necrotizing fasciitis: the howard university hospital experience
5
NECROTIZING FASCIITIS: THE HOWARD UNIVERSITY HOSPITAL EXPERIENCE Mark Walker, MD, and Macy Hall, Jr, MD, FACS Washington, DC All surgical cases from 1965 to 1980 and au- topsy cases from 1974 to 1980 diagnosed at Howard University Hospital as necrotizing fasciitis (NF) were reviewed. Eight patient ful- filled the criteria for NF, which included (1) fascial necrosis, (2) spreading cellulitis with undermining of fascial planes, and (3) sys- temic toxicity as evidenced by altered mental state and hyperthermia. Bacteroides fragilis was commonly found in our most recent cases. Poor prognostic signs included (1) documented bacteremia, (2) preoperative hypotension (systolic blood pressure lower than 80 mmHg), and (3) hypocalcemia (serum calcium less than 7.0 mg/dL). Therapy con- sisted of wide debridement with systemic an- tibiotics and delayed skin grafting when needed. Necrotizing faciitis is an uncommon surgical in- fection that involves the subcutaneous tissue and superficial fascia in a dissecting suppurative proc- ess. Originally described by Jones' in 1871 as "hospital gangrene," it carries a high mortality rate (from 30 to 80 percent).2 Although early writ- ers thought that group A hemolytic streptococcus was the main causative organism, the polymicro- bial nature of this infection has been well docu- mented more recently.3 Without aggressive and timely surgical treatment, the outcome is invari- ably fatal. From the Department of Surgery, Howard University Col- lege of Medicine, Washington, DC. Requests for reprints should be addressed to Dr. Macy Hall, Jr, Department of Surgery, Division of Plastic and Reconstructive Surgery, Howard University Hospital, 2041 Georgia Avenue, NW, Washington, DC 20060. METHODS All cases with the final diagnosis of necrotizing fasciitis between 1965 and 1980 were reviewed. Additionally, all autopsies with this diagnosis (or a likely synonym such as phlegmon or spreading fasciitis) between 1974 and 1980 also were re- viewed. The following criteria were deemed nec- essary for a diagnosis of necrotizing fasciitis: (1) clinical evidence of fascial necrosis, (2) spreading cellulitis with undermining of fascial planes, and (3) systemic toxicity as evidenced by altered men- tal state and hyperthermia. RESULTS There were eight patients (four men and four women) whose ages ranged from 45 to 78, with a mean of 57 years. Seven patients were diabetic. One patient had documented squamous cell carci- noma of the anorectum. An additional patient had suspected intestinal lymphoma. We report here the first documented case of necrotizing fasciitis in association with hidradenitis suppurativa. The sites of origin in our patients are noted in Table 1. Oftentimes the initiating factor was obscure, but trauma (operative and incidental) was indicated in 50 percent of our cases. Inadequately drained abscesses in diabetics frequently culmi- nated in this infection (37 percent in this series). Most of our patients presented with an obvious source of infection; however, one patient was admitted to the medical service in diabetic keto- acidosis. She developed necrotizing fasciitis which originated from an infected, two-week-old hemor- rhoidectomy site. Fever, chills, and pain were fre- quent complaints. Two patients presented with urinary retention secondary to penile edema. Men- JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 75, NO. 2,1983 159
Transcript of necrotizing fasciitis: the howard university hospital experience

NECROTIZING FASCIITIS:THE HOWARD UNIVERSITYHOSPITAL EXPERIENCEMark Walker, MD, and Macy Hall, Jr, MD, FACSWashington, DC
All surgical cases from 1965 to 1980 and au-topsy cases from 1974 to 1980 diagnosed atHoward University Hospital as necrotizingfasciitis (NF) were reviewed. Eight patient ful-filled the criteria for NF, which included (1)fascial necrosis, (2) spreading cellulitis withundermining of fascial planes, and (3) sys-temic toxicity as evidenced by altered mentalstate and hyperthermia. Bacteroides fragiliswas commonly found in our most recentcases. Poor prognostic signs included (1)documented bacteremia, (2) preoperativehypotension (systolic blood pressure lowerthan 80 mmHg), and (3) hypocalcemia (serumcalcium less than 7.0 mg/dL). Therapy con-sisted of wide debridement with systemic an-tibiotics and delayed skin grafting whenneeded.
Necrotizing faciitis is an uncommon surgical in-fection that involves the subcutaneous tissue andsuperficial fascia in a dissecting suppurative proc-ess. Originally described by Jones' in 1871 as"hospital gangrene," it carries a high mortalityrate (from 30 to 80 percent).2 Although early writ-ers thought that group A hemolytic streptococcuswas the main causative organism, the polymicro-bial nature of this infection has been well docu-mented more recently.3 Without aggressive andtimely surgical treatment, the outcome is invari-ably fatal.
From the Department of Surgery, Howard University Col-lege of Medicine, Washington, DC. Requests for reprintsshould be addressed to Dr. Macy Hall, Jr, Department ofSurgery, Division of Plastic and Reconstructive Surgery,Howard University Hospital, 2041 Georgia Avenue, NW,Washington, DC 20060.
METHODSAll cases with the final diagnosis of necrotizing
fasciitis between 1965 and 1980 were reviewed.Additionally, all autopsies with this diagnosis (or alikely synonym such as phlegmon or spreadingfasciitis) between 1974 and 1980 also were re-viewed. The following criteria were deemed nec-essary for a diagnosis of necrotizing fasciitis: (1)clinical evidence of fascial necrosis, (2) spreadingcellulitis with undermining of fascial planes, and(3) systemic toxicity as evidenced by altered men-tal state and hyperthermia.
RESULTSThere were eight patients (four men and four
women) whose ages ranged from 45 to 78, with amean of 57 years. Seven patients were diabetic.One patient had documented squamous cell carci-noma of the anorectum. An additional patient hadsuspected intestinal lymphoma. We report herethe first documented case of necrotizing fasciitis inassociation with hidradenitis suppurativa.
The sites of origin in our patients are noted inTable 1. Oftentimes the initiating factor wasobscure, but trauma (operative and incidental) wasindicated in 50 percent of our cases. Inadequatelydrained abscesses in diabetics frequently culmi-nated in this infection (37 percent in this series).Most of our patients presented with an obvioussource of infection; however, one patient wasadmitted to the medical service in diabetic keto-acidosis. She developed necrotizing fasciitis whichoriginated from an infected, two-week-old hemor-rhoidectomy site. Fever, chills, and pain were fre-quent complaints. Two patients presented withurinary retention secondary to penile edema. Men-
JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 75, NO. 2,1983 159

NECROTIZING FASCIITIS
TABLE 1. DISTRIBUTION OF SITES OF ORIGININ NECROTING FASCIITIS
Number ofSite of Origin Patients
Ischiorectal area 1Anus 1Perineum 1Groin (including upper 2
thigh and inguinalregion)
Sacrum 1Penis 1
tal obtundity and lethargy were sometimes seen onadmission.
Physical examination revealed cellulitis or anabscess, or both, usually without crepitation.Hyperthermia was usually present but hypother-mia can exist, especially in patients with markeddebilitation or adrenal insufficiency. Nonspecificfindings that may be present include hypoactivebowel sounds secondary to paralytic ileus andbasilar rales (from sepsis).
Laboratory data indicated that most of the pa-tients had uncontrolled diabetes; the mean serumglucose on admission was 383 mg/dL. Anemia(mean HgB of 27), hypocalcemia, and hypoalbumin-emia were common laboratory findings. Three ofthe patients died, all of whom had serum calciumlevels less than 7 mg/dL during hospitalization.X-rays were supportive; in one case, subcutane-ous emphysema was noted in the right hemi-thorax. Some authors feel that the presence ofsoft-tissue gas is important in making an earlydiagnosis of necrotizing fasciitis.4
All but one of our patients had mixed bacterialcultures. E coli and y-streptococci were the mostfrequently recovered organisms. Bacteroides wasfound commonly and was the main pathogen inour most recent cases (Table 2). Klebsiella bac-teremia was documented in two of our patientswith positive blood cultures. Both of these pa-tients died.
The treatment of necrotizing fasciitis is wideexcision and debridement.5 With inadequate orlate drainage, the outcome was usually death sec-ondary to septic shock with multiple organ failure.Antibiotics were used in all cases; penicillin or apenicillin derivative was used most frequently.
Because of the high frequency of coliform cul-tured, an aminoglycoside was used almost routine-ly. Steroids were used in 50 percent of ourpatients, whereas hyperbaric oxygen was notutilized.
CASE REPORTA 60-year-old nondiabetic black woman pre-
sented with a painful draining abscess of her backof two weeks' duration. There was a history offever but no chills. She had undergone wide exci-cion and grafting in 1972 because of hidradenitissuppurativa. She had been admitted in 1979 for anabscess of the right foot and multiple drainingsinuses of her buttocks and perineum. Culturesfrom her foot grew Bacteroides and Peptostrepto-coccus. There was a history of generalized weak-ness and an inability to walk for a few days priorto admission. She also complained of frequency ofurination and nocturia.
Physical examination revealed the following:temperature, 97°F; pulse, 80 beats/min; respira-tions, 24/min; and blood pressure, 110/80 mmHg.The patient appeared lethargic, and was confusedand disoriented. Scleral icterus and marked con-junctival pallor were noted. The chest revealedbibasilar rales. The heart revealed normal S, andS2 sounds. The point of maximum intensity wasprominent and located in the 5th intercostal space,2 cm lateral to the midclavicular line. A systolicejection murmur, grade III/VI, was heard at theapex and along the left sternal border. The abdo-men was rotund with a transverse scar in theLUQ. The bowel sounds were hypoactive, andhepatomegaly was present. Rectal examinationrevealed anal induration and loss of tone withoutany rectal masses. The stool guaiac was negative.Multiple draining sinuses involving both buttocks,perineum, and groin were noted. The musculo-skeletal examination revealed an abscess of 4x4cm in the right lumbar region (L3 level) with foul-smelling pus and an area of surrounding cellulitis.Generalized muscular weakness was present. Theneurologic examination was within normal limitsexcept for hyperactive lower extremity reflexesbilaterally. Laboratory examinations revealed:hemoglobin, 3.8 g/dL; hematocrit, 12.6 percent;WBC, 26,000/mm3, with 60 percent segments, 12percent bands, 25 percent lymphocytes, 2 percent
160 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 75, NO. 2, 1983

NECROTIZING FASCIITIS
TABLE 2. BACTERIOLOGIC FINDINGS IN NECROTIZING FASCIITIS
Organism Wound Culture Blood Culture
E coli 5 0Clostridium perfringens 2 0y-Streptococci 5 0Bacteroides 4 0Klebsiella sp 3 2Pseudomonas sp 2 0Enterobacter aerogenes 1 0a-Streptococci 1 0
monocytes, and 1 percent eosinophils; platelets,615,000 mmHg; serum calcium, 7.6 mg/dL; phos-phate, 1.0 mg/dL; albumin, 1.7 mg/dL; total pro-tein, 8.0 mg/dL; total bilirubin, 4.0 mg/dL;glucose, 117 mg/dL; creatinine, 1.4 mg/dL; elec-trolytes: Na, 131 mEq/l; K, 3.5 mEq/l; Cl, 106mEq/1; and CO2, 19 mEq/l; and BUN, 39/dL.Chest x-ray films revealed bilateral interstitialedema, and the abdominal flat plate showed ileus.
Hospital CourseThe initial impression was anaerobic abscess
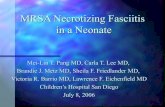
with severe anemia. The gram stain from thedrained abscess revealed many white cells andgram-negative bacilli and a few gram-positivecocci in clusters (blood and wound cultures weredone). Clindamycin (Cleocin) and tobramycinwere started. Over the next 72 hours, packed celltransfusions to increase the hematocrit to 31.0percent were accomplished. Albumin also wasgiven. Initial skin tests to tuberculosis, Candida,and mumps suggested anergy. The white bloodcount dropped to 17,000 mm3. However, physicalexamination revealed cellulitis spreading to theanterior abdominal wall, the shoulder, and theright breast (Figure 1). The presumptive diagnosisof necrotizing fasciitis was made. Wide excision ofthe skin and subcutaneous tissue of the lateral andanterior abdominal wall was performed. Multipletransverse incisions above and below the largedefect were utilized also. Silver sulfadiazine(Silvadene)-impregnated gauze was used to packthe wounds (Figure 2).
Pulmonary edema, metabolic acidosis, andhypotension were encountered postoperatively.Ventilatory support, bicarbonate, volume expan-sion with albumin and human plasma protein frac-tion (Plasmanate), and diuretics were used. Theseabnormalities, which were believed related tosepsis, were corrected. On the fourth postopera-tive day, the patient became lethargic and unre-sponsive. Her serum glucose was 32 mg/dL at thistime. Chronic adrenal insufficiency was sus-pected. Baseline cortisol levels were obtained andsystemic hydrocortisone was begun, in addition toa bolus of intravenous hypertonic glucose solution.
The patient improved, and total parenteral nu-trition was started. On the seventh postoperativeday, oozing from venipuncture sites was seen.Coagulation studies revealed a prothrombic timeof 15 seconds (control 11), thrombin time of 9 sec-onds (control 6), PTT of 46 seconds (control 35),and a platelet count of 78,000/mm:3. Fresh frozenplasma and vitamin K were given for a suspectedvitamin K deficiency. By the eighth postoperativeday, the white count had fallen to 8000/mm3 andthe wound began to show evidence of healthygranulation tissue. She was weaned from steroidswithout incident.Two weeks after the initial operation, skin graft-
ing was done with a 98 percent take (Figure 3).Postoperatively, adrenal insufficiency was sus-pected again and clinical response to steroids wasevident. A gluteal abscess developed, which re-quired incision and drainage. Because of hidrade-nitis, extensive debridement of both buttocks wasaccomplished, followed by skin grafting. The pa-tient represents one of the survivors of this series.
JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 75, NO. 2,1983 161

NECROTIZING FASCIITIS
Figure 1. Progressive cellulitis involving the ante-rior chest wall with pitting edema of the skin overly-ing the breast
DISCUSSIONThe etiology of necrotizing fasciitis certainly is
based on a host-pathogen interaction as describedby Tehrani and Ledingham.3 Host factors such asdiabetes mellitus, protein-calorie malnutrition,and hypoglobulinemia reflect compromised hostdefense mechanisms which play a large role insusceptibility to this infection. Specifically regard-ing diabetes, chemotactic defects of polymorpho-nuclear leukocytes, especially in the uncontrolleddiabetic, have been documented.6 Reticuloendo-thelial cell dysfunction also has been defined inlongstanding diabetics,7 and may play a role in thepresence or absence of septicemia in necrotizingfasciitis.
Protein-calorie malnutrition, with its attendantanergy (as documented in one patient), in a generalway prevents the host from combatting infection.Hypoalbuminemia and hypoglobulinemia may in-deed reflect this state. Clearly the role of cancer inthe etiology of this infection is open to specula-tion. Because of the small size of our series, noconclusions can be drawn.
Hidradenitis suppurativa is a chronic infectionof the apocrine glands usually involving the axilla,groin, and perineum. A review of the literaturerevealed no previous documentation of necrotiz-ing fasciitis associated with hidradenitis sup-purativa.
Figure 2. Healed transverse incisions with healthygranulation tissue at the base of the operativewound
Figure 3. Complete coverage with split thicknessskin graft from right thigh donor site
In terms of pathogen factors, the streptococcuselaborates collagenases, hemolysins, and otherenzymes, which helps to explain the fascial de-struction and hemolytic anemia frequently foundwith this infection. The presence of sialic acids onthe cell walls of the streptococcus and E coli helpsto inactivate the alternate complement pathwayand may facilitate the evasion of host defense bythese microorganisms.8'
162 JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 75, NO. 2, 1983

NECROTIZING FASCIITIS
Anaerobic organisms were recovered in half ofour cases. Fecal contamination in the ischiorectal,perineum, and groin areas provides a source andportal of entry for these organisms. The loweredredox potential (accomplished by the aerobic of-fenders) allows the anaerobes to flourish.
Some authors have claimed that the presence ofsoft-tissue gas is an early indicator of necrotizingfasciitis.4 This has not been our experience. In thefour patients who had evidence of gas (clinically orby x-ray), two died and the two who survived hada longstanding process.
The presence of necrotic fascia, spreading cel-lulitis with undermining, and systemic toxicity issufficient for the diagnosis. Leukocytosis, hypo-calcemia, hypoalbuminemia, and anemia are sup-portive. The differential diagnosis of necrotizingfasciitis includes:
1. Bacterial synergistic gangrene (Meleney'sulcer): Usually seen postoperatively and locatedaround drains or retention sutures. There is lim-ited necrosis and no undermining.
2. Erysipelas: Characterized by an erythema-tous area with sharply defined borders, induration,and marked pain.
3. Gas gangrene: A deep infection usuallyfound in contaminated wounds. It involves muscleas well as subcutaneous tissue. Gram stain showspositive bacilli.
It must be emphasized that necrotizing fasciitiscan affect underlying muscle and deep fascia,especially when it goes untreated for a long time.One of our patients had necrosis of the anteriorabdominal wall and burrowing of the infectiousprocess into the peritoneum, with subsequent peri-tonitis. The cases reported by Stone and Martin,9termed synergistic necrotizing cellulitis, probablyfall in this category.
Early diagnosis can be made only if this infec-tion is anticipated. Diabetics with soft-tissueabscesses must have adequate incision and drain-age. Failure to provide complete drainage may re-sult in this infection.
Although this entity has been described amongdrug addicts none of our patients fell into this cat-egory. 10 We admonish all practitioners to keep thisentity in mind when treating abscesses in drugaddicts.
The only known successful treatment for thiscondition is wide surgical debridement. All ne-crotic and devitalized tissue must be removed. In
addition, transverse incisions may be utilized toprovide wide tissue plane drainage.1 Althoughsystemic antimicrobials must be used, they cannotreplace surgery. One should not hesitate to usechloramphenicol, clindamycin, or aminoglyco-sides, as needed. A frequent efficacious combina-tion used at this institution includes clindamycinand gentamicin, with or without penicillin. Ste-roids should be used when adrenal insufficiency issuspected and may be of some value in patientswith septic shock. Central hyperalimentationplays a large role in the peri- and postoperativemanagement of our more debilitated patients. Ouroverall mortality rate was indeed high (62 per-cent), but comparable to that of most series. Wefeel that the following are poor prognostic signs inthis infection: (I) documented bacteremia, (2) pre-operative hypotension (systolic of 80 mmHg), and(3) serum calcium of less than 7.0 mg/dL.
All physicians should be familiar with this dis-ease entity, especially those responsible for treat-ing diabetics. Necrotizing fasciitis is a surgicalemergency, and wide debridement and delayedskin grafting are acceptable therapy.
Literature Cited1. Jones J. Investigation Upon the Nature, Causes and
Treatment of Hospital Gangrene as it Prevailed in the Con-federate Armies, 1861-1865. New York: US Sanitary Com-mission Surgical Memoirs of the War of Rebellion, 1871.
2. Kyle RF, Gustilo RB. Necrotizing fasciitis-A lethalinfection. Minnesota Medicine 1979; 62:775-777.
3. Tehrani JR, Ledingham IM. Necrotizing fasciitis.Post Grad Med J 1977; 53:237-242.
4. Fisher JR, Conway MJ, Takeshita RT, et al. Necrotiz-ing fasciitis-importance of roentgenographic studies forsoft-tissue gas. JAMA 1979; 241:803-808.
5. Tehrani MA, Webster HC, Robinson DW, et al. Nec-rotizing fasciitis treated by radical excision of the overlyingskin. Br J Plast Surg 1976; 29:74-77.
6. Edwards JE, Tillman DB, Miller ME, et al. Infectionand diabetes mellitus. West J Med 1979; 130:515-521.
7. Drivas G, Wardie N. Reticuloendothelial cell dys-function and hyperlipidemia. Metabolism 1980; 27:1533-1538.
8. Fearon DT, Austen KW. Current concepts in immu-nology: the alternative pathway of complement-a systemfor host resistance to microbial infection. N Engl J Med1980; 303:259-263.
9. Stone HH, Martin JD, Jr. Synergistic necrotizing cel-lulitis. Ann Surg 1972; 175:702-71 1.
10. Melluzzo PJ, Willscer M, Mason HD, et al. Necrotiz-ing fasciitis in narcotic addicts. Am Surg 1976; 42:251-253.
11. Bahary CM, Joel-Cohen SJ, Neri A. Necrotizing fas-ciitis. Obstet Gynecol 1977; 50:633-637.
JOURNAL OF THE NATIONAL MEDICAL ASSOCIATION, VOL. 75, NO. 2,1983 163