Neonatal Diabetes: A Case Series - Indian Pediatrics · indian pediatrics 33 volume 54__january 15,...
4
INDIAN PEDIATRICS 33 VOLUME 54 __ JANUARY 15, 2017 Neonatal Diabetes: A Case Series RAMASWAMY GANESH, NATARAJAN SURESH, THIRUVENGADAM VASANTHI AND *KG RAVIKUMAR From Departments of Pediatrics and *Endocrinology, Kanchi Kamakoti CHILDS Trust Hospital and The CHILDS Trust Medical Research Foundation, Chennai, Tamil Nadu, India. M onogenic diabetes results from the inheritance of a mutation or mutations in a single gene [1], and accounts for 1-5% of all childhood diabetes [2]. Neonatal diabetes mellitus (NDM) and maturity-onset diabetes of the young (MODY) are the two main forms of monogenic diabetes. NDM first occurs in newborns and young infants; MODY usually first occurs in children or adolescents but may be mild and not detected until adulthood. Most patients with monogenic diabetes are incorrectly diagnosed as either type 1 or type 2 diabetes. Identifying this entity correctly not only helps to initiate appropriate treatment but also helps us to explain the other associated clinical features and offer genetic counseling to the family for subsequent pregnancies [3]. An earlier study from Chennai [4] had reported 28 children with neonatal diabetes (0.05%) and 12 children with diabetes onset between 6 months to 1 year of age out of 506 diabetic children registered in their institute. The common gene mutations reported in their series were ABCC8 followed with EIF2AK3 and KCNJ11. We describe the clinical features and follow-up of children with neonatal diabetes from an urban children’s hospital in Chennai, India. METHODS A retrospective analysis of case records of children admitted with neonatal diabetes mellitus in the Department of Pediatrics and Endocrinology of Kanchi Kamakoti CHILDS Trust hospital, Chennai from January 2004 to December 2014 were analyzed. The study was approved by the institutional review board. A diagnosis of neonatal diabetes mellitus was established in infants who had their onset of diabetes within the first 6 months of life and presented with features of polyuria, polydipsia, weight loss, DKA and had their fasting blood sugar >126 mg/dL with HbA1C >6.5%. The case records of infants with neonatal diabetes mellitus were analyzed for birth weight, the age at onset of symptoms, the clinical features, laboratory investigations (FBS, HbA1C values), Genetic mutation testing results, treatment and follow-up details. We collected 3 mL of whole blood in EDTA tube from the proband and their parents, and sent it to Royal Devon and Exeter NHS Foundation Trust laboratory, Exeter, UK for genetic analysis. Molecular genetic testing included gene sequencing by PCR technique. All infants were treated with subcutaneous insulin at 05 -0.8 U/kg/day and were followed up. RESULTS During the study period, a total of 137 children were diagnosed as Type 1 diabetes mellitus as per WHO diagnostic criteria and 10 (5 boys) were diagnosed as neonatal diabetes mellitus. The age range at onset was from 3 days to 160 days. Six children were born to parents with consanguineous marriage and none had history of diabetes in their first degree relatives. All were born at term and six were born with a birth weight <2.5 kg. Diabetic ketoacidosis was the mode of presentation in 3 (30%) children (INS,EIF2AK3 and NEUROD1 gene). Glutamic Correspondence to: Dr Ramaswamy Ganesh, Consultant Pediatrician, Kanchi Kamakoti CHILDS Trust Hospital, Chennai 600 034, India. [email protected] Received: October 26, 2015; Initial review: January 11, 2016; Accepted: September 02, 2016. Background: Neonatal diabetes mellitusis a rare disorder with an incidence of 1 in 2,60,000 live births. Methods: Retrospective analysis of clinical and genetic profile of children admitted with neonatal diabetes mellitus in a tertiary-care hospital in Chennai, India over 11 years. Results: Ten children were diagnosed with neonatal diabetes of whom 9 had permanent neonatal diabetes mellitus. The age range at onset was from 3 days- 5 months. Of the 9 children, KCNJ11 gene mutation was positive in one, and ABCC 8 and INS gene mutation in two children each. Children with KCNJ11 and ABCC 8 gene mutations were switched over to oral sulfonyl urea therapy. Conclusion: Few genotypes causing NDM can be managed effectively with oral sulfonyl ureas. Keywords: Diabetes mellitus, Genetics, Permanent, Transient. Published online: November 05, 2016. PII:S097475591600020 RESEARCH P H P H P H P H PAPER Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Transcript of Neonatal Diabetes: A Case Series - Indian Pediatrics · indian pediatrics 33 volume 54__january 15,...

INDIAN PEDIATRICS 33 VOLUME 54__JANUARY 15, 2017
Neonatal Diabetes: A Case SeriesRAMASWAMY GANESH, NATARAJAN SURESH, THIRUVENGADAM VASANTHI AND *KG RAVIKUMARFrom Departments of Pediatrics and *Endocrinology, Kanchi Kamakoti CHILDS Trust Hospital and The CHILDS Trust MedicalResearch Foundation, Chennai, Tamil Nadu, India.
Monogenic diabetes results from theinheritance of a mutation or mutations in asingle gene [1], and accounts for 1-5% ofall childhood diabetes [2]. Neonatal
diabetes mellitus (NDM) and maturity-onset diabetes ofthe young (MODY) are the two main forms of monogenicdiabetes. NDM first occurs in newborns and younginfants; MODY usually first occurs in children oradolescents but may be mild and not detected untiladulthood. Most patients with monogenic diabetes areincorrectly diagnosed as either type 1 or type 2 diabetes.Identifying this entity correctly not only helps to initiateappropriate treatment but also helps us to explain theother associated clinical features and offer geneticcounseling to the family for subsequent pregnancies [3].An earlier study from Chennai [4] had reported 28children with neonatal diabetes (0.05%) and 12 childrenwith diabetes onset between 6 months to 1 year of age outof 506 diabetic children registered in their institute. Thecommon gene mutations reported in their series wereABCC8 followed with EIF2AK3 and KCNJ11. Wedescribe the clinical features and follow-up of childrenwith neonatal diabetes from an urban children’s hospitalin Chennai, India.
METHODS
A retrospective analysis of case records of childrenadmitted with neonatal diabetes mellitus in theDepartment of Pediatrics and Endocrinology of KanchiKamakoti CHILDS Trust hospital, Chennai from January
2004 to December 2014 were analyzed. The study wasapproved by the institutional review board. A diagnosis ofneonatal diabetes mellitus was established in infants whohad their onset of diabetes within the first 6 months of lifeand presented with features of polyuria, polydipsia,weight loss, DKA and had their fasting blood sugar >126mg/dL with HbA1C >6.5%. The case records of infantswith neonatal diabetes mellitus were analyzed for birthweight, the age at onset of symptoms, the clinicalfeatures, laboratory investigations (FBS, HbA1C values),Genetic mutation testing results, treatment and follow-updetails. We collected 3 mL of whole blood in EDTA tubefrom the proband and their parents, and sent it to RoyalDevon and Exeter NHS Foundation Trust laboratory,Exeter, UK for genetic analysis. Molecular genetictesting included gene sequencing by PCR technique. Allinfants were treated with subcutaneous insulin at 05 -0.8U/kg/day and were followed up.
RESULTS
During the study period, a total of 137 children werediagnosed as Type 1 diabetes mellitus as per WHOdiagnostic criteria and 10 (5 boys) were diagnosed asneonatal diabetes mellitus. The age range at onset wasfrom 3 days to 160 days. Six children were born to parentswith consanguineous marriage and none had history ofdiabetes in their first degree relatives. All were born at termand six were born with a birth weight <2.5 kg. Diabeticketoacidosis was the mode of presentation in 3 (30%)children (INS,EIF2AK3 and NEUROD1 gene). Glutamic
Correspondence to:Dr Ramaswamy Ganesh,Consultant Pediatrician,Kanchi Kamakoti CHILDS TrustHospital, Chennai 600 034, [email protected]: October 26, 2015;Initial review: January 11, 2016;Accepted: September 02, 2016.
Background: Neonatal diabetes mellitusis a rare disorder with an incidence of 1 in 2,60,000live births. Methods: Retrospective analysis of clinical and genetic profile of childrenadmitted with neonatal diabetes mellitus in a tertiary-care hospital in Chennai, India over 11years. Results: Ten children were diagnosed with neonatal diabetes of whom 9 hadpermanent neonatal diabetes mellitus. The age range at onset was from 3 days- 5 months.Of the 9 children, KCNJ11 gene mutation was positive in one, and ABCC 8 and INS genemutation in two children each. Children with KCNJ11 and ABCC 8 gene mutations wereswitched over to oral sulfonyl urea therapy. Conclusion: Few genotypes causing NDM canbe managed effectively with oral sulfonyl ureas.
Keywords: Diabetes mellitus, Genetics, Permanent, Transient.
Published online: November 05, 2016. PII:S097475591600020
RRRRR EEEEE SSSSS EEEEE AAAAA RRRRR CCCCC H PH PH PH PH P AAAAA PPPPP EEEEE RRRRR
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites

INDIAN PEDIATRICS 34 VOLUME 54__JANUARY 15, 2017
GANESH, et al. NEONATAL DIABETES
TABL
E 1
CLIN
ICA
L AN
D G
ENET
IC P
RO
FILE
OF C
HIL
DR
EN W
ITH
NEO
NAT
AL D
IAB
ETES
MEL
LITU
S
Case
Age
atSe
xC
linic
al fe
atur
esCo
nsan
-Bi
rth-
Gen
etic
ana
lysi
sD
iagn
osis
Trea
tmen
tFo
llow
-up
No
diag
nosi
sgu
inity
wei
ght
13
dF
Hyp
ergl
ycem
ia, M
acro
glos
sia,
No
2 kg
Com
plet
e lo
ss o
f met
hyla
tion
atTN
DM
Insu
lin ×
5 m
o,16
mo
of a
ge,
umbl
ical
hern
iath
e TN
D d
iffer
entia
lly m
ethy
late
dth
en o
ffins
ulin
off i
nsul
in,
regi
on o
n ch
rom
osom
e 6q
24.
doin
g w
ell
260
dM
Poly
uria
, poo
r wei
ghtg
ain
No
2.4
kgH
eter
ozyg
ous m
isse
nse
mut
atio
nPN
DM
Insu
lin In
itial
ly,
5 y,
On
(R20
1C) i
n th
e K
CN
J11g
ene.
Glib
encl
amid
eG
liben
clam
ide,
(0.5
mg/
kg)
doin
g w
ell
316
0 d
MPo
lyur
ia, s
eizu
res
No
2.5
kgN
ovel
het
eroz
ygou
s fra
me-
PND
MIn
sulin
Initi
ally
,3
y, O
nde
letio
nc.3
808_
3813
delA
ACTC
CG
liben
clam
ide
Glib
encl
amid
e,in
exo
n 31
of t
he A
BCC
8 ge
ne.
(0.5
mg/
kg)
doi
ng w
ell
414
dF
Poly
uria
, sei
zure
s2
degr
ee3.
6 kg
Hom
ozyg
ous s
plic
ing
mut
atio
n,PN
DM
Insu
lin In
itial
ly,
3 y,
on
IVS1
6+1G
>A, i
n in
tron
16 o
f the
Glib
encl
amid
eG
liben
clam
ide,
ABC
C8
gene
; Fat
her a
nd m
othe
r car
riers
.(0
.5m
g/kg
)doi
ngw
ell
545
dM
Poly
uria
, poo
r wei
ghtg
ain
2 de
gree
2.4k
gH
eter
ozyg
ous m
isse
nse m
utat
ion,
PND
MIn
sulin
3 y,
On
insu
lin,
Y10
8D, i
nexo
n 3
of th
e IN
Sgen
e.do
ing
wel
l6
90 d
FPo
lyur
ia, F
TT, D
KA
No
2.3
kgH
omoz
ygou
s nov
el m
utat
ion.
PND
MIn
sulin
5 y,
On
insu
lin,
c-21
8A>C
/c.-2
18A
>C, i
n th
e pr
omot
erdo
ing
wel
lof
the
INS
gen
e; M
othe
r car
rier.
720
dF
Poor
feed
ing,
leth
argy
, fev
er3
degr
ee1.
7 kg
Hom
ozyg
ous f
or a
nov
el m
isse
nse
PND
MIn
sulin
8 y,
on
insu
lin,
mut
atio
n, R
176
Q in
exo
n 2
of th
edo
ing
wel
lPD
X1 (I
PF1)
gen
e.8
150
dM
DK
A (5
Mon
ths)
,2
degr
ee3
kgH
omoz
ygou
s for
a n
ovel
PND
M-
Insu
lin,
Die
d at
4 y
rsH
epat
itis (
1,2
y), s
hort
mis
sens
e m
utat
ion,
R58
7Q, i
nW
olco
ttliv
erof
age
due
tost
atur
e (2
y)
exon
10
of th
e EI
F2AK
3 ge
ne;
Ral
lison
supp
ortiv
eM
OD
SFa
ther
and
mot
her c
arrie
rs.
synd
rom
e9
137
dF
Poly
uria
, FTT
, Ane
mia
3 de
gree
2.8
kgH
eter
ozyg
ous n
ovel
mis
sens
ePN
DM
-In
sulin
,10
ys,
on(8
mo)
, Ret
initi
spig
men
tosa
mut
atio
n, G
105
E in
exo
n 2
ofTR
MA
Thia
min
ein
sulin
+thi
amin
e,(7
mo)
, coc
hlea
r im
plan
t (2
y)th
e SL
C19
A2 g
ene.
Doi
ng w
ell
1060
dM
DK
A, R
ight
foca
l sei
zure
,2
degr
ee2.
4 kg
Hom
ozyg
ous f
or a
fram
ePN
DM
Insu
lin20
mo
onin
ferio
r cer
ebel
lar v
erm
issh
ift m
utat
ion
c.23
5_23
6 in
sT,
insu
lin, h
ashy
popl
asia
in th
e N
EURO
D1g
ene.
Fat
her a
ndm
ild m
otor
mot
her c
arrie
rs.
deve
lopm
enta
lde
lay
F- F
emal
e; M
-Mal
e; F
TT- F
ailu
re to
thri
ve; D
KA-
Dia
betic
ket
oaci
dosi
s; T
ND
M-T
rans
ient
neo
nata
l Dia
bete
s m
ellit
us; P
ND
M-p
erm
anen
t Neo
nata
l Dia
bete
s m
ellit
us.
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites

INDIAN PEDIATRICS 35 VOLUME 54__JANUARY 15, 2017
GANESH, et al. NEONATAL DIABETES
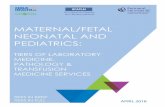
acid decarboxylase and islet cell autoantibodies werenegative in all children. The mean blood sugar was 499mg/dL. Of the 10 children, one child had transient neonataldiabetes mellitus and nine had permanent neonataldiabetes mellitus. The child with transient neonataldiabetes presented with hyperglycemia on D3 of life,required insulin for 5 months, and mutation analysisrevealed complete loss of methylation on chromosome 6q24. She is off insulin and at her 16 month follow-up, she isgrowing well. Of the nine children with permanentneonatal diabetes mellitus, KCNJ11 gene mutation waspositive in 1, ABCC 8 gene and INS gene mutation in 2each, PDX1 gene mutation in 1, NEURO D1 mutation in 1,EIF2AK3 mutation in 1 and SLC19A2 gene mutation in 1child. Children with KCNJ11 gene mutation and ABCC 8gene mutation were treated with oral sulfonyl urea andothers were treated with Insulin. On follow up, the childwith Wolcott Rallison Syndrome died and other patientsare growing well without problems. The details are shownin Table I.
DISCUSSION
Nine children were diagnosed with permanent NDM inthe present series. Heterozygous activating mutations inthe KCNJ11 gene, that encodes the KATP channel subunitKir6.2, accounts for 47% of permanent NDM [5,6] and afew cases of treatment NDM [7,8]. Similarly mutations inABCC8 gene which encodes the SUR1 regulatory subunit
of the ATP-sensitive potassium channels in beta cells cancause both permanent and transient neonatal diabetes. Inclinical practice it is difficult to differentiate betweenpatients with KCN J11or ABCC8 mutations and oralsulfonyl urea becomes the treatment of choice fordiabetes resulting from both these mutations [9,10]. Ourpatients were switched on treatment from insulin to oralglibenclamide (0.5 mg/kg/day) once the geneticdiagnosis was established, and on follow up theirglycemic control was good.
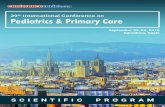
The present study describes the clinical and geneticprofile of children with neonatal diabetes mellitus. As themolecular genetic testing is expensive, we suggest analgorithm to approach a child with neonatal diabetes forordering genetic testing in resource limited setting likeours (Fig. 1). Molecular genetic testing has a big impacton management of NDM as switching over to oralsulfonyl urea is required in children with KCNJ11/ABCC8 gene mutation. Complete history, thorough clinicalexamination with a high suspicion and correlation withphysical findings may help us to guide further thegenotype work up of neonatal diabetes mellitus.Acknowledgements: Prof Sian Ellard, Consultant MolecularGeneticist, Peninsula Medical School (Royal Devon and ExeterNHS Foundation Trust, Exeter) and Professor Karen Temple,Wessex Regional Genetics laboratory, University ofSouthampton School of Medicine for carrying out the moleculargenetic work-up.
Neonatal diabetes mellitus
Associated clinical featuresNo associated clinical features
↓↓ ↓
Do KCNJ11 /ABCC 8 mutation
Negative- but Transient NDM
↓
↓
↓ZAC/HYMA1 gene mutation
Positive
Spontaneous resolutionby 12 weeks; close follow
up of these patients
↓
↓
Relapse; Treat accordingly↓
Negative but Permanent NDM↓
Positive; treat with sulfonylurea ↓
USG abdomen to look at pancreas
Normal Abnormal
INS gene mutation PDX/IPF, PTF1A,GATA6 mutations
Wolcott Rallison syndrome (EIF2AK3 gene)Thiamine responsive megaloblastic anemia (SLC19A2 gene)
Wolfram syndrome (WFS1 gene)
↓
↓↓ ↓
↓ ↓
FIG. 1 Proposed algorithm for ordering genetic mutation testing in patients with neonatal diabetes (NDM).
↓
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites

INDIAN PEDIATRICS 36 VOLUME 54__JANUARY 15, 2017
GANESH, et al. NEONATAL DIABETES
Contributors: RG, NS, TV: reviewed literature, draftedmanuscript and were involved in patient management; KGR:reviewed manuscript for intellectual content and will act as theguarantor.Funding: None; Competing interests: None stated.
REFERENCES
1. Hattersley A, Bruining J, Shield J, Njolstad P, DonaghueKC. The diagnosis and management of monogenic diabetesin children and adolescents. Pediatric Diabetes.2009;10:33-42.
2. National diabetes information clearing house. MonogenicForms of Diabetes: Neonatal Diabetes Mellitus andMaturity-onset Diabetes of the Young. Available from:www.diabetes.niddk.nih.gov. Accessed February 24, 2012.
3. Slingerland AS. Monogenic diabetes in children and youngadults: Challenges for researcher, clinician and patient. RevEndocr Metab Disord. 2006;7:171-85.
4. Varadarajan P, Sangaralingam T, Senniappan S, Jahnavi S,Radha V, Mohan V. Clinical profile and outcome ofinfantile onset diabetes mellitus in southern India. IndianPediatr. 2013;50:759-63.
5. Gloyn AL, Pearson ER, Antcliff JF, Proks P, Bruining GJ,
WHAT THIS STUDY ADDS?
• The present study reports the molecular genetics of nine children with permanent neonatal diabetes mellitus.
Slingerland AS, et al. Activating mutations in the geneencoding the ATP-sensitive potassium channel subunitKir6.2 and permanent neonatal diabetes. N Engl J Med.2004;350:1838-49.
6. Hattersley AT, Ashcroft FM. Activating mutations inKir6.2 and neonatal diabetes: new clinical syndromes, newscientific insights, and new therapy. Diabetes. 2005;54:2503-13.
7. Gloyn AL, Reimann F, Girard C, Edghill EL, Proks P,Pearson ER, et al. Relapsing diabetes can result frommoderately activating mutations in KCNJ11. Hum MolGenet. 2005;14:925-34.
8. Colombo C, Delvecchio M, Zecchino C, Faienza MF,Cavallo L, Barbetti F. Transient neonatal diabetes mellitusis associated with a recurrent (R201H) KCNJ11 (KIR6.2)mutation. Diabetologia. 2005;48:2439-41.
9. Pearson ER, Flechtner I, Njolstad PR, Malecki MT,Flanagan SE, Larkin B, et al. Switching from insulin to oralsulfonylureas in patients with diabetes due to Kir6.2mutations. N Engl J Med. 2006;355:467-77.
10. Babenko AP, Polak M, Cave H, Busiah K, Czernichow P,Scharfmann R, et al. Activating mutations in the ABCC8gene in neonatal diabetes mellitus. N Engl J Med.2006;355:456-66.
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites
Copyright of Indian Pediatrics 2017 For personal use only. Not for bulk copying or unauthorized posting to listserv/websites