the deep digital flexor tendon and the suspensory ligament, approximately halfway up the length of the cannon bone (to avoid the flexor tendon sheath). The lateral & medial palmar metacarpal nerves can be blocked via injecting just distal to the ‘button’ of the lateral & medial splint bone. - Structures Blocked: Desensitizes the fetlock joint, branches and insertion of the suspensory ligament, DDFT/SDFT up to the level of the block, and all structures distal to the fetlock.
6

4) Six Point Nerve Block (hindlimb)- Volume: 2 – 3cc- Needle: 1 inch, 22 gauge- Technique: The lateral & medial plantar nerves, and lateral & medial plantar metatarsal nerves are blocked in similar fashion to the 4-point block in the forelimb (above). In the hindlimb, ‘dorsal metatarsal’ nerves provide innervation on the dorsal surface. Therefore, this block requires an additional subcutaneous ring block directed dorsally. This ring block originates from the location where the lateral & medial plantar metatarsal nerves were blocked. Keep safe during this block!- Structures Blocked: Desensitizes the fetlock joint, branches and insertion of the suspensory ligament, DDFT/SDFT up to the level of the block, and all structures distal to the fetlock.
5) Proximal Meta-carpal/tarsal- Volume: 2 – 3cc- Needle: 1.5 inch, 22 gauge- Technique: Three different techniques exists:
(i) High 4-point: block the palmar nerves between the DDFT & suspensory ligament (as in the 4-point block), and block the palmar metacarpal nerves axial to the splint bone adjacent to the suspensory ligament. Can inadvertently enter carpal-metacarpal joint in forelimb or tarsal sheath in hindlimb. (ii) Local infiltration of suspensory ligament: Directly infiltrate anesthetic solution along the axial aspect of the splint bones, directly next to the suspensory ligament.(iii) Lateral palmar (forelimb only): Anesthetize the nerve as it courses along the medial aspect of the accessory carpal bone.
- Structures Blocked: Blocks all structures distal to the carpus, including the proximal suspensory ligament.
6) Median & Ulnar Nerve Block (forelimb)- Volume: 10-20cc- Needle: 1.5 inch, 22 gauge- Technique:
(i) The median nerve can be blocked by inserting the needle 5cm distal to the elbow joint, on the medial aspect of the limb. The needle is walked off the caudal aspect of the radius. (ii) The ulnar nerve can be blocked by inserting the needle 10cm proximal to the accessory carpal bone, between the flexor carpi ulnaris muscle and ulnaris lateralis muscle.
- The medial cutaneous antebrachial nerve only innervates the skin, therefore is not usually blocked to identify a cause of lameness.- Structures Blocked: Distal radius, carpus, all structures below the carpus.
7

7) Peroneal & Tibial Nerve Block (hindlimb)- Volume: 10-20cc- Needle: 1.5 inch, 22 gauge- Technique:
(i) The deep and superficial peroneal nerve is anesthetized on the lateral aspect of the limb, 10cm proximal to the point of the hock, in a groove created by the long and lateral digital extensor muscles. To anesthetize the deep peroneal nerve, deposit solution next to the tibia. To anesthetize the superficial peroneal nerve, deposit solution superficially just under the skin. (ii) The tibial nerve can be blocked 10cm proximal to the calcaneous, between the gastrocnemius & superficial digital flexor tendon. The nerve lies closer to the medial aspect of the limb.
- Structures Blocked: Distal tibia, hock, all structures below the hock.
8

JOINT BLOCKS
1) Distal Interphalangeal Joint Block- Needle: 1.5 inch, 20 gauge- Volume: 4 -6 cc- Coffin joint is most easily and commonly approached from the dorsal aspect of distal limb, via inserting the needle through the common digital extensor tendon approximately 1-2cm proximal to the coronary band. The needle should be aligned either perpendicular to the surface of the skin or parallel to the ground. Horses can be sensitive to needle insertion so stay in safe position. This site is also vascular, so the skin may bleed noticeably. - Alternatively, a lateral approach can be used via palpating the proximal edge of the collateral cartilage, halfway between the dorsal and palmar/plantar aspect of P2. The needle is angled medial and slightly down-wards.- Consider placing bandage over injection site.- Structures blocked include the entire coffin joint, and navicular bursa by diffusion.
2) Metacarpal/tarsal-phalangeal Joint Block- Needle: 1.5 inch, 20 gauge- Volume: 8 – 12 cc- Numerous approaches to the fetlock joint. Most common is the proximal palmar/plantar pouch, which is located palmar/plantar to the cannon bone, dorsal to the lateral branch of the suspensory ligament, and immediately distal to the button of the lateral splint bone. Needle is inserted in lateral aspect of pouch angled in a downward direction. Technique easier with limb flexed (assistant). Can bleed more so not great for synoviocentesis.- Dorsal pouch is injected via palpating the dorsal aspect of the fetlock, and inserting the needle lateral and parallel to the frontal plane, such that the needle enters deep to the common/long digital extensor tendon.- Distal palmar pouch is injected via palpating a recess present along the distal dorsal aspect of the lateral sesamoid bone, proximal to the proximal palmar/plantar process of P1. The needle is angled upward and dorsal-medial. Watch for neurovascular bundle, which is immediately palmar/plantar. - Collateral Sesamoidean approach is to insert the needle in between the palmar/plantar aspect of the cannon bone and dorsal articular surface of the sesamoid bone, thereby penetrating the lateral collateral sesamoidean ligament. Best accomplished with the limb flexed.- Consider placing bandage over injection site.- Structures blocked: Fetlock Joint
9

3) Radio-carpal & Inter-carpal Joint Block- Needle: 20 gauge, 1.5inch- Volume: 7-10 cc- Radiocarpal joint is injected dorsally, with the carpus flexed. The radiocarpal joint can be palpated as an indentation present on medial or lateral aspect of extensor carpi radialis tendon. The proximal border is the dorsal-distal radius and the distal border is the dorsal-proximal radial or intermediate carpal bone. The needle is directed straight into the indentation.- The intercarpal joint is located similar – with the carpus flexed and as an indentation on either side of the extensor carpi radialis tendon. The proximal border is the dorsal-distal radial or intermediate carpal bone, and the distal border is the proximal border of the third carpal bone. The needle is directed straight into the indentation.- A lateral approach to the radiocarpal and intercarpal joint exists, via palpating a notch created by the ulnaris lateralis tendon and lateral digital extensor tendon - and inserting the needle into small depressions immediately distal to this notch. The benefit of this approach is that it can be performed with the horse standing on the limb.- Structures blocked: The radiocarpal joint block is isolated only to that joint. Due to communication, the intercarpal joint block also blocks the carpal-metacarpal joint.
4) Tibial Tarsal Joint Block- Needle: 1.5 inch, 20 gauge- Volume: 10 - 20 cc- Tibiotarsal joint is approached on the dorsal-medial aspect of the hock, where the joint pouch is easily palpated. The needle is inserted directly inwards. Important to be aware of the saphenous vein and avoid during needle insertion. - When effusive, you can also attempt to inject the plantar pouches on the medial or lateral plantar aspect of the hock.- Structures blocked: The tibiotarsal itself is blocked. Due to communication, the proximal inter-tarsal joint is also blocked.
5) Distal Inter-tarsal & Tarsal-Metatarsal Joint Block - DIT Needle: 1 inch, 22 gauge- DIT Volume: 3 – 5cc- The distal intertarsal joint is injected on the medial aspect (approached from the opposite side of the horse). The limb is situated so that it is more forward than it would be during a squared-up stance. The needle is inserted into a T-shaped gap formed by the junction of the fused first & second tarsal bone, the third tarsal bone,
10

and the central tarsal bone. The T-shaped gap is immediately distal to the cuneal tendon.- TMT Needle: 1.5 inch, 20 gauge- TMT Volume: 3 – 5 cc- The tarsal-metatarsal joint is injected on the plantar-lateral aspect of the hock. The needle is inserted immediately above the head of the lateral splint bone. The needle is angled in a dorsal-medial and distal direction.- Structures blocked: In approximately 25% of cases, the distal intertarsal and tarsal-metatarsal joints communicate. In approximately 10% of cases, the distal intertarsal joint communicates higher with the proximal intertarsal & tibiotarsal joint.
6) Medial Femoral-Tibial, Femoral-Patellar, Lateral Femoral-Tibial Joint Block- Needle: 18 gauge, 1.5 inch- Volume: >20 cc- Medial Femoral-Tibial: Needle is inserted in between the medial patellar ligament and medial collateral ligament, proximal to the tibial tuberosity.- Femoral Patellar: Needle is inserted in between the medial and middle patellar ligament, proximal to the tibial tuberosity. Needle is angled upwards, towards the patellar recess.- Lateral Femoral-Tibial: Needle is inserted caudal to the lateral collateral ligament, proximal to the proximal-lateral edge of the tibia.- Structures blocked: Approximately 25% communication between femoral-patellar and medial femoral-tibial. Approximately 15% communication between femoral patellar and lateral femoral-tibial. Approximately 30% communication between medial femoral-tibial and lateral femoral-tibial
7) Other- Be aware that any synovial structure can be amendable to intra-articular, intra-bursal, or intra-thecal anesthesia if clinical examination creates suspicion. As some anatomical structures are not commonly anesthetized, review the specific injection technique in a textbook prior to performing.- Less common structures that can be anesthetized include:
o Proximal Inter-phalangeal Jointo Tendon Sheatho Carpal Canalo Elbow Jointo Shoulder Jointo Hip Joint
11

o Bicepital Bursao Navicular Bursao Tarsal Sheatho Sacroiliac Joint
CONCLUSION & TAKE HOME POINTS:• Knowledge of anatomy is essential in understanding
diagnostic perineural and intra-synovial anesthesia.• Know the mechanism of action for local anesthetics• Understand when to use blocks during your exam, how to
prepare the injection site, how to determine if block worked, etc.
• Understand what structures are blocked with each nerve or joint block.
• You will not always remember where to perform each nerve or joint block until you perform the procedures a few times. Know where to find a description so you can review the technique prior to performing the nerve/joint block clinically.
12