Neonatal problems
40
Neonatal problems November 14 th 2012
description
Neonatal problems. November 14 th 2012. Aims. Neonatal and 6-8/52 exam Common problems: Feeding Breathing Infection Constipation Skin Sleep SIDs. Newborn and 6/52 check. Head to toe… General Head Fontanelles Eyes Palate Tongue Ears Chest Abdo Umbilicus Genitals Anus. - PowerPoint PPT Presentation
Transcript of Neonatal problems

Neonatal problems
November 14th 2012

Aims
• Neonatal and 6-8/52 exam• Common problems:
• Feeding• Breathing• Infection• Constipation• Skin• Sleep • SIDs

Newborn and 6/52 check• Head to toe…
– General– Head
• Fontanelles• Eyes• Palate• Tongue• Ears
– Chest– Abdo
• Umbilicus• Genitals• Anus
– Spine– Hips & femorals– Feet– Skin– Tone



HEAD
• All tongue ties require referral for surgery.
False
Only requires surgery if interferes with feeding talkingIf they need referral then send to ENT

• Cleft palates can be a routine OPA with paeds.
FalseRefer into cleft palate specialist team – they link in with Leeds if requires surgery
Help with specialist feeding bottles and support
Cleft palate, unilateral cleft palate, bilateral cleft palate

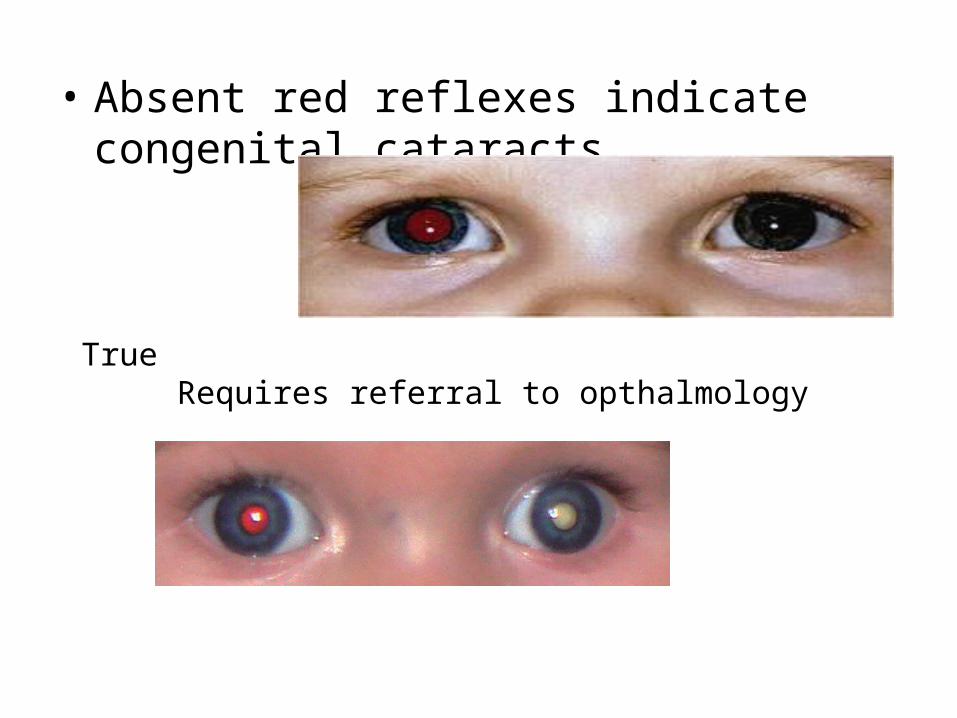
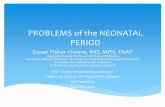
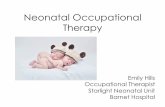
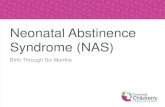
• Absent red reflexes indicate congenital cataracts.
True Requires referral to opthalmology
• Squints do not require referral to secondary care – they always correct themselves.
False
Require referral into paediatric optometryAsk about:
FHxParents notedBilateral reflexes

Chest• Only cardiac murmurs found after 6/52 need referral.
FalseAll murmurs (if I can hear them!) should be referred into paeds – particularly if doing neonatal check – when ductus arteriosus (aorta to pulmonary artery) closes baby could collapse.Refer if there is no murmur but they are symptomatic including cyanosis, breathlessness, not feeding, ‘not quite right’3 main causes : valve problems, narrowing (ie coarctation) holes – PDA/VSD/ASDTake home points: if it’s loud/diastolic/harsh/sick ADMIT Routine referral to Consultant of the Week

• Absent femoral pulses are diagnostic of Tetralogy of Fallot
False…indicates coarctation of aorta.

Pelvis
• Imperforate anus requires urgent referral to paeds and surgical intervention.
True
Remember to ask re bowel habits ie meconium…

• Bilateral undescended testes can be monitored until 1yr of age when requires referral to paeds.
FalseCould be female baby
Could have CAH and at risk of fits/serious illness and death
If there is one that is present then refer at 1yr if unable to find the other one…routine referral

• Hypospadias requires urgent referral to paeds.
FalseRoutine referral to paeds
Usually seen in combined clinic
Surgery is timed to avoid problems with pottytraining
Need to avoid being circumcised prior to repair
Case study…

• Risk factors for DDH include:• Female gender• Breech• Twin• FHx• Oligohydramnios
True All above are risk factors
Look at leg creases
Requires an USS at 6/52
Routine referral to paeds with results of USS

Spine• Referral is required if cannot see the bottom of a sacral
pit
True
Implication is of spina bifidaLook for hair, tone & power of lower limbsRoutine OPA

• All babies with talipes require a referral to paeds.
FalseCheck if positional in neonatal check
If still present at 6/52 or not correctable then refer to paediatric physio via paeds

Red Book
• Weigh, measure and plot!

Sticky eyes• Chlamydia, gonorrhoea, GBS, staph a and
pseudomonas can all cause conjunctivitis in the neonate.
TrueSwab for MC&S and treat with results
Admit if unwell - obviously!!!!

• Blocked tearducts need to be referred if not resolved by 6 months.
False
Refer to opthalmology at 1yr if not resolved but most do
Affects 1 in 5 babies
Can be unilateral/bilateral
Do nothing/ massage and keep eye clean

Feeding• Breastfeeding is a piece of cake and anyone can do it
straightaway.
FALSE!!!!
Baby Friendly Initiative implemented
Good support from midwives and health visitors

• Up to 6/12 of age babies need 100mls/kg/24hrs
False
They need 150mls/kg but should feed on demand initially
–Newborns feed three hourly, –6/52 feed four hourly, –6-16/52 reducing down as baby starts to sleep through the night –Some babies cluster feed in the evening
GORD• Nearly all symptomatic reflux will have resolved by 1yr of
age
True• ? Related to feeding/posture/maturation of sphincter• Frequent small meals• Gaviscon• Mild sx responds to thickener
– Carobel, Thick’n’easy, actimel antireflux• Cow’s milk free diet
– Nutramigen

Vomiting• Daily vomiting is not common in children at the age of 4/12
False
Regurgitation occurs at least once per day: 50% of infants between 0–3 months 67% of infants at 4 months 5% at 10 to 12 months of age
Often caused by rotavirus – will be vaccination soon

Colic• Infantile colic occurs in up to 20% of children?
– True• Differential diagnosis:
– OM– Strangulated hernia– UTI– Anal fissue– Intussusception
• Treat with infacol• Colief if they are lactose intolerant

Oral candidisis• Oral thrush always needs treating in the baby
False only treat if mum/baby is symptomatic (ie
painful/affecting feeding
Treat with nystatin solution for baby and topical miconazole for mum

Breathing problems• 90% of cases of bronchiolitis are caused by respiratory
syncytial virus
True• Parainfluenza, influenza, rhinovirus, adenoviruses• Recovery lasts for 7-10 days

• Whooping cough vaccines need to be given to pregnant women between 28-32wks gestation.
TrueGives immediate but short-lived immunity to newborn
Transmitted by droplets
7-14 day incubation period
5/7 exclusion (nursery) from start of Abx
Azithromycin, clarithromycin, erythromycin

Constipation• Red flags include:
– From birth/first few weeks
– Ribbon stools
– No meconium within 48hrs
– Locomotor delay/leg weakness
– Abdominal distension with vomiting
– Abnormal abdo, leg, spinal exam

• Faltering growth is an amber flag
TrueTreat constipation
Ix for hypothyroidism and coeliac disease
Consider maltreatment
• Refer urgently

• It is important to discuss diet and fluid intake with parents/guardians.
True. • Medication steps include:
– 1. macrogol– 2. lactulose– 3. senna
• Behavioural measures

Skin• Nappy rash can have secondary infection which requires
treatment
True
Treat with antifungal (canestan/timodine)
More likely to be fungal if spread to flexures
Persists despite tx and hygiene measures/avoidance of detergents then non-urgent referral

• Naevus > 2cm need referral to paediatricsTrue
At risk of malignant changeNot usually before puberty

Sleeping habits• Newborn babies sleep for 16hrs per day
True– At about 8/52 babies should be starting to get used to
sleeping in a cot and being put down to sleep whilst they are still awake…
• Newborn babies should sleep in their parents bed until they are 1.
– Ummm definitely not!!!– Sleep in the same room for first 6 months

• Newborn babies should sleep in their parents bed until they are 1.
FalseSleep in the same room for first 6 months
Can lay on front if is being observed from about 8/52

Cot death• 90% occur within the first 6/12 of life
TrueMost occur during the second month then risk gradually reduces– Risk factors include:
• Parental smoking• laying baby on front or side to sleep• Male• Prematurity• Low birth weight• Formula feeding

Cot death

Summary• If in doubt call the friendly paeds reg/consultant – better
to be safe than sorry.

References• Nice Guidelines: Routine postnatal care of women and
their babies 2006• www.patient.co.uk• Department of Health (2005) Reduce the risk of cot
death: an easy guide. London: Department of Health. Available from: www.dh.gov.uk
• Nice Guidelines: Constipation in children and young people