NephSAP Vol 8.Num 2. March 2009 Fluid, Electrolytes, And Acid-Base Disturbances
118
® Volume 8 • Number 2 • March 2009 Fluid, Electrolytes, and Acid-Base Disturbances Co-Editors: Biff F. Palmer, MD, and Richard H. Sterns, MD ■ Editor-in-Chief: Stanley Goldfarb, MD ■ Deputy Editor: Jeffrey S. Berns, MD NephSAP Nephrology Self-Assessment Program ®
-
Upload
alessandro-barilli-alves -
Category
Documents
-
view
354 -
download
19
Transcript of NephSAP Vol 8.Num 2. March 2009 Fluid, Electrolytes, And Acid-Base Disturbances

®
Volume 8 • Number 2 • March 2009
Fluid, Electrolytes, andAcid-Base DisturbancesCo-Editors:
Biff F. Palmer, MD, and
Richard H. Sterns, MD
■ Editor-in-Chief: Stanley Goldfarb, MD
■ Deputy Editor: Jeffrey S. Berns, MD
NephSAPNephrology Self-Assessment Program
®

EDITOR-IN-CHIEFStanley Goldfarb, MDUniversity of Pennsylvania Medical SchoolPhiladelphia, PA
DEPUTY EDITORJeffrey S. Berns, MDUniversity of Pennsylvania Medical SchoolPhiladelphia, PA
MANAGING EDITORGisela Deuter, BSN, MSAWashington, DC
ASSOCIATE EDITORSRajiv Agarwal, MDIndiana University School of MedicineIndianapolis, IN
David J. Cohen, MDColumbia UniversityNew York, NY
Steven Fishbane, MDStony Brook School of MedicineMinneola, NY
Richard J. Glassock, MDProfessor Emeritus, The David Geffen Schoolof Medicine at the University of CaliforniaLos Angeles, CA
Kevin J. Martin, MBBChSt. Louis University School of MedicineSt. Louis, MO
Rajnish Mehrotra, MDHarbor UCLA Research and Education InstituteTorrance, CA
Patrick T. Murray, MDUniversity College DublinDublin, Ireland
Patrick H. Nachman, MDUniversity of North CarolinaChapel Hill, NC
Paul M. Palevsky, MDUniversity of Pittsburgh School of MedicinePittsburgh, PA
Biff F. Palmer, MDUniversity of Texas Southwestern Medical CenterDallas, TX
Richard H. Sterns, MDUniversity of Rochester School of Medicineand DentistryRochester, NY
Stephen C. Textor, MDMayo ClinicRochester, MN
Raymond R. Townsend, MDUniversity of Pennsylvania Medical SchoolPhiladelphia, PA
John P. Vella, MDMaine Medical CenterPortland, ME
PrefaceNephSAP® is one of the three major publications of the American Society of Nephrology(ASN). Its primary goals are self-assessment, education, and the provision of ContinuingMedical Education (CME) credits and Maintenance of Certification (MOC) credits forindividuals certified by the American Board of Internal Medicine. Members of the ASNautomatically receive NephSAP with their monthly issue of The Journal of the AmericanSociety of Nephrology (JASN).
EDUCATION: Medical and Nephrologic information continually accrues at a rapid pace.Bombarded from all sides with demands on their time, busy practitioners, academicians,and trainees at all levels are increasingly challenged to review and understand all this newmaterial.
Each bimonthly issue of NephSAP is dedicated to a specific theme, i.e., to a specificarea of clinical nephrology, hypertension, dialysis, and transplantation, and consists of anEditorial, a Syllabus, a Commentary on the Syllabus, and self-assessment questions. Overthe course of 24 months, all clinically relevant and key elements of nephrology will bereviewed and updated. The authors of each issue digest, assimilate, and interpret keypublications from the previous issues of other years and integrate this new material with thebody of existing information.
SELF-ASSESSMENT: Twenty-five single-best-answer questions will follow the 50 to 75 pagesof Syllabus text. The examination is available online with immediate feedback. Those answer-ing �75% correctly will receive CME credit, and receive the answers to all the questions alongwith brief discussions and an updated bibliography. To help answer the questions, readers maygo to the ASN web site, where relevant material from UpToDate in nephrology will be posted.Thus, members will find a new area reviewed every 2 months, and they will be able to test theirunderstanding with our quiz. This format will help readers stay abreast of developing areas ofclinical nephrology, hypertension, dialysis, and transplantation, and the review and update willsupport those taking certification and recertification examinations.
CONTINUING MEDICAL EDUCATION: Most state and local medical agencies as well ashospitals are demanding documentation of requisite CME credits for licensure and for staffappointments. A maximum of 36 credits annually can be obtained by successfully completingthe NephSAP examination. In addition, individuals certified by the American Board of InternalMedicine may obtain credits towards Maintenance of Certification (MOC) by successfullycompleting the self-assessment portion of NephSAP.
BOARD CERTIFICATION AND INSERVICE EXAMINATION PREPARATION: Each issuewill also contain 5 questions and answers examining core topics in the particular disciplinereviewed in the Syllabus. These questions are designed to provide trainees with challengingquestions to test their knowledge of key areas of nephrology.
� This paper meets the requirements of ANSI/NISO Z39.48-1921 (Permanence of Paper),effective with July 2002, Vol. 1, No. 1.
FOUNDING EDITORSRichard J. Glassock, MD, MACP
Editor-in-Chief EmeritusRobert G. Narins, MD, MACP
NephSAP® (Print: 1536-836X; Online: 1934-3175)©2009 by The American Society of Nephrology
NephSAP®

Fluid, Electrolytes, and Acid-Base Disturbances
Editorial 61SGK1 in the Regulation of Renal Function and in the Pathogen-
esis of Salt-Sensitive Hypertension—Florian Lang, MD, Fer-ruh Artunc, MD, Teresa F. Ackermann, Daniela S. Kempe,MD, Krishna M. Boini, PhD, and Volker Vallon, MD
Commentary 66Fluid, Electrolyte, and Acid-Base Disorders—Tomas Berl, MD
Syllabus 70Fluid, Electrolyte, and Acid-Base Disturbances—Biff F. Palmer,
MD and Richard H. Sterns, MD
Potassium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .70
New Physiologic Concepts . . . . . . . . . . . . . . . . . . . . . . . . .70
Hypokalemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .73
Approach to the Patient with Hypokalemia . . . . . . . . . . . .73
Cellular Redistribution . . . . . . . . . . . . . . . . . . . . . . . . . . . .73
Extrarenal K� Loss from the Body . . . . . . . . . . . . . . . . . .76
Renal K� Wasting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .77
Primary Increase in Mineralocorticoid Activity . . . . . . .78
Increased Renin, Increased Aldosterone . . . . . . . . . . . . .78
Suppressed Renin, Increased Aldosterone . . . . . . . . . . . .78
Suppressed Renin and Aldosterone . . . . . . . . . . . . . . . . .79
Primary Increase in Distal Na� Delivery . . . . . . . . . . . . . .82
Complications and Treatment of Hypokalemia . . . . . . . . .84
NephSAP®
Volume 8, Number 2, March 2009

Hyperkalemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .88
Pseudohyperkalemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .89
Clinical Manifestation of Hyperkalemia . . . . . . . . . . . . . . .89
Excessive K� Loads: Exogenous or Endogenous . . . . . . .90
Cell Shift . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .92
Decreased Renal Excretion of K� . . . . . . . . . . . . . . . . . . .93
Primary Decrease in Mineralocorticoid Levels orActivity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .93
Primary Decrease in Distal Delivery (Acute and ChronicRenal Failure) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .94
Distal Tubular Defects . . . . . . . . . . . . . . . . . . . . . . . . . . .94
Acid Base . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .98
Metabolic Alkalosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .98
Exogenous Addition of Base . . . . . . . . . . . . . . . . . . . . . .99
Gastrointestinal Acid Loss . . . . . . . . . . . . . . . . . . . . . . . .99
Renal Acid Loss . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .100
Primary Increase in Distal Na� Delivery . . . . . . . . . . . . .100
Acetazolamide in Metabolic Alkalosis Treatment . . . . . .102
Metabolic Acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .103
New Physiologic Insights . . . . . . . . . . . . . . . . . . . . . . . . .103
Clinical Approach to Metabolic Acidosis . . . . . . . . . . . . . .105
Lactic Acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .106
Diabetic Ketoacidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . .107
Starvation Ketosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .109
Alcoholic Ketoacidosis . . . . . . . . . . . . . . . . . . . . . . . . . . .109
Ethylene Glycol and Methanol Poisoning . . . . . . . . . . . .109
Pyroglutamic Acidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . .110
Normal (Hyperchloremic) Anion Gap Acidosis . . . . . . . .110
NephSAP®
Volume 8, Number 2, March 2009

Extrarenal Causes of Normal (Hyperchloremic) Anion GapAcidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .110
Renal Causes of Normal (Hyperchloremic) Anion GapAcidosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .110
Hyponatremia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .114
Isotonic and Hypertonic Hyponatremia . . . . . . . . . . . . . .114
Pseudohyponatremia . . . . . . . . . . . . . . . . . . . . . . . . . . . . .115
Solute-Induced Nonhypotonic Hyponatremia . . . . . . . . . .116
Hypotonic Hyponatremia . . . . . . . . . . . . . . . . . . . . . . . . . . .117
Brain Responses to Hyponatremia . . . . . . . . . . . . . . . . . .117
Brain Responses to Correction of Hyponatremia: OsmoticDemyelination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .119
Acute Hyponatremia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .121
Exercise-Associated Hyponatremia . . . . . . . . . . . . . . . . . .122
Self-Induced Water Intoxication in Psychosis . . . . . . . . .124
Postoperative Hyponatremia . . . . . . . . . . . . . . . . . . . . . . .125
Chronic Hyponatremia . . . . . . . . . . . . . . . . . . . . . . . . . . . . .126
Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .126
Differential Diagnosis of Chronic Hyponatremia . . . . . .127
SIAD versus Cerebral Salt Wasting . . . . . . . . . . . . . . . . .128
Symptoms of Chronic Hyponatremia . . . . . . . . . . . . . . . .129
Beer Potomania . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .130
Drug-Induced Hyponatremia . . . . . . . . . . . . . . . . . . . . . . .131
Tumor-Associated Hyponatremia . . . . . . . . . . . . . . . . . . .132
Pneumonia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .132
Endocrine Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . .133
Meningitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .134
Traumatic Brain Injury . . . . . . . . . . . . . . . . . . . . . . . . . . .134
Cirrhosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .134
NephSAP®
Volume 8, Number 2, March 2009

Heart Failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .135
Treatment Options for Hypotonic Hyponatremia . . . . . . .136
Treatment Goals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .136
Water Restriction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .137
Hypertonic Saline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .137
Vasopressin Receptor Antagonists . . . . . . . . . . . . . . . . .138
Desmopressin for Overcorrection. . . . . . . . . . . . . . . . . .139
Hypernatremia and Diabetes Insipidus . . . . . . . . . . . . . . . . .142
Basic Mechanisms of Osmoregulation . . . . . . . . . . . . . . .142
Age-Related Hypodipsia . . . . . . . . . . . . . . . . . . . . . . . . . .144
Renal Concentrating Mechanism . . . . . . . . . . . . . . . . . . .144
Hypernatremia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .145
Therapeutic Hypernatremia . . . . . . . . . . . . . . . . . . . . . . . .146
Diabetes Insipidus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .147
Central DI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .147
Adipsic DI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .148
Acquired Nephrogenic DI . . . . . . . . . . . . . . . . . . . . . . . . .149
Lithium . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .149
Hypercalcemia and Hypercalciuria . . . . . . . . . . . . . . . .150
Congenital Nephrogenic DI . . . . . . . . . . . . . . . . . . . . . .150
Nocturnal Enuresis and Nocturnal Polyuria . . . . . . . . .151
CME Self-Assessment Questions . . . . . . . . . . . . . . . . . . . . . 154Questions Linked to UpToDate in Green
Core Knowledge Questions. . . . . . . . . . . . . . . . . . . . . . . . . . 164
Upcoming Issues
Acute Kidney Injury and Critical Care Nephrology—
Paul M. Palevsky, MD, and Patrick T. Murray, MD . . . . . . . .May 2009
NephSAP®
Volume 8, Number 2, March 2009

Interventional Nephrology—
Arif Asif, MD, and Anil Agarwal, MD . . . . . . . . . . . . . . . . . .July 2009
Chronic Kidney Disease and Progression—
Jeffrey S. Berns, MD, and Steven Fishbane, MD. . . . . .September 2009
Transplantation—
John P. Vella, MD, and David J. Cohen, MD. . . . . . . .November 2009
Primary Care for the Nephrologist—Denise M. Dupras, MD, PhD . . . . . . . . . . . . . . . . . . . . .January 2010
NephSAP®
Volume 8, Number 2, March 2009

Disclosure of Unapproved or Off-Label Usage:This educational activity may contain discussion of published and/or investigational uses of agents that are not currently labeled for useby the US Food and Drug Administration (FDA). The faculty have been informed of their responsibility to disclose to the audience ifthey will be discussing off-label or investigation uses. The American Society of Nephrology does not recommend the use of any agentoutside of the labeled indications. Please refer to the official prescribing information for each product for discussion of approved indi-cations, contraindications and warnings.
Commercial Support:There is no commercial support for this issue.
NephSAP®
Volume 8, Number 2, March 2009

EditorialSGK1 in the Regulation of Renal Function and in the Pathogenesis ofSalt-Sensitive Hypertension
Florian Lang, MD* Ferruh Artunc, MD† Teresa F. Ackermann,* Daniela S. Kempe, MD*Krishna M. Boini, PhD* and Volker Vallon, MD‡
Departments of *Physiology and †Nephrology, University of Tubingen, Tubingen, Germany;and ‡Departments of Medicine and Pharmacology, University of California, San Diego, andVeterans Affairs San Diego Healthcare System, San Diego, California
In the past several years, new information hasemerged on the complex regulatory network that governsrenal control of electrolyte and water balance. In additionto the molecular and atomic specificity of various chan-nel proteins, signaling pathways have emerged centeringon enzymatic mechanisms of protein phosphorylationwell beyond the familiar G-protein cAMP system. Thefollowing brief review highlights some recent literaturethat is beginning to form the view that one particularenzyme system, the serum- and glucocorticoid-induciblekinase 1 (SGK1), is a central regulator of a myriad ofrenal functions and electrolyte balance. It may play acentral role in the hypertension associated with the met-abolic syndrome through its key role in regulating thesodium retention associated with high insulin levels.
SGK1 serves a wide variety of functions, includingstimulation of renal ion channels, carriers, and the Na�/K�-ATPase, and is emerging as an important factor inthe regulation of renal Na� retention and K� elimination.In addition, it has been shown in a variety of animalmodels to regulate mineralocorticoid stimulation of saltappetite, glucocorticoid stimulation of the Na�/H� ex-changer and nutrient transport, insulin-dependent saltsensitivity of BP, salt sensitivity of peripheral glucoseuptake, and renal and cardiac fibrosis attributed to min-eralocorticoid hormones and salt excess. A commonSGK1 gene variant (3 to 5% prevalence in Caucasianindividuals, 10% in African individuals) is associatedwith obesity, hypertension, and development of diabetes.Owing to space limitation, this editorial cannot cite themany excellent original articles contributing to our cur-rent knowledge. Instead, the reader is encouraged tocollect pertinent references from previous reviews (1,2).
SGK1 was originally cloned as an immediateearly gene transcriptionally stimulated by serum andglucocorticoids in rat mammary tumor cells (3). Thehuman isoform was discovered as a cell volume–regulated gene, which is upregulated by cell shrinkage(for review, see reference [1]). SGK1 expression isubiquitous but may vary profoundly among differentcells. Within cells, SGK1 may be localized in nuclei,cytosol, or mitochondrial membranes (3).
Regulation of SGK1 Transcription and ActivitySGK1 transcription is affected by a wide variety of
hormones, cytokines, medications, and clinical condi-tions such as glucocorticoids, mineralocorticoids, 1,25-dihydroxyvitamin D3 [1,25(OH)2D3], TGF-�, IL-6, en-dothelin, peroxisome proliferator–activated receptor �(PPAR-�) agonists, hyperglycemia, metabolic acidosis,ischemia, heat shock, and oxidative stress (1,4–6).SGK1 transcription is inhibited by nucleotides, heparin,and mutations in the MECP2 gene (1,7). Signaling in-volved in stimulation of SGK1 transcription includesincrease of cytosolic Ca2� concentration, protein kinaseC and other kinases, cAMP, nitric oxide, and otherfactors (1,8). The rat SGK1 gene promoter containsseveral transcription factor–binding sites, including theglucocorticoid, mineralocorticoid, progesterone, and vi-tamin D receptors, PPAR-�, and others. SGK1 is acti-vated by phosphorylation through a signaling cascadeinvolving phosphatidylinositol-3-kinase, the 3-phospho-inositide–dependent kinase PDK1, and mammaliantarget of rapamycin in a cascade and is activated byinsulin, IGF-1, and other growth factors and hormones(1) (Figure 1).
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009
61

SGK1-Dependent Transport RegulationAs listed in Table 1, SGK1 regulates a wide variety
of transport systems. The first channel shown to beregulated by SGK1 was the renal epithelial Na� channel(ENAC). Mechanisms implicated in SGK1-dependentregulation of ENaC include (1) direct phosphorylation ofENaC protein (1); (2) phosphorylation of the ubiquitinligase Nedd4-2, which otherwise ubiquitinates ENaC andthus prepares the channel protein for degradation; SGK1-dependent phosphorylation fosters binding of Nedd4-2 to14-3-3, thereby impeding the interaction of Nedd4-2 withENaC; (3) phosphorylation of WNK4, a kinase thatinhibits ENaC activity (9); (4) inhibition of induciblenitric oxide synthase, thereby blunting the inhibitoryeffect of nitric oxide on ENaC activity; and (5) stimula-tion of ENaC transcription (10). The stimulation ofENaC activity by mineralocorticoids is only partiallydependent on the presence of SGK1, whereas the stim-
ulation of ENaC by antidiuretic hormone or insulin fullydepends on SGK1. The sum of these effects results inincreased ENaC at the cell surface and an increase insodium transport.
SGK1 affects the activity of a host of renal trans-porters; it increases the activity of the Na�/K�-ATPase,an effect at least partially due to enhanced Na�/K�-ATPase abundance in the cell membrane, enhancesabundance in the plasma membrane of the epithelialCa2� channel TRPV5, and stimulates a variety of K�
channels (Table 1), including the renal outer medullaryK� channel ROMK1 (1). SGK1 activates ROMK1 ac-tivity by increasing the channel protein abundance in theplasma membrane, and by direct phosphorylation of thechannel protein. SGK1 also stimulates a variety of Cl�
channels (Table 1) including the Cl� channel complexClC-Ka,b/barttin (1,11), the Na�/H� exchanger NHE3(12), the Na�,K�,2Cl� co-transporter NKCC2, and pre-
Figure 1. Renal transport systems regulated by SGK1. Transport systems in proximal tubule, thick ascending limb, early distaltubule, and collecting duct, which have been shown either in Xenopus oocytes or in vivo to be regulated by SGK1. Note that SGK1may be expressed in proximal tubules and thick ascending limbs only under distinct physiologic or pathophysiologic conditions,such as hyperglycemia. Only under those conditions may SGK1 contribute to transport regulation in those nephron segments.
62 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

sumably the Na�,Cl� co-transporter NCC (13). SGK1also stimulates several glucose transporters, including theNa�-glucose co-transporter SGLT1 and the facilitativeglucose transporters GLUT1 and GLUT4 (14), and up-regulates a variety of amino acid transporters, theNa�,dicarboxylate co-transporter NaDC-1, and others(1,15–17). As is shown next, defects in the function ofSGK1 induced by genetic manipulation produce impor-tant defects in sodium conservation when animals areplaced on a sodium-restricted diet. Conversely, theSGK1 gene variant noted already may be associated withexcess rates of sodium transport and other cellular eventsleading to pathogenetic disturbances in BP control andglucose metabolism.
SGK1-Dependent Regulation of Salt Appetite andRenal Electrolyte Excretion
Effects on Renal Sodium RegulationRenal tubular SGK1 expression is most abundant
in kidney medulla and distal nephron but may extend toglomeruli, proximal tubules, and thick ascending limb
(1). As indicated already, SGK1 stimulates a variety ofrenal epithelial ion channels, carriers, and Na�/K�-AT-Pase. Thus, SGK1 participates in the regulation of renalNa� excretion by aldosterone, insulin, and IGF-1 (1).
In addition to the widely known renal transporteffects of mineralocorticoids, salt appetite is stimulatedby mineralocorticoids, an effect largely dependent on thepresence of SGK1 (1). An increase of salt intake typi-cally seen after mineralocorticoid hormone administra-tion is blunted in SGK1-deficient mice (sgk1�/�) ascompared with their wild-type littermates (sgk1�/�).sgk1�/� mice suffer from subtle impairment of renal saltretention (1,13). Under normal salt intake, arterial BP andsalt excretion are similar in sgk1�/� and sgk1�/� mice,but plasma aldosterone concentrations are significantlyhigher in sgk1�/� mice, pointing to volume depletion inthose mice (1). After NaCl-deficient diet, sgk1�/� micewaste sodium compared with normal mice despite moreprofound increase of plasma aldosterone concentration,decrease of arterial BP, decrease of GFR, and enhancedproximal tubular Na� reabsorption.
Table 1. Channels, carriers, and pumps known to be regulated by SGK1
Ion channelsENaC Epithelial Na� channelROMK1 Renal outer medullary K� channelTRPV5 Renal epithelial Ca2� channelClC-Ka/barrtin Renal (and stria vascularis) epithelial Cl� channelClC2 Ubiquitous Cl� channelCFTR Cystic fibrosis transmembrane conductance regulatorSCN5A Cardiac voltage-gated Na� channelKCNE1/KCNQ1 Cardiac and epithelial K� channelsKCNQ4 Inner ear K� channelsKv1.3, Kv1.5, and Kv4.3 Voltage-gated K� channels4F2/LAT Cation channels created by oxidation of the amino acid transporter
complex 4F2/LATGluR6 Glutamate receptors (cation channel)
Carriers and pumpsNHE3 Na�/H� exchangerNKCC2 Na�,K�,2Cl� co-transporterNCC Na�,Cl� co-transporterSGLT1 Na�-coupled glucose co-transporterGLUT1 and GLUT4 Facilitative glucose transportersASCT2 Amino acid transporterSN1 Glutamine transporterEAAT1, EAAT2, EAAT3, EAAT4, EAAT5 Glutamate transportersSMIT Na�, myoinosital cotransporterNaDC-1 Na�,dicarboxylate co-transporterCreaT Creatine transporterNaPiIIb Na�-coupled phosphate carrier in intestineNa�/K�-ATPase Na�/K� pump
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 63

According to a recent study, the salt loss ofsgk1�/� mice may at least in part be the result ofdecreased expression of the Na�,Cl� co-transporter pro-tein, whereas, presumably as a result of hyperaldosteron-ism, under salt-depleted diet, ENaC activity was evenenhanced in sgk1�/� mice (13). Clearly, upregulation ofENaC by aldosterone does not require the participation ofSGK1, and the hypertensive effect of acute hyperaldo-steronism is similar in sgk1�/� and sgk1�/� mice. Con-versely, SGK1 deficiency virtually abrogates the antina-triuretic effect of insulin and antidiuretic hormone (i.e.,renal Na� excretion is lowered after insulin infusion insgk1�/� mice but not sgk1�/� mice [1]).
Effects on Renal Potassium RegulationDeficiency of SGK1 activity leads to impaired
excretion of K�. The sgk1�/� mice fail to rapidlyexcrete an acute K� load, and during a chronic K�
load, plasma K� concentration increases more sharplyin sgk1�/� mice than in sgk1�/� mice (reviewed inreference [1]) despite increased basal plasma aldoste-rone levels, which should favor K� elimination. SGK1further participates in the stimulation of cellular K�
uptake by insulin. Accordingly, the hypokalemic re-sponse to administration of insulin and glucose issignificantly blunted in sgk1�/� mice (18).
Despite the ability of SGK1 to stimulate theTRPV5 Ca2� channel and despite decreased TRPV5expression in sgk1�/� mice, renal Ca2� excretion israther decreased in sgk1�/� mice (for review, seereference [1]). The salt depletion of sgk1�/� miceupregulates renal tubular Na� and presumably Ca2�
reabsorption in proximal renal tubules and possibly thickascending limbs.
Under normal conditions, SGK1 is not expressed inproximal renal tubules and thus does not participate inthe regulation of proximal renal tubular transport; how-ever, hyperglycemia may stimulate SGK1 expressionthroughout the kidney, including proximal renal tubules,raising the possibility that, in diabetes, SGK1 may stim-ulate renal tubular nutrient transport by upregulation ofthe respective carriers (e.g., SGLT1, EAAT3) and byenhancing the driving force through stimulation of theapical K� channel and the basolateral Na�/K�-ATPase.SGK1-dependent renal salt retention could also contrib-ute to the development of edema after administration ofPPAR-� agonists, in nephrotic syndrome, and duringascites formation (1,19).
Putative Role of SGK1 in Metabolic SyndromeHypertension, obesity, insulin resistance, and
type 2 diabetes are typical characteristics of metabolicsyndrome, and there has been speculation that excessSGK1 may contribute to development of some fea-tures of this syndrome. The influence of SGK1 on saltintake and elimination render the SGK1 gene a can-didate for the development of hypertension. A distinctSGK1 gene variant (combined polymorphisms in in-tron 6 [I6CC] and in exon 8 [E8CC/CT]) is indeedassociated with moderately elevated BP (1). TheSGK1 gene variant affects 3 to 5% of a Caucasianpopulation and approximately 10% of an African-American population (20). Individuals who carry thisgene variant are particularly prone to develop hyper-tension during hyperinsulinemia. Thus, SGK1 may beimportant or even necessary for the hypertension thatis caused by hyperinsulinemia. In support of thistheory is the observation that induction of hyperinsu-linemia sensitized BP to high-salt intake in sgk1�/�
but not in sgk1�/� mice (1).Carriers of the I6CC/E8CC/CT SGK1 gene vari-
ant further suffer from enhanced body mass index (forreview, see reference [1]). The gene variant thus pre-disposes to obesity in addition to its effect on BPcontrol. The obesity is possibly due to stimulation ofSGK1-dependent intestinal SGLT1 activity leading toaccelerated intestinal glucose absorption and enhancedglucose deposition in peripheral tissues by stimulationof the glucose transport protein, GLUT1. Presumably as aresult of enhanced prevalence of obesity, carriers of theI6CC/E8CC/CT SGK1 gene variant are more prone todevelop type 2 diabetes compared with individuals with-out the gene variant (20). Although additional experi-mental effort is needed to define the putative role ofSGK1 in the development of metabolic syndrome, inter-estingly, in experiments in genetically manipulated mice,the metabolic syndrome of offspring after dietary stress(low-protein diet) of the mother, a result of so-called fetalprogramming, seems to be dependent on maternal SGK1(21).
Some patients who have ESRD and have arterialhypertension express a Nedd4-2 variant (P355LNedd4-2)with enhanced sensitivity to phosphorylation by SGK1.This genetic variant would result in increased ENaCactivity and thus be prone to salt-sensitive hypertension.This observation further underlines the role of SGK1 inthe development of hypertension.
64 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

SGK1-Sensitive Renal Fibrosis and ProteinuriaBeyond its effect on renal tubular transport and BP,
SGK1 has been implicated in renal and extrarenal fibro-sing disease, such as diabetic nephropathy, glomerulone-phritis, liver cirrhosis, and cardiac fibrosis (1,22,23).SGK1 may be particularly important in diabetic nephrop-athy, because it is upregulated by excessive glucoseconcentrations and mediates the upregulation of connec-tive tissue growth factor (1). SGK1 is also expressed inpodocytes and upregulated in those cells by aldosteroneand oxidative stress (6,24). Experimental studies haveshown that proteinuria during mineralocorticoid and saltexcess is significantly more pronounced in sgk1�/� micethan in sgk1�/� mice (25).
ConclusionsThis brief review highlights how genetic tech-
niques that allow studying targeted gene expression inexperimental animals can provide important insightsinto the role of renal transport systems in the patho-genesis of disorders of wide clinical impact. Furtherstudies of the SGK1 system hold promise for provid-ing important insights into disease pathogenesis, andone may anticipate development of therapeutic agentsthat target this important regulatory system.
References1. Lang F, Bohmer C, Palmada M, Seebohm G, Strutz-Seebohm N, Vallon V:
(Patho)physiological significance of the serum- and glucocorticoid-inducible kinase isoforms. Physiol Rev 86: 1151–1178, 2006
2. Verrey F, Fakitsas P, Adam G, Staub O: Early transcriptional control ofENaC (de)ubiquitylation by aldosterone. Kidney Int 73: 691–696, 2008
3. Firestone GL, Giampaolo JR, O’Keeffe BA: Stimulus-dependentregulation of the serum and glucocorticoid inducible protein kinase(Sgk) transcription, subcellular localization and enzymatic activity.Cell Physiol Biochem 13: 1–12, 2003
4. Chang CT, Wu MS, Tian YC, Chen KH, Yu CC, Liao CH, HungCC, Yang CW: Enhancement of epithelial sodium channel expres-sion in renal cortical collecting ducts cells by advanced glycationend products. Nephrol Dial Transplant 22: 722–731, 2007
5. Kim MJ, Chae JS, Kim KJ, Hwang SG, Yoon KW, Kim EK, Yun HJ,Cho JH, Kim J, Kim BW, Kim HC, Kang SS, Lang F, Cho SG, ChoiEJ: Negative regulation of SEK1 signaling by serum- and glucocorti-coid-inducible protein kinase 1. EMBO J 26: 3075–3085, 2007
6. Shibata S, Nagase M, Yoshida S, Kawachi H, Fujita T: Podocyte asthe target for aldosterone: Roles of oxidative stress and Sgk1.Hypertension 49: 355–364, 2007
7. Li L, Wingo CS, Xia SL: Downregulation of SGK1 by nucleotidesin renal tubular epithelial cells. Am J Physiol Renal Physiol 293:F1751–F1757, 2007
8. Poulin H, Filion C, Ladanyi M, Labelle Y: Serum- and glucocorticoid-regulated kinase 1 (SGK1) induction by the EWS/NOR1(NR4A3)fusion protein. Biochem Biophys Res Commun 346: 306–313, 2006
9. Ring AM, Leng Q, Rinehart J, Wilson FH, Kahle KT, Hebert SC,Lifton RP: An SGK1 site in WNK4 regulates Na� channel and K�
channel activity and has implications for aldosterone signaling andK� homeostasis. Proc Natl Acad Sci U S A 104: 4025–4029, 2007
10. Zhang W, Xia X, Reisenauer MR, Rieg T, Lang F, Kuhl D, VallonV, Kone BC: Aldosterone-induced Sgk1 relieves Dot1a-Af9-medi-ated transcriptional repression of epithelial Na� channel alpha.J Clin Invest 117: 773–783, 2007
11. Bergler T, Stoelcker B, Jeblick R, Reinhold SW, Wolf K, RieggerGA, Kramer BK: High osmolality induces the kidney-specificchloride channel CLC-K1 by a serum and glucocorticoid-induciblekinase 1 MAPK pathway. Kidney Int 74: 1170–1177, 2008
12. Wang D, Zhang H, Lang F, Yun CC: Acute activation of NHE3 bydexamethasone correlates with activation of SGK1 and requires afunctional glucocorticoid receptor. Am J Physiol Cell Physiol 292:C396–C404, 2007
13. Fejes-Toth G, Frindt G, Naray-Fejes-Toth A, Palmer LG: EpithelialNa� channel activation and processing in mice lacking SGK1. Am JPhysiol Renal Physiol 294: F1298–F1305, 2008
14. Jeyaraj S, Boehmer C, Lang F, Palmada M: Role of SGK1 kinase inregulating glucose transport via glucose transporter GLUT4. Bio-chem Biophys Res Commun 356: 629–635, 2007
15. Shojaiefard M, Strutz-Seebohm N, Tavare JM, Seebohm G, Lang F:Regulation of the Na(�), glucose cotransporter by PIKfyve and theserum and glucocorticoid inducible kinase SGK1. Biochem BiophysRes Commun 359: 843–847, 2007
16. Strutz-Seebohm N, Shojaiefard M, Christie D, Tavare J, SeebohmG, Lang F: PIKfyve in the SGK1 mediated regulation of the creatinetransporter SLC6A8. Cell Physiol Biochem 20: 729–734, 2007
17. Klaus F, Palmada M, Lindner R, Laufer J, Jeyaraj S, Lang F,Boehmer C: Up-regulation of hypertonicity-activated myo-inositoltransporter SMIT1 by the cell volume-sensitive protein kinaseSGK1. J Physiol 586: 1539–1547, 2008
18. Boini KM, Graf D, Kuhl D, Haussinger D, Lang F: SGK1 depen-dence of insulin induced hypokalemia. Pflugers Arch July 30, 2008[epub ahead of print]
19. Artunc F, Nasir O, Amann K, Boini KM, Haering HU, Risler T,Lang F: Serum- and glucocorticoid-inducible kinase 1 in doxorubi-cin-induced nephrotic syndrome. Am J Physiol Renal Physiol 295:F1624–F1634, 2008
20. Schwab M, Lupescu A, Mota M, Mota E, Frey A, Simon P, MertensPR, Floege J, Luft F, Asante-Poku S, Schaeffeler E, Lang F:Association of SGK1 gene polymorphisms with type 2 diabetes.Cell Physiol Biochem 21: 151–160, 2008
21. Rexhepaj R, Boini KM, Huang DY, Amann K, Artunc F, Wang K,Brosens JJ, Kuhl D, Lang F: Role of maternal glucocorticoidinducible kinase SGK1 in fetal programming of blood pressure inresponse to prenatal diet. Am J Physiol Regul Integr Comp Physiol294: R2008–R2013, 2008
22. Nishimura H, Ito Y, Mizuno M, Tanaka A, Morita Y, Maruyama S,Yuzawa Y, Matsuo S: Mineralocorticoid receptor blockade amelio-rates peritoneal fibrosis in new rat peritonitis model. Am J PhysiolRenal Physiol 294: F1084–F1093, 2008
23. Terada Y, Kuwana H, Kobayashi T, Okado T, Suzuki N, Yoshimoto T,Hirata Y, Sasaki S: Aldosterone-stimulated SGK1 activity mediates profi-brotic signaling in the mesangium. J Am Soc Nephrol 19: 298–309, 2008
24. Nagase M, Yoshida S, Shibata S, Nagase T, Gotoda T, Ando K,Fujita T: Enhanced aldosterone signaling in the early nephropathy ofrats with metabolic syndrome: Possible contribution of fat-derivedfactors. J Am Soc Nephrol 17: 3438–3446, 2006
25. Artunc F, Amann K, Nasir O, Friedrich B, Sandulache D, Jahovic N,Risler T, Vallon V, Wulff P, Kuhl D, Lang F: Blunted DOCA/highsalt induced albuminuria and renal tubulointerstitial damage ingene-targeted mice lacking SGK1. J Mol Med 84: 737–746, 2006
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 65

CommentaryFluid, Electrolyte, and Acid-Base DisordersTomas Berl, MDDepartment of Medicine, University of Colorado Denver, Division of Renal Diseases andHypertension, Aurora, Colorado
The authors of this issue of NephSAP, Drs.Sterns and Palmer, undertook a thorough review andupdate of the developments in the area of electrolytesand acid-base disorders. More than any other aspect ofour specialty, the one reviewed in this issue is almostentirely devoid of prospective, controlled trials. Theauthors therefore had to rely primarily on small observa-tional studies and illustrative case reports. Nonetheless,they are to be commended for the clarity of the presen-tation reflecting their well-established credentials as out-standing teachers who can put forth complex conceptsand make them readily understandable.
This issue contains a particularly lucid descrip-tion of the cellular mechanisms by which the WNK4kinase allows for the dissociation of the effects ofaldosterone to retain sodium and excrete potassium(K). The text and Figure 1 clearly depict how thiskinase modulates the activity of the Na-Cl co-trans-porter to enhance sodium retention and independentlycontrols SGK1 phosphorylation of WNK4 to promoteK excretion. Equally provocative is the discussion onthe kidney-specific short WNK1 and how its relationto a longer WNK1 is modulated by K intake and canaffect K excretion, lead to sodium retention, and po-tentially have a role in sodium-sensitive hypertension,making these kinases attractive targets for new anti-hypertensive drugs.
Dyskalemic Disorders
HypokalemiaThe discussion on the approach to the patient
with hypokalemia is worthy of any textbook. Of par-ticular value is the interpretation of urinary K and thelimitations of the transtubular K gradient (TTKG) inthe diagnosis of disorders of plasma K concentration,emphasizing that its most valuable role may be in the
discrimination between aldosterone deficiency and al-dosterone resistance; an increment in TTKG after theadministration of a mineralocorticoid supports a diag-nosis of aldosterone deficiency.
Although most of the clinical settings associatedwith redistribution of K into cells are well known tomost clinicians, the author weaves in some less rec-ognized causes, such as hydrofluoric acid dermal in-jury, hydroxycloroquine overdose, and use of pegy-lated interferon in a thyrotoxic patient. In this regard,the erudite discussion on periodic paralysis, both ge-netic and acquired, is worthy of mention. A referenceto � adrenergic agents, that in their long-acting formcan cause substantial decrements in serum K, is sur-prisingly absent from what is otherwise a very com-prehensive review of translocational hypokalemias.
Several other aspects of the update on hypokale-mic disorders are also noteworthy. One refers to theemerging concept that there may be gastrointestinalsensors and factors that control the renal excretion ofnot only K but also sodium and phosphate. As itrelates to K, the nature of the factor has not beendetermined but does not seem to be insulin. The othernoteworthy discussion revolves around the increasingunderstanding of the biology of the epithelial sodiumchannel, which is central not only to K homeostasisbut also to the renal control of sodium excretion andthereby of BP. Modulation of channel activity byubquitination and phosphorylation mediated by extra-cellular signal–regulated kinase are just two examplesof biochemical events that can increase or decreasechannel activity, respectively. On a more clinicallyrelevant note, the discussion on diuretic induced Klosses and the influence of sodium intake is particu-larly pertinent, emphasizing the importance of moder-ate sodium intake, because both very high and verylow intakes of sodium can enhance renal losses of K
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009
66

by different mechanisms. It is important also to pointout studies that link the hypokalemia that is associatedwith thiazide administration to glucose intolerance andan increase in blood sugar. This is most likely medi-ated by a mechanism that involves a failure to secreteinsulin normally under kaliopenic conditions, ratherthan peripheral insulin resistance.
HyperkalemiaIn this section of the syllabus, after highlighting
the insensitivity of the electrocardiogram as a prog-nosticator of hyperkalemic arrhythmias and cardiacarrest, the author has amassed a fascinating group ofcase reports, many unusual and rare, but nonethelessinteresting that can lead to hyperkalemia by excessiveexogenous or endogenous loads of K even in thebackground of normal renal function. Such a commentalso applies to causes for cell shifts of K out of cells.Of greater clinical relevance is the increasing inci-dence of hyperkalemia associated with attempts toinhibit more fully the renin-angiotensin-aldosteronesystem (RAAS) by a variety of combination treat-ments. Although the syllabus does make reference tothis problem, it is in my view underemphasized. Nu-merous studies have now reported an increased risk forhyperkalemia with combination RAAS inhibiting orblocking regimens, even at a time when their cardio-vascular and renal protective effects are being increas-ingly questioned (see results of the ONTARGET trial).Finally, this section has an elegant discussion of themechanism of distal tubular defects that lead to hyper-kalemia such as the role of mutations in the afore-mentioned WNK4 in the pathogenesis of pseudohy-poaldosteronism type II, also designated as Gordon’ssyndrome, which is characterized by hypertension andhyperkalemic metabolic acidosis. By enhancing clath-rin-dependent endocytosis of the ROMK channel, pa-tients with these mutations have decreased cell surfaceexpression of this channel that is vital for K secretion.
Acid-Base Disorders
Metabolic AlkalosisThe most novel aspect of this section of the
syllabus relates to the recognition that alteration in thetransepithelial transport of chloride and bicarbonate,which are critical to the function of many epithelia,can culminate in metabolic alkalosis. Thus, for exam-
ple, congenital chloride diarrhea seems to be a conse-quence of a mutation in the solute carrier family 26member 3 gene (SCLC26A3) affecting the function ofthe colonic Cl�/HCO3 exchangers. Similar defectsoccur in other syndromes and may contribute to themetabolic alkalosis that is seen in infants with cysticfibrosis. As regards inherited disorders that lead tometabolic alkalosis, the use of a thiazide test to dis-tinguish Bartter syndrome from Gitelman syndrome isof interest. Because the latter group is afflicted by amutation of the thiazide-sensitive Na-Cl co-trans-porter, they do not increase their fractional excretionof chloride with this diuretic, whereas those withBartter (as well as pseudo-Bartter) syndrome do.
Metabolic AcidosisThe authors present a lucid description of the
mechanisms involved in tubular H secretion and itscontrol. It must be noted, however, that any role ofangiotensin II on the renal handling of ammonia mustbe viewed as preliminary and of questionable clinicalsignificance, because there is no clinical evidence thatinhibition of angiotensin II action results in acid-basederangements, an effect that would have been ob-served given the widespread use of such drugs.
The section on the clinical approach to metabolicacidosis is equally erudite. Besides alluding to thecommon clinical settings, the section is punctuated bya hefty number of case reports of unusual causes ofmetabolic acidosis brought about by various drugingestions. Among these, the different alcohols play aprominent role. In their discussion of ethanol versusfomepizole in the treatment of certain alcohol inges-tions, the latter is described as the treatment of choice.Although it clearly has many advantages over ethanol,the cost exceeds 5000 USD for a 48-h treatment and isnot available in all settings, a more comprehensivediscussion of the relative merits of each treatmentmodality might be useful in future NephSAP editions.
The renal tubular acidoses are clearly described.Of particular note is the description of an alternativetest to diagnose the distal variety of this disorder. Few,if any, nephrologists have ever used the classicalNH4Cl loading test to ascertain that the patient cannotnormally acidify the urine. An alternative test involv-ing the simultaneous administration of fludrocortisoneand furosemide seems to be well tolerated, is simpler,and provides the same degree of diagnostic accuracy.
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 67

Dysnatremic Disorders
HypornatremiaAs the most common electrolyte disorder in
clinical medicine, the update on hypernatremia is ofparticular importance. The opening section onpseudohyponatremia includes the formula recently de-rived by Nguyen and his collaborators from studiesperformed in their laboratory involving the addition oflipids and proteins to plasma. This formula is likely tobe the best yet to arrive at a correction for watercontent when these large molecules take up a largevolume of the measured samples.
The adaptive responses of the brain to changes intonicity have been the subject of great interest. Thereare significant intraindividual variations in the adap-tive response to decrements in tonicity and the degreeof brain edema that follows the onset of hyponatremia.The observation that the levels of expression of aqua-porin 4 can determine the degree of brain swellingraises the possibility that variability in the expressionof this water channel could underlie the observeddifferences. Likewise, because the adaptation also in-volves the release of organic osmolytes, variation in Gprotein–coupled receptors involved in their releaseprovide another potential source for the variability.Furthermore, the pathogenesis of the osmotic demy-elination remains poorly understood. Recent studiespointing to a downregulation of neutral amino acidtransporters SNAT2 during hypotonicity, particularlyin oligodendrocytes (the cells most affected by thispathologic process), by delaying the reaccumulation ofosmolytes during the correction phase may shed somelight on the pathogenesis of this often devastatingcomplication of treatment. The authors correctly al-lude to the protective effects of urea and for complete-ness refer to a case that was reported in a dialysispatient. This is a very rare occurrence considering thelarge number of such patients who undergo correctionof hyponatremia on an ongoing basis in this setting.
In view of the increasing interest in exercise-induced hyponatremia, the syllabus deals extensivelywith this subject, summarizing studies that examinedthe endocrine responses to exercise and attempts tomonitor sodium and water balances, including thecontributions of sweat. What emerges is that nonos-motic vasopressin secretion is a mediator of the pro-cess and that weight gain, reflecting excessive waterintake, underlies much of the problem. It is pertinent to
emphasize the conclusions of the consensus confer-ence pointing to the importance of administering 100ml of 3% NaCl as the initial treatment for individualswho present with cerebral symptoms in this setting.
The very comprehensive and thoughtful updateon hyponatremia also brings into focus several otherimportant issues. The first of these is the difficultyencountered in differentiating euvolemic from hypo-volemic hyponatremia. None of the tools available—the spot urinary sodium concentration, the fractionalexcretion of sodium, the fractional excretion of urea,the fractional excretion of uric acid, or the response toisotonic saline—either alone or in combination, canreliably discriminate these entities. Along the samelines, it is equally challenging to establish that patientsdesignated as having cerebral salt wasting truly havethis entity. The other emerging view is the recognitionthat hyponatremia may not be entirely asymptomaticeven when it seems to be so. Given the cellularadaptive mechanisms that come into play with chronichyponatremia, this is perhaps not surprising. A re-cently described gait disturbance has been comple-mented by the increase risk for fractures in this pop-ulation. This section also reviews recent publicationson the emergence of vasopressin antagonists in thetreatment of hyponatremic disorders in both euvolemicand hypervolemic conditions. Although at this timeonly one intravenous form of the drug is available(conivaptan), the release of oral agents is under activediscussion with the Food and Drug Administration.Finally, the increasingly accepted view that DDAVPcan and should be used for overcorrection of hypona-tremia to prevent a demyelinating syndrome is clearlyworthy of the reader’s careful attention.
Hypernatremia and Diabetes InsipidusThe introduction to this section of the syllabus
has a detailed summary on osmoregulation and thecellular mechanisms involved in the perception ofchanges in tonicity. Of interest is the recent descrip-tion of the importance of transient receptor potentialvanilloid channels in the response of osmoreceptorneurons to changes in tonicity, as studied in knockoutmice deficient in transient receptor potential vanilloid1 channels (elegantly illustrated in Figure 3).
It has been known for some time that the elderlyare prone to developing hypernatremia, partially be-cause they have hypodypsia. Positron emission tomog-raphy scanning has been performed in elderly and
68 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

younger patients given hypertonic solutions to observewhether there are alterations in regional blood flow.No difference in patterns was unveiled, but the authorsof the study concluded that the defect lay not in theperception of thirst but in the satiation of thirst.
The central role of the vasopressin-dependentwater channel aquaporin 2 continues to evolve becauseit is clearly involved in the most important cause ofacquired nephrogenic diabetes insipidus, namely, lith-ium use. It seems that the water channel also fails toreach the luminal membrane of the collecting duct inhypercalciuria, another setting in which maximal uri-nary concentrating ability is impaired. Finally, of note
is the attempt to bypass vasopressin receptor signalingto treat congenital forms of diabetes insipidus by anumber of maneuvers, including the use of chaperonesthat will target the protein to the membrane (in theform of vasopressin agonists), the use of cGMP-generating compounds such as sildenafil, and evenstatins to decrease endocytosis of water channels andallow them to remain in the membrane. The greaterunderstanding of the mechanisms that are involved inthe control of water excretion on the cellular level andtheir derangements in pathologic states should in timelead to better targeted treatments of water-losing dis-orders.
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 69

SyllabusFluid, Electrolyte, and Acid-Base Disturbances
Biff F. Palmer, MD* and Richard H. Sterns, MD†
*Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas,Texas; and †University of Rochester School of Medicine and Dentistry, Rochester, New York
Learning Objectives:1. To understand recent scientific advances in our
understanding of the pathophysiology of disor-ders of potassium, acid base, sodium, and waterbalance
2. To understand how pathophysiology can be ap-plied to the bedside
3. To understand how recent clinical trials related tofluid, electrolyte, and acid-base disorders can beapplied to clinical decision making
Potassium
New Physiologic ConceptsAldosterone plays and an important role in de-
termining the final composition of the urine througheffects in the distal nephron. Aldosterone stimulateselectrogenic Na� reabsorption through the epithelialNa� channel (ENaC), creating a lumen-negative po-tential. This luminal electronegativity serves as a driv-ing force for Cl� reabsorption through the paracellularpathway and secretion of potassium (K�) and hydro-gen (H�) into the lumen (reviewed in reference 1).
Two physiologic stimuli for aldosterone secre-tion are extracellular fluid volume depletion and hy-perkalemia. In the setting of volume depletion, aldo-sterone release is mediated by a direct stimulatoryeffect of angiotensin II on cells in the zona glomeru-losa of the adrenal gland. In this setting, aldosteronecontributes to salt retention and restoration of extra-cellular fluid volume without the development of hy-pokalemia. In the setting of hyperkalemia, aldosteronerelease occurs through a direct effect of K� on thezona glomerulosa. The increase in aldosterone stimu-lates renal K� excretion, restoring the serum K�
concentration to normal but does so without concom-itant renal salt retention.
The ability of the kidney to provide an appropri-ate response to two different physiologic perturbations(salt retention without K� secretion in volume deple-tion and K� secretion without salt retention in hyper-kalemia) despite the same physiologic stimuli (in-creased aldosterone) is not immediately apparent.Although flow rates and distal delivery of salt andwater may account for part of this ability, recentreviews have suggested a more direct mechanismcentered on the WNK4 protein kinase in the distalnephron (2,3).
WNK4 is a member of the with-no-lysine [K](WNK) family of kinases. The name is derived fromthe atypical placement of the catalytic lysine as com-pared with other types of kinases. There are fourmammalian WNK family members, each of which isencoded by a different gene. Inactivating mutations inWNK4 lead to the development of pseudohypoaldo-steronism type II (PHAII; Gordon syndrome). PHAIIis an autosomal dominant disorder in which increasedrenal NaCl reabsorption and impaired renal K� secre-tion lead to hypertension and hyperkalemia. Plasmaaldosterone levels are low despite the presence ofhyperkalemia, which normally exerts a stimulatoryeffect on aldosterone release from the adrenal gland.Administration of NaCl worsens the hypertension, butNa� given with a nonchloride anion such as sulfate orbicarbonate has a beneficial effect. The hypertensionand hyperkalemia are particularly responsive to theadministration of thiazide diuretics.
Wild-type WNK4 acts to reduce the surfaceexpression of the thiazide-sensitive Na�-Cl� co-trans-porter and also stimulates the clathrin-dependent en-docytosis of the renal outer medullary K� (ROMK)channel in the renal collecting duct. The inactivatingmutation of WNK4 responsible for PHAII leads toincreased co-transporter activity and further stimulates
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009
70

endocytosis of ROMK. The net effect is increasedNaCl reabsorption along with decreased K� secretion.Mutated WNK4 also enhances paracellular Cl� per-meability as a result of increased phosphorylation ofclaudins, which are tight junction proteins involved inregulating paracellular ion transport. In addition toincreasing salt retention, this change in permeabilityfurther impairs K� secretion because the lumen-neg-ative charge, which normally serves as a driving forcefor K� secretion, is dissipated.
Because volume expansion and hyperkalemiaresulting from the PHAII-mutated WNK4 protein canbe viewed as an exaggerated response of what nor-mally should occur as the kidney responds to a reduc-tion in extracellular fluid volume (salt retention with-out increased K� secretion), it has been proposed thatwild-type WNK4 may act as a molecular switch de-termining the balance between renal NaCl reabsorp-tion and K� secretion. In the basal state, nephronfunction would be characterized by decreased NaClreabsorption and K� secretion. Under conditions ofvolume depletion, the switch would be altered in away reminiscent of the PHAII mutant such that NaClreabsorption is increased but K� secretion is furtherinhibited.
WNK4 may assume a third state to account forK� secretion without salt retention under conditions inwhich aldosterone is directly stimulated by elevationsin the serum K� concentration (4). The WNK4 proteinpossesses a site that is phosphorylated by the serum-and glucocorticoid-dependent protein kinase SGK1.This site is highly conserved and far removed from theregion of WNK4 in which PHAII mutations are clus-tered. In turn, SGK1 is an immediate transcriptionaltarget of the mineralocorticoid receptor. Evidence sug-gests that SGK1-mediated phosphorylation of WNK4leads to a loss in the ability of WNK4 to inhibitROMK, providing increased K� secretion capability.In addition, phosphorylation removes the inhibitoryeffect of the wild-type WNK4 on ENaC (5). Increasedelectrogenic Na� reabsorption with greater luminalelectronegativity would provide an additional stimula-tory effect for K� secretion.
The precise signals that are required to allowWNK4 to switch to the form appropriate for thephysiologic stimuli that drive aldosterone release arenot entirely clear. Under conditions of volume deple-tion, WNK4 may switch in the direction of the PHAIImutant protein as a result of aldosterone signaling in
the context of other effectors such as angiotensin II,sympathetic nerve activity, and antidiuretic hormone,all of which are increased in this setting. This envi-ronment would be distinct from that in which aldoste-rone is increased solely as a result of a direct stimu-latory effect of K� in the adrenal gland. Increasedaldosterone either alone or along with increased serumK� concentration may provide the signals required toallow SGK1-mediated phosphorylation to dominate(Figure 1).
In the previous fluid and electrolyte edition ofNephSAP, a discussion was provided about the role ofWNK proteins in modulating K� secretion in responseto changes in dietary K� intake (6). This area wasdiscussed further in two recent reviews with particularemphasis placed on the potential role of WNK1 in thepathogenesis of salt-sensitive hypertension (7,8). Thisarea is briefly summarized as follows.
WNK1 is ubiquitously expressed throughout thebody in multiple spliced forms. By contrast, a shorterWNK1 transcript lacking the amino terminal 1 through437 amino acids of the long transcript is highly ex-pressed in the kidney but not in other tissues and isreferred to as kidney-specific WNK1 (KS-WNK1).Changes in the ratio of KS-WNK1 and long WNK1 inresponse to dietary K� play an important role in thephysiologic regulation of renal K� excretion. LongWNK1 inhibits ROMK by stimulating its endocytosis,whereas KS-WNK1 functions as a physiologic antag-onist to the actions of long WNK1. Under condition ofdietary K� restriction, the relative abundance of longWNK1 to KS-WNK1 is increased. These changes leadto decreased abundance of ROMK in the renal corticalcollecting duct, which is an adaptive response impor-tant for renal K� conservation. Conversely, dietaryK� loading increases the abundance of KS-WNK1relative to long WNK1. This change is accompaniedby upregulation of ROMK, which again is an appro-priate response to facilitate K� secretion in the settingof a high-K� diet.
The changes in KS-WNK1 and long WNK1 thatoccur in response to dietary K� intake also haveeffects on renal Na� handling that may be of impor-tance in the observed reciprocal relationship betweendietary K� intake and hypertension. Long WNK1 hasbeen shown to stimulate ENaC activity through acti-vation of SGK1. SGK1 inactivates the ubiquitin-pro-tein ligase Nedd4-2 through phosphorylation, resultingin less retrieval of ENaC from the apical membrane.
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 71

Increased activity of long WNK1 also releases theinhibitory affect of WNK4 on Na� reabsorption me-diated by the NaCl co-transporter. These effects sug-gest that the decrease in K� secretion under conditionsof K� deficiency will occur at the expense of in-creased Na� retention.
The simultaneous conservation of K� and Na�
during dietary K� deficiency is evolutionarily advan-tageous for early humans, who had limited access toNa� and for whom dietary K� and Na� deficiencylikely occurred together (9); however, such an effect ispotentially deleterious if present in the setting ofplentiful Na� intake. In this regard, throughout theevolutionary course, there has been a 50-fold increasein the ratio of dietary intake of Na� versus K�. Theratio of dietary Na� to K� intake was approximately1:16 for Paleolithic humans and is approximately 3:1for present-day North Americans. The effect of anincreased ratio of WNK1 to KS-WNK1 in the kidneyfrom a high-Na�/low-K� diet could be central to thepathogenesis of salt-sensitive hypertension.
The precise role of WNK proteins in regulatingfluid homeostasis through the coordination of iontransport in the distal nephron is an area that continuesto be actively pursued. This area is of particular
interest because WNK proteins and the pathways thatthey influence are also potential targets for the devel-opment of novel antihypertensive drugs (10).
References1. Giebisch G, Krapf R, Wagner C: Renal and extrarenal regulation of
potassium. Kidney Int 72: 397–410, 20072. Kahle K, Ring A, Lifton R: Molecular physiology of the WNK
Kinases. Annu Rev Physiol 70: 329–355, 20083. Kahle K, Rinehart J, Giebisch G, Gamba G, Hebert S, Lifton R: A
novel protein kinase signaling pathway essential for blood pressureregulation in humans. Trends Endocrinol Metab 19: 91–95, 2008
4. Ring A, Cheng S, Leng Q, Kahle K, Rinehart J, Lalioti M, VolkmanH, Wilson F, Hebert S, Lifton R: WNK4 regulates activity of theepithelial Na� channel in vitro and in vivo. Proc Natl Acad Sci U S A104: 4020–4024, 2007
5. Ring A, Leng Q, Rinehart J, Wilson F, Kahle K, Hebert S, Lifton R:An SGK1 site in WNK4 regulates Na� channel and K� channelactivity and has implications for aldosterone signaling and K�homeostasis. Proc Natl Acad Sci U S A 104: 4025–4029, 2007
6. Sterns R, Palmer BF: Fluid and electrolyte and acid-base distur-bances. NephSAP 6: 210–272, 2007
7. Huang C, Kuo E, Toto R: WNK kinases and essential hypertension.Curr Opin Nephrol Hypertens 17: 1062–4821, 2008
8. Huang C, Kuo E: Mechanisms of disease: WNK-ing at the mecha-nism of salt-sensitive hypertension. Nat Clin Pract Nephrol 3: 623–630, 2007
9. Eaton S: The ancestral human diets: What was it and should it be aparadigm for contemporary nutrition? Proc Nutr Soc 65: 1–6, 2006
10. San-Cristobal P, de los Heros P, Ponce-Coria J, Moreno E, Gamba G:WNK kinases, renal ion transport and hypertension. Am J Nephrol28: 860–870, 2008
ECF volume
PHAII like WNK4
Aldosterone in setting ofneurohumoral activation
( All, ADH, Catecholamines)
Na+-Cl– cotransporter, ROMK
Serum K+
Norml ECF Volume
SGK1-MediatedPhosphorylation of WNK4
Aldosteronein isolation
ENaC, ROMK
Salt retentionwithout K+ wasting
K+ Secretion withoutsalt retention
WNK4BASAL STATE
Figure 1. The WNK4 protein may play an important role in ensuring the transport function of the distal nephron isappropriate to conditions in which aldosterone is increased as a result of volume depletion as compared with conditions inwhich aldosterone is increased solely as a result of hyperkalemia. With volume depletion, increased circulating levels ofaldosterone occur in the setting of increased levels of other neurohumoral effectors. In this environment, the WNK4 proteinis altered in a way reminiscent of the PHAII mutant protein. As a result, NaCl reabsorption is enhanced in the absence of K�
secretion. By contrast, K� can directly stimulate aldosterone release at the level of the adrenal gland such that higher levelsoccur in isolation. In this setting, the WNK4 protein is altered in such a way that K� secretion can be enhanced in the absenceof salt retention. AII, angiotensin II; ADH, antidiuretic hormone (see references [2–5] for excellent discussions regarding theseconcepts).
72 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

Hypokalemia
Approach to the Patient with HypokalemiaHypokalemia is frequently encountered in clini-
cal practice. Transient causes of hypokalemia are dueto cell shift, whereas sustained hypokalemia is dueeither to inadequate intake or to excessive potassium(K�) loss. Hypokalemia resulting from excessive K�
loss can be due to renal or extrarenal losses. Theclinical history, physical examination with particularemphasis on determination of volume status, and de-termination of the acid–base status will allow thecause of hypokalemia to be readily determined in mostcases.
A variety of urine studies are frequently used toaid in the determination of hypokalemia with the ideathat findings indicative of renal K� conservation sup-port either cell shift or an extrarenal cause of hypoka-lemia; urine K� wasting confirms a renal source.Renal K� handling can be assessed with a 24-h urinecollection or a spot urine test determining the K�/creatinine ratio. A 24-h urinary K� of �15 mEq or aK� (mmol)/creatinine (mmol) ratio �1 suggests anextrarenal cause of hypokalemia.
A random urine K� is oftentimes used as aninitial test to discriminate renal from extrarenal K�
losses but is limited by the influence of renal waterhandling on urine K� concentration. Determining thetranstubular K� gradient (TTKG) remains a populartool among some clinicians to assess renal K� handling:TTKG � [K�
urine/(Uosmolality/Sosmolality)]/K�
serum
Determining the tubular fluid K� concentrationat the end of the collecting duct is the ideal measure ofaldosterone activity because most K� secretion takesplace in the collecting duct. Thereafter, the K� con-centration in the urine progressively rises as a result ofwater reabsorption. The TTKG is intended to estimatethe tubular fluid K� concentration at the end of thecortical collecting duct by accounting for water reab-sorption that takes place distal to where K� secretionhas ceased.
It is worthwhile considering some of the assump-tions made in calculating the TTKG as reviewed in arecent clinical commentary (1). First, the calculationassumes that there is no significant solute transportand only water reabsorption as fluid enters the med-ullary collecting duct. Any Na� or urea reabsorptionin this segment would tend to lower urine osmolalityand cause the TTKG to overestimate the gradient for
K� secretion in the upstream collecting duct. Second,conditions should be optimal for K� secretion at thetime the TTKG is measured. In this regard, urine Na�
should be no less than 25 mEq/L to ensure that Na�
delivery to the collecting duct is not rate limiting inK� secretion. In addition, urine osmolality should beequal to—and ideally greater than—the plasma. Ahigher urine osmolality reflects increased vasopressin,which is known to exert a stimulatory effect on K�
secretion in the collecting duct.During the workup of a patient with hypokale-
mia, one can argue whether the TTKG offers anyadditional insight compared with a spot urine K� testand clinical assessment. The TTKG may be mosthelpful in the evaluation of hyperkalemia when one isattempting to discriminate between low aldosteronelevels and aldosterone resistance. The best way to usethe test is to compare a basal measurement with oneobtained within 4 h after administration of a physio-logic dosage (0.05 mg) of 9-�-fludrocortisone. Anincrease in the TTKG to �6 within this time framesuggests aldosterone deficiency. Administration of apharmacologic dosage (0.2 mg) may elicit an increasein the TTKG during 24 h in the setting of aldosteroneresistance.
The TTKG may be most useful in the eval-uation of hyperkalemia when one is at-tempting to discriminate between lowaldosterone levels and aldosterone resis-tance. An increase in the TTKG to >6 afterthe administration of fludrocortisonessuggests aldosterone deficiency as thecause of the increased serum K� concen-tration.
Cellular RedistributionThe regulation of K� distribution between the
intracellular and extracellular space is referred to asinternal K� balance. Although the kidney is ultimatelyresponsible for maintenance of total body K�, factorsthat modulate internal balance are important in thedisposal of acute K� loads. Cell shifts are extremelyimportant, in that only 2% of total body K� is locatedin the extracellular fluid. A large K� meal couldpotentially double extracellular K� levels were it notfor the rapid shift of the K� load into cells. The kidney
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 73

cannot excrete K� rapidly enough in this setting toprevent life-threatening hyperkalemia. Thus, it is im-portant that this excess K� be rapidly shifted andstored in cells until the kidney has successfully ex-creted the K� load. The major regulators of K� shiftinto cells are insulin and catecholamines with a lessereffect mediated by metabolic and respiratory alkalosis.
The various physiologic effects of insulin, in-cluding glucose and K� regulation, are mediatedthrough the binding to cell surface receptors. Thisbinding stimulates glucose uptake in insulin-respon-sive tissues through the insertion of the glucose trans-porter protein GLUT 4. K� uptake is stimulated as aresult of increased activity of the Na�-K�-ATPase.Metabolic studies in a patient with leprechaunismdemonstrated that the effects of insulin on glucose andK� disposal can be separated from one another (2).
Leprechaunism is an extreme form of insulinresistance related to mutations in the insulin receptor.Patients present with a lack of subcutaneous fat, de-creased muscle mass, and an inability to regulateblood glucose levels properly. Metabolic studies wereperformed in a patient with two naturally occurringmutant alleles of the receptor that markedly impairedposttranslational processing and intracellular transportof the receptor to the cell surface. Using a glucoseclamp technique, the patient was found to have virtu-ally no anabolic effects of insulin on measures ofcarbohydrate, lipid, and protein metabolism. By con-trast, the effect of insulin to stimulate cellular K�
uptake was intact. The mechanism behind this disas-sociation is not known but may be due to differencesin the folding and surface expression in various insulintarget tissues.
The release of insulin can be responsible forsignificant drops in extracellular K� concentration aswell as drops in other ions when glucose is given topatients with significant malnutrition. Some of theearliest reports of the refeeding syndrome were ofstarved prisoners of war who developed fatal cardio-vascular complications in association with the admin-istration of nutritional therapy. A similar complicationhas been seen in patients who had anorexia nervosaand were administered aggressive nutritional therapy.A more modern-day occurrence of the syndrome isseen in malnourished patients with cancer. Such patientsare frequently malnourished as a result of direct effects ofthe tumor as well as adverse effects of chemotherapy,such as nausea, vomiting, and mucositis (3).
The administration of a carbohydrate load tomalnourished patients can unmask total-body deficitsof K�, phosphate, and Mg2� as a result of insulin-mediated shifts into the intracellular compartment(4,5). Depletion of extracellular K� and Mg2� canalter cell membrane function in such a way that pa-tients are predisposed to arrhythmias. Depletion ofphosphate can lead to severe muscle weakness (poten-tially respiratory failure), rhabdomyolysis, and hemo-lysis. Hypophosphatemia-induced depletion of redblood cell 2,3-DPG can lead to a shift in the O2
disassociation curve, predisposing patients to the de-velopment of tissue hypoxemia and potentially lacticacidosis.
The administration of a carbohydrate loadcan unmask total-body deficits of K�,phosphate, and Mg2� as a result of insulin-mediated shifts into the intracellular com-partment.
A similar pathophysiology can develop in indi-viduals with long-term alcoholism. Upon admission tothe hospital, such patients often have relatively normalserum chemistry values. Treatment with glucose-con-taining maintenance fluids and development of respi-ratory alkalosis as a result of alcohol withdrawal cancause precipitous drops in extracellular K�, Mg2�,and phosphate as a result of the presence of total-bodydeficits. For patients with alcoholic ketoacidosis, glu-cose administration is an effective way to terminatethe ketogenic state in the liver and to correct theacidemia. The additional administration of bicarbon-ate-containing solutions can cause rapid serum alka-linization and be complicated by life-threatening ar-rhythmias such as ventricular tachycardia (6).
Hydrofluoric acid is an inorganic acid used in thechemical- and oil-refining industry as well as ceramicand graphite production, frosting of glass, and elec-tropolishing of certain metals. Dermal exposure of thisagent has primarily been reported to cause hypocalce-mia and hypomagnesemia but on occasion has beenimplicated in the development of hypokalemia (7–10).These cases have been observed in the setting ofextensive dermal chemical burns. Depletion of theseions is thought to be a result of binding to the fluorideanion. The degree of hypocalcemia and hypomag-
74 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

nesemia can be severe and result in prolongation of theQT interval and recurrent ventricular tachycardia.
One of the features of hydroxychloroquine andchloroquine overdose is the development of hypoka-lemia because of a cell shift (11). This intracellularshift of K� is exacerbated in patients who have hypo-tension and require pressor support with � adrenergicagents. Because total body K� is normal in this situ-ation, caution should be used in administering K� toavoid rebound hyperkalemia as the clinical conditionof the patient improves.
Hypokalemic periodic paralysis is a rare disorderthat is characterized by muscle weakness or paralysisas a result of the sudden movement of K� into cells.Measurement of the TTKG at the time of the attackstypically shows values of �1 (12). The attacks areprecipitated by rest after exercise, stress, intake ofmeals that contain large amounts of carbohydrates,and events accompanied by increased release of cat-echolamines or insulin.
This disorder may be familial or acquired. Theacquired form of hypokalemic periodic paralysis typ-ically develops in association with thyrotoxicosis.Thyrotoxic periodic paralysis is more commonly seenin Asian individuals but has also been reported withhigher frequency in American Indian and Hispanicindividuals (13). A series of 40 Turkish patients withthe disorder has now been described (14). The clinicalcharacteristics of these patients were similar to otherat-risk populations.
Although the incidence of thyrotoxicosis is morecommon in women, there is a male-to-female predom-inance that ranges from 17:1 to 70:1 for those whodevelop hypokalemic periodic paralysis. The typicalpatient is a young adult man who is between ages 20and 40 and presents with weakness most commonlybetween the hours of 9:00 p.m. and 9:00 a.m. in thesummer months. The attacks are precipitated by con-ditions characterized by increased release of cat-echolamines or insulin such as stress, intake of mealsthat contain large amounts of carbohydrates, and ex-ercise. With regard to exercise, the timing of attacks istypically in the initial rest period after exertion. Of-tentimes, the attacks are heralded by muscle crampsand aches, and many patients learn to avoid paralyticepisodes by exercising the involved muscles. Hy-pophosphatemia and hypomagnesemia are also com-mon during acute attacks and, like K�, are the result ofshifts into the intracellular compartment.
Excess thyroid hormone may predispose to par-alytic episodes by increasing Na�/K�-ATPase activ-ity. The activity of this pump is likely to be increasedfurther by catecholamines, which are typically in-creased in this setting. The underlying cause of thyro-toxicosis is most commonly Graves disease but canalso be a solitary thyroid adenoma (Plummer disease)(15), a thyroid-stimulating hormone-secreting pitu-itary adenoma, or abuse of exogenous thyroid hor-mone. Iodine-induced thyrotoxicosis (Jod-Basedowsyndrome) and associated hypokalemic periodic paral-ysis has been reported after the administration ofiodine-containing radiocontrast agents, amiodarone,and iodine-containing herbal supplements. A knowncomplication of IFN-� therapy is the development ofthyroid abnormalities. Two reports described the onsetof thyrotoxic periodic paralysis in patients who re-ceived IFN-� therapy for hepatitis C and hepatitis B(16,17).
The acute attacks of hypokalemic periodic paral-ysis are best treated with intravenous KCl and pro-pranolol. It is important to administer KCl in non–dextrose-containing solutions because glucose willstimulate insulin release, potentially exacerbating themovement of K� into cells. To minimize the likeli-hood of rebound hyperkalemia, K� should be given atdosages of �10 mmol/h. Propranolol (a nonspecific �adrenergic blocker) blocks the effects of cat-echolamines and inhibits the peripheral conversion ofT4 to T3. The definitive treatment is to remove theunderlying cause of thyrotoxicosis.
Mutations in the genes implicated in the familialform of the disease discussed next are not found inpatients with thyrotoxic hypokalemic periodic paraly-sis (18). In fact, periodic paralysis does not recur oncethe patient is euthyroid. Nevertheless, in a populationof Thai patients, single-nucleotide polymorphisms atintron 3 of the �-aminobutyric acid receptor �3 sub-unit were found to be associated with hypokalemicperiodic paralysis (19). How this single-nucleotidepolymorphism might relate to the pathogenesis of thedisorder is not clear.
The familial form of hypokalemic periodic pa-ralysis is inherited as an autosomal dominant disorderand has similar clinical features as the acquired form.Notable differences include a younger age at presen-tation (usually �20 yr), an equal male/female distri-bution, and longer duration of attack; it is mostly seenin Caucasian individuals. A slowly progressive perma-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 75

nent proximal weakness can develop in some patients(20). The familial disorder is most commonly a resultof mutations in the muscle calcium channel �-1 sub-unit gene (CACNA1S) on chromosome 1q3132(21,22). The �-1 subunit of the calcium channel servesas the pore for movement of calcium into the T tubuleof muscle sarcoplasmic reticulum and also containsthe dihydropyridine-binding site. Mutations of thissubunit reduce the calcium current into the T tubule.The precise mechanism by which impaired function ofthe calcium channel dihydropyridine receptor causesthe influx of K� into muscle cells is not clear. Asmaller number of cases have been localized to muta-tions in the skeletal muscle sodium channel SCN4Aand the R83H mutation in the K� channel subunitgene KCNE3.
A presumed variant of hypokalemic paralysiswith a normal K� has been described in a mother andson who both manifested symptoms of sensory over-load (23). In addition to leg cramps, the mother expe-rienced a sensation of auditory and visual overload.She complained of difficulty in filtering out extrane-ous conversation and background noise. She also hada feeling of visual impingement for which she wouldpurposely ignore peripheral vision. These symptomswere typically worse after consuming large amounts ofcarbohydrates as well as after exercise and would beameliorated by exogenous K�. She also was noted tobe resistant to the anesthetic effects of lidocaine.
The son presented with occasional foot cramps,fatigue, and irritability reminiscent of an attention-deficit disorder. As in the mother, these findings weretypically worse after carbohydrate intake and exercise.He similarly was resistant to the effects of lidocaineanesthesia. On the basis of the favorable experience inthe mother, the son was also treated with exogenousK� supplements with marked improvement in symp-toms.
Extrarenal K� Loss from the BodyGastrointestinal loss is a common cause of hy-
pokalemia and is generally due to diarrhea. Secretorydiarrhea is generally believed to be caused by one oftwo processes that can occur either alone or together.First, inhibition of active intestinal NaCl and NaHCO3
reabsorption may be present, and, second, stimulationof active chloride secretion followed by passive secre-tion of an equal amount of Na� so as to maintainelectrochemical balance may take place. In both of
these instances, the stool electrolyte content is similarto plasma with high concentration of NaCl and muchlower K� concentration. The sodium salts in stoolcause an isotonic increase in stool water output suchthat the fecal content of sodium salts roughly parallelsthe volume of diarrhea. Despite the low K� concen-tration in fecal fluid, significant total body K� lossescan occur in the setting of large stool volumes.
Vasoactive intestinal peptide (VIP) normally in-hibits gastric acid secretion, promotes glycogenolysisand hyperglycemia, and exerts a peripheral vasodila-tory effect. A variety of tumors have been found tooversecrete VIP in patients who present with waterydiarrhea, hypokalemia, and achlorhydria. Other find-ings include flushing, weight loss, hypercalcemia, andhyperglycemia. The syndrome most commonly occursas a complication of pancreatic islet cell tumors buthas been reported with bronchogenic carcinoma, med-ullary thyroid carcinoma, and retroperitoneal histiocy-toma. There are now several reports linking pheochro-mocytoma as a source for VIP hypersecretion (24).
Infectious diarrhea can also be a cause of signif-icant hypokalemia. Of note is a recent review concern-ing alterations in fluid and electrolyte disorders in avariety of tropical diseases, emphasizing those foundwith malaria and leptospirosis (25). Hypokalemia isparticularly common in children with severe malariaand tends to occur within several hours of initiation oftherapy. The cause is multifactorial and includes gas-trointestinal loss in patients with diarrhea and in-creased renal excretion as a result of increased deliv-ery of Na� in the form of ketoacid salts. Quininetherapy is associated with stimulation of insulin re-lease, which in turn, can cause K� to shift into cells.The poor dietary intake characteristic of many ruralareas will further exacerbate the tendency for hypoka-lemia in the setting of tropical infectious diseases.
Hypokalemia develops in approximately onethird of patients with leptospirosis. Such patients are atrisk for both gastrointestinal and renal losses. Theouter membrane of the organism has an inhibitoryeffect on the Na�-K�-ATPase within the nephron. Ithas been postulated that this inhibitory effect impairsNa� reabsorption proximally and increases distal Na�
delivery, resulting in kaliuresis (25). In an animalmodel, leptospirosis leads to downregulation of thesodium/hydrogen exchanger isoform 3 (NHE3) andaquaporin 2, whereas expression of the Na�-K�-2Cl�
(NKCCl) co-transporter is increased (26). In the lung,
76 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

the organism decreases expression of ENaC and up-regulates expression of NKCCl. Alterations in thefunction of such transporters caused by the organismcould play a role in the development of Weil disease,a severe form of leptospirosis characterized by theacute respiratory distress syndrome and acute renalfailure. For patients with acute renal failure, mortalityis improved with intensive daily dialysis comparedwith traditional alternate-day dialysis (27).
Abnormalities in K� transport have not previ-ously been known to be the primary cause of secretorydiarrhea. A previous report described a patient whohad colonic pseudo-obstruction (Ogilvie syndrome)and developed a secretory diarrhea that was driven byactive K� secretion (28). In contrast to the high-Na�/low-K� concentration typically found in variouscauses of secretory diarrhea, fecal electrolyte concen-tration in this patient was reversed. Fecal K� concen-tration ranged from 130 to 170 mEq/L; values for Na�
concentration varied between 4 and 15 mEq/L. Fiveadditional patients with Ogilvie syndrome have nowbeen described, in which active K� secretion (100 to180 mEq/L) was the primary mechanism for develop-ment of diarrhea (29).
Surgical diversion of the ureter into an ilealpouch is sometimes used in the treatment of patientswith a neurogenic bladder or after cystectomy. Theprocedure may rarely be associated with the develop-ment of hyperchloremic normal gap metabolic acido-sis (30,31). The main factors that influence the devel-opment and severity of acidosis are the length of timethe urine is in contact with the bowel and the totalsurface area of bowel exposed to urine. Acidosis mayoccur in part as a result of reabsorption of urinaryNH4Cl by the intestine. The ammonia is transportedthrough the portal circulation to the liver, where it ismetabolized to urea. This metabolic process consumesequimolar amounts of bicarbonate; therefore, it canresult in the development of metabolic acidosis. Met-abolic acidosis may also develop because urinary Cl�
can be exchanged for HCO3� through activation of a
Cl�/HCO3� exchanger on the intestinal lumen. Hypo-
kalemia is also common with sigmoid loops, althoughthe mechanism is not clear. One possibility is that highconcentration of ammonium in the colonic lumenenhances net K� secretion by removing any compo-nent of K� reabsorption as a result of a direct com-petition effect.
This same type of clinical picture was described
in a patient who had uterine cancer and was treatedwith radiotherapy and later developed an enterovesicalfistula (32). The fistula caused diversion of urine fromthe bladder into the distal ileum, resulting in severenormal gap metabolic acidosis and hypokalemia. Anegative urinary anion gap was consistent with anappropriate response of the kidney to the generation ofan extrarenal acidosis.
A series of articles has provided evidence tosupport the existence of enteric solute sensors that arecapable of responding to Na�, K�, and phosphate,which can then signal the kidney to alter rapidly ionexcretion or reabsorption (33,34). For example, insalt-depleted normal patients, urine Na� excretion isgreater when a Na� load is given orally as comparedwith the same Na� load given intravenously. Thisdifference in Na� handling was independent of circu-lating aldosterone levels. Guanylin and uroguanylinderived from the gut may play a role in modulatingthis effect.
Receptors within the gastrointestinal tractcan signal alterations in renal solute han-dling in response to changes in dietaryNa�, K�, and phosphate.
A similar effect may be present in response todietary K�. The effect of a K� load given as asystemic, intraportal, or intragastric infusion on uri-nary K� excretion was studied in rats (35). In thefasting state, plasma K� concentration increased to asimilar degree with all three maneuvers, as did renalK� excretion. By contrast, when studied in rats thatwere fasted overnight and simultaneously fed alow-K� diet, the intragastric infusion caused nochange in plasma K�; plasma K� increased similarlyto the unfed rats with either the systemic or the portalinfusion routes. These data are consistent with anenhanced renal response to K� infusion when com-bined with a meal, suggesting the presence of a gutfactor that is capable of enhancing the efficiency ofrenal K� excretion.
Renal K� WastingThe circulating levels of aldosterone and distal
delivery of Na� and water are two important factors inthe renal excretion of K�. Although increased distaldelivery of Na� and water and increased aldosterone
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 77

activity each can stimulate renal K� secretion, undernormal physiologic conditions, these two determinantsare inversely related. It is for this reason that K�
excretion is independent of volume status. For exam-ple, under conditions of a contracted extracellular fluidvolume, aldosterone levels increase. At the same time,proximal salt and water absorption increase, resultingin decreased distal delivery of Na� and water. RenalK� excretion remains fairly constant under these con-ditions because the stimulatory effect of increasedaldosterone is counterbalanced by the decreased deliv-ery of filtrate to the distal nephron. A similar situationoccurs in the setting of expansion of the extracellularfluid volume. In this setting, distal delivery of filtrateis increased as a result of decreased proximal tubularfluid reabsorption. Under conditions of volume expan-sion, circulating aldosterone levels are decreased. Theeffect of the increased delivery of Na� and water tostimulate K� excretion is opposed by decreased cir-culating aldosterone levels such that renal K� excre-tion again remains constant. Thus, there is a balancedreciprocal relationship between urinary flow rates andcirculating aldosterone levels, which serves to main-tain K� balance during normal volume regulation.
It is only under pathophysiologic conditions thatdistal Na� delivery and aldosterone become coupled.In this setting, renal K� wasting will occur. Whentreating patients who have hypokalemia as a result ofrenal K� wasting, it must be determined whether thereis a primary increase in mineralocorticoid activity or aprimary increase in distal Na� delivery.Primary Increase in Mineralocorticoid Activity.These patients typically have evidence of an expandedextracellular fluid volume and present with hyperten-sion, hypokalemia, and metabolic alkalosis. The dif-ferential diagnosis rests on measurement of plasmarenin activity and plasma aldosterone levels.Increased Renin, Increased Aldosterone. Renin-secreting tumors fall into this category and have beenthe subject of a recent review (36). These tumorsshould be considered in young patients (mean age 27)who present with severe hypertension (mean BP 201/130 mmHg) and hypokalemia. On average, the plasmarenin activity and aldosterone levels are increased by12 times and four times the upper limit of normal,respectively. Both magnetic resonance imaging andcomputed tomography scanning are effective means ofdetecting the presence of renin-secreting tumors in thekidney. Tumors located peripherally can be success-
fully removed with partial nephrectomy; radical ne-phrectomy is typically required in deep-seated tumors.Surgical removal of the tumors cures the hypertensionin most patients.
The tumors are typically vascular and have fea-tures characteristic of hemangiopericytomas. Thesetumors can also secrete fibroblast growth factor 23 andcan be responsible for oncogenic osteomalacia. Thevascular nature of the tumors can also give rise to aconsumptive coagulopathy in which thrombocytope-nia is a feature, the Kasabach-Merritt syndrome.
At least one report raised the possibility of a Pagekidney giving rise to hypokalemia in the setting ofhypertension (37). The Page kidney was originallydescribed in an experimental model of hypertension inwhich canine kidneys were wrapped with cellophane.The human counterpart of this disorder refers to thedevelopment of hypertension as a result of some pro-cess that extrinsically compresses the kidney, resultingin activation of the renin-angiotensin-aldosterone sys-tem. The most common cause of a Page kidney isaccumulation of blood around the kidney as a result oftrauma, but it can also occur in association with asubcapsular bleed after a native or allograft renalbiopsy (38). Complication of extracorporeal shock-wave lithotripsy by subcapsular bleeds is also a po-tential cause of this disorder (37).Suppressed Renin, Increased Aldosterone. Primaryhyperaldosteronism as a result of an adrenal adenomaand bilateral adrenal hyperplasia are the two most com-mon disorders to consider in this category. The workupof patients who are suspected of having primary hyper-aldosteronism continues to be the subject of reviews toinclude the most recent NephSAP devoted to hyperten-sion (39–41). The best screening test is the plasmaaldosterone-renin ratio. When plasma aldosterone levelsare measured in ng/dl and plasma renin activity (PRA) ismeasured in ng/ml per h, a value of �20 to 30 reliablyexcludes primary hyperaldosteronism. To avoid overin-flating the ratio and to avoid false-positive tests, thelowest value for PRA should be fixed at 0.5 ng/ml per h.Requiring a plasma aldosterone level of at least 12 to 15ng/dl will also increase the predictive value of the test.After a positive screening test, confirmatory tests areindicated to document the nonsuppressibility of aldoste-rone secretion. Saline or oral salt loading, fludrocortisoneadministration, and acute captopril administration aremaneuvers that are used for this purpose. Imaging studies
78 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

and, in some cases, adrenal vein sampling are required tocomplete the workup (42).
Bilateral adrenal hyperplasia (BAH) has nowbeen categorized into at least six different forms (43).These forms are characterized by either micronodularor macronodular hyperplasia. BAH may occur as anisolated finding or part of a systemic disorder andshows variability in the presentation age. Recent find-ings disclosed abnormalities in cAMP signaling path-ways in the majority of BAH cases (44,45).
Glucocorticoid-remediable aldosteronism (GRA)is an autosomal dominant disorder that should besuspected in a patient who has hypertension and hy-pokalemia and similarly affected family members(46). GRA results from the unequal crossover of twogenes: The CYP11B1 gene that encodes the enzyme11�-hydroxylase and the CYP11B2 gene that encodesthe enzyme aldosterone synthase (18-hydroxylase).The product of this event creates a chimeric gene inwhich the adrenocorticotropin hormone (ACTH)-re-sponsive promoter is fused to the aldosterone-synthasecoding sequence. As a result, aldosterone-synthase isectopically expressed in the cortisol-producing zone ofthe adrenal cortex (zona fasciculata) and is under thecontrol of ACTH. Suppression of aldosterone withexogenous administration of dexamethasone is a use-ful diagnostic and therapeutic strategy. Measurementof urinary cortisol metabolites can also be useful as adiagnostic tool. Increased urinary excretion of 18-hydroxycortisol and 18-oxocortisol is typical for thisdisease.
For unclear reasons, random plasma K� levelsare frequently normal for patients with GRA. Onepossibility is that the stimulatory effect on aldosteronerelease is only intermittent because ACTH is secretedcentrally in a diurnal manner with peaks in the earlymorning and evening. In addition, the normal stimu-latory effect of K� on aldosterone release is absent inthis condition, likely a result of aldosterone releaseoriginating in the zona fasciculata rather than the zonaglomerulosa. To the extent that dietary K� normallystimulates aldosterone release, this insensitivity wouldfurther diminish aldosterone secretion. Althoughplasma K� concentration may be normal, the likeli-hood of developing hypokalemia is increased whenpatients with GRA are treated with either thiazide orloop diuretics.Suppressed Renin and Aldosterone. Cushing dis-ease refers to an excessive cortisol state, resulting
from pituitary overproduction of ACTH. Cushing syn-drome refers to cortisol excess that is either ACTHindependent (glucocorticoid-secreting adrenocorticaladenomas or carcinomas) or ACTH dependent; how-ever, it arises from a site other than the pituitary.Ectopic secretion of ACTH is most commonly re-ported in association with tumors such as small celllung carcinoma, carcinoid tumors, pancreatic islet tu-mors, and a host of others. A patient who presentedwith severe muscle weakness in association with hy-pertension, hypokalemia (K� 1.8 mEq/L), and meta-bolic alkalosis was recently reported (47). The patientwas found to have ectopic secretion of ACTH from apreviously unreported tumor type, large cell neuroen-docrine carcinoma of the lung. As is typical for pa-tients with ectopic secretion of ACTH, this patient didnot manifest features of Cushing disease such as buf-falo hump and striae because oversecretion of cortisolis typically acute. Rather, the clinical presentationtends to be dominated by hypertension and electrolyteabnormalities.
The aldosterone-like effect of excess cortisol isdue to the high concentrations that overwhelm theability of 11-�-hydroxysteroid dehydrogenase type II(11�-HSDH) in the principal cells of the collectingduct to convert cortisol into cortisone. The mineralo-corticoid receptor is capable of binding aldosteroneand cortisol but has no affinity for cortisone. Becausecortisol normally circulates in the blood at muchhigher concentrations than aldosterone, the enzymaticactivity of 11�-HSDH is essential in keeping themineralocorticoid receptor free to interact only withaldosterone.
Normal concentrations of cortisol can gain ac-cess to the mineralocorticoid receptor under conditionsof decreased activity of 11�-HSDH. The syndrome ofapparent mineralocorticoid excess is a rare recessivedisorder characterized by hypertension, hypokalemia,metabolic alkalosis, and suppressed circulating aldo-sterone levels as a result of an inherited deficiency ofthe enzyme. Patients with apparent mineralocorticoidexcess can be effectively treated with either spirono-lactone or a sodium channel blocker such as amilorideor triamterene.
For patients whose BP remains uncontrolled,recent findings in an animal model of 11�-HSDHdeficiency suggested that an adrenergic blocking agentmay be useful (48). In an 11�-HSDH type II nullmouse, BP was found to be increased in association
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 79

with evidence of impaired renal Na� excretion. Dur-ing a period of several weeks, the mouse began toshow evidence of volume contraction. Despite thenatriuresis, hypertension was persistent but becamemediated by increased adrenergic activity as evi-denced by an increase in urinary catecholamines. Themechanism for this change from a volume-dependentto an adrenergically mediated form of hypertension isnot clear but was postulated to be a result of either K�
deficiency or the initial period of Na� retention.Decreased activity of 11�-HSDH type II can
occur as an acquired disorder as a result of the long-term ingestion of licorice (49). The active componentin licorice is glycyrrhetinic acid, which has an inhib-itory effect on the enzyme. Plasma K� concentrationsas low as 1.13 to 1.7 mmol/L have been reported inpatients who consumed large amounts of licorice thatcontained glycyrrhetinic acid, after the discontinuationof smoking (50,51). Glycyrrhetinic acid is found in avariety of flavoring agents, such as “Asam Boi,”which is used widely in Malaysia and Singapore aswell as in Japanese traditional herbal medicationsknown as Kampo medicines (52).
There have been two reported cases for whichingestion of licorice may have inadvertently served atherapeutic purpose. One patient had undiagnosed Ad-dison disease but had been clinically stable as a resultof the ingestion of approximately 46 g/d salt in theform of soy sauce combined with large quantities oflicorice sticks (53). It was postulated that licorice-induced inhibition of 11�-HSDH type II potentiatedthe effect of diminishing adrenal gland secretion ofglucocorticoids on the mineralocorticoid receptor,thereby averting full-blown adrenal crisis. Eventually,the amount of cortisol secretion became so minimalthat this potentiation effect was no longer sufficient toprevent overt signs of adrenal failure.
A second patient had undergone unilateral adre-nalectomy and required corticosteroid replacementtherapy so as to maintain a normal glucocorticoid state(54). The patient later self-discontinued replacementtherapy and presented with findings of hypercalcemia,hypertension, hypernatremia, and hypokalemic meta-bolic alkalosis. Although hypercalcemia is a feature ofacute adrenal insufficiency and readily responded tothe administration of hydrocortisone, the other find-ings were not readily explainable. Acute adrenal in-sufficiency is normally characterized by hypotension,hyponatremia, hyperkalemia, and a hyperchloremic
metabolic acidosis. It was later discovered the patienthad been consuming large quantities of licorice as alaxative. The lack of hemodynamic instability andother electrolyte abnormalities in the setting of adrenalcrisis was attributed to presumed inhibition of 11�-HSDH type II. In this setting, the effect of residualcortisol secretion from the remaining adrenal glandwould be potentiated, thereby averting overt adrenalcrisis.
Acquired inhibition of 11�-HSDH type II maybe of importance in the salt retention that occursamong some patients with cirrhosis of the liver (55).Aldosterone is generally believed to play a major rolein the renal salt retention observed in patients withcirrhosis; however, there are many examples of pa-tients who present with ascites and marked total-bodysodium excess and have either normal or suppressedaldosterone levels. Bile acids that can accumulate inthe setting of chronic liver disease have been shown toinhibit the activity of 11�-HSDH type II. Such aneffect would allow cortisol-mediated stimulation ofthe mineralocorticoid receptor and potentially explainaldosterone-independent salt retention in the distalnephron in liver cirrhosis. Studies of the bile ductligation and carbon tetrachloride models of chronicliver disease are consistent with a component of cor-tisol-mediated stimulation of the mineralocorticoid re-ceptor.
A recent report described a patient who hadsickle cell disease and developed two separate epi-sodes of hypokalemia as a result of renal K� wastingin association with sickle cell crisis (56). At baseline,the patient had a normal serum K� concentration buthad a total bilirubin of approximately 9 mg/dl, pre-sumably as a result of intrahepatic cholestasis, whichis typical of patients with this disease. During the twoseparate episodes of hemolytic crisis, the total biliru-bin increased to values between 36 and 42 mg/dl.During these episodes, the serum K� concentrationdecreased to 2.5 and 3.1 mEq/L in association with ahigh TTKG and low to normal aldosterone levels. Itwas hypothesized that worsening cholestasis led togreater bile acid inhibition of 11�-HSDH type II in thedistal nephron, allowing for cortisol-mediated renalK� wasting.
Hereditary forms of hypertension to includethose with suppressed circulating levels of renin andaldosterone has been the subject of a recent review(57). 11�-Hydroxylase deficiency and 17 �-hydroxy-
80 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

lase deficiency are rare autosomal recessive disordersthat prevent the production of cortisol. The lack offeedback control results in high ACTH levels, which,in turns, drives the synthesis of mineralocorticoids,giving rise to hypertension and hypokalemic metabolicalkalosis. Glucocorticoid administration provides cor-tisol replacement and normalizes ACTH, thereby re-moving the drive for oversecretion of metabolites withmineralocorticoid effects.
Na� retention and renal K� wasting are due tothe effects of 11-deoxycortisol and 11-deoxycortico-sterone among patients with 11�-hydroxylase defi-ciency (58). Virilization is typically present in thesepatients as a result of the overproduction of adrenalandrogens. Patients with 17 �-hydroxylase deficiencydevelop hypertension and hypokalemia as a result ofaccumulation of 11-deoxycorticosterone, corticoste-rone, and 18-hydroxycorticosterone (59,60). The en-zymatic block in these patients leads to lack of sexhormones, resulting in the clinical picture of sexualinfantilism in female patients and ambiguous or fe-male external genitalia in male patients.
The reabsorption of Na� across the apical mem-brane in the collecting duct occurs through an amilo-ride-sensitive Na� channel formed by the assembly ofthree subunits: �, �, and �. Liddle syndrome is aninherited form of hypertension and hypokalemic met-abolic alkalosis caused by mutations in this channel.These mutations either delete or alter residues in theC-terminal PY motif of the � and � subunits. Novelmutations in these subunits continue to be described(61). The PY motif of the �, �, and � subunits is thebinding site for the WW domain of a cytoplasmicprotein called Nedd4-2. The binding of Nedd4-2 to thePY motif on each of the three subunits leads toubiquination of the epithelial sodium channel, taggingit for eventual endocytosis and degradation. Interfer-ence in this binding leads to an inability to retrieve thechannel from the membrane and results in increasedchannel density. The resultant increase in channeldensity gives rise to the clinical characteristics, sug-gesting constitutive activation of the epithelial sodiumchannel.
The details of the Nedd4-2–induced ubiquinationprocess, and channel removal from the membranecontinues to be explored and has offered insight toother factors that are capable of influencing ENaCactivity (62,63). One such factor that has been shown
to be capable of modulating Na� transport throughENaC is epidermal growth factor (EGF). EGF leads tointracellular events through activation of extracellularsignal–regulated kinases. Studies show that EGF de-creases ENaC activity in association with extracellularsignal–regulated kinase–mediated phosphorylation ofa specific site on the � subunit near the PY motif (64).This phosphorylation reduces Na� transport initiallyby decreasing the open probability of the channel andlater through increased channel removal. In collectingduct cells derived from a mouse model of Liddlesyndrome caused by a � subunit truncating mutation,this inhibitory effect of EGF on ENaC activity is nolonger seen.
Although renal Na� retention leads to volumeexpansion and suppression of plasma renin and aldo-sterone, findings in a mouse model of Liddle syn-drome also suggested that the activity of ENaC in thecolon is increased (65). In this model, the Liddlemutation leads to a gain of function in colonic ENaCsuch that Na� reabsorption from the gastrointestinaltract is increased. This activity could further contributeto the volume expansion observed in these animals.
An autosomal dominant form of hypertensionand hypokalemia that presents at a young age andcharacteristically worsens during pregnancy has beendescribed in a single kindred. This disorder resultsfrom an activating mutation (S810L) in the mineralo-corticoid receptor. Under normal circumstances, themineralocorticoid receptor is activated by agonists thatcontain a 21-hydroxyl group such as aldosterone andcortisol. Steroids that lack the 21-hydroxyl group butcontain a 17-keto group still bind to the normal recep-tor but are incapable of activating it. By contrast, thesecompounds can both bind and activate the mutatedreceptor. Progesterone (a 17 � hydroxyl steroid) acti-vates the mutated receptor, thereby explaining theworsening of hypertension that occurs during preg-nancy when, progesterone levels are increased. Spi-ronolactone (a synthetic steroid with a 17 � lactonethat normally exhibits antagonist activity) activates themutated receptor and therefore should be avoidedbecause the drug will worsen the clinical manifesta-tions of the disorder. Recent studies detailed the bind-ing characteristics of spironolactone to both the nor-mal and the mutated receptor (66). Blocking ENaCwith amiloride or triamterene is a treatment option forthis disorder.
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 81

Primary Increase in Distal Na� DeliveryThe word “primary” refers to conditions
whereby distal Na� delivery is increased for reasonsother than expansion of extracellular fluid volume. Infact, extracellular fluid volume is either normal ordecreased, so hypertension is not a feature of thesedisorders. Impaired Na� reabsorption proximal to thecollecting duct from genetic causes or administrationof diuretics are examples of a primary increase indistal Na� delivery. Increased distal Na� delivery canalso be primary as a result of the effects of a nonre-absorbable anion. One can further categorize theseconditions as to the presence of metabolic alkalosis ormetabolic acidosis.
Active vomiting and nasogastric suction are clas-sic examples in which hypokalemia develops due tothe effects of a nonreabsorbable anion. Loss of gastricacid from the body results in the delivery of a HCO3
�
load to the kidney that exceeds the reabsorptive ca-pacity of the proximal nephron. The subsequent deliv-ery of large amounts of NaHCO3 to the distal nephron,coupled with increased aldosterone, provides the nec-essary requirements for increased renal K� excretion.
Recurrent protracted vomiting resulting in inter-mittent but severe hypokalemia can result in potentiallong-term nephrotoxicity. A renal biopsy was per-formed in such a patient with chronic peptic ulcerdisease as part of the evaluation of a reduced creati-nine clearance (67). The finding of chronic tubuloin-terstitial disease was attributed to recurrent and unre-mitting hypokalemia, a condition sometimes referredto as kaliopenic nephropathy.
Hyperemesis gravidarum is a syndrome of severevomiting that typically occurs early in pregnancy. Inaddition to HCO3
�, increased urinary excretion ofketoanions acts as a nonreabsorbable anion, obligatinglarge amounts of Na� to the distal nephron. Thedevelopment of hypokalemia in this condition hasbeen shown to be an independent risk factor for thesubsequent need for emergent operative delivery (68).
Characteristic urine electrolytes in the setting ofincreased excretion of a nonreabsorbable anion areincreased urine Na� and K� but a low urinary Cl�.One would expect such findings in volume-depletedpatients who develop hypokalemia after the adminis-tration of ticarcillin and carbenicillin. These antibiot-ics are excreted as Na� salts and act as nonreabsorb-able anions. In the setting of increased aldosteronelevels, the high distal Na� delivery led to increased
renal K� excretion. A recent report described thedevelopment of severe hypokalemia in associationwith the administration of flucloxacillin (69). UrineNa� and K� both were increased as expected, buturinary Cl� was also high. Measurement of renin andaldosterone levels was suppressed, suggesting that thispatient was not volume depleted. The development ofhypokalemia in this patient was likely due to a solutediuresis driven by the large Na� load that accompa-nied the antibiotic as opposed to a nonreabsorbableanion effect, although both mechanisms may havebeen operative.
A discussion of hypokalemia in association withuse of loop and thiazide diuretics has been the subjectof a recent review (70). In patients who have hyper-tension and take thiazide diuretics, the serum K�
concentration falls on average by 0.5 mEq/L. Thisdecline can be as high as 0.9 mEq/L with the long-acting agent chlorthalidone. Although loop diureticsare more potent natriuretic agents, they typically resultin a milder degree of hypokalemia; the average declinein the serum K� concentration is 0.3 mEq/L. Thislesser effect may be related to the much shorter half-life of loop diuretics compared with the thiazide di-uretics. Although not proved, this smaller decline mayalso be related to the ability of loop diuretics to inhibitCa2� absorption in the loop of Henle. The ensuingincrease in Ca2� delivery to the lumen of the distalnephron may inhibit Na� reabsorption and thereforemay diminish distal K� secretion.
The degree of diuretic-induced hypokalemia isinfluenced by the amount of dietary salt intake. Theadministration of a diuretic in conjunction with theingestion of large amounts of dietary Na� (180 to 200mEq/L) renders a patient particularly vulnerable to thedevelopment of hypokalemia. This particular combi-nation would allow for maximal Na� and fluid deliv-ery to the distal nephron at the very time aldosteronesecretion is stimulated by the initial diuretic-inducedNa� depletion; however, extreme dietary Na� restric-tion also tends to worsen the degree of hypokalemiaassociated with the use of diuretics. The basis for thiseffect is the curvilinear relationship between dietaryNa� intake and serum renin and aldosterone levels.This relationship is gradual at Na� intakes of �80mEq/L. With Na� intakes of �50 mEq/L, however, asteep rise in renin and aldosterone levels results(71,72). At these levels, the kaliuretic effect of aldo-sterone is the predominate factor in promoting renal
82 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

K� excretion. Na� intake between these extremes (70to 100 mEq/L) causes only a slight rise in aldosteronelevels, which, when coupled with less delivery of Na�
to the distal nephron, results in an overall decrease inrenal K� excretion. Thus, moderate dietary Na� in-take in patients who have hypertension and are treatedwith diuretics not only will provide the maximal an-tihypertensive effect but also may limit the degree ofK� depletion.
The decline in the serum K� concentration usu-ally develops within the first 2 wk of therapy and thenstabilizes as a new steady state is achieved. Thereafter,the serum K� concentration should remain stable.Further declines in the serum K� concentration areprevented by several factors that serve to decreaserenal K� secretion. Increased reabsorption of Na� inthe proximal nephron as a result of the diuretic-induced decreases in extracellular fluid volume servesto dampen Na� and fluid delivery to the distalnephron. In addition, a progressive increase in miner-alocorticoid activity is prevented because the develop-ment of hypokalemia tends to inhibit release of aldo-sterone from the adrenal gland. Chronic hypokalemiais also associated with a direct cellular effect, leadingto decreased distal nephron K� excretion. Finally, K�
reabsorption is stimulated in the collecting duct underconditions of chronic hypokalemia as a result of in-creased activity of the H�-K�-ATPase pump. Thedevelopment of more severe hypokalemia in the set-ting of long-term diuretic administration suggestssome other perturbation in K� balance such as anintercurrent illness, leading to extrarenal K� loss (di-arrhea), a decrease in K� intake (vomiting), or achange in diuretic dosage.
Liver failure as a result of overdose of paraceta-mol is commonly associated with acute kidney injury;however, renal injury can also occur in the absence ofliver disease. Several recent reports emphasized thedevelopment of hypokalemia as a complication ofparacetamol overdose. The decline in the serum K�
concentration can be to values �3.0 mmol/L andtypically develops in the first 36 h after ingestion (73).In a retrospective examination of 155 patients withparacetamol overdose, an inverse relationship wasfound between the serum paracetamol level 4 h afteringestion and the decline in serum K� concentration(74). In a prospective study of 41 overdose patients,the degree of kaliuresis as measured by the fractionalexcretion of K� and the TTKG was significantly
correlated with the paracetamol concentration on ad-mission. The mechanism of K� wasting in this situa-tion is not known but is presumably due to a directtoxic effect of the drug on the kidney.
Quetiapine is an oral antipsychotic drug used inthe treatment of schizophrenia and bipolar disorder.Large doses of the drug can precipitate the develop-ment of hypokalemia within several hours of admin-istration (75). The rapidity of development suggests aK� shift into cell; however, the exact mechanism isnot known. Although not well studied, this complica-tion is said to occur more commonly in patients ofAsian descent.
Cleistanthus collinus is a plant used in suicidaland homicidal poisoning in India. A life-threateningcomplication of the poisoning is the precipitation of amyasthenic crisis–like syndrome as a result of neuro-muscular blockade (76). Hypokalemia has also beendescribed in this setting and attributed to renal K�
wasting, although the exact mechanism is not known.A variety of fluid and electrolyte disorders to
include hypokalemia can occur in association withleukemia and lymphomas either through direct effectsof the tumor or as a result of treatment strategies (77).Increased urinary excretion of lysozyme, particularlyin the setting of acute monocytic and myelomonocyticleukemia, leads to renal K� wasting (78). Both tubulartoxicity and a nonreabsorbable anion effect of ly-sozyme has been suggested to account for this effect.
Hypokalemia is particularly common in the bonemarrow transplant setting, developing in �80% ofcases (79). Administration of diuretics, amphotericinB, and hypomagnesemia are just a few of severalpotential causes of renal K� wasting in this setting.With regard to amphotericin B, patients with protein-uria are less prone to develop renal K� wasting (80).This protective effect may be a result of binding ofamphotericin B to protein in the tubular lumen, result-ing in less available free drug to cause tubular toxicity.
Hypomagnesemia is also a widely recognizedcause of renal K� wasting. A recent review summa-rized evidence to support an inhibitory effect of intra-cellular Mg2� on K� secretion through ROMK chan-nels in the distal nephron (81). A decrease inintracellular Mg2� in the setting of Mg2� deficiencywould release this inhibitory effect, causing increasedrenal K� secretion. This kaliuretic effect is likely to beexacerbated under conditions of increased distal Na�
delivery and increased aldosterone.
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 83

Intracellular Mg2� acts to inhibit K� secre-tion through ROMK in the distal nephron.Depletion of intracellular Mg2� in the set-ting of hypomagnesemia may account forthe renal K� wasting typically present inthis setting.
Direct infiltration into the kidney occurs in 30 to40% of lymphoma cases. Renal involvement can leadto bilateral enlargement of the kidney and occasionallyacute kidney injury, possibly as a result of increasedintrarenal pressures (82). These tumors are typically ofB cell origin and can be diagnosed with tissue obtainedon renal biopsy. In one patient, diffuse lymphomatousinfiltration of the kidneys resulted in tubular dysfunc-tion, causing hypokalemia in association with renaltubular acidosis (83). The patient presented with acuteonset flaccid paralysis in the setting of a K� of 1.5mEq/L.
Capecitabine is an antineoplastic agent used inthe treatment of colorectal carcinoma. In a retrospec-tive study, 20% of patients who were treated with thisdrug developed hypokalemia (84). The degree of hy-pokalemia was proportional to urinary K�, suggestingthat the drug caused renal K� wasting. Ondansetron,used in the treatment of nausea and vomiting associ-ated with administration of chemotherapy, has alsobeen implicated in the development of renal K� wast-ing and hypokalemia (85).
Hypokalemia is a cardinal feature of type 1 distalrenal tubular acidosis (dRTA). The mechanism bywhich hypokalemia develops is likely to vary accord-ing to the underlying defect, as emphasized in a review(86). Systemic acidosis can lead to renal K� wasting.Metabolic acidosis is associated with decreased netproximal Na� reabsorption. The subsequent increasein distal delivery leads to volume contraction andactivation of the renin-angiotensin-aldosterone sys-tem. The combination of increased distal Na� deliveryand aldosterone as discussed previously would causerenal K� excretion. K� wasting can be the result ofleakage into the tubular lumen as a result of anionophoric effect as seen in the gradient type of dRTAassociated with administration of amphotericin B. Agenetic or acquired defect in the H�-K�-ATPase willincrease renal K� excretion by directly impairing K�
reabsorption in the distal nephron. The most severe
hypokalemia is seen in patients with mutations incertain subunits of the H�-ATPase pump.
Complications and Treatment of HypokalemiaHypokalemia can cause a variety of clinical man-
ifestations as a result of alterations in the excitabilityof neuromuscular tissues. Decrease in extracellular K�
concentration leads to hyperpolarization of the cellmembrane, causing the cell to become less sensitive toexciting stimuli. Clinically, this effect accounts for theassociation of hypokalemia and muscle weakness. Oc-casionally, muscle weakness can be severe enough tocause paralysis, as in patients with hypokalemic dRTAsecondary to Sjogren syndrome (87,88). Severe mus-cle weakness can also occur in the setting of dialysis.One patient who was depleted of total-body K� as aresult of severe gastroenteritis developed quadriplegiaduring the course of several hours after a hemodialysistreatment (89). The postdialysis K� concentration was0.98 mmol/L. It is important for clinicians to anticipatewhich patients are at risk for postdialysis hypokalemiaand to adjust the dialysate K� accordingly.
Under normal circumstances, exercise is associ-ated with movement of intracellular K� into the inter-stitial space in skeletal muscle. The increase in inter-stitial K� can be as high as 10 to 12 mmol with intenseexercise. This accumulation of K� has been impli-cated as a factor limiting the excitability and contrac-tile force of muscle accounting for the development offatigue (90,91). In addition, increases in interstitial K�
are thought to be an important factor in eliciting rapidvasodilation, allowing for blood flow to increase inexercising muscle (92).
Hypokalemia is a cause of rhabdomyolysis. Al-though the mechanism is likely to be multifactorial,total-body K� depletion may blunt the accumulationof K� into the interstitial space, thereby limiting bloodflow to skeletal muscle and resulting in muscle break-down. Total-body K� depletion from any cause canpotentially result in this complication and has beendescribed with vomiting, ingestion of herbal medica-tions that contain licorice, and inherited 11-hydrox-yase deficiency (93–95).
Hypokalemic nephropathy or kaliopenic ne-phropathy is a tubulointerstitial disease characterizedby polyuria, proteinuria, development of renal cysts,and loss of renal function. Histologically, there isevidence of tubular atrophy, interstitial infiltration ofmacrophages, and interstitial fibrosis. Mediators of
84 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

renal injury in this setting include local ischemia,complement activation as a result of increased ammo-niagenesis, and local effects of angiotensin II andendothelin. Studies of Sprague-Dawley rats that werefed a low-K� diet implicated impaired angiogenesis asan additional mechanism of renal injury in this disor-der (96). The renal lesion in these animals is charac-terized by an influx of macrophages likely as a resultof increased expression of monocyte chemoattractantpeptide 1 and osteopontin. A decrease in capillarydensity in the interstitium that correlated closely withthe development of interstitial fibrosis was noted.There was a significant reduction in the amount ofvascular endothelial growth factor and evidence ofoxidative stress possibly related to the local accumu-lation of macrophages.
Other studies of the Sprague-Dawley rat exam-ined whether renal injury would differ among ratsmade hypokalemic by feeding a moderately low-K�
diet or through the administration of a thiazide diuretic(97). In both groups of rats, there was evidence ofdecreased endothelial-dependent vasorelaxation thatcorrelated with the degree of hypokalemia; however,despite the same BP and degree of hypokalemia, onlythiazide-treated rats developed renal injury. The mech-anism is unclear. In addition, thiazides can causehyperaldosteronism secondary to contraction of extra-cellular fluid volume. Aldosterone has been implicatedin the development of renal injury in other types ofexperimental models. In addition, renal cysts arehighly frequent among patients with various types ofprimary hyperaldosteronism. Medical or surgical treat-ment of these disorders effectively halts the progres-sion of cysts, supporting a pathologic role of persis-tently elevated levels of aldosterone (98).
Hypokalemia may play a role in the associationbetween new-onset diabetes and use of thiazide diuret-ics. In a review of �50 trials in which thiazides werecompared with other drugs or placebo, a significantinverse relationship was found between the decrease inK� and the increase in glucose level (99). For every1-mEq/L decrease in K�, there was an approximately10-mg/dl increase in glucose. Further strengtheningthe argument that hypokalemia plays an important rolein the genesis of glucose intolerance is the observationthat prevention of hypokalemia with K� supplementsprevented the development of thiazide-induced glu-cose intolerance (100). In addition, changes in glucose
levels can be normalized after K� repletion in patientswho have hypokalemia.
The mechanism of thiazide-induced hyperglyce-mia is thought to be the result of decreased insulinreleased from the pancreatic � cell. ATP-sensitive K�
channels couple � cell metabolism to electrical activ-ity, thereby playing an essential role in the control ofinsulin secretion (101). The involvement of K� in thisprocess at least raises the possibility that K� depletionmight alter � cell insulin release. Impaired insulinrelease that is reversible with drug discontinuation orK� supplements is in contrast to the persistent insulinresistance that is typical of patients with type 2 diabe-tes. This difference in mechanism of glucose intoler-ance may help to explain the lack of convincingevidence that thiazide-induced diabetes increases theincidence of morbid or fatal cardiovascular events(102).
Central pontine myelinosis (CPM) is a lesiontypically ascribed to the rapid correction of hypona-tremia but rarely may occur in association with hypo-kalemia. A patient with a normal serum Na� concen-tration but severe hypokalemia as a result ofhyperemesis gravidarum underwent a magnetic reso-nance imaging scan after presenting with urinary in-continence, weakness, and lower extremity pain (103).A diagnosis of CPM was made on the basis of thefindings of hyperintensity within the central pons.During the course of several months, the symptomsresolved, and a repeat scan 4 mo later was normal.Hypokalemia has also been reported to be a risk factorfor CPM in patients who present with hyponatremia(104).
In the patient with hypokalemia, K� can begiven orally or intravenously as the KCl salt. KHCO3
or potassium citrate can be given when there is con-comitant metabolic acidosis. Oral administration ofKCl is safest. KCl can be given in dosages of 100 to150 mEq/d. Liquid KCl is bitter tasting, and the tabletcan be irritating to the gastric mucosa. The microen-capsulated or wax-matrix forms of KCl are bettertolerated.
Intravenous administration of K� may be neces-sary when the patient cannot take oral medications orwhen the K� deficit is large and is resulting in cardiacarrhythmias, respiratory paralysis, or rhabdomyolysis.Intravenous KCl should be given at a maximum rate of20 mEq/h and maximum concentration of 40 mEq/L.Higher concentrations will result in phlebitis. Replace-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 85

ment of KCl in dextrose-containing solutions can re-sult in further lowering of the serum K� secondary toinsulin release; therefore, saline solutions are pre-ferred.
On rare occasions, higher concentrations of K�
may have to be given. In a patient with a serum K� of2.6 mmol/L and an implantable cardiac defibrillator,rapid administration of K� successfully led to thetermination of recurrent unstable ventricular tachycar-dia (105). This patient was given a rapid bolus of 20mEq of KCl solution using a central access, followedby an additional 80 mEq orally and intravenouslyduring the next 2 h. A 12-yr-old boy with a K� of 1.2mEq/L as a result of gastrointestinal losses was given140 mEq of KCl as a hand-pushed bolus after devel-oping pulseless ventricular tachycardia (106). The bo-lus administration led to resolution of the arrhythmia.Aggressive K� administration of this type requiresfrequent measurement of serum K� and continuouselectrocardiographic monitoring to prevent iatrogenichyperkalemia. In a retrospective look at 140 hospital-ized patients with hypokalemia, 16% of patients de-veloped therapy-induced hyperkalemia. Comparedwith patients who simply corrected to normal, theamount of K� given was greater for patients withiatrogenic hyperkalemia (107).
References1. Choi M, Ziyadeh F: The utility of the transtubular potassium
gradient in the evaluation of hyperkalemia. J Am Soc Nephrol 19:424–426, 2008
2. Luzi L, Zoppini G, Targher G, Battezzati A, Muggeo M, Bonora E:Insulin effect on serum potassium and auto-inhibition of insulinsecretion is intact in a patient with leprechaunism despite severeimpairment of substrates metabolism. Diabetes Metab Res Rev 24:205–210, 2008
3. Marinella M: Refeeding syndrome in cancer patients. Int J ClinPract 62: 3: 460–465, 2008
4. Gariballa S: Refeeding syndrome: A potentially fatal condition butremains underdiagnosed and undertreated. Nutrition 24: 604–606,2008
5. Miller S: Death resulting from overzealous total parenteral nutrition:The refeeding syndrome revisited. Nutr Clin Pract 23: 166–171,2008
6. Lin C, Chen Y, Chen H, Liu C, Wu C: Life-threatening ventriculararrhythmia induced by hypokalemia during sodium bicarbonateinfusion. South Med J 101: 215–216, 2008
7. Dalamanga M, Karmaniolas K, Nikolaidou A, Papadavid E: Hy-pocalcemia, hypomagnesemia, and hypokalemia following hy-drofluoric acid chemical injury. J Burn Care Res 2, 2008
8. Yamaura K, Kao B, Iimori E, Urakami H, Takahashi S: Recurrentventricular tachyarrhythmias associated with QT prolongation fol-lowing hydrofluoric acid burn. J Toxicol Clin Toxicol 35: 3: 311–313, 1997
9. Sanz-Gallen P, Nogue S, Munne P, Faraldo A: Hypocalcaemia and
hypomagnesaemia due to hydrofluoric acid. Occup Med 51: 294–295, 2001
10. Gallerani M, Bettoli V, Peron L, Manfredini R: Systematic andtopical effects of intradermal hydrofluoric acid. Am J Emerg Med16: 521–522, 1998
11. Wong A, Cheung I, Graham C: Hydroxychloroquine overdose: Casereport and recommendations for management. Eur J Emerg Med 15:16–18, 2008
12. El-Hennawy A, Nesa M, Mahmood A: Thyrotoxic hypokalemicperiodic paralysis triggered by high carbohydrate diet. Am J Ther14: 499–501, 2007
13. Hsieh M, Lyu R, Chang W, Chang K, Chen C, Chang H, Wu Y,Chen S, Ro L: Hypokalemic thyrotoxic periodic paralysis: Clinicalcharacteristics and predictors of recurrent paralytic attacks. EurJ Neurol 15: 559–564, 2008
14. Cesur M, Bayram F, Temel M, Ozkaya M, Kocer A, Ertorer M, KocF, Kaya A, Gullu S: Thyrotoxic hypokalaemic periodic paralysis ina Turkish population: Three new case reports and analysis of thecase series. Clin Endocrinol 68: 143–152, 2008
15. Tagami T, Usui T, Shimatsu A, Naruse M: Toxic thyroid adenomapresenting as hypokalemic periodic paralysis. Endocrine J 54:797–803, 2007
16. Yang W, Chu P, Liu C, Chung G, Wu K: Thyrotoxic periodicparalysis induced by pegylated interferon alpha plus ribavirin forchronic hepatitis C. J Clin Gastroenterol 42: 112–113, 2008
17. Cesur M, Gursoy A, Avcioglu U, Erdogan M, Corapciglu D, KamelN: Thyrotoxic hypokalemic periodic paralysis as the first manifes-tation of interferon-�-induced graves disease. J Clin Gastroenterol40: 864–865, 2006
18. Wang W, Jian L, Ye L, Zhu N, Tingwei Su, Guan L, Li X, Ning G:Mutation screening in Chinese hypokalemic periodic paralysis pa-tients. Mol Genet Metab 87: 359–363, 2006
19. Jongjaroenprasert W, Chanprasertyotin S, Butadeg S, Nakasatien S,Charatcharoenwitthaya N, Himathongkam T, OngphiphadhankakulB: Association of genetic variants in GABRA3 gene and thyrotoxichypokalaemic periodic paralysis in Thai population. Clin Endocri-nol 68: 646–651, 2008
20. Finsterer J: Primary periodic paralyzes. Acta Neurol Scand 117:145–158, 2008
21. Kim J, Kim M, Lee S, Kim D, Lee B: The genotype and clinicalphenotype of Korean patients with familial hypokalemic periodicparalysis. J Korean Med Sci 22: 946–951, 2007
22. Ryan A, Matthew E, Hanna M: Skeletal-muscle channelopathies:Periodic paralysis and nondystrophic myotonias. Curr Opin Neurol20: 558–563, 2007
23. Segal M, Rogers G, Needleman H, Chapman C: Hypokalemicsensory overstimulation. J Child Neurol 22: 1408–1410, 2007
24. Ikuta S, Yasui C, Kawanaka M, Aihara T, Yoshie H, Yanagi H,Mitsunobu M, Sugihara A, Yamanaka N: Watery diarrhea, hypoka-lemia and achlorhydria syndrome due to an adrenal pheochromo-cytoma. World J Gastroenterol 13: 4649–4652, 2007
25. Sitprija V: Altered fluid, electrolyte and mineral status in tropicaldisease, with an emphasis on malaria and leptospirosis. Nat ClinPract 4: 91–101, 2008
26. Andrade L, Rodrigues A, Sanches T, Souza R, Seguro A: Lepto-spirosis leads to dysregulation of sodium transporters in the kidneyand lung. Am J Physiol Renal Physiol 292: F586–F592, 2007
27. Andrade L, Cleto S, Seguro A: Door-to-dialysis time and dailyhemodialysis in patients with leptospirosis: Impact on mortality.Clin J Am Soc Nephrol 2: 739–744, 2007
28. Van Dinter T, Fuerst F, Richardson C, Santa Ana C, Polter D,Fordtran J, Binder H: Stimulated active potassium secretion in apatient with colonic pseudo-obstruction: A new mechanism ofsecretory diarrhea. Gastroenterology 129: 1268–1273, 2005
29. Blondon H, Bechade D, Desarame J, Algayres J: Secretory diarrheawith high faecal potassium concentrations: A new mechanism of
86 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

diarrhea associated with colonic pseudo-obstruction? Report of fivepatients. Gastroenterol Clin Biol 32: 401–404, 2008
30. Tanrikut C, McDougal S: Acid-base and electrolyte disorders afterurinary diversion. World J Urol 22: 168–171, 2004
31. Cruz D, Huot S: Metabolic complications of urinary diversion: Anoverview. Am J Med 102: 477–484, 1997
32. Murakami K, Tomita M, Kawamura N, Hasegawa M, Nabeshima K,Hiki Y, Sugiyama S: Severe metabolic acidosis and hypokalemia ina patient with enterovesical fistula. Clin Exp Nephrol 11: 225–229,2007
33. Thomas L, Kumar R: Control of renal solute excretion by entericsignals and mediators. J Am Soc Nephrol 19: 207–212, 2008
34. Michell A, Debnam E, Unwin R: Regulation of renal function by thegastrointestinal tract: Potential role of gut-derived peptides andhormones. Annu Rev Physiol 70: 379–403, 2008
35. Lee F, Oh G, McDonough A, You J: Evidence for gut factors in K�homeostasis. Am J Physiol Renal Physiol 293: F541–F547, 2007
36. Wong L, Hsu T, Perlroth M, Hofmann L, Haynes C, Katznelson L:Reninoma: Case report and literature review. J Hypertens 26:368–373, 2008
37. Okura T, Irita J, Enomoto D, Manabe S, Kurata M, Miyoshi K,Fukuoka T, Higaki J: A case of hyperreninemic hypertension withbilateral positive captopril renography but without renovascularstenosis. Hypertens Res 31: 383–386, 2008
38. Patel T, Goes N: Page kidney. Kidney Int 72: 1562, 200739. Rossi G, Pessina A, Heagerty A: Primary aldosteronism: An update
on screening, diagnosis and treatment. J Hypertens 26: 613–621,2008
40. Bernini G, Moretti A, Orlandini C, Berti P, Miccoli P, Bardini M,Taurino C, Bernini M, Salvetti A: Plasma and urine aldosterone toplasma rennin activity ratio in the diagnosis of primary aldosteron-ism. J Hypertens 26: 981–988, 2008
41. Mazza A, Zambon S, Armigliato M, Zennaro R, Cuppini S, Rem-pelou P, Rubello D, Pessina A: Endocrine arterial hypertension:Diagnostic approach in clinical practice. Minerva Endocrinol 33:127–146, 2008
42. Mulatero P, Bertello C, Rossato D, Mengozzi G, Milan A, GarroneC, Giraudo G, Passarino G, Garabello D, Verhoves A, Rabbia F,Veglio F: Roles of clinical criteria, computed tomography scan, andadrenal vein sampling in differential diagnosis of primary aldoste-ronism subtypes. J Clin Endocrinol Metab 93: 1366–1371, 2008
43. Stratakis C, Boikos S: Genetics of adrenal tumors associated withCushing’s syndrome: A new classification for bilateral adrenocor-tical hyperplasias. Nat Clin Pract 3: 748–757, 2007
44. Horvath A, Giatzakis C, Tsang K, Greene E, Osorio P, Boikos S,Libe R, Patronas Y, Robinson-White A, Remmers E, Bertherat J,Nesterova M, Stratakis C: A cAMP-specific phosphodiesterase(PDE8B) that is mutated in adrenal hyperplasia is expressed widelyin human and mouse tissues: A novel PDE8B isoform in humanadrenal cortex. Eur J Hum Genet 16: 1245–1253, 2008
45. Horvath A, Stratakis C: Unraveling the molecular basis of mi-cronodular adrenal hyperplasia. Curr Opin Endocrinol DiabetesObes 15: 227–233, 2008
46. Quack I, Vonend O, Sellin L, Segbauer J, Dekomien G, Rump L: ATale of two patients with Mendelian hypertension. Hypertension 51:609–614, 2008
47. Lin C, Yao N, Cheng M, Lin S: Ectopic ACTH syndrome associatedwith large-cell neuroendocrine carcinoma of the lung. Am J Med Sci334: 487–490, 2007
48. Bailey M, Paterson J, Hadoke P, Wrobel N, Bellamy C, BrownsteinD, Seckl J, Mullins J: A switch in the mechanism of hypertension inthe syndrome of apparent mineralocorticoid excess. J Am SocNephrol 19: 47–58, 2008
49. Sontia B, Mooney J, Gaudet L, Touyz R: Pseudohyperaldosteron-ism, liquorice, and hypertension. J Clin Hypertens 10: 153–157,2008
50. Mumoli N, Cei M: Licorice-induced hypokalemia. Int J Cardiol124: e42–e44, 2008
51. Tancevski I, Eller P, Spiegel M, Kirchmair R, Patsch J: Maliciouslicorice. Circulation 117: e299, 2008
52. Ohtake N, Kido A, Kubota K, Tsuchiya N, Morita T, Kase Y,Takeda S: A possible involvement of 3-monoglucuronyl-glycyrrhe-tinic acid, a metabolite of glycyrrhizin (GL), in GL-inducedpseudoaldosteronism. Life Sci 80: 1545–1552, 2007
53. Cooper H, Bhattacharya B, Verma V, McCulloch AJ, Smellie W,Heald A: Liquorice and soy sauce, a life-saving concoction in apatient with Addison’s disease. Ann Clin Biochem 44: 397–399,2007
54. Isaia G, Pellissetto C, Ravazzoli M, Tamone C: Acute adrenal crisisand hypercalcemia in a patient assuming high liquorice doses.Minerva Med 99: 91–94, 2008
55. Frey F: Impaired 11�-hydroxysteroid dehydrogenase contributes torenal sodium avidity in cirrhosis: Hypothesis or fact? Hepatology44: 795–801, 2006
56. Jaitly M, Mohan S, Park C, Anderson H, Cheng J, Pogue V:Hypokalemia during sickle cell crises apparently due to intermittentmineralocorticoid excess. Am J Kidney Dis 51: 319–325, 2008
57. Vehaskari V: Heritable forms of hypertension. Pediatr Nephrol July24, 2007 [epub ahead of print]
58. Nimkarn S, New M: Steroid 11beta-hydroxylase deficiency congen-ital adrenal hyperplasia. Trends Endocrinol Metab 19: 96–99, 2008
59. Shoemaker L, Eaton B, Buchino J: A three-year-old with persistenthypokalemia. J Pediatr 151: 696–699, 2007
60. Benetti-Pinto C, Vale D, Garmes H, Bedone A: 17-Hydroxyproges-terone deficiency as a cause of sexual infantilism and arterialhypertension: Laboratory and molecular diagnosis—A case report.Gynecol Endocrinol 23: 94–98, 2007
61. Rossi E, Farnettie E, Debonneville A, Nicoli D, Grasselli C, Regol-isti G, Negro A, Perazzoli F, Casali B, Mantero F, Staub O: Liddle’ssyndrome caused by a novel missense mutation (P617L) of theepithelial sodium channel beta subunit. J Hypertens 26: 921–927,2008
62. Wiemuth D, Ke Y, Rohlfs M, McDonald F: Epithelial sodiumchannel (ENaC) is multi-ubiquitinated at the cell surface. BiochemJ 405: 147–155, 2007
63. Kabra R, Knight K, Zhou R, Snyder P: Nedd4–2 induces endocy-tosis and degradation of proteolytically cleaved epithelial Na�channels. J Biol Chem 283: 6033–6039, 2008
64. Falin R, Cotton C: Acute downregulation of ENaC by EGF involvedthe PY motif and putative ERK phosphorylation site. J Gen Physiol130: 313–328, 2007
65. Bertog M, Cuffe J, Pradervand S, Hummler E, Hartner A, Porst M,Hilgers K, Rossier B, Korbmacher C: Aldosterone responsiveness ofthe epithelial sodium channel (ENaC) in colon is increased in amouse model for Liddle’s syndrome. J Physiol 586: 459–475, 2008
66. Huyet J, Pinon G, Fay M, Fagart J, Rafestin-Oblin M: Structuralbasis of spirolactone recognition by the mineralocorticoid receptor.Mol Pharmacol 72: 563–571, 2007
67. Akimoto T, Saito O, Kotoda A, Nishino K, Umino T, Muto S,Kusano E: A case of recurrent renal failure associated with meta-bolic alkalosis induced by protracted vomiting. Clin Exp Nephrol10: 279–283, 2006
68. Tan P, Jacob R, Quek K, Omar S: Pregnancy outcome in hypereme-sis gravidarum and the effect of laboratory clinical indicators ofhyperemesis severity. J Obstet Gynaecol 33: 457–464, 2007
69. Hoorn E, Zietse R: Severe hypokalemia caused by flucloxacillin. JAntimicrob Chemother 61: 1396–1398, 2008
70. Palmer B, Naderi A: Metabolic complications associated with use ofthiazide diuretics. J Am Soc Hypertens 1: 381–392, 2007
71. Van Brummelenp P, Schalekamp M, De Graeff J: Influence ofsodium intake on hydrochlorothiazide-induced changes in blood
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 87

pressure, serum electrolytes, renin and aldosterone in essentialhypertension. Acta Med Scand 204: 151–157, 1978
72. Landmann-Suter R, Struyvenberg A: Initial potassium loss andhypokalaemia during chlorthalidone administration in patients withessential hypertension: The influence of dietary sodium restriction.Eur J Clin Invest 8: 155–164, 1978
73. Godber I, Jarvis S, Maguire D: Hypokalaemia following paraceta-mol overdoes in two teenage girls. Ann Clin Biochem 44: 403–405,2007
74. Pakravan N, Bateman D, Goddard J: Effect of acute paracetamoloverdose on changes in serum and urine electrolytes. Br J ClinPharmacol 64: 824–832, 2007
75. Lin Y, Chen H, Chang T, Lane H: Hypokalemia following rapidtitration of quetiapine treatment. J Clin Psychiatry 69: 165–166,2008
76. Damodaram P, Manohar I, Kumar D, Mohan A, Vengamma B:Myasthenic crisis-like syndrome due to cleistanthus collinus poi-soning. Indian J Med Sci 62: 62–64, 2008
77. O’Regan S, Carson S, Chesney R, Drummon K: Electrolyte andacid-base disturbances in the management of leukemia. Blood 49:345–353, 1977
78. Muggia F, Heinemann H, Farhangi M, Osserman E: Lysozyrmuriaand renal tubular dysfunction in monocytic and myelomonocyticleukemia. Am J Med 47: 351–366, 1969
79. Philibert D, Desmeules S, Filion A, Poirier M, Agharazii M:Incidence and severity of early electrolyte abnormalities followingautologous hematopoietic stem cell transplantation. Nephrol DialTransplant 23: 359–363, 2008
80. Mohan S, Ahmed S, Alimohammadi B, Jaitly M, Cheng J, Pogue V:Proteinuria lowers the risk of amphotericin B-associated hypokal-aemia. J Antimicrob Chemother 60: 690–693, 2007
81. Huang C, Kuo E: Mechanism of hypokalemia in magnesium defi-ciency. J Am Soc Nephrol 18: 2649–2652, 2007
82. Tornroth T, Heiro M, Marcussen N, Franssila K: Lymphomasdiagnosed by percutaneous kidney biopsy. Am J Kidney Dis 42:960–971, 2003
83. Jhamb R, Gupta N, Gar S, Kumar S, Gulati S, Michra D, BeniwalP: Diffuse lymphomatous infiltration of kidney presenting as renaltubular acidosis and hypokalemic paralysis: Case report. Croat MedJ 48: 860–863, 2007
84. Saif M, Fekrazad M, Ledbetter L, Diasio R: Hypokalemia secondaryto capecitabine: A hidden toxicity? Ther Clin Risk Manag 3:177–180, 2007
85. Turner S, Pinsk M: Ondansetron-associated hypokalemia in a2-year-old with pre-B-cell ALL. J Pediatr Hematol Oncol 30:58–60, 2008
86. Batlle D, Moorthi K, Schlueter W, Kurtzman N: Distal renal tubularacidosis and the potassium enigma. Semin Nephrol 26: 471–478,2006 [published erratum appears in Semin Nephrol 27: 373, 2007]
87. Comer D, Droogan A, Young I, Maxwell A: Hypokalaemic paral-ysis precipitated by distal renal tubular acidosis secondary toSjogren’s syndrome. Ann Clin Biochem 45: 221–225, 2008
88. Aygen B, Dursun F, Dogukan A, Ozercan I, Celiker H: Hypokale-mic quadriparesis associated with renal tubular acidosis in a patientwith Sjogren’s syndrome. Clin Nephrol 69: 306–309, 2008
89. Saif I, Halim A, Saif M, Siddiqui U, Rahman M, Azam N: Severepost-dialysis hypokalaemia leading to quadriparesis. J Pak MedAssoc 58: 41–43, 2008
90. Clausen T, Nielsen O: Potassium, Na�, K�-pumps and fatigue inrat muscle. J Physiol 584: 295–304, 2007
91. McKenna M, Bangsbo J, Renaud J: Muscle K�, Na�, and C1�disturbances and Na�-K� pump inactivation: Implications forfatigue. J Appl Physiol 104: 288–295, 2008
92. Clifford P: Skeletal muscle vasodilatation at the onset of exercise.J Physiol 583: 825–833, 2007
93. Atabek M, Pirgon O, Sert A: Hypokalemic rhabdomyolysis in a
child with 11-hydroxylase deficiency. J Pediatr Endocrinol Metab21: 93–96, 2008
94. Yasue H, Itoh T, Mizuno Y, Harada E: Severe hypokalemia,rhabdomyolysis, muscle paralysis, and respiratory impairment in ahypertensive patient taking herbal medicines containing licorice.Intern Med 46: 575–578, 2007
95. Possamai L, Waring W: Acute myopathy in a patient with esopha-geal stricture. Age Ageing 36: 698–699, 2007
96. Reungjui S, Roncal C, Sato W, Glushakova O, Croker B, Suga S,Ouyang X, Tunsanga K, Nakagawa T: Hypokalemic nephropathy isassociated with impaired angiogenesis. J Am Soc Nephrol 19:125–134, 2008
97. Reungjui S, Hu H, Mu W, Roncal C, Croker B, Patel J, NakagawaT, Srinivas T, Byer K, Simoni J, Wesson D, Sitprija V, Johnson R:Thiazide-induced subtle renal injury not observed in states ofequivalent hypokalemia. Kidney Int 72: 1483–1492, 2007
98. Novello M, Catena C, Nadalini E, Colussi G, Baroselli S, Chiuch A,Lapenna R, Bazzocchi M, Sechi L: Renal cysts and hypokalemia inprimary aldosteronism: Results of long-term follow-up after treat-ment. J Hypertens 25: 1443–1450, 2007
99. Zillich A, Garg J, Basu S, Bakris G, Carter B: Thiazide diuretics,potassium, and the development of diabetes: A quantitative review.Hypertension 48: 219–224, 2006
100. Alderman M: New onset diabetes during antihypertensive therapy.Am J Hypertens 21: 493–499, 2008
101. Koster J, Remedi M, Masia R, Patton B, Tong A, Nichols C:Expression of ATP-insensitive KATP channels in pancreatic beta-cells underlies a spectrum of diabetic phenotyes. Diabetes 55:2957–2964, 2006
102. Barzilay J, Cutler J, Davis B: Antihypertensive medications and riskof diabetes mellitus. Curr Opin Nephrol Hypertens 16: 256–260,2007
103. Patel S, Parish D, Patel R, Grimsley E: Resolution of MRI findingsin central pontine myelinosis associated with hypokalemia. Am JMed Sci 334: 490–492, 2007
104. Heng A, Vacher P, Aublet-Cuvelier B, Garcier J, Sapin V, Deteix P,Souweine B: Centropontine myelinolysis after correction of hypo-natremia: Role of associated hypokalemia. Clin Nephrol 67: 345–351, 2007
105. Philips D, Bauch T: Rapid correction of hypokalemia in a patientwith an ICD and recurrent ventricular tachycardia. J Emerg MedMarch 27, 2008 [epub ahead of print]
106. Garcis E, Nakhleh N, Simmons D, Ramsay C: Profound hypokale-mia: Unusual presentation and management in a 12-year-old boy.Pediatr Emerg Care 24: 157–160, 2008
107. Crop M, Hoorn E, Lindemans J, Zietse R: Hypokalaemia andsubsequent hyperkalaemia in hospitalized patients. Nephrol DialTransplant 22: 3471–3477, 2007
HyperkalemiaThe normal adult is in potassium (K�) balance
such that dietary intake is matched by K� excretionprimarily by the kidney, with a lesser contribution bythe gastrointestinal tract. K� is freely filtered by theglomerulus and then reabsorbed in the proximal tubuleand loop of Henle such that only 10% of the filteredload reaches the distal nephron. In this segment, K�
secretion primarily occurs in the initial collecting ductand the cortical collecting duct. Under most physio-logic and pathologic conditions, K� delivery to thedistal nephron remains small and is fairly constant. By
88 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

contrast, the rate of K� secretion by the distal nephronvaries and is regulated according to physiologic needs.K� secretion in the distal nephron is generally respon-sible for most urinary K� excretion.
Two populations of K� channels have been iden-tified in the cells of the cortical collecting duct. TheROMK channel is considered the major K�-secretorypathway. This channel is characterized by having lowconductance and a high probability of being openunder physiologic conditions. The maxi-K� channel ischaracterized by a large single-channel conductanceand is relatively quiescent in the basal state. Thischannel is activated by increases in intracellular Ca2�
concentration, and stress and is thought to play a majorrole in flow-stimulated K� secretion. This channel isfound in both principal cells and intercalated cells butmay have a density greater in the latter (1).
In contrast to adults, growing infants and chil-dren are in a state of positive K� balance, whichcorrelates with growth and increasing cell number. Inearly developmental stages, there is a limited capacityof the distal nephron to secrete K� as a result ofdecreased numbers of apically located K� channels.The increase in K� secretory capacity with maturationis initially a result of increased expression of ROMK.Several weeks later, there is evidence of flow-medi-ated K� secretion as maxi-K� channels begin to beexpressed (reviewed in reference2). This temporalsequence in K� channel expression helps to explainthe transient hyperkalemia typically seen in the peri-natal period of infants with type II Bartter syndrome.These patients have a mutation in ROMK that severelylimits K� secretion in the collecting duct. With time,maxi-K� channel expression begins to appear, andhyperkalemia gives way to the typical hypokalemia asa result of increased flow-mediated K� secretion.
The H�-K�-ATPase is a pump that coupleshydrogen (H�) secretion to K� reabsorption in thedistal nephron. The activity of this pump is similar innewborns and adults. K� reabsorption through thepump along with decreased expression of K�-secre-tory channels contributes to K� retention in the neo-natal kidney. These features of distal K� handling bythe developing kidney are a likely explanation for thehigh incidence of nonoliguric hyperkalemia in preterminfants (3). When therapy is needed in such patients,salbutamol infusion is more effective and safer thanuse of a rectal cation-exchange resin (4).
In contrast to adults, growing infants andchildren are in a state of positive K� bal-ance, which correlates with growth andincreasing cell number. An intact H�-K�-ATPase along with decreased expressionof K�-secretory channels contributes toK� retention in the neonatal kidney.
PseudohyperkalemiaPseudohyperkalemia is an in vitro phenomenon
that is a result of the mechanical release of K� fromcells during the phlebotomy procedure or specimenprocessing. Common causes of pseudohyperkalemiainclude fist clenching during the phlebotomy proce-dure, application of tourniquets, and use of small-boreneedles (5). Variations in ambient temperature canalso influence the laboratory determination of K�
values. The incidence of pseudohyperkalemia in-creases during the winter, when samples are likely tobe exposed to lower ambient temperatures duringtransport (6). Higher ambient temperatures decreasethe frequency of this complication.
A spurious increase in plasma K� concentrationshould be considered when accompanied by a verylow plasma Ca2� concentration. In vitro contamina-tion with K-EDTA, a liquid used as an anticoagulantin certain sampling tubes, can cause this problemthrough Ca2� chelation and simultaneous release ofK� (7). Pathologic causes of pseudohyperkalemia aremostly seen in the setting of hematologic disorderssuch as thrombocytosis and pronounced leukocytosis.This disorder was recently described in a patient withmyelofibrosis complicated by giant platelets and nu-cleated red blood cells (8).
The incidence of pseudohyperkalemia in-creases during the winter, when samplesare likely to be exposed to lower ambienttemperatures during transport. Higher am-bient temperatures decrease the fre-quency of this complication.
Clinical Manifestation of HyperkalemiaAll of the clinically important manifestations of
hyperkalemia occur in excitable tissue. Neuromuscu-lar manifestations include paresthesias and fascicula-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 89

tions in the arms and legs. As the serum K� continuesto rise, an ascending paralysis with eventual flaccidquadriplegia supervenes. Classically, trunk, head, andrespiratory muscles are spared, but rarely respiratoryfailure can occur.
The depolarizing effect of hyperkalemia on theheart is manifested by changes that are observablein the electrocardiogram (ECG). The progressivechanges of hyperkalemia are classically listed as peak-ing of T waves, ST-segment depression, widening ofthe PR interval, widening of the QRS interval, loss ofthe P wave, and development of a sine-wave pattern(9). The appearance of a sine-wave pattern is ominousand is a harbinger of impending ventricular fibrillationand asystole (10,11).
Hyperkalemia can also be associated with a num-ber of less common patterns on the ECG. Brugadasyndrome is a genetic disease associated with suddencardiac death as a result of mutations in a cardiac Na�
channel. ECG changes are characterized by a right-bundle branch block pattern and right precordial ST-segment elevations. A similar pattern has been re-ported in patients with hyperkalemia; however, thehyperkalemic Brugada pattern differs from the geneticdisorder in that P waves are often absent, abnormalaxis deviation is present, and the QRS complex iswider (12).
Hyperkalemia can also give rise to ECG changesthat are typical of cardiac ischemia. The tall, narrow,and symmetrical peaked T waves that are typical ofhyperkalemia can occasionally be confused with thehyperacute T-wave change associated with a ST-seg-ment elevation myocardial infarction (13); however, inthis latter condition, the T waves tend to be morebroad based and asymmetric in shape. A pseudoinfarctpattern has also been described, resembling both ananteroseptal and an inferior wall myocardial infarction(14,15). These changes resolve with treatment of thehyperkalemia and in the absence of increased cardiacenzymes. Double counting of the heart rate by ECGinterpretation software can also occur as a result ofhyperkalemic ECG changes (16).
The correlation of ECG changes and serum K�
concentration depends on the rapidity of the hyperka-lemia onset. Generally, with acute onset of hyperka-lemia, ECG changes appear at a serum K� of 6 to 7mEq/L; however, with chronic hyperkalemia, the ECGmay remain normal up to a concentration of 8 to 9mEq/L. Despite these generalities, clinical studies
show a poor correlation between serum K� concen-tration and cardiac manifestations. In a retrospectivereview, only 16 of 90 cases met strict criteria for ECGchanges reflective of hyperkalemia (defined as newpeaked and symmetric T waves that resolved on fol-low-up) (17). In 13 of these cases, the cardiologist readthe ECG as showing no T-wave changes. Strict ECGchanges were noted in only one of 14 hyperkalemicpatients who manifested arrhythmias or cardiac arrest,which calls into question the prognostic use of theECG in this setting. Given the poor sensitivity andspecificity of the ECG, the authors stressed that theclinical scenario and serial measurements of K� arethe preferred tools to guide the treatment of patientswith hyperkalemia.
Excessive K� Loads: Exogenous or EndogenousIn the presence of normal renal and adrenal
function, it is difficult to ingest sufficient K� in thediet to produce hyperkalemia. Rather, dietary intake ofK� as a contributor to hyperkalemia is usually ob-served in the setting of impaired kidney function.There are examples of unusual dietary habits leadingto hyperkalemia. A 51-yr-old man developed ascend-ing symmetric paralysis in association with a serumK� of 9.0 mEq/L (18). Upon further investigation, thepatient noted daily intake of 2.5 L of orange juice,giving him an estimated K� load of 1125 mEq/d for 3wk. A 15-yr-old woman with anorexia nervosa admit-ted to a diet that consisted of up to 20 bananas eachday and small amounts of mineral water (19). Mea-surement of the serum K� on this diet ranged from 4.7to 6.1 mEq/L. The large quantity of banana intake alsocaused increased dopamine levels, which led tochanges in behavior consistent with dysthymia. A55-yr-old woman developed a serum K� of 9.6mmol/L after self-medication of potassium citrate fortreatment of dysuria (20). This patient was ingesting500 ml of the solution each week, which provided adaily K� intake of 200 mmol.
Hyperkalemia can also occur as an iatrogeniccomplication in the hospital setting. A 16-d-old infantwith newly diagnosed maple syrup urine disease wasplaced on continuous venovenous hemofiltration totreat markedly elevated levels of leucine, isoleucine,and valine (21). To treat a decrease in serum K�, a10-ml vial containing 20 mEq of KCl was injected intoa 5-L bag of replacement fluid. Within 4 min, ventric-ular premature beats that rapidly deteriorated into
90 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

ventricular fibrillation developed. The serum K� con-centration was 9.6 mEq/L. The rapid development ofhyperkalemia was attributed to injecting the KCl intothe dependent portion of the hanging 5-L bag througha port immediately adjacent to the exit port. As a resultof poor mixing, the concentrated KCl was immedi-ately delivered into the patient, resulting in life-threat-ening hyperkalemia.
Surgical diversion of the ureter into the sigmoidcolon or the terminal ileum can be associated with thedevelopment of a normal gap metabolic acidosis, par-ticularly when the exposure of urine to the intestinalmucosa is extensive and prolonged. Patients with ure-terosigmoid anastomosis can occasionally develop hy-pokalemia as a result of colonic secretion of K�. Bycontrast, anastomosis of the ureter to the jejunum canlead to hyperkalemia because this segment of theintestine normally reabsorbs K�. This complicationarose in a 77-yr-old man who underwent extensivepelvic surgery for treatment of rectal carcinoma (22).Because of the presence of multiple pelvic adhesions,the ureters were inadvertently diverted into a sectionof the jejunum. Upon institution of enteral feedingsthat contained a high K� content, the patient quicklydeveloped hyperkalemia.
Hyperkalemia can also be the result of endoge-nous K� loads. A 37-yr-old woman with stage 4chronic kidney disease (CKD) at 26 wk gestationnoted the onset of abdominal pain and cessation offetal movement (23). She was admitted to the hospitaland found to have a serum K� concentration of 6.1mEq/L that later increased to 7.5 mmol/L, despiteintensive medical management. Because of increasingabdominal pain, she was taken to the operating roomand found to have a ruptured uterus and dead fetus.The fetus was noted to have peeling skin consistentwith intrauterine death that had occurred several daysbefore the surgery. After removal of the fetus, theserum K� concentration normalized. The developmentof hyperkalemia was attributed to a K� load deliveredinto the maternal circulation from the degeneratingfetus.
Severe hemolysis can produce an endogenousK� load sufficient to cause hyperkalemia, particularlyin the setting of impaired renal function. A long-termdialysis patient with a prosthetic aortic valve devel-oped severe hemolysis and hyperkalemia after theabrupt onset of atrioventricular nodal reentrant tachy-cardia (24). The hemolysis and release of K� was
attributed to fragmentation of red blood cells by theprosthetic value as a result of the hemodynamic tur-bulence brought on by the arrhythmia.
Hyperkalemia as a result of hemolysis is also apotential complication of tropical diseases such asmalaria and leptospirosis (25). In addition to directeffects of the organism, hemolysis can develop fromdrugs that are used in the treatment of these infections,such as patients who have glucose-6-phosphate dehy-drogenase deficiency and are given primaquine.
An exogenous K� load can be one of severalfactors contributing to the development of hyperkale-mia in the setting of orthotopic liver transplantation. Aretrospective observational study identified factorsthat were associated with development of hyperkale-mia at three different time periods surrounding theprocedure (26,27). These periods included the 2 hbefore reperfusion of the allograft, the first 15 minafter reperfusion, and a late period of 1 h after reper-fusion until the end of the case. At all time periods,there was a direct correlation between the baseline K�
value and risk for hyperkalemia. In the first timeperiod, red blood cell transfusions added to this risk. Inthe second time period, hyperkalemia was more likelyto occur when the allograft was taken from a cardiacdeath donor. In the later period, risk factors includeddecreased urine output, use of venovenous bypass, andlonger warm ischemia time.
An observational prospective cohort study con-ducted in Iraq examined the prevalence of hyperkale-mia (�5.5 mmol/L) in patients with penetrating, blunt,or explosive trauma in the 12-h period beginning fromthe time of emergency department evaluation (28).Exclusion criteria were hyperkalemia and a creatininelevel of �1.5 mg/dl at the time of initial evaluation,burn, or crush injury. The period prevalence of hyper-kalemia was 29%. Risk factors included a baseline K�
concentration of �4.0 mmol/L and transfusion of cell-or plasma-based products. A subsequent report fromthe same group found that transfusion of �7 U ofpacked red blood cells (PRBCs) was independentlyassociated with this risk (29).
The risk for transfusion-associated hyperkalemiais related not only to the number of red blood celltransfusions but also to the rapidity in which the unitsare given. Concomitant conditions such as low cardiacoutput, metabolic acidosis, hypocalcemia, hyperglyce-mia, and hypothermia increase this risk (30).
Whole blood and PRBCs are stored in anticoag-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 91

ulant preservative solution and have a shelf-life ofapproximately 35 d. The duration of storage can beextended to 42 d through the addition of an additivesolution that contains varying concentrations of ade-nine, dextrose, and other substances (31). During stor-age, K� leaks into the supernatant as a result of agingof red blood cell membranes and decreased synthesisof adenosine triphosphate. The magnitude of this leakincreases with duration of storage. Irradiation of bloodto inactivate T lymphocytes and minimize the risk forgraft-versus-host disease enhances K� leakage fromred cells as a result of subtle membrane injury. De-pending on the conditions, the supernatant of storedred blood cell units may contain �60 mEq/L K�.When fresh PRBCs are unavailable, the risk for post-transfusion hyperkalemia can be minimized by wash-ing the cells and decreasing the amount of additivesolution. These maneuvers are of particular use forneonatal patients who undergo surgery for congenitalheart disease and require irradiated blood as a result ofthe concomitant presence of cell-mediated immunode-ficiency disorders (32).
Cell ShiftTissue damage is one of the most common
causes of hyperkalemia resulting from a redistributionof K� out of cells. Common clinical examples includerhabdomyolysis, trauma, massive hemolysis, and tu-mor lysis. The major regulators of K� shift into cellsare insulin and catecholamines, with a lesser effectmediated by metabolic and respiratory alkalosis.
Congenital hyperinsulinism is characterized bythe unregulated secretion of insulin from pancreatic �cells mostly as a result of mutations in subunits of thepancreatic � cell ATP-sensitive K� channel (33). Arecent report described a neonatal patient who had thisdisorder and required several weeks of intravenousglucose to avoid hypoglycemia (34). The patient ulti-mately underwent a pancreatectomy to treat the hyper-insulinemic state. In the immediate postoperative pe-riod, the patient developed a serum K� concentrationof 12.3 mmol/L complicated by ventricular tachycar-dia. The hyperkalemia was successfully treated withno further recurrence. The authors postulated thatweeks of hyperinsulinemia led to sequestration oflarge quantities of K� in the intracellular compart-ment. After pancreatectomy and the sudden removalof insulin, K� was free to exit the cells, resulting in aperiod of short-lived rebound hyperkalemia.
Another example of rebound hyperkalemia hasbeen reported in association with the infusion of thio-pental. This drug is a short-acting barbiturate thatsometimes is used in patients who experienced headtrauma to control increased intracranial pressure. In-fusion of the drug is known to cause hypokalemia as aresult of a shift into cells. Three patients who receivedlarge amounts of K� to maintain normokalemia duringthiopental infusion therapy were recently reported(35). In each case, hyperkalemia developed immedi-ately after cessation of the intravenous infusion, con-sistent with a rebound effect.
Hyperkalemia as a result of a shift out of cells isa widely known complication of the paralytic agentsuccinylcholine. Risk factors for this complicationinclude denervation, prolonged immobilization,chronic infection, and burn injury (36). Under theseconditions, acetylcholine receptors become upregu-lated and widespread throughout the skeletal musclemembrane as opposed to the normal state, wherebythey are primarily confined to the neuromuscular junc-tion. As a result, succinylcholine-induced depolariza-tion leads to a magnitude of K� efflux sufficient tocause hyperkalemia. Patients who have received pre-vious radiation therapy may also be at risk for thiscomplication (37). Such treatment can lead to chronicthermal injury to skeletal muscle and potentially causeredistribution of acetylcholine receptors similar towhat is seen with immobilization and burns.
Cell shift is a potential complication of hyper-tonic states as well. Hyperglycemia leads to watermovement from the intracellular to extracellular com-partment. This water movement favors K� efflux fromthe cell through the process of solvent drag. In addi-tion, cell shrinkage causes intracellular K� concentra-tion to increase, creating a more favorable concentra-tion gradient for K� efflux. This same phenomenonhas been described in neurosurgical patients who weregiven large amounts of hypertonic mannitol (38).
Intravenous Ig preparations contain sugar addi-tives such as sorbitol, maltose, and sucrose to preventIg aggregation. These sugars have been implicated inthe development of Ig-induced acute renal failure.Risk factors include preexisting CKD, volume deple-tion, and advanced age. Renal histology typicallyshows marked vacuolization of the tubular cells, alesion referred to as osmotic nephrosis. A less com-mon adverse effect of such therapy is the developmentof hyponatremia and hyperkalemia. In a manner sim-
92 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

ilar to that of hyperglycemia or administration ofmannitol, accumulation of these sugars in the bloodwill increase tonicity and potentially increase the se-rum K� concentration (39).
Rhabdomyolysis can cause severe hyperkalemiaas a result of leakage of K� from damaged skeletalmuscle. Malignant hyperthermia is a rare clinical syn-drome manifested by muscle rigidity, tachycardia,increased CO2 production, skin cyanosis and mottling,rhabdomyolysis, and potentially hyperkalemia (40).The onset of the disorder is usually within 1 h of theadministration of general anesthesia, with the mostcommon triggers being halothane and succinylcholine.The syndrome is due to a mutation in the gene thatencodes the skeletal muscle ryanodine receptor. Thisreceptor is a calcium channel that, when mutated,allows excess amounts of calcium to exit the sarco-plasmic reticulum, resulting in tetany and heat produc-tion. Mutational analysis is now available to identifyindividuals who are at risk for this syndrome.
The neuroleptic malignant syndrome is a similardisorder that occurs in association with ingestion ofhaloperidol and other antipsychotic drugs; however,there is no crossover susceptibility to malignant hy-perthermia, and there is no diagnostic test to predictwhich patients will develop the complication.
Cell shift is the cause of the increased serum K�
concentration in patients with hyperkalemic periodicparalysis (41,42). This disorder is most commonly dueto mutations in the sodium channel SCN4A gene. Incontrast to familial hypokalemic periodic paralysis, pa-tients with the hyperkalemic form are typically younger(�10 versus 5 to 20 yr) and have a greater frequency ofattacks that tend to be of shorter duration (�24 versus�24 h). The attacks tend to occur more commonly in themorning, whereas nighttime attacks dominate in the fa-milial hypokalemic form. The attacks can be precipitatedby fasting and K� administration.
Decreased Renal Excretion of K�
Decreased renal excretion of K� can be dividedinto one or more of three abnormalities: Abnormalcortical collecting duct function, a primary decrease inmineralocorticoid levels, and a primary decrease indistal delivery of salt and water. The relevant literatureis divided according to these categories.
Primary Decrease in Mineralocorticoid Levels orActivity. Decreased mineralocorticoid activity canresult from disturbances that originate at any point
along the renin-angiotensin-aldosterone system(RAAS). Such disturbances can be the result of adisease state or be due to effects of various drugs.Diabetes, CKD, and advancing age all are associatedwith decreased renin and aldosterone levels and havebeen identified as independent risk factors for thedevelopment of hyperkalemia (43). Elderly patientsmay also have a component of mineralocorticoid re-sistance, given the lack of increase in transtubular K�
gradient noted after the administration of fludrocorti-sone (44). The risk for hyperkalemia is further in-creased when such patients are treated with drugs thatinhibit the RAAS.
The development of hyperkalemia after the ad-ministration of angiotensin-converting enzyme inhib-itors (ACEIs) and angiotensin receptor blockers(ARBs) is of particular concern because patients whoare at highest risk for this complication are oftentimesthe same ones who derive the greatest cardiovascularbenefit. These drugs are now being used with muchgreater frequency in the posttransplantation period,when factors such as a reduced GFR and administra-tion of calcineurin inhibitors increase the likelihood ofhyperkalemia (45,46).
There is a great deal of clinical interest in com-bining drugs that block the RAAS at different points inan attempt to improve cardiovascular outcome (47,48).The downside of this approach is a greater risk forhyperkalemia, particularly because at-risk patientstend to be the target of such strategies (49,50). Studiesdesigned to assess the frequency with which cliniciansmonitor patients for the development of hyperkalemiais less than optimal (51). Perhaps more disturbing isthe time that it takes for follow-up after receipt oflaboratory results to indicate the presence of hyperka-lemia (52). Even in the setting of an emergency de-partment, there is often a delay from the time ofhyperkalemia discovery until appropriate therapy isinstituted (53).
The oral contraceptive Yasmin-28 contains thenon–testosterone-derived progestin drospirenone,which possesses mineralocorticoid-blocking effectssimilar to what is seen with spironolactone. The prod-uct labeling recommends K� monitoring in the firstmonth after prescribing the drug for patients who arereceiving K� supplements, renin-angiotensin block-ers, or nonsteroidal anti-inflammatory drugs (54). De-spite this recommendation, there are many instances inwhich monitoring does not occur or patients are pre-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 93

scribed the contraceptive in the setting of other drugsthat either provide a K� load or interfere in renal K�
secretion (55,56).
The oral contraceptive Yasmin-28 con-tains the non–testosterone-derived pro-gestin drospirenone that possesses min-eralocorticoid-blocking effects similar towhat is seen with spironolactone. The se-rum K� should be monitored when thisdrug is prescribed for patients who receiveK� supplements, renin-angiotensin block-ers, or nonsteroidal anti-inflammatorydrugs.
Factors that interfere with adrenal mineralocor-ticoid secretion are in the differential of impaired renalK� secretion. Adrenal insufficiency should be consid-ered for patients who present with abdominal pain andhyperkalemia (57). Both unfractionated and low mo-lecular weight heparin can suppress adrenal aldoste-rone production and can cause hyperkalemia (58).
Primary Decrease in Distal Delivery (Acute andChronic Renal Failure). Acute kidney injury maylead to marked decreases in distal delivery of salt andwater, which may secondarily decrease distal K� se-cretion. For this reason, hyperkalemia tends to occurmore commonly in oliguric renal failure. Hyperkale-mia is much less common in nonoliguric renal failurebecause distal delivery of salt and water is plentiful.
CKD is more complicated than acute renal fail-ure. In addition to the decreased GFR and secondarydecrease in distal delivery, there is nephron dropoutand a smaller number of collecting ducts to secreteK�; however, this is counterbalanced by an adaptiveprocess in which the remaining nephrons develop anincreased ability to excrete K�. In a study of nor-mokalemic patients with stage 4 CKD, the fractionalexcretion of K� was 126% compared with 26% innormal control subjects (59). The fractional excretionof Na� in the two groups was 2.3 and 15%, respec-tively. After the intravenous administration of amilo-ride, the fractional excretion of K� decreased by 87%in the patients with CKD compared with 19.5% incontrol patients. These findings support the idea thatpatients with CKD are able to maintain a normalserum K� concentration through an adaptive increase
in renal K� secretion that is largely amiloride sensi-tive.
Two other defenses against hyperkalemia in-clude a more rapid shift of K� into cells in responseto a K� load and a markedly increased rate of K�
excretion in the colon. Aldosterone continues toplay a role in regulating K� even in anephric pa-tients through stimulatory effects on colonic secre-tion. In this regard, fludrocortisone has been usedsporadically to control better the plasma K� con-centration in long-term dialysis patients with hyper-kalemia. In a prospective study, fludrocortisoneadministered at 0.1 mg/d was compared with notreatment in 21 hemodialysis patients with hyperka-lemia (60). At the end of 10 mo, the serum K�
concentration in the two groups was not statisticallydifferent; however, there was a decrease in serumK� compared with pretreatment values in patientswho received the drug. The emergent therapy ofhyperkalemia has been the subject of two recentreviews (61,62).
Renin-angiotensin system blockers are fre-quently used to treat hypertension in patients withESRD. Hyperkalemia is a potential concern withthese drugs, even in the functionally anephric pa-tient, to the extent that aldosterone levels fall andcolonic K� excretion decreases. Indeed, a smallnumber of patients who underwent dialysis anddeveloped hyperkalemia in association with ACEIand ARB therapy have been described. By contrast,this complication did not occur in a prospectivecrossover study of 69 maintenance hemodialysispatients who were treated with either ACEI or ARBtherapy alone or in combination (63).Distal Tubular Defects. Tubulointerstitial renal dis-eases can affect the distal nephron and lead to hyper-kalemia in the presence of only mild decreases in GFRand normal aldosterone levels. Obstructive uropathyshould be included in the differential diagnosis ofunexplained hyperkalemia (64). For patients who havebladder outlet obstruction and fail to respond to inser-tion of a Foley catheter, concomitant ureteral obstruc-tion should be considered (65). Trimethoprine-sulfa-methoxazole can interfere in renal K� secretion in amanner similar to amiloride and triamterene (66). Asimilar mechanism may account for hyperkalemia af-ter the administration of nafamostat mesylate (67,68).This drug is a synthetic serine protease inhibitor that isused for pancreatitis treatment.
94 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

Pseudohypoaldosteronism type II (PHAII; Gor-don syndrome) is an autosomal dominant form ofhypertension in which hyperkalemia and metabolicacidosis are key features. Plasma concentrations ofaldosterone are low despite the presence of hyperka-lemia, which normally exerts a stimulatory effect onaldosterone released from the adrenal gland. Admin-istration of NaCl worsens the hypertension, but Na�
given with a non-Cl anion such as sulfate or bicarbon-ate has a beneficial effect. The hypertension and hy-perkalemia are particularly responsive to the adminis-tration of thiazide diuretics.
The protein kinases WNK4 and WNK1 are re-sponsible for this disease. Wild-type WNK4 acts toreduce the surface expression of the thiazide-sensitiveNa�-Cl� co-transporter, likely through a lysosome-mediated degradation pathway. The mutant protein(inactivating mutation of WNK4) loses this ability,resulting in increased co-transporter activity accompa-nied by marked hyperplasia of the distal convolutedtubule.
In a mutant WNK4 knockin mouse model of thedisease, the apical surface area of the distal convolutedtubule was increased (69). This change was accompa-nied by increased expression of the Na�-Cl� co-transporter, providing a histologic basis to account forthe clinical findings and suggesting increased NaClreabsorption in this segment. In an attempt to deter-mine whether humans with PHAII have similarchanges in protein expression, immunoblot studieswere performed on urine samples to quantify theabundance of the Na�-Cl� co-transporter (70). Aprecedent for this approach is the known shedding ofapically located tubular proteins into the urine. Forexample, aquaporin 2 is present in the urine andincreases in concentration under conditions in whicharginine vasopressin is increased. Using this approach,urinary Na�-Cl� co-transporter protein was found tobe approximately four times higher when measured ineight patients with the disease compared with eightunrelated control patients.
Wild-type WNK4 normally stimulates clathrin-dependent endocytosis of the ROMK channel in therenal collecting duct, leading to decreased cell surfaceexpression. The mutant protein enhances this removal,giving rise to decreased K� secretion and hyperkale-mia. The process by which both wild-type and mutantWNK4 mediate the endocytosis involves a scaffoldingprotein known as intersectin (71).
WNK4 has also been shown to affect Cl� per-meability through the paracellular pathway. The mu-tated WNK4 protein causes an increase in paracellularCl� permeability by phosphorylating claudins, whichare tight junction proteins that are involved in regu-lating paracellular ion transport. This increase in per-meability dissipates the lumen-negative charge thatnormally is generated by Na� reabsorption throughthe ENaC. The reduction in luminal electronegativitywill decrease the driving force for K� secretion, pro-viding an additional mechanism by which the mutatedprotein can cause hyperkalemia. This reduction inluminal electronegativity also contributes to the devel-opment of metabolic acidosis as a result of the lessfavorable electrical gradient for H� secretion. In ad-dition, hyperkalemia slows H� secretion by limitingbuffer availability through its suppressive effect onammoniagenesis.
Mutations in WNK1 can give rise to the man-ifestations of Gordon syndrome as well. Wild-typeWNK1 normally exerts an inhibitory effect onWNK4. Mutations in WNK1 that give rise to PHAIIare gain-of-function mutations that augment thisinhibitory effect on WNK4 activity. As a result,Na�-Cl� co-transport activity is increased, andthere is increased removal of ROMK from the apicalmembrane. WNK1 can also cause salt retention byincreasing the activity of ENaC through a stimula-tory effect on SGK1. In addition, increased activityof WNK1 enhances paracellular Cl� permeability ina similar manner as disease-causing mutations inWNK4. This increase in Cl� permeability may berelated to WNK1-mediated phosphorylation of clau-din 4. The observation that hypertension in patientswith the WNK1 mutation is less sensitive to theeffects of thiazide diuretics suggests that these non–Na�-Cl� co-transporter mechanisms of salt reten-tion are quantitatively more important in causingvolume expansion in this setting.
One additional difference in the clinical manifes-tations that result from mutations in WNK4 andWNK1 relates to urinary calcium excretion. IncreasedNa�-Cl� co-transporter activity is normally associ-ated with hypercalciuria; inhibition of the co-trans-porter decreases urinary calcium excretion. This lattereffect explains the hypocalciuric effect of thiazidediuretics. Patients with the WNK4 mutation have hy-percalciuria and show a heightened sensitivity to the
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 95

hypocalciuric effects of thiazide diuretics comparedwith normal patients. These findings are consistentwith constitutive activation of the Na�-Cl� co-trans-porter as the major cause of salt retention in patientswith the WNK4 mutation. By contrast, hypercalciuriais not a feature in patients with the WNK1 mutation,suggesting that increased ENaC activity and paracel-lular Cl� permeability play a more important role inmediating salt retention in these patients comparedwith increased Na�-Cl� co-transporter activity (72).
WNK4 has also been shown to have effects onthe epithelial Ca2� channel transient receptor potentialvanilloid subfamily member 5 (TRPV5). Studies ofXenopus laevis oocytes showed that both wild-typeand mutant WNK4 exerted a positive effect onTRPV5-mediated Ca2� uptake (72). Coexpression ofthe Na�-Cl� co-transporter inhibits this stimulatoryeffect in a dosage-dependent manner. These studiessuggested that the increased expression of the Na�-Cl� co-transporter in patients with PHAII may lead tohypercalciuria through inhibitory effects on TRPV5.
Pseudohypoaldosteronism type I (PHAI) is adisorder characterized by mineralocorticoid resistancethat typically presents in newborns. Clinical findingsinclude hyperkalemia, metabolic acidosis, and a ten-dency toward volume depletion as a result of renal saltwasting. Two modes of inheritance give rise to slightlydifferent characteristics. In the autosomal recessiveform of PHAI, the defect has been localized to ho-mozygous mutations in the three subunits of theENaC. This form of the disease tends to be moresevere and requires lifelong therapy with salt to pre-vent recurrent life-threatening volume depletion. Ex-trarenal manifestations include frequent respiratorytract infections as a result of the presence of dysfunc-tional channels in the lung. Cutaneous lesions can alsodevelop as a result of the chronic irritative effect ofhigh salt concentrations in sweat.
The autosomal dominant form of PHAI resultsfrom mutations in the mineralocorticoid receptor that,in turn, results in mineralocorticoid resistance. Theclinical manifestations are limited to the kidney andtend to resolve with time such that therapy withK-binding resins and salt supplementation can even-tually be discontinued. The maintenance of normalvolume homeostasis and electrolyte values occurs atthe expense of a persistent increase in circulatingaldosterone levels in adults with the disorder. Al-
though the majority of cases are inherited in an auto-somal dominant manner, de novo mutations may beresponsible for the disease in approximately one fifthof patients (73).
The autosomal dominant and autosomal reces-sive forms of PHAI are typically diagnosed shortlyafter birth with the discovery of salt wasting andhyperkalemia. These genetic disorders need to bedistinguished from secondary causes of salt wastingand hyperkalemia as can occur in acute pyelonephritis,congenital urinary obstruction, and other renal malfor-mation disorders (74).
References1. Palmer L, Frindt G: High-conductance K channels in intercalated
cells of the rat distal nephron. Am J Physiol Renal Physiol 292:F966–F973, 2007
2. Gurkan S, Estilo G, Wei Y, Satlin L: Potassium transport in thematuring kidney. Pediatr Nephrol 22: 915–925, 2007
3. Thayyil S, Kempley S, Sinha A: Can early-onset nonoliguric hyper-kalemia be predicted in extremely premature infants? Am J Perinatol25: 129–134, 2008
4. Yaseen H, Khalaf M, Dana A, Yaseen N, Darwich M: Salbutamolversus cation-exchange resin (kayexalate) for the treatment of nono-liguric hyperkalemia in preterm infants. Am J Perinatol 25: 193–198,2008
5. Smellie W: Spurious hyperkalaemia. BMJ 334: 693–695, 20076. Bailey I, Thurlow V: Is suboptimal phlebotomy technique impacting
on potassium results for primary care? Ann Clin Biochem 45: 266–269, 2008
7. Stevens R, Laina V, Wong C, Coulson C: A case of hyperkalaemiaassociated with hypocalcaemia. Emerg Med J 25: 6, 2008
8. Duplessis C, Rakowski D, Yeung E, Hopkins M: Psuedohyperkal-emia identified in a myelofibrosis patient exhibiting giant plateletsand nucleated red blood cells. Clin Nephrol 68: 57–59, 2007
9. Petrov D, Petrov M: Widening of the QRS complex due to severehyperkalemia as an acute complication of diabetic ketoacidosis.J Emerg Med 34: 459–461, 2008
10. Scarabeo V, Baccillieri M, Di Marco A, de Conti F, Contessotto F,Piovesana P: Sine-wave pattern on the electrocardiogram and hy-perkalaemia. J Cardiovasc Med 8: 729–731, 2007
11. Pluijmen M, Hersbach F: Sine-wave pattern arrythmia and suddenparalysis that result from severe hyperkalemia. Circulation 116:e2–e4, 2007
12. Littmann L, Monroe M, Taylor K, Brearley W: The hyperkalemisBrugada sign. J Electrocardiol 40: 53–59, 2007
13. Sovari A, Assadi R, Lakshminarayanana B, Kocheril A: HyperacuteT wave, the early sign of myocardial infarction. Am J Emerg Med 25:859.e1–859.e7, 2007
14. Bellazzini M, Meyer T: Pseudo-myocardial infarction in diabeticketoacidosis with hyperkalemia. J Emerg Med September 10, 2007[epub ahead of print]
15. Tatli E, Buyuklu M, Onal B: Electrocardiographic abnormality:Hyperkalaemia mimicking isolated acute inferior myocardial infarc-tion. J Cardiovasc Med (Hagerstown) 9: 210, 2008
16. Tomcsanyi J, Wagner V, Bozsik B: Littman sign in hyperkalemia:Double counting of heart rate. Am J Emerg Med 25: 1077–1080, 2007
96 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

17. Montague B, Ouellette J, Buller G: Retrospective review of thefrequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol3: 324–330, 2008
18. Javed R, Marrero K, Rafique M, Khan M, Jamarai D, Vieira J:Life-threatening hyperkalaemia developing following excessive in-gestion of orange juice in a patient with baseline normal renalfunction. Singapore Med J 48: 11: e293–e295, 2007
19. Tazoe M, Narita M, Sakuta R, Nagai T, Narita N: Hyperkalemia andhyperdopaminemia induced by an obsessive eating of banana in ananorexia nervosa adolescent. Brain Dev 29: 369–372, 2007
20. Lyons K, McGlinchey P: Hyperkalaemic cardiac arrhythmia due toprolonged ingestion of potassium citrate. Int J Cardiol October 19,2007 [Epub ahead of print]
21. Bar-Joseph G, Tarabia M, Halberthal M, Khatib I, Eisenstein I,Zelikovic I: Mysterious hyperkalemia and cardiac arrest in a newborninfant undergoing continuous ven-venous hemofiltration dialysis:Question. Pediatr Nephrol 23: 1053–1054, 2008
22. Eskandar N, Holley J: Hyperkalaemia as a complication of ureteroi-leostomy: A case report and literature review. Nephrol Dial Trans-plant 23: 2081–2083, 2008
23. Naderi A, Palmer B: An unusual case of acute hyperkalemia duringpregnancy. Am J Obstet Gynecol 197: e7–e8, 2007
24. Papadogiannakis A, Xydakis D, Sfakianaki M, Kostakis K,Zouridakis A: An unusual cause of severe hyperkalemia in a dialysispatient. J Cardiovasc Med 8: 541–543, 2007
25. Sitprija V: Altered fluid, electrolyte and mineral status in tropicaldisease, with an emphasis on malaria and leptospirosis. Nat ClinPract 4: 91–101, 2008
26. Xia V, Ghobrial R, Du B, Chen T, Hu K, Hiatt J, Busuttil R,Steadman R: Predictors of hyperkalemia in the prereperfusion, earlypostreperfusion, and late postreperfusion periods during adult livertransplantation. Anesth Analg 105: 780–785, 2007
27. Xia V, Ghobrial R, Du B, Chen T, Hu KQ, Hiatt JR: Hyperkalemiaand liver transplantation. Liver Transplant 14: 252–256, 2008
28. Perkins R, Aboudara M, Abbott K, Holcomb J: Resuscitative hyper-kalemia in noncrush trauma: A prospective, observational study. ClinJ Am Soc Nephrol 2: 313–319, 2007
29. Aboudara M, Hurst F, Abbott K, Perkins R: Hyperkalemia afterpacked red blood cell transfusion in trauma patients. J Trauma 64:S86–S91, 2008
30. Smith H, Farrow S, Ackerman J, Stubbs J, Sprung J: Cardiac arrestsassociated with hyperkalemia during red blood cell transfusion: Acase series. Anesth Analg 106: 1062–1069, 2008
31. Bansal I, Calhoun B, Joseph C, Pothiawala M, Baron B: A compar-ative study of reducing the extracellular potassium concentration inred blood cells by washing and by reduction of additive solution.Transfusion 47: 248–250, 2007
32. Swindell C, Barker T, McGuirk S, Jones T, Barron D, Brawn W,Horsburgh A, Willetts R: Washing of irradiated red blood cellsprevents hyperkalaemia during cardiopulmonary bypass in neonatesand infants undergoing surgery for complex congenital heart disease.Eur J Cardiothorac Surg 31: 659–664, 2007
33. Hussain K, Flanagan S, Smith V, Ashworth M, Day M, Pierro A,Ellard S: An ABCC8 gene mutation and mosaic uniparental isodis-omy resulting in atypical diffuse congenital hyperinsulinism. Diabe-tes 57: 259–263, 2008
34. Austin J, Hofman P, Anderson B: Life-threatening hyperkalemiafollowing partial pancreatectomy for neonatal hyperinsulinism. Pe-diatr Crit Care Med 9: 3: e17–e19, 2008
35. Bouchard P, Frenette A, Williamson D, Perreault M: Thiopental-associated dyskalemia in severe head trauma. J Trauma 64: 838–842, 2008
36. Piotrowski A, Fendler W: Hyperkalemia and cardiac arrest followingsuccinylcholine administration in a 16-year-old boy with acute non-
lymphoblastic leukemia and sepsis. Pediatr Crit Care Med 8: 183–185, 2007
37. Holak E, Connelly J, Pagel P: Suxamethonium-induced hyperkalae-mia 6 weeks after chemoradiotherapy in a patient with rectal carci-noma. Br J Anaesth 98: 766–768, 2007
38. Hassan Z, Kruer J, Fuhrman T: Electrolyte changes during craniot-omy caused by administration of hypertonic mannitol. J Clin Anesth19: 307–309, 2007
39. Daphnis E, Stylianou K, Alexandrakis M, Xylouri I, Vardaki E,Stratigis S, Kyriazis J: Acute renal failure, translocational hypona-tremia and hyperkalemia following intravenous immunoglobulintherapy. Nephron Clin Pract 106: c143–c148, 2007
40. Rosenberg H, Davis M, James D, Pollock N, Stowell K: Malignanthyperthermia. Orphanet J Rare Dis 2: 21, 2007
41. Lengele J, Belge H, Devuyst O: Periodic paralyses: When channelsgo wrong. Nephrol Dial Transplant 23: 1098–1101, 2008
42. Grgic I, Si H, Depboylu C, Hoglinger G, Busch C, Heyken W,Kuhlmann U, Maier T, Kohler R, Hoyer J: Hyperkalaemia in atetraplegic adolescent due to de novo sodium channel mutation.Nephrol Dial Transplant 23: 1449–1451, 2007
43. Takaichi K, Takemoto F, Ubara Y, More Y: Analysis of factorscausing hyperkalemia. Intern Med 46: 823–829, 2007
44. McGreevy C, Horan J, Jones D, Biswas K, O’Meara Y, Mulkerrin E:A study of tubular potassium secretory capacity in older patients withhyperkalaemia. J Nutr Health Aging 12: 152–155, 2008
45. Salzberg D: Is RAS blockade routinely indicated in hypertensivekidney transplant patients? Curr Hypertens Rep 9: 422–429, 2007
46. Mitterbauer C, Heinze G, Kainz A, Kramar R, Horl W, Oberbauer R:ACE-inhibitor or AT2-antagonist therapy of renal transplant recipi-ents is associated with an increase in serum potassium concentrations.Nephrol Dial Transplant 23: 1742–1746, 2008
47. Bomback A, Kshirsagar A, Amamoo M, Klemmer P: Change inproteinuria after adding aldosterone blockers to ACE inhibitors ofangiotensin receptor blockers in CKD: A systematic review. Am JKidney Dis 51: 199–211, 2008
48. Weir R, McMurray J, Puu M, Solomon S, Olofsson B, Granger C,Yusuf S, Michelson E, Swedberg K, Pfeffer M: Efficacy and toler-ability of adding an angiotensin receptor blocker in patients withheart failure already receiving an angiotensin-converting inhibitorplus aldosterone antagonist, with or without a beta blocker. Findingsfrom the Candesartan in Heart Failure: Assessment of reduction inmortality and morbidity (CHARM)-Added trial. Eur J Heart Fail 10:157–163, 2008
49. Hauben M, Reich L, Gerrits C, Madigan D: Detection of spironolac-tone-associated hyperkalaemia following the Randomized AldactoneEvaluation Study (RALES). Drug Saf 30: 1143–1149, 2007
50. Desai A, Swedberg K, McMurray J, Granger C, Yusuf S, Young J,Dunlap M, Solomon S, Hainer J, Olofsson B, Michelson E, PfefferM: Incidence and predictors of hyperkalemia in patients with heartfailure. J Am Coll Cardiol 50: 1959–1966, 2007
51. Raebel M, McClure D, Chan K, Simon S, Feldstein A, Elston J,Andrade S, Gunter M, Nelson W, Roblin D, Platt R: Laboratoryevaluation of potassium and creatinine among ambulatory patientsprescribed spironolactone: Are we monitoring for hyperkalemia? AnnPharmacother 41: 193–200, 2007
52. Moore C, Lin J, McGinn T, Halm E: Factors associated with fol-low-up of severe hyperkalemia in the ambulatory setting. Am J MedQual 22: 428–437, 2007
53. Freeman K, Feldman J, Mitchell P, Donovan J, Dyer K, Eliseo L,White K, Temin E: Effects of presentation and electrocardiogram ontime to treatment of hyperkalemia. Acad Emerg Med 15: 239–249,2008
54. McAdams M, Staffa J, Pan G: The concomitant prescribing of ethinylestradiol/drospiernone and potentially interacting drugs. Contracep-tion 76: 278–281, 2007
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 97

55. Eng P, Seeger J, Loughlin J, Oh K, Walker A: Serum potassiummonitoring for users of ethinyl estradiol/drospirenone taking medi-cations predisposing to hyperkalemia: physician compliance andsurvey of knowledge and attitudes. Contraception 75: 101–107, 2007
56. Schutt B, Kunz M, Blode H: Coadministration of estradiol/dro-spirenone and indomethacin does not cause hyperkalemia in healthypostmenopausal women: A randomized open-label crossover study.J Clin Pharmacol 47: 774–781, 2007
57. Lelubre C, Lheureux P: Epigastric pain as presentation of an addiso-nian crisis in a patient with Schmidt syndrome. Am J Emerg Med 26:251.e3–251.e4, 2008
58. Thomas C, Thomas J, Smeeton F, Leatherdale B: Heparin-inducedhyperkalemia. Diabetes Res Clin Pract 80: e7–e8, 2008
59. Yeyati N, Fellet A, Arranz C, Balaszczuk A, Adrogue H: Amiloride-sensitive and amiloride-insensitive kaliuresis in advance chronickidney disease. J Nephrol 21: 93–98, 2008
60. Dong-Min K, Chung J, Yoon S, Kim H: Effect of fludrocortisonesacetate on reducing serum potassium levels in patients with end-stagerenal disease undergoing haemodialysis. Nephrol Dial Transplant 22:3273–3276, 2007
61. Sood M, Sood A, Richardson R: Emergency management and com-monly encountered outpatient scenarios in patients with hyperkale-mia. Mayo Clin Proc 82: 1553–1561, 2007
62. Putcha N, Allon M: Management of hyperkalemia in dialysis pa-tients. Semin Dial 20: 431–439, 2007
63. Han S, Won Y, Yi J, Kim H: No impact of hyperkalaemia withrenin-angiotensin system blockade in maintenance haemodialysispatients. Nephrol Dial Transplant 22: 1150–1155, 2007
64. Mirandi A, Williams T, Holt J, Kassotis J: Hyperkalemia secondaryto a postobstructive uropathy manifesting as complete heart block ina hypertensive patient receiving multiple atrioventricular nodalblocking agents. Angiology 59: 121–124, 2008
65. Segal A: A case of acute kidney injury due to complex partial,multifocal ureteral strictures. Nat Clin Pract 4: 102–108, 2008
66. Sanjay S, Annigeri R, Gopalakrishnana R: Refractory hyperkaleamiadue to trimethoprim, successfully treated with fludrocortisones. JAssoc Physicians India 55: 74–75, 2007
67. Kurisu S, Inoue I, Kawagoe T, Ishihara M, Shimatani Y, Nakama Y,Maruhashi T, Kagawa E, Dai K, Aokage T: Role of medications insymptomatic hyperkalemia. Q J Med 100: 591–596, 2007
68. Kitagawa H, Change J, Fujita T: Hyperkalemia due to nafamostatmesylate. N Engl J Med 332: 687, 1995
69. Yang S, Morimoto T, Rai T, Chiga M, Sohara E, Ohno M, Uchida K,Lin S, Moriguchi T, Shibuya H, Kondo Y, Sasaki S: Molecularpathogenesis of pseudohypoaldosteronism type II: Generation andanalysis of a Wnk4D561A/� knockin mouse model. Cell Metab 5:331–344, 2007
70. Mayan H, Attar-Herzberg D, Shaharabany M, Holtzman E, Farfel Z:Increased urinary Na-Cl cotransporter protein in familial hyperkal-aemia and hypertension. Nephrol Dial Transplant 23: 492–496, 2008
71. He G, Want H, Huang S, Huang C: Intersectin links WNK kinases toendocytosis of ROMK1. J Clin Invest 117: 1078–1087, 2007
72. Jiang Y, Ferguson W, Peng J: WNK4 enhances TRPV5-mediatedcalcium transport: potential role in hypercalciuria of familial hy-perkalemic hypertension caused by gene mutation of WNK4. Am JPhysiol Renal Physiol 292: F545–F554, 2007
73. Pujo L, Fagart J, Gary F, Papadimitriou D, Claes A, Jeunemaite X,Zennaro M: Mineralocorticoid receptor mutations are the principalcause of renal type 1 pseudohypoaldosteronism. Hum Mutat 28:33–40, 2007
74. Belot A, Ranchin B, Fichtner C, Pujo L, Rossier B, Liutkus A, MorlatC, Nicolino M, Zennaro M, Cochat P: Pseudohypoaldosteronisms,report on a 10-patient series. Nephrol Dial Transplant 23: 1636–1641, 2008
Acid Base
Metabolic AlkalosisMetabolic alkalosis is a common disorder. In a
long-term care facility a plasma HCO3� concentration
of �34 mEq/L was found in 12% of bedridden pa-tients (1). The alkalotic state was more likely to bepresent in people who required nasogastric feedingcompared with oral feeding. Although generally con-sidered a benign condition, a high blood pH is asso-ciated with pathophysiologic effects that can adverselyaffect patient outcomes. First, increases in blood pH(alkalemia) cause respiratory depression. This effect ismediated via both central and peripheral chemorecep-tors. Second, alkalosis decreases oxygen delivery tothe tissues by exerting a vasoconstrictor effect and byimpairing hemoglobin’s ability to release oxygen. Al-kalosis-induced tissue hypoxemia can adversely affectcerebral, coronary, and peripheral circulation.
The initial approach for the patient who is sus-pected of having metabolic alkalosis begins with arte-rial blood gas analysis to ensure that one is dealingwith a primary metabolic alkalosis rather than a com-pensation for a respiratory acidosis. A primary in-crease in PCO2 because of respiratory failure will leadto increased kidney HCO3
� reabsorption as a compen-satory response. In the chronic respiratory acidosissetting, the serum HCO3
� concentration increases by3.5 mEq/L for every 10-mmHg increase in PCO2. Aninadequate metabolic response to chronic hypercapniahas been associated with increased mortality (2). Thereader is referred to a recent review detailing theapproach to fluid and electrolyte and acid-base disor-ders (3).
The two ingredients that are required for meta-bolic alkalosis pathogenesis are new bicarbonate gen-eration combined with an augmentation in the kid-ney’s capacity to reclaim the filtered bicarbonate.Metabolic alkalosis generation occurs through addingnonvolatile base or removing nonvolatile acid from theblood; however, when the kidneys are functioningnormally, metabolic alkalosis causes a marked inhibi-tion of renal HCO3
� absorption, which leads to bicar-bonaturia and rapid metabolic alkalosis correction. Tomaintain a metabolic alkalosis, the kidney’s capacityto correct the alkalosis must be impaired, or, equiva-lently, the capacity to reclaim HCO3
� must be en-hanced. The relevant literature regarding this subject isgrouped according to the three ways in which meta-
98 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

bolic alkalosis can be generated: Exogenous additionof base, gastrointestinal acid loss, and renal acid loss.A comprehensive review of this subject has beenpublished (4).Exogenous Addition of Base. In the previous edi-tion of NephSAP, several cases in which metabolicalkalosis developed because of exogenous administra-tion of alkali in reduced renal function were cited. Oneunusual case was a dialysis patient who developedmetabolic alkalosis from an alkali load contained incrack cocaine. Net gain of HCO3
� can occur in thesetting of massive transfusion as a result of adminis-tration of citrate found in packed red blood cells (5). Asimilar situation can complicate plasmapheresis whencitrate containing fresh-frozen plasma is used as areplacement fluid. Self-administration of large quanti-ties of antacids that contain NaHCO3 can occur as amanifestation of pica during pregnancy or for self-treatment of abdominal pain (6,7). Severe metabolicalkalosis will develop when administered in the settingof volume depletion or renal insufficiency. Metabolicalkalosis accompanied by hypercalcemia and renalfailure can occur when excessive quantities of antacidsthat contain calcium are ingested, a condition referredto as “milk-alkali syndrome” (8).
A bicarbonate load can be delivered to a new-born transplacentally from the mother. Such a situa-tion was described in a newborn with hypokalemicmetabolic alkalosis resulting in respiratory depression(9). Measurement of serum chemistries in the motherat delivery showed similar results. NaCl and KCladministration to the infant through a nasogastric tubecorrected the metabolic alkalosis over a 3-d period.The mother was suspected of having an eating disor-der, namely bulimia, as an explanation for the meta-bolic alkalosis.Gastrointestinal Acid Loss. In vomiting or naso-gastric suction, gastric acid loss generates a metabolicalkalosis, whereas NaCl loss in the gastric fluid leadsto volume contraction (10). While the patient is vom-iting, the plasma HCO3
� concentration tends to behigher than the threshold for proximal HCO3
� reab-sorption. The delivery of large HCO3
� quantities tothe distal nephron leads to renal loss of NaHCO3
(further exacerbating total body Na� depletion) andKHCO3 (leading to K� depletion). The volume deple-tion leads to an increase in aldosterone secretion. Atthis point in time, urinary electrolytes show a urineCl� �15 mEq/L, in the presence of a high urine Na�,
a high urine K�, and a urine pH of 7 to 8. When thepatient stops vomiting, bicarbonaturia disappears, buta metabolic alkalosis is maintained by the volumecontraction and K� depletion. At this time, urine Na�
and Cl� both are low. When saline is infused into thepatient, bicarbonaturia ensues and the metabolic alka-losis is corrected.
Gastric acid loss leading to a metabolic alkalosiscan also be a complication of gastrocystoplasty (11).Although not commonly performed, this procedureinvolves implantation of a gastric patch onto the blad-der. The gastric mucosa retains its normal secretoryfunction and, depending on the patch’s size, can leadto significant acid loss from the body into the urine.The aciduria can be minimized with administration ofa proton pump inhibitor. An increased risk for malig-nancy in the gastric patch is an additional long-termcomplication of bladder augmentation procedures ofthis type (12).
The solute carrier 26 family of proteins functionsas anion exchangers or Cl� channels in the luminalmembrane of epithelial cells (reviewed in refer-ence13). Gene mutations that encode these proteinshave been associated with well-defined disease states.
Congenital chloride diarrhea is an autosomalrecessive disorder caused by mutations in the solutecarrier family 26 member 3 gene (SCLC26A3). Muta-tions lead to misfolding and abnormal trafficking of acolonic Cl�/HCO3
� exchanger (14). Patients presentat birth with watery Cl�-rich, HCO3
�-poor diarrheaand develop metabolic alkalosis. Lifelong NaCl andKCl therapy is required to prevent volume depletionand electrolyte abnormalities. The protein product ofthe SCLC26A3 gene is also found in the sweat glandand in the male seminal vesicle. Sweat Cl� is higher inthese patients but not to an extent to cause clinicalsequelae. Disturbances in sweat salt transport are min-imal because the cystic fibrosis transmembrane con-ductance regulator is the major protein regulating salttransport in the sweat glands. By contrast, these pa-tients frequently have fertility disturbances.
Mutations in the solute carrier family 26 member4 gene (SCLC26A4) gene have been linked to Pendredsyndrome. This disorder is autosomal recessive char-acterized by thyroid goiter and sensorineural hearingloss. The SCLC26A4 protein is thought to function inboth I� transport and Cl�/HCO3
� exchange. Impairedprotein function disrupts organification of I� in thethyroid and causes aberrant HCO3
� secretion in the
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 99

inner ear, leading to acidified endolymph. The pendrinprotein is also thought to mediate apical Cl�/HCO3
�
exchange in the � intercalated cell of the kidney;however, patients with Pendred syndrome have norenal manifestations in the basal state. A single patientwho had Pendred syndrome and developed a profoundhypokalemic metabolic alkalosis (K� 1.7 mEq/L,HCO3
� 43.8 mEq/L) after the routine administrationof a thiazide diuretic has been described (15). Theauthors postulated that subtle disturbances in pendrinin the distal nephron may have provoked this exces-sive response.
Metabolic alkalosis and volume depletion can bethe initial manifestation of cystic fibrosis in infantsand rarely in adults (16–18). Decreased HCO3
� se-cretion in the distal nephron is a likely explanation forthe development of this complication. There are twofunctionally distinct subtypes of intercalated cells inthe collecting duct. The � intercalated cell secretes H�
by an apical H�-ATPase. As mentioned, the � inter-calated cell secretes HCO3
� in exchange for Cl�
through an apically located Cl�/HCO3� exchanger
(pendrin). Under conditions of metabolic acidosis, �intercalated cells can convert to � type (19). Analkaline pH increases both the gene and protein ex-pression of pendrin (20). Patients with cystic fibrosisare at increased risk for volume depletion because ofexcessive loss of salt in sweat. In this setting, distalCl� delivery is markedly reduced. Because HCO3
�
secretion by the � intercalated cell requires luminalCl�, the HCO3
� secretion rate will be reduced, po-tentially explaining the development of metabolic al-kalosis in patients without a vomiting history or di-uretic use.Renal Acid Loss. In most cases, the renal generationof bicarbonate involves three features that functionsynergistically to increase H� secretion in the distalnephron and cause renal net acid excretion to exceedmetabolic acid production: (1) High distal delivery ofNa� salts, (2) mineralocorticoid excess, and (3) K�
deficiency. To augment net acid excretion and therebygenerate a metabolic alkalosis through renal mecha-nisms, Na� salt delivery to the distal nephron mustoccur with sustained or increased mineralocorticoidactivity. Aldosterone stimulates electrogenic Na� re-absorption in the principal cell of the cortical collect-ing duct, leading to an increased negative voltage inthe tubular lumen. In addition to providing a morefavorable driving force for K� secretion, this change
in lumen voltage increases the rate of H� secretion bythe � intercalated cell. For every H� secreted into thelumen, a new bicarbonate ion is returned to the blood.This coupling of increased distal Na� delivery andincreased mineralocorticoid activity leading to therenal generation of new bicarbonate is similar to theconditions that give rise to renal K� wasting and canbe approached similarly.
Primary Increase in Distal Na� DeliveryA primary increase in distal Na� delivery is
defined as increased distal delivery that is not due toexpansion of effective arterial blood volume. Effectivevolume is either normal or low, and BP is notincreased. These disorders are best differentiated onclinical grounds and measurement of urinary Na�
and Cl� concentration and/or excretion rates. Themajority of new publications regarding these condi-tions have already been discussed in the Hypokale-mia section.
Bartter syndrome is a group of complex heredi-tary disorders characterized by renal salt wasting andhypokalemic metabolic alkalosis resembling the fea-tures of chronic loop diuretic therapy. These disordersresult from gene defects that lead to decreased NaClreabsorption in the thick ascending limb of Henle.
Genetic defects of the Na�-K�-2Cl� (NKCC2)co-transporter usually present with evidence of severesalt wasting in the prenatal period (21). Typically,late-onset and mild Bartter syndrome is due to defectsin the CLCNKB gene coding for the CLC-Kb chloridechannel (22). The most recent gene defect described togive rise to Bartter syndrome is a digenic disorderinvolving both chloride channels (CLC-Kb and CLC-Ka) that normally reside on the basolateral surface ofthe thick ascending limb. Similar to patients with thegene defect in the � subunit of CLC-K (barttin), thesepatients show evidence of deafness; however, theinability to insert the channels into the membrane isdue to abnormalities in both Cl� channels as opposedto defects in the accessory Barttin protein (23).
Gitelman syndrome is an inherited disorder withclinical manifestations that mimic the long-term use ofa thiazide diuretic. This disease is due to an inactivat-ing mutation in the gene (SLC12A3) for the thiazide-sensitive NaCl co-transporter (NCC) in the distal convo-luted tubule (24,25). Immunohistochemistry performedon renal biopsy material taken from two adults withGitelman syndrome were devoid of intact NCC immu-
100 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

nostaining (26). Immunoblot studies of urine takenfrom patients also showed absent or markedly de-creased band signal for the co-transporter (27). Thedisease is generally benign, with most individualsexperiencing either no or minimal symptoms. Paraly-sis and prolongation of the QT interval with malignantarrhythmias attributed to hypokalemia and hypomag-nesemia have rarely been described (28,29).
The clinical presentation of adult patients withBartter and Gitelman syndrome is similar with re-spect to the findings of hypokalemia, metabolicalkalosis, and normal or low BP. Urinary Ca2�
excretion has been one tool used to differentiate thetwo conditions. Urine Ca2� excretion in Barttersyndrome is increased, whereas hypocalciuria is atypical feature of Gitelman syndrome. One mecha-nism to explain the hypocalciuria in patients withGitelman syndrome is increased proximal reabsorp-tion resulting from a contracted extracellular fluidvolume. In a recent study of eight patients withGitelman syndrome, extracellular fluid volume ex-pansion with isotonic saline caused only a smallincrease in urinary Ca2� excretion despite a largeincrease in urinary Na� excretion (30). This studysuggested that increased tubular Ca2� reabsorptionin more distal sites is an important component of thehypocalciuria that typically is seen in these patients.
Another test that may be useful in distinguishingpatients with Bartter and Gitelman is the change inurinary Cl� excretion after the administration of athiazide diuretic. Because patients with Gitelmansyndrome have impaired function of the thiazide-sensitive NaCl co-transporter, one would predict nochange in urinary Cl� excretion after administrationof the drug. By contrast, patients with Bartter shoulddemonstrate an increase in urinary Cl� excretion.This difference should be particularly evident be-cause the distal nephron in patients with Bartter islikely to have undergone hypertrophy because of thelong-term delivery of large NaCl quantities thatescape reabsorption in the upstream thick limb.Indeed, these predictions were verified in a cohortof patients who had Gitelman or Bartter syndromeand were given 50 mg of hydrochlorothiazide (31).The Cl� fractional clearance was increased in thepatients with Bartter syndrome, whereas only ablunted response was observed in those with Gitel-man syndrome.
Patients Bartter or Gitelman syndrome canbe distinguished by examining the changein urinary Cl� excretion after the adminis-tration of a thiazide diuretic. The Cl� frac-tional clearance will increase in patientswith Bartter syndrome, whereas only ablunted response is seen in patients withGitelman syndrome.
Because the recessive loss-of-function mutationsthat are responsible for Bartter and Gitelman syn-dromes give rise to salt wasting and normal or low BP,there has been interest in whether heterozygous muta-tions in these genes might exert a protective effect forhypertension development. Patients who participatedin the Framingham Heart Study were screened forvariations in two of the genes that are responsible forBartter syndrome (SLC12A1 encoding NCCT andKCNJ1 encoding ROMK) and the one gene that isresponsible for Gitelman syndrome (SLC12A3 encod-ing NCCT) (32). In more than 3000 individualsscreened, 49 were identified as mutation carriers.Eighty percent of the carriers had long-term systolicBP below the cohort’s mean. In particular, the long-term systolic BP among the carriers was 6.3 mmHglower that the mean of the entire cohort. The carriersshowed reduced BP from the earliest age measured tothe last. It is likely that the protection against devel-opment of hypertension in the carriers is related toeffects on renal salt handling.
Mutations in CLCNKB results in a loss of func-tion in CLC-Kb and can give rise to an adult form ofBartter syndrome. A common polymorphism in theCLC-Kb protein leads to increased Cl� transport whenexpressed in vitro, and this polymorphism is known tobe associated with essential hypertension (33). In ad-dition to providing information about the pathogenesisof essential hypertension, examination of these raregenetic diseases has given insight to novel mecha-nisms of action for therapeutic agents. For example,angiotensin II affects the trafficking of the NCC be-tween the apical membrane and submembrane vesiclesin the distal nephron (34,35). The ACEI captoprilreduces cell surface expression of the protein, suggest-ing that the drug also may lower BP by reducing saltabsorption in this segment.
As previously discussed, inactivating mutationsin WNK4 and activating mutations in WNK1 give rise
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 101

to pseudohypoaldosteronism type II in which patientsdevelop hypertension, hyperkalemia, and normal gapmetabolic acidosis. There is a great deal of interest inwhether variations in the gene mutations and alteredsignaling pathways present in pseudohypoaldosteronismtype II also might be responsible for the more commonhypertension found in the general population (34).
Acetazolamide in Metabolic Alkalosis TreatmentIn certain patients, it may be difficult to correct
the factors that are responsible for maintenance ofmetabolic alkalosis. This most frequently occurs inpatients whose metabolic alkalosis is maintained bydecreased effective arterial volume but whose cardio-vascular system cannot tolerate NaCl administration.Patients who warrant aggressive metabolic alkalosistreatment include the following: (1) Patients who havechronic lung disease and for whom intubation is im-minent or extubation is difficult and metabolic alka-losis must be corrected to improve the drive to respi-ration; (2) patients with myocardial ischemia withevolving myocardial infarction, patients who are hav-ing chest pain after infarction, or patients with unsta-ble angina; and (3) ill patients who have cerebraldysfunction and for whom cerebral hypoperfusion is apossible contributing factor.
The most commonly used approach toward cor-recting alkalosis in these patients is administration ofcarbonic anhydrase inhibitors such as acetazolamide(36,37). Carbonic anhydrase catalyzes the dehydrationof luminal carbonic acid (produced when filteredHCO3
� reacts with secreted H�) to water and CO2
and the hydration of cellular CO2 to carbonic acid,allowing the formation of H� for secretion into theluminal fluid. The uncatalyzed dehydration of car-bonic acid occurs very slowly. By inhibiting the en-zyme’s activity, carbonic anhydrase inhibitors hinderrenal acidification and thereby cause the kidney atleast partially to correct the metabolic alkalosis. Themagnitude of the bicarbonaturia induced is directlyrelated to the serum HCO3
� concentration. As theHCO3
� concentration falls, the drug’s clinical effec-tiveness declines in a parallel manner. As a result, onlyrarely does the plasma HCO3
� concentration return tonormal.
Acetazolamide is frequently used for patientswho have chronic respiratory acidosis and develop ametabolic alkalosis. Normally, among patients withchronic respiratory acidosis, the kidney’s capacity to
reabsorb bicarbonate increases, resulting in a rise inplasma HCO3
� concentration. Use of loop diureticsfor such patients, as in the treatment of cor pulmonale,can result in further increases in the serum HCO3
�
concentration. In this setting, the induction of a met-abolic alkalosis can depress ventilation, aggravatingboth the hypoxemia and hypercapnia. Normally themetabolic alkalosis can be treated by discontinuing thediuretic and administering NaCl. For the patient whois significantly edematous, however, this approachmay not be practical; in this circumstance, acetazol-amide can be used to inhibit HCO3
� reabsorption andthus lower serum HCO3
� concentration.A potential problem associated with use of car-
bonic anhydrase inhibitors in patients with lung dis-ease is a worsening of hypercapnia. Carbonic anhy-drase in normally present within red blood cells and isinvolved in CO2 movement into red cells in peripheraltissues and movement from red cells into the alveoli inthe lungs. Thus, carbonic anhydrase inhibition canprevent red cell uptake of CO2 in peripheral tissuesand can prevent CO2 release in the lung. The latter canlead to an increase in the PCO2 of the arterial blood,whereas the former leads to an even further increase inPCO2 in peripheral tissues. Generally, patients withnormal lungs can respond to this by increasing respi-ration and preventing the increase in the PCO2 of thearterial blood; however, patients with lung diseasemay not be able to respond adequately and manifestfurther increases in arterial and tissue PCO2 .
Acetazolamide is also used in the prophylaxisand treatment of acute mountain sickness. The readeris referred to a recent review of this subject (38).Monges disease (chronic mountain sickness) is char-acterized by excessive erythrocytosis frequently asso-ciated with pulmonary hypertension among peoplewho live at high altitude. The daily administration ofacetazolamide reduces erythrocytosis and improvesthe pulmonary circulation in these patients (39). Thetherapy is well tolerated, and the beneficial effects aresustained over time.
References1. Segal R, Iaina A, Lubart E, leikin I, Leibovitz A: Metabolic alkalosis
in skilled nursing patients. Arch Gerontol Geriatr 10: 1016, 20082. Uegan I, Oztuna F, Dagli CE, Yildirim H, Bal C: Relationship of
metabolic alkalosis, azotemia and morbidity in patients with chronicobstructive pulmonary disease and hypercapnia. Respiration 2008, inpress
3. Palmer B: Approach to fluid and electrolyte disorders and acid-baseproblems. Prim Care 35: 195–213, 2008
102 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

4. Laski M, Sabatini S: Metabolic alkalosis, bedside and bench. SeminNephrol 26: 404–421, 2006
5. Nagai Y, Itabashi M, Mizutani M, Ogawa T, Yumura W, Tsuchiya K,Nitta K: A case report of uncompensated alkalosis induced by dailyplasmapheresis in a patient with thrombotic thrombocytopenic pur-pura. Ther Apher Dial 12: 86–90, 2007
6. Ajbani K, Chansky M, Baumann B: Homespun remedy, homespuntoxicity: Baking soda ingestion for dyspepsia. J Emerg Med Decem-ber 26, 2007 [epub ahead of print]
7. Gawarammana L, Coburn J, Greene S, Dargan P, Jones A: Severehypokalaemic metabolic alkalosis following ingestion of gaviscon.Clin Toxicol 45: 176–178, 2007
8. Gabriely I, Leu J, Barzel U: Back to basics. N Engl J Med 358:1952–1956, 2008
9. Schimert P, Bernet-Buettiker V, Rutishauser C, Schams M, Frey B:Transplacental metabolic alkalosis. J Paediatr Child Health 43:851–853, 2007
10. McCauley M, Gunawardane M, Cowan M: Severe metabolic alkalo-sis due to pyloric obstruction: Case presentation, evaluation, andmanagement. Am J Med Sci 332: 346–350, 2006
11. Renaud C: Conventional bicarbonate haemodialysis in postgastrocys-toplasty metabolic alkalosis. Singapore Med J 49: e121, 2008
12. Castellan M, Gosalbex R, Perez-Brayfield M, Healey P, McDonaldR, Labbie A, Lendvay T: Tumor in bladder reservoir after gastrocys-toplasty. J Urol 178: 1771–1774, 2007
13. Dorwart M, Shcheynikov N, Yang D, Muallem S: The solute carrier26 family of proteins in epithelial ion transport. Physiology (Be-thesda) 23: 104–114, 2008
14. Dorwart M, Shcheynikov N, Baker J, Forman-Kay J, Muallem S,Thomas P: Congenital chloride-losing diarrhea causing mutation inthe STAS domain result in misfolding and mistrafficking ofSLC26A3. J Biol Chem 283: 8711–8722, 2008
15. Pela I, Bigozzi M, Bianchi B: Profound hypokalemia and hypochlo-remic metabolic alkalosis during thiazide therapy in a child withPendred syndrome. Clin Nephrol 69: 450–453, 2008
16. Augusto J, Sayegh J, Malinge M, Illouz F, Subra J, Ducluzeau P:Severe episodes of extra cellular dehydration: An atypical adultpresentation of cystic fibrosis. Clin Nephrol 69: 302–305, 2008
17. Yalcin S, Akca T, Genc O, Celik M, Dogru D, Ozcelik U: Modifiedoral rehydration therapy in a case with cystic fibrosis. Turk J Pediatr49: 102–104, 2007
18. Ballestero Y, Hernandez M, Rojo P, Manzanares J, Nebreda V,Carbajosa H, Infante E, Baro M: Hyponatremic dehydration as apresentation of cystic fibrosis. Pediatr Emerg Care 22: 725–727,2006
19. Al-Awqati Q: Control of terminal differentiation in epithelia. J AmSoc Nephrol 19: 443–449, 2008
20. Adler L, Efrati E, Zelikovic I: Molecular mechanisms of epithelialcell-specific expression and regulation of the human anion exchanger(pendrin) gene. Am J Physiol Cell Physiol 294: C1261–C1276, 2008
21. Adachi M, Asakura Y, Sato Y, Tajima T, Nakajima T, Yamamoto T,Fujieda K: Novel SLC12A1 (NKCC2) mutations in two families withBartter syndrome type 1. Endocr J 54: 1003–1007, 2007
22. Kramer B, Bergler T, Stoelcker B, Waldegger S: Mechanisms ofdisease: The kidney-specific chloride channels C1CKA and C1CKB,the barttin subunit, and their clinical relevance. Nat Clin PractNephrol 4: 38–46, 2008
23. Nozu K, Inagaki T, Fu X, Nozu Y, Kaito H, Kanda K, Sekine T,Igarashi T, Nakanishi K, Yoshikawa N, Iijima K, Matuso M: Molec-ular analysis of digenic inheritance in Bartter syndrome with senso-rineural deafness. J Med Genet 48: 182–186, 2008
24. Aoi N, Nakayama A, Tahira Y, Haketa A, Yabuki M, Sekiyama Y,Nakane C, Mano H, Kawachi H, Sato N, Soma M, Matsumoto K:Two novel genotypes of the thiazide-sensitive Na-Cl cotransporter(SLC12A3) gene in patients with Gitelman’s syndrome. Endocrine31: 149–153, 2007
25. Aoki K, Tajima T, Yabushita Y, Nakamura A, Nezu U, Takahashi M,Kimura M, Terauchi Y: A novel initial codon mutation of thethiazide-sensitive Na-Cl cotransporter gene in a Japanese patient withGitelman’s syndrome. Endocr J 55: 557–560, 2008
26. Jang H, Lee J, Oh Y, Na K, Joo K, Jeon U, Cheong H, Kim J, HanJ: From bench to bedside: Diagnosis of Gitelman’s syndrome—Defect of sodium-chloride cotransporter in renal tissue. Kidney Int70: 813–817, 2006
27. Joo K, Lee J, Jang H, Heo N, Jeon U, Oh Y, Lim C, Na K, Kim J,Cheong H, Han J: Reduced urinary excretion of thiazide-sensitiveNa-Cl cotransporter in Gitelman syndrome: Preliminary data. Am JKidney Dis 50: 765–773, 2007
28. Pachulski R, Lopez F, Sharaf R: Gitelman’s not-so-benign syndrome.N Engl J Med 353: 850–851, 2005
29. Akinci B, Celik A, Saygili F, Yesil S: A case of Gitelman’s syndromepresenting with extreme hypokalaemia and paralysis. Exp Clin En-docrinol Diabetes June 3, 2008 [epub ahead of print]
30. Cheng C, Shiang J, Hsu Y, Yang S, Lin S: Hypocalciuria in patientswith Gitelman syndrome: Role of blood volume. Am J Kidney Dis 49:693–700, 2007
31. Colussi G, Bettinelli A, Tedeschi S, De Ferrari M, Syren M, Borsa N,Mattiello C, Casari G, Bianchetti M: A thiazide test for the diagnosisof renal tubular hypokalemic disorders. Clin J Am Soc Nephrol 2:454–460, 2007
32. Weizhen J, Foo J, O’Roak B, Zhao H, Larson M, Simon D, Newton-Cheh C, State M, Levy D, Lifton R: Rare independent mutations inrenal salt handling genes contribute to blood pressure variation. NatGenet 40: 592–599, 2008
33. Ariceta G, Rodriguez-Soriano J: Inherited renal tubulopathies asso-ciated with metabolic alkalosis: Effects on blood pressure. SeminNephrol 26: 422–433, 2006
34. Flatman P: Cotransporters, WNKs, and hypertension: An update.Curr Opin Nephrol Hypertens 17: 186–192, 2008
35. Sandberg M, Riquier A, Pihakaski-Maunsbach K, McDonough A,Maunsbach A: ANG II provokes acute trafficking of distal tubuleNa�-C1� co transporter to apical membrane. Am J Physiol RenalPhysiol 293: F662–F669, 2007
36. Moffett B, Moffett T, Dickerson H: Acetazolamide therapy forhypochloremic metabolic alkalosis in pediatric patients with heartdisease. Am J Ther 14: 331–335, 2007
37. Caramelo C, Albalate M, Tejedor A, Alcazar R, Baldovi S, Perez A,Marin M: Actuality of the use of acetazolamide as a diuretic:Usefulness in refractory edema and in aldosterone-antagonist-relatedhyperkalemia. Nefrologia 28: 234–238, 2008
38. Leaf D, Goldfarb D: Mechanisms of action of acetazolamide in theprophylaxis and treatment of acute mountain sickness. J Appl Physiol102: 1313–1322, 2007
39. Richalet J, Rivera M, Maignan M, Privat C, Pham I, Macarlupu J,Petitjean O, Leon-Velarde F: Acetazolamide for Monge’s disease:Efficiency and tolerance of a 6 month treatment. Am J Respir CritCare Med 177: 1370–1376, 2008
Metabolic AcidosisNew Physiologic Insights
The kidney’s role in regulating acid-base balanceincludes two components: (1) Reclamation of filteredHCO3
� and (2) regeneration of HCO3� consumed by
net acid production. In the proximal tubule, approxi-mately two thirds of the filtered HCO3
� is reabsorbedvia the apical membrane Na�-H� antiporter NHE-3.A vacuolar apical membrane, H�-ATPase, mediatesthe remaining one third of HCO3
� absorption. Both of
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 103

these H� transporters generate bicarbonate in the cell,which must exit across the basolateral membrane toaffect transepithelial transport. The Na�-3HCO3
� co-transporter NBCe1-A, encoded by the gene SLC4A4,mediates the majority of proximal tubule basolateralbicarbonate exit.
The NBCe1-A protein shows evidence of post-translational regulation in response to metabolic acid-base disorders. Under conditions of acute metabolicacidosis, the mRNA and protein level of the co-transporter is unchanged, but the co-transporter isrecruited into the basolateral membrane (1). By con-trast, under conditions of metabolic alkalosis, wherebyHCO3
� absorption should be inhibited, there is cyto-plasmic redistribution. This type of regulation is incontrast to respiratory acid-base disturbances. Undercondition of hypercapnia, there is an actual increase inprotein abundance as opposed to the same amount ofprotein being simply redistributed (2).
The distal nephron is responsible for reabsorbingthe small quantity of filtered HCO3
� that escapes theproximal tubule and thick ascending limb. In addition,the distal nephron secretes a quantity of H� equal tothat generated systemically by metabolism to maintainacid-base balance. Depending on chronic acid-basestatus, the cortical collecting duct is capable of eitherH� or HCO3
� secretion. These functions are mediatedby one of two types of intercalated cells: The acid-secreting � intercalated cell and the base-secreting �intercalated cell.
H� secretion by the � intercalated cell is medi-ated by one of two transporters: A vacuolar H�-ATPase and an H�-K�-ATPase. The activity of theH�-K�-ATPase increases in K� depletion and thusprovides a mechanism by which K� depletion en-hances both collecting duct H� secretion and K�
absorption (3). Intracellular base generated by thesetransporters exits the basolateral membrane by way ofa Cl�/HCO3
� exchanger. The Cl� that enters the cellin exchange for HCO3
� exits the cell through a baso-lateral membrane Cl� conductance channel.
The HCO3�-secreting � intercalated cell is in
many respects a mirror image of the � intercalatedcell. It possesses an H�-ATPase on the basolateralmembrane, which mediates active H� extrusion. Al-kali that is generated within the cell then exits on anapical membrane Cl�-HCO3
�. As mentioned in theMetabolic Alkalosis section, this exchanger is thependrin protein and is distinct from the basolateral
Cl�-HCO3� exchanger present in the � intercalated
cell. In a model of chronic hypercapnia, expression ofpendrin was found to be significantly decreased (2).This is the same model mentioned previously in whichhypercapnia led to redistribution of the Na�-3HCO3
�
co-transporter to the basolateral membrane in theproximal tubule. These findings suggest that the renaladaptation to chronic hypercapnia is due not only toenhanced proximal HCO3
� absorption but also todeceased distal HCO3
� secretion.For the distal nephron to secrete an adequate
amount of H�, buffer must be available to preventextreme luminal acidity. Quantitatively, the most im-portant urinary buffer is the NH3/NH4
� system. Un-like other buffers, the rate of NH3 production andexcretion can be varied according to physiologicneeds. Under normal circumstances, excretion ofNH4
� accounts for more than half of the net acidexcreted per day.
The proximal tubule is responsible for both am-monia production and luminal secretion. Ammonia issynthesized in the proximal tubule predominantlyfrom glutamine metabolism through enzymatic pro-cesses in which phosphoenolpyruvate carboxykinaseand phosphate-dependent glutaminase are the rate-limiting steps. This results in production of 2 NH4
�
and 2 HCO3� ions from each glutamine ion. Ammonia
is then preferentially secreted into the lumen.Most of the ammonia that leaves the proximal
tubule does not return to the distal tubule. Rather, thethick ascending limb of Henle reabsorbs the majorityof luminal ammonia into the renal interstitium, whereit becomes available for secretion into the collectingduct in response to H� secretion. Although tradition-ally thought that NH3/NH4
� then enters the collectingduct by nonionic diffusion driven by the acid luminalpH, increasing evidence suggests that the nonerythroidglycoproteins RhBg and RhCg may be involved inammonia secretion (4). The polarized location in ma-jor sites of ammonia transport along with the increasein RhCg expression in response to acidosis suggeststhat these proteins may play an important role in thevectorial transport of ammonia. In addition, redistri-bution of these proteins into the cell membrane maycontribute to the adaptive increase in single-nephronammonia transport under reduced renal mass condi-tions (5).
In addition to an increased ability to transportammonia, metabolic acidosis leads to increased am-
104 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

monia production in the proximal tubule. Metabolicacidosis increases the mobilization of glutamine formskeletal muscle and intestinal cells. Glutamine is pref-erentially taken up by the proximal tubular cell via theNa�- and H�-dependent glutamine transporterSNAT3. This transporter is a member of the SCL38gene family of Na�-coupled neutral amino acid trans-porters. SNAT3 expression increases severalfold inmetabolic acidosis, and it is preferentially expressedon the cell’s basolateral surface, where it is poised forglutamine uptake (6). The increase in plasma glu-cocorticoids that typically accompanies metabolic ac-idosis plays a role in this transporter’s upregulation(7). Metabolic acidosis also causes increased expres-sion and activity of phosphate-activated glutaminaseand glutamate dehydrogenase. Proteomic analysis ofrat proximal tubules taken from acidotic rats is con-sistent with upregulation of these enzymes (8).
The primary mechanism for secretion of NH4�
into the lumen is transport on the apical Na�-H�
antiporter NHE-3. This transport process is influencedby angiotensin II (9). Metabolic acidosis is known tostimulate the systemic renin-angiotensin system. An-giotensin II either generated systemically or producedlocally increases the protein expression of luminalNHE3 and as a result causes increased secretion ofNH4
� into the tubular lumen. Although this theory isnot proved, patients who take inhibitors of the renin-angiotensin system might be prone to more overtacid-base problems when faced with an acid loadresulting from an inability to augment ammonia secre-tion through this transporter.
Obstructive uropathy is typically associated withmetabolic acidosis development and a defect in uri-nary acidification that frequently persists even afterreestablishment of free urinary flow. Alterations in theexpression of several proteins involved in acid-basehomeostasis may explain these disturbances. In a ratmodel of bilateral urinary obstruction protein, expres-sion of NHE3 and the Na�-3HCO3
� co-transporter inthe proximal nephron and pendrin in the distal nephronwere significantly decreased (10). The H�-ATPaseexpression in the inner medullary collecting duct ini-tially is increased but later falls after obstruction re-lease. The other transporters also remain reduced afterobstruction release. The persistent decrease in expres-sion of NHE3, the Na�-3HCO3
� co-transporter, andH�-ATPase after release of urinary obstruction willimpair both HCO3
� reclamation and regeneration. The
pendrin expression decrease may be a compensatoryresponse to limit HCO3
� secretion in metabolic aci-dosis.
References1. Brandes A, Oehlke O, Schumann A, Heidrich S, Thevenod F, Roussa
E: Adaptive redistribution of NBCe1-A and NBCe1-B in rat kidneyproximal tubule and striated ducts of salivary glands during acid-basedisturbances. Am J Physiol Regul Integr Comp Physiol 293: R2400–R2411, 2007
2. de Seigneux S, Malte H, Dinke H, Frekiaer J, Nielsen S, Frishce S:Renal compensation to chronic hypoxic hypercapnia: Downregula-tion of pendrin and adaptation of the proximal tubule. Am J PhysiolRenal Physiol 292: F1256–F1266, 2006
3. Codina J, DuBose T: Molecular regulation and physiology of theH�,K�-ATPases in kidney. Semin Nephrol 26: 345–351, 2006
4. Planelles G: Ammonium homeostasis and human Rhesus glycopro-teins. Nephron Physiol 105: 11–17, 2007
5. Kim H, Baylis C, Verlander J, Han K, Reungjui S, Harellgton M,Weiner I: Effect of reduced renal mass on renal ammonia transporterfamily, Rh C glycoprotein and Rh B glycoprotein, expression. Am JPhysiol Renal Physiol 293: F1238–F1247, 2007
6. Moret C, Dave M, Schulz N, Jiang J, Verrey F, Wagner C: Regula-tion of renal amino acid transporters during metabolic acidosis. Am JPhysiol Renal Physiol 292: F555–F566, 2007
7. Karinch A, Lin C, Meng Q, Pan M, Souba W: Glucocorticoids havea role in renal cortical expression of the SNAT3 glutamine transporterduring chronic metabolic acidosis. Am J Physiol Renal Physiol 292:F448–F455, 2007
8. Curthoys N, Taylor L, Hoffert J, Knepper M: Proteomic analysis ofthe adaptive response of rat renal proximal tubules to metabolicacidosis. Am J Physiol Renal Physiol 292: F140–F147, 2007
9. Nagami G: Role of angiotensin II in the enhancement of ammoniaproduction and secretion by the proximal tubule in metabolic acido-sis. Am J Physiol Renal Physiol 294: F874–F880, 2008
10. Wang G, Li C, Kim S, Ring T, Wen J, Djurhuss J, Wang W, NielsenS, Frokaer J: Ureter obstruction alters expression of renal acid-basetransport proteins in rat kidney. Am J Physiol Renal Physiol 295:F497–F506, 2008
Clinical Approach to Metabolic AcidosisMetabolic acidosis is diagnosed by a low pH, a
reduced HCO3� concentration, and respiratory com-
pensation resulting in a decrease in the PCO2. A lowHCO3
� concentration alone is not diagnostic of met-abolic acidosis because it also results from the renalcompensation to chronic respiratory alkalosis. Mea-surement of the arterial pH differentiates betweenthese two possibilities. The pH is low in hyperchlor-emic metabolic acidosis and high in chronic respira-tory alkalosis. A two-part overview of metabolic aci-dosis with an emphasis on the critically ill patientrecently was published (1,2).
After confirming the presence of metabolicacidosis, calculation of the serum anion gap is auseful step in determining the differential diagnosisof the disorder. The anion gap is equal to thedifference between the plasma concentrations of the
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 105

major cation (Na�) and the major measured anions(Cl� � HCO3
�).Although calculation of the anion gap is a valu-
able clinical tool, a recent review highlighted some ofthe tool’s limitations (3). As a result of changes in howserum Na� and Cl� are measured, the normal valuefor the anion gap has tended to fall over time. Inhealthy individuals, the anion gap has typically beenreported to range from 11 to 15 mEq/L. These valueswere based on the use of flame photometry for Na�
measurement and a colorimetric assay for Cl�. Aslaboratories moved to using ion selective electrodes,the serum Na� values have largely remained the same,whereas the serum Cl� values have tended to behigher. As a result, the normal value for the anion gaphas decreased to as low as 6 mEq/L in some reports.Recognizing this change, some laboratories have ac-tually adjusted the calibration set point for Cl� so as toreturn the normal value for the anion gap back to the11- to 15-mEq/L range. It is important for the clinicianto be aware that the average anion gap and range ofnormal values will vary among health care facilities.
In patients with high anion gap acidosis (e.g.,�30 mEq/L), the contributing anion’s identity is usu-ally identifiable. The most common anions found inthis setting are lactate and ketoacid anions resultingfrom lactic acidosis and ketoacidosis, respectively.With less pronounced elevations in the gap, the un-measured anion’s identity often is not apparent. Krebcycle intermediates, amino acids, and uric acid mayaccount for some of the gap in this setting (4). Inaddition, the anion gap—even when adjusted for theserum albumin concentration—may be only minimallyoutside the normal range among patients with docu-mented organic acidosis, suggesting that the test is aninsensitive screen for mild to moderate disturbances(5). The review by Kraut and Madias (3) acknowl-edged that the anion gap will remain an inexpensiveand effective means to detect various disorders butemphasized the need to interpret the results in thecontext of the history, physical examination, and otherclinical information.
Lactic AcidosisOne of the most common causes of anion gap
metabolic acidosis is lactic acidosis. Under normalcircumstances, virtually all tissues in the body metab-olize glucose via the glycolytic pathway and generatelactate, with the greater part of lactate production
occurring in brain, erythrocytes, and skeletal muscle.In turn, lactate is extracted predominately by the liverand renal cortex and either is reconverted to glucose orbecomes fuel for oxidation for CO2 and H2O. Thisdynamic relationship between lactate and glucose istermed the Cori cycle. The importance of this cyclicalrelationship can best be appreciated when one con-siders that the normal daily production of lactate hasbeen estimated to be 15 to 30 mmol/kg (equivalentto 15 to 30 mmol/kg H� per d). Because daily netacid excretion by the kidney is only 1 mmol/kg, thequantitative importance of this pathway in disposingof the H� that is produced during glycolysis be-comes obvious. Furthermore, it is apparent that onlya mild disruption in the equilibrium between lactateproduction and consumption in the Cori cycle canlead to the rapid development of devastating meta-bolic acidosis.
Type A lactic acidosis is characterized by disor-ders in which there is underperfusion of tissue or acutehypoxia. Such disorders include patients with cardio-pulmonary failure, severe anemia, hemorrhage, hypo-tension, sepsis, and CO poisoning. In blood samplestaken from collapsed Boston Marathon runners, lactatelevels were increased in virtually all individuals (6). Inalmost half of the cases, the lactate level was abovewhat would be considered a critical value (�31.5mg/dl, 3.5 mmol/L).
Adult patients with salicylate poisoning charac-teristically present with evidence of an anion gapmetabolic acidosis and respiratory alkalosis (7). Thissame acid-base disturbance may also be a distinctivefeature of thiamine deficiency presenting as Wer-nicke’s encephalopathy (8). Significant increases inlactate levels ranging from 5.5 to 7.9 mmol/L werefound in three of four such patients with this acid-basepattern.
Type B lactic acidosis occurs in patients with avariety of disorders that share the development oflactic acidosis in the absence of overt hypoperfusion orhypoxia. These conditions include congenital defectsin glucose or lactate metabolism, diabetes, liver dis-ease, effects of drugs and toxins, and neoplastic dis-eases.
Lactic acidosis is a feature of genetic mitochon-drial disease. Chronic oral dichloroacetate therapy iseffective in such patients. This drug stimulates theactivity of the pyruvate dehydrogenase complex,thereby facilitating aerobic glucose and lactate oxida-
106 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

tion. In an observational study of 36 individuals withdisorders such as congenital lactic acidosis resultingfrom pyruvate dehyrogenase deficiency, defects invarious respiratory chain complexes, or MELAS (mi-tochondrial encephalopathy, lactic acidosis, andstroke-like episodes), both the basal and carbohydrate-induced increases in lactate were blunted with thisdrug (9). Long-term therapy lowered cerebrospinalfluid lactate levels and improved various measures ofperipheral nerve function.
Mitochondrial dysfunction leading to lactic aci-dosis can also be an acquired disorder. Highly activeantiretroviral therapy to include didanosine and stavu-dine can cause fatal lactic acidosis. These drugs causesevere biochemical and ultrastructural damage to mi-tochondria in multiple tissues to include the liver,kidney, and skeletal and cardiac muscles (10). Prelim-inary evidence suggests that exogenous supplementa-tion with uridine may be an effective treatment for thiscomplication (11).
Mangosteen (Garcinia mangostana) is a tropicalfruit from Southeast Asia that is available for USimportation. The fruit contains �-mangostin, which isa known potent inhibitor of mitochondrial function.Daily ingestion of mangosteen juice was recentlyimplicated in the development of severe lactic aci-dosis in a 58-yr-old man who used the juice to loseweight (12).
Metformin therapy is a widely known cause oflactic acidosis, particularly when administered topatients with decreased renal function. In patientswho have diabetes, are treated with renin-angioten-sin system blockers, and develop volume depletionor are given a nonsteroidal anti-inflammatory drugor both can quickly develop acute kidney injury,precipitating severe lactic acidosis in the setting ofmetformin therapy (13,14). Intentional metforminoverdose can also cause lactic acidosis (15,16).Continuous renal replacement therapy is useful inthis setting because it removes both lactate andmetformin and corrects the acidosis without the riskfor volume overload.
Propofol used for sedation can lead to lacticacidosis particularly in high dosages and for prolongedperiods (17). Similarly, sedation with high-dosagelorazepam infusions can lead to propylene glycol tox-icity. Accumulation and metabolism of this diluentcauses lactic acidosis, increased osmolar gap, andacute kidney injury (18).
Clenbuteral is a long-acting � adrenergic agonistthat frequently is used in veterinary medicine to treatbronchoconstriction in animals. The drug also hasanabolic properties, and body builders have used itillicitly to increase muscle mass. An outbreak of lacticacidosis has recently been reported with use of heroinadulterated with clenbuterol (19). The development ofmetabolic acidosis is likely similar to that reported inpatients who had asthma and were treated with eitherinhaled or parenteral � adrenergic agonists (20,21).
Given the popularity of coffee and other caffein-ated beverages, it should be mentioned that caffeinetoxicity has been reported to cause increases in plasmalactate levels (22). Toxic levels of caffeine causeexcessive sympathetic stimulation, leading to in-creased glycogenolysis and lipolysis and causing ac-cumulation of pyruvate. To the extent that pyruvatefails to be aerobically metabolized, it will be convertedto lactate. �-Adrenergic blockade is a useful therapy inpatients with caffeine overdose.
Type B lactic acidosis can also be a complicationof certain tumors. A recent review and case reportdiscussed the association of lactic acidosis with hema-tologic malignancies (23,24).
Diabetic KetoacidosisDiabetic ketoacidosis is a metabolic condition
characterized by the accumulation of acetoacetic acidand �-hydroxybutyric acid. Its development is theresult of insulin deficiency and a relative or absoluteincrease in glucagon concentration. These hormonalchanges lead to increased fatty acid mobilization fromadipose tissue and, at the same time, alter the oxidativemachinery of the liver such that delivered fatty acidsare primarily metabolized into keto acids. In addition,peripheral glucose utilization is impaired and the glu-coneogenic pathway in the liver is maximally stimu-lated. The resultant hyperglycemia results in an os-motic diuresis and volume depletion.
Ketoacidosis results when the rate of hepaticketo acid generation exceeds peripheral utilization andthe blood keto acid concentration increases. The H�
accumulation in the extracellular fluid combines withand reduces HCO3
� concentration, whereas the ketoacid anion concentration increases. The reduction inserum HCO3
� concentration approximates the in-crease in anion gap initially. The degree to which theanion gap is elevated will depend on the rapidity,
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 107

severity, and duration of the ketoacidosis as well as thestatus of the extracellular fluid volume (25).
Although an anion gap acidosis is the dominantdisturbance in diabetic ketoacidosis, a hyperchloremicnormal gap acidosis is often present, depending on thestage of the disease process. In the earliest stages ofketoacidosis, when extracellular volume is near nor-mal, keto acid anions that are produced are rapidlyexcreted by the kidney as Na� and K� salts. Excretionof these salts is equivalent to the loss of potentialHCO3
�. This loss of potential HCO3� in the urine at
the same time as the kidney is retaining dietary NaClresults in a hyperchloremic normal gap acidosis. Asthe ketogenic process becomes more accelerated andvolume depletion becomes more severe, a larger pro-portion of the generated keto acid anions are retainedwithin the body, thereby increasing the anion gap.During treatment, the anion gap metabolic acidosistransforms once again into a hyperchloremic normalgap acidosis. Treatment leads to a termination in ketoacid production. As the extracellular fluid volume isrestored, there is increased renal excretion of the Na�
salts of the keto acid anions. The loss of this potentialHCO3
� combined with the retention of administeredNaCl accounts for the emergence of a hyperchloremicnormal gap acidosis. In addition, K� and Na� admin-istered in solutions that contain NaCl and KCl enterinto cells in exchange for H�. The net effect isinfusion of HCl into the extracellular fluid. The rever-sal of the hyperchloremic acidosis is accomplishedover several days as the HCO3
� deficit is corrected bythe kidney.
Confirmation of the presence of keto acids canbe achieved with use of nitroprusside tablets or reagentstrips; however, this test can be misleading in assess-ing the severity of ketoacidosis because it detects onlythe presence of acetone and acetoacetate and does notpermit reaction with �-hydroxybutyrate. Acetoaceticacid and �-hydroxybutyric acid are interconvertible,with the NADH:NAD� ratio being the primary deter-minant as to which moiety predominates. In a highratio, formation of �-hydroxybutyric acid is favored,and the nitroprusside test will become less positive oreven negative despite significant ketoacidosis. Thissituation can occur when ketoacidosis is accompaniedby lactic acidosis or in alcoholic ketoacidosis. Duringtreatment, the NADH:NAD� ratio tends to decline,favoring the formation of acetoacetic acid. As a result,it is common for the nitroprusside test to register more
strongly positive during the treatment of diabetic ke-toacidosis.
Readily available assays are now available forthe detection of �-hydroxybutyrate. In the presence ofuncontrolled diabetes, serum �-hydroxybutyrate levels�3.0 and �3.8 mmol/L in children and adults, respec-tively, can be used to diagnose diabetic ketoacidosis(26). When compared with urinary ketone measure-ments, capillary blood levels of �-hydroxybutyratemore strongly correlate with the degree of systemicacidosis and offer a more precise way to monitorpatients’ response to therapy (27).
Diabetic ketoacidosis treatment involves the useof insulin and intravenous fluids to correct volumedepletion. Deficiencies in K�, Mg2�, and phosphateare common; therefore, these electrolytes are typicallyadded to intravenous solutions, although there is notclear evidence of a benefit of routine administration ofphosphate. Alkali therapy is generally not requiredbecause insulin administration leads to the metabolicconversion of keto acid anions into HCO3
� and allowspartial correction of the acidosis. HCO3
� therapy maybe indicated in patients who present with severe aci-demia (pH �7.0). The pros and cons of bicarbonatetherapy among patients with severe acidosis is thesubject of a recent discussion (28).
Tris-hydroxymethyl aminomethane (THAM) is aweak base that is used in the treatment of metabolicand respiratory acidosis. THAM binds H� and regen-erates HCO3
� without releasing CO2. The drug alsoeasily penetrates cells and provides an intracellularbuffering effect (29). The drug’s protonated form iseliminated in the urine. THAM was given to a hemo-dynamically unstable 13-yr-old girl who presentedwith diabetic ketoacidosis and a pH of 6.8 (30).THAM along with conventional therapy produced arapid improvement in the patient’s metabolic profileand hemodynamic condition. There is limited experi-ence with the use of THAM in treatment of metabolicacidoses.
One also must be open to the possibility of morethan one process in patients who have diabetes andpresent with severe academia (31,32). A 19-yr-oldpatient with diabetes presented with ketoacidosis and apH of 6.7 but had only moderately elevated �-hy-droxybutyrate levels (31). A drug screen disclosed thepresence of ketamine. This drug is consumed inten-tionally or via spiked drinks and gives rise to dosage-dependent effects ranging from relaxation (referred to
108 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

by users as “K-land”) to near-death experiences (“K-hole”). Drug ingestion can lead to metabolic acidosis,rhabdomyolysis, and seizures.
Starvation KetosisAbstinence from food can lead to a mild anion gap
metabolic acidosis secondary to increased production ofketo acids. The pathogenesis of this disorder is similar tothat of diabetic ketoacidosis in that starvation leads torelative insulin deficiency and glucagon excess. As aresult, there is increased mobilization of fatty acids whilethe liver is set to oxidize fatty acids to keto acids. Theserum HCO3
� concentration rarely falls to values �18mmol/L. More fulminant ketoacidosis is aborted by thefact that ketone bodies stimulate the pancreatic islets torelease insulin, and lipolysis is held in check. This breakin the ketogenic process is notably absent in patients withinsulin-dependent diabetes. More severe reduction inserum HCO3
� should prompt a search for other condi-tions (32).
Alcoholic KetoacidosisKetoacidosis develops in patients with a history
of long-term ethanol abuse, decreased food intake, andoften a history of nausea and vomiting. The clinicianmust consider this condition in young people becausealcohol use is on the rise in the adolescent population(33). Alcoholic ketoacidosis is a serious condition thathas been associated with sudden cardiac death (34).
As with starvation ketosis, a decrease in theinsulin to glucagon ratio leads to accelerated fatty acidmobilization and alters the enzymatic machinery of theliver to favor keto acid production; however, severalfeatures differentiate this disorder from simple starva-tion ketosis. First, the presence of alcohol withdrawalcombined with volume depletion and starvation mark-edly increases the circulating catecholamine levels(35). As a result, the peripheral mobilization of fattyacids is much greater than that typically found withstarvation alone. This sometimes massive mobilizationof fatty acids can lead to marked keto acid productionand severe metabolic acidosis. Second, alcohol metab-olism leads to NADH accumulation. The increase inthe NADH:NAD� ratio is reflected by a higher �-hy-droxybutyrate to acetoacetate ratio. As mentioned, thenitroprusside reaction may be diminished by this redoxshift despite the presence of severe ketoacidosis.Treatment of this disorder is centered on administeringglucose. Glucose administration leads to the rapidresolution of the acidosis, because insulin release stim-
ulation leads to diminished fatty acid mobilizationfrom adipose tissue as well as decreased hepatic outputof keto acids.
Ethylene Glycol and Methanol PoisoningEthylene glycol metabolism by alcohol dehydro-
genase generates various acids, including glycolic,oxalic, and formic acids. Ethylene glycol is a compo-nent of antifreeze and solvents and is ingested byaccident or as a suicide attempt. The initial effects ofintoxication are neurologic and begin with acute ine-briation similar to that of alcohol but can quicklyprogress to seizures and coma. When left untreated,cardiopulmonary symptoms such as tachypnea, non-cardiogenic pulmonary edema, and cardiovascular col-lapse may appear. Twenty-four to 48 h after ingestion,patients may develop flank pain and renal failure oftenaccompanied by abundant calcium oxalate crystals inthe urine. Renal biopsy shows tubular necrosis andwidespread deposition of calcium oxalate crystalswithin the tubular epithelial cells (36).
Methanol also is metabolized by alcohol dehydro-genase and forms formaldehyde, which is then convertedto formic acid. Methanol is found in a variety of com-mercial preparations such as shellac, varnish, and de-icing solutions. As with ethylene glycol ingestion, meth-anol is ingested by accident or as a suicide attempt.Clinically, methanol ingestion is associated with an acuteinebriation followed by an asymptomatic period lasting24 to 36 h. Thereafter, pancreatitis, seizures, blindness,and coma may develop. The blindness is due to directretinal toxicity of formic acid. Methanol intoxication canlead to the delayed onset of a Parkinson-like syndromebecause it may induce hemorrhage in the white matterand putamen. Lactic acidosis also is a feature of metha-nol and ethylene glycol poisoning and contributes to theelevated anion gap.
Together with the appearance of the anion gap,an osmolar gap becomes manifest and is an importantclue to ethylene glycol diagnosis and methanol poi-soning. In addition to supportive measures, the treat-ment of ethylene glycol and methanol poisoning iscentered on reducing the metabolism of the parentcompound and accelerating its removal from the body.Decreasing metabolism of the parent compound isimportant because the metabolites rather than the par-ent compound are primarily responsible for the toxiceffects. Fomepizole (4-methylpyrazole) is now theagent of choice to inhibit the enzyme alcohol dehy-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 109

drogenase and prevent formation of toxic metabolites.If fomepizole is unavailable, then intravenous ethanolcan be used to prevent the formation of toxic metab-olites. Ethanol has �10-fold greater affinity for alco-hol dehydrogenase than other alcohols. With fo-mepizole and ethanol therapy, hemodialysis therapyshould be used to remove both the parent compoundand metabolites. The reader is referred to a recentin-depth review of the diagnosis and management oftoxic alcohol ingestions (37).
Pyroglutamic AcidosisThe diagnosis of pyroglutamic acidosis should
be considered in patients with unexplained anion gapmetabolic acidosis and recent acetaminophen inges-tion (38,39). In this setting, glutathione levels arereduced because of the oxidative stress associated withcritical illness. In addition, acetaminophen metabolismdepletes glutathione. The reduction in glutathione sec-ondarily leads to increased production to pyroglutamicacid. High pyroglutamic acid concentrations are foundin the blood and urine, and plasma concentrationsparallel the increase in the anion gap.
Normal (Hyperchloremic) Anion Gap AcidosisA hyperchloremic normal anion gap metabolic
acidosis can be of renal or extrarenal origin. Metabolicacidosis of renal origin is the result of abnormalities intubular H� transport. Metabolic acidosis of extrarenalorigin is most commonly caused by gastrointestinallosses of HCO3
�. Other causes include the externalloss of biliary and pancreatic secretions and ureteraldiversion procedures.
Extrarenal Causes of Normal (Hyperchloremic)Anion Gap Acidosis
Surgical diversion of the ureter into an ilealpouch is a procedure often used to treat patients withneurologic bladder abnormalities and urologic tumors.The procedure may rarely be associated with thedevelopment of a hyperchloremic normal gap meta-bolic acidosis. Acidosis may occur in part because ofreabsorption of NH4
� and Cl� from the urinary fluidby the intestine, which then metabolizes the NH4
� inthe liver to NH3 and H�. Urinary Cl� may also bereabsorbed in exchange for HCO3
� through activationof the Cl�/ HCO3
� exchanger on the intestinal lumen.In some patients, a renal defect in acidification candevelop and exacerbate the acidosis. Such a defectmay result from tubular damage caused by pyelone-
phritis or high colonic pressures secondarily causingurinary obstruction.
The main factors that influence the developmentand severity of acidosis are the length of time the urineis in contact with the bowel and the total surface areaof bowel exposed to urine. Among patients with anureterosigmoid anastomosis, the acidosis tends to bemore common and more severe than in those with anileal conduit. One patient who presented with quadri-paresis and rhabdomyolysis was found to have a pH of7.05 and a serum K� concentration of 1.27 mmol/L(40). Patients who undergo this procedure and developan acidosis should be examined for the possibility ofan ileal loop obstruction, because this would lead to anincrease in contact time between the urine and theintestinal surface.
Renal Causes of Normal (Hyperchloremic)Anion Gap Acidosis
Under normal circumstances, approximately90% of the filtered load of HCO3
� is reabsorbed in theproximal tubule. Normally the serum HCO3
� concen-tration is maintained slightly below the threshold atwhich bicarbonaturia develops. In this manner, whenthe serum concentration of HCO3
� exceeds 26 to 28mmol/L, the excess HCO3
� is excreted in the urine.In proximal renal tubular acidosis (RTA), the
threshold for HCO3� reabsorption is lower and results
in a self-limited bicarbonaturia. This defect causes aportion of the filtered HCO3
� to escape reabsorptionin the proximal tubule and to be delivered into thedistal nephron. The distal nephron has a low capacityfor HCO3
� reabsorption, and HCO3� appears in the
urine. The net effect is that the serum concentrationand filtered load of HCO3
� begin to fall. Despitesystemic acidemia development, the urine pH is alka-line because of the presence of HCO3
� in the urine.Eventually a steady state is reached, at which point allof the filtered HCO3
� is reabsorbed. Now the deliveryof HCO3
� to the distal nephron may be abnormallyincreased, but it is of a magnitude that can be reab-sorbed in the distal nephron. The urine is acidified toa pH of �5.5, and net acid excretion is equal toendogenous acid production but at a lower serumHCO3
� concentration. In the steady state, the serumHCO3
� concentration in proximal RTA usually is inthe range of 16 to 18 mmol/L.
One of the characteristic findings in proximalRTA is the presence of hypokalemia. The develop-
110 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

ment of hypokalemia is the result of renal K� wastingcaused by the coupling of increased aldosterone levelsand increased distal Na� delivery. In the steady state,when virtually all of the filtered HCO3
� is reabsorbedin the proximal and distal nephron, renal K� wastingis minimal and the degree of hypokalemia tends to bemild. By contrast, treatment of metabolic acidosis withHCO3
� improves the acidosis but worsens the degreeof hypokalemia. An increase in the filtered concentra-tion of HCO3
� above the kidney’s reabsorptivethreshold will result in an increase in excretion ofNaHCO3 and KHCO3. An example of this effect wasrecently reported in a 39-yr-old man with proximalRTA because of myeloma kidney (41).
Basolateral NaHCO3 co-transporter (NBCe1/SLC4A4) gene mutations give rise to an inherited formof proximal RTA (42). This form of proximal RTA isaccompanied by ocular abnormalities such as cataracts,glaucoma, and band keratopathy. Only two families havebeen described with isolated pure proximal RTA. In onefamily, nine genes that are known to be involved inproximal acidification were studied, but a molecularbasis for the disease could not be identified (43).
Topiramate is a drug that initially was approved asan antiepileptic drug and increasingly is used to treat of anumber of neurologic and metabolic disorders. The drugexerts an inhibitory effect on renal carbonic anhydraseactivity, resulting in a proximal acidification defect sim-ilar to that observed with acetazolamide. Use of the drugalso is associated with hypocitraturia, hypercalciuria, andelevated urine pH, leading to an increased risk for kidneystone disease (44–46).
Proximal RTA may occur as an isolated defect inacidification alone but is more commonly associatedwith widespread proximal tubule dysfunction (Fanconisyndrome). In addition to decreased HCO3
� reabsorp-tion, patients with Fanconi syndrome have impairedreabsorption of glucose, phosphate, uric acid, aminoacids, and low molecular weight proteins. Severalinherited and acquired disorders have been associatedwith the development of Fanconi syndrome and prox-imal RTA. The most common inherited cause is cysti-nosis. Adults with Fanconi syndrome most commonlyhave a dysproteinemic condition such as multiplemyeloma. Fanconi syndrome has occurred in associa-tion with administration of imatinib mesylate in apatient with chronic myeloid leukemia and in a livertransplant patient who was treated with tacrolimus andlamivudine (47,48). Fanconi syndrome can be a clin-
ical manifestation of the syndrome of tubulointerstitialrenal disease and uveitis (TINU syndrome) (49,50).
Tenofovir is commonly used as a component inhighly active antiretroviral therapy. Its principal renaladverse effects are related to tubular toxicity, givingrise to manifestations such as RTA, Fanconi syn-drome, and nephrogenic diabetes insipidus (51). In astudy designed to investigate its renal toxicity, ratswere fed varying dosages of tenofovir during a sever-al-week period (52). The rats developed phosphaturia,proximal RTA, and a reduced concentrating ability.These renal manifestations were accompanied bydownregulation of the sodium-phosphorus co-trans-porter (NaPi-IIa), NHE3, and aquaporin 2. Becauseprevious studies had shown that normal rats that weregiven the peroxisome proliferator–activated receptor �agonist rosiglitazone led to increased expression ofthese same transporters, the investigators hypothesizedthat the nephrotoxicity of tenofovir could be preventedby this drug. Indeed, rosiglitazone reversed tenofovirnephrotoxicity and normalized the altered membranetransporter protein expression.
In contrast to patients with proximal RTA, thosewith distal RTA (dRTA) do not acidify their urinedespite severe metabolic acidosis. This disorder resultsfrom a reduction in net H� secretion in the distalnephron, which gives rise to an impairment in HCO3
�
regeneration. As a result, these patients are in a state ofpersistent positive acid balance that requires bonebuffers to prevent severe systemic acidemia. Thepathophysiologic basis for this defect could be eitherimpaired H� secretion (secretory defect) or an abnor-mally permeable distal tubule, resulting in increasedbackleak of normally secreted H� (gradient defect).The RTA that is seen in the setting of amphotericin Badministration is an example of impaired H� secretionresulting from a gradient defect.
For patients with a secretory defect, the inability toacidify the urine below pH 5.5 results from an abnormal-ity in one or both of the H� secretory mechanisms. Somepatients may have an isolated defect in the H�-K�-ATPase that impairs H� secretion and K� reabsorption.The second mechanism of H� secretion in the distalnephron is the vacuolar ATPase. This pump couples theenergy from hydrolysis of ATP to the active transport ofH� from the cytoplasm into the tubular lumen (reviewedin reference [53]). Mutations in ATP6V1B1 (B1 subunit)or ATP6V0A4 (a4 subunit) are responsible for the rareautosomal recessive from of dRTA in which sensorineu-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 111

ral deafness also is present (54). It has been proposed thatsubtle defects in these subunits could give rise to anormal blood pH and bicarbonate concentration but im-pair maximal acidification of the urine when challengedwith an acid load (55,56). Given the link between re-duced urinary acidification and calcium stone formation,such defects could play a role among calcium stoneformers in the general population.
A dRTA diagnosis should be considered for apatient with hyperchloremic normal gap acidosis, hypo-kalemia, and an inability to lower the urine pH maxi-mally. A urine pH �5.5 in the setting of systemicacidosis is consistent with a dRTA, as is a positiveurinary anion gap. In patients with only minimal distur-bances in blood pH and plasma HCO3
� concentration, atest of urinary acidification is required. Traditionally,such a test involved oral NH4Cl administration to inducemetabolic acidosis and then assess the renal response byserially measuring the urine pH. Many patients poorlytolerate NH4Cl ingestion because of gastric irritation,nausea, and vomiting. An alternative way to test thecapacity for distal acidification is to administer furo-semide and mineralocorticoid fludrocortisone simulta-neously. The combination of both increased distal Na�
delivery and mineralocorticoid effect will stimulate distalH� secretion by both increasing the luminal electronega-tivity and having a direct stimulatory on H� secretion.
In a study of 10 patients with known dRTA and11 control subjects, urinary acidification assessmentwas compared between NH4Cl loading and simulta-neous administration of furosemide and fludrocorti-sone (57). The control subjects could lower their urinepH to �5.3, whereas all of the patients with dRTAfailed to acidify their urine with either test; however,two aspects of the study favored the furosemide/fludrocortisones protocol. The test was better toleratedand the time to maximal reduction in urine pH wassignificantly shorter when compared NH4Cl loading.
The administration of furosemide and themineralocorticoid fludrocortisone is an ef-fective way to test the capacity for distalacidification. This approach is better toler-ated than NH4Cl ingestion.
The systemic acidosis in dRTA tends to be moresevere than in patients with a proximal RTA. The
serum HCO3� concentration can reach values as low
as 10 mmol/L. Hypokalemia can also be severe; it canlead to musculoskeletal weakness and symptoms ofnephrogenic diabetes insipidus in patients with dRTA.
Unlike patients with proximal RTA, patientswith dRTA frequently manifest nephrolithiasis andnephrocalcinosis. This predisposition to renal calcifi-cation results from a number of factors. Urinary Ca2�
excretion is high secondary to acidosis-induced bonemineral dissolution. This increase in urinary Ca2�
excretion is worsened by the low intraluminal concen-tration of HCO3
� in the distal nephron. Normally,HCO3
� acts to increase distal Ca2� absorption. Sys-temic acidemia lowers the luminal concentration ofHCO3
� in the distal nephron, with the result that Ca2�
absorption is decreased and urinary Ca2� excretion isfurther augmented (58). The increased Ca2� excretionis more likely to result in urine supersaturation in thepresence of an alkaline pH. The high urine pH de-creases the solubility of calcium phosphate complexes.Stone formation is further enhanced because of lowurinary citrate excretion. Citrate is metabolized toHCO3
�, and thus its reabsorption contributes to cor-rection of metabolic acidosis. Unfortunately, urinarycitrate serves as the major Ca2� chelator in the urine;therefore, its enhanced reabsorption in acidosis predis-poses to nephrolithiasis and nephrocalcinosis.
The results of intraoperative renal papillae biop-sies obtained during percutaneous nephrolithotomy infive stone-forming patients with dRTA were recentlyreported (59). The degree of papillary renal diseasewas more diffuse compared with patients with otherforms of renal stone disease. In particular, there wasplugging of inner medullary collecting ducts andBellini ducts with deposits of calcium phosphate. Thedegree of interstitial fibrosis was marked and diffuselypresent. By comparison, biopsy material from patientswith idiopathic calcium oxalate stones did not showintratubular crystals or interstitial fibrosis.
dRTA may be a primary disorder, either idio-pathic or inherited, but most commonly occurs inassociation with a systemic disease, one of the mostcommon causes of which is Sjogren syndrome (60). Intwo cases, dRTA developed in association with a waspsting (61).
The inherited form of dRTA because of genemutations that encode H� secretory pumps was dis-cussed already. Mutations in the human SLC4A1 geneencode the erythroid and kidney isoform of anion
112 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

exchanger 1. The erythroid isoform (eAE1) is presentin red blood cell membranes and mediates Cl�/HCO3
� exchange. The kidney isoform (kAE1) isfound in the basolateral surface of the � intercalatedcell and is required for normal urinary acidification.Human SLC4A1 gene mutations are responsible for thedevelopment of dRTA and ovalocytosis primarily re-ported in patients from Southeast Asia and rarely inother ethnic groups (62,63). The disturbance in trans-port properties of the anion exchanger varies depend-ing on the precise SLC4A1 gene mutations (64).
References1. Morris C, Low J: Metabolic acidosis in the critically ill: Part 1.
Classification and pathophysiology. Anaesthesia 63: 294–301, 20082. Morris C, Low J: Metabolic acidosis in the critically ill: Part 2.
Causes and treatment. Anaesthesia 63: 396–411, 20083. Kraut J, Madias N: Serum anion gap: Its uses and limitations in
clinical medicine. Clin J Am Soc Nephrol 2: 162–174, 20074. Moviat M, Terpstra A, Ruitenbeek W, Kliijtmans L, Pickkers P, van
der Hoeven J: Contribution of various metabolites to the “unmea-sured” anions in critically ill patients with metabolic acidosis. CritCare Med 36: 752–758, 2008
5. Chawla L, Jagasia D, Abell L, Seneff M, Egan M, Danino N, NguyenA, Ally M, Kimmel P, Junker C: Anion gap, anion gap corrected foralbumin, and base deficit fail to accurately diagnose clinically sig-nificant hyperlactatemia in critically ill patients. J Intensive CareMed 23: 122–127, 2008
6. Siegel A, Januzzi J, Sluss P, Lee-Lewandrowski E, Wood M, ShireyT, Lewandrowski K: Cardiac biomarkers, electrolytes, and otheranalytes in collapsed marathon runners: Implications for the evalua-tion of runners following competition. Am J Clin Pathol 129: 948–951, 2008
7. Kent K, Ganetsky M, Cogen J, Bird S: Non-fatal ventricular dys-rhythmias associated with severe salicylate toxicity. Clin Toxicol(Phila) 46: 297–299, 2008
8. Donnino M, Miller J, Garcia A, McKee E, Walsh M: Distinctiveacid-base pattern in Wernicke’s encephalopathy. Ann Emerg Med 50:722–725, 2007
9. Stacpoole P, Gilbert L, Neiberger R, Carney P, Valenstein E, Theri-aque D, Shuster J: Evaluation of long-term treatment of children withcongenital lactic acidosis with dichloroacetate. Pediatrics 121:e1223–e1228, 2008
10. Thoden J, Lebrecht D: Highly active antiretroviral HIV therapy-associated fatal lactic acidosis: Quantitative and qualitative mito-chondrial DNA lesions with mitochondrial dysfunction in multipleorgans. AIDS 22: 1093–1094, 2008
11. Lebrecht D, Deveaud C, Beauvoit B, Bonnet J, Kirschner J, WalkerU: Uridine supplementation antagonizes zidovudine-induced mito-chondrial myopathy and hyperlactatemia in mice. Arthritis Rheum58: 318–326, 2008
12. Wong L, Klemmer P: Severe lactic acidosis associated with juice ofthe mangosteen fruit Garcinia mangostana. Am J Kidney Dis 51:829–833, 2008
13. Bruijstens L, van Luin M, Buscher-Jungerhans P, Bosch F: Reality ofsevere metformin-induced lactic acidosis in the absence of chronicrenal impairment. Neth J Med 66: 185–190, 2008
14. Audia P, Feinfeld D, Dubrow A, Winchester J: Metformin-inducedlactic acidosis and acute pancreatitis precipitated by diuretic, cele-coxib, and candesartan-associated acute kidney dysfunction. ClinToxicol (Phila) 46: 164–166, 2008
15. Dell’aglio D, Perino L, Todino J, Algren D, Morgan B: Metforminoverdose with a resultant serum pH of 6.59: Survival without se-quelae. J Emerg Med March 14, 2008 [epub ahead of print]
16. Hong Y, O’Boyle C, Chen I, Hsiao C, Kuan J: Metformin-associatedlactic acidosis in a pregnant patient. Gynecol Obstet Invest 66:138–141, 2008
17. Fodale V, La Monaca E: Propofol infusion syndrome: An overviewof a perplexing disease. Drug Saf 31: 293–303, 2008
18. Zar T, Yusufzai I, Sullivan A, Graeber C: Acute kidney injury,hyperosmolality and metabolic acidosis associated with lorazepam.Nat Clin Pract Nephrol 3: 515–520, 2007
19. Hoffman R, Kirrane B, Marcus S: A descriptive study of an outbreakof clenbuterol-containing heroin. Ann Emerg Med 52: 548–553, 2008
20. Creagh-Brown B, Ball J: An under-recognized complication of treat-ment of acute severe asthma. Am J Emerg Med 26: 514.e1–514.e3,2008
21. Veenith T, Pearce A: A case of lactic acidosis complicating assess-ment and management of asthma. Int Arch Med 1: 3, 2008
22. Schmidt A, Karlson-Stiber C: Caffeine poisoning and lactate rise: Anoverlooked toxic effect? Acta Anaesthesiol Scand 52: 1012–1014,2008
23. Friedenberg A, Brandoff D, Schiffman F: Type B lactic acidosis as asevere metabolic complication in lymphoma and leukemia: A caseseries from a single institution and literature review. Medicine (Bal-timore) 86: 225–232, 2007
24. Udayakumar N, Rajendiran C, Muthuselvan R: A typical presentationof acute myeloid leukemia. J Cancer Res Ther 2: 82–84, 2006
25. Gowrishankar M, Carlotti A, George-Hyslop C, Bohn D, Kamel K,Davids M, Halperin M: Uncovering the basis of a severe degree ofacidemia in a patient with diabetic ketoacidosis. QJM 100: 721–735,2007
26. Sheikh-Ali M, Karon B, Basu A, Kudva Y, Muller L, Xu J, SchwenkW, Miles J: Can serum beta-hydroxybutyrate be used to diagnosediabetic ketoacidosis? Diabetes Care 31: 4: 643–647, 2008
27. Turan S, Omar A, Bereket A: Comparison of capillary blood ketonemeasurement by electrochemical method and urinary ketone in treat-ment of diabetic ketosis and ketoacidosis in children. Acta Diabetol45: 83–85, 2008
28. Sabatini S, Jurtzman N: Bicarbonate therapy in severe metabolicacidosis. J Am Soc Nephrol March 5, 2008 [epub ahead of print]
29. Giunti C, Priouzeau F, Allemand D, Levraut J: Effect of tris-hydroxymethyl aminomethane on intracellular pH depends on theextracellular non-bicarbonate buffering capacity. Transl Res 150:350–356, 2007
30. Marano M, Iodice F, Stoppa F, Tomasello C, Perrotta D, Cecchetti C,Di Nardo M, Ciampalini P, Pirozzi N: Treatment of severe diabeticacidosis with tris-hydroxymethyl aminomethane in a thirteen-year-old child. Minerva Anestesiol 74: 93–95, 2008
31. Lee P, Campbell L: Diabetic ketoacidosis: The usual villain or ascapegoat? A novel cause of severe metabolic acidosis in type 1diabetes. Diabetes Care 31: e13, 2008
32. Vermeersch N, Stolte C, Fostier K, Delooz H: An unusual case ofhyperglycemia, abdominal pain, and increased anion gap acidosis.J Emerg Med February 13, 2008 [epub ahead of print]
33. Manini A, Hoffman R, Nelson L: Alcoholic ketoacidosis in an11-year-old boy. Pediatr Emerg Care 24: 170–171, 2008
34. Yanagawa Y, Sakamoto T, Okada Y: Six cases of sudden cardiacarrest in alcoholic ketoacidosis. Intern Med 47: 113–117, 2008
35. Bilbault P, Levy J, Vinzio S, Castelain V, Schneider F: Abruptalcohol withdrawal: Another cause of ketoacidosis often forgotten.Eur J Emerg Med 15: 100–101, 2008
36. Pomara C, Fiore C, D’Errico S, Riezzo I, Finshcei V: Calciumoxalate crystals in acute ethylene glycol poisoning: A confocal laserscanning microscope study in a fatal case. Clin Toxicol (Phila) 46:322–324, 2008
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 113

37. Kraut J, Kurtz I: Toxic alcohol ingestions: Clinical features, diagno-sis, and management. Clin J Am Soc Nephrol 3: 208–225, 2008
38. Fenves A, Kirkpatrick H, Patel V, Sweetman L, Emmett M: Increasedanion gap metabolic acidosis as a result of 5-oxoproline (pyroglu-tamic acid): A role for acetaminophen. Clin J Am Soc Nephrol 1:441–447, 2006
39. Brooker G, Jeffery J, Nataraj T, Sair M, Ayling R: High anion gapmetabolic acidosis secondary to pyroglutamic aciduria (5-oxoprolin-uria): Association with prescription drugs and malnutrition. Ann ClinBiochem 44: 406–409, 2007
40. Ozmen S, Danis R, Akin D, Gullu N, Ozmen C, Yazanel O:Ureterosigmoidostomy-associated quadriparesis, non-traumatic rhab-domyolysis, and tetany in an adult. Int Urol Nephrol 40: 245–247,2008
41. Hoorn E, Zietse R: Combined renal tubular acidosis and diabetesinsipidus in hematological disease. Nat Clin Pract Nephrol 3: 171–175, 2007
42. Dinour D, Chang M, Satoh J, Smith B, Angle N, Knecht A, SerbanI, Holtzman E, Romero M: A novel missense mutation in the sodiumbicarbonate cotransporter (NBCe1/SLC4A4) causes proximal tubularacidosis and glaucoma through ion transport defects. J Biol Chem279: 52238–52246, 2004
43. Katzir Z, Dinour D, Reznik-Wolf H, Nissenkorn A, Holtzman E:Familial pure proximal renal tubular acidosis–a clinical and geneticstudy. Nephrol Dial Transplant 23: 1211–1215, 2008
44. Vega D, Maalouf N, Sakhaee K: Increased propensity for calciumphosphate kidney stones with topiramate use. Expert Opin Drug Saf6: 547–557, 2007
45. Welch B, Graybeal D, Moe O, Maalouf N, Sakhaee K: Biochemicaland stone-risk profiles with topiramate treatment. Am J Kidney Dis48: 555–563, 2006
46. Warner B, LaGrange C, Tucker T, Bensalem-Owen M, Pais V:Induction of progressive profound hypocitraturia with increasingdoses of topiramate. Urology 72: 29–32, 2008
47. Francois H, Coppo P, Hayman J, Fouqeray B, Mougenot B, Ronco P:Partial Fanconi syndrome induced by imatinib therapy: A novel causeof urinary phosphate loss. Am J Kidney Dis 51: 298–301, 2008
48. Bayrakci U, Baskin E, Ozcay F, Handan B, Karakayali H, Haberal M:Renal Fanconi syndrome and myopathy after liver transplantation:Drug-related mitochondrial cytopathy? Pediatr Transplant 12: 109–112, 2008
49. Koike K, Lida S, Usui M, Matsumoto Y, Fukami K, Ueda S, TamakiK, Kato S, Okuda S: Adult-onset acute tubulointerstitial nephritis anduveitis with Fanconi syndrome: Case report and review of theliterature. Clin Nephrol 64: 255–259, 2007
50. Chow K, Lai F, Szeto C, Chan N, Wong E, Li P: Quiz page March2008: Fever, anorexia, and renal failure. TINU syndrome. Am JKidney Dis 51: A39–A40, 2008
51. Shepp D, Curtis S, Rooney J: Causes and consequences of hypoka-lemia in patients on tenofovir disoproxil fumarate. AIDS 21: 1479–1481, 2007
52. Liborio A, Andrade L, Pereira L, Sanches T, Shimizu M, Seguro A:Rosiglitazone reverses tenofovir-induced nephrotoxicity. Kidney Int74: 910–918, 2008
53. Jefferies K, Cipriano D, Forgac M: Function, structure and regulationof the vacuolar (H�)-ATPases. Arch Biochem Biophys 476: 33–42,2008
54. Tasic V, Korneti P, Gucev Z, Hoppe B, Blau N, Cheong H: Atypicalpresentation of distal renal tubular acidosis in two siblings. PediatrNephrol 23: 1177–1181, 2008
55. Wagner C: When proton pumps go sour: Urinary acidification andkidney stones. Kidney Int 73: 1103–1105, 2008
56. Fuster D, Zhang J, Xie X, Moe O: The vacuolar-ATPase B1 subunitin distal tubular acidosis: Novel mutations and mechanisms fordysfunction. Kidney Int 73: 1151–1158, 2008
57. Walsh S, Shirley D, Wrong O, Unwin R: Urinary acidificationassessed by simultaneous furosemide and fludrocortisone treatment:an alternative to ammonium chloride. Kidney Int 71: 1310–1316,2007
58. Bonny O, Rubin A, Huang C, Frawley W, Pak C, Moe O: Mechanismof urinary calcium regulation by urinary magnesium and pH. J AmSoc Nephrol 19: 1530–1537, 2008
59. Evan A, Lingeman J, Coe F, Shao Y, Miller N, Matlaga B, PhillipsC, Sommer A, Worcester E: Renal histopathology of stone-formingpatients with distal renal tubular acidosis. Kidney Int 71: 795–801,2007
60. Ren H, Wang M, Chen X, Zhang W, Pan X, Wang X, Lin Y, ZhangS, Chen N: Renal involvement and followup of 130 patients withprimary Sjogren’s syndrome. J Rheumatol 35: 278–284, 2008
61. D’Cruz S, Chauhan S, Singh R, Sachdev A, Lehl S: Wasp stingassociated with type 1 renal tubular acidosis. Nephrol Dial Trans-plant 23: 1754–1755, 2008
62. Khositseth S, Sirikanaeret A, Khopraset S, Opastiakul S, Kingwatan-akul P, Thongoppinkhun W, Yenchitsomanus P: Hematological ab-normalities in patients with distal renal tubular acidosis and hemo-globinopathies. Am J Hematol 83: 465–471, 2008
63. Jamard B, Allard J, Caron P, Corberand J, Blanchard A, Vargas-Poussou R, Mahou S, Constantin A, Cantagrel A, Mazieres B,Laroche M: Distal renal tubular acidosis and ovalocytosis: A casereport. Osteoporos Int 19: 119–122, 2008
64. Walsh S, Borgese F, Gabillat N, Unwin R, Guizouarn H: Cationtransport activity of anion exchanger 1 (AE1) mutations found ininherited distal renal tubular acidosis (dRTA): structure-functionimplications for AE1. Am J Physiol Renal Physiol 295: F343–F350,2008
Hyponatremia
Isotonic and Hypertonic HyponatremiaNonhypotonic hyponatremia can be recognized
by the presence of an “osmolar gap”—a differencebetween the measured plasma osmolality and the os-molality calculated from the plasma sodium concen-tration, blood urea nitrogen (BUN), and blood glucose.If the laboratory reports the concentration of thesesolutes in mmol/L, then the calculated osmolalityequals the doubled sodium concentration (so as toaccount for sodium’s accompanying anions) plus themillimolar concentrations of urea and glucose. If theBUN and glucose are expressed in mg/dl, then theseconcentrations are converted to mmol/L by dividingthe BUN by 2.8 and blood glucose by 18. The pres-ence of an osmolar gap in a patient with hyponatremiausually means that the patient has pseudohyponatre-mia or that hyponatremia is caused by the presence ofexcessive concentrations of a non–sodium-effectiveosmole in the circulation. An osmolar gap is alsopresent when the plasma contains high concentrationsof ethanol, methanol, or isopropyl alcohol; however,these solutes are not effective osmoles (i.e., they do
114 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

not osmotically attract water from cells, and they donot cause hyponatremia). Patients with azotemia andhyponatremia may have a normal or high plasmaosmolality, but they do not have an osmolar gap. Ureais not an effective osmole unless its concentration ischanging rapidly because of urea infusion or dialysis.Attention to the “effective osmolality” (i.e., the plasmaosmolality minus the osmotic contribution of urea)may help in the evaluation of these patients.
PseudohyponatremiaSodium’s biologic effects are determined by its
concentration in plasma water. Thus, “true hyponatre-mia” or “hypotonic hyponatremia” is characterized bya decreased concentration of sodium in the aqueousphase of plasma. Plasma is normally 93% water and7% proteins and lipids. Hyperproteinemia or hyperlip-idemia decreases the fraction of the plasma samplethat is aqueous. Under these conditions, each volumeof plasma measured will contain less Na� (becauseNa� is present only in plasma water), and most auto-mated clinical laboratory determinations will report anartifactually low plasma sodium concentration despitea normal sodium concentration in plasma water—aphenomenon called “pseudohyponatremia.” Potentio-metric methods have come into widespread use be-cause of advances in ion-sensitive electrodes (ISEs).Instruments for routine chemical analysis typically useindirect ISEs to measure sodium levels. With an indi-rect ISE, the plasma sample is diluted before the actualmeasurement is obtained, and the plasma sodium con-centration is then determined by correcting for thedilution degree and by assuming that plasma waterequals 93% of the total sample volume; therefore, thesodium level as determined by indirect ISE will beartificially low when the plasma water content is�93%. Instruments used for measuring arterial bloodgases use direct ISE without any dilution and measurethe activity of sodium in the water phase only. Thus,pseudohyponatremia does not occur when the mea-surement is made with direct ISE (sometimes called“direct potentiometry”). These differences in methodshould be taken into account to explain discrepanciesbetween results obtained with classical biochemistryanalyzers and with blood gas apparatus, and they canbe exploited in evaluating patients in whom pseudohy-ponatremia is suspected.
In the absence of a direct-reading ISE system, an
approach to circumvent the problem of pseudohyponatre-mia is first to estimate plasma water from the formula
plasma water content (%)� 99.1 � (0.1 � L) � (0.07 � P) [equation 1],
where L and P refer to the total lipid and protein con-centrations in g/L, respectively, and then to adjust thisvalue to the normal value for plasma water content of93% (1–3); however, values that are obtained by direct-reading ISEs are likely to be more accurate than calcu-lated values that are based on protein and lipid concen-trations using equation 1. Nguyen et al. (1) inducedpseudohyponatremia in the laboratory by dissolving salt-free albumin in human plasma to vary the plasma proteinconcentration from 7.4 to 28.4 g/L. The investigatorsthen measured the plasma water content gravimetrically(by drying). Then they compared the directly measuredwater content of the samples with a calculated valuebased on equation 1 (based on plasma lipid and proteinconcentrations) and with a calculated value based ondifferences between plasma sodium concentrations usingdirect-reading ISE (which was unaffected by the in-creased plasma protein concentration) and indirect (withdilution) ISE. The experiment showed that there is ex-cellent agreement between the ISE-determined plasmawater content and the gravimetrically determined plasmawith no discernible statistical difference between thesevalues but a substantial discrepancy from the value cal-culated using estimates such as equation 1; therefore, fora given patient, the plasma water content can be deter-mined from the difference between a simultaneous directand indirect ISE reading. This calculated value couldthen be used to correct subsequent measurements that arebased on indirect ISE, permitting serial sodium concen-tration measurements for that patient using an automateddevice.
For example, hypergammaglobulinemia is acommon finding in HIV-infected patients and is theresult of both virus-specific and polyclonal B cellactivation. It is also common among patients withcirrhosis and/or hepatitis C infection. Whereas hypo-natremia in end-stage liver disease usually is causedby cirrhosis, pseudohyponatremia should be consid-ered in the differential diagnosis for patients withhypergammaglobulinemia and liver disease. Patientswho are co-infected with hepatitis C and HIV areespecially likely to have high IgG levels. A recent case
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 115

report of a co-infected patient with a polyclonal hy-pergammaglobulinemia (total protein concentration11.7 g/dl) nicely illustrates this observation (4). Thepatient presented with a serum sodium of 119 mEq/L,a plasma osmolality of 290 mOsm/kg, and an osmolargap of 29 mOsm/kg. In the absence of any otherexplanation for the osmolar gap, the serum sodiumwas repeated using direct ISE and was found to be 128mEq/L, reducing the osmolar gap to 11 mOsm/kg.Thus, the patient had a combination of true hypona-tremia (likely caused by diuretics and liver disease)and pseudohyponatremia caused by hyperproteinemia.Using equation 1, the authors calculated the patient’splasma aqueous volume to be 0.90 rather than 0.93.Using a dilution factor based on a plasma watercontent of 93% rather than 90% led to an underesti-mation of the plasma sodium concentration when thelaboratory measured the serum sodium concentrationusing an automated indirect ISE method.
Solute-Induced Nonhypotonic HyponatremiaHypertonic hyponatremia is caused by abnor-
mally high concentrations of an effective osmole in thecirculation, diluting the plasma sodium concentrationby osmotically attracting water from cells. Unlikehypotonic hyponatremia, in which cells are swollen,body cells are dehydrated in hypertonic hyponatremia.Hyperglycemia, mannitol infusions, and Ig infusionpreparations that contain maltose or sucrose are themost common causes. Hypertonic mannitol and thehypertonic sugars contained in Ig preparations arenephrotoxic. The development of hyponatremia in amannitol recipient is an early warning sign of mannitolaccumulation; treatment with hypertonic saline orother measures aimed at increasing the serum sodiumconcentration are contraindicated, and early hemodi-alysis to remove the offending solute is probably thebest approach (5). Hyponatremia is a known compli-cation of intravenous Ig (IVIG). Because IVIG hasbeen reported to result in postinfusional hyperpro-teinemia, IVIG-induced hyponatremia has often beenattributed to pseudohyponatremia. More recently, thesugar additives in Ig preparations is an identifiedmajor factor in IVIG-related hyponatremia. These ad-ditives help prevent Ig aggregation and have reducedthe frequency and severity of systemic reactions, butthey have also resulted in osmotic renal injury andhyponatremia resulting from an osmotic translocationof cellular water. Thus, hyponatremia resulting from
IVIG is likely to be multifactorial: (1) Pseudohy-ponatremia secondary to the increased protein phase(associated with an increased osmolal gap), (2) truehyponatremia resulting from sucrose-induced translo-cation of water from the intracellular compartment tothe extracellular compartment (associated with an in-creased osmolal gap), and (3) true dilutional hypona-tremia because of retention of the large volume ofsolvent required for reconstitution of the IVIG product(associated with a normal osmolal gap).
A Greek single-center study retrospectively evalu-ated a cohort of 66 unselected patients who had idio-pathic thrombocytopenic purpura and received 140courses of IVIG (Sandoglobulin 3%, which containssucrose) in an average dosage of 35 g/d (2). Acute kidneyinjury was observed in 10 (15%) of 66 patients. IVIG-related hyponatremia, defined as a sodium level �134mmol/L, was only observed in nine (9%) patients, andthe lowest serum sodium value was 130 mmol/L. Asignificant inverse correlation (r � �0.308; P � 0.01)was found between the changes in serum sodium andcreatinine, and the mean reduction in serum sodiumconcentration in patients with acute kidney injury wassignificantly (P � 0.01) higher than in patients whoserenal function remained stable (5.7 versus 2.7 mmol/L).The serum protein concentration increased from 7.2 to8.9 g/dl, which would be expected to decrease plasmawater by 1.1% with a corresponding decrease in plasmasodium by 1.1%, or 1.6 mmol/L from the initial value of141 mmol/L. This anticipated change of 1.6 mmol/L insodium concentration, however, was half of the 3.1-mmol/L fall in sodium that occurred; the remainder canbe attributed to an osmotic shift caused by the sucroseconstituent of the IVIG preparation. As with hypergly-cemia, the sucrose present in the IVIG decreases theserum sodium concentration by provoking net movementof water out of cells. When renal function is impaired,renal clearance of sucrose diminishes, magnifying thiseffect. Rather similar findings were found in two patientswith renal failure described by Nguyen et al. (3). AfterIVIG, both patients had 5- to 6-mEq/L differences be-tween indirect ISE- and direct ISE-measured plasmasodium concentrations (suggesting an element ofpseudohyponatremia), but, in both cases, the DSE valueswere low and therefore reflective of “true hyponatremia”secondary to IVIG (i.e., a low sodium concentration inplasma water). The authors noted that impaired waterexcretion and the large water load provided by IVIG (a2-g/kg dose for a 70-kg patient provides 2.33 L of water)
116 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

can cause “true hyponatremia.” Without measuring theplasma osmolality with an osmometer as well as theplasma sodium by DSE, one cannot distinguish betweenhypotonic hyponatremia caused by positive water bal-ance and hypertonic or isotonic hyponatremia caused byretained sucrose or a combination of the two. Althoughhypertonic and isotonic hyponatremia are “true hypona-tremia” in the sense that they represent sodium concen-trations that are low in the extracellular fluid in vivo,therapeutic measures to increase the plasma sodium con-centration are not indicated.
Isotonic hyponatremia may complicate transure-thral prostate surgery when isosmotic or hypo-osmoticirrigants abruptly enter the circulation via the surgi-cally disrupted prostatic venous plexus. A similarsyndrome can complicate endoscopic intrauterine sur-gery. In these cases, the solute responsible for the lowplasma sodium concentration is rapidly absorbed withwater so that the plasma osmolality is not increasedand there is no water shift from cells. Rather, there isan expansion of the extracellular space with fluid, andas long as the absorbed solute remains extracellular,the water that is absorbed with the solute remainsextracellular as well, diluting the plasma sodium con-centration. Depending on the osmolality of the irrig-ant, the plasma osmolality either remains unchangedor falls slightly. Accumulation of glycine, the mostcommonly used irrigant, causes neurotoxicity becauseof direct effects of the amino acid itself and because ofthe hyperammonemia that results from its metabolism.Use of nonconducting nonelectrolyte irrigants (glu-cose, mannitol, glycine, or sorbitol) was introducedbecause the use of electrocautery contraindicated con-ductive solutions such as isotonic saline as an irrigant.Water was initially used in lieu of saline, but becauseof reports of hemolysis, renal failure, and sometimesfatal circulatory collapse, other solutions were devel-oped. Although the safety of pure water as an irrigat-ing solution in prostate surgery remains controversial,this fluid is still commonly used in some countries. Astudy of 1600 prostatectomies in a single center in Iranfound only a 2.5% incidence of clinically significanthyponatremia (serum Na �130 mmol/L) and a 1%incidence of severe hemolysis with no deaths (6). Thenewly developed bipolar electrocautery resectoscopepermits isotonic saline as an irrigant and avoids boththe hypotonic hyponatremia caused by water absorp-tion and the isotonic hyponatremia caused by solutesthat containing nonelectrolyte solutes (7–9).
References1. Nguyen MK, Ornekian V, Butch AW, Kurtz I: A new method for
determining the plasma water content: Application in pseudohy-ponatremia. Am J Physiol Renal Physiol 292: F1652–F1656, 2007
2. Daphnis E, Stylianou K, Alexandrakis M, Xylouri I, Vardaki E,Stratigis S, Kyriazis J: Acute renal failure, translocational hyponatre-mia and hyperkalemia following intravenous immunoglobulin therapy.Nephron Clin Pract 106: c143–c148, 2007
3. Nguyen MK, Rastogi A, Kurtz I: True hyponatremia secondary tointravenous immunoglobulin. Clin Exp Nephrol 10: 124–126, 2006
4. Garibaldi BT, Cameron SJ, Choi M: Pseudohyponatremia in a patientwith HIV and hepatitis C coinfection. J Gen Intern Med 23: 202–205,2008
5. Yun JJ, Cheong I: Mannitol-induced hyperosmolal hyponatraemia.Intern Med J 38: 73, 2008
6. Moharari RS, Khajavi MR, Khademhosseini P, Hosseini SR, Najafi A:Sterile water as an irrigating fluid for transurethral resection of theprostate: Anesthetical view of the records of 1600 cases. South Med J101: 373–375, 2008
7. Michielsen DP, Debacker T, De Boe V, Van Lersberghe C, KaufmanL, Braeckman JG, Amy JJ, Keuppens FI: Bipolar transurethral resec-tion in saline: An alternative surgical treatment for bladder outletobstruction? J Urol 178: 2035–2039, discussion 2039, 2007
8. Gilleran JP, Thaly RK, Chernoff AM: Rapid communication: BipolarPlasmaKinetic transurethral resection of the prostate: Reliable trainingvehicle for today’s urology residents. J Endourol 20: 683–687, 2006
9. Ho HS, Yip SK, Lim KB, Fook S, Foo KT, Cheng CW: A prospectiverandomized study comparing monopolar and bipolar transurethralresection of prostate using transurethral resection in saline (TURIS)system. Eur Urol 52: 517–522, 2007
Hypotonic Hyponatremia
Brain Responses to HyponatremiaHypotonic hyponatremia causes swelling of all
body cells, but it is particularly harmful in the brainbecause of the limitations posed by the rigid skull. Asthe brain swells in a confined space, blood flow isimpaired, potentially causing ischemia, infarct, excito-toxicity, and neuronal death. In rare cases, brain hernia-tion through the foramen magnum affects brain stemfunction, causing death by respiratory and cardiac arrest.Fortunately, the brain responds to hyponatremia in waysthat limit the amount of swelling (1,2). Within minutes,the increase in hydrostatic pressure increases the flow ofsodium-rich interstitial fluid into the cerebrospinal fluidand from there to the general circulation. Soon after,brain cells respond with a volume regulatory responsethat diminishes the degree of cell swelling.
The ability to regulate cell volume is an ancienttrait conserved throughout evolution in animal cells frommost species. Volume control is evidently essential topreserve a variety of cell functions. When cells areexposed to a hypotonic environment, they first swell andthen activate a mechanism of volume regulatory decrease(RVD), in which osmotically active solutes are extrudedfollowed by water. The osmolytes involved in RVD are
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 117

the main intracellular ions K� and Cl� and a largenumber of small organic molecules, known as organicosmolytes. Organic osmolytes are considered to act as“compatible” or “nonperturbing” cell solutes that func-tion as osmoregulators without severely compromisingcell function; cells release them in response to hypoto-nicity and import them in response to hypertonicity orcorrection of hypotonicity. By extruding electrolytes andorganic osmolytes, cells can achieve a low intracellularosmolality—equal to that of plasma—without a largeincrease in cell water. Changes in osmolyte concentra-tions, both inorganic and organic, can be quite large, andthey can virtually eliminate brain swelling despite verysevere hyponatremia. In animals that have completelyadapted to hyponatremia, brain concentrations of organicosmolytes can decrease by 40 to 90%, whereas chlorideand potassium concentrations decrease by 10 to 20%.
The brain is separated from the systemic circulationby the blood–brain barrier, which impedes the entry ofsubstances that are not lipid soluble (2,3). Anatomically,the barrier consists of tight junctions between vascularendothelial cells that interface with glial cells (astrocytes)whose foot processes abut the endothelial cells of braincapillaries. In hyponatremia, water enters the brain pri-marily through the astrocytic endfeet. In experimentalmodels, water is shunted through the astrocytes, whichswell to more than double their normal size, whereasneurons maintain their cell volume; astrocytes that areclose to blood vessels increase their volume by a factor of2 to 3, whereas astrocytes with no obvious relation toblood vessels fail to show a volume increase (4). Waterchannels, particularly aquaporin 4 (AQP4), permit waterto cross the blood–brain barrier in response to osmoticgradients. Recent evidence suggests that the AQP4 waterchannels influence the severity of cerebral edema thatoccurs in response to acute hyponatremia and otherinsults. Knockout mice that do not express AQP4 de-velop less brain swelling in response to acute experimen-tal hyponatremia, and selective deletion of AQP4 fromthe astrocytic endfeet that surround brain microvessels isalso protective against brain swelling (4,5). Conversely,transgenic mice overexpressing AQP4 have exaggeratedbrain swelling, with an increase in intracranial pressurenearly twice that of controls, often producing brain her-niation and death (6). Recently, multiple polymorphismsin the human AQP4 gene have been identified, some ofwhich affect water flow; these findings suggest that theremay be genetic variability in the susceptibility to brainswelling from acute hyponatremia (7).
The blood–brain barrier consists of tightjunctions between vascular endothelial cellsthat interface with glial cells (astrocytes)whose foot processes abut the endothelialcells of brain capillaries. In hyponatremia,water enters the brain through the astrocyticendfeet. Astrocytes close to blood vesselsswell to more than double their normal size,whereas neurons maintain their cell volume.Water channels, particularly AQP4, permitwater to cross the blood–brain barrier inresponse to osmotic gradients.
The reason that astrocytes swell more than neu-rons in response to hypotonicity may relate to greaterexpression of AQP4 in astrocytes or to a more efficientoperation of volume regulation in neurons as com-pared with astrocytes. Consistent with the latter hy-pothesis, Purkinje cells in the cerebellum have beenshown to release a large amount of taurine, which istransferred to neighboring astrocytes. As a conse-quence of this taurine translocation, neurons preservetheir volume, whereas astrocytes swell (1,2). Taurine,a sulfur-containing amino acid, is the most abundantfree amino acid in mammalian tissue. Maintenance ofthe large intracellular taurine pool requires cellularamino acid uptake from the blood against a substantialconcentration gradient, because the concentration oftaurine is 100-fold less in the plasma than in thetissues. Taurine is present in high concentrations inmost animal cells, largely free in the cytosol. It ismetabolically inert and not a protein constituent. Com-pared with other osmolytes, taurine responds to os-motic swelling with the lowest release threshold andthe largest amount released. Taurine efflux occursthrough a leak pathway known as volume-sensitiveorganic anion channel (1,2,8–10).
Other organic osmolytes that are involved in RVDare a group of small, heterogeneous organic molecules:Amino acids (taurine, glutamate, glycine, and GABA),polyalcohols (sorbitol and myoinositol), amines (creat-ine, phosphoethanolamine, and glycerophosphorylcho-line), and N-acetyl-aspartate. Despite structural differ-ences, these molecules are believed to permeate throughthe same pathway. Because GABA and glutamate aremajor neurotransmitters, their release from intracellularpools may affect neuronal excitability.
118 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

Recent evidence has shown the potential impor-tance of G protein–coupled receptors (GPCRs) in en-hancing the release of organic osmolytes from neuralcells in response to hypotonicity (1,2). GPCRs representthe largest family of membrane proteins, and approxi-mately 300 such receptors are expressed in the brain.Importantly, receptor activation significantly lowers theosmotic threshold at which osmolyte release occurs,allowing cells to respond to small, physiologically rele-vant decreases in tonicity. The widespread occurrence ofthese receptors in the central nervous system and thecritical importance of regulating brain cell volume makethis observation especially intriguing because it mayexplain the unique ability of neural cells to resist osmoticswelling. Receptor regulation of volume-dependent os-molyte release means that the adaptation to hyponatremiacould be accelerated by specific ligands that are known toactivate GPCRs, and it may also explain individual vari-ations in the ability to tolerate hyponatremia.
Regulation of osmolyte release has been observedin response to a variety of neurotransmitters or neuro-modulators, including neuropeptides (vasopressin, en-dothelin, and oxytocin), cholinergic and adrenergicagonists, adenosine, ATP, thrombin, and phospho-lipids; the ligand concentrations required to elicitosmolyte release in vitro are within the range ofthese compounds found in the central nervous sys-tem (2,8 –10).
Organic osmolyte efflux from astrocytes may playa role in the regulation of vasopressin release by theneurohypophesis. Acting through V1a receptors, vaso-pressin potentiates the volume-dependent release of tau-rine. Once released, taurine activates glycine receptors onnerve terminals that originate in the supraoptic nucleusand inhibits vasopressin secretion. Thus, the ability ofvasopressin to stimulate taurine efflux provides a nega-tive paracrine feedback loop. Vasopressin secretion mayalso be regulated by adenosine, which inhibits the releaseof taurine from pituitcytes
In response to hypertonicity or after correction ofhyponatremia, organic osmolytes are transported intocells. Taurine uptake is mediated by a sodium-depen-dent transporter (TauT), which uses the Na� gradientacross the cell membrane to drive taurine accumula-tion. Myoinositol, another important organic osmolyte, istransported by the sodium-dependent myoinositol trans-porter. Amino acids are transported by the sodium-cou-pled neutral amino-acid transporter member 2 (SNAT2).It has been known for many years that these transporters
are upregulated in chronic hypertonicity, a phenomenonthat helps to explain the stubborn persistence of accu-mulated osmolytes in patients with hypernatremia andthe resultant cerebral edema that occurs when hyper-natremia is corrected too rapidly. Recent evidencesuggests that chronic hypotonicity may downregulatethese transporters (11).
Chronic hyponatremia downregulates thesignaling pathway, regulating expressionof the neutral amino acid transporterSNAT2. Oligodendrocytes may rely primar-ily on amino acid accumulation to recovertheir cell volume. Any deficiency in tonici-ty-induced SNAT2 expression would ren-der oligodendrocytes selectively vulnera-ble after systemic hypertonicity or rapidcorrection of chronic hyponatremia. Thismight be the case in osmotic demyelina-tion syndrome.
Hyponatremia that develops rapidly (�24 h) isassociated with more severe cerebral edema, moresevere neurologic symptoms, and a risk for death fromherniation. In experimental models, the brain’s adap-tation to hyponatremia is completed within approxi-mately 48 h; therefore, many investigators have de-fined hyponatremia that has evolved over �48 h as“chronic,” and more rapidly developing hyponatremiahas been called “acute” (12–18).
Brain Responses to Correction ofHyponatremia: Osmotic Demyelination
Depletion of brain organic osmolytes permitssurvival in chronic hyponatremia and limits the sever-ity of neurologic symptoms, but it may also lead toneurologic injury when the electrolyte disturbance iscorrected too rapidly. Perhaps because of downregu-lation of transporters, organic osmolytes are slow toreturn to the brain when chronic hyponatremia iscorrected. As a result, excessive correction of hypo-natremia can cause neurologic complications, whichmanifest as the osmotic demyelination syndrome(2,17,19–23).
Clinical manifestations of osmotic demyelinationtypically emerge 1 d to several days after a large, rapidincrease in sodium concentration. Observational stud-ies and reviews of published case reports suggested
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 119

that increases of 10 to 12 mEq/L within 24 h andincreases of 18 to 25 mEq/L within 48 h are sufficientto cause the syndrome; patients with alcoholism, liverdisease, and malnutrition are most vulnerable to os-motic demyelination and may occasionally be affectedby even slower rates of correction (24). Patients andexperimental animals with acute hyponatremia (�24 hduration) have a lower risk for osmotic demyelinationand often tolerate large, rapid increases in the serumsodium concentration that are uniformly injurious inthe chronic condition (18).
In patients who have the osmotic demyelinationsyndrome and die, brain lesions known as “myelinol-ysis,” characterized by a loss of oligodendrocytes andmyelin without inflammation, are found (17). Classi-cally, the lesions are located in the center of the pons(“central pontine myelinolysis”), but similar lesionsare often found symmetrically distributed in manyregions of the brain where gray and white matter areclosely associated (“extrapontine myelinolysis”).
The response to correction of chronic hyponatre-mia is analogous to the response to hypertonicity. Inhypertonicity, cells must accumulate organic os-molytes to avoid osmotic shrinkage. With correctionof chronic hyponatremia, cells must re-accumulatethese osmolytes. Indeed, myelinolysis has been re-ported in patients who were never known to havehyponatremia and who were subjected to an acuteonset of hypertonicity (25). Uremia, which is associ-ated with resistance to myelinolysis, seems to enhancethe reuptake of organic osmolytes by the brain, par-ticularly myoinositol; however, patients with hypona-tremia and uremia are not immune from osmoticdemyelination (20). Exogenous administration of my-oinositol during correction of hyponatremia has beenshown to reduce the incidence and severity of myeli-nolysis (17).
It has been suggested that shrinkage of brainvascular endothelial cells disrupts their tight junctions,opening the blood–brain barrier; circulating comple-ment, cytokines, and lymphocytes can then enter thebrain, causing oligodendrocyte damage and demyeli-nation. Alternatively, oligodendrocytes might be in-jured directly by shrinkage, triggering apoptosis. Dif-ferences in the way that various populations of braincells respond to osmotic stress may explain why my-elin-producing oligodendrocytes are selectively in-jured by rapid correction of hyponatremia (26,27).
Osmoprotective genes that are involved in cellu-
lar osmoadaptation to hypertonicity are regulated by aspecific transcription factor called tonicity-responsiveenhancer-binding protein (TonEBP). In the brain,TonEBP is expressed only in neurons, but neurons invarious brain regions differ in the degree to whichTonEBP responds to hypertonicity (27). Induction ofsodium-dependent myoinositol transporter–mRNA la-beling (which encodes the myoinositol transporter)seems to occur in non-neuronal cells, presumablyastrocytes, where TonEBP is neither expressed nortonicity induced. Thus, brain cells, even from the sameclass, activate distinct osmoprotective genes throughdistinct activation processes to adapt to hypertonicity.
Chronic hyponatremia downregulates the signal-ing pathway, regulating expression of the neutralamino acid transporter SNAT2. Tonicity-inducedSNAT2 expression is restricted to oligodendrocytesbut occurs in virtually all of them. Oligodendrocytesmay rely primarily on amino acid accumulation torecover their cell volume, whereas other brain cellsthat do not rely on amino acid accumulation throughtonicity-induced SNAT2 expression are not affected(26). Any deficiency in tonicity-induced SNAT2 ex-pression would render oligodendrocytes selectivelyvulnerable after systemic hypertonicity or rapid cor-rection of chronic hyponatremia. This might be thecase in osmotic demyelination syndrome.
References1. Fisher SK, Cheema TA, Foster DJ, Heacock AM: Volume-dependent
osmolyte efflux from neural tissues: Regulation by G-protein-cou-pled receptors. J Neurochem 106: 1998–2014, 2008
2. Vazquez-Juarez E, Ramos-Mandujano G, Hernandez-Benitez R, Pas-antes-Morales H: On the role of G-protein coupled receptors in cellvolume regulation. Cell Physiol Biochem 21: 1–14, 2008
3. Ayus JC, Achinger SG, Arieff A: Brain cell volume regulation inhyponatremia: Role of gender, age, vasopressin and hypoxia. Am JPhysiol Renal Physiol 295: F619–F624, 2008
4. Nase G, Helm PJ, Enger R, Ottersen OP: Water entry into astrocytesduring brain edema formation. Glia 56: 895–902, 2008
5. Papadopoulos MC, Verkman AS: Aquaporin-4 and brain edema.Pediatr Nephrol 22: 778–784, 2007
6. Yang B, Zador Z, Verkman AS: Glial cell aquaporin-4 overexpres-sion in transgenic mice accelerates cytotoxic brain swelling. J BiolChem 283: 15280–15286, 2008
7. Sorani MD, Zador Z, Hurowitz E, Yan D, Giacomini KM, ManleyGT: Novel variants in human aquaporin-4 reduce cellular waterpermeability. Hum Mol Genet 17: 2379–2389, 2008
8. Vazquez-Juarez E, Ramos-Mandujano G, Lezama RA, Cruz-RangelS, Islas LD, Pasantes-Morales H: Thrombin increases hyposmotictaurine efflux and accelerates ICI-swell and RVD in 3T3 fibroblastsby a src-dependent EGFR transactivation. Pflugers Arch 455: 859–872, 2008
9. Cruz-Rangel S, Hernandez-Benitez R, Vazquez-Juarez E, Lopez-Dominguez A, Pasantes-Morales H: Potentiation by thrombin of
120 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

hyposmotic glutamate and taurine efflux from cultured astrocytes:Signalling chains. Neurochem Res 33: 1518–1524, 2008
10. Ramos-Mandujano G, Vazquez-Juarez E, Hernandez-Benitez R, Pas-antes-Morales H: Thrombin potently enhances swelling-sensitiveglutamate efflux from cultured astrocytes. Glia 55: 917–925, 2007
11. Franchi-Gazzola R, Dall’Asta V, Sala R, Visigalli R, Bevilacqua E,Gaccioli F, Gazzola GC, Bussolati O: The role of the neutral aminoacid transporter SNAT2 in cell volume regulation. Acta Physiol 187:273–283, 2006
12. Ellison DH, Berl T: Clinical practice: The syndrome of inappropriateantidiuresis. N Engl J Med 356: 2064–2072, 2007
13. Gross P: Treatment of hyponatremia. Intern Med 47: 885–891, 200814. Halperin ML, Kamel KS: A new look at an old problem: Therapy of
chronic hyponatremia. Nat Clin Pract Nephrol 3: 2–3, 200715. Hoorn EJ, Zietse R: Hyponatremia revisited: Translating physiology
to practice. Nephron Physiol 108: 46–59, 200816. Lien YH, Shapiro JI: Hyponatremia: Clinical diagnosis and manage-
ment. Am J Med 120: 653–658, 200717. Sterns RH, Silver S, Kleinschmidt-DeMasters BK, Rojiani AM:
Current perspectives in the management of hyponatremia: Preventionof CPM. Expert Rev Neurother 7: 1791–1797, 2007
18. Verbalis JG, Goldsmith SR, Greenberg A, Schrier RW, Sterns RH:Hyponatremia treatment guidelines 2007: Expert panel recommen-dations. Am J Med 120: S1–S21, 2007
19. Gutenstein M: Osmotic myelinolysis syndrome after treatment ofsevere deamino arginine vasopressin-associated hyponatraemia: Pit-falls in emergency medicine. Emerg Med Australas 19: 68–70, 2007
20. Huang WY, Weng WC, Peng TI, Ro LS, Yang CW, Chen KH:Central pontine and extrapontine myelinolysis after rapid correctionof hyponatremia by hemodialysis in a uremic patient. Ren Fail 29:635–638, 2007
21. Snell DM, Bartley C: Osmotic demyelination syndrome followingrapid correction of hyponatraemia. Anaesthesia 63: 92–95, 2008
22. Lin CM, Po HL: Extrapontine myelinolysis after correction of hypo-natremia presenting as generalized tonic seizures. Am J Emerg Med26: 632.e5–632.e6, 2008
23. Roh JH, Kim JH, Oh K, Kim SG, Park KW, Kim BJ: Cortical laminarnecrosis caused by rapidly corrected hyponatremia. J NeuroimagingMay 19, 2008 [epub ahead of print]
24. Georgy V, Mullhi D, Jones AF: Central pontine myelinolysis follow-ing ‘optimal’ rate of correction of hyponatraemia with a good clinicaloutcome. Ann Clin Biochem 44: 488–490, 2007
25. O’Malley G, Moran C, Draman MS, King T, Smith D, Thompson CJ,Agha A: Central pontine myelinolysis complicating treatment of thehyperglycaemic hyperosmolar state. Ann Clin Biochem 45: 440–443,2008
26. Maallem S, Mutin M, Gonzalez-Gonzalez IM, Zafra F, Tappaz ML:Selective tonicity-induced expression of the neutral amino-acid trans-porter SNAT2 in oligodendrocytes in rat brain following systemichypertonicity. Neuroscience 153: 95–107, 2008
27. Maallem S, Wierinckx A, Lachuer J, Kwon MH, Tappaz ML: Geneexpression profiling in brain following acute systemic hypertonicity:Novel genes possibly involved in osmoadaptation. J Neurochem 105:1198–1211, 2008
Acute HyponatremiaAlthough acute hyponatremia is defined biolog-
ically by the time course of its evolution, this defini-tion can seldom be applied to patients who develophyponatremia outside the hospital. Ambulatory pa-tients who present to the hospital with hyponatremiararely have recent previous laboratory values, and thedesignation of “acute” hyponatremia is often based on
the circumstances that led to the electrolyte distur-bance. For example, hyponatremia in marathon run-ners, ecstasy users, and psychotic patients with self-induced water intoxication may be characterized as“acute” because it typically presents after a few hoursof unusually large water intakes coupled with impairedwater excretion. These patients, like hospitalized pa-tients with iatrogenic hyponatremia, often present withsevere neurologic symptoms, and death from hernia-tion in ambulatory patients have been reported almostexclusively in these settings. Unlike patients who havehad hyponatremia for �48 h, patients who are knownto have hyponatremia of brief duration seem to toleratea rapid return of their serum sodium concentrations tonormal without adverse consequences. As discussed inthe previous fluid and electrolyte issue of NephSAP,there are data to suggest that hypoxia impairs thebrain’s adaptation to hyponatremia, increasing the se-verity of cerebral edema, which in turn results inneurogenic pulmonary edema and a vicious cycle (1).
It has been noted that young women and childrenaccount for most reports of fatal or neurologicallycrippling complications from cerebral edema causedby acute postoperative hyponatremia. One group at-tempted to explain these clinical observations mecha-nistically in a recent review of brain cell volumeregulation (1). The increased susceptibility of youngchildren is explained by the brain’s size (which is fullsize by age 6) relative to the skull (which does notreach full size until adulthood). Consistent with thishypothesis, acute hyponatremia in young infantswhose fontanel is open does not result in herniation.To explain the susceptibility of young women withhyponatremia to fatal cerebral edema, the review sug-gested that estrogens impair volume regulation by thebrain; however, the experimental evidence offered tosupport this idea is problematic. The review suggestedthat estrogens regulate water movement and neuro-transmission by affecting aquaporin 4 expression;however, the article cited to support this assertiondemonstrated that aquaporin 4 regulates the functionsof ovarian hormones and neurotransmission and notvice versa (2). The review suggested that estrogensdecrease Na-K-ATPase in the brain and that astrocytesrely on active export of cellular sodium by the enzymein their adaptation to hyponatremia, citing an articlepublished in 1986; however, astrocytes are nowknown to volume regulate through loss of potassiumchloride and organic osmolytes and not by active
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 121

sodium transport (3–6). Importantly, there was nodifference between brain water and sodium contents inmale and female rats that were subjected to acute orchronic hyponatremia (7).
Exercise-Associated HyponatremiaExercise-associated hyponatremia (Na �135
mmol/L) is a potentially serious condition reportedinitially in ultraendurance athletes and more recentlyin marathon runners (8). Exercise-associated hypona-tremia was unknown before 1981, when recommen-dations for fluid intake during exercise were conser-vative; it first appeared after publication of a positionstatement advising athletes to drink as much as possi-ble during exercise (8,9). Athletes may drink largevolumes of water before exercise in an attempt to wardoff dehydration and, despite large fluid losses during arace, may drink enough fluid to gain weight. Occa-sionally, some athletes may drink up to 3 L/h in anattempt to produce dilute urine to escape detection ofbanned drugs in the urine. Although the dangers ofthese practices are now well recognized and have beenemphasized in the sports medicine community, someauthors suggested that excessive drinking is still beingpromoted by the global sports drink industry (9,10).
Hew-Butler et al. (11) conducted a comprehen-sive evaluation of the endocrine secretion of pituitary,natriuretic, and adrenal steroid hormones, as well ascytokines, in 82 well-trained endurance athletes im-mediately before and after running a 56-km ultramara-thon in Cape Town, South Africa. Plasma argininevasopressin (AVP) concentrations were markedly el-evated despite unchanged plasma sodium concentra-tions for the group as a whole, and AVP levels alsoincreased in those whose plasma sodium levels de-creased slightly. Mathematical pathway modeling at-tributed nonosmotic stimulation of AVP secretion todecreased plasma volume, with potential influencefrom brain natriuretic peptide, oxytocin, and cortico-sterone. A linear relationship was found between ex-ercise-induced plasma volume contraction (presum-ably related to sodium losses from sweat) and plasmaaldosterone, indicating that this provided an adequatestimulus to the volume-sensing baroreceptors that pro-voke AVP secretion. There was a statistically signifi-cant mathematical influence of plasma oxytocin onpostrace plasma AVP and plasma sodium levels inwomen but not in men. This finding is intriguingbecause female gender has been proposed as a risk
factor for morbidity associated with hyponatremia.Significant increases in IL-6 have been reported inrunners because actively contracting muscles produceIL-6. Because IL-6 stimulates AVP production innonexercising humans, IL-6 has been proposed as acause of inappropriate antidiuretic hormone secretionamong runners. The data of this study do not supportthis hypothesis, however, because higher IL-6 levelswere weakly associated with decreased plasma AVP.
A similar study of selected Boston marathonrunners also failed to show a correlation between IL-6and AVP levels (12). This study found that AVP wasmeasurable (�0.5 pg/ml) in seven of 16 runners whodeveloped hyponatremia during the race. Like theindividuals with detectable levels of AVP, individualswith hyponatremia and without measurable hormonedid not pass urine during the race, suggesting thatvasopressin levels were sufficient to impair maximalurine free-water excretion. The investigators sug-gested that in vitro proteolysis of AVP is the likelyexplanation for the negative findings in some speci-mens. Individuals with hyponatremia (Na �135mmol/L) had lower blood urea nitrogen levels thanindividuals with high serum sodium levels (�145mmol/L), supporting the hypothesis that exercise-in-duced hyponatremia is caused by fluid intake in excessof losses in the presence of antidiuresis provoked bythe nonosmotic secretion of AVP. Similar evidence fornonosmotic release of vasopressin was documentedamong cyclists who completed a 109-kg race (13).High-urine osmolalities and inappropriate plasmaAVP levels have been measured in athletes who werehospitalized with critical hyponatremia associatedwith exercise (10).
Chorley et al. (14) conducted a rigorous study of96 marathon runners who volunteered for a researchproject conducted during four Houston marathons.Eighty-seven percent of runners decreased their serumsodium during the race, and 22% had postrace values�135 mmol/L (range 130 to 134 mmol/L); none hadhyponatremic symptoms. Those who lost no weightwere significantly more likely to develop hyponatre-mia than those who did lose weight. Those who lost�0.75 kg were 7.03 times more likely to develophyponatremia than those who lost at least 0.75 kg.Fluid overconsumption was more likely among thosewho lost less fluid from sweating. Sweat rate is de-pendent on degree of acclimatization, gender (womensweat less), intensity of exercise, body weight (smaller
122 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

runners sweat less), environmental heat stress, andindividual variation. Runners with lower sweat rates(e.g., untrained, lightweight women running under coolerconditions) are more likely to consume more water thanthey lose, developing hyponatremia. Slower runnerswere more likely to drink more and more likely to sweatless. The authors proposed that runners who are slowerthan 5 h 10 min or �60 to 65 kg should be keenly awareof their risk for overconsumption and hyponatremia.Although women weighed less, had less weight loss,had less estimated sweat loss, and had slower finishtimes than men, female gender was not an independentfactor for hyponatremia or lower postrace plasmasodium concentration.
Changes in plasma sodium concentration duringexercise are determined by net water and net electro-lyte balance. Studies undertaken in the field cannotaccurately record electrolyte losses, which are likely tobe substantial; in a 90-km ultramarathon race, anathlete may lose approximately 8.6 L of sweat. Sweat-ing is a potential source of large sodium losses. Sweatgland adaptations can reduce these losses (15). Sweatglands consist of a secretory coil, which produces anisosmotic precursor sweat, and the reabsorptive duct,which actively reabsorbs salt from the precursorsweat. Sodium reabsorption occurs via an amiloride-sensitive sodium channel, and chloride uses the cysticfibrosis transmembrane conductance regulator on theluminal membrane. When sweat production is low,most of the sodium chloride is reabsorbed and veryhypotonic sweat appears at the skin surface; however,because the sodium chloride reabsorption rate is lim-iting, at high sweat rates, the sodium concentration ofthe sweat increases, exhibiting a linear relationshipwith the sweat rate. Acclimation to heat increases thereabsorptive capacity so that lower sodium concentra-tions occur at all sweating rates, but the linear rela-tionship between sweat rate and sodium concentrationremains. The mechanism for heat acclimation is un-known, but it is believed to involve aldosterone-me-diated increases in Na-K-ATPase and sodium channelsin the sweat gland reabsorption duct. Spironolactone(an aldosterone antagonist) increases sweat sodiumconcentration during heat acclimation. Lower sweatsodium concentrations decrease the likelihood of devel-oping hyponatremia during exercise. Patients with cysticfibrosis, who lack the chloride channel in the reabsorp-tive duct of the sweat gland, are predisposed to develop-ing hyponatremia when exposed to heat (16).
Baker et al. (17) conducted a rigorous balancestudy of volunteers who were subjected to treadmillexercise in the heat. Sodium and potassium losses inthe urine and in sweat were quantified, and sodiumand water intake were varied. The measured serumsodium concentrations (which ranged from 136 to 154mEq/L) were compared with what would be predictedfrom known empirical relationships between totalbody sodium and potassium and total body water usingthe “Nguyen-Katz” balance equation (18):
SNa � {[(SNai � 23.8)TBWi � 1.03 �E]/(TBWi � �TBW)} � 23.8
where SNa is the predicted serum sodium concentra-tion, SNa is the initial serum sodium concentration,�E is the net loss of sodium plus potassium, TBW isthe initial total body water (assumed to be 0.73 offat-free mass), and �TBW is the change in total bodywater taken to be the body weight change. Urinesodium losses were small during the 2-h experiment,averaging 6 to 11 mEq, but sweat sodium losses,averaging 112 to 150 mEq, had a significant effect onthe serum sodium concentration. The investigatorsfound that the Nguyen-Katz equation accurately pre-dicted the change in serum sodium concentration inthose whose fluid intake was adjusted so that theyeither maintained their weight or lost 2 or 4% of theirbody weight during exercise; however, when partici-pants overdrank relative to their sweat losses so as togain 2% of their body weight, the Nguyen-Katz equa-tion was not accurate; among runners who gainedweight, the serum sodium concentration did not fall asmuch as was predicted. By assuming that the bodyweight change reflects a change in total body water,this analysis ignores the release of bound water asglycogen is used for fuel; each kilogram of glycogencan contain upwards of 3 kg of associated water (8). Ifloss of body weight overestimates the loss of totalbody water, then the Nguyen-Katz equation shouldhave predicted sodium concentrations higher thanthose observed (the opposite of what occurred). Asnoted by the authors, delayed absorption of ingestedwater from the gastrointestinal tract would cause themeasured serum sodium to be higher than the pre-dicted value (as occurred among those who had todrink enough to exceed their urinary losses and gainweight). Other investigators have noted that maratho-ners who gain weight during a race do not uniformallydevelop hyponatremia; in one study, 70% of those
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 123

who overconsumed fluids maintained normal serumsodium concentrations despite external losses thatwould be expected to be substantial. As detailed in arecent review (8), some authors suggested that athletesare protected from developing hyponatremia becausethey are able to mobilize sodium from internal storesthat otherwise are osmotically inactive. Although thisis an intriguing possibility, that some athletes developmore hyponatremia than would be expected from theirweight change (which would have to be explained byosmotic inactivation of circulating sodium) seemsmore consistent with delayed absorption of ingestedwater and variability in the timing of blood samples.
There are conflicting data regarding nonsteroidalanti-inflammatory drug (NSAID) use as an importantpredisposing factor for exercise-associated hyponatre-mia. A prospective study of 131 of the 360 runnersentered in a 60-km mountain run in New Zealandassessed the effects of nonselective (NSAIDs andcyclooxygenase-2 (COX-2) selective nonsteroidal an-ti-inflammatory medication (COXIBs) in the inci-dence of exercise-associated hyponatremia (19). Fiveathletes developed hyponatremia (130 to 134 mmol/L). As in other studies, hyponatremia was associatedwith a mean weight gain of 1.32 kg (range �1.5 to 1.6kg), and serum sodium varied inversely with weightchange. Twenty percent of runners had used NSAIDsand 15% had taken COXIBs, whereas 65% did not useeither medication. There were no significant differ-ences between NSAID and COXIB users in any mea-sured parameters or between all NSAID and COXIBusers when compared with nonusers.
It is generally accepted that symptomatic patientswith exercise-induced hyponatremia are best treatedwith 3% saline. Siegel et al. (12) reported data fromtwo previously healthy women who were aged 24 and32 and collapsed while participating as charity fund-raisers in the 2002 Boston and Marine Corps mara-thons. After endotracheal intubation on arrival atemergency services, isotonic (0.9%) saline was ini-tially infused at 150 ml before serum [Na�] values of113 and 123 mmol/L were reported. Blood urea nitro-gen levels were �10 mg/dl, urine osmolalities were329 and 121 mOsm/kg H2O, and urine [Na�] was 81and 25 mEq/L, respectively. AVP and cortisol levelswere elevated and thyroid profiles were normal in bothcases, consistent with a diagnosis of syndrome ofinappropriate antidiuretic hormone secretion (SI-ADH). Computed tomography of the brain and chest
radiography showed diffuse cerebral and pulmonaryedema, and neither runner survived. By contrast, casesof hypotonic encephalopathy in the 2004 to 2005Marine Corps and Boston marathons were treated withintravenous infusions of hypertonic (3%) saline at arate of 1 ml/kg per h, resulting in an increase in serum[Na�] by 4 to 6 mmol/L during the first few hours;two severely affected runners whose encephalopathyrapidly improved without adverse effects were re-ported. The Second International Exercise-AssociatedHyponatremia (EAH) Consensus Development Con-ference convened in Queenstown, New Zealand (No-vember 2007). A panel of 18 international expertsrecommended that any athlete with hyponatremia andencephalopathy be immediately treated with a bolusinfusion of 100 ml of 3% NaCl to reduce brain edemaacutely with up to two additional 100-ml 3% NaClbolus infusions given at 10-min intervals if there is noclinical improvement. According to the consensus re-port, the first successful use of a bolus of hypertonicsaline was reportedly documented onsite in the 2005Two Oceans Marathon and subsequently in the TwinCities Marathon October 2005 in unpublished obser-vations. One published case report documented a rapidclinical response to the administration of 50 ml of 5%saline; however, the patient had only mild hyponatre-mia and mild symptoms (20).
Self-Induced Water Intoxication in PsychosisPolydipsia is common among institutionalized
psychotic patients, particularly among those with schizo-phrenia (21,22). Water intake can exceed normal excre-tory capacity, resulting in large diurnal weight gains andhyponatremia. One study reported a history of hypona-tremia among 11% of patients who were admitted to along-term care unit of a state psychiatric hospital. Self-induced water intoxication can occur despite an intactability to excrete maximally dilute urine, or it may beaccompanied by impaired water excretion as a result ofSIADH. Hallucinations with psychomotor agitation ordepression resembling delirious mania or catatoniacaused by acute hyponatremia may mimic primary psy-chiatric symptoms.
Several case reports have documented rhabdo-myolysis among patients with self-induced water in-toxication. A recent study from a single Japanesehospital found evidence of rhabdomyolysis in six(27.3%) of 22 psychotic patients who were hospital-ized for acute hyponatremia (mean maximum CK
124 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

level 104,638 IU; range 12,138 to 319,400 IU/L) (23).Two patients developed renal dysfunction with maxi-mum creatinine levels of 2.7 and 6.9 mg/dl (onerequired hemodialysis). One patient developed extrap-ontine myelinolysis. There were no deaths. Patientswho developed rhabdomyolysis had similar values forpresenting serum sodium (116.5 � 8.0 versus 119.6 �8.0 mEq/L) and were equally likely to have presentedwith seizures (one of six versus four of 16), alcoholintake before admission (one in each group), or over-dose of antipsychotic medications (one in each group);however, the six patients with rhabdomyolysis werecorrected more rapidly (2.0 � 1.3 versus 0.9 � 0.7;P � 0.017) and underwent a larger increase in serumsodium concentration in the initial 24 h (21.3 � 6.0versus 10.0 � 4.6 mEq/L; P � 0.001) despite beinggiven virtually identical amounts of sodium intrave-nously (117.7 � 20.3 versus 119.8 � 17.3 mEq).
Postoperative HyponatremiaVasopressin levels are increased for �2 d after
surgical procedures; therefore, hypotonic fluid admin-istration in the postoperative period risks acute iatro-genic hyponatremia. Postoperative hyponatremia is amajor problem in pediatric populations, for whomtraditional prescribing practices based on guidelinesdeveloped 50 yr ago still prevail in many medicalcenters (24). Because of postoperative deaths fromhyponatremia in young children, a nationwide educa-tional effort has been undertaken in the United King-dom to change prescribing practices; however, pre-scription of hypotonic fluid remains common. A cross-sectional survey of 17 English hospitals on all childrenwho received intravenous fluids during 1 d of a spec-ified week in December 2004 showed that 77 of 99children were given hypotonic solutions and 38%received �105% of fluid requirements; 21 of 86 chil-dren with available data had hyponatremia (25).
Fluid management of pediatric patients continuesto be guided by theoretical concerns that isotonicmaintenance fluids carry a risk for hypernatremia. Auet al. (26) conducted a retrospective analysis of 145postoperative admissions to a pediatric intensive careunit; 80% of patients had been given isotonic fluidpostoperatively, and 20% had been given hypotonicfluid (none more dilute than 0.3% saline). Moderatehyponatremia (�130 mEq/L) was found in 12 patientswho received hypotonic fluids (two were �125mEq/L) and in one patient who received isotonic fluid.
All of the patients with hyponatremia survived withoutsequelae. Among patients who received isotonic flu-ids, hypernatremia (145 to 159 mEq/L) developed in11 patients (an incidence of 7.5%) and hypernatremiadid not occur among patients who received hypotonicfluid. The authors concluded that they could not makea recommendation on the basis of these data andsuggested a controlled trial. A small, double-blind,randomized, controlled trial compared 0.9% salinewith 4% dextrose and 0.18% saline (dextrose saline),at either the traditional maintenance fluid rate or twothirds of that rate in 50 pediatric patients (37 surgical)and found a 3-mEq/L greater fall in sodium in patientswho received hypotonic fluid (27). The incidence ofhyponatremia was not significantly affected by thefluid administration rate.
References1. Ayus JC, Achinger SG, Arieff A: Brain cell volume regulation in
hyponatremia: Role of gender, age, vasopressin. and hypoxia. Am JPhysiol Renal Physiol 295: F619–F624, 2008
2. Sun XL, Ding JH, Fan Y, Zhang J, Gao L, Hu G: Aquaporin 4regulates the effects of ovarian hormones on monoamine neurotrans-mission. Biochem Biophys Res Commun 353: 457–462, 2007
3. Fisher SK, Cheema TA, Foster DJ, Heacock AM: Volume-dependentosmolyte efflux from neural tissues: Regulation by G-protein-cou-pled receptors. J Neurochem 106: 1998–2014, 2008
4. Vazquez-Juarez E, Ramos-Mandujano G, Hernandez-Benitez R, Pas-antes-Morales H: On the role of G-protein coupled receptors in cellvolume regulation. Cell Physiol Biochem 21: 1–14, 2008
5. Ringel F, Plesnila N: Expression and functional role of potassium-chloride cotransporters (KCC) in astrocytes and C6 glioma cells.Neurosci Lett 442: 219–223, 2008
6. Kimelberg HK: Supportive or information-processing functions ofthe mature protoplasmic astrocyte in the mammalian CNS? A criticalappraisal. Neuron Glia Biol 3: 181–189, 2007
7. Verbalis JG: Hyponatremia induced by vasopressin or desmopressinin female and male rats. J Am Soc Nephrol 3: 1600–1606, 1993
8. Rosner MH, Kirven J: Exercise-associated hyponatremia. Clin J AmSoc Nephrol 2: 151–161, 2007
9. Beltrami F, Hew-Butler T, Noakes T: Drinking policies and exercise-associated hyponatraemia: Is anyone still promoting overdrinking?Br J Sports Med 42: 496–501, 2008
10. Hew-Butler T, Ayus JC, Kipps C, Maughan RJ, Mettler S, Meeu-wisse WH, Page AJ, Reid SA, Rehrer NJ, Roberts WO, Rogers IR,Rosner MH, Siegel AJ, Speedy DB, Stuempfle KJ, Verbalis JG,Weschler LB, Wharam P: Statement of the Second InternationalExercise-Associated Hyponatremia Consensus Development Confer-ence, New Zealand, 2007. Clin J Sport Med 18: 111–121, 2008
11. Hew-Butler T, Jordaan E, Stuempfle KJ, Speedy DB, Siegel AJ,Noakes TD, Soldin SJ, Verbalis JG: Osmotic and nonosmotic regu-lation of arginine vasopressin during prolonged endurance exercise.J Clin Endocrinol Metab 93: 2072–2078, 2008
12. Siegel AJ, Verbalis JG, Clement S, Mendelson JH, Mello NK, AdnerM, Shirey T, Glowacki J, Lee-Lewandrowski E, Lewandrowski KB:Hyponatremia in marathon runners due to inappropriate argininevasopressin secretion. Am J Med 120: 461 e11–e17, 2007
13. Hew-Butler TD, Dugas JP, Noakes TD, Verbalis JG: Changes inplasma arginine vasopressin concentrations in cyclists participating
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 125

in a 109 km cycle race. Br J Sports Med July 15, 2008 [epub aheadof print]
14. Chorley J, Cianca J, Divine J: Risk factors for exercise-associatedhyponatremia in non-elite marathon runners. Clin J Sport Med 17:471–477, 2007
15. Buono MJ, Claros R, Deboer T, Wong J: Na� secretion rate in-creases proportionally more than the Na� reabsorption rate withincreases in sweat rate. J Appl Physiol 105: 1044–1048, 2008
16. Augusto JF, Sayegh J, Malinge MC, Illouz F, Subra JF, DucluzeauPH: Severe episodes of extra cellular dehydration: An atypical adultpresentation of cystic fibrosis. Clin Nephrol 69: 302–305, 2008
17. Baker LB, Lang JA, Kenney WL: Quantitative analysis of serumsodium concentration after prolonged running in the heat. J ApplPhysiol 105: 91–99, 2008
18. Kurtz I, Nguyen MK: A simple quantitative approach to analyzing thegeneration of the dysnatremias. Clin Exp Nephrol 7: 138–143, 2003
19. Page AJ, Reid SA, Speedy DB, Mulligan GP, Thompson J: Exercise-associated hyponatremia, renal function, and nonsteroidal antiinflam-matory drug use in an ultraendurance mountain run. Clin J Sport Med17: 43–48, 2007
20. Hew-Butler T, Anley C, Schwartz P, Noakes T: The treatment ofsymptomatic hyponatremia with hypertonic saline in an Ironmantriathlete. Clin J Sport Med 17: 68–69, 2007
21. Siegel AJ: Hyponatremia in psychiatric patients: Update on evalua-tion and management. Harv Rev Psychiatry 16: 13–24, 2008
22. Dundas B, Harris M, Narasimhan M: Psychogenic polydipsia review:Etiology, differential, and treatment. Curr Psychiatry Rep 9: 236–241, 2007
23. Morita S, Inokuchi S, Yamamoto R, Inoue S, Tamura K, Ohama S,Nakagawa Y, Yamamoto I: Risk factors for rhabdomyolysis inself-induced water intoxication (SIWI) patients. J Emerg Med April23, 2008 [epub ahead of print]
24. Moritz ML, Ayus JC: Hospital-acquired hyponatremia: Why arehypotonic parenteral fluids still being used? Nat Clin Pract Nephrol3: 374–382, 2007
25. Armon K, Riordan A, Playfor S, Millman G, Khader A: Hyponatrae-mia and hypokalaemia during intravenous fluid administration. ArchDis Child 93: 285–287, 2008
26. Au AK, Ray PE, McBryde KD, Newman KD, Weinstein SL, BellMJ: Incidence of postoperative hyponatremia and complications incritically-ill children treated with hypotonic and normotonic solu-tions. J Pediatr 152: 33–38, 2008
27. Yung M, Keeley S: Randomised controlled trial of intravenousmaintenance fluids. J Paediatr Child Health November 25, 2007[epub ahead of print]
Chronic Hyponatremia
EpidemiologyConclusions about costs and outcomes in hypo-
natremia are sometimes drawn from billing data, usingInternational Classification of Diseases, Ninth Revi-sion, Clinical Modification (ICD-9-CM) codes. Acomparison of inpatient hospital discharge recordswith inpatient laboratory data reported a sensitivity of30% for even the strictest definition of hyponatremia(�115 mmol/L). Because that study did not addressthe validity of coding for hyponatremia outside theinpatient setting, Shea et al. (1) sought to examine thevalidity of ICD-9-CM diagnosis codes for hyponatre-mia identification in an outpatient managed care pop-
ulation. Patients who were undergoing dialysis wereexcluded, and a correction factor for blood glucoses�300 mg/dl was used. A total of 40,668 outpatientserum sodium laboratory results were identified ashyponatremic (serum sodium �136 mmol/L). Thesensitivity of ICD-9-CM codes for hyponatremia inoutpatient professional claims within 15 d before orafter the laboratory date was 3.5%. Sensitivity valuesfor the �133 mmol/L, �130 mmol/L, and �125mmol/L strata were 7.5, 13.9, and 29.6%, respectively.The authors concluded that administrative claims arenot reliable for use in epidemiologic studies, even forpatients with severe hyponatremia.
Because only a small percentage of patients withhyponatremia receive an ICD-9-CM diagnosis codefor hyponatremia, the same group obtained the resultsof outpatient laboratory tests on patients who wereenrolled in �30 health insurance plans in the UnitedStates to determine the medical costs associated withhyponatremia (serum sodium �135 mmol/L) (2). Di-alysis patients and patients with serum creatinine �2.0mg/dl were excluded, and serum sodium concentra-tions were corrected for hyperglycemia (1.6 mg/dl forevery 100-mg/dl increase in blood sugar) when theblood glucose was �300 mg/dl. During the study period,there were 1274 (0.9%) patients with hyponatremia and3196 (1.9%) with hypernatremia. Controlling for age,gender, region, and comorbidities, hyponatremia was anindependent predictor of cost, increasing overall costs by41.2 to 45.7% and inpatient costs by 76.4 to 95.6%. Coststhat were associated with hypernatremia were not signif-icantly different from those that were incurred by patientswith normonatremia, and cost increases that were asso-ciated with hyponatremia were more than seven timesgreater than those that were associated with hypernatre-mia. Because these data were derived from an employer-based, commercially sponsored population and includedonly health plan members with laboratory data, they arenot necessarily generalizable: The elderly are likely tohave been underrepresented, as were patients withcomorbidities.
Zilberberg et al. (3) performed a retrospective co-hort study of hospitalized patients to quantify the effectof admission hyponatremia on hospital costs and out-comes. Data were derived from a large administrativedatabase with laboratory components, representing198,281 discharges from 39 US hospitals. The incidenceof hyponatremia (�135 mmol/L) at admission was 5.5%(n � 10,899). Patients with hyponatremia were older
126 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

(65.7 � 19.6 versus 61.5 � 21.8 yr; P � 0.001) and hada higher number of comorbidities than patients withnormonatremia. A higher proportion of patients withhyponatremia required intensive care (17.3 versus10.9%; P � 0.001) and mechanical ventilation (5.0versus 2.8%; P � 0.001) within 48 h of hospitalization.Hospital mortality (5.9 versus 3.0%; P � 0.001), meanlength of stay (8.6 versus 7.2 d; P � 0.001) and costs($16,502 versus $13,558; P � 0.001) were significantlygreater among patients with hyponatremia than thosewithout. After adjustment for confounders, hyponatremiawas independently associated with an increased need forintensive care unit care, mechanical ventilation, andhigher hospital mortality. The authors encouraged studiesto explore how prompt correction of admission hypona-tremia may affect these outcomes.
Differential Diagnosis of Chronic HyponatremiaBecause nearly all patients with chronic hypona-
tremia have an abnormality in free water excretion, thediagnostic approach to the electrolyte disturbanceseeks to define the cause of that abnormality. Exceptfor patients with severely compromised renal functionor impaired renal dilution caused by thiazide diuretics,impaired water excretion usually results from persis-tent secretion of vasopressin despite osmotic stimulithat would normally suppress secretion of the hormone.Vasopressin-mediated hyponatremia may result fromdisorders that decrease effective arterial blood volume(thereby provoking a hemodynamic stimulus for vaso-pressin secretion mediated by volume and pressure re-ceptors), or it may result from vasopressin secretion thatis independent of any hemodynamic stimulus. Hemody-namically mediated vasopressin secretion and hyponatre-mia occur in advanced heart failure and cirrhosis withascites; these conditions can be easily recognized clini-cally and are defined by sodium retention and edema.The greater diagnostic challenge comes with the distinc-tion between true hypovolemia caused by sodium deple-tion from euvolemic hyponatremia, often called the syn-drome of inappropriate antidiuretic hormone secretion(SIADH). Because the presence of antidiuretic hormonecannot always be proved in cases of euvolemic hypona-tremia, it has been suggested that a better term for thecondition is the syndrome of inappropriate antidiuresis(SIAD).
Several recent reviews summarized the currentstate of our knowledge in distinguishing between saltdepletion and SIAD. For diagnosing SIAD, the following
criteria are needed: (1) Hypo-osmolality, (2) urine that isless than maximally dilute (i.e., urine osmolality �100mOsm/kg), (3) absence of diuretics or clinical signs ofvolume depletion or edema, (4) urine sodium concentra-tion �30 mEq/L (some say �40 mEq/L on an adequatesodium intake), (5) reversal of “sodium wasting” andcorrection of hyponatremia with water restriction, and (6)absence of severely impaired renal function. Tradition-ally, a diagnosis of “SIADH” has required that hypothy-roidism and adrenal function be normal, a requirementbased on the Bartter and Schwartz criteria published in1967; however, as discussed here, patients with theseendocrine disturbances often present clinically with eu-volemic hyponatremia with all of the other features ofSIAD, and they are likely to respond to vasopressinantagonists. Similarly, there is disagreement as towhether to include drug-induced hyponatremia under theSIAD rubric. These distinctions are largely semantic.From a practical clinical standpoint, drug-induced hypo-natremia and hyponatremia caused by endocrine disor-ders should be part of the differential diagnosis of apatient who fulfills the biochemical and physical exam-ination criteria for SIAD.
It is sometimes difficult to distinguish SIADfrom hypovolemic hyponatremia on clinical groundsbecause the volume deficit in sodium-depleted patientshas usually been partially repaired by retained water.Physical findings are often nondiagnostic, andazotemia may be lacking. In two studies, approxi-mately half of the patients’ hypovolemic hyponatremiawas not diagnosed by history and physical examina-tion. The most definitive test for hypovolemic hypo-natremia is assessment of the response to isotonicsaline; by expanding the extracellular volume, vaso-pressin secretion is suppressed and the urine becomesdilute. The validity of laboratory tests that are used todistinguish between SIAD and hypovolemic hypona-tremia are best measured against this gold standard.
Spot urine samples reveal urine sodium concen-trations �30 mEq/L in most saline-responsive patientswith hyponatremia and �30 mEq/L in most patientswith SIAD; however, in older patients, who may beslower to adapt to hypovolemia with sodium retention,urine sodium concentrations may be as high as 50 to60 mEq/L in patients with volume depletion. Frac-tional excretion of sodium (FENa), which requiresmeasurement of the creatinine (creat) and sodium (Na)concentrations in concurrent urine (U) and plasma (P)samples may be helpful in these patients:
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 127

FENa � UNa/PNa/Ucreat/Pcreat
A FENa �0.5% supports a diagnosis of volumedepletion. The FENa can be supplemented with mea-surements of the fractional excretion (FE) of urea anduric acid, which requires the concurrent measurementof these substances in the plasma and urine. Thus, theFE of urea (FEurea) can be computed from the plasmaand urine urea concentrations as follows:
FEurea � Uurea/Purea/Ucreat/Pcreat
In a recent series of sodium-depleted patientswith hyponatremia, 30% had a UNa �30% (and there-fore might have received a misdiagnosis of SIAD). Allof these patients had a FENa �0.5%; however, 42% ofpatients with SIAD had a FENa �0.5%. Combineduse of FENa and FEurea was proposed, with FENa�0.5% and FEurea �55% defining SIAD; however, asubsequent study showed that these limits were unre-liable in patients with low urine outputs (defined byU/P creatine ratios �140). A FENa �0.15% or FEurea�45% in such patients identified those who wereunresponsive to isotonic saline.
As noted, the therapeutic response to isotonicsaline is the closest thing we have to a gold standard fora SIAD diagnosis. The distinction should not be basedsolely on the plasma sodium concentration (PNa) re-sponse to isotonic saline; in one study, 29% of patientswith sodium depletion failed to increase their PNa by �5mEq/L after 2 L of saline, whereas 30% of patients withSIAD did increase their PNa by �5 mEq/L. A rapidincrease in FENa to �0.5% after 2 L of isotonic sodiumwithout correction of PNa (or appropriate dilution of theurine) supports a SIAD diagnosis. The response of PNato isotonic saline is related to the baseline urine osmola-lity. Patients with a urine osmolality of approximately300 mOsm/kg increased their PNa after isotonic saline,whereas patients with a urine osmolality �530 mOsm/kgrespond with a decrease in PNa.
The fractional excretion of uric acid is higher inpatients with SIAD because of decreased proximaltubular reabsorption at presecretory and postsecretorysites. Plasma uric acid levels of �4 mg/dl and FEuricacid �12 or 16% have been proposed as criteria for aSIAD diagnosis; however, potomania, diuretics, andrenal salt wasting may duplicate these findings. Des-mopressin-induced hyponatremia increases FEuricacid to a much lower degree than as vasopressin-induced hyponatremia, suggesting that increased
FEuric acid in SIAD is mediated by V1 receptors. Thehigh FEuric acid in SIAD also is influenced by thechronicity of hyponatremia and the GFR.
SIAD versus Cerebral Salt WastingIn the early 1950s, before the pathophysiology of
SIAD was understood, a few patients who had neuro-logic disease and continued to excrete sodium in theirurine despite hyponatremia were reported; although thesepatients did not have hypotension, they were described ashaving “cerebral salt wasting” (CSW) (4). After thedescription of SIADH in 1957, urinary sodium losses inpatients with hyponatremia and neurologic disease weregenerally attributed to a physiologic response to an ex-panded intravascular volume caused by primary waterretention. In 1981, contracted isotopically measuredblood volumes were found in patients with hyponatremiaand subarachnoid hemorrhage, and the finding was at-tributed to CSW. The term CSW was resurrected primar-ily in the neurosurgery and critical care literature. Manyneurointensivists now accept that CSW is a common ifnot the most common cause of hyponatremia amongtheir patients (5–10).
To make a valid diagnosis of “salt wasting,”evidence of inappropriate urinary salt losses and areduced “effective arterial blood volume” is required(4,8). The CSW literature relies on several criteria forvolume depletion: Direct determinations of blood andplasma volume, negative sodium balance, clinical im-pressions, plasma levels of arginine vasopressin(AVP) and natriuretic peptides, and responses to ther-apy. As discussed in a recent editorial, none of thesemeasures can define hypovolemia unambiguously (4).
To make a valid diagnosis of “salt wasting,”evidence of inappropriate urinary salt lossesand a reduced “effective arterial blood vol-ume” is required. The literature on cerebralsalt wasting relies on several criteria for vol-ume depletion: Direct determinations ofblood and plasma volume, negative sodiumbalance, clinical impressions, plasma levelsof AVP and natriuretic peptides, and re-sponses to therapy. None of these measurescan define hypovolemia unambiguously.
Elevated levels of natriuretic peptides, ostensibly ofcerebral origin, have helped fuel the idea that hyponatre-
128 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

mia in neurologic disease is related to “salt wasting”;however, so-called brain natriuretic peptide usually is ofcardiac origin; in a recent study, jugular venous samplingin suspected CSW did not support cerebral release of thepeptide (11). Elevated natriuretic peptides are also con-sistent with a diagnosis of SIAD with secondary natri-uresis caused by volume expansion with water (12).Patients with subarachnoid hemorrhage or other acuteneurologic injuries respond with an increase in cat-echolamines, causing venoconstriction; as a result, thearterial circulation would be overfilled, leading to apressure natriuresis and a decrease in plasma volume.
Renin and aldosterone levels are low in patientswith purported CSW, a finding that could be a primarycause of salt wasting, but also could be a response toan overfilled circulation (4). Fludrocortisone has beenshown to be effective in decreasing urinary sodiumlosses and increasing the serum sodium concentrationin patients who have hyponatremia and are believed tohave CSW (13,14); however, parenteral preparationsof fludrocortisone are not available for clinical use. Ina series from Japan, where fludrocortisone was firstproposed as a therapy for CSW, 13 patients withtraumatic brain injury and hyponatremia that was re-sistant to sodium replacement (serum sodium 129.3 �1.5 mEq/L) were given high-dosage hydrocortisone(300 mg every 12 h) as a substitute for fludrocortisone;hyponatremia normalized over 2 d. Before hydrocor-tisone treatment, urinary sodium losses averaged563.5 � 95.9 mEq/d, and urine volume was 3.3 � 0.7L/d. After the hydrocortisone treatment, sodium ex-cretion fell significantly to 204.8 � 74.7 mEq/d, andurine volume fell significantly to 2.2 � 0.4 L/d.
To follow up these findings, the same group con-ducted a multicenter, randomized, placebo-controlledtrial of hydrocortisone (300 mg every 6 h for 10 d andthen tapered) given prophylactically to prevent hypona-tremia among patients with subarachnoid hemorrhage(15). Fluid intake was adjusted to achieve positive fluidbalance and to maintain central venous pressure within 8to 12 cmH2O. Seventy-one patients (placebo group n �36; hydrocortisone group n � 35) entered the study.Sodium excretion (P � 0.04), urine volume (P � 0.04),and the amount of fluid and orally ingested water werereduced in the group that received hydrocortisone. Theserum sodium concentration and plasma osmolarity weresignificantly higher in the hydrocortisone group (P �0.001), remaining above 140 mEq/L and approximately290 mOsm/kg; however, control subjects do not seem to
have developed hyponatremia. There was no significantdifference in the incidence of symptomatic cerebral va-sospasm or in overall outcome. Hyperglycemia, hypoka-lemia, and hypoproteinemia were significantly morecommon in the hydrocortisone group (P � 0.001); twopatients developed gastrointestinal hemorrhage and onedeveloped congestive heart failure in the hydrocortisonegroup. No patients had surgery or permanent sequelaebecause of adverse events. In our opinion, the investiga-tors have not shown that steroid therapy has significantadvantages over hypertonic saline given in adequatedosages.
Symptoms of Chronic HyponatremiaChronic hyponatremia should not be equated
with “asymptomatic” hyponatremia; a high percentage ofpatients with serum sodium concentrations �125mmol/L have symptoms of fatigue, vomiting, confusion,dysarthria, gait disturbances, or lethargy. Patients withchronic hyponatremia and very low serum sodium con-centrations or underlying neurologic conditions may oc-casionally present with seizures, stupor, or coma; how-ever, asymptomatic, mild chronic hyponatraemia is amore common finding and is associated with a risk forthe development of worsening hyponatraemia and moreserious neurologic symptoms. Even patients who seem tobe “asymptomatic” can be shown to be neurologicallyimpaired on formal testing.
In a 3-yr retrospective survey in a single hospital,Bissrum et al. (16) identified 31 patients who werehospitalized with neurologic symptoms attributable tohyponatremia (average serum sodium 118.8 mmol/L).A large majority (70.9%) of these patients had preex-isting untreated hyponatremia believed to be asymp-tomatic. The authors next investigated the prevalenceof presumed asymptomatic hyponatraemia in the out-patient setting. Of 27,496 patients analyzed, 14% hadserum sodium levels �134 mEq/L, and 4% had values�130 mEq/L.
“Asymptomatic” hyponatremia has been associ-ated with an increased risk for falls. Despite theabsence of clinically apparent symptoms, hyponatre-mia impairs performance on both attention and tandemgait tests to a similar degree as that produced by ablood alcohol level of 0.06%, and these tests arerestored to normal with correction of hyponatremia.These findings provide a rationale for therapeuticinterventions for all patients with hyponatremia, re-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 129

gardless of symptoms, with an attempt to maintain anear-normal serum sodium concentration.
Despite the absence of clinically apparentsymptoms, hyponatremia impairs perfor-mance on both attention and tandem gaittests to a similar degree as that produced bya blood alcohol level of 0.06%, and thesetests are restored to normal with correctionof hyponatremia. These findings provide arationale for therapeutic interventions for allpatients with hyponatremia, regardless ofsymptoms, with an attempt to maintain anear-normal serum sodium concentration.
Further support for therapeutic intervention wasprovided by a case-control study of 513 cases of bonefracture after falling in ambulatory patients who wereaged �65 yr and treated in a university hospital (17).The prevalence of hyponatremia (serum sodium �135mEq/L) among patients with bone fracture after fallingwas 13.06 versus 3.90% in age- and gender-matchedcontrol subjects. Hyponatremia was mild and asymp-tomatic in all patients (mean serum sodium 131 � 3mEq/L) and in most cases was drug induced (36%diuretics, 17% selective serotonin reuptake inhibitors)or from idiopathic SIADH (37%). Of the 67 patientswith hyponatremia and bone fractures, only one hadhyponatremia mentioned as a diagnosis in the medicalrecord or discharge summary; many were dischargedwith uncorrected hyponatremia, and 25% had no mea-surement of the serum sodium at discharge. Fourpatients with hyponatremia had recurrent bone frac-tures.
Beer PotomaniaHyponatremia has been observed in people who
drink large quantities of beer, so-called “beer potoma-nia.” Beer has a very low sodium and protein content;therefore, unless it is ingested with food, it provideslittle solute for excretion in the urine. The overall rateof solute excretion profoundly influences the capacityfor water excretion, because the urine flow rate equalsthe rate of solute excretion divided by the urine osmo-lality (18). For any given urine osmolality, soluteexcretion sets the ceiling for how much water isactually excreted. Normally, 50 to 100 mmol of urea isproduced each day by catabolism, and dietary protein
intake provides the rest; every 10 gm of protein pro-vides approximately 50 mmol of urea for excretion.On a salt- and protein-rich diet that provides 900mOsm of solute for excretion, 12 L of free water willbe cleared daily at a urine osmolarity (Uosm) of 60mOsm/L.
On a diet that consists primarily of beer thatprovides only 300 mOsm of solute for excretion, freewater clearance would be only 4 L/d. It should benoted that this calculation provides a value for freewater clearance, whereas electrolyte-free water clear-ance is a better predictor of the effect of urine outputon the plasma sodium concentration. Electrolyte-freewater clearance is calculated by replacing urine andplasma osmolarity with their concentrations of sodiumplus potassium. Because a beer diet contains littlesodium or potassium, the value for electrolyte-freewater would be closer to 5 L/d. Enthusiastic beerdrinkers can consume �5 L/d, exceeding urinary wa-ter losses, causing hyponatremia.
Traditionally, beer potomania is attributed tosolute-limited water excretion with normal dilutingability; however, a single observation that the urineosmolality is low may not accurately reflect whatoccurred during the development of hyponatremia.Sanghvi et al. (19) reported two beer drinkers who hadprofound hyponatremia (100 and 104 mmol/L) andinitially presented with inappropriately concentratedurine (218 and 547 mOsm/kg). After small amounts ofintravenous fluid, urine osmolalities fell to 48 and 71mOsm/kg, and a massive water diuresis emerged. Ifthe urine osmolalities had not been measured beforeintravenous fluid, then one could have concluded er-roneously that hyponatremia developed despite anintact ability to dilute the urine; hyponatremia mighthave been attributed to self-induced water intoxica-tion, with an acute onset and a well-tolerated rapidresolution of hyponatremia. In fact, beer drinkers usu-ally have chronic hyponatremia with transiently im-paired water excretion resulting from the nonosmoticrelease of vasopressin caused by volume depletionfrom gastrointestinal losses, alcohol withdrawal, nau-sea, or medications. A low solute intake and conse-quent limited delivery of the glomerular filtrate to thedistal nephron allows the urine to be concentrated atlow levels of vasopressin; the ability to dilute the urinemaximally can be restored with very little volumeresuscitation. A review of 20 previously publishedcases of hyponatremia that resulted from beer poto-
130 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

mania showed that only six included urine osmolalitymeasurements and three in which those values weremaximally dilute (19). Hyponatremia in these caseswas very severe (14 of 20 �110 mmol/L; eight of 20�105 mmol/L), and hypokalemia was frequent (13 of20 �3 mmol/L). Osmotic demyelination was docu-mented in one of the authors’ two cases (after correc-tion by 15 mmol/L in 24 h and 24 mmol/L in 48 h) andin at least three of the cases in the literature. Theauthors advocated matching urinary water losses withD5W to avoid excessive correction, a strategy that wassuccessful in one of their cases and unsuccessful inanother. Alternatively, urinary water losses could havebeen controlled by giving desmopressin; this strategyis discussed later in this section.
Drug-Induced HyponatremiaDrug-induced hyponatremia is becoming the most
common cause of hyponatremia seen in clinical practice.A host of drugs have been identified, and the subject hasbeen recently reviewed (20). Thiazide diuretics are themost common cause of community-acquired hyponatre-mia. Most patients are elderly with a female preponder-ance; individuals with a low body mass are most likely tobe affected. The pathophysiology is not completely un-derstood but includes sodium and potassium depletion,vasopressin-mediated water retention, transcellullar cat-ion exchange resulting from hypokalemia, magnesiumdepletion, and a direct effect of the diuretic on the renaldiluting site. Acute hyponatremia may be seen in indi-viduals who consume large amounts of water. Serum uricacid levels are often low, and thiazide-induced hypona-tremia may mimic SIAD; therefore, unless there is strongevidence to suggest an underlying SIAD cause, an ex-tensive diagnostic search for other causes should bepostponed for 2 to 3 wk. It should be remembered,however, that thiazides may aggravate hyponatremia thatis caused by other conditions.
Other than diuretics, drugs can impair renal di-lution by one of three basic mechanisms: Increasedcentral release of AVP, resetting the osmostat to lowerthe threshold for AVP secretion, or increased sensitiv-ity of the collecting duct to AVP. The various drugsthat commonly cause hyponatremia and their probableunderlying mechanisms are listed in Table 1.
Because they are used so commonly, selectiveserotonin reuptake inhibitors (SSRIs) have become themost important cause of drug-induced hyponatremiaother than thiazide diuretics. Older age and concomi-
tant use of diuretics are the most important risk fac-tors, and hyponatremia has been reported to affect upto 32% of susceptible individuals. Although hypona-tremia typically presents within the first 2 wk ofstarting therapy, one study showed that 29% of pa-tients who presented with SSRI-induced hyponatremiadid so �3 mo after starting the drug (21). The cause ofSSRI-induced SIAD is still unknown. Although thedrugs are thought to be highly selective in their effecton serotonin reuptake, there is some evidence that theyinhibit reuptake of dopamine and norepinephrine,which may induce AVP release (21). A high incidence
Table 1. Principal causes and underlying mechanismsof drug-induced SIAD
Increased hypothalamic vasopressin secretionantidepressants
SSRIsserotonin and norepinephrine reuptake inhibitorstricyclicsmonoamine oxidase inhibitors
antipsychotic agentsphenothiazinesbutyrophenones (haloperidol)
antiepileptic drugscarbamazepineoxcarbazepinesodium valproate
anticancer agentsvincristine and vinblastineintravenous cyclophosphamidemelphalanifosfamidemethotrexate
opiatesmiscellaneous
IFN-� and -�levamisolepentostatinmAb
Potentiation of vasopressin action on the collecting ductantiepileptic drugs
carbamazepinelamotrigine
intravenous cyclophosphamideantidiabetic drugs
chlorpropamidetolbutamide
nonsteroidal anti-inflammatory drugsDirect antidiuretic action
desmopressin (DDAVP)oxytocin (Pitressin)
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 131

of drug-induced SIAD with a rapid onset of hypona-tremia has been documented in patients treated withVenlafaxine, a serotonin and norepinephrine reuptakeinhibitor (21a). As with diuretics, younger patientswith psychogenic polydipsia may develop hyponatre-mia on SSRIs, and a history for excessive water orbeer drinking should be obtained before prescribingthese medications.
Carbamazepine is a widely known cause of hy-ponatremia and is thought to increase the sensitivity ofthe renal tubule to normal plasma levels of AVP, andanother antiepileptic drug, lamotrigine, has been re-ported to have a similar action; carbamazepine hasalso been reported to cause the reset osmostat variantof SIAD (20). Oxcarbazepine, which has a lowerincidence of drug interactions than carbamazepine, hascome into widespread use. The incidence of hypona-tremia resulting from oxcarbazepine was found to be9.2% (serum sodium 119 to 133 mEq/L) in a retro-spective study of 414 patients with epilepsy; serumsodium values �125 mEq/L were found in only twopatients (22)
Desmopressin, a selective vasopressin 2 (V2)receptor agonist, was recently used to treat nocturiaand the syndrome of nocturnal polyuria in both elderlyand pediatric patients (23,24). Multiple case reports ofsymptomatic hyponatremia in these patients have ap-peared in the literature. One study showed that amongpatients aged �65, a baseline serum sodium valuebelow normal carries a high risk for developing clin-ically relevant hyponatremia, even with oral desmo-pressin administration. As a result of concerns abouthyponatremia, the US Food and Drug Administration(FDA) published a warning about the use of desmo-pressin, particularly for primary nocturnal enuresistreatment in children. The FDA reported 61 cases ofhyponatremia-related seizures, two of which were fa-tal; 25 of these cases occurred in children. Manyaffected patients had been using other medications thataffect water excretion, primarily SSRIs and thiazidediuretics. Similarly, in 2007, several European Unioncountries decided to remove the indication of nocturiain the elderly for nasal formulations of desmopressinbecause of the increased risk for hyponatremia. Astudy of prescribing patterns in Sweden found amarked increase in filled prescriptions for desmopres-sin in patients who were older than 60 yr after the drugwas approved for enuresis treatment in that country in2002. More than half of patients who were given
desmopressin were also given other agents that areknown to increase the risk for hyponatremia, includingdiuretics, tricyclic antidepressants, SSRIs, chlorprom-azine, carbamazepine, loperamide, and nonsteroidalanti-inflammatory drugs (24).
Tumor-Associated HyponatremiaMost tumors that produce vasopressin ectopi-
cally are small cell lung cancers. Hyponatremia occursat presentation in small cell lung cancer in 15 to 30%of cases, whereas up to 70% of patients have increasedhigh levels of plasma vasopressin that normalize withtherapy. SIAD resulting from ectopic secretion ofvasopressin also occurs in patients with head and neckcancer. These tumors are usually located in the oralcavity and less often in the larynx, nasopharynx, hy-popharynx, nasal cavity, maxillary sinus, pharyngealspace, salivary glands, and oropharynx. Ectopic hor-mone secretion has been reported in a handful of othertumors, primarily in isolated case reports, includingolfactory neuroblastoma, small cell neuroendocrinecarcinomas, adenoid cystic carcinomas, and undiffer-entiated carcinomas and sarcomas. Antineoplastictherapy with vincristine, vinblastine, and cyclophos-phamide are widely known causes of hyponatremia,possibly because of cytotoxicity that affects paraven-tricular and supraoptic neurons. Cerebral metastasesfrom a variety of tumors may cause hyponatremia thathas been variably attributed to SIAD and cerebral saltwasting. Nephrotoxicity because of cisplatinum causesrenal salt wasting and hypovolemic hyponatremia.Hyponatremia with salt wasting can also be caused byadrenal metastases in advanced breast cancer, coloncancer, and adrenal lymphoma. Approximately onethird of patients with hyponatremia associated withsmall cell lung cancer have no evidence of ectopicvasopressin secretion and express atrial natriureticpeptide.
Occult neoplasms are sometimes found to be thecause of what seems to be “idiopathic” SIADH. Inmost cases, these tumors become apparent soon afterthe discovery of hyponatremia. Olfactory neuroblasto-mas, although rare, may present with SIADH and canremain occult for many years; particularly in youngpatients with “idiopathic” SIADH, an examination ofthe sinuses may be warranted (25).
PneumoniaThe association between pneumonia and hypo-
natremia was first described in 1962, but there have
132 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

been few studies to define this relationship. Nair et al.retrospectively reviewed a 342-patient cohort treatedin their hospital over 2 yr with data gathered as part ofa 2-yr project to develop a standardized community-acquired pneumonia order set (25a). Admission serumsodium concentrations ranged from 122 to 175 mEq/L,and 27.9% of patients had hyponatremia (�135 mEq/L). Patients with hypernatremic tended to be nursinghome residents, reflecting impaired thirst associatedwith advanced age and dementia. Hyponatremia oc-curred among patients who were not from nursinghomes and was equally common in men and women;it usually was mild on admission, but 4.1% of thecohort had admission serum sodium concentrations�130 mEq/L. Patients with hyponatremia had signif-icantly higher heart rate and white blood cell (WBC)count and were more likely to have a pneumoniaseverity index of 4 or 5, but, surprising, their arterialPO2 and oxygen saturation were nearly identical tothose of the patients with normonatremia. A heart rate�100 with a WBC count �15,000 carried a 48.9%likelihood of developing hyponatremia. Multivariateanalysis showed that hyponatremia severity index wasthe only independent risk predictor for hyponatremia.As has been true for many disorders, hyponatremiawas associated with longer hospital stays and hospitalmortality (9.5 versus 3.4%), most likely reflecting theseverity of the pneumonia rather than morbidity fromthe usually mild and asymptomatic hyponatremia. Be-tween the second and eighth hospital days, 10.5% ofpatients developed hyponatremia (122 to 135 mEq/L),and only nine patients with hospital-acquired hypona-tremia had sodium levels �130 mEq/L. Hospital-acquired hyponatremia was equally likely to occur inmen and women, was not related to the severity of thepneumonia or hypoxia, but was associated with thechoice of intravenous fluid; the incidence of hypona-tremia after use of isotonic fluid was 3.9 versus 14.5%with hypotonic fluid. It is interesting that patients whoreceived no intravenous fluid were nearly as likely asthose who received intravenous hypotonic fluid todevelop hyponatremia in the hospital.
A study of 108 children with community-ac-quired pneumonia of varying severity found a 45.4%incidence of hyponatremia (�135 mEq/L), which wasmild (�130 mEq/L) in 92% of cases. Patients withhyponatremic had higher temperature and WBC countthan patients with normonatremia and were morelikely to express inflammatory markers than those
with normonatremia. Hyponatremia did not affectlength of stay (26).
Endocrine DisordersData are conflicting regarding the incidence and
pathogenesis of hyponatremia in hypothyroidism(27,28). The appearance of hyponatremia during with-drawal of thyroid hormone replacement and resolutionof hyponatremia with thyroid replacement supports anetiologic role of hypothyroidism in the electrolytedisturbance. To improve uptake of radioactive iodinein thyroid carcinoma, levothyroxine is sometimeswithdrawn and a low-iodine diet is administered. Sha-kir et al. (27) reported five patients who had papillaryor follicular thyroid carcinoma and developed symp-tomatic hyponatremia during this maneuver. Baselineserum sodium levels had been normal before replace-ment therapy withdrawal. The patients presented witha variety of complaints, including weakness, dizziness,fainting spells, lethargy, and/or nausea in associationwith serum sodium concentrations ranging from 110 to121 mmol/L. Despite hyponatremia, the plasma reninactivity and serum aldosterone levels were suppressed,indicating volume expansion, consistent with a diag-nosis of SIAD. The hyponatremia responded to fluidrestriction and normalized after thyroid hormone re-placement. Lung or cerebral metastases (present infour of the patients) may have contributed to hypona-tremia.
Autoimmune polyendocrine syndrome type 2, orSchmidt syndrome, is characterized by the associationof autoimmune Addison disease with autoimmunethyroid disease and/or type 1 diabetes. When hypothy-roidism and hypoadrenalism coexist, hyponatremiaseems to be more severe than when either of thesediseases occur in isolation (29).
Hypopituitarism because of Sheehan syndromeoccurs as a result of ischemic pituitary necrosis fromsevere postpartum hemorrhage; it is more common indeveloping countries. Kurtulumus et al. (30) reportedfive elderly multiparous women (mean age 69; range62 to 78 yr) who had a history of complicated deliveryand presented with hyponatremia (serum sodium�128 mEq/L) as a result of previously undiagnosedSheehan syndrome (for up to 42 yr after the initialevent). Longstanding unrecognized Sheehan syn-drome was unmasked in one patient who developedhyponatremia (123 mEq/L) 2 d after treatment withpegylated interferon for hepatitis C (31).
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 133

Although Addison disease (combined aldoste-rone and cortisol deficiency) and hypopituitarism (iso-lated cortisol deficiency) are widely recognized causesof hyponatremia, isolated hypoaldosteronism is sel-dom mentioned as a cause. Talapatra et al. (32) re-ported on three patients who were aged 64 to 82 andpresented with hyponatremia (serum sodium 128, 116,and 117 mEq/L) and high-normal serum potassiumconcentrations (5.0 to 5.2 mEq/L). Renal function wasnear normal, urine osmolalities ranged from 370 to658, and urine sodium concentrations were 30, 128,and 170 mEq/L. The patients had normotension buthad orthostatic changes in BP, which in one case wassymptomatic. All patients had low plasma aldosteronelevels and normal cortisol levels; two patients had lowplasma renin values (the third was on lisinopril). Onlow dosages of fludrocortisone (50 to 100 �g/d), thepatients gained weight, postural changes in BP re-solved, serum potassium concentrations fell, and se-rum sodium concentrations returned to normal.
MeningitisHyponatremia is a frequent complication of bac-
terial meningitis (6). Brouwer et al. conducted a na-tionwide observational cohort study in the Netherlandsof 696 episodes of community-acquired acute bacterialmeningitis assessed prospectively in 671 patients(32a). The authors found a surprisingly benign prog-nosis. Hyponatremia was defined as mild (130 to 135)or severe (�130 mmol/L). Hyponatremia was presenton admission in 30% of patients and was classified assevere in 6%; the lowest serum sodium on admissionwas 120 mEq/L. Hyponatremia was significantly morecommon in Listeria meningitis (73%) than with otherinfecting organisms (in other series, comparably highrates of hyponatremia have been described in tubercu-lous and group A streptococcal meningitis, which wasnot encountered in this cohort) (33). Symptoms ofheadache, seizures, and impaired consciousness onadmission occurred with equal frequency among pa-tients with severe hyponatremia, mild hyponatremia,and normonatremia; however, a longer duration ofsymptoms (�24 h) was more common among patientswith hyponatremia. Cerebrospinal fluid opening pres-sures were measured in 216 of 696 patients, but therewas no association between high cerebrospinal fluidpressure and hyponatremia. Likewise, the proportionof patients with cerebral edema on computed tomog-raphy was similar among patients with and without
hyponatremia. During the clinical course, hyponatre-mia was seen in 27% of cases and was classified assevere in 6%; the proportion of patients with seizures,impaired consciousness, hydrocephalus, and stroke inpatients with normonatremia and patients with severeor mild hyponatremia was similar. Treatment for hy-ponatremia was given for 16 (29%) of 55 episodes ofsevere hyponatremia and 26 (13%) of 206 episodes ofmild hyponatremia. Despite this nonaggressive thera-peutic approach, hyponatremia resolved in 79% ofcases within 3 d, and neither mild nor severe hypona-tremia was associated with death or neurologic se-quelae.
Traumatic Brain InjuryHyponatremia has been shown to be a common
complication of traumatic brain injury, affecting 13.7to 33% of patients in two small published series. Moroet al. confirmed these findings in a retrospective anal-ysis of 298 patients who had traumatic brain injury andwere admitted during 12 mo to a single hospital inJapan; 50 (16.8%) developed hyponatremia (33b).Hyponatremia was not observed among the 63 patientswith cerebral concussion, the 49 patients with skullfracture, or the eight patients with traumatic subarach-noid hemorrhage; however, hyponatremia was com-mon among patients with cerebral contusion (n � 48[48%]), acute and chronic subdural hematoma (n � 16[25%] and n � 88 [16%]), and acute epidural hema-toma (n � 16 [25%]). Most patients developed hypo-natremia within 3 d of injury; however, some patientsdeveloped hyponatremia after 8 d. No patients devel-oped diabetes insipidus. Hyponatremia was associatedwith longer hospital stay (P � 0.001) and bad outcome(P � 0.02).
CirrhosisIn severe hepatic cirrhosis, reduced effective cir-
culating volume because of arterial splanchnic vaso-dilation leads to baroreceptor-mediated nonosmoticstimulation of vasopressin release and an impairedability to excrete electrolyte-free water (34). Reducedsodium delivery to the distal tubule because of a lowGFR and/or increase of proximal sodium reabsorptionadds to susceptibility to hyponatremia of patients withcirrhosis. The prevalence of hyponatremia (defined asa serum sodium �130 mmol/L) has been reported tobe 21.6% in patients with cirrhosis (35). Hyponatremiashould theoretically pose a risk to patients hyperam-
134 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

monemia, who often have low-grade cerebral edemabecause of glutamine accumulation in the brain. Con-sistent with this prediction, hyponatremia increases theprobability of developing hepatic encephalopathy. Hy-ponatremia also increases morbidity and mortalityfrom hepatic transplantation and is associated withosmotic demyelination in the postoperative periodbecause of the large increase in sodium concentrationassociated with the procedure (35).
When V2 receptor antagonists become clinicallyavailable, they may prove useful in hyponatremiamanagement among patients with cirrhosis. Gines etal. (36) conducted a multicenter, double-blinded, ran-domized, controlled trial that compared placebo withfixed dosages (5, 12.5, or 25 mg once daily) ofsatavaptan, a highly selective V2 receptor antagonist,in 110 patients with cirrhosis, ascites, and hyponatre-mia (serum sodium �130 mmol/L). Treatment contin-ued for 14 d, during which all patients continued toreceive spironolactone. Satavaptan improved the con-trol of ascites, reducing body weight and abdominalgirth significantly more than placebo. The serum so-dium concentration was significantly higher than pla-cebo in all treatment groups, and, at the highest dosageused (25 mg once daily), the serum sodium had in-creased by 6.6 � 4.3 mmol/L after 5 d versus 1.3 �4.2 mmol/L in control subjects. The number of pa-tients who showed an increase in serum sodium of �5mmol/L during the first 5 d ranged from 54 to 61% insatavaptan-treated patients and 18% in patients whoreceived placebo. Thirst was significantly more com-mon in the treatment groups, whereas the frequency ofother adverse effects did not differ from that of controlsubjects. The drug did not affect BP. In some patients,the increase in urine volume was striking. In fact, 11patients who were treated with satavaptan had urineoutputs of �5 L/d at some point during the study.There were no changes in serum creatinine concentra-tion in any of the satavaptan-treated patients comparedwith placebo. A rapid increase in serum sodium (de-fined as �8 mmol/L in this high-risk population) wasobserved in four of 28 patients who were given withplacebo and nine of 82 patients who were treated withconivaptan; no patient developed neurologic compli-cations.
Heart FailureHyponatremia is a common complication of left-
sided heart failure, and several studies have shown that
it is an independent mortality predictor (37–40).Gheorghiade et al. (37) followed patients who hadheart failure and were enrolled in a study of theeffectiveness of pulmonary catheterization (EvaluationStudy of Congestive Heart Failure and PulmonaryArtery Catheterization Effectiveness [ESCAPE]) for180 d after discharge to compare outcomes amongpatients with persistent hyponatremia (n � 71), cor-rected hyponatremia (n � 32), and normonatremia(n � 327). Patients with persistent hyponatremia had ahigher risk for postdischarge mortality and rehospital-ization for heart failure than patients with normonatre-mia despite similar clinical improvements (weightloss, improved symptoms, and hemodynamic chang-es); however, although there was a trend for improvedoutcomes in patients with corrected hyponatremiacompared with those with persistent hyponatremia,this did not reach statistical significance.
Patients who have heart failure and have hypo-natremia have higher circulating levels of neurohor-mones (catecholamines, renin, angiotensin II, aldoste-rone, and vasopressin) than individuals withnormonatremia and are more likely to have prerenalazotemia. It is therefore possible that hyponatremia issimply a marker of increased neurohormonal activa-tion and more severe disease. Conversely, it also ispossible that the volume regulatory responses of myo-cytes responding to hypotonicity might be maladaptiveor that vasopressin itself, through its action on cardiacand coronary V1a receptors, might have adverse ef-fects (41). Hyponatremia in heart failure is mediatedby vasopressin, and it responds to vasopressin antag-onists. The availability of orally active vasopressinantagonists has made it possible to conduct long-termoutcome studies to compare corrected with uncor-rected hyponatremia. In the acute and chronic thera-peutic impact of a vasopressin antagonist in chronicheart failure (ACTIV in CHF) study, there were nodifferences in 60-d outcomes in patients who had heartfailure and were treated with tolvaptan (a V2 receptorantagonist) compared with placebo. A post hoc anal-ysis of this study suggested that patients with correctedhyponatremia had a lower mortality compared withplacebo (42). At hospital discharge, 45 (66.2%) of 68patients with hyponatremia had improvements in se-rum sodium levels of �2 mEq/L. Patients who hadhyponatremia and whose serum sodium concentrationimproved had a mortality rate of 11.1% at 60 d afterdischarge, compared with a 21.7% mortality rate in the
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 135

17 patients with persistent hyponatremia; however, inthe much larger Efficacy of Vasopressin Antagonismin Heart Failure Outcome Study With Tolvaptan(EVEREST), 2072 patients who had heart failure andwere treated with tolvaptan had virtually identicalclinical outcomes (overall mortality, cardiovascularmortality, cardiovascular death or hospitalization, andworsening heart failure) compared with 2061 patientswho received placebo (43). Given that only 8% of thetrial’s study population had hyponatremia, however,the question of whether correction of hyponatremiawill improve prognosis in heart failure remains open.
Even if survival is not improved, patients withhyponatremia and heart failure are likely to benefit inother ways (subtly improved cognitive function and areduced risk for falls) from sustained normalization oftheir serum sodium concentration. Evidence of benefitfrom increased urine output in patients with normon-atremia and heart failure is unconvincing. Hyponatre-mia in right heart failure has received much lessattention. Forfia et al. (44) found that 13 of 40 patientswho had primary pulmonary hypertension and wereevaluated in a referral center had hyponatremia (mean132.4 � 4.4 mEq/L; range 119 to 136) at the time ofcardiac catheterization. Patients with hyponatremia(serum sodium �136 mEq/L) were significantly moresymptomatic, were more likely to be hospitalized, hadmore peripheral edema (69 versus 26%; P � 0.009),had higher hospitalization rates (85 versus 41%; P �0.009), and had higher right atrial pressure (14 � 6versus 9 � 3 mmHg; P � 0.001) than patients withnormonatremia. Patients with hyponatremia had a 10-fold higher mortality rate than patients with normon-atremia; all 10 patients with a serum sodium �135mEq/L died during the 2-yr follow-up, whereas nopatient with a serum sodium �140 mEq/L died. Di-uretic use had no bearing on the relationship betweenhyponatremia and outcome, and the prognostic signif-icance of hyponatremia persisted after adjustment forfunctional class, treatment status, and renal function,and it was independent of hemodynamic, echocardio-graphic, and clinical markers of poor outcome.
Treatment Options for Hypotonic HyponatremiaTreatment Goals. Although the treatment of hy-ponatremia has often been called “controversial,” ageneral consensus has emerged (45–53). There islongstanding agreement that the serum sodium con-centration should be increased rapidly among patients
who present with severe neurologic symptoms orwhose risk for herniation is high (e.g., a known acuteonset of hyponatremia, presence of intracranial pathol-ogy) and that this requires hypertonic saline adminis-tration. There is also general agreement that, espe-cially for patients with chronic hyponatremia, themagnitude of correction over 24 and 48 h should belimited to avoid iatrogenic injury.
There are still some differences in the details ofthese general principles. For clear-cut hyponatremicemergencies associated with acute hyponatremia,some authors recommended correction by 1 to 2mEq/L per h by infusing 3% saline at 1 to 2 ml/kg perh, whereas others advocated bolus infusions of hyper-tonic saline. Data from patients who had normonatre-mia and neurosurgical emergencies suggested that a5-mmol/L increase will reliably reverse impendingherniation (see the Hypernatremia section), and a rapidinfusion of hypertonic saline should cause a greaterincrease in sodium concentration of the arterial bloodperfusing the brain (51). Thus, the bolus strategy maymake the most sense. For patients who present withseizures, one group infuses 3 mmol of hypertonicNaCl per liter of total body water (3 ml/kg 3% salinein a young woman) per hour for 2 h (51). Even ifseizures have stopped, bolus infusion is still usedbecause of the risk that the serum sodium concentra-tion may fall: (1) Seizures are known to increasetransiently the plasma sodium concentration becauseof an internal water shift into muscle cells caused byan increase in intracellular solute, and there is a the-oretical risk that water might return to the plasma frommuscle cells postictally, lowering the plasma sodiumconcentration; and (2) in patients who have developedhyponatremia by drinking water rapidly (e.g., psy-chotic patients, runners, ecstasy users), delayed ab-sorption from the intestinal tract can lower the serumsodium concentration. Once the acute emergency hasbeen dealt with expeditiously and aggressively, thisgroup advocates limiting the overall daily correction to8 mmol/L, similar to the goal for patients with chronichyponatremia (51).
Although virtually all authors agree that overcor-rection of hyponatremia risks iatrogenic brain damage,there is not uniformity of opinion as to what overcor-rection is; however, differences seem to be narrowing.Whereas one author once suggested that correction ofhyponatremia was not harmful unless the increase inserum sodium concentration exceeded 25 mmol/L in
136 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

48 h, his more current recommendation is to limitcorrection over 48 h to 15 to 20 mmol/L (a standardthat is consistent with a 48-h limit of 18 mmol/Lsuggested by others) (52). Not all authors mention a24-h limit. Although this was once set at 12 mmol/Lper d, reports of osmotic demyelination at slower ratesof correction have led to recommendations for a 24-hlimit of 8 to 12 mmol/L (49). These should be re-garded as limits not to be exceeded rather than thera-peutic goals. To avoid overshooting the mark, a “tar-get” of 8 mmol/L per d has been suggested by severalauthors. For patients at high risk for osmotic demyeli-nation (patients with alcoholism, liver disease, or mal-nutrition), even slower daily rates of correction may beindicated.Water Restriction. Restriction of water intake canbe an effective treatment for mildly symptomaticchronic hyponatremia if there is enough electrolyte-free water excretion in the urine. Electrolyte-free wa-ter clearance is computed by multiplying the ratio ofsodium and potassium concentrations in the urine andplasma (the urine:plasma electrolyte ratio) by the urineflow rate. The urine:plasma electrolyte ratio alone ona spot urine sample (omitting urine output) is suffi-cient to estimate electrolyte-free water clearance . Ifthe ratio is 0.5, then electrolyte-free water clearance ishigh and the plasma sodium concentration can beexpected to increase acceptably if water is restricted; ifit is between 0.5 and 1.0, then electrolyte-free waterclearance is low but still positive, and, to be effective,water intake must be drastically reduced; if it is 1.0,then electrolyte-free water clearance is negative, theplasma sodium concentration may actually fall withoutintervention, and fluid restriction alone will be inef-fective (54).
Increasing solute intake may augment water re-striction’s effectiveness as a treatment for hyponatre-mia. A recent editorial review illustrated this pointusing patient data derived from the literature (18). Forexample, consider a patient who has a fixed urineosmolarity of 664 mOsm/L caused by SIAD becauseof lung cancer and whose diet provides 600 mOsm/dsolute. If the concentration of sodium plus potassiumin his urine were 166 mEq/L, then the urine-electrolyteratio would be �1.0 and hyponatremia will worsen nomatter how much fluid intake is restricted. Adminis-tering urea (or more dietary protein) to double soluteexcretion from 600 to 1200 mOsm/d would also dou-ble his urine flow, diluting the urine sodium and
potassium concentrations in half. As a result, electro-lyte-free water excretion becomes positive; however,large dietary protein intakes may not be achievable,and urea is not readily available as a therapeutic choicein North America; it may also not suit the NorthAmerican palate. Alternatively, a high salt intake com-bined with water restriction allows the electrolyteconcentration of what is ingested to match the elec-trolyte concentration of what is excreted in the urine.Combining a high salt intake with furosemide, whichdecreases urine osmolality, can be an effective strat-egy.Hypertonic Saline. Hypertonic saline has been usedto treat hyponatremia since the first description of itsuse in 1938; however, there is a paucity of data toguide clinicians. Dosing guidelines have thereforebeen derived from anecdotal clinical experience andphysiologic principles.
Most patients who are hospitalized for hypona-tremia have mild to moderate symptoms. If they havefeatures of SIAD and are expected to be or have beenshown to be resistant to isotonic saline, then adminis-tration of hypertonic saline may be indicated. Amongpatients with mildly symptomatic chronic hyponatre-mia, hypertonic saline can be infused at much slowerrates than are used for acute water intoxication. Aretrospective study of all 62 patients who had hypo-natremia and received hypertonic saline at a singlemedical center showed that despite a low rate ofinfusion (mean 23.5 ml/h, interquartile range 17.0 to32.2 ml/h), frequent adjustments in the rate of infu-sion, and in some cases administration of D5W as anantidote, the serum sodium concentration often in-creased by more than would be predicted and by morethan the prescribers intended: Correction exceeded 12mEq/L at 24 h in 11% of the cases, and 10% correctedby �18 mEq/L within 48 h (55). By hospital policy,all patients were treated under the supervision ofnephrologists who sought to maintain correction rateswithin these guidelines. The magnitude of correctionwithin 48 h was directly correlated with the plasmasodium concentration, with more severe hyponatremiaassociated with more rapid correction.
The Adrogue-Madias formula is widely used topredict the effect of an intravenous infusate on theserum sodium concentration (SNa):
� SNa after 1 L of infusate� (infusate [Na] � SNa)/(total body water � 1)
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 137

In patients with a plasma sodium concentration�120 mEq/L, the actual increase in plasma sodiumexceeded the increase predicted by the formula in 74%of the patients; the average ratio of actual to expectedwas 1.7 � 0.2, and actual correction was as much asfive times predicted. In approximately half the cases, adocumented water diuresis could account for the ex-cessive correction.
A number of conditions temporarily or reversiblyimpair water excretion. Once the impairment resolves,excretion of dilute urine increases the serum sodiumconcentration by much more than would be predictedby calculations that ignore urine output. Multifactorialcauses of hyponatremia are common, and it is oftendifficult to determine which factor is controlling or topredict which patients will respond to volume reple-tion, the passage of time, or discontinuation of medi-cations with a water diuresis. For example, Mohmandet al. (55) described an 87-yr-old who was takingthiazides (which would be expected to correct withvolume repletion) and was admitted with a serumsodium of 106 mEq/L 2 wk after starting an SSRIantidepressant (a common cause of drug-inducedSIAD). Despite stopping her medications and infusionof 0.9% saline with potassium supplements, the serumsodium increased by only 3 mEq/L during the first14 h and urine output was 60 ml/h; therefore, with theassumption that she had SIAD, 3% saline was pre-scribed at 20 ml/h. A few hours later, a water diuresisdeveloped with a urine osmolality of 90 mOsm/kg.Hypertonic saline was discontinued after 120 ml hadbeen administered (enough to increase the serum so-dium by a calculated 3 mEq/L); however, primarilybecause of the water diuresis, the serum sodium in-creased 15 mEq/L in 18 h. Drescher et al. (56) de-scribed a similar patient who presented with seizures,a serum sodium of 100 mmol/L, urine osmolality of271, and urine sodium of 39 mmol/L (Figure 2). ASIAD diagnosis prompted administration of 3% saline;however, in the first hour of the infusion, the urineoutput increased to 750 ml/h and urine osmolality fellto 68 mOsm/kg. Despite stopping hypertonic salineand infusing D5W, the serum sodium concentrationcontinued to increase. As more history emerged, in-vestigators learned that the patient was psychotic andhad been drinking large volumes of water while takingthiazide diuretics. Her transiently concentrated urineon presentation was attributed to an effect of her
seizure or nausea or might also have reflected an effectof thiazides.
Vasopressin Receptor Antagonists. The main ef-fects of AVP on water balance are mediated throughV2 receptors in the renal collecting ducts. Stimulationof V2 receptors upregulates renal expression of aqua-porin 2 water channels and initiates their insertion intothe cellular membranes of the renal collecting duct,increasing water reabsorption. AVP also affects vas-cular tone and platelet activity by stimulating V1A
receptors. Vasopressin receptor antagonists, collec-tively known as the “vaptans,” provide a new ap-proach to the treatment of hyponatremia. Anticipationof the availability these agents has sparked the publi-cation of several recent reviews, including an editorialin the last fluid and electrolyte edition of NephSAP(48,54,57).
Conivaptan, which blocks both the V2 and V1A
receptors, is currently the only drug of its class avail-able for use in the United States, although mozavaptanhas been approved for use in paraneoplastic SIADH inJapan. In humans, 99% of conivaptan is bound byplasma proteins, over a wide plasma concentrationrange. A potent inhibitor of CYP3A4, conivaptaninteracts with many medications, including the statins
Figure 2. An example of a reversible defect in waterexcretion. A young woman with severe hyponatremia (se-rum sodium 100 mmol/L) and seizures associated withpreviously unrecognized polydipsia and thiazides. The ini-tial laboratory data suggest SIAD, but after receiving 70 mlof 3% saline over 1 h, the urine became dilute and the serumsodium concentration increased by more than intended de-spite an attempt to replace urine losses with 5% dextrose inwater. Reprinted with permission from Elsevier (The Lan-cet, 2008, Vol 371, page 2144; ref. 59).
138 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

(simvastatin, lovastatin, atorvastatin, rosuvastatin, ke-toconazole, itraconazole, clarithromycin, ritonavir,and indinavir). Because of concern about seriousdrug–drug interactions if the drug were used for pro-longed periods, the FDA approved only the intrave-nous form of conivaptan for the short-term manage-ment of euvolemic hyponatremia and hyponatremiabecause of heart failure in hospitalized patients.Conivaptan is contraindicated in hypovolemic hypo-natremia (because the antagonism of the V1A receptorcould cause hypotension) and in patients with hypo-natremia caused by cirrhosis with ascites (for fear ofprecipitating hepatorenal syndrome, a disorder ame-liorated by agonists of the V1A receptor). A number oforally active V2 receptor antagonists are in clinicaltrials and may potentially be approved for outpatienttreatment of hyponatremia.
As yet, there is little published experience withconivaptan, currently the only FDA approved vaptan.Zeltser et al. (58) conducted a placebo-controlled trialof 84 hospitalized patients with euvolemic or hyper-volemic (congestive heart failure) hyponatremia (se-rum sodium 115 to �130 mmol/L). Patients wereassigned to receive intravenous placebo or conivaptanadministered as a 30-min, 20-mg loading dose fol-lowed by a 4-d continuous infusion of either 40 or 80mg/d conivaptan. Conivaptan significantly increasedthe plasma sodium concentration by a variety of mea-sures over placebo, and it increased electrolyte-freewater clearance, whereas placebo did not. The drugwas generally well tolerated, although infusion-sitereactions led to the withdrawal of 3% of patients whowere given the 40-mg dose and 15% of patients whowere given the 80-mg dose. As would be expected fora V1A receptor antagonist, conivaptan infusion at ei-ther dosage was associated with significant but clini-cally unimportant changes in supine systolic and dia-stolic BP, and postural hypotension occurred in five of55 patients who received conivaptan and none of the29 patients who received placebo. Two patients ineach of the groups given conivaptan—but none in theplacebo group—experienced excessive correction ofhyponatremia (at 40 mg/d 13 mmol/L over 24 h and 8mmol/L over 4 h; at 80 mg/d 25 mmol/L over 24 h and12 mmol/L after 24 h); overcorrection did not lead toneurologic symptoms suggestive of osmotic demyeli-nation. Verbalis et al. (59) conducted a subgroupanalysis of the 56 patients who had euvolemic hypo-natremia (SIAD) and participated in the original trial.
All but one of the 19 patients who received conivaptanhad significantly higher serum sodium concentrationsthan placebo after the first day of therapy, and theseaveraged 5.70 � 0.90 mEq/L in the 40-mg/d groupand 6.40 � 0.95 mEq/L in the 80-mg/d group. Onlyone patient in the subgroup experienced excessivecorrection (12 mmol/L over 24 h). The authors sug-gested that 4 d of intravenous conivaptan could be auseful therapy for patients who are hospitalized withtransient SIAD, as seen with surgical procedures,acute pneumonia, respiratory failure, or subarachnoidhemorrhage. More data are needed for patients withsubarachnoid hemorrhage; if, as is commonly be-lieved, these patients have hypovolemia because ofcerebral salt wasting, then the hypotensive effect ofthe drug could adversely affect cerebral perfusion. Ifthe drug were combined with isotonic saline, however,then this theoretical risk could be avoided.
Rianthorn et al. reported a novel use of conivaptanin a 13-yr-old patient who had SIAD associated withan anaplastic large cell lymphoma and required largevolumes of intravenous fluid to prevent tumor lysissyndrome (59a). The increase in free water clearanceallowed the administration of isotonic saline at 3 L/m2
per d, and the serum sodium concentration increasedfrom 121 to 129 mmol/L over 24 h.
Vaptans are a welcome addition to our therapeu-tic armamentarium. They make it possible to treatpatients who have hyponatremia and heart diseasewithout saline, and they will greatly simplify outpa-tient treatment of hyponatremia. For patients withseizures or coma, hypertonic saline remains the drugof choice. There has been no experience with givinghypertonic saline and vaptans together, but this is atheoretically attractive maneuver. For patients withmoderate neurologic symptoms from severe hypona-tremia, vaptans are an option, but they must be usedwith caution to avoid overcorrection. Clinicians whouse these agents must focus their attention on the urineoutput and must be prepared to replace urinary waterlosses when therapeutic goals have been reached.Desmopressin for Overcorrection. As discussedearlier, a water diuresis often emerges during thetreatment of hyponatremia, risking inadvertent over-correction. There are several settings in which this canoccur: (1) Volume resuscitation in patients with excessvasopressin because of hypovolemia or low soluteintakes; (2) discontinuation of thiazide diuretics ordrugs that cause SIAD; (3) cortisol replacement in
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 139

patients with adrenal insufficiency; and (4) spontane-ous resolution of a reversible cause of SIAD, such asnausea, hypoxia, or recent surgery. In three separatecase reports of individual patients, desmopressin wassuccessfully used therapeutically to relower the serumsodium concentration after inadvertent overcorrectionof hyponatremia and the onset of symptoms suggestiveof osmotic demyelination. Perianayagam et al. (60)reported their experience with desmopressin in 20patients as a therapeutic agent to avoid overcorrectionof hyponatremia and to relower the plasma sodiumconcentration after inadvertent overcorrection beforesymptoms of osmotic demyelination could appear.Hyponatremia was multifactorial in most cases, and,with few exceptions, the cause of water retention waseliminated during the course of hospitalization; thia-zide diuretics and SSRIs, alone or in combination,were causative factors in 11 cases. Six patients weregiven desmopressin acetate as a rescue maneuver afterthe 24-h limit of 12 mmol/L had already been reachedor exceeded; correction was prevented from exceedingthe 48-h limit of 18 mmol/L in five of the six (theexception had exceeded the goal before desmopressinwas given). Fourteen patients were given desmopres-sin acetate in anticipation of overcorrection after theplasma sodium concentration had increased by 1 to 12mmol/L. In all 14 patients who were treated withdesmopressin acetate as a preventive measure, correc-tion was prevented from exceeding either the 24- or48-h limit. After desmopressin acetate was adminis-tered, the plasma sodium concentration of 14 of the 20patients fell by 2 to 9 mmol/L. In all six patients whowere treated after overcorrection and five patients whowere treated prophylactically, the plasma sodium con-centration was actively lowered again by the concur-rent administration of desmopressin acetate and 5%dextrose in water; no serious adverse consequencesfrom this maneuver were observed. In most cases,desmopressin was administered subcutaneously or in-travenously in 1- or 2-�g doses. The authors recom-mended a dosing interval of 6 to 8 h to avoid escapefrom the drug and the unwanted reemergence of awater diuresis.
References1. Shea AM, Curtis LH, Szczech LA, Schulman KA: Sensitivity of
International Classification of Diseases codes for hyponatremiaamong commercially insured outpatients in the United States. BMCNephrol 9: 5, 2008
2. Shea AM, Hammill BG, Curtis LH, Szczech LA, Schulman KA:
Medical costs of abnormal serum sodium levels. J Am Soc Nephrol19: 764–770, 2008
3. Zilberberg MD, Exuzides A, Spalding J, Foreman A, Jones AG,Colby C, Shorr AF: Epidemiology, clinical and economic outcomesof admission hyponatremia among hospitalized patients. Curr MedRes Opin 24: 1601–1608, 2008
4. Sterns RH, Silver SM: Cerebral salt wasting versus SIADH: Whatdifference? J Am Soc Nephrol 19: 194–196, 2008
5. Brimioulle S, Orellana-Jimenez C, Aminian A, Vincent JL: Hypona-tremia in neurological patients: Cerebral salt wasting versus inappro-priate antidiuretic hormone secretion. Intensive Care Med 34: 125–131, 2008
6. Cerda-Esteve M, Cuadrado-Godia E, Chillaron JJ, Pont-Sunyer C,Cucurella G, Fernandez M, Goday A, Cano-Perez JF, Rodriguez-Campello A, Roquer J: Cerebral salt wasting syndrome: Review. EurJ Intern Med 19: 249–254, 2008
7. Vespa P: Cerebral salt wasting after traumatic brain injury: Animportant critical care treatment issue. Surg Neurol 69: 230–232,2008
8. Rivkees SA: Differentiating appropriate antidiuretic hormone secre-tion, inappropriate antidiuretic hormone secretion and cerebral saltwasting: The common, uncommon, and misnamed. Curr Opin Pedi-atr 20: 448–452, 2008
9. Lu DC, Binder DK, Chien B, Maisel A, Manley GT: Cerebral saltwasting and elevated brain natriuretic peptide levels after traumaticbrain injury: 2 case reports. Surg Neurol 69: 226–229, 2008
10. Brimioulle S, Orellana-Jimenez C, Aminian A, Vincent JL: Hypona-tremia in neurological patients: Cerebral salt wasting versus inappro-priate antidiuretic hormone secretion. Intensive Care Med 34: 125–131, 2008
11. Powner DJ, Hergenroeder GW, Awili M, Atik MA, Robertson C:Hyponatremia and comparison of NT-pro-BNP concentrations inblood samples from jugular bulb and arterial sites after traumaticbrain injury in adults: A pilot study. Neurocrit Care 7: 119–123,2007
12. Coenraad MJ, Bolk JH, Frolich M, Meinders AE: Plasma argininevasopressin and atrial natriuretic peptide concentration in patientswith hyponatremia at diagnosis and following treatment. Eur J InternMed 18: 221–229, 2007
13. Papadimitriou DT, Spiteri A, Pagnier A, Bayle M, MischalowskiMB, Bourdat G, Passagia JG, Plantaz D, Bost M, Garnier PE:Mineralocorticoid deficiency in post-operative cerebral salt wasting.J Pediatr Endocrinol Metab 20: 1145–1150, 2007
14. Lee P, Jones GR, Center JR: Successful treatment of adult cerebralsalt wasting with fludrocortisone. Arch Intern Med 168: 325–326,2008
15. Katayama Y, Haraoka J, Hirabayashi H, Kawamata T, Kawamoto K,Kitahara T, Kojima J, Kuroiwa T, Mori T, Moro N, Nagata I, OgawaA, Ohno K, Seiki Y, Shiokawa Y, Teramoto A, Tominaga T,Yoshimine T: A randomized controlled trial of hydrocortisoneagainst hyponatremia in patients with aneurysmal subarachnoid hem-orrhage. Stroke 38: 2373–2375, 2007
16. Bissram M, Scott FD, Liu L, Rosner MH: Risk factors for symptom-atic hyponatraemia: The role of pre-existing asymptomatic hy-ponatraemia. Intern Med J 37: 149–155, 2007
17. Gankam Kengne F, Andres C, Sattar L, Melot C, Decaux G: Mildhyponatremia and risk of fracture in the ambulatory elderly. QJM101: 583–588, 2008
18. Berl T: Impact of solute intake on urine flow, water excretion. J AmSoc Nephrol 19: 1076–1078, 2008
19. Sanghvi SR, Kellerman PS, Nanovic L: Beer potomania: An unusualcause of hyponatremia at high risk of complications from rapidcorrection. Am J Kidney Dis 50: 673–680, 2007
20. Liamis G, Milionis H, Elisaf M: A review of drug-induced hypona-tremia. Am J Kidney Dis 52: 144–153, 2008
21. Ozturk S, Ozsenel EB, Kazancioglu R, Turkmen A: A case of
140 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

fluoxetine-induced syndrome of inappropriate antidiuretic hormonesecretion. Nat Clin Pract Nephrol 4: 278–282, 2008
21a. Roxanas M, Hibbert E, Field M: Venlafaxine hyponatraemia: inci-dence, mechanism and management. Aust N Z J Psychiatry 41:411–418, 2007
22. Ortenzi A, Paggi A, Foschi N, Sabbatini D, Pistoli E: Oxcarbazepineand adverse events: Impact of age, dosage, metabolite serum concen-trations and concomitant antiepileptic therapy. Funct Neurol 23:97–100, 2008
23. Kujubu DA, Aboseif SR: An overview of nocturia and the syndromeof nocturnal polyuria in the elderly. Nat Clin Pract Nephrol 4:426–435, 2008
24. Ljung R: Use of desmopressin and concomitant use of potentiallyinteracting drugs in elderly patients in Sweden. Eur J Clin Pharmacol64: 439–444, 2008
25. Renneboog B, Decaux G: Idiopathic hyponatremia in a young pa-tient: Look at the sinus. Am J Med 121: e5–e6, 2008
25a. Nair V, Niederman MS, Masani N, Fishbane S: Hyponatremia incommunity-acquired pneumonia. Am J Nephrol 27: 184–190, 2007
26. Don M, Valerio G, Korppi M, Canciani M: Hyponatremia in pediatriccommunity-acquired pneumonia. Pediatr Nephrol 23: 2247–2253,2008
27. Shakir MK, Krook LS, Schraml FV, Hays JH, Clyde PW: Symptom-atic hyponatremia in association with a low-iodine diet and levothy-roxine withdrawal prior to i(131) in patients with metastatic thyroidcarcinoma. Thyroid 18: 787–792, 2008
28. Krishnamurthy VR, McDougall IR: Severe hyponatremia: A dangerof low-iodine diet. Thyroid 17: 889–892, 2007
29. Wehbe E, Grant ME: Severe hyponatremia and Schmidt’s syndrome.Clin Exp Nephrol 12: 211–214, 2008
30. Kurtulmus N, Yarman S: Hyponatremia as the presenting manifes-tation of Sheehan’s syndrome in elderly patients. Aging Clin Exp Res18: 536–539, 2006
31. Kanda K, Kayahara T, Seno H, Yamashita Y, Chiba T: Conversionfrom latent to symptomatic Sheehan’s syndrome by pegylated inter-feron therapy for chronic hepatitis C. Intern Med 47: 939–941, 2008
32. Talapatra I, Kalavalapalli S, Tymms DJ: Isolated hypoaldosteronism:An overlooked cause of hyponatraemia. Eur J Intern Med 18:246–248, 2007
32a. Brouwer MC, van de Beek D, Heckenberg SG, Spanjaard L, de GansJ: Hyponatraemia in adults with community-acquired bacterial men-ingitis. Qjm 100: 37–40, 2007
32b. Moro N, Katayama Y, Igarashi T, Mori T, Kawamata T, Kojima J:Hyponatremia in patients with traumatic brain injury: incidence,mechanism, and response to sodium supplementation or retentiontherapy with hydrocortisone. Surg Neurol 68: 387–393, 2007
33. Roca B, Tornador N, Tornador E: Presentation and outcome oftuberculous meningitis in adults in the province of Castellon, Spain:A retrospective study. Epidemiol Infect 136: 1455–1462, 2008
34. Schrier RW: Decreased effective blood volume in edematous disor-ders: What does this mean? J Am Soc Nephrol 18: 2028–2031, 2007
35. Gines P, Cardenas A: The management of ascites and hyponatremiain cirrhosis. Semin Liver Dis 28: 43–58, 2008
36. Gines P, Wong F, Watson H, Milutinovic S, del Arbol LR, OlteanuD: Effects of satavaptan, a selective vasopressin V(2) receptor an-tagonist, on ascites and serum sodium in cirrhosis with hyponatremia:A randomized trial. Hepatology 48: 204–213, 2008
37. Gheorghiade M, Rossi JS, Cotts W, Shin DD, Hellkamp AS, Pina IL,Fonarow GC, DeMarco T, Pauly DF, Rogers J, DiSalvo TG, ButlerJ, Hare JM, Francis GS, Stough WG, O’Connor CM: Characteriza-tion and prognostic value of persistent hyponatremia in patients withsevere heart failure in the ESCAPE Trial. Arch Intern Med 167:1998–2005, 2007
38. Ghali JK: Mechanisms, risks, and new treatment options for hypo-natremia. Cardiology 111: 147–157, 2008
39. Gheorghiade M, Abraham WT, Albert NM, Gattis Stough W, Green-
berg BH, O’Connor CM, She L, Yancy CW, Young J, Fonarow GC:Relationship between admission serum sodium concentration andclinical outcomes in patients hospitalized for heart failure: An anal-ysis from the OPTIMIZE-HF registry. Eur Heart J 28: 980–988,2007
40. Tribouilloy C, Rusinaru D, Mahjoub H, Souliere V, Levy F, PeltierM, Slama M, Massy Z: Prognosis of heart failure with preservedejection fraction: A 5 year prospective population-based study. EurHeart J 29: 339–347, 2008
41. Chen SY, Abrahams Z, Sokos GG, Mullens W, Hobbs R, Taylor DO,Gonzalez-Stawinski GV: Conivaptan: Potential therapeutic implica-tions in heart failure. Recent Patents Cardiovasc Drug Discov 3:137–140, 2008
42. Rossi J, Bayram M, Udelson JE, Lloyd-Jones D, Adams KF, OconnorCM, Stough WG, Ouyang J, Shin DD, Orlandi C, Gheorghiade M:Improvement in hyponatremia during hospitalization for worseningheart failure is associated with improved outcomes: Insights from theAcute and Chronic Therapeutic Impact of a Vasopressin Antagonistin Chronic Heart Failure (ACTIV in CHF) trial. Acute Card Care 9:82–86, 2007
43. Konstam MA, Gheorghiade M, Burnett JC Jr, Grinfeld L, MaggioniAP, Swedberg K, Udelson JE, Zannad F, Cook T, Ouyang J, ZimmerC, Orlandi C: Effects of oral tolvaptan in patients hospitalized forworsening heart failure: The EVEREST Outcome Trial. JAMA 297:1319–1331, 2007
44. Forfia PR, Mathai SC, Fisher MR, Housten-Harris T, Hemnes AR,Champion HC, Girgis RE, Hassoun PM: Hyponatremia predicts rightheart failure and poor survival in pulmonary arterial hypertension.Am J Respir Crit Care Med 177: 1364–1369, 2008
45. Hoorn EJ, Zietse R: Hyponatremia revisited: Translating physiologyto practice. Nephron Physiol 108: 46–59, 2008
46. Decaux G: V2-antagonists for the treatment of hyponatraemia. Neph-rol Dial Transplant 22: 1853–1855, 2007
47. Verbalis JG, Goldsmith SR, Greenberg A, Schrier RW, Sterns RH:Hyponatremia treatment guidelines 2007: Expert panel recommen-dations. Am J Med 120: S1–S21, 2007
48. Gross P: Treatment of hyponatremia. Intern Med 47: 885–891, 200849. Ellison DH, Berl T: Clinical practice: The syndrome of inappropriate
antidiuresis. N Engl J Med 356: 2064–2072, 200750. Adrogue HJ, Madias NE: Hyponatremia. N Engl J Med 342: 1581–
1589, 200051. Halperin ML, Kamel KS: A new look at an old problem: Therapy of
chronic hyponatremia. Nat Clin Pract Nephrol 3: 2–3, 200752. Moritz ML, Ayus JC: Hospital-acquired hyponatremia: Why are
hypotonic parenteral fluids still being used? Nat Clin Pract Nephrol3: 374–382, 2007
53. Hew-Butler T, Ayus JC, Kipps C, Maughan RJ, Mettler S, Meeu-wisse WH, Page AJ, Reid SA, Rehrer NJ, Roberts WO, Rogers IR,Rosner MH, Siegel AJ, Speedy DB, Stuempfle KJ, Verbalis JG,Weschler LB, Wharam P: Statement of the Second InternationalExercise-Associated Hyponatremia Consensus Development Confer-ence, New Zealand, 2007. Clin J Sport Med 18: 111–121, 2008
54. Chen S, Jalandhara N, Batlle D: Evaluation and management ofhyponatremia: An emerging role for vasopressin receptor antagonists.Nat Clin Pract Nephrol 3: 82–95, 2007
55. Mohmand HK, Issa D, Ahmad Z, Cappuccio JD, Kouides RW, SternsRH: Hypertonic saline for hyponatremia: Risk of inadvertent over-correction. Clin J Am Soc Nephrol 2: 1110–1117, 2007
56. Drescher T, Klima T, Schifferli J: Seizures, hyponatraemia, and“poison.” Lancet 371: 2144, 2008
57. Decaux G, Soupart A, Vassart G: Non-peptide arginine-vasopressinantagonists: The vaptans. Lancet 371: 1624–1632, 2008
58. Zeltser D, Rosansky S, van Rensburg H, Verbalis JG, Smith N:Assessment of the efficacy and safety of intravenous conivaptan ineuvolemic and hypervolemic hyponatremia. Am J Nephrol 27: 447–457, 2007
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 141

59. Verbalis JG, Zeltser D, Smith N, Barve A, Andoh M: Assessment ofthe efficacy and safety of intravenous conivaptan in patients witheuvolaemic hyponatraemia: Subgroup analysis of a randomized,controlled study. Clin Endocrinol (Oxf) 69: 159–168, 2008
59a. Rianthavorn P, Cain JP, Turman MA: Use of conivaptan to allowaggressive hydration to prevent tumor lysis syndrome in a pedi-atric patient with large-cell lymphoma and SIADH. Pediatr Neph-rol 2008
60. Perianayagam A, Sterns RH, Silver SM, Grieff M, Mayo R, Hix J,Kouides R: DDAVP is effective in preventing and reversing inad-vertent overcorrection of hyponatremia. Clin J Am Soc Nephrol 3:331–336, 2008
Hypernatremia and Diabetes Insipidus
Basic Mechanisms of OsmoregulationAlthough osmoregulatory systems in humans
and other mammals strive to maintain a set point ofconstant plasma osmolality, rapid fluctuations occuraround that set point because of changes in the rates ofwater intake and water loss (through the skin or urine)and because of variations in sodium intake and excre-tion rates. Forty minutes of strenuous exercise in theheat or 24 h of water deprivation increases the plasmaosmolality by �10 mOsm/kg, whereas drinking theequivalent of two large glasses of water (850 ml)lowers osmolality by approximately 6 mosmol/kgwithin 30 min. Ingestion of 13 g of salt increasesplasma osmolality by approximately 5 mosmol/kgwithin 30 min (1). Osmotic fluctuation within the 1 to3% range that is compatible with health controls body-fluid homeostasis by inducing proportional homeo-static responses through negative feedback. Sensoryosmoreceptors actively generate a basal signal at thedesired set point and can modulate this signal toencode both the direction and the magnitude of thestimulus (1).
Extracellular hyperosmolality stimulates the sen-sation of thirst to promote water intake, and the releaseof arginine vasopressin (AVP), also known as antidi-uretic hormone, to increase water reabsorption by therenal tubules. It is known that cell shrinkage is re-quired for thirst and AVP release because these re-sponses are evoked by infusions of concentrated solu-tions that contain membrane-impermeable solutes,which extract water from cells, but not by infusions ofsolutes that readily equilibrate across the cell mem-brane (e.g., urea).
Osmoreceptors are neurons that can detectchanges in extracellular osmolality. The osmotic setpoint is determined by the resting electrical activity ofthese cells, and osmotic perturbations result in signals
to downstream neurons by proportional changes in theaction-potential firing rate (or firing pattern) (1). Bothcerebral and peripheral osmoreceptors contribute tothe body fluid balance. Peripheral osmoreceptors havebeen identified along the oropharynx and the intestinallumen and in the blood vessels that collect solutesabsorbed from the intestines (splanchnic mesenteryand hepatic portal vein). Osmoreceptors in these areascan detect the osmotic strength of what is eaten ordrunk and, through afferent connections to the centralnervous system, can induce anticipatory responses thatbuffer the effect of ingestion-related osmotic pertur-bations. Water intake satisfies thirst and decreasesvasopressin release before extracellular hyperosmolalityis fully corrected, whereas salt ingestion stimulates argi-nine vasopressin (AVP) release and thirst before plasmaosmolality increases. Hypertonic saline infusions directlyinto the hepatic portal vein can provoke anticipatoryosmoregulatory responses in the absence of significantchanges in extracellular fluid osmolality (1).
Information collected by peripheral osmorecep-tors reach the central nervous system through fibersthat ascend in the vagus nerve and form synapses inthe nucleus tractus solitarius and through peripheralprojections of dorsal root ganglion neurons that pro-vide input to the thoracic spinal cord, where first-ordersynapses are made onto ascending relay neurons in thesuperficial layers of the dorsal horn (1).
Cerebral osmoreceptors are located in circum-ventricular organs, a brain region that lacks a blood–brain barrier. The organum vasculosum laminae ter-minalis (OVLT) located in the anterior region of thethird ventricle is a key osmosensing site; functionalmagnetic resonance imaging studies have shown thatthe anterior region of the third ventricle becomesactivated during the onset of hypertonicity in humans.
Osmoreceptor neurons display an intrinsic abilityto transduce osmotic perturbations into changes in therate or pattern of action-potential discharge. Neuronsin the OVLT, the subfornic organ, and magnocellularneurosecretory cells in the supraoptic nucleus, canoperate as intrinsic osmoreceptors. Most of these cellsare proportionally excited by hypertonic stimuli andinhibited by hypo-osmotic stimuli. Thus, the basalelectrical activity of these cells effectively encodes theosmotic set point. Unlike many cells in the body,which resist changes in volume through various regu-latory mechanisms, magnocellular neuronal cells be-have as osmometers, displaying reversible changes in
142 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

volume that are inversely proportional to extracellularfluid osmolality. Osmoreceptor neurons become depo-larized when they are exposed to hypertonic condi-tions, and hypotonic stimuli cause hyperpolarizationbecause of the suppression of a nonselective cationcurrent (1,2). It is thought that a single population ofcation channels may mediate osmosensory transduc-tion through modulation of their probability of open-ing during changes in fluid osmolality. The increase inmembrane conductance provoked by a hypertonicstimulus is linked to a cell volume decrease. It ispossible that changes in physical strain caused by cellshrinkage could regulate a mechanosensitive channel.Alternatively, the increased concentration of cell sol-ute caused by loss of water from cells could play a rolein osmosensory transduction. Experiments in whichcell volume was decreased by pipette suction or in-flated by increased pipette pressure while maintaininga constant concentration of solute suggested thatchanges in cell volume are the controlling variable (2).By increasing membrane stretch, hypotonic cell swell-ing seems to suppress stretch-inhibited channel activ-ity, which reduces cation conductance, hyperpolariz-ing the cell. Conversely, hypertonic cell shrinkagerelaxes membrane stretch, thereby increasing channelactivity and membrane cation conductance, depolariz-ing the cell. Transient receptor potential vanilloid(TRPV) channels may play a role in osmoregulation,affecting osmosensation and the generation of thirst;channels encoded by trpv2 and trpv4 genes are ex-pressed in osmoreceptor neurons, and trpv4 knockoutmice drink less water and become hypernatremic andfail to increase AVP secretion normally when injectedwith hypertonic saline. Osmoreceptor neurons in thesupraoptic nucleus also express a variant of TRPV1, inwhich a portion of the N-terminal domain is truncated.Products of the trpv1 gene may contribute to theintrinsic osmosensitivity of these neurons. Althoughhypertonicity shrinks osmoreceptor cell volume, intrpv1�/� knockout mice, this stimulus no longer in-creases membrane conductance, membrane depolar-ization, or firing frequency (Figure 3). Hypertonicity-evoked thirst and AVP release are significantlyattenuated in trpv1�/� mice, and trpv1�/� animalsmaintain a plasma osmolality comparable to that foundin rats subjected to 24 h of dehydration.
Information derived from peripheral and cerebralosmoreceptors is transmitted to many parts of thebrain, where these signals are integrated with sensory
inputs provided by changes in blood volume, BP,extracellular sodium concentration, and body temper-ature (3). Little is known about the mechanisms bywhich osmotic and nonosmotic signals are integrated;however, previous work showed that at least six areasof the central nervous system participate in this process.
AVP is synthesized by a subset of magnocellularneuronal cells (MNCs) located in the paraventricularand supraoptic nuclei of the hypothalamus. Theseneurons project axons into the neurohypophysis,where the hormone is released when action potentialsstimulate voltage-gated Ca2� influx and exocytosis.The firing rate of MNCs under resting conditions medi-
Figure 3. Osmosensory signal transduction. The positionsof the OVLT and supraoptic nucleus (SON) relative to otherhypothalamic structures in the rodent brain are shown.Hypertonicity depolarizes osmoreceptor neurons in theOVLT of wild-type (WT) animals, increasing their rate ofaction potential discharge (upper traces in the bottom leftinset). These neurons send axonal projections to the SON,where they release the excitatory transmitter glutamate andexcite neurons that release vasopressin (VP). OVLT neu-rons also project to cortical areas such as the insula (Ins) andthe anterior cingulate gyrus (AC), which are believed to beinvolved in the perception of thirst. The depolarization andexcitation of VP-releasing neurons in the SON induced byhyperosmolality (upper traces in the top right inset) arecaused by the combined action of stretch-inhibited (SI)channels and ionotropic glutamate receptors expressed inthese cells. OVLT and SON neurons from TRPV1 geneknockout mice (Trpv1�/�) fail to exhibit the normal re-sponses to hypertonic stimuli (lower sets of traces in theinsets). Reprinted by permission from Macmillan PublishersLtd: Kidney Int 73:811–5, 2008 (ref. 2).
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 143

ates basal AVP secretion; decreased firing frequency inhypotonicity response inhibits hormone release, and in-creased frequency in response to hypertonicity enhancesit. Taurine release from glia contributes to the osmoticcontrol of firing rate in MNCs, and these neurons alsoreceive synaptic afferents from the nucleus tractus soli-tarius and from peripheral osmoreceptors and from neu-rons in the OVLT.
Newly synthesized AVP prohormone is pack-aged into secretory granules and then transporteddown the supraopticohypophyseal tract to the posteriorpituitary (4). During its passage, the prohormone isenzymatically cleaved into AVP, neurophysin, and aC-terminal glycopeptide. Once released, circulatingAVP binds to vasopressin V2 receptors on the baso-lateral membrane of the renal collecting duct, activat-ing a cAMP-mediated signal transduction pathwaythat results in the insertion of aquaporin 2 (AQP2)water channels in the luminal membrane. AQP2 chan-nels increase the water permeability of the collectingduct, permitting luminal fluid to come into osmoticequilibrium with the surrounding hypertonic renal me-dulla.
Age-Related HypodipsiaAging alters thirst and drinking responses, mak-
ing older people vulnerable to body fluid imbalance(3). Systemic infusion of hypertonic solutions de-crease thirst responses in older men in some but not allstudies. Head-out-of-water immersion (which driveswater into the intrathoracic cavity, mimicking volumeexpansion) decreases thirst in young but not in olderindividuals. Reduced responses to hypovolemia couldbe explained by changes in baroreceptor function or byhigher-order processing of signals generated bychanges in blood volume.
Regardless of how much thirst they record, olderpeople tend to drink less than their younger counter-parts when dehydrated. This aged-related decrease indrinking has been reported after hypertonic infusionsand fluid restriction, acutely after exercise, and inresponse to exercise–heat acclimation (3). After dehy-dration, young people drink rapidly until their thirst issatisfied. Thirst satiation occurs before water has beenabsorbed from the gastrointestinal tract and before theplasma osmolality has fallen; it is controlled by affer-ent signals from the mouth, pharynx, esophagus, andstomach. Farrell et al. (3) investigated the generationof thirst in 12 older (age 68.1 � 3.4) and 10 younger
(age 23.7 � 2.8) men by infusing of hypertonic salineand using positron emission tomography to measureregional cerebral blood flow during the developmentand then the satiation of thirst. Older and younger menhad similar increases in blood osmolality and experi-enced nearly identical thirst levels as measured on ananalogue scale during and after hypertonic saline. Thetwo age groups also exhibited similar patterns ofregional blood flow on positron emission tomographyscanning; however, when given free access to water,older men drank much less than younger men. Thus,aging did not affect the perception of thirst but ratherthe satiation of thirst; it remains unknown whetherdiminished responses to dehydration in older peoplereflects an effect of age on afferent inputs from thepharynx and intestine or in the central processing ofthirst and the satiation process.
Renal Concentrating MechanismThe glomerular filtrate that enters the proximal
tubule has essentially the same osmolality as plasma.Water and solute are absorbed isotonically along theproximal tubule. Water flows out of the S2 segment ofthe proximal tubule though the proximal tubular cells,a process that is dependent on the presence of AQP1water channels on the cells’ luminal membranes. Asthe fluid enters the descending limb of the loop ofHenle, it is exposed to a higher osmolality in thesurrounding interstitial fluid that has been generatedby transport in the thick ascending limb of the loop ofHenle. AQP1 also provides the route for water flowout of the descending limb and the outer medullarydescending vasa recta. Deletion of AQP1 in mice andmutations in AQP1 in humans result in impairedability to concentrate the urine by interfering with thecountercurrent multiplication and exchange that arerequired for the medullary concentration gradient (5).The ascending thick limb exports sodium chloridefrom its lumen through an apical membrane Na-K-2Clco-transporter; however, lacking water channels, thissegment is relatively impermeable to water, so salt isreabsorbed without water, diluting the luminal con-tents and increasing the salt concentration of the sur-rounding interstitium (6). Fluid that enters the distaltubule becomes isotonic from continued salt and waterreaborption as it enters the collecting duct. The lumi-nal membrane of collecting duct principal cells be-comes permeable to water in the presence of AVP,which inserts AQP2 water channels in the membrane,
144 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

but it is relatively impermeable to urea. Water exits thecells through AQP3 and AQP4, which are expressedon the basolateral (blood side) membrane of the cor-tical and outer medullary collecting duct, and AQP4,which is expressed in the inner medullary collectingduct (5). Deletion of AQP3 results in marked polyuriain mice, but, to date, there have been no reports ofAQP3 mutations causing polyuria in humans. AQP4null mice have only a mild concentrating defect, sug-gesting that most of the water is reabsorbed in thecortical and outer medullary segments of the collectingduct. As the luminal fluid descends in the collectingduct, it becomes more concentrated as water diffusesout, attracted by the high salt concentration of thesurrounding interstitium, and the luminal urea concen-tration rises. The medullary collecting duct is perme-able to both water and urea in the presence of AVP,owing to vasopressin-responsive AQP2 water chan-nels and vasopressin-responsive urea channels in itsluminal membrane. Urea diffuses out of the medullarycollecting duct into the interstitium down its concen-tration gradient, and the accumulating interstitial urearaises the interstitial osmolality that, in turn, attractswater from the descending limb of the loop of Henle,a segment that is highly permeable to water andrelatively impermeable to salt and urea. Because themedullary collecting duct is highly permeable to bothwater and urea, the final urine has a concentration thatis similar to that of the fluid at the bend of the loop ofHenle and the deep medullary interstitial tissue, atmaximum, approximately 1200 mOsm/kg (6).
References1. Bourque CW: Central mechanisms of osmosensation and systemic
osmoregulation. Nat Rev Neurosci 9: 519–531, 20082. Sharif-Naeini R, Ciura S, Zhang Z, Bourque CW: Contribution of
TRPV channels to osmosensory transduction, thirst, and vasopressinrelease. Kidney Int 73: 811–815, 2008
3. Farrell MJ, Zamarripa F, Shade R, Phillips PA, McKinley M, Fox PT,Blair-West J, Denton DA, Egan GF: Effect of aging on regionalcerebral blood flow responses associated with osmotic thirst and itssatiation by water drinking: A PET study. Proc Natl Acad Sci U S A105: 382–387, 2008
4. Loh JA, Verbalis JG: Disorders of water and salt metabolism associ-ated with pituitary disease. Endocrinol Metab Clin North Am 37:213–234, x, 2008
5. Verkman AS: Dissecting the roles of aquaporins in renal pathophysi-ology using transgenic mice. Semin Nephrol 28: 217–226, 2008
6. Linshaw MA: Back to basics: Congenital nephrogenic diabetes insip-idus. Pediatr Rev 28: 372–380, 2007
HypernatremiaHypernatremia, a common electrolyte distur-
bance in hospitalized patients, is characterized by an
absolute or relative free water deficit. In hypovolemichypernatremia, total body water content is reduced. Ifthere has been a net loss of water with no change inelectrolyte balance, then the patient may not exhibitsigns of volume depletion unless the deficit is large. Ifelectrolytes have been lost in addition to water, thenthe patient will have hypotension and azotemia. Inhypervolemic hypernatremia, there is a relative freewater deficit (i.e., total body water content is eithernormal or reduced, but the ratio of body electrolytecontent [exchangeable sodium plus potassium] is in-creased because of positive balance of these cations).The relationship among the plasma sodium concentra-tion (PNa), body water, and body electrolyte contentwas first described empirically by Edelman. Simplis-tically, that relationship has been reduced to a concep-tual equation:
PNa � Exchangeable (Na� � K�) Body Water
The actual equation derived from empirical isotopicmeasurements has an intercept of �24.30 and a slopeof 1.03, and mechanistic explanations have been of-fered to explain why these values differ from 0 (1). Inaddition, the relationship is distorted by hyperglyce-mia. Thus, a rigorous prediction of how the plasmasodium concentration will change during hypernatre-mia development and during efforts to repair thedisturbance requires an equation that incorporates theslope; the intercept; the blood glucose; and changes inwater, sodium, and potassium balance (1).
In a 2-yr study of all patients who were admittedto a single center in Greece, hypernatremia was iden-tified at admission in 0.5% of patients, and 0.7%developed hypernatremia in the hospital (2). A total of113 patients with hypernatremia were analyzed. Theages of patients with admission hypernatremia (76.3 �12.2) and hospital-acquired hypernatremia (73.9 �14.4) were similar. Patients with hypernatremia onadmission had a significantly lower mortality rate thanthose with hospital-acquired hypernatremia (28 versus48%) despite having higher serum sodium concentra-tions (160 � 10 versus 154 � 2 mmol/L). In all fatalcases, hypernatremia occurred in the setting of seriousunderlying disease, mainly sepsis or stroke, and 85%of the patients who died had normonatremia at time ofdeath. Thus, it seemed that hypernatremia was amarker for severe underlyling disease rather than acause of death.
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 145

Defined by a fractional excretion of sodium�0.5% and a blood urea nitrogen/creatinine �40, alarge majority (82%) of patients with hypernatremiaon admission were classified as having hypovolemichypernatremia. The most common causes of excessivewater loss for this group were fever (84%), mostlyresulting from pulmonary infections, uncontrolled di-abetes (40%), high environmental temperature (36%),osmotic diarrhea because of lactulose (8%), and furo-semide (4%). In almost all cases, water intake wasobviously diminished because of altered mental status.Only 45% of patients who developed hypernatremia inthe hospital were classified as having hypovolemia,and 5% had marked edema associated with heartfailure, cirrhosis, or attempts at volume resuscitationfor shock. Sources of water loss in the hospitalizedpatients were also dominated by fever, primarily be-cause of pulmonary infections (72%), uncontrolleddiabetes (30%), osmotic diarrhea from lactulose(10%), and furosemide (9%); in addition, 10% ofpatients had been treated with mannitol.
A study of all patients who were admitted to themedical, surgical, or neurologic intensive care units(ICU) of a university hospital in the Netherlandsidentified 130 patients who developed hypernatremiain the ICU (serum sodium 156 � 6 mmol/L) (3).Sepsis, hypokalemia, renal dysfunction, hypoalbumin-emia, and the use of mannitol and bicarbonate weremore common in patients with hypernatremia com-pared with those with normonatremia. During hyper-natremia, fluid balance was negative in approximately60% of cases, but in a substantial minority, it waspositive. Patients with positive fluid balance receivedmore sodium and potassium but a similar amount ofelectrolyte-free water, and they tended to have poly-uria despite hypernatremia. No patients had beengiven hypertonic saline. Urinary sodium and potas-sium losses were not measured, so a quantitativeanalysis of the changes in fluid and electrolyte balancecausing hypernatremia could not be made; however,the authors argued that many patients developed hy-pernatremic in the ICU by “too much sodium and notenough water” (i.e., large volumes of isotonic fluidcoupled with unreplaced water losses caused by hy-perglycemia, renal concentrating defects because ofhypercalcemia or hypokalemia, renal dysfunction, fu-rosemide, or mannitol). Another factor, which was notmentioned or measured by the investigators, is in-creased urea excretion caused by catabolism and/or
protein feeding. For fluid overloaded patients withhypernatremia, the proper therapy is water administra-tion (or its parenteral equivalent, 5% dextrose in wa-ter) in conjunction with furosemide to achieve nega-tive sodium balance with neutral or negative fluidbalance (1,3).
The mortality rate among ICU patients withhypernatremia was 48% (five times higher than pa-tients with normonatremia), and they were generallysicker with higher APACHE II and lower GlasgowComa Scale scores (3). A multivariate analysis iden-tified hypernatremia as an independent risk factor fordeath (odds ratio 4.3; 95% confidence interval 2.5 to7.2) as were age and renal dysfunction. Just more thanhalf of the patients with fatal cases had hypernatremiawhen they died; these patients had a more acuteincrease in serum sodium concentration comparedwith other cases (14 versus 6 mmol/L per d; P �0.002) and reached a higher serum sodium level(160 � 8 versus 155 � 4 mmol/L). Correction ratesdid not differ between patients who lived and thosewho died (3).
Therapeutic HypernatremiaHypertonic saline solutions have emerged as a
preferable alternative to mannitol to treat increasedintracranial pressure (4). Koenig et al. (5) reported a4-yr single-center study of 63 patients who had nor-monatremia and were treated for transtentorial herni-ation (caused by a variety of neurosurgical conditions)with hypertonic saline. Extending a preliminary report,the investigators administered 23.4% saline as a bolusof 30 ml (85.5% of cases) or 60 ml (14.5% of cases).Prompt reversal of clinical signs of herniation (unilat-erally or bilaterally dilated, nonreactive pupils associ-ated with a decline in the Glasgow Coma Scale score)was observed in 57 (75%) of 76 events. Amongpatients with intracranial pressure (ICP) monitors, ICPdecreased from 23.3 � 16.2 to 13.8 � 10.3 mmHg(P � 0.001) within 1 h. Patients with successfulreversal of herniation had a higher serum sodium at 1 h(149.8 � 9.3 mmol/L). Univariate predictors of suc-cessful reversal of herniation included an increase inserum sodium of �5 mmol/L and an absolute serumsodium �145 mmol/L. Twenty-two (32.4%) patientssurvived to discharge, five of whom (8% of the totaltreated cohort) had minimal to mild disability. The30-ml bolus of 23.4% saline used in this study isequivalent in sodium content to 240 ml of 3% saline.
146 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

Thus, the treatment is similar to what has been advisedfor patients with acute hyponatremic emergencies.Larger doses of 23.5% saline were reported in a studyof patients who had subarachnoid hemorrhage andwere assigned poor clinical grades because of cerebralischemia caused by vasospasm (6). Infusion of 2 ml/kgover 20 to 30 min, increasing the serum sodium by11.2 � 4.0 mmol/L at 1 h, significantly increasedcerebral perfusion pressure and decreased ICP by93%, including six patients whose ICP went lowerthan 0 after the infusion, suggesting shrinkage of theintracranial contents. It should be noted that 23.4%saline can cause severe extravasation injury andshould be administered only in a central vein; itsadvantage over 3 or 5% solution has not been demon-strated.
Aggressive use of hypertonic saline has alsobeen reported in patients with normonatremia andsubarachnoid hemorrhage to decrease elevated ICPbefore signs of transtentorial herniation. In a placebo-controlled study, infusion of 2 ml/kg 7.2% saline in6% hydroxyethyl starch over 30 min into a centralvenous catheter was compared with an equal-volumeinfusion of isotonic saline. Among patients who weregiven hypertonic saline, the maximum increase inserum sodium averaged 5.6 mmol/L (range 4 to 7mmol/L) at 30 min and 3.3 mmol/L (range 1 to 5mmol/L) after 210 min; the serum sodium concentra-tion did not change in patients who were given iso-tonic saline. In response to hypertonic saline, intracra-nial pressure decreased significantly, within 1 h of thestart of the infusion, by a mean maximum of 5.6mmHg and increased cerebral perfusion pressure,whereas no change occurred after isotonic saline. Aswould be expected, the ICP change was less than aprevious uncontrolled study by this group, using thesame regimen in sicker patients with ICP �20 mmHg.On the basis of these findings and a review of otherpublished observations, the authors now recommendthat the initial bolus be �2 ml/kg of the 7% solution.
References1. Nguyen MK, Kurtz I: Correction of hypervolaemic hypernatraemia by
inducing negative Na� and K� balance in excess of negative waterbalance: A new quantitative approach. Nephrol Dial Transplant 23:2223–2227, 2008
2. Liamis G, Tsimihodimos V, Doumas M, Spyrou A, Bairaktari E, ElisafM: Clinical and laboratory characteristics of hypernatraemia in aninternal medicine clinic. Nephrol Dial Transplant 23: 136–143, 2008
3. Hoorn EJ, Betjes MG, Weigel J, Zietse R: Hypernatraemia in critically
ill patients: Too little water and too much salt. Nephrol Dial Trans-plant 23: 1562–1568, 2008
4. Himmelseher S: Hypertonic saline solutions for treatment of intracra-nial hypertension. Curr Opin Anaesthesiol 20: 414–426, 2007
5. Koenig MA, Bryan M, Lewin JL 3rd, Mirski MA, Geocadin RG,Stevens RD: Reversal of transtentorial herniation with hypertonicsaline. Neurology 70: 1023–1029, 2008
6. Tseng MY, Al-Rawi PG, Czosnyka M, Hutchinson PJ, Richards H,Pickard JD, Kirkpatrick PJ: Enhancement of cerebral blood flow usingsystemic hypertonic saline therapy improves outcome in patients withpoor-grade spontaneous subarachnoid hemorrhage. J Neurosurg 107:274–282, 2007
Diabetes InsipidusDiabetes insipidus (DI) is caused by deficient
arginine vasopressin (AVP) secretion (central DI),physiologic inhibition of AVP secretion because ofprimary water intake (dipsogenic DI), or diminishedrenal response to the hormone (nephrogenic DI). Allpolyuric disorders, regardless of whether they areneurogenic, nephrogenic, or psychogenic, are associ-ated with dilation of the renal collecting system andbladder. Chronic renal failure resulting from bilateralhydronephrosis has been reported. Renal and bladderultrasounds are advisable annually. Scheduled voidingand double voiding can prevent complications (1).
Central DICentral DI is caused by a variety of acquired or
congenital disorders that affect the hypothalamic-pos-terior pituitary axis, including tumors, trauma, hemor-rhage and infarction, granulomatous disease, and pi-tuitary surgery (2,3). Because the synthesis of AVPoccurs in the supraoptic and paraventricular nuclei ofthe hypothalamus, pituitary tumors themselves do notusually cause DI; however, postoperative polyuriaoccurs in 18 to 31% of patients after transphenoidalsurgery. The course of postoperative DI is usuallytransient but can be permanent or triphasic, as wasdescribed in experimental studies of transaction of thepituitary stalk. Permanent DI occurs in only 2 to 10%of patients because 80 to 90% of vasopressin-secretingneurons must be destroyed for this to occur. TransientDI and the first phase of triphasic DI is caused bydysfunction of vasopressin-secreting neurons causedby direct trauma or ischemia. The triphasic pattern isquite rare, occurring in only 3.4% of patients, but it isalso quite interesting (2). The first phase of DI, lastingfor 5 to 7 d, is followed by syndrome of inappropriateantidiuresis (SIAD) resulting from uncontrolled AVPleakage from degenerating posterior pituitary tissue orfrom vasopressin-secreting neurons whose axons have
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 147

been severed. Typically, continued administration ofhypotonic fluid, started in the first phase to avoiddehydration, results in hyponatremia when an antidi-uresis appears in the second phase, which lasts 2 to14 d. Some patients with more limited damage presentwith an isolated second phase (i.e., SIAD withoutprevious DI). Once AVP stores are depleted, the thirdphase of chronic DI begins. Magnetic resonance im-aging can facilitate DI diagnosis. The presence ofvasopressin and oxytocin is normally revealed by abright spot in the posterior pituitary on T1-weightedimages; the absence of a bright spot can help confirma diagnosis of postoperative DI. However, the brightspot may not disappear early in the course of thedisease, so its presence does not exclude the diagnosis.Desmopressin is the drug of choice for the acute andchronic DI management. The drug promptly reducesurine output, and its effect generally lasts 6 to 12 h.Urine output must be carefully monitored in the earlypostoperative course, and output of 200 to 250 ml/hwith a urine osmolality �200 mOsm/kg or urinespecific gravity �1.005 is an indication for a dose ofdesmopressin (2).
Some authors advocated administration of des-mopressin on an as-needed basis rather than a fixedschedule (2). In addition to avoiding hyponatremia,this strategy allows detection of decreasing urine out-put, if SIAD should develop. An alternative strategy isto give a fixed dose of desmopressin frequently andtreat the patient as though he or she has SIAD, avoid-ing hypotonic fluids and giving hypertonic fluids whennecessary, or to give continuous infusions of diluteAVP in a dosage of 0.25 to 2.70 mU/kg per h (2). AVPhas a half-life of 10 to 20 min, so the continuousinfusion approach permits a rapid resolution of antidi-uresis if the serum sodium falls too low. Regardless ofthe strategy chosen and regardless of whether SIADoccurs, a large series of patients with postoperative DIafter transphenoidal surgery found that 8.4% of pa-tients developed hyponatremia and 2.1% had symp-tomatic hyponatremia. Thus, careful monitoring of theserum sodium concentration is mandatory.
Central DI is the most common manifestation ofneuroendocrine sarcoidosis (4,5); however, the centralnervous system is involved in only 5% of patients withsarcoid, making this an uncommon disorder. A long-term study of nine patients with known sarcoidosis andhypothalamic involvement by magnetic resonance im-aging found that all patients had anterior pituitary
dysfunction, especially hypogonadism, which was uni-versally present, and diabetes insipidus developed inseven (4). Although brain parenchymal lesions im-proved in response to steroids, the hormone deficien-cies were irreversible, suggesting permanent destruc-tion of the pituitary or hypothalamic cells bygranulomas.
Adipsic DIWhen vasopressin secretion and thirst both are
impaired, affected patients are vulnerable to recurrentepisodes of hypernatremia. Once called “essential hy-pernatremia,” the disorder is now called “central DIwith deficient thirst” or “adipsic DI.” A recent reviewof the literature identified a total of 70 patients withcentral DI and deficient thirst in 41 studies (6). Re-ported causes include congenital/developmental con-ditions (predominantly septo-optic dysplasia; 20%),germinoma (17%), rupture or clipping of anteriorcommunicating artery aneurysms (14%), craniophar-yngioma (13%), pinealoma (4%), Langerhans cell his-tiocytosis (4%), neurosarcoidosis (3%), head trauma(3%), cytomegalovirus encephalitis (3%), nonfunc-tioning pituitary adenoma (3%), macroprolactinoma(1%), and toluene exposure (1%).
Small perforating arterial branches from the an-terior communicating artery supply the hypothalamicosmoreceptors that mediate thirst and vasopressin re-lease, explaining why patients with aneurysms thatinvolve this artery sometimes develop adipsic DI (6,7).Most patients with adipsic DI caused by anteriorcommunicating artery aneurysms retain the ability tosecrete vasopressin and concentrate their urine in re-sponse to a decrease in arterial BP (100% of the fivepatients who have been studied); this response ismediated by baroreceptors in the aortic arch, carotidarteries, and atria. Patients with adipsic DI from cra-niopharyngioma (0% of four patients studied) are lesslikely to retain baroceptor-mediated vasopressin secre-tion.
All patients reported in the literature had featuresof central DI; they were unable to concentrate theirurine when dehydrated or after hypertonic saline butwere able to concentrate the urine in response toexogenous vasopressin or desmopressin (6,7). Thirstwas absent despite an intact sensorium and free accessto water. The diagnosis of adipsic DI can be confirmedin a dehydrated patient or during hypertonic salineinfusion by measuring plasma vasopressin by radio-
148 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

immunoassay and by quantifying thirst using an ana-log scale; however, these tests are seldom required inroutine clinical practice.
Patients who have central DI and whose thirst isintact maintain normal serum sodium levels despiteextremely large urine outputs, provided that they havefree access to water and are physically able to drink.By contrast, patients with adipsic DI are prey tolife-threatening dehydration, renal failure, and sei-zures. Severe hypernatremia is common, with serumsodium levels ranging from 148 to 221 mEq/L. Sev-enteen (24%) patients in the literature experiencedseizures (most because of hyponatremia), and 44(63%) patients had been admitted at least once withhypernatremia or hyponatremia. Acute renal failure(3%) and rhabdomyolysis (4%) are serious but lesscommonly reported complications (6,7).
Anterior pituitary dysfunction was documentedin 46 (72%) of 64 patients, including panhypopituita-rism in 28 (44%) patients and partial defects in ante-rior pituitary hormone secretion in 18 (28%) patients.Patients with adipsic DI associated with anterior com-municating aneurysms were significantly less likelythan patients with craniopharyngioma, germinoma, orcongenital/developmental conditions to have panhypo-pituitarism (6,7). Other hypothalamic abnormalitieswere identified in 23 (33%) patients, including distur-bances of appetite (16 patients) and temperature reg-ulation (10 patients). In addition, 56 patients (80% ofthe entire cohort) had neurologic abnormalities relatedto their underlying condition (vision loss, hemiplegia,short-term memory deficits, or cognitive dysfunction).
A carefully documented single-center series of13 patients with adipsic DI (cited in the previouslymentioned literature review) found a high mortalityrate at a young age (7). A review of death certificatessuggested that the cause of death was respiratoryfailure resulting from sleep apnea. Symptomatic ob-structive sleep apnea was recognized among more thanhalf of the patients. In addition, a high percentage ofpatients experienced thromboembolic events, seriousobesity, and seizure disorders. Two patients were ad-mitted with symptomatic hyponatremia, one case aftera binge on cider, with continued vasopressin.
All of the patients in this series had polyuria (�4L/d), and, indeed, this feature was one of the criteriaused to define the disorder; however, some patientsexhibit more subtle abnormalities of osmoregulation,most commonly an upward resetting of the osmotic
thresholds for vasopressin secretion and thirst (6–8).Such patients are protected from extreme hypernatre-mia by their ability to experience thirst and elaboratea concentrated urine at higher plasma osmolalities thannormal. Because patients with an upwardly reset os-mostat may not have oliguria when they have hyper-natremia, their underlying DI may not be recognized.In this series, patients with adipsic DI caused byanterior communicating artery aneurysms had briskAVP responses to hypotension, indicating intact su-praoptic and paraventricular nuclei and normal-func-tioning posterior pituitary glands. This finding sug-gests a lesion in the osmoreceptors in the anteriorhypothalamus. Patients with adipsic DI associatedwith tumors had undergone extensive surgery that hadcreated lesions in the neurohypophesis as well as theosmoreceptors.
Treatment of patients with adipsic DI includesdesmopressin for patients with polyuria at high normalserum sodium concentrations; regimens of scheduledfluid drinking should be recommended to all patients.In one report, a behavior modification approach wasused successfully to ensure adequate fluid intake in apatient with severe amnesia. Fluid intake must beadjusted by monitoring of body weight and serumsodium levels while taking into account variations inambient temperature. Because of the high incidence ofthrombosis (most likely a complication of plasmavolume contraction and hyperviscosity), routine use ofprophylactic heparin is advisable during periods ofdehydration.
Holley et al. (9) reported a 44-yr-old man withextreme hypernatremia (208 mmol/L) as a result ofadipsic DI, caused by a gunshot wound to the head atage 18. Computed tomography revealed a residualprojectile fragment near the third ventricle. Presum-ably, the severe hypernatremia was related to workingin the heat (an ambient temperature of 42°C wasrecorded on the day of his admission). A 19-L waterdeficit was replaced over 4 d, gradually decreasing theserum sodium concentration. At a serum sodium of147 mmol/L, his urine osmolality was 743 mOsm/kg,consistent with hypodipsia and partial central DI—anupwardly reset (hypertonic) osmostat. The patientmade a full neurologic recovery.
Acquired Nephrogenic DILithium. One of every 1000 people in the UnitedStates is treated with lithium, and approximately one
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 149

fourth of them develop polyuria (10). Undoubted,lithium is the most important cause of nephrogenic DI.Lithium inhibits vasopressin-stimulated translocationof cytoplasmic aquaporin 2 (AQP2) to the luminalmembrane of the collecting duct by inactivating ade-nyl-cylase and inhibiting protein kinase A–inducedphosphorylation of cytoplasmic AQP2 (10). Polyuriabecause of lithium is associated with downregulationof AQP2 and AQP3 gene expression and decreasedtrafficking of the vasopressin-regulated water channelAQP2 to the apical membrane of the collecting duct.Patients with lithium-induced nephrogenic DI excreteless cAMP and less AQP2 in their urine (11). There isalso evidence that lithium downregulates expression ofthe urea transport proteins, which could contribute todecreased concentrating ability by diminishing theconcentration gradient in the renal medulla. In addi-tion to its effects on water and urea channels, long-term use of lithium causes major changes in thecellular composition of the collecting duct, reducingthe percentage of principal cells, which are the sitesfor regulated water reabsorption. Proteins that areinvolved in cell death, apoptosis, cell proliferation,and morphology are altered after 1 to 2 wk of lithiumtreatment, suggesting that these proteins may play arole in the remodeling of the collecting duct associatedwith lithium treatment (12).
It has been known for nearly 50 yr that thiazidediuretics paradoxically decrease urine output in lithi-um-induced and congenital nephrogenic DI. In ratswith lithium-induced nephrogenic DI, hydrochlorothi-azide upregulates AQP2 and the Na-K-2Cl transporterin the ascending limb (which is responsible for creat-ing the medullary concentration gradient). Nonsteroi-dal anti-inflammatory drugs, which are also known todecrease polyuria clinically, also increase the abun-dance of AQP2 and Na-K-2Cl transporter in lithium-treated rats (13). Recently, mineralocorticoids havebeen shown to affect experimental nephrogenic DI asa result of lithium. Aldosterone administration dramat-ically increases urine production (an effect that isassociated with decreased expression of AQP2 onluminal membranes of the collecting duct), whereasadministration of the mineralocorticoid receptorblocker spironolactone decreased urine output andincreased AQP2 expression (14). Aldosterone and spi-ronolactone have similar effects on the subcellulardistribution of AQP2 in vasopressin-deficient polyuricBrattleboro rats, suggesting that the mineralocorticoid
effect is related to the absence of vasopressin signalingrather than to lithium per se. To date, these observa-tions have been limited to lithium-treated experimentalanimals; it is not yet known whether spironolactonewould be a useful treatment for humans with lithium-induced nephrogenic DI.
The epithelial sodium channel (ENaC) is theentrance pathway for lithium into collecting duct prin-cipal cells. ENaC shows high selectivity for bothsodium and lithium ions, and the channel is upregu-lated by aldosterone and is inhibited by spironolac-tone. Amiloride is known to inhibit lithium uptake bythe collecting duct and has been used clinically to treatnephrogenic DI caused by lithium. A study of 45patients who were on long-term lithium and 42 controlsubjects with a mood disorder but no lithium treatmentshowed impaired urine-concentrating ability and re-duced urinary AQP2 and cAMP excretion correlatedwith the duration of lithium therapy. Eleven of thepatients were enrolled in a randomized, placebo-con-trolled trial to investigate the action of amiloride (10mg/d for 6 wk) on desmopressin-stimulated urine-concentrating ability and AQP2 excretion. After 6 wkof amiloride therapy but not after placebo, urine os-molality after desmopressin increased by 64.5 � 8.0%(P � 0.05) in association with increased urinary AQP2excretion (10).Hypercalcemia and Hypercalciuria. Calcium re-ceptors (CaR) expressed on the basolateral membraneof the thick ascending limb and the luminal membraneof collecting duct can affect the ability to concentratethe urine, and hypercalcemia causes polyuria. CaRactivation by hypercalcemia inhibits the Na-K-2Cltransporter on the ascending limb, reducing the med-ullary concentration gradient in a manner analogous tofurosemide (15). A high luminal calcium concentra-tion has been shown to activate the CaR, reducingcoupling efficiency between the vasopressin 2 (V2)receptor and adenylate cyclase via a calmodulin-de-pendent mechanism in cultured cortical collecting ductcells (16).Congenital Nephrogenic DI. X-linked nephrogenicDI is primarily a disease of males, whereas femaleheterozygotes may have mild polyuria and polydipsiabecause of skewed inactivation of the X chromosome(1). X-linked DI is caused by a loss-of-function mu-tation of the gene that encodes the V2 receptor(AVPR2). A total of 193 disease-causing mutations ofAVPR2 have been identified, 95 of which result in a
150 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

misfolded protein that becomes trapped in the endo-plasmic reticulum, unable to reach the basolateral cellmembrane of the cell, where it can function as avasopressin receptor. There is a great deal of interestin developing pharmacologic chaperones to promoteescape of the misfolded protein from the endoplasmicreticulum. Vasopressin analogues can bind with mis-folded receptors, causing them to refold, escaping theendoplasmic reticulum and reaching the plasmamembrane, where endogenous vasopressin can sub-sequently displace the analogue and activate thereceptor. Administration of an investigational V1a
vasopressin antagonist, SR49059, which seems to actas a chaperone, slightly increased urine osmolality infive patients with nephrogenic DI (1). Other potentialstrategies for treating the disease include activation ofthe nitric oxide–cGMP signaling pathway, which mayplay a role in AQP2 trafficking; sildenafil, a selectiveinhibitor of cGMP phosphodiesterase, increases intra-cellular cGMP and increases insertion of AQP2 in theapical membrane of principal cells in the outer med-ullary collecting duct but not the cortical collectingduct, the major site of water reabsorption (17).
Nephrogenic DI, resulting from mutations of thegene encoding AQP2, was first recognized in a Dutchmale patient with nephrogenic DI that did not seem tobe X linked; the patient responded to desmopressinwith an increase in factor VIII, von Willebrand factor,and tissue-type plasminogen and a decrease in BP.These normal V2 receptor–mediated responses sug-gested that extrarenal receptors were intact. Subse-quently, the patient was found to harbor two pointmutations in the AQP2 gene on chromosome 12,encoding the AQP2 water channel. Approximately10% of patients with congenital nephrogenic DI havemutations of the AQP2 gene; of these, �90% haverecessively inherited disease. To date, 39 mutations inAQP2 have been reported, and 32 are associated withrecessive nephrogenic DI. In the recessive form of thedisease, polyuria and polydipsia are present at birth,whereas in the much rarer dominant form, these fea-tures appear in the second year of life or later. Genemutations, which have now been identified in sevenfamilies, are inherited as a recessive trait. Urine os-molality in the recessive disease never exceeds 200mOsm/kg, whereas, in the dominant form, higherurine osmolality can be found, and some patientsrespond to desmopressin or dehydration with a tran-sient increase in urine osmolality. AQP2 proteins in
dominant nephrogenic DI have mutations in theCOOH terminus of the protein; they are functionalwater channels that are mis-sorted, failing to reach theluminal membrane of principal cells in the collectingduct, moving instead to other parts of the cell, wheremost of them are retained by lysosomes, stored inother vesicles, or routed to the basolateral membrane.Strategies to increase basolateral membrane AQP2abundance by reducing their removal by endocytosisare currently under investigation; statins are potentialcandidates for this strategy (17).
Some patients with congenital nephrogenic DIhave a mild phenotype that responds to AVP. Onevariant of autosome recessive disease manifest bymarked polyuria and polydipsia responded to desmo-pressin with a modest improvement in urine osmolal-ity and a subjective improvement in polyuria andthirst. Presumably, the mutant water channel was par-tially functional and was better able to route to itstarget apical membrane in response to antidiuretichormone (18).Nocturnal Enuresis and Nocturnal Polyuria. Noc-turnal enuresis and nocturnal polyuria are related dis-orders that affect children and elderly patients, respec-tively. Neither syndrome is well understood, and theyboth share elements of vasopressin deficiency andimpaired response to vasopressin. Both have beentreated with desmopressin, and, as discussed previ-ously, this sometimes causes hyponatremia.
Nocturnal enuresis is a children’s disease char-acterized by urine loss during the night at an age whenbladder control is usually present. Normally, urineproduction at night is reduced by a nocturnal increasein vasopressin secretion, which may be blunted inchildren with enuresis. In addition, approximately40% of children with enuresis have hypercalciuria,which may reduce the response to vasopressin byreducing the amount of AQP2 that reaches the luminalmembrane in response to the hormone (15). In chil-dren who have enuresis and whose nocturnal vasopres-sin levels are lower than that of control children, theday-night ratio of AVP2 is approximately twice ashigh as in children without enuresis. When low noc-turnal vasopressin levels are associated with hypercal-ciuria, the day-night ratio of AQP2 is nearly three-foldnormal. Treatment of patients who have hypercalciuriawith a low-calcium diet and desmopressin restores theday-night AQP2 ratios to normal, and with suspensionof the low-calcium diet, bedwetting recurred despite
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 151

continued therapy with desmopressin. The failure ofpatients to awake before, during, or after voiding is notwell explained by either low levels of vasopressin ormild nephrogenic DI caused by hypercalciuria.Robben et al. (19) described two patients with primarynocturnal enuresis and co-segregating nephrogenic DIcaused by mutations in the AQP2 gene and one patientwith a co-segregating mutation in the AVPR2 gene.Despite the mutations and despite continuing largeurine volumes at night, enuresis responded to desmo-pressin; on the drug, the patients aroused in responseto the sensation of a full bladder and went to thebathroom. In the patient with the AVPR2 gene muta-tion, urinary calcium levels were low. These findingssuggest that success of desmopressin in nocturnalenuresis is not dependent on the urine-concentratingmechanism, activation of the V2 receptor, or insertionof AQP2 in the luminal membrane. The authors sug-gested that desmopressin acts on the V1b receptor,which has a similar affinity for desmopressin as theV2R receptor and is localized in the brain. The affect ofspecific agonists for this receptor awaits further study.
Nocturnal polyuria is a syndrome that occursprimarily in older patients and in which the day-nightratio of urine production is altered in a manner similarto that seen in children with nocturnal enuresis. Al-though urine output is normal, more than one third ofurine output occurs at night, and, in some affectedpatients, urine production at night may exceed thatduring the day. Low nocturnal levels of AVP havebeen found in some but not all patients.
References1. Bichet DG: Vasopressin receptor mutations in nephrogenic diabetes
insipidus. Semin Nephrol 28: 245–251, 20082. Loh JA, Verbalis JG: Diabetes insipidus as a complication after
pituitary surgery. Nat Clin Pract Endocrinol Metab 3: 489–494,2007
3. Loh JA, Verbalis JG: Disorders of water and salt metabolism asso-ciated with pituitary disease. Endocrinol Metab Clin North Am 37:213–234, x, 2008
4. Bihan H, Christozova V, Dumas JL, Jomaa R, Valeyre D, Tazi A,Reach G, Krivitzky A, Cohen R: Sarcoidosis: Clinical, hormonal, andmagnetic resonance imaging (MRI) manifestations of hypothalamic-
pituitary disease in 9 patients and review of the literature. Medicine(Baltimore) 86: 259–268, 2007
5. Miyoshi T, Otsuka F, Takeda M, Inagaki K, Otani H, Ogura T, IchikiK, Amano T, Makino H: An elderly patient with sarcoidosis mani-festing panhypopituitarism with central diabetes insipidus. Endocr J54: 425–430, 2007
6. Mavrakis AN, Tritos NA: Diabetes insipidus with deficient thirst:Report of a patient and review of the literature. Am J Kidney Dis 51:851–859, 2008
7. Crowley RK, Sherlock M, Agha A, Smith D, Thompson CJ: Clinicalinsights into adipsic diabetes insipidus: A large case series. ClinEndocrinol (Oxf) 66: 475–482, 2007
8. Hayashi T, Murata M, Saito T, Ikoma A, Tamemoto H, KawakamiM, Ishikawa SE: Pathogenesis of chronic hypernatremia with dehy-drated and non-dehydrated states in hypothalamic space-occupyinglesions. Endocr J 55: 651–655, 2008
9. Holley AD, Green S, Davoren P: Extreme hypernatraemia: A casereport and brief review. Crit Care Resusc 9: 55–58, 2007
10. Bedford JJ, Weggery S, Ellis G, McDonald FJ, Joyce PR, Leader JP,Walker RJ: Lithium-induced nephrogenic diabetes insipidus: Renaleffects of amiloride. Clin J Am Soc Nephrol 3: 1324–1331, 2008
11. Wilting I, Baumgarten R, Movig KL, van Laarhoven J, Apperloo AJ,Nolen WA, Heerdink ER, Knoers NV, Egberts AC: Urine osmolality,cyclic AMP and aquaporin-2 in urine of patients under lithiumtreatment in response to water loading followed by vasopressinadministration. Eur J Pharmacol 566: 50–57, 2007
12. Nielsen J, Kwon TH, Christensen BM, Frokiaer J, Nielsen S: Dys-regulation of renal aquaporins and epithelial sodium channel inlithium-induced nephrogenic diabetes insipidus. Semin Nephrol 28:227–244, 2008
13. Kim GH, Choi NW, Jung JY, Song JH, Lee CH, Kang CM, KnepperMA: Treating lithium-induced nephrogenic diabetes insipidus with aCOX-2 inhibitor improves polyuria via upregulation of AQP2 andNKCC2. Am J Physiol Renal Physiol 294: F702–F709, 2008
14. Nielsen J, Kwon TH, Frokiaer J, Knepper MA, Nielsen S: Lithium-induced NDI in rats is associated with loss of alpha-ENaC regulationby aldosterone in CCD. Am J Physiol Renal Physiol 290: F1222–F1233, 2006
15. Procino G, Mastrofrancesco L, Mira A, Tamma G, Carmosino M,Emma F, Svelto M, Valenti G: Aquaporin 2 and apical calcium-sensing receptor: New players in polyuric disorders associated withhypercalciuria. Semin Nephrol 28: 297–305, 2008
16. Bustamante M, Hasler U, Leroy V, de Seigneux S, Dimitrov M,Mordasini D, Rousselot M, Martin PY, Feraille E: Calcium-sensingreceptor attenuates AVP-induced aquaporin-2 expression via a calm-odulin-dependent mechanism. J Am Soc Nephrol 19: 109–116, 2008
17. Bouley R, Hasler U, Lu HA, Nunes P, Brown D: Bypassing vaso-pressin receptor signaling pathways in nephrogenic diabetes insipi-dus. Semin Nephrol 28: 266–278, 2008
18. Linshaw MA: Back to basics: Congenital nephrogenic diabetes in-sipidus. Pediatr Rev 28: 372–380, 2007
19. Robben JH, Sze M, Knoers NV, Eggert P, Deen P, Muller D: Reliefof nocturnal enuresis by desmopressin is kidney and vasopressin type2 receptor independent. J Am Soc Nephrol 18: 1534–1539, 2007
152 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

The Editorial Board of NephSAP extends its sincere appreciation to the following reviewers. Their efforts and insights have helped toimprove the quality of this postgraduate education offering.
NephSAP Review PanelGeorgi Abraham, MDSri Ramachandra Medical Collegeand HospitalChennai, IndiaPablo H. Abrego, MD, FASNMarshfield ClinicWausau, WIAnil K. Agarwal, MD, FASNOhio State UniversityColumbus, OHKamal E. Ahmed, MD, FASNYuma Nephrology, PCYuma, AZAdel E. Berbari, MDAmerican University of Beirut-MedicalCenterBeirut, LebanonBruce E. Berger, MDUniversity Hospitals, Case Medical CenterCleveland, OHPaul Bolin, MDBrody School of Medicine at EastCarolina UniversityGreenville, NCMauro Braun, MDCleveland Clinic FloridaWeston, FLLaurence E. Carroll, MD, FASNHypertension & Kidney SpecialistsLancaster, PAJorge Cerda, MD, FASNCapital District Renal PhysiciansAlbany, NYChokchai Chareandee, MD, FASNRegions HospitalSt. Paul, MNMahmoud El-Khatib, MD, PhD,FASNUniversity of CincinnatiCincinnati, OHLynda A. Frassetto, MD, FASNUniversity of California at San FranciscoSan Francisco, CADuvuru Geetha, MDJohns Hopkins UniversityBaltimore, MD
Richard N. Hellman, MDIndiana University School of MedicineIndianapolis, IN
R. Morrison Hurley, MDUniversity of British ColumbiaVancouver, BC, Canada
Ekambaram Ilamathi, MD, FASNSuffolk Nephrology ConsultantStony Brook, NY
Sharon L. Karp, MDIndiana University School of MedicineIndianapolis, IN
Pranay Kathuria, MD, FASNUniversity of Oklahoma College ofMedicineTulsa, OK
Quresh T. Khairullah, MD, FASNSt. Clair Specialty PhysiciansDetroit, MI
Ramesh Khanna, MDUniversity of Missouri, ColumbiaColumbia, MO
Edgar V. Lerma, MD, FASNUniversity of Illinois at ChicagoCollege of MedicineChicago, IL
Philippe Madhoun, MDChu CharleroiCharleroi, Belgium
Jolanta Malyszko, MD, FASNMedical UniversityBialystok, Poland
Hanna W. Mawad, MD, FASNUniversity of KentuckyLexington, KY
Pascal Meier, MD, FASNCentre Hospitalier Universitaire VaudoisLausanne, Switzerland
Jacob Mooij, MD, PhDAl Hada HospitalTaif, Saudi Arabia
Mamiko Ohara, MD, FASNKameda Medical CenterChiba, Japan
Pairach Pintavorn, MD, FASNEast Georgia Kidney and HypertensionAugusta, GA
Paul H. Pronovost, MD, FASNYale University School of MedicineWaterbury, CT
Mohammad A. Quasem, MD, FASNState University of New YorkBinghampton, NY
Venkat Ramanathan, MD, FASNBaylor College of MedicineHouston, TX
Robert Richardson, MDUniversity of Toronto and TorontoGeneral HospitalToronto, ON, Canada
Bijan Roshan, MDJoslin Diabetes Center HarvardMedical SchoolBoston, MA
Mohammad G. Saklayen, MDWright State UniversityDayton, OH
Ramesh Saxena, MD, PhDUniversity of Texas SouthwesternMedical CenterDallas, TX
Gaurang M. Shah, MDLong Beach VA Healthcare SystemLong Beach, CA
Neil E. Soifer, MD, FASNLakeside Nephrology, LTDChicago, IL
Harold Szerlip, MD, FASNMedical College of GeorgiaAugusta, GA
Luigi Vernaglione, MDM. Giannuzzi HospitalManduria, Italy
Antonio R. Vilches, MD, PhDInstituto Universitario CemicBuenos Aires, Argentina
NephSAP®
Volume 8, Number 2, March 2009

Program Mission and ObjectivesThe mission of the Nephrology Self-Assessment Program (NephSAP) is to regularly provide a vehicle that will be useful for clinicalnephrologists who seek to renew and refresh their clinical knowledge and diagnostic and therapeutic skills. This Journal consists of aseries of challenging, clinically oriented questions based on case vignettes, a detailed Syllabus that reviews recent publications,and an Editorial on an important and evolving topic. Taken together, these parts should assist individual clinicians under-taking a rigorous self-assessment of their strengths and weaknesses in the broad domain of nephrology.
Accreditation and Credit DesignationThe American Society of Nephrology is accredited by the Accreditation Council for Continuing Medical Education to provide con-tinuing medical education for physicians.
The ASN designates this educational activity for a maximum of 8.0 AMA PRA Category 1 Credits™. Physicians should only claimcredit commensurate with the extent of their participation in the activity.
Continuing Medical Education (CME) Information
Date of Original Release: March 2009Examination Available Online: Monday, March 9, 2009
CME Credit Eligible Through: February 28, 2010
Answers: Correct answers with explanations will be posted on the ASN website in March 2010 when the issue is archived.UpToDate Links Active: March and April 2009
Core Nephrology question links active: March, April, and May 2009.
CME Credit: 8.0 AMA PRA Category 1 Credits™
Target Audience: Nephrology Board and recertification candidates, practicing nephrologists, and internists.
Method of Participation:● Read the syllabus that is supplemented by original articles in the reference lists, and complete the online self-assessment
examination.● Examinations are available online only after the first week of the publication month. There is no fee. Each participant is
allowed two attempts to pass the examination (�75% correct).● Your score and a list of question/s (by number) answered incorrectly can be printed immediately.● Your CME certificate can be printed immediately after passing the examination.● Answers and explanations are provided ONLY with a passing score on the first or second attempt.● Your ASN transcript will be updated in 6 to 8 weeks after passing the examination.
Instructions to access the Online CME Center to take the examination and complete the evaluation:● Access the ASN website: www.asn-online.org● Click on “CME” tab at the top of the homepage and then click on the Online CME Center icon to go to the login page.● After login, click on the icon for “NephSAP”● Select a topic and click on “Start Now”● On the CME Information page, click on “Continue”● On the MOC page, select whether or not you want MOC points.● On the next page, click on “Examination Questions/Evaluation” to answer the questions.● Your score and a list of question numbers answered incorrectly can be printed immediately.● Follow the prompts to retake the examination if you failed, or print your certificate and the correct answers if you passed.● You can retake the examination at any time. Each participant is allowed two attempts.
NephSAP®
Volume 8, Number 2, March 2009

Instructions to Obtain American Board of Internal Medicine (ABIM) Maintenance of Certification(MOC) Points:
Each issue of NephSAP provides 10 MOC points. Respondents must meet the following criteria:● Be certified by ABIM in internal medicine and/or nephrology and must be enrolled in the ABIM–MOC program
via the ABIM website (www.abim.org).● Pass the self-assessment examination within the timeframe specified in this issue of NephSAP.● Designate the issue for MOC points by clicking on the MOC link on the CME certificate page after passing the examination.
You will be leaving the ASN-CECity site and transferring the information directly to the ABIM in real-time.● Provide your ABIM Certificate ID number and your date of birth.● You will receive a confirmation message from the ABIM indicating the receipt of your information.
MOC points will be applied to only those ABIM candidates who have enrolled in the program. It is your responsibility to completethe ABIM MOC enrollment process.
Instructions to access the ASN website, NephSAP, and the UpToDate link
Compatible Browser: The ASN website (asn-online.org) has been formatted for cross-browser functionality, and shoulddisplay correctly in all modern web browsers. We recommend that you use Internet Explorer.
Monitor Settings: The ASN website was designed to be viewed in a 1024 � 768 or higher resolution.
Technical Support: If you are having difficulty viewing any of the pages, please refer to the ASN technical support pagefor possible solutions. If you continue having problems, contact Hal Nesbitt at [email protected] provides an additional source of information that should help you answer up to 5 selected NephSAPquestions from each issue. The link is free and will remain active for the first 60 days after publication for eachissue.
● On the ASN home page, double click on the NephSAP link (NephSAP cover) on the bottom side of the page.● On the NephSAP page, click on the UpToDate button on the left hand side to access the current links.
NephSAP®
Volume 8, Number 2, March 2009

Disclosure InformationThe ASN is responsible for identifying and resolving all conflicts of interest prior to presenting any educational activity to learners to ensurethat ASN CME activities promote quality and safety, are effective in improving medical practice, are based on valid contents, and are inde-pendent of the control from commercial interests and free of commercial bias. All faculty are instructed to provide balanced, scientificallyrigorous and evidence-based presentations. In accordance with the disclosure policies of the Accreditation Council for Continuing MedicalEducation (ACCME) as well as guidelines of the Food and Drug Administration (FDA), individuals who are in a position to control the con-tent of an educational activity are required to disclose relationships with a commercial interest if (a) the relation is financial and occurredwithin the past 12 months; and (b) the individual had the opportunity to affect the content of continuing medical education with regard to thatcommercial interest. For this purpose, ASN consider the relationships of the person involved in the CME activity to include financial relation-ships of a spouse or partner. Peer reviewers are asked to abstain from reviewing topics if they have a conflict of interest. Disclosure informa-tion is made available to learners prior to the start of any ASN educational activity.
Agarwal, Rajiv—Grants/research support: Abbott; Consultant/Scientific advisor: Rockwell Medical, Watson Pharma; Honoraria: Abbott,Astra-Zeneca, Merck
Berns, Jeffrey S.—Consultant: Baxter, Affymax; Advisory Board: Amgen, LitholinkCohen, David J.—Grants/research support: Novartis, Roche; Honoraria: RocheFishbane, Steven—noneFuchs, Elissa (Medical Editor)—noneGlassock, Richard J.—Consultant: Aspreva, FibroGen, Novartis, Genentech, Keryx, Quest Diagnostics/Nichols Institute, Science
Partners; Honoraria: Visiting professorships at various medical schools; Ownership Interests: LaJolla Pharmaceutical; Paid ExpertTestimony: Various legal firms regarding product reliability; Royalties: Lippincott Williams and Wilkins, Textbook of Nephrology;Scientific Advisor or Membership: American Renal Associates, Aspreva, Los Angeles Biomedical Institute, University KidneyResearch Associates
Goldfarb, Stanley—Consultant: Lupitold, Omeros; Ownership Interests: Polymedix; Honoraria: GE Healthcare, Fresenius; ExpertTestimony: Bayer; Editorial Board: Journal of Clinical Investigation
Martin, Kevin J.—Grants/research support/honoraria: Abbott; Advisory Board: Abbott, CytochromaMehrotra, Rajnish—Grants/research support: Amgen, Baxter, Shire; Consultant: Novartis; Honoraria: AMAG, Baxter Healthcare,
ShireMurray, Patrick T.—Grants/research support: Biosite, GlaxoSmithKline, NxStage Medical; Consultant: Scios; Honoraria: GE
Healthcare; Advisory Board: NxStage Medical, Quantum BiotechnologiesNachman, Patrick H.—Grants/research support: OtsukaPalevsky, Paul M.—nonePalmer, Biff F.—Honoraria: Boehringer Ingelheim, NorvartisSterns, Richard H.—Consultant: Astellas, Otsuka; Honoraria: Astellas, Otsuka; UpToDate; Scientific advisor: UpToDateTextor, Stephen C.—Honoraria: Visiting professorships; Editorial Board Membership: Journal of the American Society of
Nephrology; Royalties: Lippincott Williams and Wilkins, Handbook of Kidney TransplantationTownsend, Raymond R.—Consultant: Abbott Laboratories, Atcor Medical, GlaxoSmithKline; Research support: Novartis; Honoraria:
Bristol Myers-Squibb, Pfizer; Other financial relationship: UpToDate, PIER (ACP/ASIM)Vella, John P.—noneEditorial authors:Ackerman, Teresa F.—noneArtunc, Ferruh—noneBoini, Krishna—noneKempe, Daniela S.—noneLang, Florian—noneVallon, Volker—noneReview Commentary Author:Berl, Tomas—Grants/research support/scientific advisor: Otsuka; Honoraria: Astellas
NephSAP®
Volume 8, Number 2, March 2009

Nephrology Self-Assessment Program
Examination QuestionsInstructions to obtain 8 AMA PRA Category 1 CreditsTM
Credit expiration date: February 28, 2010
Continuing Medical Education (CME) Information
Date of Original Release: March 2009Examination Available Online: Monday, March 9, 2009
CME Credit Eligible Through: February 28, 2010
Answers: Correct answers with explanations will be posted on the ASN website in March 2010 when the issue is archived.UpToDate Links Active: March and April 2009
Core Nephrology question links active: March, April, and May 2009.
CME Credit: 8.0 AMA PRA Category 1 Credits™
Target Audience: Nephrology Board and recertification candidates, practicing nephrologists, and internists.
Method of Participation:● Read the syllabus that is supplemented by original articles in the reference lists, and complete the online self-assessment
examination.● Examinations are available online only after the first week of the publication month. There is no fee. Each participant is
allowed two attempts to pass the examination (�75% correct).● Your score and a list of question/s (by number) answered incorrectly can be printed immediately.● Your CME certificate can be printed immediately after passing the examination.● Answers and explanations are provided ONLY with a passing score on the first or second attempt.● Your ASN transcript will be updated in 6 to 8 weeks after passing the examination.
Instructions to access the Online CME Center to take the examination and complete the evaluation:● Access the ASN website: www.asn-online.org● Click on “CME” tab at the top of the homepage and then click on the Online CME Center icon to go to the login page.● After login, click on the icon for “NephSAP”● Select a topic and click on “Start Now”● On the CME Information page, click on “Continue”● On the MOC page, select whether or not you want MOC points.● On the next page, click on “Examination Questions/Evaluation” to answer the questions.● Your score and a list of question numbers answered incorrectly can be printed immediately.● Follow the prompts to retake the examination if you failed, or print your certificate and the correct answers if you passed.● You can retake the examination at any time. Each participant is allowed two attempts.
Instructions to Obtain American Board of Internal Medicine (ABIM) Maintenance of Certification(MOC) Points:
Each issue of NephSAP provides 10 MOC points. Respondents must meet the following criteria:● Be certified by ABIM in internal medicine and/or nephrology and must be enrolled in the ABIM–MOC program
via the ABIM website (www.abim.org).● Pass the self-assessment examination within the timeframe specified in this issue of NephSAP.● Designate the issue for MOC points by clicking on the MOC link on the CME certificate page after passing the examination.
You will be leaving the ASN-CECity site and transferring the information directly to the ABIM in real-time.● Provide your ABIM Certificate ID number and your date of birth.● You will receive a confirmation message from the ABIM indicating the receipt of your information.
MOC points will be applied to only those ABIM candidates who have enrolled in the program. It is your responsibility to completethe ABIM MOC enrollment process.
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009
154

Volume 8, Number 2, March 2009 –Fluid, Electrolyte, and Acid-Base Disturbances1. A 47-yr-old man presents with new-onset as-
cites. He has a significant history of heavyalcohol use during the past several years. Hislast drink was approximately 12 h ago. Onphysical examination, BP is 110/70 mmHg,pulse is 110, and respiratory rate is 28. Spiderangiomas are noted on the skin. The abdomenshows shifting dullness, and there is 2� periph-eral edema. Laboratory examination shows thefollowing: Na� 130 mEq/L, K� 2.8 mEq/L, Cl�
90 mEq/L, HCO3 14 mEq/L, phosphate 3.5mg/dl, calcium 6.5 mg/dl, and magnesium 1.6mg/dl. Urine and serum ketones are positive.The patient is admitted and treated with thia-mine, folic acid, and multivitamins followed bymaintenance fluids with D5% 1/2NS. Approxi-mately 18 h after admission, the patient is rest-less and agitated and complains of severe weak-ness. The serum phosphate concentration is 0.9mg/dl.
Which ONE of the following is TRUE re-garding the change in serum phosphate inthis patient?
A. On admission, total-body phosphate waslikely normal.
B. Alcoholic ketoacidosis tends to cause ashift of phosphate into cells.
C. Respiratory alkalosis that develops in asso-ciation with alcohol withdrawal shiftsphosphate into cells.
D. The weakness is likely due to hypermagnese-mia developing during the hospitalization.
2. A 38-yr-old man with a known history re-ceives a diagnosis of chronic liver diseasesecondary to hepatitis C. He is treated with a24-wk course of pegylated IFN-�-2a, com-bined with ribavirin. He tolerates the therapywithout complications. Four weeks after com-pleting treatment, he begins to complain ofepisodic weakness in the proximal limbs, par-ticularly in the early-morning hours. He statesthat on one occasion, his weakness suddenly
became worse immediately after completing a30-min run on a treadmill. One day beforeadmission, he developed sudden weakness afterfinishing his dessert at a work-associated ban-quet. He is on no medications. Physical exami-nation reveals the following: BP 140/70 mmHg,pulse 120, and respiratory rate (RR) 18. There isno ophthalmopathy or lymphadenopathy. Thethyroid gland is normal on palpation. He isnoted to have severe symmetrical proximalweakness in the thighs (1/5) with intact distalmuscle power. Laboratory examination revealsthe following: White blood cell (WBC) count7.8 mm3, Hg 13.5 gm/dl, Na 142 mEq/L, K 2.1mEq/L, Cl 104 mEq/L, HCO3 23 mg/dl, creati-nine 1.0 mg/dl, and blood urea nitrogen (BUN)15 mg/dl. Urine chemistries are as follows: Na96 mEq/L, K 10 mEq/L, and Cl 110 mEq/L. Thethyroid stimulating hormone is 0.1 �IU/ml.
Which ONE of the following statements isTRUE regarding the underlying cause ofweakness in this patient?
A. This disorder tends to occur more fre-quently in women.
B. The patient should be immediately startedon acetazolamide for treatment of theweakness.
C. Pegylated IFN was likely responsible forprecipitating this disorder.
D. The serum magnesium is likely to be in-creased.
E. High K� intake is known to exacerbatethis disorder.
3. A 68-yr-old man presents 2 wk after havingundergone surgical treatment for a hip fracture.During the past 3 to 4 d, he has noticed abdom-inal distention and diarrhea. Physical examina-tion shows decreased bowel sounds and a mildlytender abdomen but no rebound tenderness. Ab-domen percussion is tympanitic. Imaging stud-ies reveal a markedly dilated colon with nosmall intestine dilation. Laboratory findings
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 155

show the following: Na 151 mEq/L, K 1.9mEq/L, Cl 120 mEq/L, and HCO3 16 mEq/L.Despite the use of a rectal tube for drainage ofstool and flatus, the patient continues to mani-fest colonic distention, and a diagnosis of co-lonic pseudo-obstruction is made. Over 8 wk,the patient’s gastrointestinal manifestations re-solve spontaneously.
Which ONE of the following findings ischaracteristic of the diarrhea found in pa-tients with colonic pseudo-obstruction?
A. Secretory diarrhea as a result of inhibitionof active intestinal absorption of NaCl
B. Secretory diarrhea as a result of active Cl�
secretion followed by passive Na� secre-tion
C. Markedly increased stool osmotic gap
D. Secretory diarrhea as a result of activecolonic K� secretion
4. A 58-yr-old man with type 2 diabetes and stage3 chronic kidney disease receives a diagnosis oftransitional cell carcinoma of the bladder. Hehas received chemotherapy and radiation ther-apy during the past year for treatment of thisdisorder. His clinical course has been compli-cated by the development of an enterocutaneousfistula. The surgical team now recommends thatthe patient undergo a radical cystectomy. Giventhe likelihood of extensive pelvic fibrosis andpresence of the fistula, the surgeons are con-cerned that the procedure will be complicated.The surgeons inform the patient that a urinarydiversion into the bowel will be performed, butthe segment of bowel used can be determinedonly at the time of the procedure. Preoperativelaboratory examination shows the following: Na138 mEq/L, K 4.7 mEq/L, Cl 100 mEq/L, HCO3
22 mEq/L, and creatinine 1.8 mg/dl. The patientundergoes the procedure without complications.Repeat laboratory examination 7 d after theprocedure shows the following values: Na 138mEq/L, K 2.9 mEq/L, Cl 85 mEq/L. HCO3 36mEq/L, pH 7.51, and creatinine 1.7 mg/dl.
On the basis of postoperative laboratoryvalues, which ONE of the following seg-
ments of bowel did the surgeon use for theurinary diversion procedure?
A. Stomach
B. Jejunum
C. Ileum
D. Sigmoid colon
� 5. A 33-yr-old African American man withsickle cell disease presents with severe backpain typical of sickle cell crisis. His medicalhistory is pertinent for frequent episodes ofhemolytic crisis. The patient was not on di-uretic therapy. Physical examination shows ananxious man in mild discomfort with BP of156/94 mmHg, pulse 98, RR 22. There isscleral icterus. Lung examination shows basi-lar crackles, and he has hepatomegaly andtrace peripheral edema. Laboratory examina-tion shows hematocrit of 21%, reticulocytecount of 12%, and total bilirubin of 38 mg/dl.Chemistry studies reveal the following: Na136 mEq/L, K 2.2 mEq/L, Cl 85 mEq/L,HCO3 29 mEq/L, and creatinine 0.6 mg/dl.Urine studies reveal the following: Na 63mEq/L, K 49 mEq/L, Cl 58 mEq/L, plasmarenin activity 1.1 ng/ml per h (3 to 9 ng/ml perh), and aldosterone 2 ng/dl (n � 10). The patientis treated with exchange transfusion and given Ksupplements to correct the hypokalemia. BP atthe time of discharge is 118/78 Hg, and labora-tory studies show a total bilirubin of 8 mg/dl anda serum potassium of 4.1 mEq/L off potassiumsupplements. Five months later, the patient isreadmitted with a hemolytic crisis. BP is againnoted to be increased at 158/98 mmHg. Labora-tory examination shows a total bilirubin of 45mg/dl. The serum potassium is 2.1 mEq/L. Atranstubular K gradient at this time shows avalue of 12. The serum aldosterone is 2.5 ng/dl.
Which ONE of the following is the BESTexplanation for the recurrent hypokalemiain this patient?
A. Liddle syndrome
B. Shift of K into cells
C. Acquired deficiency of 11�-hydroxysteroiddehydrogenase II
156 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

D. Surreptitious loop diuretic use
E. Dexamethasone-suppressible hyperaldoste-ronism
6. A 45-yr-old man with ESRD presents to theemergency department with the chief complaintof palpitations and weakness. He has been stableon dialysis for 2 yr. He had an aortic valvereplacement as a result of rheumatic aortic ste-nosis approximately 4 yr ago. Physical exami-nation shows a pleasant, slightly anxious man inno acute distress. The BP is 100/65 mmHg, andthe pulse is 180 bpm. An electrocardiogramshows atrioventricular nodal reentrant tachycar-dia. Laboratory examination shows the follow-ing: Na 136 mEq/L, K 8.2 mEq/L, Cl 100mEq/L, HCO3 19 mEq/L, creatinine 12 mg/dl,BUN 68 mg/dl, hemoglobin 8.1 g/dl, lactatedehydrogenase 512 U/L (normal 100 to 190U/L), and indirect bilirubin 4.5 mg/dl. Hyperka-lemia has not been an issue for this patientbefore. His most recent Kt/V is 1.5. His diet isunchanged, and he has not missed any dialysistreatments.
Which ONE of the following is the BESTexplanation for the hyperkalemia in thispatient?
A. Recirculation in vascular access
B. Use of an angiotensin-converting enzymeinhibitor (ACEI)
C. Hemolysis as a result of shear stress acrossthe prosthetic aortic valve
D. Disseminated intravascular coagulationsecondary to methycillin-resistant Staphy-lococcus aureus
E. Occult hyperthyroidism
7. Which ONE of the following is TRUE regard-ing the risk for developing hyperkalemia inassociation with packed red blood cell trans-fusion?
A. Hyperkalemia risk is related to the numberbut not the rate of red blood cell transfu-sions.
B. Washing cells before transfusion increaseshyperkalemia risk.
C. Increasing the amount of additive solutionminimizes hyperkalemia risk.
D. Hyperkalemia risk is increased with use ofirradiated blood.
E. Hyperkalemia risk is inversely related tothe duration of blood storage.
8. A 14-yr-old boy was observed to collapse on atennis court during a midmorning practice session.He was conscious and oriented but unable to movehis arms or legs. He stated that his last meal was at7:00 the night before. The weakness spontane-ously resolved during the course of 2 h. His historywas significant for several other episodes of inter-mittent weakness that all resolved within 30 to 45minutes after onset. On several of these occasions,the weakness occurred after the ingestion of largequantities of orange juice. Physical examinationreveals the following: BP 130/80 mmHg, pulse 86,RR 18, cranial nerves intact, and 1/5 strength in allmajor muscle groups. The sensory examination isnormal. Laboratory values that were obtained 30min after collapse reveal the following: Na 143mEq/L, K 5.7 mEq/L, Cl 100 mEq/L, HCO3 22mEq/L, and creatinine 0.9 mg/dl.
Which ONE the following statement is cor-rect regarding treatment of the underlyingdisease in this patient?
A. The patient should be prescribed a �
blocker to reduce the frequency of attacks.
B. ACEI therapy will decrease the frequencyof attacks.
C. He should initiate exercise or eat a high-carbohydrate meal to abort attacks.
D. Albuterol inhaler is likely to worsen theacute weakness.
� 9. A 38-yr-old woman with a strong family historyof cardiovascular diseases and hypertension re-cently received a diagnosis of essential hyper-tension. Her BP on three separate measurementsaverages 154/94 mmHg. Current medicationsinclude a daily multivitamin and birth controlpills. The physical examination and laboratoryexamination are normal. Because the patient isusing birth control pills, her primary care phy-
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 157

sician was comfortable prescribing lisinopril 10mg/d. One month later, the patient returns forfollow-up. BP is 142/88 mmHg. Laboratory ex-amination shows the following: Na 140 mEq/L,K 5.5 mEq/L, Cl 100 mEq/L, HCO3 22 mEq/L,creatinine 0.8 mg/dl, and BUN 10 mg/dl. Thephysician refers the patient to a nephrologist forhyperkalemia evaluation.
Which ONE of the following is the MOSTlikely risk factor for hyperkalemia develop-ment after prescribing an ACEI for thispatient?
A. High-grade bilateral renal artery stenosis
B. Pseudohypoaldosteronism type II
C. Acquired adrenal insufficiency
D. Mineralocorticoid-blocking activity in birthcontrol pill
E. Daily ingestion of bananas
�10. A 65-yr-old man is referred for evaluation of anincreased serum creatinine and hyperkalemia.The patient complains of intermittent abdominalpain during the past month. Medications includelisinopril/hydrochlorothiazide 10/25 mg/d forhypertension treatment for the past 7 yr. Hismedical history is significant only for a motorvehicle accident 8 mo ago, in which he sustaineda retroperitoneal bleed. Laboratory studies at thetime of discharge are normal. Physical exami-nation reveals BP of 158/94 mmHg and pulse of92 bpm. The remainder of the examination issignificant only for mild periumbilical tender-ness. Laboratory examination reveals the fol-lowing: WBC 9.0 mm3, hematocrit 32%, Na 138mEq/L, K 5.9 mEq/L, Cl 108 mEq/L, HCO3 19mEq/L, creatinine 2.3 mg/dl, and BUN 38 mg/dl. Urinalysis reveals specific gravity 1.010trace protein, 0 to 1 red blood cells, and 0 to 1WBC. An abdominal sonogram shows normal-sized kidneys with slight enlargement of theurinary pelvis on both sides. There is no hy-droureter.
Which ONE of the following is the MOSTlikely cause of the development of hyperka-lemia and renal failure in this patient?
A. Pseudohypoaldosteronism type 1
B. Use of over-the-counter nonsteroidal anti-inflammatory drugs
C. Urinary obstruction
D. ACEI therapy
E. Use of the herb Chan Su
11. A 38-yr-old man presents for evaluation ofchronic weakness. His family history is stronglypositive for hypertension. Physical examinationis remarkable only for a BP of 148/100 mmHg.Laboratory studies reveal the following: Na 141mEq/L, K 6.0 mEq/L, Cl 109 mEq/L, HCO3 19mEq/L, and creatinine 0.9 mg/dl. Urine studiesreveal he following: Na 75 mEq/L, K 20 mEq/L,and Cl 98 mEq/L. Subsequent workup disclosesthat the patient has pseudohypoaldosteronismtype II.
Which ONE of the following is correct re-garding this patient’s clinical disorder?
A. The patient’s hypertension would likely beresistant to treatment with hydrochlorothia-zide.
B. Plasma renin activity and aldosterone lev-els both are increased.
C. K excretion in response to NaCl loading isnormal.
D. An immunoblot assay would show in-creased urinary abundance of the Na-Clco-transporter.
E. The patient is likely to have an inactivat-ing mutation in the NaCl co-transporter inthe distal convoluted tubule.
12. A 5-yr-old boy is brought to the emergencydepartment because he complains of light-head-edness upon standing. The parents tell the phy-sician that their son has received a diagnosis ofa condition that causes potassium problems, butthey do not recall the name of the disease. Agreat grandfather is said to have experienced asimilar condition. The patient has required oralsalt supplementation as well as some other med-icine designed to help correct abnormalities inblood potassium, but the family has run out ofboth medications. Physical examination shows aBP of 95/70 mmHg that decreases to 80/55mmHg upon standing. Serum chemistries show
158 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

the following: Na 135 mEq/L, K 6.5 mEq/L, Cl105 mEq/L, HCO3 16 mEq/L, glucose 105 mg/dl, creatinine 1.0 mg/dl, and BUN 35 mg/dl. Anarterial blood gas shows a pH of 7.33 and a PCO2
of 32.
Which ONE of the following diagnoses isMOST likely in this case?
A. Pseudohypoaldosteronism type II
B. Pseudohypoaldosteronism type I
C. Liddle syndrome
D. Hyporeninemic hypoaldosteronism relatedto diabetic nephropathy
E. Long-term use of nonsteroidal anti-inflam-matory drugs
�13. A 38-yr-old man is referred for evaluation ofhypertension. He tells you that his father hashypertension and has problems with high K� inhis blood. Physical examination shows a BP of150/100 mmHg. Laboratory examination showsthe following: Na 140 mEq/L, K 6.2 mEq/L, Cl110 mEq/L, HCO3 16 mEq/L, creatinine 1.1mg/dl, and BUN 14 mg/dl. Plasma renin activityand aldosterone levels are markedly suppressed.He is placed on hydrochlorothiazide, and 3 wklater his BP and serum chemistries have largelynormalized. Genetic analysis shows that he hasan inactivating mutation of the WNK4 protein.
Which ONE of the following is correct re-garding Ca2� homeostasis in this patient?
A. A 24-hr urinary Ca2� excretion is ele-vated.
B. A 24-hr urinary Mg2� excretion is de-creased.
C. Urinary Ca2� excretion in this patient isunaffected by thiazide diuretics.
D. The activity of the selective Ca2� channelTRPV5 is increased.
E. Urinary Ca2� handling would be the samewith an activating mutation of WNK1.
14. A 30-yr-old woman is referred for evaluation ofa goiter. When she was 14 yr old, she had athyroid operation in which part of a goiter wasremoved. She was euthyroid at that time and hasremained euthyroid. She states that she has had
impaired hearing since childhood, and a recentexamination by an otolaryngologist showed en-largement of the endolymphatic duct and sac.BP is 110/70 mmHg. The remainder of thephysical examination is normal. Her baselinelaboratory examination is normal. The patient isplaced on 12.5 mg of hydrochlorothiazide in anattempt to treat the inner ear disorder. Twoweeks later, the patient presents with markedweakness and orthostasis. Laboratory examina-tion shows the following: Na 129 mEq/L, K 1.7mEq/L, Cl 70 mEq/L, HCO3 44 mEq/L, pH7.52, creatinine 1.1 mg/dl, and BUN 35 mg/dl.
Which ONE of the following disordersBEST accounts for the findings in this case?
A. Gitelman syndrome.
B. Pseudohypoaldosteronism type II
C. Congenital chloridorrhea
D. Pendred syndrome
E. Liddle syndrome
15. A 77-yr-old woman develops increased intraoc-ular pressure after cataract surgery and is treatedwith 2.5 L of 20% mannitol intravenously andoral ibuprofen for pain. Her history includescongestive cardiac failure, hypertension, andmild renal impairment with baseline creatinineof 1.5 mg/dl. Her regular medications includecaptopril and furosemide. On day 4, she devel-ops confusion, dyspnea, and anuria. Chest x-rayshows acute pulmonary edema. Laboratory datareveal the following: serum sodium of 112mEq/L, urea of 37 mg/dl, glucose of 90 mg/dl,creatinine of 3.2 mg/dl, and a serum osmolalityof 326 mOsm/kg. That same afternoon, shedevelops multiple seizures that require urgentventilation in an intensive care unit.
Which ONE of the following is the BESTemergency therapeutic intervention?
A. 100 ml 3% saline bolus intravenously fol-lowed by continuous veno-venous hemodi-afiltration using replacement fluid adjustedto a sodium concentration of 130 mEq/L
B. 40-mg bolus of conivaptan intravenously
C. Furosemide intravenously plus 3% salineat 1 ml/kg per h until the serum sodium is118 mEq/L
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 159

D. Continuous veno-venous hemodiafiltrationusing replacement fluid adjusted to a so-dium concentration of 118 mEq/L
E. Conventional hemodialysis against a dialy-sate with a sodium concentration of 140mEq/L
16. A 72-yr-old woman who has multiple sclerosisand weighs 50 kg receives 400 mg/kg intrave-nous immunoglobulin infused for 3 h. At the endof the infusion, she has an acute and dramaticworsening of neurologic symptoms. She is sud-denly unable to bear weight or coordinate armand leg movements and describes paresthesiasand hyposthesias of all extremities. Blood chem-istries are normal except for a serum sodium of130 mEq/L.
Which ONE of the following is the BESTtreatment for this patient?
A. 3% saline in 50-ml bolus
B. 3% saline in 150-ml bolus
C. 3% saline at 50 ml/h for 4 h
D. 0.9% saline, 1000 ml, infused as rapidly aspossible with furosemide 80 mg intrave-nously
E. Make patient nil per os and observe
�17. A 50-yr-old man with hemophilia complicated byHIV/AIDS and cirrhosis caused by hepatitis C isadmitted for renal failure. He is treated with furo-semide and spironolactone for management ofascites and sulfamethoxazole and trimethoprim forprophylaxis against Pneumocystis jiroveci pneu-monia. There is no history of alcoholism. Onadmission, BP is 98/62 mmHg, and physical ex-amination shows scleral icterus, stigmata of cirrho-sis, an abdominal fluid wave, and pitting edema ofhis lower extremities. He is alert and oriented buthas asterixis.Laboratory data show serum Na 128 mEq/L, K 5.7mEq/L, Cl 95 mEq/L, CO2 23 mEq/L, BUN 49mg/dl, glucose 110 mg/dl, and creatinine 2.3 mg/dl, and plasma osmolality 290 mOsm/kg. Urineosmolality is 580 mOsm/kg. Other laboratory val-ues included urine Na 53 mEq/L, random cortisol25 �g/dl, uric acid 14.2 mg/dl, serum triglycerides50 mg/dl, total cholesterol 95 mg/dl, total protein
11.7 gm/dl, and albumin 2.4 gm/dl.
Which ONE of the following is the MOSTlikely cause of the patient’s hyponatremia?
A. Addison disease
B. Trimethroprim therapy
C. Syndrome of inappropriate antidiuretichormone secretion (SIADH)
D. Pseudohyponatremia
18. An infant is born at 27 wk gestation. Laboratoryexamination 24 h after birth shows a serum K�
concentration of 6.5 mEq/L. Urine output is 1.5ml/kg per h. The patient is given a diagnosis ofearly-onset nonoliguric hyperkalemia in a verylow birth weight infant.
Which ONE of the following is TRUE re-garding hyperkalemia in this infant?
A. It is likely the result of excess sodium re-absorption proximal to potassium secretorysites in the premature kidney.
B. It is likely due to immaturity in develop-ment of aldosterone production in the pre-mature adrenal gland.
C. The maxi-K channel is expressed in thedistal nephron before the ROMK secretorychannel.
D. There is a relative predominance of apicalH-K-ATPase compared with ROMK in theneonate.
19. A 55-yr-old woman presents with a subarach-noid hemorrhage caused by a saccular aneurysmoriginating from the anterior communicating ar-tery. Three days after surgical clipping of theaneurysm, the patient develops polyuria (urineoutput up to 300 ml/h) and increasing confusion.Serum sodium level is 165 mEq/L. Serum con-centrations of potassium, calcium, and glucoseare normal, and urine osmolality is 122 mOsm/kg. Administration of 2 �g of desmopressinsubcutaneously decreases urine output to 50ml/h, and the serum sodium concentration isnormalized with 0.45% saline. Intranasal des-mopressin is prescribed in a dosage of 20 �gtwice daily, and she is discharged to an inter-mediate-care facility with a serum sodium con-
160 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

centration of 140 mEq/L. One week later, herserum sodium is found to be 156 mEq/L.
Which ONE of the following is the BESTintervention?
A. Administer desmopressin subcutaneously 2�g twice daily.
B. Increase the intranasal desmopressin dos-age to 40 �g twice daily.
C. Increase the dose interval of desmopressinto 20 �g three times daily.
D. Continue the present dosage of desmopres-sin and reduce dietary sodium.
E. Continue the present dosage of desmopres-sin and implement a regimen of timed oralfluid intake.
20. A 44-yr-old man is admitted from home 3 d afterworking outside in the extreme heat (42°C). Hehad come home with a headache and nausea andhad been unable to eat or drink for 3 d. Onadmission, he is unresponsive with a BP of80/54 mmHg and a temperature of 38.9°C. Mu-cous membranes are dry, and skin turgor is poor.Plantar reflexes are extensor bilaterally. Labora-tory data show the following: serum Na 208mEq/L, K 3.0 mEq/L, BUN 30 mg/dl, and cre-atinine 2 mg/dl. A computed tomography scanof the head reveals a retained bullet fragment,believed secondary to a gunshot wound at age18 near the third ventricle. He is given 3 L ofisotonic saline followed by 0.45% saline. Urineoutput is 4.2 L on the second hospital day, whenhis serum sodium is 155 mEq/L. After recovery,a water deprivation test is performed. At a serumosmolality of 325 mOsm/kg and serum sodiumconcentration of 147 mEq/L, urine osmolality is743 mOsm/kg, urine sodium is 190 mEq/L, andhe expresses no desire for water.
Which ONE of the following is the MOSTlikely diagnosis?
A. Adipsia with normal vasopressin secretion
B. Adipsia with complete central diabetesinsipidus (DI)
C. Adipsia with partial central DI
D. Dehydration as a result of heat exposurewith temporary resetting of the osmostat
E. Psychiatric disturbance with surreptitioussalt ingestion
21. A 28-yr-old woman undergoes trans-sphenoidalresection of a large pituitary tumor. The first dayafter surgery, she begins to complain of thirst,and her urine output is 500 ml/h. Serum sodiumis 150 mEq/L, and urine specific gravity is1.003. A diagnosis of central DI is made, andshe is started on 1 �g of desmopressin subcuta-neously, every 12 h. Urine output decreases to25 ml/h and urine specific gravity increases to1.018, and by the second postoperative day, herserum sodium is 140 mEq/L. On the sixth hos-pital day, the serum sodium decreases to 127mEq/L and desmopressin is discontinued. Urineoutput is 1L/d for the next 3 d. On the ninth day,she begins to complain of extreme thirst, urineoutput increases to 300 ml/h, the serum sodiumincreases to 145 mEq/L, plasma osmolality is298 mOsm/kg, and the urine specific gravity is1.004. An magnetic resonance imaging scanshows no pituitary bright spot.
Which ONE of the following statements isthe BEST explanation for this sequence ofevents?
A. The patient is a slow acetylator of desmo-pressin.
B. The patient has episodic secretion of avasopressin inhibitor from residual pitu-itary tumor.
C. The fluctuating urine output is caused byepisodic secretion of vasopressin from atemporarily dysfunctional osmoreceptor,and syndrome of inappropriate antidiuresisis likely to recur in the next 3 d.
D. The patient had SIADH on day 6 to 9 andnow has permanent DI as a result of injuryto the pituitary stalk.
E. The patient developed transient DI on thefirst and ninth hospital days, and this islikely to resolve in the next 2 wk.
22. A 65-yr-old woman with a history of a schizo-affective disorder has been treated with lithium400 mg/d for the past 20 yr. She developedaphasia 4 yr ago secondary to a sagittal vein
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 161

thrombosis. She is now admitted because offever and a change in mental status. Physicalexamination reveals the following: BP 90/50mmHg, heart rate 120 bpm, temperature 39°C,dry mucous membranes, clear lungs, and noedema. Laboratory data reveal the following:Serum Na 148 mEq/L, K 3.6 mEq/L, Cl 114mEq/L, CO2 28 mEq/L, BUN 26 mg/dl, creati-nine 0.6 mg/dl, and calcium 13.5 mg/dl. Urineand blood cultures are positive for Escherichiacoli. Computed tomographic scan of the abdo-men shows nonobstructing calcium stones. Lith-ium is discontinued, and she is treated withisotonic saline, antibiotics, and pamidronate.Five days later, she is alert, normotensive, andafebrile. Urine output is 5 L/d. Serum calcium is9.5 mg/dl, and serum sodium is 148 mEq/L.Urine osmolality is 180 mOsm/kg. After desmo-pressin, urine osmolality increases to 230mOsm/kg.
Which ONE of the following is the BESTexplanation for her polyuria?
A. Psychogenic polydipsia
B. Central DI
C. Osmotic dieresis
D. Nephrogenic DI as a result of lithium
23. A 40-yr-old woman is admitted with the worstheadache of her life. Physical examination re-veals weight of 56 kg and BP of 170/60 mmHg.Meningeal signs are present, but the rest of theexamination is nonrevealing. Admission labora-tory values show the following: Na 140 mEq/L,K 3.9 mEq/L, Cl 105 mEq/L, CO2 22 mEq/L,BUN 17 mg/dl, creatinine 1.0 mg/dl, and hemat-ocrit 37%. Computed axial tomography of thebrain shows a small subarachnoid hemorrhage.During the first 6 d of hospitalization, she istreated with nimodipine and 0.9% saline at 200ml/h. Gradually the serum sodium concentrationfalls to 125 mEq/L. Mannitol 12.5 g is admin-istered, and saline is continued. The next day,BP is 148/66, and weight is 58 kg. She is alertand oriented but complains of a headache. Lab-oratory data on day 6 reveal the following: Na124 mEq/L, K 4.2 mEq/L, Cl 91 mEq/L, CO2 22
mEq/L. BUN 11 mg/dl, creatinine 0.9 mg/dl,glucose 260 mg/dl, and hematocrit 34. Serumosmolality is 260 mOsm/kg; urine osmolality is800 mOsm/kg. Urine values include the follow-ing: Na 240 mEq/L, K 20 mEq/L, and output200 ml/h.
Which ONE of the following is the MOSTlikely cause of her hyponatremia?
A. Pseudohyponatremia
B. Translocational hyponatremia as a result ofmannitol
C. SIADH
D. Cerebral salt wasting
24. A 32-yr-old woman with von Willebrand dis-ease is treated with preoperative desmopressinbefore cesarean section for a term pregnancy.Intravenous fluids are discontinued 24 h afterdelivery. Three days after surgery, she is alert,oriented, and eating and drinking normally. Sheis observed walking unsteadily to the nursingstation, when she falls and experiences a briefseizure. Laboratory data show a serum sodiumof 108 mEq/L, and computed tomography scanof the head is normal. It is discovered thatdesmopressin had inadvertently been continuedin a dose of 2 �g every 8 h for the past 3 d. Sheis treated with 3% saline at 40 ml/h (0.5 ml/kgper h). Eight hours later, the serum sodium is119 mEq/L and she is awake but confused.
Which ONE of the following therapiesshould be instituted at this time?
A. Continue 3% saline at 40 ml/h
B. 100-ml bolus of 3% saline and then dis-continue intravenous fluids
C. Stop 3% saline and start 0.9% saline at100 ml/h
D. Stop 3% saline and administer desmopres-sin
E. Stop 3% saline and restrict fluids
25. A 20-yr-old woman is referred for recurrent boutsof weakness associated with hypokalemia. Sheoccasionally has used laxatives to lose weight butdenies recent history of vomiting or diarrhea. She
162 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

does not use illicit drugs and is HIV negative. BPis 110/80 supine and 92/70 upright; the remainderof the examination is normal. Laboratory valuesare as follows: Na 135 mmol/L, K 2.0 mmol/L, Cl80 mmol/L, HCO3 40 mmol/L, plasma aldoste-rone 32 ng/dl, and plasma renin activity 40 ng/mlper h. Urine values are as follows: Na 50 mmol/L,K 20 mmol/L, Cl 5 mmol/L, and pH 7.5.
Which ONE of the following is the MOSTlikely cause of the laboratory abnormalities?
A. Recent abuse of ipecac
B. Recent ingestion of loop diuretics
C. Bartter syndrome
D. Gitelman syndrome
E. Laxative abuse
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 163

Nephrology Self-Assessment Program
Core Knowledge QuestionsFluid, Electrolyte, and Acid-Base Disturbances
The Core Knowledge questions feature 5 multiple choice questions which are designed to test knowledge of coreaspects of clinical nephrology and are therefore more useful in preparing for Board certification, recertification andfuture inservice examinations. The questions and answers are available in each issue of NephSAP and on theNephSAP page on the ASN website by clicking on the Core Nephrology Questions button. Each question isassociated with an UpToDate link that will remain active for the first 3 months after publication. The Editorsbelieve that this feature enhances the utility of NephSAP as a comprehensive self study, self-assessment programfor ASN members.
1. A young man is found to have hypertension and hypokalemia. A resident taking a careful history discoversthat the patient is extremely fond of European licorice.
Which ONE of the following genetic defects produces a similar syndrome?
A. A mutation in the gene for the inwardly rectifying potassium channel ROMK
B. A mutation in the gene for the basolateral chloride channel CLC-Kb
C. A mutation in the gene for the NaCl co-transporter
D. A mutation in the gene for 11�-hydroxysteroid dehydrogenase
E. A chimeric gene with portions of the 11�-hydroxylase gene and the aldosterone synthase gene
2. A 45-yr-old previously healthy woman who weighs 50 kg undergoes surgery for a ruptured ovarian cyst.During surgery, she is given 2 L of lactated Ringer solution, and she is given 5% dextrose in 0.45% NaCl with20 mEq/L KCl at 250 ml/h postoperatively. Forty-eight hours after surgery, she complains of headache andvomiting. BP is 140/80 mmHg. She is alert and oriented, and the general physical and neurologicexaminations are unremarkable. Laboratory data reveal the following: Serum Na 115 mEq/L, plasmaosmolality 241 mOsm/kg H2O, and urine osmolality 850 mOsm/kg H2O. The patient is not taking anythingby mouth.
In addition to stopping the 5% dextrose in 0.45% NaCl infusion, which ONE of the following wouldbe the MOST appropriate treatment?
A. 5% dextrose in 0.9% saline with 20 mEq KCl at 50 ml/h
B. 5% dextrose in 0.9% saline with 20 mEq KCl at 250 ml/h
C. 3% saline at 100 ml/h plus intravenous furosemide until serum sodium concentration is 132 mEq/L
D. 3% saline at 50 ml/h plus intravenous furosemide until the serum sodium is 120 mEq/L
3. A 40-yr-old man with ESRD that requires hemodialysis presents with proximal muscle weakness. The serumpotassium is 8 mEq/L, and an electrocardiogram shows peaked T waves.
Which ONE of the following agents would lower his serum potassium concentration most quickly?
A. Calcium gluconate intravenously
B. Propranolol intravenously
C. Kayexalate in sorbitol orally
D. Sodium bicarbonate intravenously
E. Glucose and insulin intravenously
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009
164

4. A homeless man is discovered unconscious in the park and is brought to the emergency department. Hewreaks of alcohol, is unkempt, and is incoherent. Physical examination shows a BP of 90/50 mmHg, heart rateof 120 bpm, temperature of 39°C, slight scleral icterus and dullness, and bronchial breath sounds over theright lower lung fields. Laboratory data reveal the following: Serum Na 131 mEq/L, K 2.9 mEq/L, Cl 70mEq/L, CO2 21 mEq/L, blood urea nitrogen 34, creatinine 1.4 mg/dl, glucose 240 mg/dl, serum osmolality320 mOsm/kg H2O, serum ketones weakly positive, pH 7.53, PaCO2 25 mmHg, PaO2 60 mmHg, and serumalbumin 3.8 g/dl.
Which ONE of the following choices BEST describes his acid-base disturbance?
A. Metabolic acidosis
B. Respiratory alkalosis
C. Metabolic acidosis and respiratory alkalosis
D. Metabolic acidosis and metabolic alkalosis
E. Metabolic acidosis, metabolic alkalosis, and respiratory alkalosis
5. A 9-yr-old girl complains of profound weakness, dizziness, and polyuria. She is taking no medications andhas no gastrointestinal complaints. Pertinent clinical finding is BP of 90/50 mmHg with orthostatic dizziness.Laboratory data reveal the following: Na 140 mEq/L, K 2.5 mEq/L, Cl 100 mEq/L, CO2 33 mEq/L, blood ureanitrogen 25 mg/dl, and creatinine 0.7 mg/dl. A 24-h urine collection reveals the following: Sodium 90 mEq,potassium 60 mEq, Cl 110 mEq, and calcium 280 mg. Plasma renin and aldosterone are elevated.
These findings are MOST suggestive of which ONE of the following?
A. Adrenal adenoma
B. Gitelman syndrome
C. Bartter syndrome
D. Licorice ingestion
E. Hemangiopericytoma
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 165

Answer and Explanation Key
1. Answer: D. A mutation in the gene for 11�-hydroxysteroid dehydrogenaseAldosterone, the most important mineralocorticoid, increases sodium reabsorption and potassium secretionin the distal nephron. Excessive secretion of mineralocorticoids or abnormal sensitivity to mineralocorticoidhormones may result in hypokalemia, suppressed plasma renin activity, and hypertension. The syndrome ofapparent mineralocorticoid excess is an inherited form of hypertension in which 11�-hydroxysteroiddehydrogenase is defective. This enzyme converts cortisol to its inactive metabolite, cortisone. Becausemineralocorticoid receptors themselves have similar affinities for cortisol and aldosterone, the deficiencyallows these receptors to be occupied by cortisol, which normally circulates at much higher plasma levelsthan aldosterone. Licorice that contains glycyrrhetinic acid mimics the hereditary syndrome because itinhibits 11�-hydroxysteroid dehydrogenase.
● White PC: 11Beta-hydroxysteroid dehydrogenase and its role in the syndrome of apparent mineralocor-ticoid excess. Am J Med Sci 322: 308–315, 2001
● Brem AS: Insights into glucocorticoid-associated hypertension. Am J Kidney Dis 37: 1–10, 2001
● Farman N, Bocchi B: Mineralocorticoid selectivity: Molecular and cellular aspects. Kidney Int 57:1364–1369, 2000
● Iida R, Otsuka Y, Matsumoto K, Kuriyama S, Hosoya T: Pseudoaldosteronism due to the concurrent useof two herbal medicines containing glycyrrhizin: Interaction of glycyrrhizin with angiotensin-convertingenzyme inhibitor. Clin Exp Nephrol 10: 131–135, 2006
2. Answer: D. 3% saline at 50 ml/h plus intravenous furosemide until the serum sodium is 120 mEq/LThe patient has developed hypotonic hyponatremia because of the nonosmotic release of vasopressincaused by the stress of surgery coupled with the intravenous administration of a large volume ofhypotonic fluid. Her complaints of headache and vomiting are strongly suggestive of cerebral edema,a complication that has been reported primarily in premenopausal women with postoperative hypona-tremia. Because this syndrome may be fatal, prompt, definitive treatment is needed to raise the serumsodium concentration over the next few hours. Neither isotonic saline nor fluid restriction is asatisfactory strategy to accomplish this goal. Extracellular fluid volume expansion created by thepostoperative and perioperative fluid will cause the patient to excrete large amounts of sodium in herurine. Vasopressin levels may remain elevated for several days after surgery, which will cause her urineto be concentrated. Thus, the sodium in each liter of isotonic saline that she is given may be excretedin �1 L of urine; the infusate will thus be “desalinated,” causing positive water balance and worseningof hyponatremia. Because of her volume-expanded state, the patient may excrete the equivalent ofhypertonic saline in her urine even if intravenous fluids are discontinued; as a result, her serum sodiumconcentration may continue to fall spontaneously. Thus, intravenous hypertonic saline is needed todecrease the severity of cerebral edema and eliminate the risk for herniation. Because hyponatremia hasevolved over 48 h, there is some risk for osmotic demyelination if the serum sodium concentration isincreased too much (�18 mEq/L in 48 h). Choice C will raise the serum sodium concentration by 5,17 mEq/L in �24 h; as postoperative vasopressin levels begin to fall spontaneously, the ensuing waterdiuresis may result in excessive correction. Because brain swelling of �5 to 10% is incompatible withlife, a 5% increase in serum sodium concentration (an increase of 6 mEq/L) is enough to bring thepatient out of danger without risking iatrogenic injury from excessive correction.
● Steele A, Gowrishankar M, Abrahamson S, Mazer CD, Feldman RD, Halperin ML: Postoperativehyponatremia despite near-isotonic saline infusion: A phenomenon of desalination. Ann Intern Med126: 20 –25, 1997
● Lien YH, Shapiro JI: Hyponatremia: Clinical diagnosis and management. Am J Med 120: 653– 658,2007
166 Nephrology Self-Assessment Program - Vol 8, No 2, March 2009

3. Answer: E. Glucose and insulin intravenouslyCalcium gluconate (choice A) is indicated in the treatment of hyperkalemic emergencies because itselectrophysiologic effect prevents cardiac arrest. Although the drug works extremely rapidly, it does notactually lower the serum potassium concentration. Propranolol (choice B) is a �-adrenergic–blocking agentthat has a mild hyperkalemic effect and is therefore contraindicated in this patient. Kayexalate (choice C)must first reach the rectum to be effective in lowering the serum potassium concentration; when the drug isgiven orally, it does not work rapidly. Sodium bicarbonate (choice D) is theoretically beneficial because itfavors uptake of potassium by cells; however, studies of sodium bicarbonate in patients with ESRD haveshown that potassium falls minimally within the first 2 h. Glucose and insulin (choice E) are effective inlowering the serum potassium concentration within minutes. Insulin acts on sodium-potassium ATPase topromote cellular uptake of potassium, an effect that is independent of glucose. Glucose is given concurrentlywith insulin to avoid hypoglycemia.
● Evans K, Reddan D, Szczech L: Nondialytic management of hyperkalemia and pulmonary edema amongend-stage renal disease patients: An evaluation of the evidence. Semin Dial 17: 22–29, 2004
4. Answer: E. Metabolic acidosis, metabolic alkalosis, and respiratory alkalosisThe patient has an alkaline blood pH indicting that he must have either metabolic or respiratory alkalosis.The low PaCO2 in the presence of alkalemia makes the diagnosis of respiratory alkalosis; however, the patientalso has a large anion gap (40 mEq/L), which indicates that he must also have a metabolic acidosis. The presenceof serum ketones suggests that the metabolic acidosis may be caused in part by alcoholic ketoacidosis, and thepresence of an osmolar gap (calculated osmolality 287 versus measured osmolality 320 mOsm/kg) should promptan evaluation for ethanol, methanol, or ethylene glycol intoxication. Circulating acetone in patients withketoacidosis will contribute to the osmolar gap despite the extremely large anion gap (28 mEq/L higher thannormal); the serum bicarbonate concentration is only 3 mEq/L lower than normal. The discrepancy between thechange in the anion gap from baseline and the change in the bicarbonate concentration from baseline is suggestiveof a third disturbance, metabolic alkalosis (in this setting, most likely as a result of vomiting), which raised theserum bicarbonate concentration to a higher than normal level before it was reduced by the metabolic acidosis.
● Kraut JA, Madias NE: Approach to patients with acid-base disorders. Respir Care 46: 392–403, 2001
● Kraut JA, Madias NE: Serum anion gap: Its uses and limitations in clinical medicine. Clin J Am Soc Nephrol2: 162–174, 2007
5. Answer: C. Bartter syndromeThe term Bartter syndrome denotes a group of renal diseases that share a common denominator of metabolicalkalosis and renal potassium wasting without hypertension. Bartter syndrome falls into four subgroups: (1)Antenatal Bartter syndrome (hyperprostaglandin E2 syndrome), (2) the Gitelman variety of Bartter syndrome(Gitelman syndrome), (3) classical Bartter syndrome, and (4) pseudo-Bartter syndrome. This patient is an exampleof classical Bartter syndrome, characterized by early childhood onset. Symptoms may include polyuria,polydipsia, vomiting, constipation, salt craving, and a tendency to volume depletion. Growth retardation followsif treatment is not initiated. Affected patients have hypokalemic metabolic alkalosis and, unlike patients withGitelman syndrome, their urinary calcium excretion is elevated. Adrenal adenoma, licorice ingestion, andhemangiopericytoma (choices A, D, and E) all are causes of hypokalemia, but these disorders are associated withhypertension.
● Seyberth HW: An improved terminology and classification of Bartter-like syndromes. Nat Clin Pract Nephrol4: 560–567, 2008
● Shaer AJ: Inherited primary renal tubular hypokalemic alkalosis: A review of Gitelman and Bartter syndromes.Am J Med Sci 322: 316–332, 2001
Nephrology Self-Assessment Program - Vol 8, No 2, March 2009 167


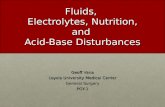



![SCISCITATOR 2015 · [1]. Riverine communities experience two main types of disturbances: natural disturbances and anthropogenic disturbances. Natural disturbances in riverine ecosystems](https://static.fdocuments.in/doc/165x107/5f27dd3959f0c41da22eeec5/sciscitator-1-riverine-communities-experience-two-main-types-of-disturbances.jpg)