Neonatal Status Epilepticus
6
Neonatal Status Epilepticus Russell Lawrence, MD,* ,† and Terrie Inder, MD* ,‡ Seizures are more prevalent during the neonatal period than at any other time in the human lifespan. During early development, neonates are developmentally predisposed to excita- tory neuronal activity increasing their susceptibility to seizures. Status epilepticus is poorly defined in this subpopulation with a lack of a consensus definition. In this review, we discuss the common etiologies of recurrent seizures in the newborn in addition to current trends on monitoring and treatment. Finally, we discuss the current evidence in both animal and human studies that indicate that neonatal seizures may be harmful to the immature brain with adverse long-term neurodevelopment outcomes. Semin Pediatr Neurol 17:163-168 © 2010 Elsevier Inc. All rights reserved. R ecurrent seizures occur more commonly in the neonatal period than at any other time during the human lifespan with an incidence of 1 to 3.5 per 1000 births. 1,2 Although recurrent seizures are consistently associated with poor out- comes in the neonatal population, much controversy remains about whether the seizures themselves contribute to outcome or are just a symptom of cerebral injury. In this article, several aspects of neonatal status epilepticus are discussed. This in- cludes aspects of development that predispose neonates to seizures, common etiologies of neonatal seizures, challenges in definition, diagnosis, and current treatment options. Fi- nally, the impact of seizures on neurodevelopmental out- come is also discussed. Definition In adults and children, the conventional definition for status epilepticus (SE) is any continuous clinical seizure activity lasting longer than 30 minutes or 2 or more discrete seizures without interictal resumption of baseline mental status. 3,4 One of the challenges in discussing neonatal SE is the lack of a definitive definition that is relevant to the newborn brain. Much of this ambiguity stems from the fact that seizures in the newborn infant are different in phenomenology, electro- encephalographic characteristics, and clinical features. Neo- natal seizures are rarely fully generalized but conform to a multifocal migratory epileptiform pattern. Neonatal seizures are also more difficult to diagnose clinically with many subtle signs not recognized at the bedside. Therefore, any definition that focuses on clinical rather than electroencephalographic (EEG) criteria would be limited. Neonatal seizures com- monly occur in the setting of encephalopathy (85%); thus, it is challenging to recognize any return to baseline mental status between seizures. In previous studies of neonatal sei- zures, 1 commonly cited definition regards SE as any electro- graphic recording with seizure activity 50% of the length of the recording time. 5 However, recording times may vary greatly, and, thus, the total seizure burden may vary. It would appear necessary to understand the nature and impact of neonatal SE before developing a definition and guideline for management. Thus, because of a current lack of clear con- sensus on the term “status epilepticus” in the newborn brain, we avoid this term in favor of a focus on recurrent and pro- longed seizure activity in this population. Neurobiological Predisposition Factors that are integral to normal neuronal development have the potential for increased neuronal synaptic excitation, which if unbalanced will increase susceptibility to seizures. In animal models, glutamate, the major excitatory neuro- transmitter in the central nervous system, is overexpressed during the neonatal period. This is most evident in the N- methyl-d-aspartate (NMDA) and -amino-3-hydroxy-5-me- thyl-4-isoxazolepropionic acid (AMPA) subtypes. 6,7 In the rat forebrain, this peak occurs during the second postnatal week, a time that corresponds to term in the human infant. Both receptors also exhibit altered composition that further pre- disposes them to excitation. N-methyl-d-aspartate receptors show an overexpression of NR2B subunits in the neonatal brain leading to longer current decay times and increased excitation. 8,9 This is also seen in AMPA receptors, which have a high proportion lacking the GluR2 subunit leading to in- *Department of Pediatrics, Washington University, St Louis, MO. ‡Department of Neurology, Washington University, St Louis, MO. †Cook Children’s Hospital, Fort Worth, TX. Address reprint requests to Russell Lawrence, MD, 1928 Dartmoor Ct., Fort Worth, TX 76110. E-mail: [email protected] 163 1071-9091/10/$-see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.spen.2010.06.010
-
Upload
russell-lawrence -
Category
Documents
-
view
236 -
download
0
Transcript of Neonatal Status Epilepticus

NR
Rwrcaoacsinc
DIelwOaMtenmas
*‡†A
1d
eonatal Status Epilepticusussell Lawrence, MD,*,† and Terrie Inder, MD*,‡
Seizures are more prevalent during the neonatal period than at any other time in the humanlifespan. During early development, neonates are developmentally predisposed to excita-tory neuronal activity increasing their susceptibility to seizures. Status epilepticus is poorlydefined in this subpopulation with a lack of a consensus definition. In this review, wediscuss the common etiologies of recurrent seizures in the newborn in addition to currenttrends on monitoring and treatment. Finally, we discuss the current evidence in both animaland human studies that indicate that neonatal seizures may be harmful to the immaturebrain with adverse long-term neurodevelopment outcomes.Semin Pediatr Neurol 17:163-168 © 2010 Elsevier Inc. All rights reserved.
t(miszgtganmswl
NFhwItdmtfardsbe
ecurrent seizures occur more commonly in the neonatalperiod than at any other time during the human lifespan
ith an incidence of 1 to 3.5 per 1000 births.1,2 Althoughecurrent seizures are consistently associated with poor out-omes in the neonatal population, much controversy remainsbout whether the seizures themselves contribute to outcomer are just a symptom of cerebral injury. In this article, severalspects of neonatal status epilepticus are discussed. This in-ludes aspects of development that predispose neonates toeizures, common etiologies of neonatal seizures, challengesn definition, diagnosis, and current treatment options. Fi-ally, the impact of seizures on neurodevelopmental out-ome is also discussed.
efinitionn adults and children, the conventional definition for statuspilepticus (SE) is any continuous clinical seizure activityasting longer than 30 minutes or 2 or more discrete seizuresithout interictal resumption of baseline mental status.3,4
ne of the challenges in discussing neonatal SE is the lack ofdefinitive definition that is relevant to the newborn brain.uch of this ambiguity stems from the fact that seizures in
he newborn infant are different in phenomenology, electro-ncephalographic characteristics, and clinical features. Neo-atal seizures are rarely fully generalized but conform to aultifocal migratory epileptiform pattern. Neonatal seizures
re also more difficult to diagnose clinically with many subtleigns not recognized at the bedside. Therefore, any definition
Department of Pediatrics, Washington University, St Louis, MO.Department of Neurology, Washington University, St Louis, MO.Cook Children’s Hospital, Fort Worth, TX.ddress reprint requests to Russell Lawrence, MD, 1928 Dartmoor Ct., Fort
aWorth, TX 76110. E-mail: [email protected]
071-9091/10/$-see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.spen.2010.06.010
hat focuses on clinical rather than electroencephalographicEEG) criteria would be limited. Neonatal seizures com-only occur in the setting of encephalopathy (�85%); thus,
t is challenging to recognize any return to baseline mentaltatus between seizures. In previous studies of neonatal sei-ures, 1 commonly cited definition regards SE as any electro-raphic recording with seizure activity �50% of the length ofhe recording time.5 However, recording times may varyreatly, and, thus, the total seizure burden may vary. It wouldppear necessary to understand the nature and impact ofeonatal SE before developing a definition and guideline foranagement. Thus, because of a current lack of clear con-
ensus on the term “status epilepticus” in the newborn brain,e avoid this term in favor of a focus on recurrent and pro-
onged seizure activity in this population.
eurobiological Predispositionactors that are integral to normal neuronal developmentave the potential for increased neuronal synaptic excitation,hich if unbalanced will increase susceptibility to seizures.
n animal models, glutamate, the major excitatory neuro-ransmitter in the central nervous system, is overexpresseduring the neonatal period. This is most evident in the N-ethyl-d-aspartate (NMDA) and �-amino-3-hydroxy-5-me-
hyl-4-isoxazolepropionic acid (AMPA) subtypes.6,7 In the ratorebrain, this peak occurs during the second postnatal week,time that corresponds to term in the human infant. Both
eceptors also exhibit altered composition that further pre-isposes them to excitation. N-methyl-d-aspartate receptorshow an overexpression of NR2B subunits in the neonatalrain leading to longer current decay times and increasedxcitation.8,9 This is also seen in AMPA receptors, which have
high proportion lacking the GluR2 subunit leading to in-163

cp
haatoraarc
mtncKChareNrrtoGtuendbfdecnttot
EReesadpca
taffsmamalsmnvnhbi
DCtnopdmttMfltcnsTttnyono(zmd
beanrt
164 R. Lawrence and T. Inder
reased excitation and neuronal firing from enhanced Ca2�ermeability at the receptor.10,11
This predilection for excitation is also seen within the in-ibitory neurotransmitters. Rodent studies have also shownlterations in gamma-aminobutyric acid (GABA) expressionnd distribution, the principal inhibitory neurotransmitter inhe central nervous system, during the early period of devel-pment. Newborn rodents have an overall decrease in GABAeceptor expression12 with a relative overexpression of the �4nd �2 subunits compared with the �1, which is seen indult models. This distribution of GABA receptor subtypeesults in a resistance to benzodiazepines, the class of medi-ations often used to treat seizure activity.13
In addition to these alterations in the distribution of theajor receptors, there are fundamental differences between
he immature neuron that predispose to seizures. In matureeurons, there is a low concentration of Cl� ions inside theell because of a net efflux of Cl� out of the cell through theCC2 Cl� transporter. With binding of the GABA receptor,l� flows down this gradient and into the neuron leading toyperpolarization. Therefore, in the mature neuron, GABAgonists have an inhibitory effect, whereas in immature neu-ons this chloride gradient is reversed. Because of an under-xpression of KCC2 ion channels and an overexpression ofKCC1 (pumps chloride into the cell), the Cl� gradient is
eversed with a higher percentage of Cl� ions inside the neu-on. The same GABA agonist that produced hyperpolariza-ion in the mature neuron will instead lead to a net flux of Cl�
ut of the cell. This critical difference in Cl� distribution andABA binding will result in a paradoxical depolarization of
he immature neuron.14,15 This may be the basis for the fail-re of medications such as phenobarbital and benzodiaz-pines (GABA agonists) to control seizure activity in neo-ates. This Cl� gradient matures in a caudal to rostalirection during development. This can lead to a mature inhi-ition of motor neuron within the spinal cord and brainstemrom GABAergic anticonvulsant compounds but a continuedepolarization of cortical neurons with immature Cl� gradi-nts. This may help explain the phenomenon of electrome-hanical dissociation in which seizure treatment during theeonatal period with GABA receptor agonists leads to cessa-ion of the motor symptoms (inhibition) with continuation ofhe cortical electrographic phenomenon (excitation). This isften seen in newborn infants treated with common medica-ions such as phenobarbital and midazolam.16
tiologyecurrent seizures in the newborn infant have a wide range oftiologies. The most common etiology is hypoxic ischemicncephalopathy (HIE), which accounts for around 60% ofeizures during the newborn period. These infants often havehistory of perinatal compromise and show early signs ofecompensation, such as low Apgar scores, respiratory de-ression, acidosis, and encephalopathy. Seizures usually oc-ur in the first 12 to 24 hours of life and are often multifocal
nd subtle in nature. bThe second most common cause of recurrent seizures inhe neonate is arterial and venous stroke. They account forround 15% of cases. Unlike HIE, these patients often haveocal seizures that present after 24 hours of age with relativelyew signs of encephalopathy at baseline. A third etiology ofeizures in the newborn is intracranial hemorrhage, whichay occur with HIE and/or stroke. Both subdural and sub-
rachnoid hemorrhages are common in term neonates anday carry no adverse long-term consequence if there is no
ssociated cerebral injury. Intraventricular hemorrhage is aesion primarily of the premature infant and causes moreubtle seizures presenting as posturing, abnormal eye move-ents, or autonomic changes. Other possible etiologies ofeonatal seizures that deserve mention include central ner-ous system infection, developmental disturbances in centralervous system development, metabolic disturbances, andereditary seizure disorders. A complete list is shown in Ta-le 1. Prognosis can vary greatly depending on the underly-
ng etiology of the recurrent seizures.
iagnosislinical detection of recurrent neonatal seizures is poor with
he majority being missed by bedside caregivers. Most neo-atal seizures are behaviorally subtle, and the EEG patternften reflects a multifocal process rather than a coordinatedrocess as seen in older children or adults. This makes theiagnosis of neonatal seizures complicated because infantsay display stereotyped repetitive rhythmic movements that
o the naked eye resemble seizures but would not be conven-ionally classified as such because they lack EEG correlates.
urray et al17 studied 51 term encephalopathic infants andound that only 34% of EEG seizures had any clinical corre-ate observed on video monitoring. Of this 34%, only 9% ofhese EEG seizures were recognized by neonatal clinical staffaring for the infant. During the monitoring period, nursesoted a total 177 clinical events that were suspicious foreizure events, but only 27% had a true ictal EEG correlate.his resulted in 42% of the cohort receiving inappropriate
herapy. Consistent with these findings, our own study foundhat greater than 90% of EEG seizures in infants with HIE hado visible clinical correlate even by retrospective video anal-sis.18 This included patients in electrographic status. In viewf this diagnostic complexity, it can be argued that the diag-osis of neonatal seizures should not be based on clinicalbservation alone. Conventional electroencephalographycEEG) is the “gold standard” tool to diagnose neonatal sei-ures (Fig 1), but widespread implementation of continuousonitoring is often not available outside of tertiary care aca-emic centers.In clinical practice, many infants are treated for seizure
ased on clinical observation alone. Suspicious clinicalvents often lead to antiepileptic medication administrationnd a standard 1-hour electroencephalography if available. Ifo ictal events are seen on this recording, electroencephalog-aphy is often discontinued and clinical observation is con-inued. This often leads to an underestimation of seizure
urden.17,19 This lack of clinical accuracy also leads to unnec-
emt
sgtirtar
gtdt
dfgtot(fwfam
TDncPotpmpCnws
vthmsta
tKcaasanhla
mNa
T
HAI
I
D
M
LDM
Neonatal status epilepticus 165
ssary exposure to antiepileptic drugs. Both animal and hu-an data raise concern about the adverse neurodevelopmen-
al effects of long-term exposure to these drugs.20,21
As a compromise, an increasing number of neonatal inten-ive care units are adopting limited channel amplitude inte-rated EEG devices (limited channel aEEG) for their moni-oring because of the ease with which they can be applied andnterpreted. EEG sensors are placed over the central and pa-ietal regions of the brain limiting the scope compared withhe cEEG, which measures signal from 16� channels. Thedvantage of limited channel EEG monitors is the potential of
able 1 Seizure Etiology in the Neonate
ypoxic ischemic encephalpathyrterial and venous stroke
ntracranial hemorrhaoeSubarachngicGerminal matrix intraventicularSubdural
ntracranial InfectionGroup B streptococcusEscherichia coliHerpes simplexCytomegalovirusToxoplasmosisevelopmental defectsLissencephalyPachygrylePolymicrogyriaetabolicHypoglycemiaHypocalcemiaHyponatremia
SIADHWater intoxication
HypernatremiaAmino acidopathy
Nonketotic hyperglycinemiaOrganic Acidopathy
Multiple caboxylase deficiencySulfite oxidase deficiency
Mitochondrial disordersCytochrome C oxidasePyruvate dehydrogenase
HyperammonemiaUrea cycle defects
Perixisomal disorderZellweger syndromeNeonatal adrenoleukodystrophy
Pyridoxine deficiencyFolinic acid responsive seizuresGlucose Transporter deficiency
ocal anesthetic intoxicationrug withdrawaliscellaneous neonatal seizure syndromesBenign familial neonatal seizuresBenign idiopathic neonatal seizures (5th-day fits)Early myoclonic encephalopathyEarly infantile epileptic encephalopathy
eviewing the data in “real time” by the bedside neonatolo- d
ist. Unlike cEEG, no technician or epileptologist is neededo apply or interpret results. Limited channel aEEG has aetection rate approaching 80% compared with cEEG al-hough it does underestimate the overall seizure burden.22,23
We would be remiss without stating that in addition to theiagnosis and treatment of neonatal seizures, clinicians mustocus on the diagnosis of the underlying etiology. This has thereatest prognostic value for long-term outcome. Imaging inhe form of magnetic resonance imaging (MRI) needs to bebtained in a center experienced in its interpretation. Addi-ional sequences, such as magnetic resonance angiographyMRA)/magnetic resonance venography (MRV), can be help-ul in diagnosing arterial and venous strokes. Infectiousorkup, including a lumbar puncture, needs to be per-
ormed along with an evaluation for metabolic causes, suchs hypoglycemia, hypo- or hypernatremia, or inborn errors ofetabolism.
reatmentespite advances in understanding the underlying mecha-ism that predispose to seizures and the ability to undertakeEEG monitoring, little progress has been made in treatment.henobarbital remains the most commonly used first-lineption for drug therapy although its efficacy remains in ques-ion.24-27 Painter et al28 showed that both phenobarbital andhenytoin controlled less than 50% of seizures when used asonotherapy. Even when used in combination, only 60%atients showed seizure control as defined by EEG criteria.28
ommonly used second-line drugs include midazolam, Phe-ytoin, and lidocaine. Currently, there is no consensus as tohich second-line drugs to use; however, recent studies have
hown some promising results for intravenous lidocaine.29,30
Both animal and human data raise concern about the ad-erse neurodevelopmental effects of long-term exposure tohese drugs.20,21 Phenobarbital, midazolam, and phenytoinave all been linked to increased neuroapoptosis in animalodels. Given the questionable efficacy of these drugs in
topping neonatal seizures, EEG monitoring should be usedo confirm suspected clinical events to avoid overtreatmentnd limiting exposure to true electrographic seizures.
Newer antiepileptic medications are being used althoughhey have yet to be accepted into routine clinical practice.eppra (Levetiracetam, UCB Pharma, Brussels, Belgium), aommonly prescribed oral antiepileptic medication in bothdults and children, has been quickly gaining acceptance asn intravenous treatment option for neonatal seizures31,32 de-pite a lack of safety and pharmokinetic data; one of thettractive aspects of levetiracetam is that it does not induceeuroapoptosis in animal models.33 At this time, no trialsave been completed to evaluate the safety and efficacy of
evetiracetam in comparison with the more commonly usedntiepileptic drugs.
Toparimate, an antiepileptic drug with multiple proposedechanisms (glutamate antagonist via AMPA receptor anda channel blockade) is also gaining popularity in the adult
nd pediatric world. It has not yet been studied for safety,
osing, or efficacy in the neonatal population. However, it
hm
ibNalipnt
OAsbAni
scd
ATpafahghhmliPs
166 R. Lawrence and T. Inder
as been shown to have neuroprotective properties in animalodels of hypoxic ischemic injury.34-36
Finally, the commonly used diuretic bemutanide is beingnvestigated as a possible adjunctive medication to phenobar-ital to improve seizure control. Bumetanide inhibits theKCC1 cotransporter, creating a Cl� gradient more like the
dult neuron. In animal studies, this switches the GABA equi-ibrium potential from excitatory to inhibitory, thus inhibit-ng seizure activity.37,38 Although this therapy has shownromise in the laboratory setting, clinical trials are stilleeded before bumetanide can be used in the clinical set-ing.39
utcomesdvances in monitoring and treating recurrent or prolongedeizures in the newborn infant are important only if youelieve that the seizures are harmful to the immature brain.lthough still a source of some controversy among the neo-atal and neurologic community, a growing body of evidence
FigurwithThemalwithtion.
n both animal and human studies indicate that recurrent p
eizures, especially in the setting of hypoxic ischemic injury,ontribute to adverse neurodevelopmental outcomes in ad-ition to that of the underlying etiology.
nimal Datahe effect of recurrent seizures in experimental studies ap-ears to be a function of both the stage of development of thenimal and the model used. Animal models have tended toocus on the induction of seizures by excitotoxins (eg, kainiccid) or by severe ischemic injury. While the immature brainas a greater propensity to seizure genesis, there is also areater resistance to seizure induced neuronal injury.40 Thisad led to the misconception that recurrent seizures were notarmful to the newborn brain. However, seizures in the im-ature brain do have an impact on the developmental regu-
ation of subsequent vulnerability to seizures. Thus, the samemmature pup (P15 injury) when subjected to kainic acid at-45 sustained more severe damage and performed poorly onpatial learning tasks compared with pups that had not ex-
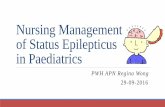
The initial portion of the electrographic seizure is subtle in onsetplitude sharp waves seen in the left temporal region (arrow). (B)
eizure 30 seconds after onset shows periodic sharp waves maxi-eft temporal region. (C) Axial T2 FSE MRI from the same patientrhage in the left hemisphere secondary to a vascular malforma-
e 1 (A)low-amsame sin the lhemor
erienced seizure activity in early life. Furthermore, cortico-

traimi
scoba
dSloagndismgsms
HOraqvcicaascMzrwls
ucdaisaw
bUgacitws
oia9t
poewii
CRpsowidmazdsocddt
R
Neonatal status epilepticus 167
rophin-releasing hormone-induced seizures in P10-13 ratsesulted in hippocampal damage, which was not seen indult rats.40 Thus, seizure-induced neuronal injury in exper-mental animal models is highly dependent on the develop-
ental stage at which it occurs and the method of seizurenduction.
Of perhaps greater clinical concern is the evidence thateizures after a hypoxic-ischemic insult (HIE) markedly in-rease the extent of cerebral injury. In 1 study, SE in thetherwise “healthy” neonatal brain did not cause major visi-le injury but when superimposed on HIE significantly ex-cerbated brain injury in a topographically specific manner.41
Studies of laboratory animals have also revealed an age-ependent vulnerability to neurocognitive impairment.42
ayin et al43 induced SE with kainic acid in immature rats andater tested them for short-term and long-term spatial mem-ry abilities. They found that the kainic acid–treated animalst all ages exhibited significant impairment and showed areater degree of anxiety compared with controls.43 The cog-itive impact of both prolonged and brief recurrent seizuresoes not appear to be model specific, indicating that deficits
n learning and memory may be a universal consequence ofignificant early-onset seizures.44 Thus, the immature animalodel literature strongly suggests that despite a minimal de-
ree of neuronal damage in the hippocampus after prolongedeizures in immature animals, long-term neurocognitiveorbidity appears to be a consequence of the seizures them-
elves.45
uman Databservational studies have shown that the severity and du-
ation of seizures in human infants with perinatal asphyxiare independently associated with brain injury and subse-uent postneonatal epilepsy. Younkin et al46 showed by inivo phosphorus-31 nuclear magnetic resonance spectros-opy that there was a 50% decrease in the phosphocreatine tonorganic phosphate ratio in 5 infants during seizures, indi-ating a disturbance in cerebral metabolism. These 5 infantsll developed adverse long-term neurologic sequelae. Theuthors concluded that their findings suggested that neonataleizures may cause or exacerbate cerebral injury by increasingerebral metabolic demands above that of energy supply.46
cBride et al47 found that the occurrence of electrographic sei-ures was significantly correlated with microcephaly, severe ce-ebral palsy, and a failure to thrive. In the subgroup of infantsith asphyxia, those with electrographic seizures were more
ikely to die of neurologic causes and have microcephaly orevere disability.47
Miller et al48 studied 90 term encephalopathic neonatessing MRI and single-voxel 1H-magnetic resonance spectros-opy. Seizure severity was based on seizure frequency anduration, EEG findings, and anticonvulsant administrationnd was associated with increased lactate/choline in both thentervascular boundary zone and the basal nuclei. Seizureeverity was independently associated with diminished N-cetylaspartate/choline in the intervascular boundary zone as
ell as a 21% increase in lactate/choline in the intervascularoundary zone and a 15% increase in the basal nuclei.48
pon follow-up of this cohort at 4 years of age, this sameroup found that clinical seizure severity was independentlyssociated with poor long-term neurodevelopmental out-ome independent of the severity of the underlying hypoxic-schemic brain injury.49 However, it should be mentionedhat seizure classification was based on clinical observation,hich as mentioned previously may underestimate the true
eizure burden.In another study of 206 term infants with neonatal seizures
r HIE, Toet et al50 reported that continuous aEEG monitor-ng and early treatment of clinical and EEG seizures wasssociated with a lower incidence of postneonatal epilepsy of.4% compared with 20% to 50% reported earlier in litera-ure.51
Finally, in a prospective, randomized study of early pro-hylactic phenobarbital, 40 mg/kg versus standard treatmentf clinical seizures in neonates with severe hypoxic ischemicncephalopathy, Hall et al52 found that the infants treatedith prophylactic phenobarbital had a 27% reduction in the
ncidence of neonatal seizures and a significant improvementn neurodevelopmental outcomes at 3 years of age.
onclusionsecurrent seizures are more common during the neonataleriod then at any other time in life. This predispostion toeizures is deeply rooted in the neurodevelopmental physi-logy occurring within the immature brain in the first feweeks of life. Although there are many etiologies, hypoxic
schemic injury remains the most common cause. Clinicaliagnosis is difficult and requires electroencephalographiconitoring. Research in experimental animal models as well
s human clinical studies are revealing that recurrent sei-ures, especially in the setting of hypoxic ischemic injury, areeleterious to the developing brain and may warrant aggres-ive treatment. However, large clinical studies of the impactf aggressive treatment of recurrent or prolonged electroen-ephalographic seizures in the newborn have not been un-ertaken. A critical need for ongoing research to refine theefinitions of seizure activity and their impact are needed inhe newborn brain.
eferences1. Volpe JJ: Neurology of the Newborn (ed 5). Philadelphia, PA, Elsevier,
20082. Ronen GM, Penney S, Andrews W: The epidemiology of clinical neo-
natal seizures in Newfoundland: a population-based study. J Pediatr134:71-75, 1999
3. Treatment of convulsive status epilepticus. Recommendations of theEpilepsy Foundation of America’s Working Group on Status Epilepti-cus. JAMA 270:854-859, 1993
4. Berg AT, Shinnar S, Levy SR, et al: Status epilepticus in children withnewly diagnosed epilepsy. Ann Neurol 45:618-623, 1999
5. Silverstein FS, Jensen FE: Neonatal seizures. Ann Neurol 62:112-120,2007
6. Insel TR, Miller LP, Gelhard RE: The ontogeny of excitatory amino acidreceptors in rat forebrain—I. N-methyl-D-aspartate and quisqualatereceptors. Neuroscience 35:31-43, 1990
7. McDonald JW, Trescher WH, Johnston MV: Susceptibility of brain to

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
168 R. Lawrence and T. Inder
AMPA induced excitotoxicity transiently peaks during early postnataldevelopment. Brain Res 583:54-70, 1992
8. Zhong J, Carrozza DP, Williams K, et al: Expression of mRNAs encod-ing subunits of the NMDA receptor in developing rat brain. J Neuro-chem 64:531-539, 1995
9. Monyer H, Burnashev N, Laurie DJ, et al: Developmental and regionalexpression in the rat brain and functional properties of four NMDAreceptors. Neuron 12:529-540, 1994
0. Burnashev N, Monyer H, Seeburg PH, et al: Divalent ion permeability ofAMPA receptor channels is dominated by the edited form of a singlesubunit. Neuron 8:189-198, 1992
1. Jonas P, Racca C, Sakmann B, et al: Differences in Ca2� permeability ofAMPA-type glutamate receptor channels in neocortical neurons causedby differential GluR-B subunit expression. Neuron 12:1281-1289,1994
2. Swann JW, Brady RJ, Martin DL: Postnatal development of GABA-mediated synaptic inhibition in rat hippocampus. Neuroscience 28:551-561, 1989
3. Dunning DD, Hoover CL, Soltesz I, et al: GABA(A) receptor-mediatedminiature postsynaptic currents and alpha-subunit expression in de-veloping cortical neurons. J Neurophysiol 82:3286-3297, 1999
4. Khazipov R, Khalilov I, Tyzio R, et al: Developmental changes inGABAergic actions and seizure susceptibility in the rat hippocampus.Eur J Neurosci 19:590-600, 2004
5. Owens DF, Boyce LH, Davis MB, et al: Excitatory GABA responses inembryonic and neonatal cortical slices demonstrated by gramicidinperforated-patch recordings and calcium imaging. J Neurosci 16:6414-6423, 1996
6. Dzhala VI, Talos DM, Sdrulla DA, et al: NKCC1 transporter facilitatesseizures in the developing brain. Nat Med 11:1205-1213, 2005
7. Murray DM, Boylan GB, Ali I, et al: Defining the gap between electro-graphic seizure burden, clinical expression, and staff recognition ofneonatal seizures. Arch Dis Child Fetal Neonatal Ed 93:187-191, 2008
8. Lawrence R, Mathur A, Nguyen TH, et al: A pilot study of continuouslimited-channel aEEG in term infants with encephalopathy. J Pediatr154:835-841, 2009
9. Mathur AM, Morris LD, Teteh F, et al: Utility of prolonged bedsideamplitude-integrated encephalogram in encephalopathic infants. Am JPerinatol 25:611-615, 2008
0. Bittigau P, Sifringer M, Genz K, et al: Antiepileptic drugs and apoptoticneurodegeneration in the developing brain. Proc Natl Acad Sci U S A99:15089-15094, 2002
1. Sulzbacher S, Farwell JR, Temkin N, et al: Late cognitive effects of earlytreatment with phenobarbital. Clin Pediatr (Phila) 38:387-394, 1999
2. Toet MC, van der Meij W, de Vries LS, et al: Comparison betweensimultaneously recorded amplitude integrated electroencephalogram(cerebral function monitor) and standard electroencephalogram in ne-onates. Pediatrics 109:772-779, 2002
3. Shah DK, Mackay MT, Lavery S, et al: Accuracy of bedside electroen-cephalographic monitoring in comparison with simultaneous continu-ous conventional electroencephalography for seizure detection in terminfants. Pediatrics 121:1146-1154, 2008
4. Sankar R, Painter MJ: Neonatal seizures: After all these years we stilllove what doesn’t work. Neurology 64:776-777, 2005
5. Bartha AI, Shen J, Katz KH, et al: Neonatal seizures: Multicenter vari-ability in current treatment practices. Pediatr Neurol 37:85-90, 2007
6. Wheless JW, Clarke DF, Arzimanoglou A, et al: Treatment of pediatricepilepsy: European expert opinion. Epileptic Disord 9:353-412, 2007
7. Boylan GB, Rennie JM, Pressler RM, et al: Phenobarbitone, neonatalseizures, and video-EEG. Arch Dis Child Fetal Neonatal Ed 86:F165-F170, 2002
8. Painter MJ, Scher MS, Stein AD, et al: Phenobarbital compared withphenytoin for the treatment of neonatal seizures. N Engl J Med 341:
485-489, 19999. Shany E, Benzaqen O, Watemberg N: Comparison of continuous dripof midazolam or lidocaine in the treatment of intractable neonatal sei-zures. J Child Neurol 22:255-259, 2007
0. Boylan GB, Rennie JM, Chorley G, et al: Second-line anticonvulsanttreatment of neonatal seizures: A video-EEG monitoring study. Neu-rology 62:486-488, 2004
1. Shoemaker MT, Rotenberg JS: Levetiracetam for the treatment of neo-natal seizures. J Child Neurol 22:95-98, 2007
2. Silverstein FS, Ferriero DM: Off-label use of antiepileptic drugs for thetreatment of neonatal seizures. Pediatr Neurol 39:77-79, 2008
3. Kim JS, Kondratyev A, Tomita Y, et al: Neurodevelopmental impact ofantiepileptic drugs and seizures in the immature brain. Epilepsia 48:19-26, 2007
4. Koh S, Tibayan FD, Simpson JN, et al: NBQX or topiramate treatmentafter perinatal hypoxia-induced seizures prevents later increases in sei-zure-induced neuronal injury. Epilepsia 45:569-575, 2004
5. Schubert S, Brandl U, Brodhun M, et al: Neuroprotective effects oftopiramate after hypoxia-ischemia in newborn piglets. Brain Res 1058:129-136, 2005
6. Sfaello I, Baud O, Arzimanoglou A, et al: Topiramate prevents excito-toxic damage in the newborn rodent brain. Neurobiol Dis 20:837-848,2005
7. Dzhala VI, Brumback AC, Staley KJ: Bumetanide enhances phenobar-bital efficacy in a neonatal seizure model. Ann Neurol 63:222-235,2008
8. Kahle KT, Staley KJ: The bumetanide-sensitive Na–K-2Cl cotransporterNKCC1 as a potential target of a novel mechanism-based treatmentstrategy for neonatal seizures. Neurosurg Focus 25:E22, 2008
9. Vanhatalo S, Hellstrom-Westas L, De Vries LS: Bumetanide for neonatalseizures: Based on evidence or enthusiasm? Epilepsia 50:1292-1293,2009
0. Ben-Ari Y, Holmes GL: Effects of seizures on developmental processesin the immature brain. Lancet Neurol 5:1055-1063, 2006
1. Wirrell EC, Armstrong EA, Osman LD, et al: Prolonged seizures exac-erbate perinatal hypoxic-ischemic brain damage. Pediatr Res 50:445-454, 2001
2. Liu Z, Gatt A, Werner SJ, et al: Long-term behavioral deficits followingpilocarpine seizures in immature rats. Epilepsy Res 19:191-204, 1994
3. Sayin U, Sutula TP, Stafstrom CE: Seizures in the developing braincause adverse long-term effects on spatial learning and anxiety. Epilep-sia 45:1539-1548, 2004
4. Holmes GL, Ben-Ari Y: Seizures in the developing brain: perhaps not sobenign after all. Neuron 21:1231-1234, 1998
5. Holmes GL: Effects of early seizures on later behavior and epileptoge-nicity. Ment Retard Dev Disabil Res Rev 10:101-105, 2004
6. Younkin DP, Delivoria-Papadopoulos M, Maris J, et al: Cerebral meta-bolic effects of neonatal seizures measured with in vivo 31P NMRspectroscopy. Ann Neurol 20:513-519, 1986
7. McBride MC, Laroia N, Guillet R: Electrographic seizures in neonatescorrelate with poor neurodevelopmental outcome. Neurology 55:506-513, 2000
8. Miller SP, Weiss J, Barnwell A, et al: Seizure-associated brain injury interm newborns with perinatal asphyxia. Neurology 58:542-548, 2002
9. Glass H, Glidden D, Jeremy RJ, et al: Clinical neonatal seizures areindependently associated with outcomes in infants at risk for hypoxicischemic injury. J Pediatr 155:318-323, 2009
0. Toet MC, Groenendaal F, Osredkar D, et al: Postneonatal epilepsyfollowing amplitude-integrated EEG-detected neonatal seizures. Pedi-atr Neurol 32:241-247, 2005
1. Brunquell PJ, Glennon CM, DiMario FJ, et al: Prediction of outcomebased on clinical seizure type in newborn infants. J Pediatr 140:707-712, 2002
2. Hall RT, Hall FK, Daily DK: High-dose phenobarbital therapy in termnewborn infants with severe perinatal asphyxia: A randomized, pro-
spective study with three-year follow-up. J Pediatr 132:345-348, 1998