NEONATAL NUTRITION pro PIT 3.ppt
69
Early Parenteral Nutrition of the Preterm Infant Benefts and risks Johanes Edy Siswanto Harapan Kita Women and Children Hospital Pernatology Working Group PIT Medan 20- 24 Peruari 20!0
-
Upload
andi-dewi-pratiwi -
Category
Documents
-
view
20 -
download
0
Transcript of NEONATAL NUTRITION pro PIT 3.ppt
-
Early Parenteral Nutrition of the Preterm Infant Benefits and risks
Johanes Edy SiswantoHarapan Kita Women and Children HospitalPernatology Working Group
PIT Medan20- 24 Pebruari 2010
-
Neonatal NutritionThe ultimate goal for growth of the infant in the neonatal intensive care unit (NICU) is replication of in utero growth.
Due to the immaturity of the prematures gut, it is often difficult to achieve full enteral feeds in a timely fashion. In addition, mothers breast milk is not sufficient to match in utero growth of the extremely premature infant.
It is however difficult to meet in utero growth accretion with strictly parenteral nutrition and complications of parenteral nutrition may cause severe problems for the premature.
-
Rate of weight gain in fetus highest between 26 and 36 weeks Aim: Growth standardGrowth of the preterm infant should be similar tointrauterine growth of a fetusat the same gestational age,approximately 15g/kg/day. AAP 1998
-
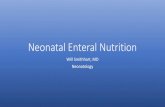
Body weight in an AGA and SGA 27 week infant who gains 15g/ kg/ day. (from Cooke R, J Perinatol 2005)
-
Caloric deficiency in the NICUDecreased caloric reserves at birthIncreased requirement forwork of breathingtissue repairgrowth
-
Estimated caloric requirement of a growing preterm infant (AAP 1985)
Kcal / kg / day
Resting metabolic rate
50
Cold stress
10
Activity
15
Synthesis / thermic effect of food
8
Fecal loss
12
Growth
25
Total
120
-
Parenteral Nutrition : Common PracticeGlucose infusions started earlyAmino acids started in first week of life and advanced slowly at 0.5 gm. IncrementsLipid infusions started in first week of life and advanced slowly at 0.5 gm. IncrementsAmino acids and lipids frequently delayed or interruptedTradition, Possible Metabolic acidosis, Possible uremia, Hyperlipidemia, Sepsis, Displacement of bilirubin
-
Reasons to withhold Parenteral nutritionTraditional Approach
Delayed initiation of TPN for 2-3 days:Electrolyte stabilityMetabolic stabilityHemodynamic stabilityPractical or technical contraindications
ProblemsNo medical or scientific reasons for delayIrrepressible gluconeogenesis and proteolysis or starvation responseState metabolic shock if no adequate nutrition
-
We Create Malnutrition In The NICU ?!!
-
Early Parenteral Nutrition
-
Intravenous Nutrition ( IVN ) : Four General Principles : Bill Hays Rules Metabolic and nutritional requirements do not stop with birthIntravenous feeding is always indicated when normal metabolic and nutritional needs are not met by normal enteral feeding
-
Intravenous Nutrition ( IVN ) : Four General Principles3. Hours, not days, are the longest periods infants should be allowed to not receive nutrition, IV or PO4. The metabolic and nutrient requirements of the newborn are equal to or greater than those of the fetus
-
Indications for TPN
Route Indication for TPN Peripheral Temporary supply of nutrients < 2 wk: Enteral intake Functional gut immaturity Temporary feeding intolerance Central Prolonged non-use of the GI tract > 2 wk: Surgical GI disorders Necrotizing enterocolitisShort bowel syndrome ELBW
-
Benefits of Early Parenteral Nutrition Using a Strategy Of Early Aggressive Parenteral Nutrition Instituted as soon as possible after birth Providing nutrient delivery at rates that are safe and beneficial has potential to :be cost effectiveAllow for reasonable nutritional continuity in the transition from intrauterine to extrauterine lifeContributes to reversing the current epidemic of postnatal growth failure in very preterm neonatesImprove developmental outcomes
-
What we know -early parenteral nutrition Significant protein and caloric deficits occur in the early neonatal period and are difficult to recoup in extremely premature infants. Embleton, Pediatrics 2001
Protein deficit early in the neonatal period is an important contributor to poor growth, particularly in extremely low birth weight infants (ELBW). Replication of intrauterine growth and nutrient accretion is difficult for ELBW infants due to their high rate of protein turnover and catabolism. Denne SC, Poindexter BB. Semin Perinatol 2007; 31:56-60
-
Studies have shown that negative nitrogen balance in sick premature infants who received glucose alone can be reversed with an amino acid (AA) intake of 1.1-2.5 gDenne SC, Poindexter BB. Semin Perinatol 2007; 31:56-60 Numerous studies indicating early parenteral protein and energy delivery in the first 2 weeks of life allows for earlier regain of birth weight that is not due to fluid retention
-
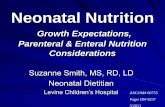
Longitudinal growth of hospitalized very low birth weight infants. ( Ehrenkranz RA, et al. Pediatrics 1999)
-
Our approach to early aggressive parenteral nutritionThe very preterm newborn :A NUTRITIONAL EMERGENCYGlucose stores of only 200 kcalCatabolic : net protein loss - with IV glucose alone, loss 1% body protein/day -10% loss of protein stores = protein malnutrition
-
Our Primary Nutrition Goal : Protein Accretion- Practical Aproach Protein gain is the best indicator of real growth Greatest rate relative protein gain throughthout life occurs prior to birth Minimum parenteral amino acid intake - zero balance (i.e. not catabolic) - can be achieved with 1.0-1.5 g/kg/d protein
-
Protein Quantity is the Primary Determinant of Protein Accretion Maximum Parenteral Intake Yet to be defined, limited by concerns of toxicity If goal is to achieve fetal delivery rates (Ziegler): - 24-25 weeks 3.75 - 4.0 g/kg/d - 27-28 weeks 3.5 g/kg/d - 32 weeks 3.2 g/kg/d - term infants 2.8 3.0 g/kg/d
-
Our Parenteral Nutrition Goal : Early Aggressive Nutritional Support Start TPN day of life # 1 Give amino acid to prevent catabolism and ideally in amount that produce growth Advance glucose and lipids as rapidly as tolerated Early protein loses in ELBW infants can be minimized by providing parenteral amino acids, event at low caloric intake
-
Example stockor stater Amino Acid (AA) solutions2% AA in D10W at 60ml/kg/d 1.2 g/kg/d/ AA2% AA in D10W at 80ml/kg/d 1.6 g/kg/d/ AA 5% AA in D10W at 60ml/kg/d 3.0 g/kg/d/ AA
If you start with 5% AA you cant increase the fluid rate! Additional fluids can be co-infused if glucose and/or electrolyte requirements change
-
Beneficial Effect of Amino Acid Intake on Hyperglysemia In our 1 vs 3 g/kg/d amino acid intake study, insulin concentration correlated with amino acid intake Our incidence of neonatal hyperglycemia has dramatically decreased since instituting : Early parenteral amino acids Glucose infusion less than the maximal oxidative glucose capacity Early minimal enteral feeding
-
Other benefits of Early Amino Acids Several studies have correlated early and high protein intake ( enteral and parenteral ) with improved growth at hospital discharge Early and Aggressive nutritional strategy (parenteral and enteral) decreases postnatal growth failure in very low birth weight infants. Dinerstein A et al, J Perinatol 2006
Both early and/or late amino acid intake has been associated with improved outcome in infants with BPD Ho MY, Nutrition 2003, PorceIII, J pediatr-Gastroenterol Nutr 2002
-
Potential Benefits of Early Protein intake on Growth and Development
Early studies by Lucas and colleagues suggested that a higher protein intake early in life in preterm infants will improve growth and neurodevelopmental out comes
They also concluded the first 2 weeks of life in the preterm infant may represent a critical growth window during which nutrition (particulary protein nutrition may have its greatest beneficial and adverse effectsLucas A, Morley R, Cole TJ, Randomized trial of early diet in protein babies and later intelligence quoitient, Br Med J 1998; 317 1: 481-7
-
How Much Protein and How Quickly ? Low vs High Amino Acid Intake StudyHypothesis :In ELBW infants in the first 48 hours of life receiving Low ( 1 g/kg/d ) versus High ( 3 g/kg/d ) IV amino acid intake, the High intake would be : 1) More efficacious (improved protein accretion) 2) Safe : no significant acidosis, elevated BUN, abnormal amino acid concentrations
-
Study Conclusions
Efficacy : ELBW neonates on 3 g/kg/d parenteral amino acids immediately after birth have significantly greater rates of protein accretion compared to those on 1 g/kg/dSafety : Based on BUN and plasma amino acid measurements, 3 g/kg/d amino acid IV amino acid intake appears to be tolerated immediately after birth in ELBW neonates
-
Poindexter, in a study for the NICHD (National Institute of Child Health and Development) Research Network, demonstrated that 3 g/kg of amino acids in the first five days of life in premature infants was associated with significantly better outcomes at 36 weeks postmenstrual age (gestational age plus chronological age) and less suboptimal head growth at 18 months chronologic age.
Poindexter BB, Langer JC. Early provision of parenteral amino acids in extremely low birth weight infants: relation to growth and neurodevelopmental outcome. J Pediatr 2006; 148: 300-5
-
The efficiency of protein retention during parenteral nutrition is approximately 70%. Based on this assumption and the proven benefits of early AA intake in limiting protein catabolism, it is reasonable to recommend 2.5 3.0 g/kg/day of AA intake directly after birth in premature infants.
Parenteral protein of 3.5-4 g/kg/day may be required in ELBW infants to maintain endogenous stores, taking into account accretion goals and the rate of protein loss in the neonatal period.
-
Safety and Benefits of Early Amino Acids Administration For VLBW Infants STUDY AA SolutionAnderson (1979)AminosynSaini (1989) Vamin-9Van Lingen (1992) AminovenousRivera (1993) Aminosyn-PFKashyap (1994) TrophamineVan Goudover (1995) PrimeneThureen (1998) TrophamineThureen (2003) Trophaminete Braake (2005) Primene
None of the above specificaly designed for the ELBW infants
-
Early Parenteral Nutrition : Risks and Unresolved Issues
Effect of Quality of Parenteral Amino Acid Intake on Maximizing Protein growthMaximal protein accretion depends on providing the perfect balance of amino acidsThe optimal ratio of amino acids in parenteral nutrition of the preterm infant is unknownIn theory, deficiency of one essential amino acid will ~ limit overall protein synthesis, and ~ all other amino acids will be in relative excess and will be preferentially oxidized (used for energy)
-
How Much Protein and How QuicklyAre Early High Amino Acids Safe ? Current markers used to determine parenteral amino acid intolerance :- Metabolic acidosis : All LBW infants receiving up to 3 g/kg/d amino acids develop metabolic acidosis between 2-5 days after birth irrespective of dose and duration of parenteral amino acid administration, and this is exaggerated by associated co-morbidities such as PDA. - High ammonia concentration - Elevated blood urea nitrogen ( BUN ) - Abnormal plasma amino acid levelsReliable and sensitive markers of amino acid intolerance still need to be defined
-
CarbohydrateIn utero the foetus glucose utilisation matches the umbilical glucose uptake; hence, there is no need for either glycogenolysis or gluconeogenesis. This changes upon birth. In the term infant, glucose utilisation is 3-5 mg/kg/min, however utilisation in the premature may be as high as 8 mg/kg/min.
The exact definition of both hypoglycaemia and hyperglycaemia has remained problematic. However, it seems prudent to maintain a premature infants blood glucose between 40-50 mg% and 150 mg% Ehrenkranz RA. Early Semin Perinatol 2007; 31: 48-55.This necessitates the initiation of an intravenous glucose infusion at a rate of roughly 6 mg/kg/min in the premature immediately following birth.
-
CarbohydrateHyperglycaemia is quite common in the extremely premature infant and has been associated with a number of significant morbidities including sepsis, intraventricular haemorrhage, retinopathy of prematurity and ultimately death.
It is most commonly caused by low insulin levels due to defective proinsulin processing, and relative insulin resistance due to the stress response Mitanchez-Mokhtari D, Lahlou N, Magny JF et al. Pediatrics 2004; 113: 537-41
-
CarbohydrateA glucose infusion of 6 mg/kg/min should be started on all premature infants upon admission to the nursery. This should be gradually increased to 10 mg/kg/min over the first week of life. The infants blood glucose level should be maintained between 50-120 mg%.
Should the infant become hyperglycaemic early on, an insulin infusion (0.01-0.1 units/kg/hr) should be started rather than decreasing the dextrose concentration to less than 5%. Ehrenkranz RA. Semin Perinatol 2007; 31: 48-55.
-
LipidStarting IV lipid in very low birth weight VLBW infants at an early age has the advantage of providing a source of essential fatty acids, as well as supplying non-carbohydrate calories. Essential fatty acid deficiency can develop in as few as three days in extremely premature infants.
Lipid infusion may be safely started on day 1 of life at 0.5-1.0 g/kg/day and may be increased by up to 1 g/kg/day to a maximum of 3-4 g/kg/day Triglyceride levels should be followed and lipid infusion temporarily discontinued if the triglyceride level exceeds 150-200 mg/dL .Valentine CJ, Puthoff TD. Enhancing parenteral nutrition therapy for the neonate. Nutr Clin Pract 2007; 22: 183-93.
-
LipidThere have been alternative lipid infusions proposed that differ in composition from current solutions. A recent review paper summarised several in vitro and in vivo studies comparing olive oil to soybean oil-based intralipid preparations.
Olive oil solutions contain decreased concentrations of n-6 poly unsaturated fatty acid (PUFA) which has been noted to adversely affect leukocyte recruitment, and also contain -tocopherol, a naturally occurring antioxidant.Olive oil-based infusions are well tolerated, and may offer advantages for immune function and decreased oxidative stress in the very-low birth weight infant.
Vila A, Barbosa VM, Calder PC. Olive oil in parenteral nutrition. Curr Opin Clin Nutr Metab Care 2007; 10: 165-174
-
Rationale for Providing Lipids Early Endogenous lipid stores are about 20 g in a 1000 g ELBW. How long will this last ?Essential Fatty Acid (EFA) status in early infancy is low and is rapidly exacerbated with lipid free nutritionLong Chain Polyunstaturated Fatty Acid (LCPUFA) derivatives from EFAs are important in brain and retinal developmentPrevention of catabolism and protein sparing
-
ENERGY REQUIREMENTSOptimal early nutrition is critical for growth, long-term outcome and decreased morbidities in the low birth weight preterm (LBW). The goal is to achieve a growth rate similar to in utero foetal growth: 15-20 g/kg/d, which requires 120 cal/kg/d enterally. Yu VYH, Simmer K, Digital Education Publishing, Inc. 2005: 311-332If on TPN, positive nitrogen balance can be attained with 60 cal/kg/d with about 2.5 g/kg/d of proteinMinimal caloric intake for weight gain is about 80 cal/kg/d if on TPN
- When to start lipidsASAP at least enough to prevent EFA deficiency (0,5 gr/kg/d)Usssually not more than 3,0 gm/kg/d should be providedHyperlipidemia tough to monitorProlonged infusions usually safe (
-
IV Lipids in Premature InfantsEssential fatty acid (EFA) deficiency - IV lipid emulsion (intralipid) is 50% EFA - Prevented and/or treated with 0.5 g/kg/d ~ 4 % energy intakeEnergy source (calorie distribution~40%) - Administer continuosly over 24 h - Use 20 % IL not 10 % IL - Increase dose daily by 1.0 g/kg/d Max dose 3.0 g/kg/d - Long-term TPN 3.5-4.0 g/kg/d Monitor serum triglycerides (arbitrary value< 150 mg/dL) - After each change in dose - Weekly - During any stress (infection,respiratory)
-
Essential Fatty Acid Deficiency in Premature infantsClinical manifestation Dermatitis Hepatic steatosis Hematologic disturbances Diminished immune system status
-
Intravenous Lipids Are Poison ?
-
Are there contraindications to parenteral lipids ?Concerns have been raised about potential adverse effects including : - Increased risk for chronic lung disease (CLD) - Increase in pulmonary vascular resistance - Impaired pulmonary gas diffusion - Bilirubin toxicity - Interference with immune function and/or platelet function - Sepsis - Free radical stress
-
May need to decrease lipid 0,5 1.0 g/kg/d for a short period of time in infants with :PPHNSevere lung diseaseSevere infectionSteroid useElevated level bilirubin concentrationsHyperglycemiaHypertriglyceridemia
-
Electrolytes and Trace Element Deficiencies
Most deficiencies of electrolytes and trace elements are secondary to improper supplementation and monitoring. Excess fluid loss, from vomiting, diarrhea, wounds or other secretions, may result in additional electrolyte losses and loss of some trace elements, such as zinc. Careful monitoring of electrolytes and fluid losses is necessary to avoid deficiencies. Adequate calcium intake is essential for bone growth.
-
Electrolyte Body Fluid Composition in Neonates (in mmol/L)13 .Fanaroff A, Martin R, editors. Neonatal-Perinatal Medicine. 5th edition. St. Louis: Mosby Year Book. Chapter 31.
-
Contoh FORMULA TPN : Total cairan yang diberikan untuk bayi = 80 mL/kg bb/hari
Kebutuhan asam aminobila dibutuhkan asam amino 3 g/kg/hari dan digunakan sediaan Aminosteril infant 6% (6gr/100mL) maka diperlukan 50 mL/kg bb/hari
Kebutuhan karbohidratGIR (mg / kg / menit) = Volume (mL / kg / hari) x Konsentrasi Glukosa 144 bila dibutuhkan karbohidrat 4 g/kg/hari dan digunakan D40% maka diperlukan 10 mL/kg bb/hari. GIR : (10 x 40 )/144 = 2,8 mg / kg /menit6 g/kg/hari D40% diperlukan 15 mL/kg bb/hari. GIR :15 x 40 )/144 = 4,2 mg / kg /menit sedangkan AA 6% 2,7 gr/kg/hari
-
Kebutuhan calsium pada infant 1 3 mEq /kg.Misal dibutuhkan calsium 1,5 mEq maka dibutuhkan calsium sebanyak 0,75 mmol. Sediaan yang ada : calsium glukonat 100mg/mL (10mL) dimana 1 gram Calsium glukonat setara dengan 2,2 mmol Calsium.Jadi , 0,75 mmol Calsium setara dengan 340 mg Ca, dibutuhkan 3,4 mL
Sediaan TPN :AA 6% : 50 mL/kg bb/ hariD40%: 10 mL/kg bb/ hariCa glukonat: 3,4 mLAd Aqua: 16,2 mL 80 mL /kg bb /hari
-
OSMOLALITASPerhitungan Osmolalitas Sediaan TPN yang biasa digunakan :Asam amino 6 % = 50 cc/kg BB/hari= 0.573 x 50 = 28.65 mOsmD40%= 10 cc/kg BB/hari= 2.018 x 10 = 20.18 mOsmCa. Gluconas= 3.2 cc= 0.308 x 3.2= 0.98 mOsmAqua inj= 16.8 cc ________________________________80 cc/kgBB/hari= 49.81 mOsm
Jika dikonversi ke dalam satuan mOsm/Liter maka diperoleh osmolalitas 622,63 mOsm/L. larutan bersifat hipertonis.Disarankan metode infus Central Parenteral Nutrition untuk mencegah terjadinya tromboplebitis dan ekstravasasi oleh adanya calsium.
Asam amino 6 % = 45 cc/kg BB/hari= 0.573 x 45 = 25.79 mOsmD40%= 15 cc/kg BB/hari= 2.018 x 15 = 30.27mOsmCa. Gluconas= 3.2 cc= 0.308 x 3.2= 0.98 mOsmAqua inj= 16.8 cc ________________________________80 cc/kgBB/hari= 57,04 mOsm
738 mOsm/L
-
OsmolaritasOsmolaritas adalah konsentrasi dari zat terlarut (solute) dalam suatu larutan per unit dari pelarut (solven), biasanya mmol solute per liter
Tonicity is the effective osmolality and is equal to the sum of the concentrations of the solutes which have the capacity to exert an osmotic force across the membrane.
-
Complications of TPN
-
Dextrose-Related Complications
Hypo- and hyperglycemia are common problems found with the administration of parenteral nutrition.11,13,15 Neonates are more prone to hypo- or hyperglycemia than older infants and children. Neonates have inadequate stores of glycogen and a limited ability for glycogenolysis, due to poor enzyme activity.
Hypoglycemia frequently occurs when parenteral nutrition solutions are stopped. For this reason, infusion rates should be tapered down prior to discontinuation of the nutrition solution.
-
Dextrose-Related ComplicationsHyperglycemia is a more common problem in the neonate. Immature alpha-cell and beta-cell function, slow release of insulin and a diminished tissue response all contribute to the development of hyperglycemia. In addition, hepatic glucose output is not reduced in response to external glucose. For this reason, parenteral nutrition solutions should be started with low dextrose concentrations or at slow infusion rates.
High blood glucose concentrations result in an increase in serum osmolarity and the development of osmotic diuresis and dehydration, and increase the risk of intracranial hemorrhage. Blood glucose should be monitored routinely and the glucose intake reduced if hyperglycemia occurs.
-
Lipid-Related Complication
Use of lipid emulsions has been associated with certain complications in the neonate, including hyperlipidemia, hyperbilirubinemia and changes in pulmonary function when the rate of administration is too fast.
Too rapid infusion of lipid emulsions may result in hyperlipidemia in the neonate. The ability of the neonate to effectively clear and utilize intravenous lipids is dependent on enzyme systems that vary with both weight and gestational age.
-
Lipid-Related ComplicationHyperbilirubinemia and jaundice occur frequently because the liver enzymes needed to conjugate bilirubin are reduced in the immature liver. When lipids are infused more quickly than they can be cleared from the blood, free fatty acid concentrations are increased. Bilirubin and free fatty acids both compete for binding to albumin. This displacement of bilirubin by free fatty acids results in higher serum concentrations of bilirubin and an increased risk of kernicterus.
Lipid may also cause changes in pulmonary function in the neonates. PO2 levels may be lowered due to changes in pulmonary microcirculation in neonates with RDS. Reducing the fat-to-carbohydrate ratio may minimize the adverse effects of lipids.
-
Complications of TPNAlthough TPN is necessary to provide nutrition to the LBW/VLBW neonate, there are several complications associated with its administration. Prolonged TPN therapy frequently necessitates placing a central IV catheter whose use carries with it several risks, including nosocomial infections, vascular thrombosis and cardiac tamponade. TPN associated cholestasis (TPNAC) has long been recognised as a metabolic complication of chronic TPN administration. It is characterised by intracanalicular and intracellular cholestasis. It has been reported that 8-50% of ELBW infants show signs of biochemical cholestasis after two weeks of TPN therapy.The incidence approaches 90% in infants who receive TPN for > 90 days Forchielli ML, Walker WA. Adv Pediatr 2003; 50: 245-68
-
Complications of TPN The pathophysiology of PNAC is still incompletely understood, but felt to be multifactorial in aetiology. Recent studies have focused on soybean oil-based lipid solution as possibly being causative of TPNAC. Phytosterols in soybean oil can damage the biliary tract and disrupt bile flow. A clinical study was performed on infants with PNAC while receiving soybean oil-based lipid emulsions. They were given fish oil-based lipid emulsions, and compared to an historical cohort that received soybean oil-based emulsions only. The fish oil group had a significantly shorter time to reversal of cholestasis compared to the soybean oil group (9 vs. 44 weeks) Gura KM, Lee S, Valim C et al. Pediatrics 2008; 121: e678-686
-
Complications of Parenteral Nutrition : PNACParenteral Nutrition Associated CholestasisEtiology of PNAC is unknown and likely to be multifactorial ; long list of associations with PNAC but minimal data on preventionRisk Factors Include : - Younger gestational age * Significantly increased if infants 3 weeks) - Absence of enteral feeding - Sepsis, cholangitis, bacterial translocation - Number of operative procedures - Male sex in surgical neonates (2002) - Length of hospital stay
-
Parenteral Nutrition Associated CholestasisPNAC defined as direct serum bilirubin above 5 mg/100 ml at any time in the first 28 days of life
Being SGA is an independent risk factor for PNACPediatrics, 2008, Robinson and EhrenkranzRisk factors include for those who developed PNAC vs those who did not : - Longer duration of TPN exposure - Higher cummulative dose of amino acids - More often had PDA, severe IVH - More often treated with steroids by 28 days of ageClark RH and the amino Acid study Group; J Perinat 2008
-
Toxicity of TPN componentsAnimal studies :Decreased bile flow with glucose infusionsCholestatic effect of amino acid infusions (esp. methionine,sulfur containing amino acids)Choline deficiency causes steatosis in ratsHuman studies :Hepatic dysfunction with infusion of excessive caloriesCholestatic effect of amino acid infusions ( trytophan, methionine, excess homocystine )Impaired bilirubin excretion in adults receiving high dose intravenous lipidsFree radical production is increased by administration of TPN in infants
-
PNAC Potential Therapeutic StrategiesAvoid glucose overloadProvide a mix of calories (dextrose, protein, and lipids) in appropriate ratios. Early detection and treatment of infectionFocused on making the transition to enteral feeds***Oral refeeding as soon as possible Ursodeoxycholic Acid ( UDCA ), a bile acid used in adult cholestatic liver disease.Prevent free radical production (cover lipid and TPN to avoid photo-oxidation )Increase anti-oxidant capacities of TPN solutions
-
PNAC Potential TherapiesThere is increasing evidence that fish oil based products may :Decrease the incidence of cholestasis andAmeliorate or even reverse existing cholestatic diseaseIts efficacy in treating and preventing TPNAC is controversial, as studies have not consistently shown benefit.
-
TPNrememberTPN is important Its not everythingBut without TPN especially in ELBW is nothing
-
ConclusionsThe goal of neonatal nutrition is to try to replicate in utero growth patterns. This is often not possible, particularly in the smallest infants.The development of intravenous solutions for nutrition of preterm infants has been a life-saving development allowing for provision of protein and energy in the immediate neonatal periodNevertheless, parenteral nutrition is still far from being the optimal method for promoting long-term growth in very preterm infants
-
ConclusionsSeveral management strategies to try to reach this goal :Amino acids of as much as 3 g/kg/day should be started parenterally as part of the infants initial IV solution. Glucose at a rate of 6 mg/kg/min should be started immediately after birth. Severe hyperglycaemia should be managed with an insulin infusion if the infant remains hyperglycaemic on a 5% dextrose infusion. An IV lipid solution of 1 g/kg/day should be started as early as day one or two of life. The major complication of parenteral nutrition, namely TPN associated cholestasis, is ultimately treated by advancing enteral feeds. Newer lipid preparations, however, show some promise in reversing the hepatic damage of prolonged TPN.
-
Terimakasih
*********************************************************************