(Neo)Adjuvant Treatment of Melanomaimages.researchtopractice.com/.../Slides/Module8.pdf ·...
20
(Neo)Adjuvant Treatment of Melanoma Jeffrey S Weber, MD, PhD Deputy Director Laura and Isaac Perlmutter Cancer Center Professor of Medicine NYU Langone Medical Center New York, New York
Transcript of (Neo)Adjuvant Treatment of Melanomaimages.researchtopractice.com/.../Slides/Module8.pdf ·...

(Neo)Adjuvant Treatment of Melanoma
Jeffrey S Weber, MD, PhD Deputy Director
Laura and Isaac Perlmutter Cancer CenterProfessor of Medicine
NYU Langone Medical CenterNew York, New York

Disclosures: Possibly, Probably or Definitely Related
• I consult for and have received less than $10,000 dollars per annum from Merck, Genentech, Astra Zeneca, GSK, Novartis, Nektar, Medivation, Celldex, Incyte and EMD Serono and $10-25,000 dollars from BMS for membership on Advisory Boards
• I hold equity in CytoMx, Biond and Altor• I am on scientific advisory boards for Celldex, CytoMx, Incyte,
Biond, Protean, CV6 and Sellas• I am not a member of any speaker’s bureau• NYU, but not me personally received research support from
BMS, Merck, GSK, Novartis and Astra Zeneca• Moffitt Cancer Center filed a patent on an IPILIMUMAB
biomarker that I am named on, and I was named on a PD-1 biomarker patent by Biodesix

Adjuvant Ipilimumab in Stage III Melanoma
Eggermont et al. N Engl J Med. 2016;375:1845-1855.Pa
tient
s al
ive
(%)
YearYear
HR for recurrence or death= 0.76 (95% CI, 0.64–0.89)P<0.001
Ipilimumab
Ipilimumab
Placebo
Placebo
HR for death = 0.72(95% CI, 0.58–0.88)P=0.001
Recurrence-Free SurvivalNo. of
Events/Total No.
Median RFS(95% CI)
mos
5-Yr Rate(95% CI)
%
Ipilimumab 264/475 27.6 (19.3–37.2) 40.8 (36.0–45.6)
Placebo 323/476 17.1 (13.6–21.6) 30.3 (26.0–34.6)
Overall SurvivalNo. of
Events/Total No.
5-Yr Rate(95% CI)
%
Ipilimumab 162/475 65.4 (60.8–69.6)
Placebo 214/476 54.4 (49.7–58.9)
Patie
nts
aliv
e an
d w
ithou
t rec
urre
nce
(%)
No. at riskIPI
Placebo
100908070605040302010
00 1 2 3 4 5 6 7 8
476 261 199 154 133 65 17 0 0475
No. at riskIPI
Placebo
100908070605040302010
00 1 2 3 4 5 6 7 8
413 348 297 273 178 58 8 0431 369 325 290 199 62 4 0
476475283 217 184 161 77 13 1 0

CheckMate 238: Study Design
Primary endpoint: RFS
Patients with:• High-risk,
completely resected stage IIIB/IIIC or stage IVa melanoma
• No prior systemic therapy
• ECOG PS 0/1
Follow-up
Maximum treatment
duration of 1 year
NIVO 3 mg/kg IV Q2W and
IPI placebo IV Q3W for 4 doses,
then Q12W from week 24
IPI 10 mg/kg IV Q3W for 4 doses,
then Q12W from week 24 and
NIVO placebo IV Q2W
1:1
n = 453
n = 453
Stratified by: 1) Disease stage: IIIB/IIIC vs IV M1a or M1b vs IV M1c2) Tumor PD-L1 status at a 5% cutoff
NCT02388906.aPer American Joint Committee on Cancer (AJCC) Cancer Staging Manual, seventh edition.
Database lock: January 31, 2019; minimum follow-up of 36 months for all patients
Weber, J et al ESMO 2019

Primary Endpoint CheckMate 238: RFS in All PatientsNIVO (n = 453) IPI (n = 453)
Events, n 188 239Median, mo (95% CI) NR (38.7‒NR) 24.9 (16.6‒35.1)HR (95% CI)a 0.68 (0.56–0.82)Pb < 0.0001
aStratified; bLog-rank test. NR, not yet reached.
58%
70%62%
45%
61%51%R
FS (%
)
Months
0
10
20
30
40
50
60
70
80
90
100
0 6 12 18 24 273 9 15 21 30 45
NIVOIPI
No. at risk
36 3933 42
453 316 254 221 203 193365 272 235 209 185 170 122 37 12 0453 353 311 280 261 249394 331 290 270 243 234 178 50 13 0
NIVOIPI
Weber, J et al ESMO 2019

Exploratory Endpoint for CheckMate 238: DMFS in Stage III Disease
NIVO(n = 370) IPI (n = 366)
Events, n 126 144Median, mo (95% CI) NR NR (41.8‒NR)HR (95% CI)a 0.78 (0.62–0.99)Pb 0.044
aStratified; bLog-rank test.
66%
80%70%
58%
73%64%
DM
FS (%
)
Months
0
10
20
30
40
50
60
70
80
90
100
0 6 12 18 24 273 9 15 21 30 45
NIVOIPI
No. at risk
36 3933 42
366 287 244 220 200 195314 258 232 208 181 168 118 40 12 0370 312 284 253 231 221334 295 270 240 215 208 157 41 11 0
NIVOIPI
Weber, J et al ESMO 2019

KEYNOTE-54 (EORTC 1325): RFSITT Population
Eggermont AMM, et al. N Eng J Med. 2018;378:1789-1801.
RFS rates were longer for PEMBRO (71.4%) vs. PBO (53.2%) at 18 months, with distant metastasis incidence of 16.7% vs 29.7% respectively.
Total No. No. with Event
Hazard Ratio
(98,4% CI)
Pembro 514 135 0.57 (0.43-0.74)
Placebo 505 216 1.00
P<0.001 by stratified log-rank test
Overall Intention-to-Treat Population
Perc
ent o
f Pat
ient
s Aliv
e an
d Re
curr
ence
-free
Months
Pembrolizumab
Placebo
PembrolizumabPlacebo
No. at Risk
100
80
60
40
20
90
70
50
30
10
0 3 6 9 12 15 18 21 24
514 438 413 392 313 182 73 15 0505 415 363 323 264 157 60 15 0
0
KEYNOTE-054 (EORTC 1325): RFSITT Population
Total No. No. with Event
Hazard Ratio (98.4% CI)
Pembro 514 135 0.57(0.43-0.74)
Placebo 505 216 1.00

COMBI-AD: Study Design — AND Extended Follow-up Analysis in 2018
Long GV, et al. N Engl J Med. 2017;377:1813-1823 and Long, G et al ESMO 2018
BID, twice daily; DMFS, distant metastasis–free survival; D+T, dabrafenib + trametinib; ECOG, Eastern Cooperative Oncology Group; FFR, freedom from relapse; FU, follow-up; QD, once daily.
Key eligibility criteria• Completely resected stage IIIA (lymph node
metastasis > 1 mm), IIIB, or IIIC cutaneous melanoma
• BRAF V600E/K mutation• ECOG performance status 0 or 1• No prior radiotherapy or systemic therapy• Tissue collection was mandatory at baseline
and optional upon recurrence
RANDOMIZATION
Stratification•BRAF mutation status (V600E, V600K)
•Disease stage (IIIA, IIIB, IIIC)
1:1
•Primary endpoint: RFS•Secondary endpoints: OS, DMFS, FFR, safetyN = 870
Treatment duration: 12 months
Primary analysisD+T median FU,
33 months
Updated analysisD+T median FU,
44 months
PRESENTED BY GV LONG AT ESMO 2018
Dabrafenib 150 mg BID + trametinib 2 mg
QD(n = 438)
2 matched placebos (n = 432)

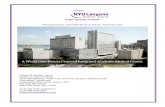
Adjuvant Dabrafenib + Trametinib:COMBI-AD: Relapse-Free survival
Dabrafenib + trametinibNo. at risk
Placebo
10090807060504030201000 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64
Months Since Randomization
Rel
apse
-Fre
e Su
rviv
al, %
438 405 381 354 324 281 262 249 236 227 183 148 92 47 13 2 0432 322 263 219 198 178 168 164 157 147 128 107 63 27 4 1 0
1-year, 88% (95% CI, 85%-91%)
1-year, 56% (95% CI, 51%-61%)
2-year, 67% (95% CI, 62%-72%) 3-year, 59%
(95% CI, 55%-64%)
3-year, 40% (95% CI, 35%-45%)
4-year, 54% (95% CI, 49%-59%)
4-year, 38% (95% CI, 34%-44%)
2-year, 44% (95% CI, 40%-49%)
HR 0.49 (95% CI, 0.40-0.59)
21% drop-off year 1>2
For stage IIIB/C only in COMBI-AD, RFS at 3 years was 54%; for the same population in CheckMate 238, it was 60%!
Long, G et al ESMO 2018

Long, G et al ESMO 2018

AE, adverse event; SAE, serious adverse event.a Most common AEs leading to treatment discontinuation in the dabrafenib plus trametinib arm were pyrexia (9%) and chills (4%).
COMBI-AD: Safety summary
AE Category, n (%)Dabrafenib Plus Trametinib
(n = 435)Placebo (n = 432)
Any AE 422 (97) 380 (88)
AEs related to study treatment 398 (91) 272 (63)
Any grade 3/4 AE 180 (41) 61 (14)
Any SAE 155 (36) 44 (10)
SAEs related to study treatment 117 (27) 17 (4)
Fatal AEs related to study drug 0 0
AEs leading to dose interruption 289 (66) 65 (15)
AEs leading to dose reduction 167 (38) 11 (3)
AEs leading to treatment discontinuationa
114 (26) 12 (3)

COMBI-AD: Common adverse eventsDabrafenib Plus Trametinib
(n = 435) Placebo (n = 432)AEs, n (%) All Grades Grade 3/4 All Grades Grade 3/4Any AE (> 20% with dabrafenib plus trametinib)a
422 (97) 180 (41) 380 (88) 61 (14)
Pyrexia 273 (63) 23 (5) 47 (11) 2 (< 1)Fatigue 204 (47) 19 (4) 122 (28) 1 (< 1)Nausea 172 (40) 4 (1) 88 (20) 0Headache 170 (39) 6 (1) 102 (24) 0Chills 161 (37) 6 (1) 19 (4) 0Diarrhoea 144 (33) 4 (1) 65 (15) 1 (< 1)Vomiting 122 (28) 4 (1) 43 (10) 0Arthralgia 120 (28) 4 (1) 61 (14) 0Rash 106 (24) 0 47 (11) 1 (< 1)
a Eleven patients (3%) in the treatment arm and 10 patients (2%) in the placebo arm had new primary melanomas; 8 (2%) and 7 (2%), respectively, had cutaneous squamous cell carcinoma/keratoacanthoma; 19 (4%) and 14 (3%), respectively, had basal cell carcinoma; and 10 (2%) and 4 (1%), respectively, had noncutaneous malignancies.

The IMMUNED Adjuvant Study: RFS
NIVO (n=59)NIVO+IPI
(n=56)Placebo (n=52)
Median RFS, mo (95% CI) 12.4 (5.30, 33.26) NR1 6.4(3.26, 9.61)
HR (95% CI) vs placebo 0.56 (0.36, 0.88) 0.23 (0.13, 0.41) -HR (95% CI) vs NIVO - 0.40 (0.22, 0.73) -
Data cut-off date July 2nd, 2019Median follow-up time: 28.4 months (n=167)
0 6 1 2 1 8 2 4 3 0 3 6 4 2 4 80
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
m o n th s
RF
S (
%)
Patients at risk:
Placebo 2652
3459NIVONIVO + IPI 4056
15
2934
11
2226
6
1921
6
1614
2
1110
-
31
52%
75%
32%
42%
70%
14%
61%
84%
53%
-
--
46%
70%
26%
1NR: not reached
Schadendorf, D et al ESMO 2019

CheckMate 915 Study Schema
NCT03068455.
N = 1950
RA
ND
OM
IZE
D
• Primary endpoint: RFS (up to 30 months). • Secondary endpoints: OS (up to 5 years), PD-L1 expression (approximately 3 years).
NIVO + IPI combination therapy
NIVO monotherapy
Randomized, phase 3 study of adjuvant NIVO ± IPI in resected high-risk stage III/IV melanoma
• ≥ 12 year old with melanoma• Stage IIIb/c/d or IV before
complete resection• Complete surgical resection• No prior medical therapy for
melanoma treatment
• No previous CTLA4 treatment
• No uveal melanoma
Trial dates: 4/2017 – 2/2020 (estimated)
1:1
11-20-19 Press Release: A statistically significant benefit was not reached for the co-primary endpoint of recurrence-free survival (RFS) in patients whose tumors expressed PD-L1 <1%. The Data Monitoring Committee recommended that the study continue unchanged. The study remains double-blinded and will continue to assess the other co-primary endpoint of RFS in the all-comers (intent-to-treat) population.

Conclusions• Adjuvant BRAF + MEK inhibition with dabrafenib and trametinib results in prolonged
RFS and OS with the longest follow-up of any adjuvant trial in resected stage III disease
• Adjuvant nivolumab has the best long term record for immunotherapy in patients with resected stage IIIB/IIIC/IV melanoma with improved RFS versus the active ipilimumab comparator
• Adjuvant IPI + NIVO ???? better than NIVO alone
• Neoadjuvant IPI + NIVO may define pCR patients requiring no further treatment
• New strategies require non-resistant mechanisms, new agents against specific resistance mechanisms to checkpoint inhibition

OpACIN-neo Study Schema
NCT02977052; Blank, C et al ESMO 2018 (#LBA39)
N = 110
NO
TR
AN
DO
MIZ
ED
• Primary endpoint: RFS (24 months), grade 3/4 immune-related adverse events (irAEs). • Secondary endpoints: RFS (3 years), late AEs, DMFS, OS.
Phase 2 study of neoadjuvant NIVO ± IPI in resectable stage III melanoma
• ≥ 18 year old with melanoma• Stage III before complete
resection• Complete surgical resection• No prior radiation therapy for
melanoma treatment
• No previous CTLA4 or PD-L1 treatment
• No distant metastases
Trial dates: 4/2017 – 2/2020 (estimated)
1:1:1
IPI 3 mg/kg + NIVO 1 mg/kgQ3 week x 2 courses –
prior to surgery at week 6
IPI 3 mg/kg followed by NIVO 3 mg/kg (> 2 hours and < 24 hours after IPI) Q3 week x 2 courses –
prior to surgery at week 6
IPI 1 mg/kg + NIVO 3 mg/kgQ3 week x 2 courses –
prior to surgery at week 6
irAEs = immune-related adverse events.

Neoadjuvant IPI+NIVO yields a high pCR rate and long-term RFS with tolerable toxicity
Rozeman L et al Lancet Oncology 2019
At 32 months of f-u, pRR is 47% arm A, 57% arm B, and 23% arm C. No pRRpts have relapsed vs relapse in 9 of 21 with no pathol. response;A 20% grade 3-4 irAE rate seen in arm B

Neoadjuvant IPI+NIVO yields a high pCR rate and long-term RFS with tolerable toxicity
Rozeman L et al Lancet Oncology 2019
At 32 months of f-u, pRR is 47% arm A, 57% arm B, and 23% arm C. No pRRpts have relapsed vs relapse in 9 of 21 with no pathol. response;A 20% grade 3-4 irAE rate seen in arm B

One dose of neoadjuvant PEMBRO, then adjuvant PEMBRO: association with relapse-free survival
“major” ORR was 27% or 8/27: 5 with pCR, 3 with >90% pPR, and
none have relapsed with 25 mos. of follow-up;1 year RFS was 63%
Huang, A et al Nat Med 2018

Alexander M Menzies, MIA ASCO 2019
Neoadjuvant Therapy: Relapse by Pathological Complete Response and Targeted Versus Immunotherapy
Menzies, A et al ESMO 2019
Immunotherapy Targeted Therapy
Med f/u 10 mo Med f/u 22 mo
100%
72%
pCR*
non-pCRpCR
non-pCR
* 1 pt died from toxicity without recurrence, censored at time of death
100%
72%
88%
43%
78%
8%