NEPHROTIC SYNDROME Nephrotic range proteinuria, (>40mg/m 2 /hour), (> 50mg/kg/day), urine to protein...
34
NEPHROTIC SYNDROME NEPHROTIC SYNDROME Nephrotic range proteinuria, ( Nephrotic range proteinuria, ( >40mg/m >40mg/m 2 /hour), /hour), (> 50mg/kg/day), urine to protein creat ratio (> 50mg/kg/day), urine to protein creat ratio (>2mg/mg), +3-4 on dipstick (>2mg/mg), +3-4 on dipstick Hypoalbumenia (<2.5g/dl) Hypoalbumenia (<2.5g/dl) Hyperlipidemia Hyperlipidemia edema edema Prevelance 2/100000 Prevelance 2/100000 M:F 2:1, 80% <6 years M:F 2:1, 80% <6 years
-
Upload
alexina-webb -
Category
Documents
-
view
242 -
download
2
Transcript of NEPHROTIC SYNDROME Nephrotic range proteinuria, (>40mg/m 2 /hour), (> 50mg/kg/day), urine to protein...

NEPHROTIC SYNDROMENEPHROTIC SYNDROME
Nephrotic range proteinuria, (Nephrotic range proteinuria, (>40mg/m>40mg/m22/hour), (> /hour), (> 50mg/kg/day), urine to protein creat ratio (>2mg/mg), 50mg/kg/day), urine to protein creat ratio (>2mg/mg), +3-4 on dipstick+3-4 on dipstick
Hypoalbumenia (<2.5g/dl)Hypoalbumenia (<2.5g/dl)
HyperlipidemiaHyperlipidemia edemaedema
Prevelance 2/100000Prevelance 2/100000
M:F 2:1, 80% <6 yearsM:F 2:1, 80% <6 years

ETIOLOGYETIOLOGY
1.1. Primary or Primary or idiopathic(MCD,FSGS,Membranous,MPidiopathic(MCD,FSGS,Membranous,MPGN,Mesangial proliferation)GN,Mesangial proliferation)
2.2. Congenital nephrotic syndrome (first Congenital nephrotic syndrome (first 3months) due TORCH,Finish type3months) due TORCH,Finish type
3.3. Secondary to infections,systemic Secondary to infections,systemic diseases (HSP,SLE)diseases (HSP,SLE)

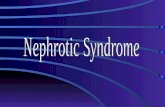
PathogenesisPathogenesis1.1. Defect in GBM,slit diaphram,genetic Defect in GBM,slit diaphram,genetic
mutations in nephrin,podocinmutations in nephrin,podocin
2.2. Circulating factor,cytokine VPF Circulating factor,cytokine VPF explains early recurrenceexplains early recurrence
3.3. Immunological abnormality,T cell Immunological abnormality,T cell dysfunction,ass with Hodgkin dysfunction,ass with Hodgkin lymphomalymphoma
PathophysiolgyPathophysiolgy1.1. Decrease Intravascular volume,urine Decrease Intravascular volume,urine
Na Na <20<20
2.2. Increased intravascular volumeIncreased intravascular volume

Podocytes and the slit diaphragm




HistopathologyHistopathology
MCD:normal LM,neg IF,EM MCD:normal LM,neg IF,EM effacement of foot processes of effacement of foot processes of podocytespodocytes
Mesangial proliferative,IgM Mesangial proliferative,IgM nephropathy:positive IgM,C3 on IFnephropathy:positive IgM,C3 on IF
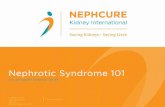
FSGS:juxtamedullary glomeruliFSGS:juxtamedullary glomeruli Most common is MCD.Most common is MCD. 80% of MCD were ≤6y,compared to 80% of MCD were ≤6y,compared to
50% of FSGS50% of FSGS

NORMAL NORMAL


Moderate FSGSModerate FSGS
Moderate FGS


History and History and examinationexamination Periorbital swelling mistaken as allergyPeriorbital swelling mistaken as allergy Increase in weight,abdominal distention Increase in weight,abdominal distention
ascitisascitis Scrotal and sacral edema,pleural Scrotal and sacral edema,pleural
effusioneffusion Abdominal pain due to Abdominal pain due to
hypovolemia,peritonitishypovolemia,peritonitis Decrease in urine outputDecrease in urine output Symptoms preceded by URTISymptoms preceded by URTI Blood pressure normal or highBlood pressure normal or high

Laboratory Laboratory investigationinvestigation Electrolytes: low Na,low albumin and Electrolytes: low Na,low albumin and
calciumcalcium ANA,C3,C4,hepatitis B,CANA,C3,C4,hepatitis B,C Hemoglobin high,platlet highHemoglobin high,platlet high Urine Na less than 10Urine Na less than 10 Urine analysis: proteinuria,microscopic Urine analysis: proteinuria,microscopic
hematuriahematuria Urine protein/creatinine more than 2 Urine protein/creatinine more than 2
mg/mgmg/mg Elevated cholesterol and triglyceridesElevated cholesterol and triglycerides



Course and outcomeCourse and outcome
93 % of MCD respond to steriods by 93 % of MCD respond to steriods by 4 weeks.4 weeks.
30% single episode,70% relapse30% single episode,70% relapse 35-50% frequent relapses35-50% frequent relapses Long term:80 % have complete Long term:80 % have complete
remission by 8 years.remission by 8 years. SRNS can progress to CKDSRNS can progress to CKD

CLASSIFICATION
DEFINTION
REMISSION Urine prot <4mg/m2/hour,urine prot/creat <.2 mg/mg, 0 on dipstick for 3 days
STERIOD RESISTANCE
Failure to respond after initial 4-8 weeks of steroids
RELAPSE Urine prot >40mg/m2/hour,urine prot/creat >2mg/mg,+3 prot on dipstick for 3 days or edema
INFREQUENT RELAPSE
1 relapse in 6 months,1 to 3 in 12 months
FREQUENT RELAPSE
2 or more relapse in 6 months,4 or more in 12 months
STERIOD DEPENDANT
Two consecutive relapses during steroid therapy or within 14 days of ceasing therapy

When a renal biobsy is When a renal biobsy is donedone
Age less than 1.Age less than 1. SRNSSRNS ARFARF Gross or persistent microscopic Gross or persistent microscopic
hematuriahematuria Biobsy sent for LM,IF,EMBiobsy sent for LM,IF,EM

TREATMENTTREATMENT
First episode :Steriods 2mg/kg/day,60 First episode :Steriods 2mg/kg/day,60 mg/mmg/m22/day single daily dose for 4 /day single daily dose for 4 weeks,followed by alternate dose for 3-weeks,followed by alternate dose for 3-6 months. 6 months.
Response in 10 to 14 daysResponse in 10 to 14 days Recent Cockrane metaanalysis found Recent Cockrane metaanalysis found
that treatment for 3m compared to 2m that treatment for 3m compared to 2m reduces risk of relapse by 30% at 12-reduces risk of relapse by 30% at 12-24m24m
No significant diff in risk of side effects No significant diff in risk of side effects or cumulative steriod doseor cumulative steriod dose
With each 1 m over 2m,RR of relapse With each 1 m over 2m,RR of relapse falls by 11%falls by 11%


Treatment of relapses:2mg/kg/day Treatment of relapses:2mg/kg/day till remission for 3 days,then till remission for 3 days,then alternate days for 2-3m.alternate days for 2-3m.
Treatment of FR or SD SSNS:Treatment of FR or SD SSNS:
1.Long alternate steriods for 12-18 1.Long alternate steriods for 12-18 mm
2.Cyclophosphamide2.Cyclophosphamide
3.cyclosporine3.cyclosporine
4.Levimazole4.Levimazole
5.Mycophenolate acetate5.Mycophenolate acetate

Side effectsSide effects
Steriods:growth,osteopenia,cataract,cuSteriods:growth,osteopenia,cataract,cushingoid,glaucomashingoid,glaucoma
Cyclosporine:hirsuitism,gum Cyclosporine:hirsuitism,gum hypertrophy,HTN,reduced GFRhypertrophy,HTN,reduced GFR
CPM:infertility,alopecia,leucopenia,hemCPM:infertility,alopecia,leucopenia,hemmrhagic cystitis.mrhagic cystitis.
MMF:abdominal MMF:abdominal pain,anemia,leucopeniapain,anemia,leucopenia

COMPLICATIONSCOMPLICATIONS
1-Infections:losses of IgG in 1-Infections:losses of IgG in urine,abn T cell function,low factor urine,abn T cell function,low factor B (C3 proactivator),steriod B (C3 proactivator),steriod use,impaired opsonizationuse,impaired opsonization
Encapsulated bact streptococcus Encapsulated bact streptococcus pneumonia,staph,Ecolipneumonia,staph,Ecoli
Primary bacterial peritonitisPrimary bacterial peritonitis Immunization against Immunization against
pneumococcus,varicellapneumococcus,varicella

2-Thromboembolism:inc clotting 2-Thromboembolism:inc clotting factors,fibrinogen,low AT3,plat factors,fibrinogen,low AT3,plat aggreg,hyperviscosiotyaggreg,hyperviscosioty
Venous,RVT,sagital sinus,veins of Venous,RVT,sagital sinus,veins of legslegs
3.ARF3.ARF

Supportive treatmentSupportive treatment
Salt restrictionSalt restriction Albumin 25% 1-2g/kg/day over 4 Albumin 25% 1-2g/kg/day over 4
hours with frusemidehours with frusemide ACEI decrease proteinuria in SRNSACEI decrease proteinuria in SRNS

CNS Finish TypeCNS Finish Type
AR,Mutation in nephrin AR,Mutation in nephrin gene,codes for nephrin part of slit gene,codes for nephrin part of slit diaphragmdiaphragm
Two mutations (Finmaj,Finminor)Two mutations (Finmaj,Finminor) Born premature,large placentaBorn premature,large placenta Edema at birth,severe proteinuria, Edema at birth,severe proteinuria,
very low albuminvery low albumin High amnoitic AFPHigh amnoitic AFP GFR normal first 6-12mGFR normal first 6-12m



Diffuse Mesangial Diffuse Mesangial SclerosisSclerosis AD,isolated or Denys-Drash (wilms AD,isolated or Denys-Drash (wilms
tumor,male pseudohermaphrodite)tumor,male pseudohermaphrodite) Proteinuria in first 3m or later in Proteinuria in first 3m or later in
infancy,less severe than CNSinfancy,less severe than CNS ESRD months after presentationESRD months after presentation Mesangial sclerosis,interstitial Mesangial sclerosis,interstitial
fibrosisfibrosis Mutations of WT1Mutations of WT1

TreatmentTreatment
No role for steriodsNo role for steriods Albumin infusionsAlbumin infusions Nutrition:130kcal/kg,4g/kg proteinNutrition:130kcal/kg,4g/kg protein HypothyroidismHypothyroidism ACEIACEI IndomethacinIndomethacin diuerticsdiuertics Anticoagulants,prophylactic Anticoagulants,prophylactic
pencillinpencillin Nephrectomy,dialysis,tranplantationNephrectomy,dialysis,tranplantation

Hereditary nephrotic syndromeHereditary nephrotic syndrome
DiseaseDisease inheritinheritanceance
locuslocus genegene proteinprotein
Denys-DrashDenys-Drash
DMSDMSADAD 1111 WT1WT1 WT1WT1
CNS,FinishCNS,Finish ARAR 1919 NPHS1NPHS1 nephrinephrinn
Familial Familial SRNS,SRNS,
ARAR 11 NPHS2NPHS2 podocipodocinn
piersonpierson ARAR 33 LAMB2LAMB2 lamininlaminin
FSGS1(late)FSGS1(late) ADAD 1919 ACTN4ACTN4 Actinin Actinin
FSGS2FSGS2 ADAD 1111 TRPC6TRPC6 TRPC6TRPC6

SRNSSRNS
Mostly FSGS,genetic Mostly FSGS,genetic forms,immune mediated recur forms,immune mediated recur after Txafter Tx
Cyclosporine better than Cyclosporine better than cyclophospamidecyclophospamide
ACEI,diuertic to control edema.ACEI,diuertic to control edema. rituximabrituximab