Neonatal Infecciology Group B Streptococcus · 2016-11-16 · GBS - overview I ! Streptococcus...
32
+ Neonatal Infecciology Group B Streptococcus - New Recommendations- Liliana Pinheiro March 2012
Transcript of Neonatal Infecciology Group B Streptococcus · 2016-11-16 · GBS - overview I ! Streptococcus...
+
Neonatal Infecciology
Group B Streptococcus - New Recommendations-
Liliana Pinheiro
March 2012
+GBS - overview I
n Streptococcus agalactiae • Group B Strep, Strep B, beta haemolytic Strep
n Causes serious disease in young infants, pregnant women and older adults.
n First recognized as a major perinatal pathogen in the 1970s1.
1Franciosi et al. Group B streptococcal neonatal and infant infections. J Pediatr 1973; 82:707-18.
+GBS - overview II
n Important cause of bacterial infection in newborns • Incidence of early-onset infection
² 0.28:1000 live births in US in 2008
² 0.5:1000 live births in Portuguese Pediatric Surveillance between April 2001 and March 2005 2
² 9:1000 live births in Braga`s region in 2005 3
• Mortality rate
² 1970`s as high as 50%; 4-6% in recent years in US 4
² 6,6% in Portuguese Pediatric Surveillance (2001-2005) 2
² Mortality higher in preterm and very low birthweight infants 2
2 Neto T et al. Arch Dis Child Fetal Neonatal Ed 2008;93:F90-F93; 3 Areal A et al. Infecção perinatal por SGB. Acta Pediatr Port 2010; 41(1):16-21; 4 Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC. 2010.

+GBS - infection
² Early-onset
• 0-6 days of life
• Up to 90% GBS infection apparent within 48 hours of birth
• Usually septicaemia with pneumonia
² Late-onset
• 6 days – 3 months
• Usually septicaemia with meningitis
• Localized infections ++

+GBS - maternal colonization I
n Maternal colonization with GBS in the genitourinary and gastrointestinal tracts is the single most important risk factor for early-onset GBS infection.
n Normal flora in intestinal tract and vagina • Intermittent and asymptomatic carriage • 30% adults carry GBS in intestines • 15-40% of pregnant women are colonized
n 34,9% of pregnant women in Braga`s region in 2005 were colonized3
n 19,4% of pregnant women in Braga`s region in 2011 were colonized4
n Colonization early in pregnancy is not predictive of early-onset GBS disease (Regan JA et al 1996)
3Areal A et al. Infecção perinatal por SGB. Acta Pediatr Port 2010; 41(1):16-21. 4Fernandes et al. Tese Mestrado, 2011.

+GBS – maternal colonization II
Mother colonized with GBS at delivery
(15-40% of women)
50% Baby colonized with GBS
50% Newborn baby not colonized
0,6% Early-onset GBS infection
septicaemia, pneumonia and/or meningitis
99,4% Asymptomatic
4 Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC. 2010.

+GBS - additional risk factors for early onset GBS infection I n Obstetric risk factors
• Preterm delivery • Prolonged rupture of membranes (≥18h) • Infection of the placental tissues or amniotic fluid / fever during
labor
n Previous infant with GBS disease
n Low maternal levels of anti-GBS antibodies
n Demographic risk factors • African American
• Young maternal age
+GBS - additional risk factors for early onset GBS infection II n GBS in urine during pregnancy
• GBS found in urine of 2-7% of pregnant women • Marker of heavy vaginal-rectal colonization • Antibiotic treatment of GBS bacteriuria during pregnancy
does not eliminate GBS from the genitourinary and gastrointestinal tracts, and recolonization after a course of antibiotics is typical
n Women with symptomatic or asymptomatic GBS urinary tract infections detected during pregnancy should be treated according to current standards of care
+Options to reduce GBS infection in newborn babies n Waiting and treating babies
after delivery • Too late for some and
wont`prevent most GBS infection
n Cesarean delivery
n Oral antibiotics • Don`t eradicate colonization
or reduce infection • Likely to increase resistance • Exception in GBS culture
from urine
n Intramuscular antibiotics • Poorly designed studies
n Intravenous antibiotics in labour • Only effective method of
prevention available at present
• Largest study performed in Chicago (Boyer et al. N Eng J Med 1986; 314:1665)
• Penicillin G recommended • Effectiveness in
observational studies: 86-89%

+GBS - how best to identify women who should receive IAP?
n ACOG and CDC (1996) and AAP (1997) • Two approaches for
identifying women in need for IAP
n CDC (2002) • Universal culture-based
screening of all pregnant women at 35-37 weeks to optimize the identification of women who should receive IAP
n Nacional guidelines (2004)
n Culture versus risk factor-based screening
• 50% of cases of early-onset GBS disease occur in infants of women who have no identifiable risk factors.
• 1:5 culture positive women did not have maternal risk factors.
• Risk factors can be used w h e n c u l t u r e s t a t u s unknown.
+GBS - testing for carriage
n Identification of women colonized with GBS plays the major role in the prevention of early-onset neonatal disease since GBS infection results from vertical transmission.
n Testing for carriage GBS mandatory by DGS since 2012 • 82% screening GBS in Braga`s region in 2005 3
• 88,8% screening GBS in Braga`s region in 2007 5
• 90% screening GBS in Braga`s region in 2011 (Fernandes et al. Tese Mestrado, 2011)
3 Areal A et al. Infecção perinatal por SGB. Acta Pediatr Port 2010; 41(1):16-21. 5 Pinheiro et al. Cuidados pré-concepcionais e vigilância pré-natal. Saúde Infantil 2009; 31 (2): 59-62.
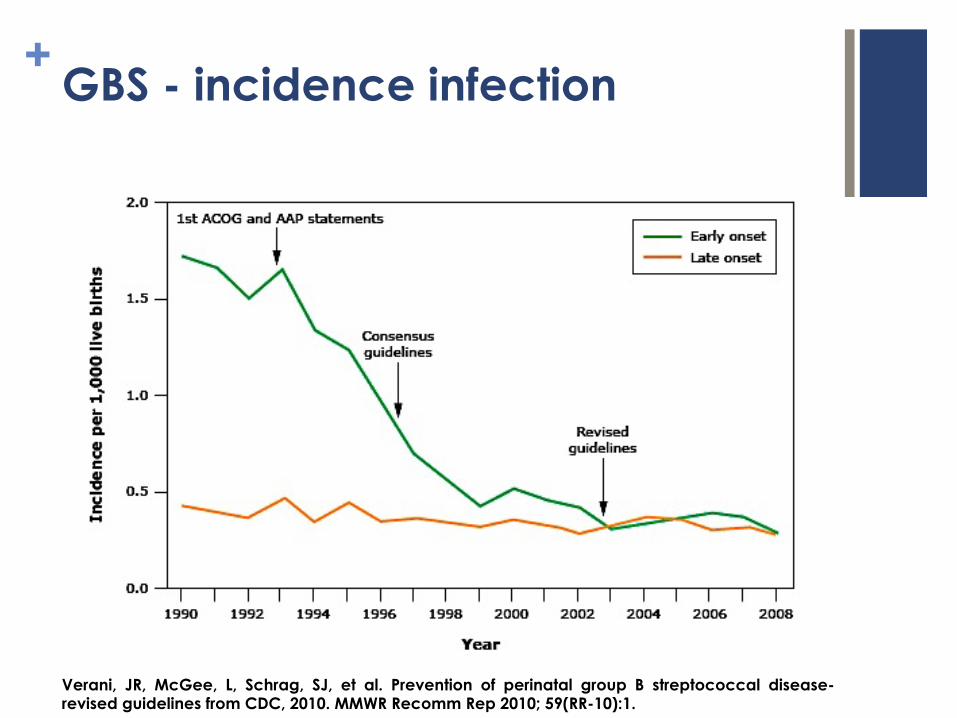
+GBS - incidence infection
Verani, JR, McGee, L, Schrag, SJ, et al. Prevention of perinatal group B streptococcal disease-revised guidelines from CDC, 2010. MMWR Recomm Rep 2010; 59(RR-10):1.
+ SGB – implementation challenges
n Missed prevention opportunities among infants born preterm • 50% screened prior to admission
• Only 18% of GBS unknown screened on admission
• Preterm 20% less likely to receive IAP when indicated than term
n Penicillin-allergic women • Only 14% at low risk for anaphylaxis
received cefazolin
• 70% at low risk for anaphylaxis received clindamycin even though
² <5% had susceptibility testing
Van Dyke et al., N Engl J Med. 2009 Jun 18;360(25):2626-36

+GBS - prophylaxis
n Remains uniformly sensitive to penicillin, ampicillin and cefazolin.
n Adequate IAP
• ≥4 hours of IV penicillin, ampicillin or cefazolin.
• A l l o t h e r a g e n t s o r durations are considered inadequate.
n Erythromycin is no longer recommended
• Increasing GBS resistant (>40%)
n Clindamycin
• GBS resistant (20%) - use depends on results of susceptibility tests
n Neither clindamycin nor v a n c o m y c i n a c h i e v e bactericidal concentrations in amniotic fluid

+GBS – antibiotic resistance I
Source: Active Bacterial Core surveillance / Emerging Infections Program

+GBS – management infant
n Evaluation and empirical antibiotic therapy • Newborn`s appearance
• Risk factor for GBS infection
• Adequacy of maternal IAP
n Clinical signs are more sensitive than hematologic test in predicting neonatal sepsis, particularly if the neonate is well-appearing
n PCR and procalcitonin have less sensitive for early-sepsis

+
Recommendations for Prevention early-onset GBS infection in newborn babies
March 2012

+GBS - key changes in 2010`s guidelines
1. Expanded recommendations on laboratory methods for identification GBS.
2. Clarification of the colony-count threshold required for reporting GBS detected in the urine of pregnant women.
3. Uptodate algorithms for GBS screening and IAP for women with preterm labour or preterm premature rupture of membranes.
4. Uptodate prophylaxis regimens for women with penicillin allergy.
5. Revised algorithm for management of newborns with respect to risk of early-onset GBS disease.
+GBS Recommendation - I
n GBS rectovaginal screening cultures for all pregnant women at 35 to 37 weeks of gestation, with the following two exceptions: • Women with GBS bacteriuria (≥104 colonies in pure culture or
mixed with a second microorganism during current pregnancy).
• Women who previously gave birth to an infant with invasive GBS disease.
n Susceptibility testing is indicated on prenatal GBS isolates from penicil l in-allergic women at high risk for anaphylaxis.

+GBS Recommendation - I
n Negative predictive value of GBS cultures performed ≤5 weeks before delivery is 95-98%.
n High vaginal swabs less efective than low vaginal plus anorectal swabs.
n Standard culture method instead of using enriched culture medium reduces detection by 50%.
n Screening GBS carriage between 35 and 37 weeks.
n Must take low vaginal and anorectal swabs.
n M u s t u s e s e l e c t i v e enr ichment medium to culture swabs.
Evidence Recommendations

+GBS Recommendation - II
• Positive screening culture for GBS from either vagina or rectum unless planned cesarean delivery in the absence of labor
• Positive history of birth of an infant with early-onset GBS disease.
• GBS bacteriuria during current pregnancy
• Unknown culture status and ü Intrapartum fever (≥38ºC) or ü Preterm labor or ü Prolonged rupture membranes (≥18
hours) or ü Intrapartum NAAT positive for GBS
• Posit ive GBS culture or GBS b a c t e r i u r i a i n a p r e v i o u s pregnancy
• Positive GBS culture and planned c e s a r e a n d e l i v e r y a t a n y gestacional age
• GBS culture negative even when one or more intrapartum risk factors
Indications for antibiotic prophylaxis
Antibiotic prophylaxis NOT recommended

+GBS Recommendation - III
No penicillin allergy
Penicillin G 5mU IV initially and then 2,5mU at 4-hourly intervals until delivery.
Ampicillin 2gr IV initially and
then 1gr at 4-hourly intervals until delivery.
Low risk anaphylaxis
Cefazolin 2gr IV and then
1gr at 8-hourly
intervals until delivery.
High risk anaphylaxis
Susceptibility clindamycin erythromycin
Clindamycin 900mg IV at
8-hourly intervals until
delivery.
High risk anaphylaxis
Resistant clindamycin erythromycin
Vancomycin 1gr IV at 12-
hourly intervals until
delivery.

+GBS Recommendation - III
4 Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC. 2010.

+GBS Recommendation - IV
n Separate algorithms are presented for GBS prophylaxis in the setting of threatened preterm delivery, one for spontaneous preterm labor (PTL) and one for preterm premature rupture of membranes (pPROM)
n Women with PTL or pPROM should all receive: • Screening on admission for GBS if GBS status unknown
• Antibiotics for GBS prophylaxis
n Antibiotics to prolong latency in pPROM can serve as GBS IAP if certain criteria are met • Ampicillin 2 g IV followed by 1 g IV every 6 hours for 48 hours
• Delivery occurs while the mother is receiving that antibiotic regime

+GBS Re
co
mm
end
atio
n - IV
4 Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC. 2010.

+GBS Re
co
mm
end
atio
n - IV
4 Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC. 2010.

+GBS Recommendation - V
n Management of infant – overview
• CBC with differential and platelet count at 6 to 12 hours of life
ü Well-appearing infants whose mothers had indications for IAP but did not received or received inadequate IAP and gestacional age <37 weeks or membranes were ruptured for ≥ 18 hours.
• Observation ≥48 hours
ü Well-appearing infants whose mothers had indications for IAP but did not received or received inadequate IAP and gestacional age ≥37 weeks or membranes were ruptured for < 18 hours.

+GBS Re
co
mm
end
atio
n - IV
4 Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC. 2010.

Maternal chorioamnionitis?
GBS prophylaxis not indicated for mothers
Mother received intravenous penicillin, ampicillin or cefazolin for ≥4 hours before delivery?
≥37 weeks or duration of membrane rupture < 18 hours?
<37 weeks or duration of membrane rupture ≥ 18 hours?
Signs of neonatal sepsis? Full diagnostic evaluation Antibiotic therapy
Limited evaluation Antibiotic therapy
Routine clinical care
Observation ≥48 hours
Observation ≥48 hours
Limited evaluation Observation ≥48 hours
Verani, JR, McGee, L, Schrag, SJ, et al. Prevention of perinatal group B streptococcal disease-revised guidelines from CDC, 2010. MMWR Recomm Rep 2010; 59(RR-10):1.
+GBS – The future
n Rapid Near Patient Testing • Better than testing at 35-37 weeks in informing which women are carrying
GBS in labour
• Unfortunately, no tests currently both fast and accurate enough
• More costly than enriched culture medium testing
n Vaccine • Best approach for preventing both EOGBS and LOGBS infection, plus
maternal GBS infection and other adult GBS infection
• Target would be pregnant women or women before they become pregnant
• Research is urgently needed into developing a viable vaccine for group B Strep infection
+GBS – References
n Centers of Disease Control and Prevention. Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC.MMWR Reports and Recommendations Vol. 51. 16 August 2002.
n Centers of Disease Control and Prevention. Prevention of Perinatal Group B Streptococcal Disease: Revised Guidelines from CDC.MMWR Reports and Recommendations Vol. 59. November 2010.
n Royal College of Obstetricians and Gynaecologists Clinical Green Top Guideline. Prevention of Early Onset Neonatal Group B Streptococcal Disease (36) – Nov 2003
n Yancey et al. The accuracy of late antenatal screening cultures in predicting genital GBS colonization at delivery. Obstet Gynecol Nov 1996; 88(5):811-5.
n Franciosi et al. Group B streptococcal neonatal and infant infections. J Pediatr 1973; 82:707-18.
n Neto T et al. Arch Dis Child Fetal Neonatal Ed 2008;93:F90-F93.
n Areal A et al. Infecção perinatal por SGB. Acta Pediatr Port 2010; 41(1):16-21.

+
Obrigada!