Neonatal jaundice
49
ن الرحيم الرحم بسم
-
Upload
alya-imad -
Category
Health & Medicine
-
view
553 -
download
1
Transcript of Neonatal jaundice

بسم هللا الرحمن الرحيم

Neonatal jaundice
علياء عماد
فاطمة احمد
فاطمة حسين
فاطمة حسن

Definition:is a yellowing of the skin and sclera of a newborn infant caused by accumulation of Bilirubin( Hyperbilirubinemia) in the skin & mucous mambrene

Hyperbilirubinemia is a common and in most cases benign problem in neonates. Jaundice is observed during the 1st wks. of life in approximately 50- 60% of term newborns and 80% of premature infants. Its clinically visible when exceeds 5 mgm/dl.
Metabolism and secretion of bilirubinBilirubin -breakdown of hemoglobinUnconjugated bilirubin (insoluble in water) transported to liver- Bound to albumin Transported into hepatocyte (Ligandin / y- protein ) & conjugated - With glucuronic acid → now water solubleSecreted into bileIn ileum & colon, converted to stercobilin10-20% (Deconjugated by β glucuronidase)reabsorbed into portal circulation (Enterohepaticcirculation )and re-excreted into bile or into urine by kidneys - urobilinogen


Clinical Manifestations
• Yellow skin and sclera • Poor feeding• Brown urine• Fever• High pitch cry• Vomiting• without treatment can progress to acutebilirubin
Encephalopathy(kernicterus)

Physiologic jaundice : (Icterus Neonatorum)
Physiologic jaundice is a common cause of hyperbilirubinemia among newborns. It is adiagnosis of exclusion, made after careful evaluation has ruled out more serious causes of jaundice, such as hemolysis, infection, and metabolic diseases.

Physiological jaundice is jaundice that is present between day 2 and day 10

Characteristics:-1-The clinical pattern of physiologic jaundice in term infants includes a peak indirect-reacting bilirubin level of no more than 12 mg/dL on day 3 of life. In premature infants, the peak is higher (15 mg/dL) and occurs later (fifth day).
2-its disappears by one weak in full term infants & two weeks in preterm infants.3-serum bilirubin is rarly rising ata rate faster than 5 mg/dL/24 hr4- Healthy baby.

Pathologic jaundice
• Appears within 24 hours of age• Increase of bilirubin > 5 mg / dl / day• Total Serum bilirubin > 13 mg / dl in term
infant or 10 mg/dl in preterm.The direct bilirubin fraction is greater than1.5 mg/dLMay associated with acute hemolysis• Signs of an underlying illness

Risk factors for jaundice
1-low birth wt & prematurity2-polycythemia3-A sibling affected4-male sex5-hemolytic conditions6-sepsis7-ABO incompatibility

Types of neonatal jaundice


In Hemolytic disease of the
newborn (ABO / Rh)
Rh incompitability:• is the most common cause • < 1 mL of Rh-positive fetal blood is sufficient to sensitize the
Rh negative mother• 90% sensitization during delivery/abortionSo , most first born infants are not affected due to the short period of exposure which is insufficient to produce a significant maternal IgG antibody response. Sensitized mother produces Ab –IgG types—crosses placenta sensitized –small doses of Ag stimulate high Ab titer .So, risk and severity of sensitization response increases with each subsequent pregnancy with Rh-positive blood fetus

Not all mother produce hemolysis in their baby ??1. The baby may be Rh negative 2. Not all mother produce enough Abs3. The mother might have been immunized
by anti D immunoglobin4. Fetomaternal trasfusion occurs only in 50%
of preg5. When mother and baby ABO
incompatibale

ABO incompatibility
• if Mother is type O and the baby is either type A or B. O +ve Mothers makes antibodies which are IgM & IgG types , IgG types crosses the placenta
• No effects if the mother & baby have same blood group or baby is grp O, as there is nothing to make antibodies against.
• If mother - type A or B Makes antibodies (IgM) type so does not cross the placenta
So, even if baby has a different blood type no effect

Physiologic jaundice is a common cause of hyperbilirubinemia
among newborns. It is a diagnosis of exclusion, madeafter careful evaluation has ruled out more serious causes ofjaundice, such as hemolysis, infection, and metabolic diseases.
Physiologic jaundice is the result of many factors thatare normal physiologic characteristics of newborns:1- increased bilirubin production resulting from an increased RBC mass,2- shortened RBC life span,3- hepatic immaturity of ligandin and glucuronosyltransferase.
Physiologic jaundice

Crigler-Najjar syndrome is a serious, rare, autosomal
recessive, permanent deficiency of glucuronosyltransferasethat results in severe indirect hyperbilirubinemia.Type IIresponds to enzyme induction by phenobarbital, producingan increase in enzyme activity and a reduction of bilirubinlevels.Type I does not respond to phenobarbital and manifestsas persistent indirect hyperbilirubinemia, often leading to kernicterus
Gilbert disease is caused by a mutation of the promoter
region of glucuronosyltransferase and results in a mildindirect hyperbilirubinemia. In the presence of another icterogenicfactor (hemolysis), more severe jaundice may develop

Breast milk jaundice
may be associated with unconjugated hyperbilirubinemia without evidence of hemolysis during thefirst to second week of life.
Bilirubin levels rarely increase to more than 20 mg/dL.Interruption of breastfeeding for 1 to 2 days results in a rapid decline of bilirubin levels, which do not increase significantly after breastfeeding resumes.
Breast milk may contain an inhibitor of bilirubin conjugation or mayincrease enterohepatic recirculation of bilirubin because ofbreast milk glucuronidase

Direct-reacting hyperbilirubinemia (defined as a direct bilirubinlevel >2 mg/dL or >20% of the total bilirubin) is neverphysiologic and should always be evaluated thoroughlyaccording to the diagnostic categories
Etiology of Direct Conjugated Hyperbilirubinemia
Direct-reacting bilirubin (composed mostly ofconjugated bilirubin) is not neurotoxic to the infant but signifies a serious underlyingdisorder involving cholestasis or hepatocellular injury.


Best classified by age of onset and duration:
Early: within 24 hrs of life
Intermediate: 2 days to 2 weeks
Late: persists for >2 weeks
Causes of neonatal jaundice

Causes of neonatal jaundice
Early Intermediate Late/prolonged
• Haemolytic causes:
– Rh isoimmunisation
– ABO incompatibility
– G6PD deficiency
• Congenital infection
• Physiological jaundice
• Breast milk jaundice
(inadequate intake)
• Sepsis
• Haemolysis
• Crigler-Najjar syndrome
(glucuronyl transferase
absent/reduced)
• Polycythaemia, bruising
• Conjugated (dark urine, pale
stools):
– Bile duct obstruction
– Biliary atresia
– Neonatal hepatitis
• Unconjugated:
– Physiological
– Breast milk jaundice
– Infection
– Hypothyroidism

Kernicterus ( bilirubin encephalopathy):is a neurologic syndrome results when indirect bilirubin is
deposited in brain cells and disrupts neuronal metabolism and
function, especially in the basal ganglia.
Indirect bilirubin may cross the blood-brain barrier because of
its lipid solubility. Other theories propose that a disruption of
the blood-brain barrier permits entry of a bilirubin-albumin
or free bilirubin–fatty acid complex
Its characterized by severe athetoid
cerebral palsy, paralysis of upward gaze,
hearing loss & intellctual impairment& its preventable
Kernicterus

Kernicterus usually is noted when the bilirubin level isexcessively high for gestational age. It usually does not developin term infants when bilirubin levels are less than 20 to25 mg/dL, but the incidence increases as serum bilirubin levelsexceed 25 mg/dL

Pathalogy
Yellow staining of the brain with neuronal injury, there are necrosis, neuronal loss and gliosisIts commonly seen in the basal ganglia, hypocampus,cerebellum,brainstem & spinal cord

Risk factor for Kernicterus
1. Sever hyperbilirubinemia2. Prematurity3. Asphyxia 4. Acidosis ,hemolysis, hypoxia, hypothermia5. Hypoglycemia, sepsis, meningitis,
Other risks for kernicterus in term infants are hemolysis, jaundicenoted within 24 hours of birth, and delayed diagnosis of hyperbilirubinemia

Clinical featureThe earliest clinical manifestations of kernicterus are lethargyHypotoniairritabilitypoor Moro response poor feeding.
A high-pitched cry and emesis also may be present.
Early signs are noted after day 4 of life.
Later signs includebulging fontanelleopisthotonic posturingpulmonary hemorrhageFeverHypertonicityparalysis of upward gaze and seizures

Complication of Kernicterus
Infants with severe cases of kernicterus die in the neonatalperiod.Spasticity resolves in surviving infants, who maymanifest later nerve deafnesschoreoathetoid cerebral palsymental retardationenamel dysplasia and discoloration of teeth as permanent sequelae
PreventionKernicterus may be prevented by-avoiding excessively high indirect bilirubin levels
-avoidingconditions or drugs that may displace bilirubin from albumin.

Diagnosis of hyperbilirubiniemia

: • History ask about Antenatal history Drugs Trauma Family H/O of jaundice Liver disease H/O delayed feeding Sepsis Sibling jaundice Splenectomy in family

Examination :
• Look for yellowish discoloration of the skin, sclera and mucous membrane
• Gently pressing by finger on the tip of the nose
• Examination of liver and spleen for hepatosplenomegaly
• Look for the color of urine and• stool

Kramer index:
1.Face-5 mg/dl
2.Abdomen 15 mg/dl
5.Palms & sloes 20 mg/dl

LABORATORY TESTS
Physical evidence of jaundice is observed in infants whenbilirubin levels reach 5 to 10 mg/dL (versus 2 to 3 mg/dL inadults). When jaundice is observed, the laboratory evaluationfor hyperbilirubinemia should include
a total bilirubin measurement to determine the magnitude of hyperbilirubinemia.Bilirubin levels greater than 5 mg/dL on the first day of lifeor greater than 13 mg/dL thereafter in term infants should beevaluated further with measurement of indirect and direct bilirubin levelsblood typing Coombs testcomplete blood count, blood smearand reticulocyte count.

These tests must beperformed before treatment of hyperbilirubinemia with phototherapyor exchange transfusion. In the absence of hemolysisor evidence for either the common or the rare causes ofnonhemolytic indirect hyperbilirubinemia, the diagnosis iseither physiologic or breast milk jaundice. Jaundice presentafter 2 weeks of age is pathologic and suggests a direct-reacting Direct-reacting hyperbilirubinemia (defined as a direct bilirubinlevel >2 mg/dL or >20% of the total bilirubin) is neverphysiologic and should always be evaluated thoroughlyaccording to the diagnostic categories Direct-reacting bilirubin (composed mostly of conjugated bilirubin)is not neurotoxic to the infant but signifies a serious underlyingdisorder involving cholestasis or hepatocellular injury.

Treatment

phototherapy•is an effective and safe method for reducing indirect bilirubin
levels, particularly when initiated before serum bilirubin increases
to levels associated with kernicterus.
•In term infants, phototherapy is begun when indirect
bilirubinlevels are between 16 and 18 mg/dL.
• Under the effects of phototherapy light with maximal
irradiancein the 425- to 475-nm wavelength band, bilirubin is
transformed into isomers that are water soluble and easily
excreted.
• Blue lights and white lights are effective in reducing bilirubin
levels.
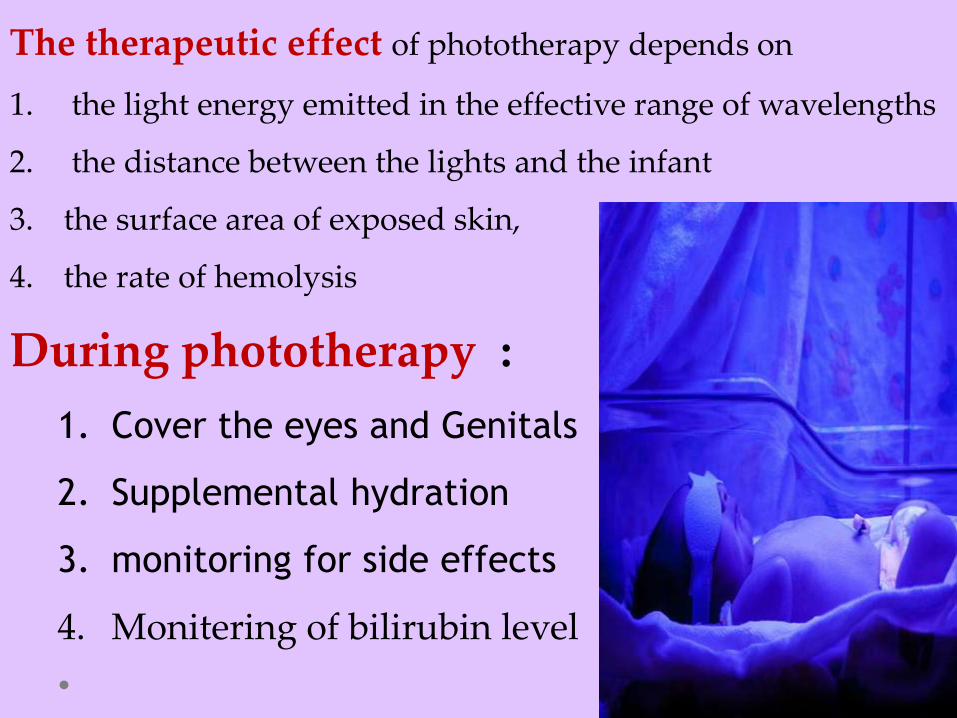
The therapeutic effect of phototherapy depends on
1. the light energy emitted in the effective range of wavelengths
2. the distance between the lights and the infant
3. the surface area of exposed skin,
4. the rate of hemolysis
During phototherapy :
1. Cover the eyes and Genitals
2. Supplemental hydration
3. monitoring for side effects
4. Monitering of bilirubin level

Serum bilirubin levels and hematocrit should be monitored every
4-8 hr in infants with hemolytic disease and those with
bilirubin levels near toxic range .
Complications of phototherapyEarly complication:
1. loose stools
2. erythematous macular rash
3. dehydration (increased insensible water loss, diarrhea)
4. bronze baby syndrome (which occurs in the presence of direct
hyperbilirubinemia)
5. lethargy, masking of cyanosis, nasal obstruction by eye pads

Late complication:
• Risk of skin malignancies
• Damage to intracellular DNA
• Retinal damage
• Testicular damage

Intensive phototherapy using light source above and beneath the infant using
in sever cases with risk of kernicterus
Home phototherapy This is an option way of treatment where facilities are
available and fiber optic blankets are commonly used
.the family should be well instructed and a well trained
nurse should be present it is usually used for simple
jaundice

Intravenous Immunoglobulin
The administration of intravenous immunoglobulin
use in treatment for hyperbilirubinemia due to
isoimmune hemolytic disease.
(0.5-1.0 g/kg/dose; repeat in 12 hr) has been shown to
reduce the need for exchange transfusion in both ABO
and Rh hemolytic disease, by reducing hemolysis

Exchange blood transfusionusually is used for infants with dangerously high
indirect bilirubin levels who are at risk for kernicterus .
The exchange transfusion usually is performed
through an umbilical venous catheter placed in the
inferior vena cava or,if free flow is obtained, at the
confluence of the umbilical veinand the portal system.

Indication:
• The appearance of clinical signs suggesting
kernicterus
• Rh and ABO incompatibility
• Unconjugated billirubin > 20 -25mg/dl in
term, >15 -18mg/dl preterm babies.
• Other disease :Septicemia ,DIC,Severe
anemia,…

Complications1. Problems related to the blood (transfusion reaction,
metabolic instability,or infection)
2. Problems related to the catheter (vessel perforation or
hemorrhage)
3. problems related to the procedure (hypotension or
necrotizing enterocolitis )
4. Unusual complications include thrombocytopenia and
graft-versus-host disease.

Prevention of neonatal jaundice :1. Promote and support breast feeding
2. Establish nursery protocols for identifying and evaluating
hyperbilirubinemia
3. Measure bilirubin levels in all neonate with jaundice in the first 24
hrs
4. Recognize that visual estimation of bilirubin level inaccurate
5. Interpret all bilirubin levels according to baby age in hrs
6. Identify preterm ,breast fed infant and provide close monitoring
7. Risk assessment for all newborn baby .
8. Give written and verbal information to familly
9. Treat newborns when indicated and appropriate follow up


فاطمة& علي بارك هللا لكما•
وبارك عليكما
وجمع بينكما
في خيـــر
مبروك الخطوبة