Neonatal intestinal obstruction
59
-
Upload
airwave12 -
Category
Health & Medicine
-
view
260 -
download
9
Transcript of Neonatal intestinal obstruction
Most common surgical emergency in neonates.
Management depends on timely diagnosis Needs radiological assessment Outcome excellent
Refusal to take feed. Vomitting. Abdominal distention. Delayed/failure to pass meconium.
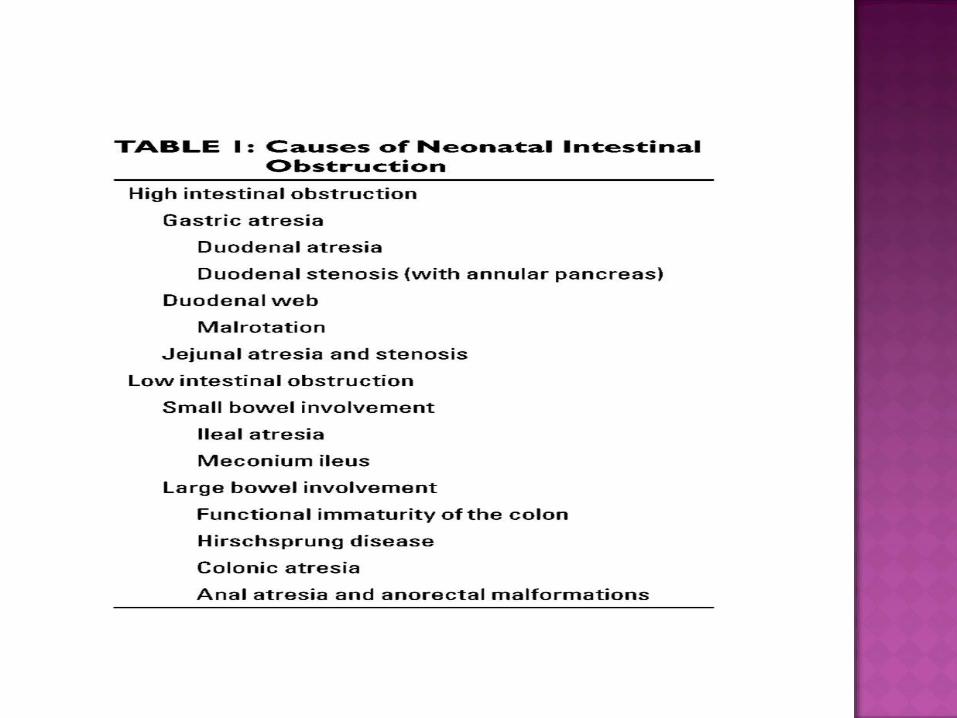
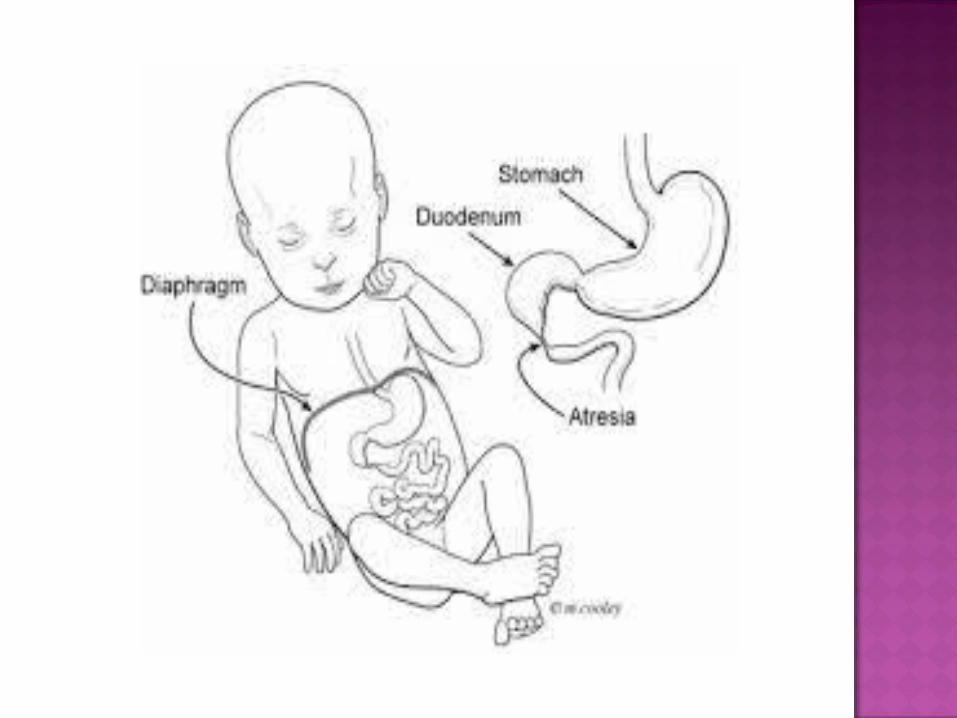
HIGH INTESTINAL OBSTRUCTION proximal to ileum i.e. gastric ,duodenal & jejunal.
LOW INTESTINAL OBSTRUCTION distal ileum & colon.
HIGH INTESTINAL OBSTRUCTION
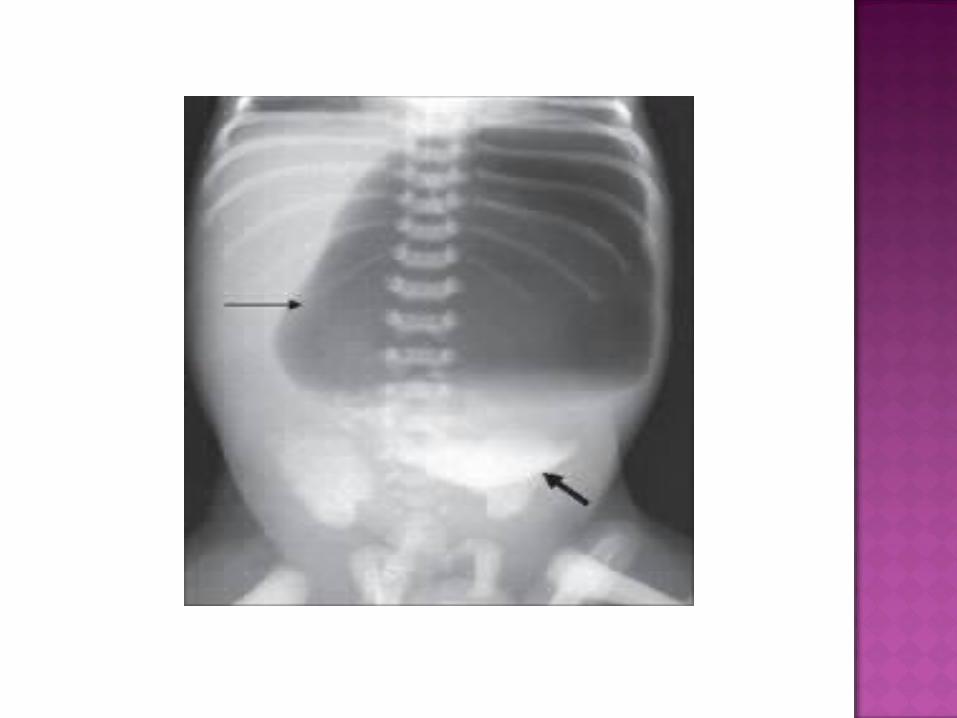
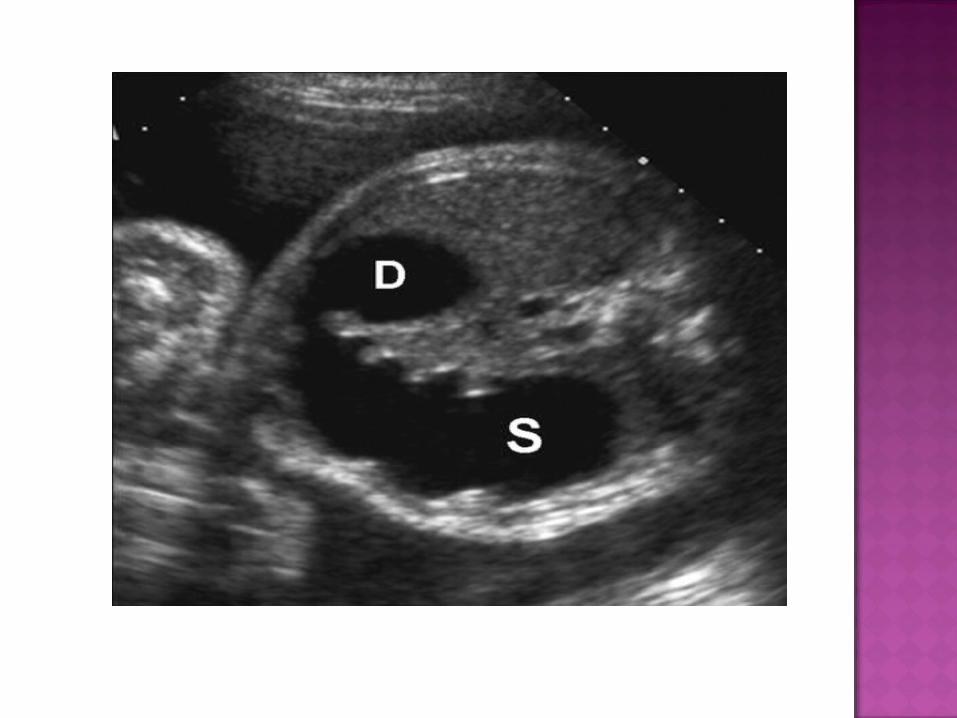
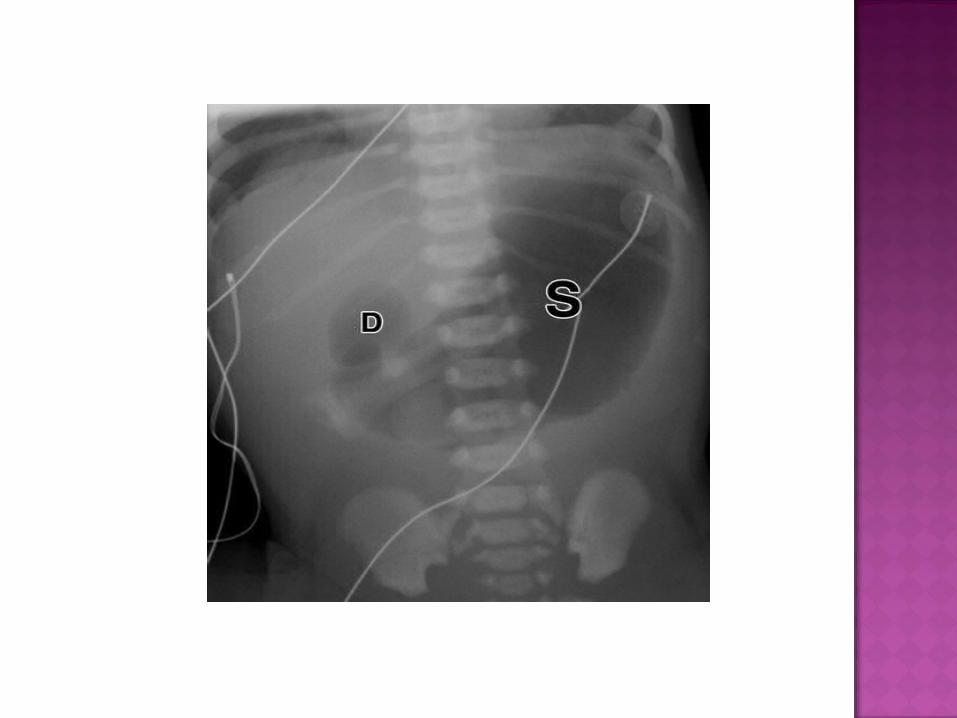
Rare Usually distal AXR—gas filled stomach without distal
intestinal air. SINGLE BUBBLE SIGN. Can be dx antenatally on ultrasound.


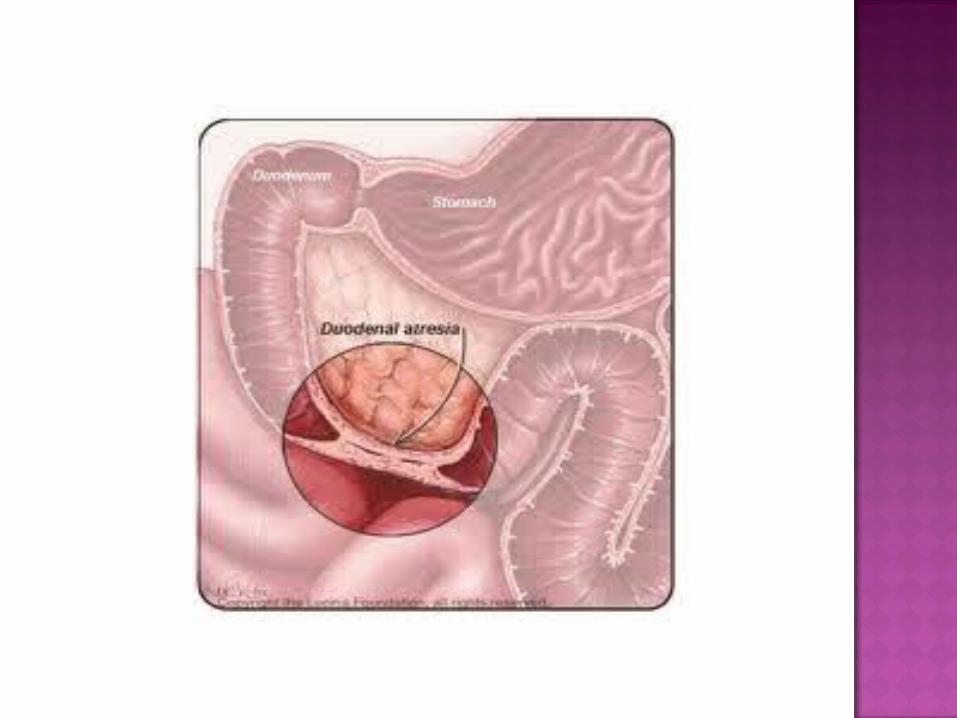
Congenital failure of recanalization. Association with VATER/VACTERL & trisomy
21. Post-ampullary. Bilous vomitting.
On AXR gas filled distended stomach & duodenal cap.
Absent distal bowel gases,

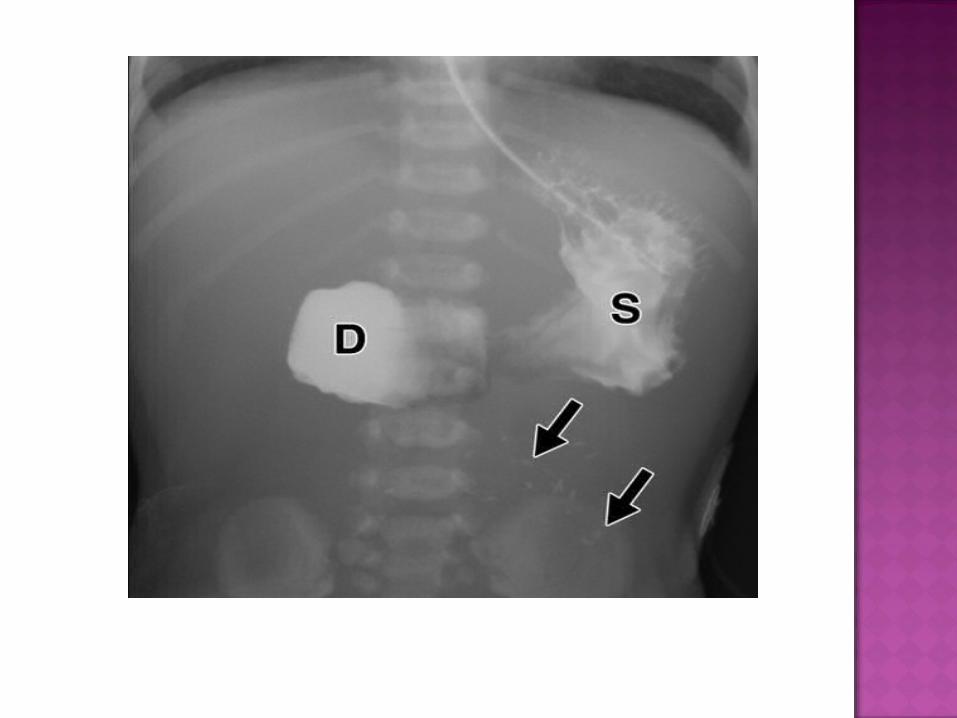
Gastro duodenal distention but distal gases present.
On contrast– slow transit of contrast distally.
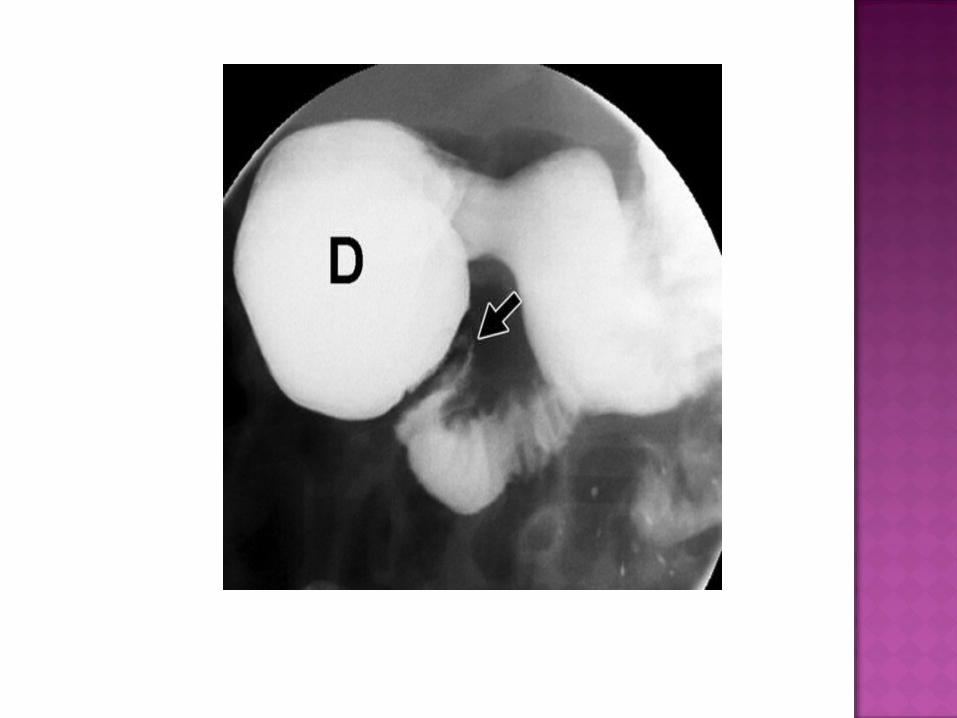
Small congenital obstructive membrane with central aperture.
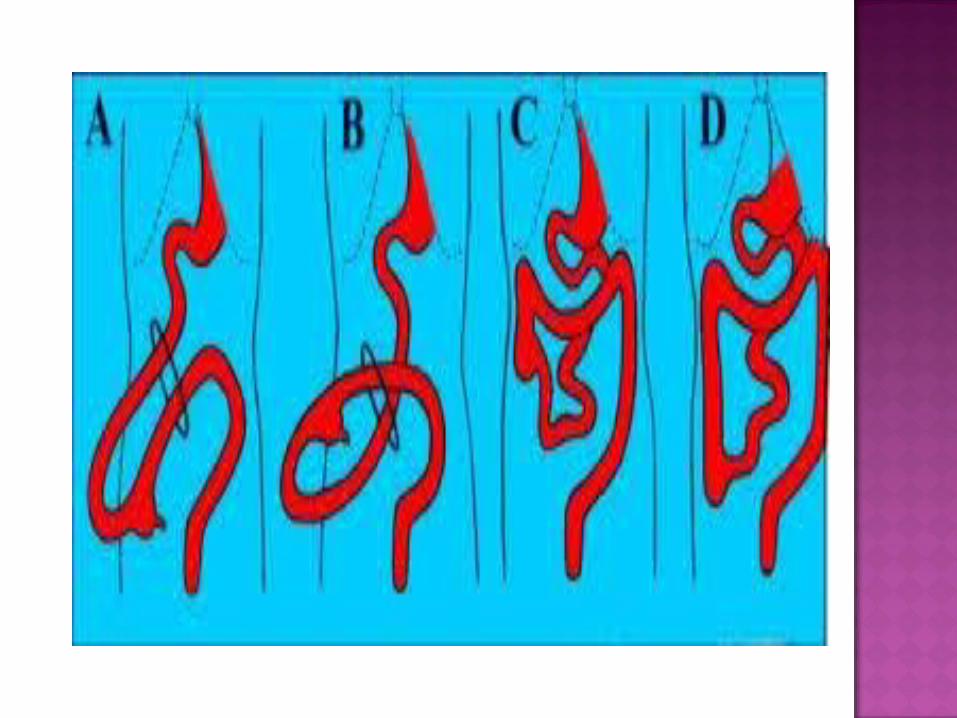
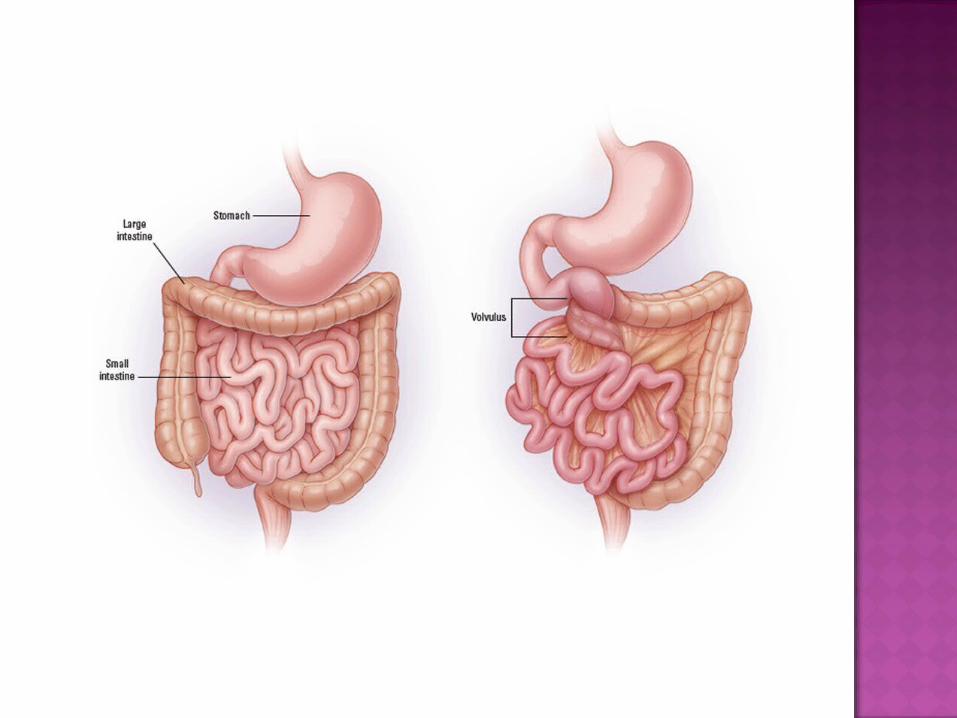
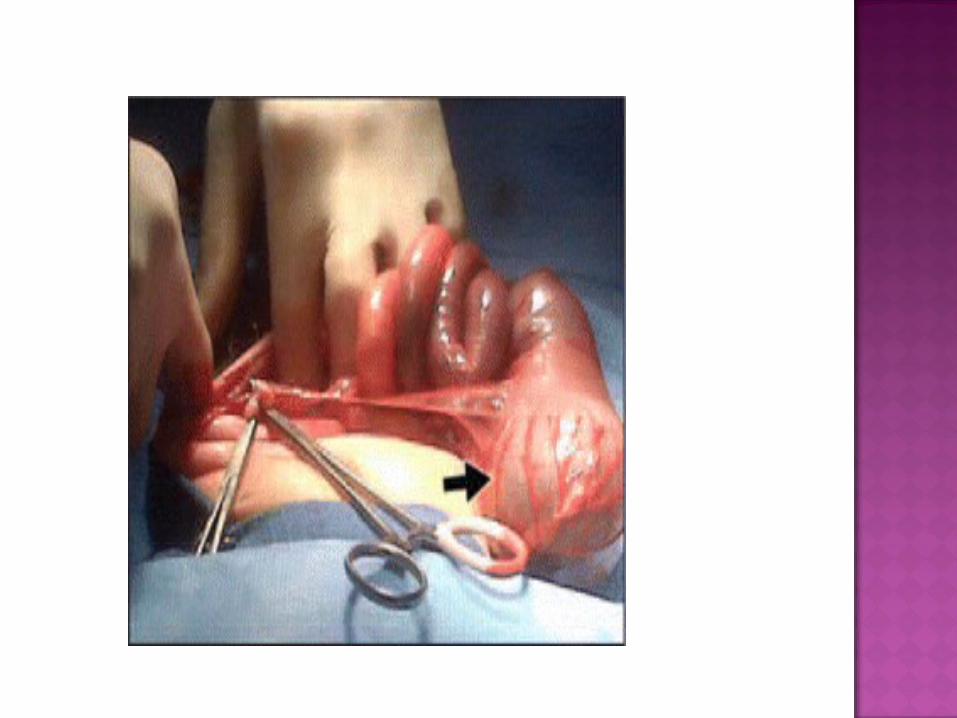
Failure of normal physloiogical herniation in embryo
Leads to narrow mesenteric attachment. Predisposes to rotation around superior
mesenteric vessels. If untreated bowel ischemia & infarction.
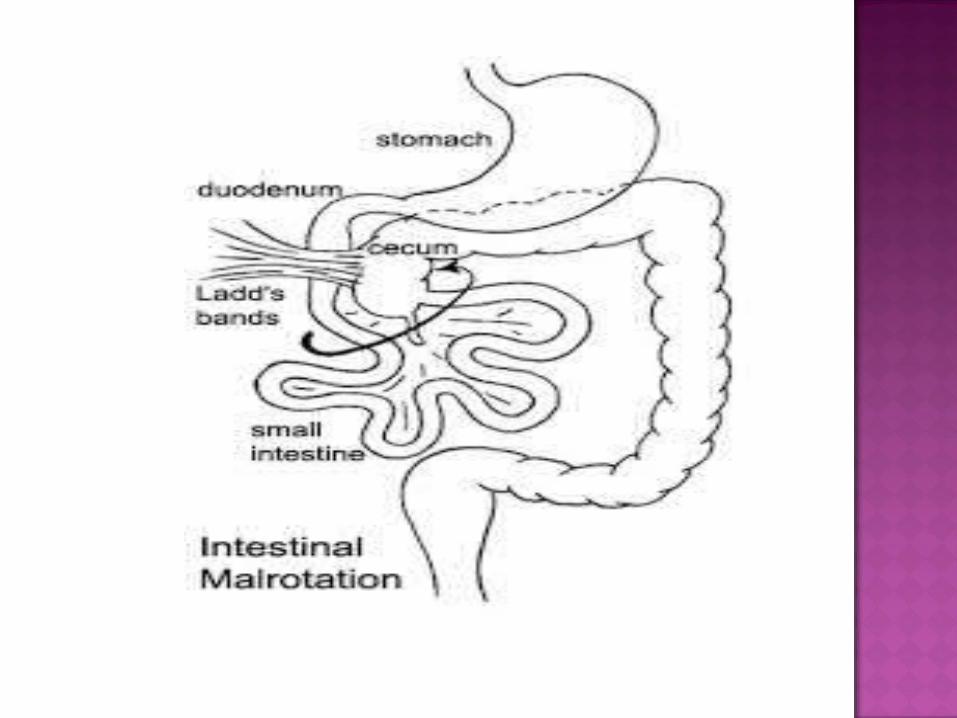
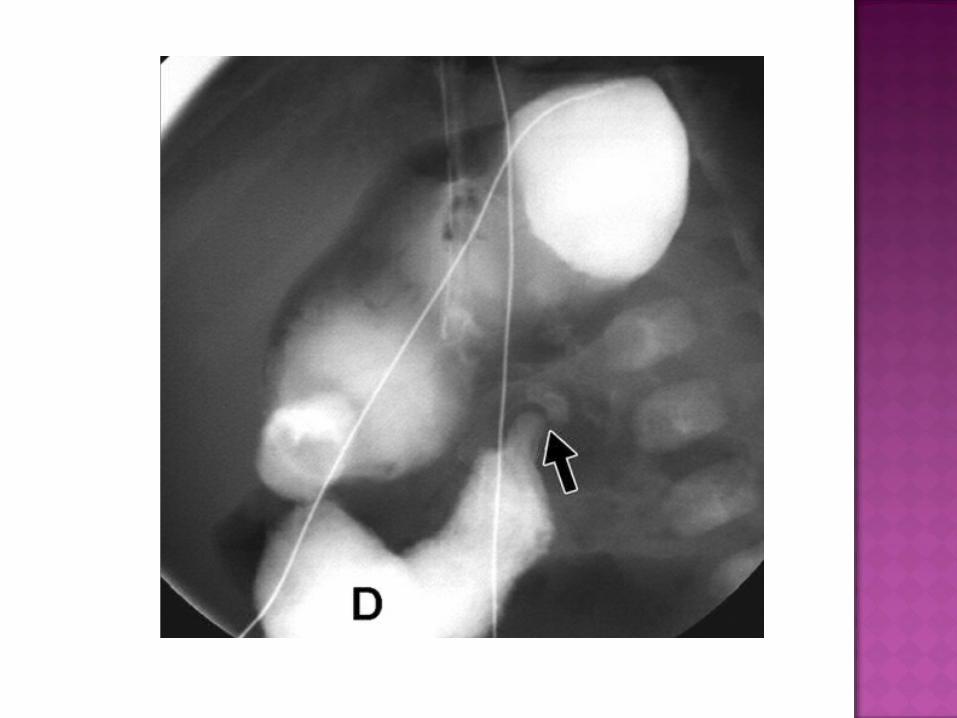
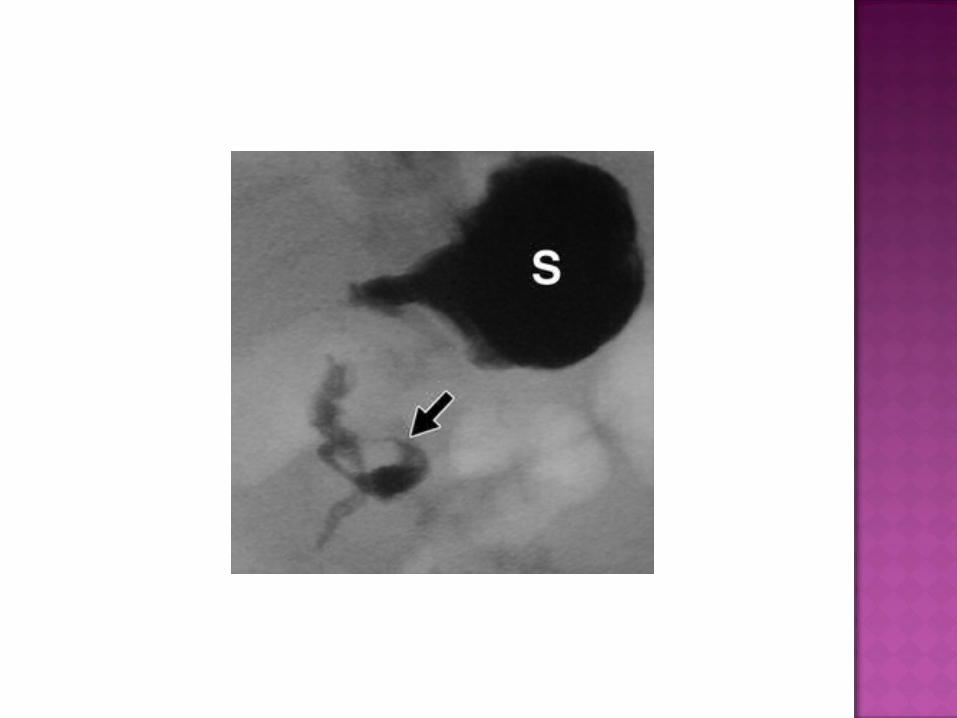
Abnormal course of duodenum that fail to cross midline has spiral appearance .


Intestinal ischemia during intra uterine life. Present with bilous vomitting & abdominal
distention.
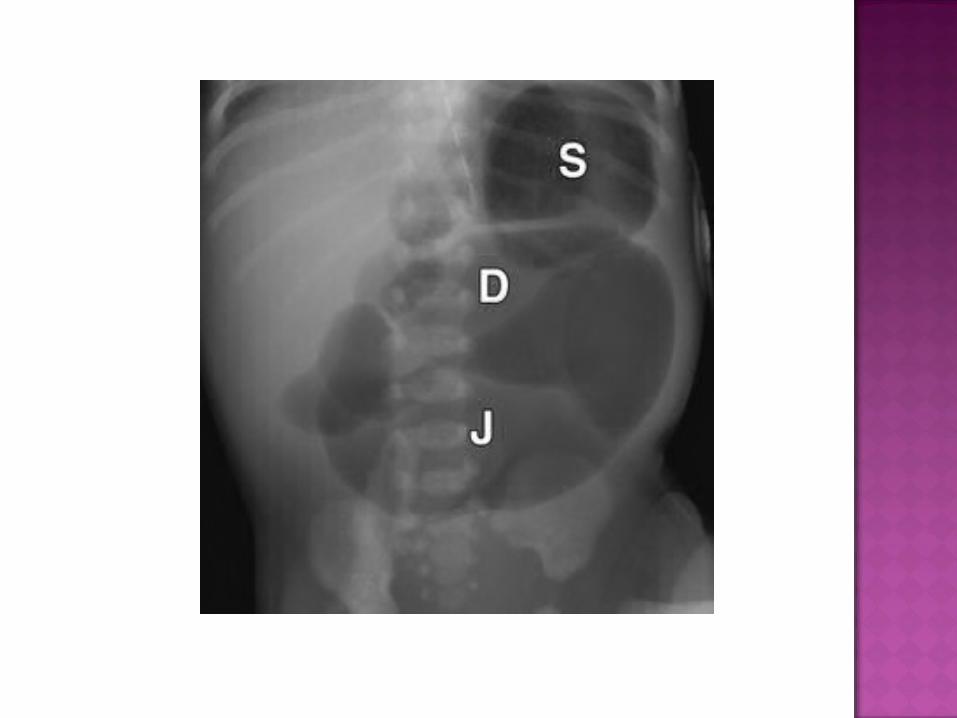
Distention of stomach ,duodenum & jejunum.

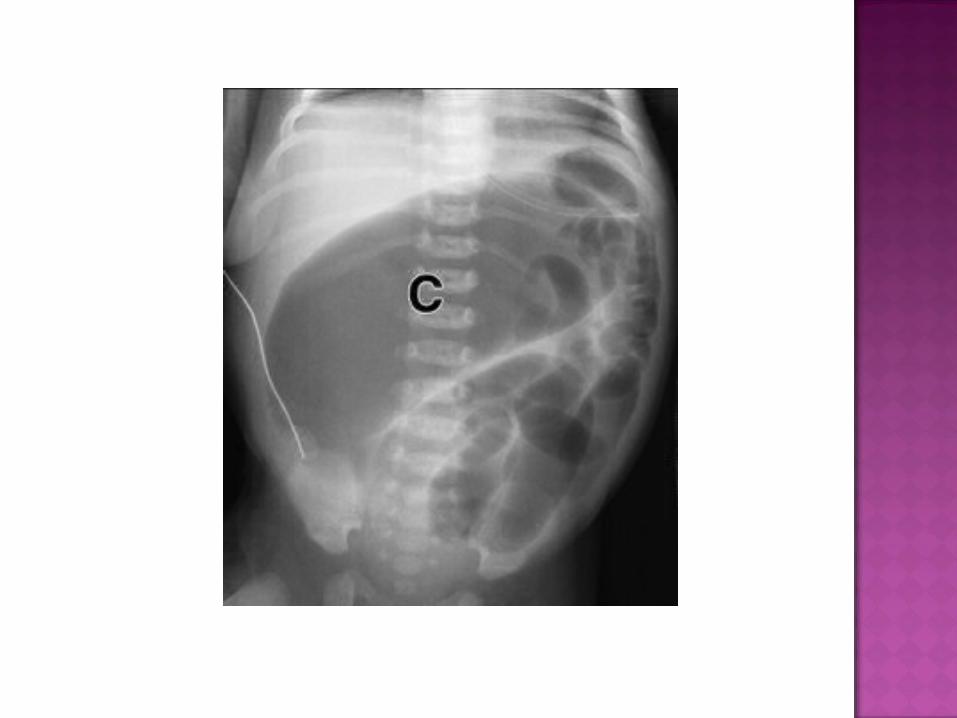
LOW INTESTINAL OBSTRUCTION
Due to intra uterine ischemic insult. Bilous vomiting & distention. Numerous dilated bowel loops.
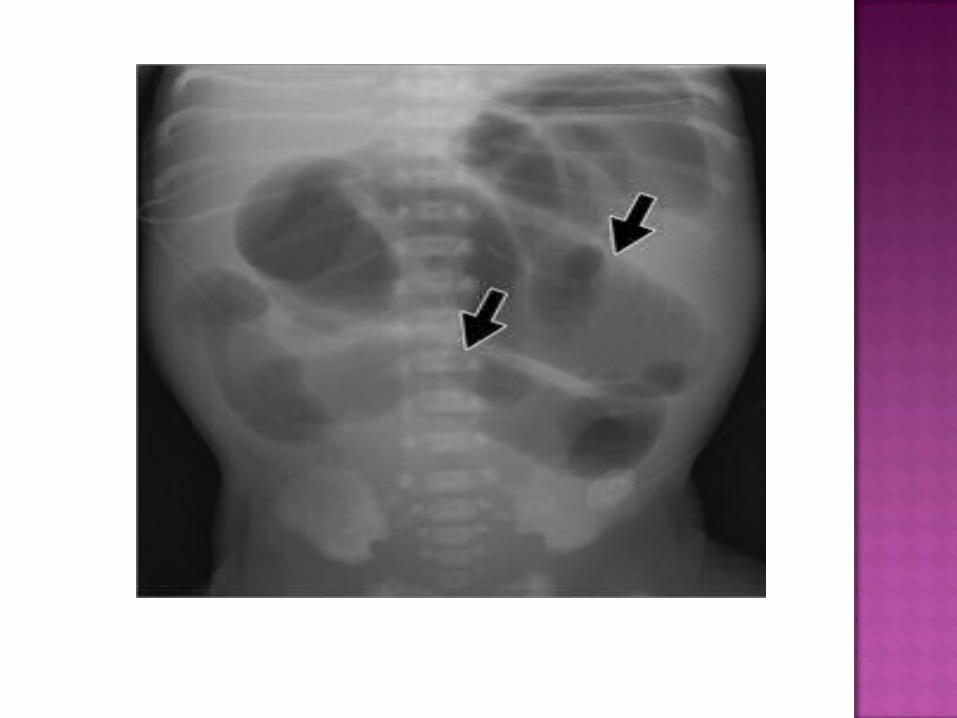

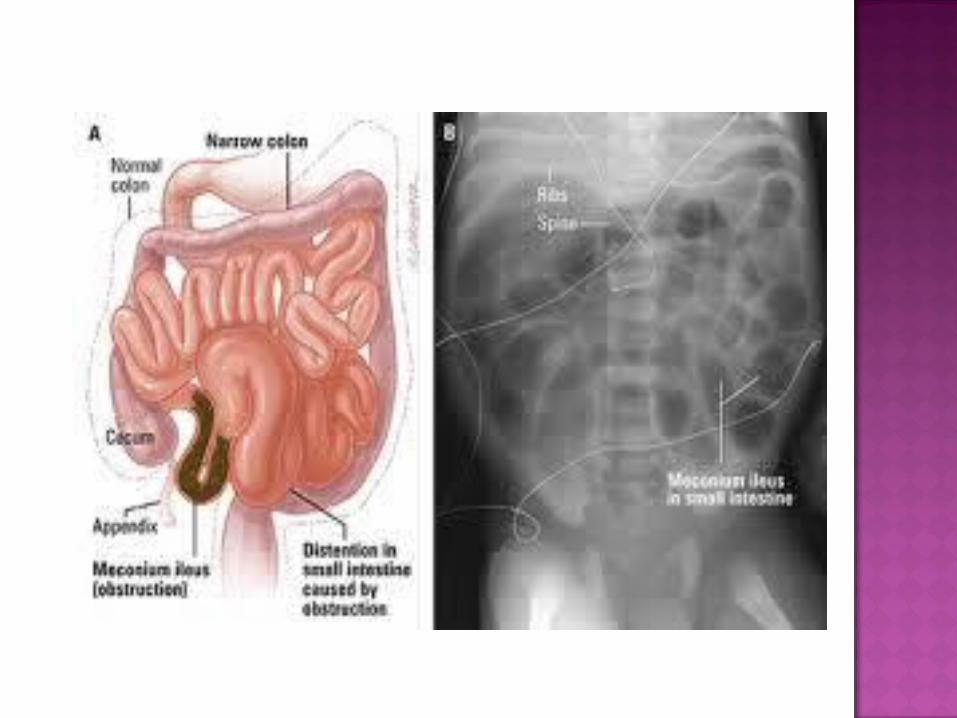
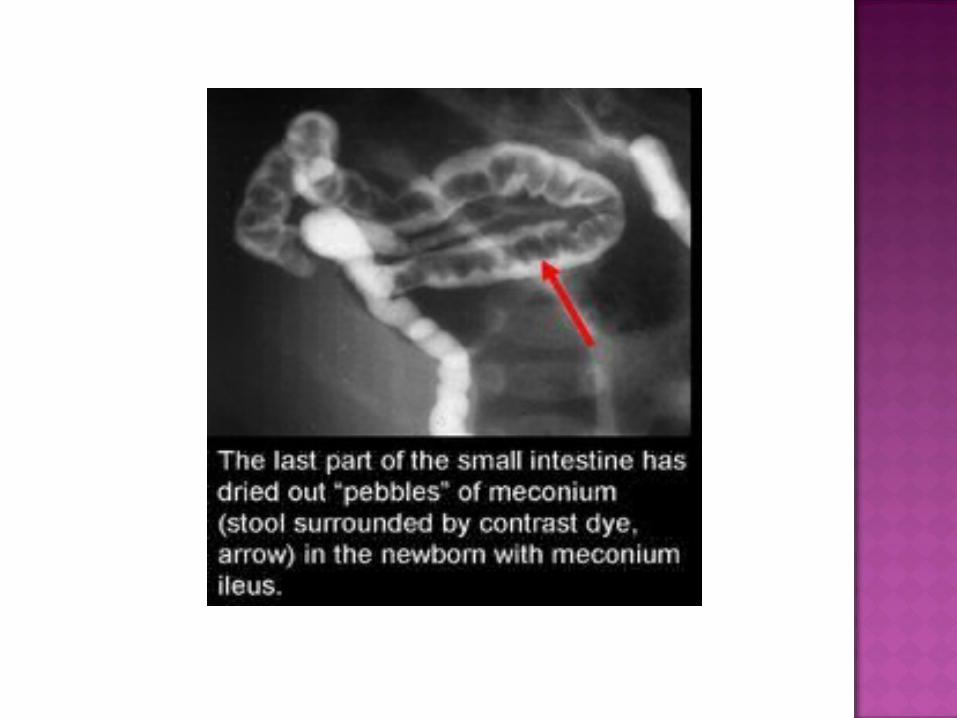
Meconium plugs obstruct colon & distal small bowel.
Associated with cystic fibrosis. AXR– multiple distended gut loops. Contrast study—meconium plugs & micro
colon.

Meconium plug /small left colon syndrome. Benign & self limiting condition. Due to immaturity of colonic ganglion cells. To infants of diabetic mothers & those who
took MgSO4 for pre eclampsia.
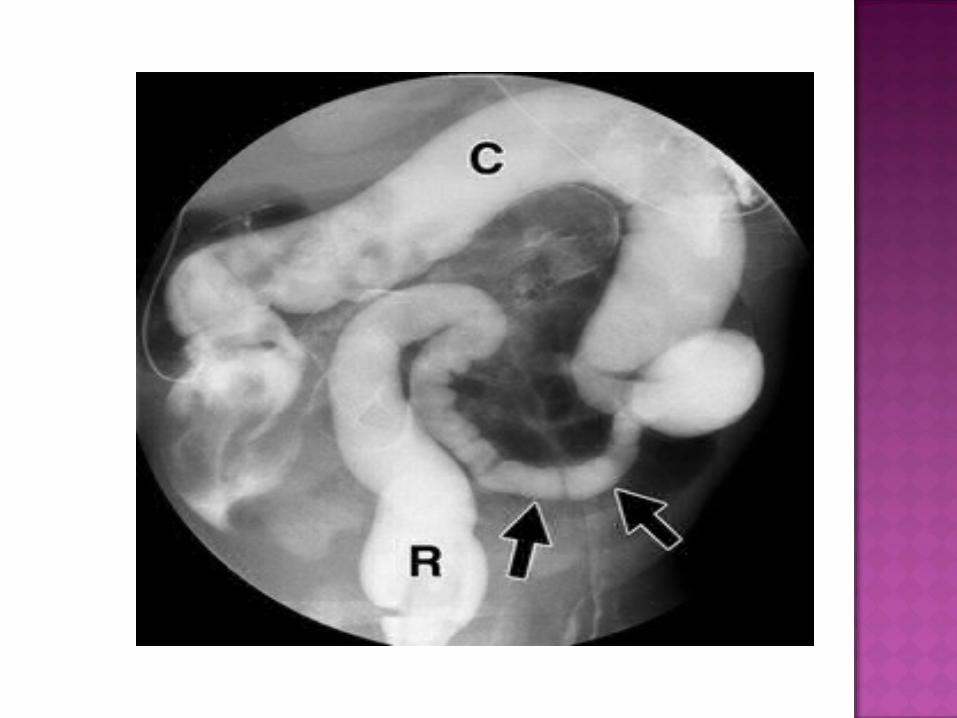
Contrast studies- dilated ascending & transverse colon small descending colon rectum normal
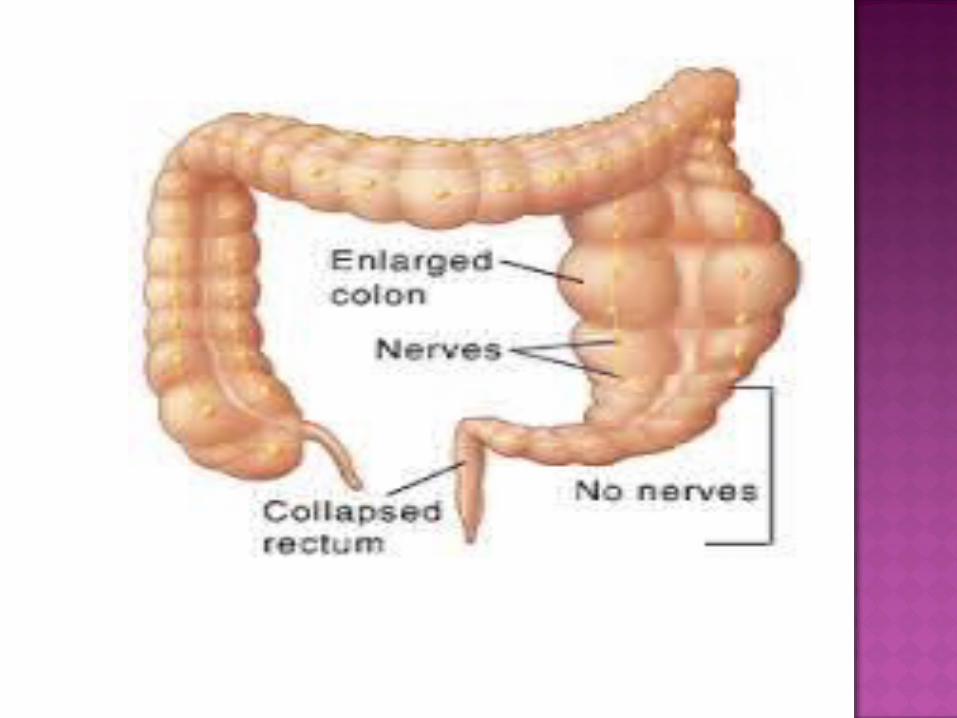
Arrest of neuron migration to distal bowel before 12th week.
rectosigmoid-75% splenic flexure-20% whole colon-5%

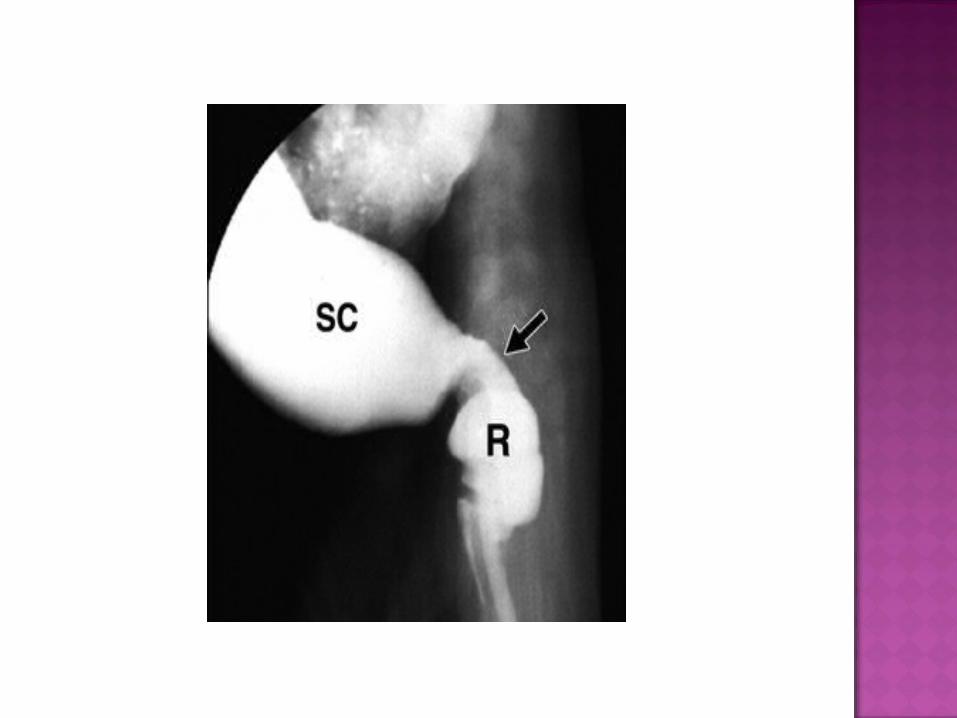
Affected segment narrowed. Proximal dilatation.

Rarely an uncommon condition Intra uterine vascular insult Proximal to splenic flexure
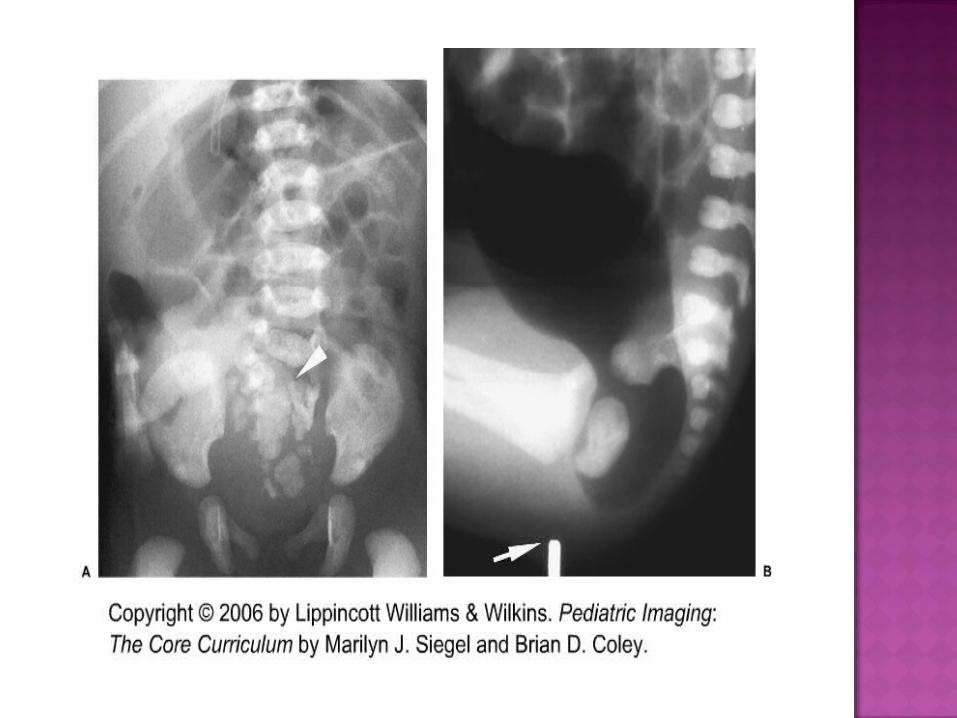
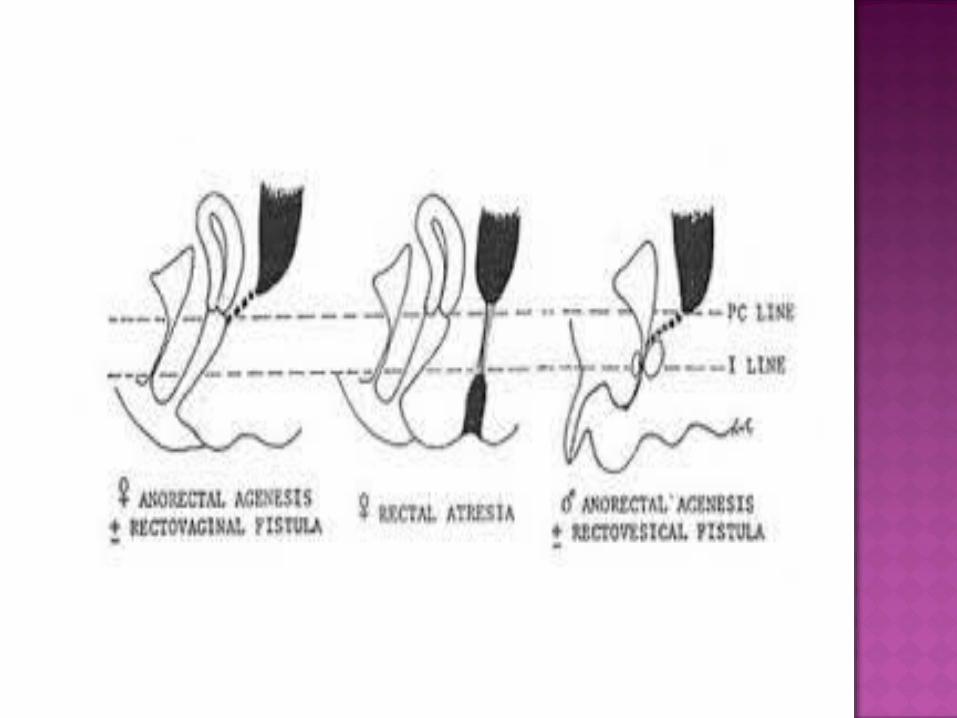
Association with VATER High/low depending levator ani muscle Low –blind ending pouch. High-associated with fistula to
bladder,urethra & vagina.

![An Unusual Cause of Neonatal Intestinal Obstruction: Left ... · cases of intestinal obstruction secondary to left paraduodenal hernia LPDH [4]. The average age at diagnosis is 38.5years](https://static.fdocuments.in/doc/165x107/5fd13dfe0abb383e45350238/an-unusual-cause-of-neonatal-intestinal-obstruction-left-cases-of-intestinal.jpg)