NCAA SPORT SCIENCE INSTITUTE UPDATE
83
Transcript of NCAA SPORT SCIENCE INSTITUTE UPDATE


NCAA SPORT SCIENCE INSTITUTE UPDATE
Brian Hainline, MD
NCAA Chief Medical Officer
Clinical Professor of Neurology
Indiana University School of Medicine
New York University School of Medicine

Neither Brian Hainline, nor any of his family members,
have any relevant financial relationships to be
discussed, directly or indirectly, referred to or
illustrated with or without recognition within the
presentation.
FACULTY DISCLOSURE

MISSIONTo promote and develop safety, excellence, and wellness
in college student-athletes, and to foster life-long
physical and mental development.
VISIONTo be the pre-eminent sport science voice for all student-
athletes and NCAA member institutions, and to be the
steward of best practices for youth and intercollegiate
sports.

Cardiac Health
Concussion
Doping and Substance Abuse
Mental Health
Nutrition, Sleep and Performance
Overuse Injuries and Periodization
Sexual Assault and Interpersonal Violence
Athletics Healthcare Administration
Data-Driven Decisions
STRATEGIC PRIORITIES

Association-wide actions in pursuit of a solution for issues that
challenge the principle of student-athlete well-being.
Conceptual framework: 9 Strategic Priorities.
Current process:
CSMAS and SSI identify issues.
Task force/summit held with membership buy-in.
Endorsement process.
Distribution of recommendations.
UNIFIED STANDARDS OF CARE 1.0

EXAMPLES OF UNIFIED STANDARDS OF CARE 1.0

CSMAS assists BoG in its responsibility to “identify core issues that affect
the Association as a whole.”
Identify issues that:
• Rise to the level of Association-wide concern for student-athlete health and
safety.
• Require a uniform, Association-wide response.
CSMAS recommended criteria (from DI BoD request):
1. The issue involves new scientific evidence with anticipated
Association-wide importance.
2. The issue will impact a core Association-wide value.
3. The issue poses a legal risk to the Association.
4. The issue poses a reputational risk to the Association.
UNIFIED STANDARDS OF CARE 2.0

UNIFIED STANDARDS OF CARE PROCESS 2.0

Transparent communication of process with membership.
Determine level of BOG communication in process.
Broad and reasonable membership participation in task
force/summit.
Integrated communication of endorsed recommendations
with all stakeholders.
Local delivery with Athletics Health Care Administrator.
SSI provides tools, checklist and oversight for AHCA.
Ongoing assessment (internal audit) of impact on health
and safety.
UNIFIED STANDARDS OF CARE (2.0) PROCESS

CONCUSSION

We do not understand the natural history of concussion.
We do not understand neurobiological recovery in concussion.
Solution:
NCAA-DoD Grand Alliance.
CARE Consortium.
Mind Matters Educational Grand Challenge.
Inter-Association Guidelines and Legislation
CONCUSSION

>80% of military TBIs are concussions.
85% of military concussions are biomechanically similar to sport-
related concussion.
15% are from blast injuries.
College s-a and military service are similar in age, athleticism, risk
taking and pushing to the edge of excellence.
The military theatre is poorly controlled; college sports are a much
more controlled environment.
Numerous meetings, evaluations, culminating in NCAA-DoD MOU
and CRADA and White House announcement.
NCAA AND DoD JOINT ENDEAVOR

Executive CommitteeRauch (DoD), Hack & Hainline (NCAA), Koroshetz (NIH)
Administrative
Coordinating Center:
Indiana U School of Medicine
McAllister (coPI)
Advanced Research
Coordinating Center:
Medical College of Wisconsin
McCrea (coPI)
Longitudinal Clinical Study
Coordinating Center:
U of Michigan
Broglio (coPI)
Longitudinal Clinical Study
Core (CSC)
Advanced Research Core
(ARC)
Indiana U
(BIG10)
Hipskind & Port
U Michigan
(BIG10)
Eckner
Washington
(PAC12)
Chrisman
U North Carolina
(ACC)
Guskiewicz &
Mihalik
U Pittsburgh
(ACC)
Kontos & Collins
U Georgia
(SEC)
Schmidt
U Florida
(SEC)
Clugston
U Oklahoma
(BIG12)
Anderson
UCLA
(PAC12)
Giza & DiFiori
Consortium Operating Committee
Anderson, Broglio (co-Chair), Clugston, Duma, Giza, Guskiewicz,
McAllister (co-Chair), McCrea (co-Chair), McGinty, Putukian
Scientific
Advisory PanelIverson, Jordan, Kelly,
Marshall, Saykin, Smith,
Talavage, Wallace, Xu
U Wisconsin
(BIG10)
Brooks
Princeton
(Ivy)
Putukian
Concussion Research Initiative
US Coast Guard
Academy
(New England)
O’Donnell
US Naval Academy
(Patriot)
Pecina
Virginia Tech
(ACC)
Duma & Rowson
U Delaware
(Colonial)
Buckley & Kaminski
Humboldt State
(California)
Ortega
Azusa Pacific
(Pacific West)
Hoy
U Rochester
(University)
Bazarian
Cal Lutheran
(Southern
California)
Kelly
Publications
CommitteeBroglio, Brooks, Eckner,
Katz, McAllister, McCrea,
Schmidt, Svoboda
Bloomsburg U
(Pennsylvania)
Hazzard
Temple U
(American)
Langford & Tierney
U Chicago
(University)
Benjamin
U Miami
(ACC)
Feigenbaum
U North Georgia
(Peach Belt)
Miles
U Pennsylvania
(Ivy)
Master
Wake Forest U
(ACC)
Miles
Wilmington
College
(Ohio)
Dykhuizen
Winston-Salem
State U
(Central)
Lintner
US Military
Academy
(Patriot)
Svoboda
US Air Force
Academy
(Mountain West)
McGinty & Campbell

CSC & ARC ASSESSMENT PROTOCOL
Pre-
SeasonAcute Concussion Sub-Acute Concussion
Post-
Concussion
Baseline<6hrs
Post-Injury
24-48hrs
Post-Injury
Asymptomatic /
Cleared for
Return to Play
Progression
Unrestricted
Return to Play 7 days
following
Return to
Play
6 Months
Post-Injury
Neurocognitive and
Behavioral Testing
(CSC)X X X X X X X
Blood Biomarker &
DNA CollectionX X X X X X
Multi-modal MRI
StudiesO X X X X
Head Impact Measurement: HITS (FB) and non-helmeted sensors (FB, SCR, LAX, IH)

Neurobiological
Pre-Injury
Factors
- Genetics
- Neurologic
Vulnerabilities
Trauma
Burden
- Injury Severity
- Repetitive
Exposure
- Polytrauma
Biomarkers
- Structural/
Functional
Imaging
- Blood
Biomarkers
Psychosocial
Psychologic
al Function
- Premorbid
- Post-injury
Comorbidities
Environmenta
l Factors
- Social Support
- Life Stressors
- Latrogenesis
Motivational
Factors
- Expectation
- Secondary
Gain
Multi-Domain Predictor Variables
NEUROBIOPSYCHOSOCIAL MODEL
Neurocognitive
FunctionNeurobehavioral
Function
Psychological
Health and
Wellness
Life Function &
Quality
Neurologic
Health
Multi-Dimensional Outcome
McCrea, McAllister & Morey, 2012
Advancing the Science of SRC and TBI

CARE Preliminary Summary to Date:
Largest prospective concussion study to date
Both sexes, all sports
“Not just football”
Short-term longitudinal study (6 months)
Short-term neurobiology
Sets the stage for long-term cohort study: “the Framingham study of
concussion…”

CARE Summary to Date
Largest prospective concussion study to date
>30,000 evaluations
>2200 concussions
Both sexes, all sports
“Not just football”
Short-term longitudinal study (6 months)
Short-term neurobiology
Sets the stage for long-term cohort study: “the Framingham study of
concussion…”

6.7
3.4
6.2
3.25
0 1 2 3 4 5 6 7 8 9 1011121314
CARE(2014-15)
NCAA1(1999-2001)
Time(Days)
Dura onofSymptoms
SFWP
RTP: 6.65 Days
RTP: 12.9 Days
RTP: Then and Now
Science Informing Clinical Practice
Average Graded Exertion Protocol: 6.6 Days (2.9)

Translational Impact: Injury Prevention
6.5
3.6
0
1
2
3
4
5
6
7
NCAA1(1999-2001) CARE(2014-15)
RateofRepeatCC(%
)
Rate=percentage of concussed players who sustained 2nd concussion in same season
CARE (2014-15)
10 SS Repeats
0 Repeat < 10 Days
Mean Interval: 74.2 Days75%
< 7 Days
92%
< 10 Days
Mean Interval:
5 days

NCAA-DoD MIND MATTERS GRAND CHALLENGE
Executive CommitteeRauch (DoD), Hack & Hainline (NCAA), Koroshetz (NIH)
Education and Research Challenge
Consortium(Operating Committee)
NCAA: Dawn Buth, Amy Dunham, Dana Thomas
DoD: Tara Cozzarelli, Stephanie Maxfield-Panker, Kathleen Quinkert
CDC: Kelly Sarmiento
Education Challenge Research Challenge
Administrative Coordinating Center:Indiana U School of Public Health
Nir Menachemi, Ross Silverman
MomsTEAM
Institute(de Lench)
University of
Arizona(Valerdi)
U. of South
Alabama(Marass)
Creative
Street Media (Katzenberger)
Johnson C.
Smith U.(Williams)
UNC
Greensboro(Wyrick)
U. Wis-
Madison(Warmath)
UNC Chapel
Hill(Mihalik)
Colorado
State U.(Coatsworth)
U. of
Georgia(Schmidt)
Northern
Arizona U.(Craig)
U.S. Air
Force(D’Lauro)
Arizona
State U.(Corman)
Chestnut Hill
College(Ernst)

Goal: To change important concussion safety behaviors and the culture
of concussion reporting and management by funding research to better
understand behavior change strategies and by identifying novel
educational approaches.
Aim 1 (Immediate Impact Challenge)
Develop a multi-media educational program based on the best
evidence currently available about how to change culture in young
and emerging adults.
Aim 2 (Long-term Impact Challenge)
Identify key factors and ways to affect change in the culture and
behavior of young and emerging adults and their influencers
around concussion.
MIND MATTERS CHALLENGE

Year-round football practice contact.
Concussion diagnosis and management.
Independent medical care.
Primary athletics health care providers.
Director of medical services.
Catastrophic injury.
Second Safety in College Football Summit(February 2016)

Inseason and bowl:
3 days of practice are non-contact/minimal.
1 day of live contact/tackling.
1 day of live contact/thud.
Preseason:
3 days of practice are non-contact/minimal contact.
3 days of live contact.
Non-contact follows scrimmage.
One day of no football practice.
Traditional 2/day not allowed. 2nd session can include walk-
throughs, but no conditioning.
Spring: day following live scrimmage is non-contact/minimal contact.
Year-Round Football Practice Contact: Draft Recommendations

An active member institution shall establish an administrative
structure that provides independent medical care and affirms the
unchallengeable autonomous authority of primary athletics health
care providers (team physicians and athletic trainers) to determine
medical management and return to play decisions related to student-
athletes.
An active institution shall designate a director of medical
services/athletics health care administrator to oversee the
institution’s athletic health care administration and delivery.
This position may become THE key for addressing the delivery
gaps at lower resource schools.
Independent Medical Care

MENTAL HEALTH

MENTAL HEALTH OCCURS ON A CONTINUUM
Mental HealthResilience and
thriving
Mental health
disorders

Mental Health is not apart
from, but rather a part of
athlete health.
To promote health is to
enhance performance.
It is important to
understand
sport specific issues
related to athlete health
and safety,
and engage a wide range
of experts.
THE NCAA BELIEVES THAT…

NCAA MENTAL HEATLH INITIATIVES
A call from the mother of a WKU
men’s basketball student-athlete
who committed suicide in 2002 in
his dorm room after experiencing a
career ending injury.
Led to a meeting in 2005 of 20
sports psychologists in their effort to
create a new professional
community.
And resulted in the publication and
dissemination of the Coaches
Handbook:

Culture of “toughness” can limit help seeking
Perception that “looking fit” or performing well means that
the athlete is healthy
Pressure to perform
High Visibility
Practice/travel = missed class = academic stress
Injury
Time demands (and compromised sleep)
Other concerns . .
ATHLETE-SPECIFIC CONCERNS

Clinicians, researchers, advocates, educators, athletics
administrators, coaches and student-athletes.
Comprehensive assessment of stressors and mental
health disorders in college student-athletes.
Goal: To develop best practices and to recommend
research that support member institutions in meeting their
membership obligations to provide a healthy and safe
environment for student-athletes.
NCAA MENTAL HEALTH TASK FORCE NOVEMBER 2013

Coach
Athlete Development
Sports Medicine
Sports Nutrition
Strength & Conditioning
Counseling & Sport Psychology
Athlete

FATALITIES IN NCAA STUDENT-ATHLETE FROM 2004-2009
Accidents51%
Cardiac16%
Suicide9%
Cancer7%
Homicide6%
Other Medical3%
Sickle Cell Trait2%
Drug Overdose2%
Heat Stroke1% Meningitis
1%
Unknown2%

DEPRESSION NCHA
Have you ever…..Felt so depressed that is was difficult to
function (Yes, in last 12 months)
STUDENT-ATHLETES NON-ATHLETES
Male 21% (1,623) 27%
Female 28% (3,303) 33%
White 24% 30%
Black 26% 30%
Other 29% 34%

ANXIETY NCHA
Have you ever…..Felt overwhelming anxiety (Yes, in last 12
months)
STUDENT-ATHLETES NON-ATHLETES
Male 31% (2,439) 40%
Female 48% (5,747) 56%
White 42% 52%
Black 29% 41%
Other 43% 50%

AGGRESSIVE BEHAVIOR IN THE LAST 12 MONTHS – Comparison by Athlete Status
Males Females Overall
SA Non-Ath SA Non-Ath SA Non-Ath
Been in a physical fight 24% 12% 6% 5% 14% 7%
Been physically assaulted
(excluding sexual assault) 9% 6% 4% 4% 6% 4%
Been verbally threatened 38% 27% 19% 17% 27% 21%
In an emotionally abusive
relationship 8% 7% 10% 11% 9% 10%
In a physically abusive
relationship 3% 2% 3% 2% 3% 2%
*highlighted items indicate a statistically significant difference, chi-square, p<.01

MEDIAN HOURS PER WEEK SPENT ON ATHLETIC ACTIVTIES PER WEEK (2015 Student-Athlete Self Report)
Notes: Yellow indicates median up 2 hours/week or more vs. 2010 study. Green indicates median down
by 2 hours/week or more vs 2010.

PERCENTAGE OF STUDENT-ATHLETES REPORTING THEY WOULD PREFER TO SPEND MORE/LESS TIME ON ATHLETICS(2015 Student-Athlete Self Report)
Outliers:
• Two-thirds of DI and DII men’s golfers want to spend more time on athletics
• DI softball, DI women’s lacrosse, DI field hockey, and DI women’s rowing – more than 30% of SAs
would prefer less time on athletics (only 15% in those sports want more)

MEDIAN HOURS PER WEEK SPENT ON ACADEMIC ACTIVTIES PER WEEK (2015 Student-Athlete Self Report)
Notes: Yellow indicates median up 2 hours/week or more vs. 2010 study. Green indicates median down
by 2 hours/week or more vs 2010.

PERCENTAGE OF STUDENT-ATHLETES REPORTING THEY WOULD PREFER TO SPEND MORE/LESS TIME ON ACADEMICS(2015 Student-Athlete Self Report)
Outliers:
• DI women’s rowing: 83% would prefer more time on academics
• Men’s golf across divisions most likely (>15%) to express wanting less time on academics
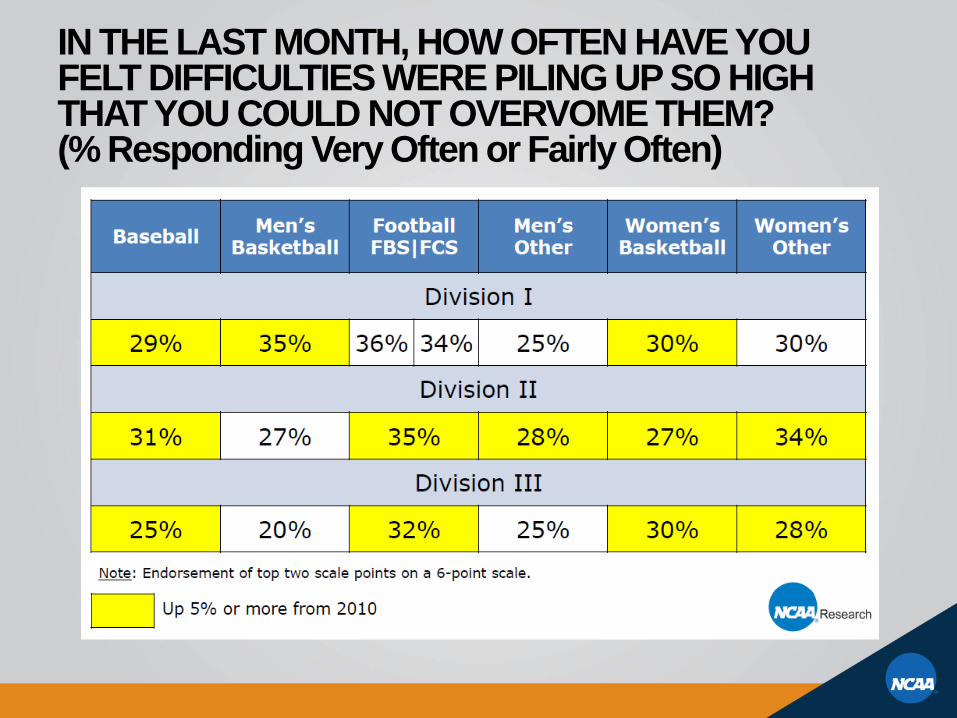
IN THE LAST MONTH, HOW OFTEN HAVE YOU FELT DIFFICULTIES WERE PILING UP SO HIGH THAT YOU COULD NOT OVERVOME THEM? (% Responding Very Often or Fairly Often)

SUMMARY OF FINDINGS

SUMMARY OF FINDINGS



Ensure that mental health care is provided by licensed
practitioners qualified to provide mental health services.
Clarify and disseminate referral protocol.
Consider mental health screening in PPEs.
Create and maintain a health-promoting environment that
supports mental well-being and resilience.
GUIDELINE SUMMARY

Care should be provided by*:
Clinical or counseling psychologists.
Psychiatrists.
Licensed clinical social workers.
Psychiatric mental health nurses.
Licensed mental health counselors.
Primary care physicians with core competencies to treat mental health disorders.
*Include registered dietician in multidisciplinary team for eating disorders.
Individual providing care should have cultural competency that addresses both societal diversity and the culture of sports.
GUIDELINE #1

“It is important to note that issues that may initially and appropriately be viewed as
related to performance may upon further engagement reveal underlying mental health
concerns.”48
Best Practice #1

Coach
Athlete Development
Sports Medicine
Sports Nutrition
Strength & Conditioning
Applied Sport & Exercise Psychology
Athlete
Licensed Clinical Psychology
Performance Enhancement Consulting
Additional considerations:
Financial support for dedicated service.
Physical location.
Autonomous authority, consistent with his or her
professional licensure, to determine mental health
management for student-athletes.
Care should be subject to relevant laws governing
patient confidentiality, including possible exemption
from mandated reporting.
GUIDELINE #1

Ensure that athletic departments have clarified their
procedures for referring athletes with potential mental
health concerns to appropriate personnel.
GUIDELINE #2

Emergency action management plan:
Should address emergency mental health-related
situations including:
• Managing suicidal and/or homicidal ideation.
• Managing victims of sexual assault.
• Managing highly agitated or threatening behavior, acute
psychosis or paranoia.
• Managing acute delirium/confusional state.
• Managing acute intoxication or drug overdose.
GUIDELINE #2

Routine mental health referrals
Provide written institutional procedures regarding
appropriate referral of student-athletes to all
stakeholders within the athletics department.
Identify a point person responsible for facilitating such
referrals (e.g., AT, team physician).
GUIDELINE #2

Consider implementing mental health screening as part
of annual pre-participation exams.
Determine screening approach in consultation with
licensed mental health professional providing mental
health care to student-athletes.
Establish procedure specifying when and to whom
symptomatic or at-risk student-athletes identified through
this screening process will be referred.
Screening tools are not validated as stand-alone
assessments for mental health disorders.
GUIDELINE #3

Create a health promoting environment that supports
mental well-being and resilience.
Student-athletes, FARs and coaches should be educated
about the importance of mental health, including how to
manage mental health concerns.
GUIDELINE #4

Coaches play a central role and should be:
educated on signs and symptoms of mental health
disorders;
trained in empathic response;
encouraged to create a positive team culture;
advised of department referral protocols.
GUIDELINE #4

Medication Management Plan
Ensure that student-athletes with medication are being
appropriately monitored.
Require student-athletes to list all medications and
supplements they are taking.
Maintain on file documentation from personal
physicians to demonstrate appropriate diagnostic
evaluation and treatment protocols for medication use.
ADDITIONAL CONSIDERATIONS

Financial Support
Clarify institutional policies related to athletic financial awards and team engagement for student-athletes who are unable to continue sport participation, either temporarily or permanently, due to mental health considerations.
Clarify institutional policies for financial support of student-athletes in need of extended outpatient treatment or inpatient care.
ADDITIONAL CONSIDERATIONS

Transitional Care
Establish a clear transition of care plan for athletes who are leaving the college sport environment.
Identify
• Who is responsible for initiating transition of care?
• Who is responsible for providing athletes with information about community mental health resources?
• Who is responsible for ensuring athletes have adequate medication, as necessary, until continuing care is established?
Establish a transition plan for returning student-athletes who have been away from campus seeking care for mental health issues.
ADDITIONAL CONSIDERATIONS

Mental health is not apart from, but rather, a part of athlete health.
Athletic environments can support help seeking and facilitate early identification, appropriate referral and care.
Establishing protocols for care means more equitable care across sports and within institutions.
Implementation of Best Practice is an important step towards ensuring a model of care for student-athlete mental health.
IN SUMMARY

www.ncaa.org/violenceprevention
ADDRESSING CAMPUS SEXUAL ASSAULT AND INTERPERSONAL VIOLENCE

SEXUAL VIOLENCE PREVENTIONAN ATHLETICS TOOL KIT FOR A HEALTHY AND SAFE CULTURE
Checklists and
implementation
tools to advance
core commitments:
1. Leadership
2. Collaboration
3. Compliance
4. Education
5. Student-athlete
Engagement
http://www.ncaa.org/sport-science-institute/sexual-violence-prevention-tool-kit

Demonstrates that sexual assault is a problem.
Describes what sexual assault looks like.
Recognition of signs of abusive behavior.
Provides information on student rights and campus obligations.
Highlights the role of alcohol.
Builds skills related to sexual assault prevention.
Communication/language.
Seeking consent.
Introduces basic bystander intervention strategies.
Risk appraisal.
Prepares student-athletes for future training in Step UP!
myPlaybook SEXUAL ASSUALT MODULE

Raise awareness of helping behaviors (why people do or
do not help).
Increase motivation to help.
Develop skills and confidence when responding to problematic behaviors.
Ensure the safety and well being of other.
www.stepupprogram.org
BYSTANDER INTERVENTION

CARDIAC HEALTH

CARDIAC TASK FORCE

Cardiovascular Risk in Student-Athletes.
The Pre-Participation Evaluation.
Evidence Supporting the Use of the Pre-Participation Evaluation for Detection of Cardiovascular Disease.
ECG as a screening tool for sudden cardiac death risk prediction.
Regional referral centers for evaluation of athletes suspected or known to have a cardiovascular condition.
Recognition and response to cardiac arrest.
Cardiac Research Initiatives.
Checklist.
INTER-ASSOCIATION CONSENSUS STATEMENT ON CARDIOVASCULAR CARE
OF COLLEGE STUDENT-ATHLETES


DOPING & RECREATIONAL DRUG USE

Doping is cheating.
Recreational drug use is different.
Inconsistency is problematic.
Need: Effective deterrence model.
Need: Conference consistency.
Need: Effective intervention.
DOPING AND RECREATIONAL DRUG USE

71

72

73

74

75
76

77

78

79

DATA ANALYTICS & INFORMATICS

Evidence-based decisions.
No centralized data collection or analysis.
Solution: Datalys.
Solution: Trust.
Target: PPE.
DATA ANALYTICS

THANK YOU
Contact info: Brian Hainline
@ncaa_ssi
www.ncaa.org/ssi