
NC I A Comprehensive Cancer CC C - RV Mais …rvmais.com.br/meetingwithexperts/Aulas/05-07/2_16h00...
48
Stage III Resectable and Unresectable NSCLC David S. Ettinger, M.D. Alex Grass Professor of Oncology The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins A Comprehensive Cancer Center Designated by the National Cancer Institute N I C C C C
-
Upload
duongnguyet -
Category
Documents
-
view
213 -
download
0
Transcript of NC I A Comprehensive Cancer CC C - RV Mais …rvmais.com.br/meetingwithexperts/Aulas/05-07/2_16h00...

Stage III Resectable and Unresectable NSCLC David S. Ettinger, M.D.
Alex Grass Professor of Oncology The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins
A Comprehensive Cancer Center Designated by the National Cancer Institute
N I C C C C

Disclosure Statement
Reported a financial interest/relationship or affiliation in the form of: Consultant, Biodesix, Boehringer-Ingelheim GmbH, Eli Lilly and Company, Gilead, Genentech: A member of the Roche Group

Discussion
• Resectable stage III NSCLC – Adjuvant therapy – Neoadjuvant therapy
• Unresectable stage III NSCLC
– Combined modality therapy • Conclusions

NSCLC Survival Stage and Survival
Stage
Frequency %
5 Year Survival (%)
1 10 58-73 2 20 36-46
3A 15 24 B 15 9
4 40 <2

Rationale for Multimodality Treatment in Localized NSCLC
• Survival after local therapy leaves room for improvement
• Most recurrences of NSCLC are distant
• Sensitive assays can detect occult metastases (micrometastases) in many “early stage” patients

Resectable Stage III NSCLC

Cisplatin-Based Adjuvant Chemotherapy in Patients with Completely Resected NSCLC International Adjuvant Lung Cancer Trial Collaborative Group
New Engl J Med 2004; 350:351-360
N=1867 • Stage I-III • Complete
surgical resection within 60 days
R
A
N
D
O
M
I
Z
E
Cisplatin 80 mg/m2 q 3 wk × 4 OR Cisplatin 100 mg/m2 q 4 wk × 3-4 OR Cisplatin 120 mg/m2 q 4 wk × 3
PLUS
Etoposide 100 mg/m2 × 3 days/cycle OR Vinorelbine 30 mg/m2 weekly OR Vinblastine 4 mg/m2 weekly OR Vindesine 3 mg/m2 weekly
No chemotherapy

0 1 2 3 4 5
Surgery
Surgery + Chemotherapy
p<0.03
Years
International Adjuvant Lung Cancer Trial International Adjuvant Lung Cancer Trial Collaborative Group
New Engl J Med 2004; 350:351-360
Ove
rall
Sur
viva
l (%
)
100
80
60
40
20
0
Received Chemo Without Benefit
Received Chemo Without Need
4% Benefit

CALGB 9633
T2N0M0 (IB) NSCLC
(Complete resection) Observation
Carboplatin (AUC=6) Taxol (200mg/m2)
4 cycles/12 wk
RANDOM I ZE
Strauss GM, et al. 2004 ASCO Abs 7019

----- Carbo/Taxol ----- Observation
HR 0.62 [0.41-0.95] p=0.028
0 20 40 60 80
Survival Time (Months)
0.00.2
0.40.6
0.81.0
Prob
abilit
y
71% 59% 4 yr
CALGB 9633 - Overall Survival Strauss G, ASCO 23:7019, 2004
CALGB 9633: Two Years Later
• Median follow-up now 54 months. • 131 of the 150 deaths for the planned
final analysis have occurred. • DFS: HR 0.74 (2 sided p=0.02) • 3 year survival:
– CP: 79% – Control: 70% p=0.045
• 5 year survival: – CP: 60% – Control: 57% p=0.32
• Median overall survival: – HR 0.8, one sided p=0.1

Adjuvant Chemotherapy: Standard of Care for Early Stage NSCLC
Trial Stage N Chemo Survival
IALT I-III 1867 Cis+Etop/Vinca +4%
NCIC IB-II 482 Cis+Vinorelbine +15%
CALGB IB 344 Carbo+Tax +14%-+2%
ANITA I-III 840 Cis+Vinorelbine +9%

Intergroup Trial Adjuvant Chemotherapy + Bevacizumab in Patients with Completely Resected Stage
1B (>/=4 cm) – IIIA NSCLC STRATIFICATION
FACTORS Type of chemotherapy Vin/Cin; Doc/Cis Gem/Cis; Pem/Cis Stage IB vs. II vs. IIIA (N2) vs. IIIA (T3N1) Histology Squamous vs. Other Gender M vs. F
R A N D O M I Z E
Chemo. Alone x 4 cycles
Chemo. + Bev. x 4 cycles (continue Bev. for up to 1 yr.)
Activated: June 2007 Chair: Heather Wakelee, M.D.

What is “Resectable”?
Resectability is all in the mind of the surgeon!
Nael Martini – 7th IASLC WLCC

Stage IIIA (N2) NSCLC Surgery in “Resectable” Disease
Survival Minimal N2 Disease
Bulky N2 Disease
MST 16-30 months 12-14 months
3-year 15-48% 7-18%
5-year 8-34% 3-11%
Rationale for Neoadjuvant Therapy
• Reduces tumor burden – Downstaging of primary – Surgery potentially easier
• Prevents tumor seeding at surgery • Better treatment compliance • Earlier treatment of micrometastatic disease
with chemotherapy • Evaluation of tumor sensitivity in vivo • Prolongs survival???

Phase III Induction Chemo-Surgery Trials for IIIA
Trial Therapy n Median survival (months)
Survival (%)
P-value
NCI PE +Surg Surg+XRT
13 14
28.7 15.6
42 (3-yr) 12 (3-yr)
0.095
Rossell MIC+Surg Surg (XRT)
30 30
26 8
30 (3-yr) 0 (3-yr)
<0.005
Roth CEP+Surg Surg
28 32
21 14
36 (5-yr) 15 (5-yr)
0.048
Depierre MIC+Surg+MIC Surg
187 186
37 26
52 (3-yr) 41 (3-yr)
0.15
Pass et al Ann Thor Surg 1992, Rosell et al NEJM 1994, Roth JNCI 1994, Depierre JCO 2002
PE = cisplatin, etoposide MIC = mitomycin, ifosfamide, cisplatin CEP = cisplatin, etoposide, cyclophosphamide
Depierre et al. found that the benefit of chemo was in N0-1 disease (RR 0.68) and not in N2 disease (RR 1.04)

Induction Chemotherapy Trials
• Bimodality Lung Oncology (BLOT) (carboplatin, paclitaxel)
• French Thoracic Cooperative Group (gemcitabine, cisplatin vs. carboplatin, paclitaxel
• Medical research Council LU-22 (MIC vs. mitomycin, vinblastine, and cisplatin)
• NATCH (carboplatin, paclitaxel)
• CLINCH (carboplatin, paclitaxel) • CHEST(gemcitabine, cisplatin)
The role of surgery in IIIA patients after neoadjuvant
chemotherapy remains controversial.
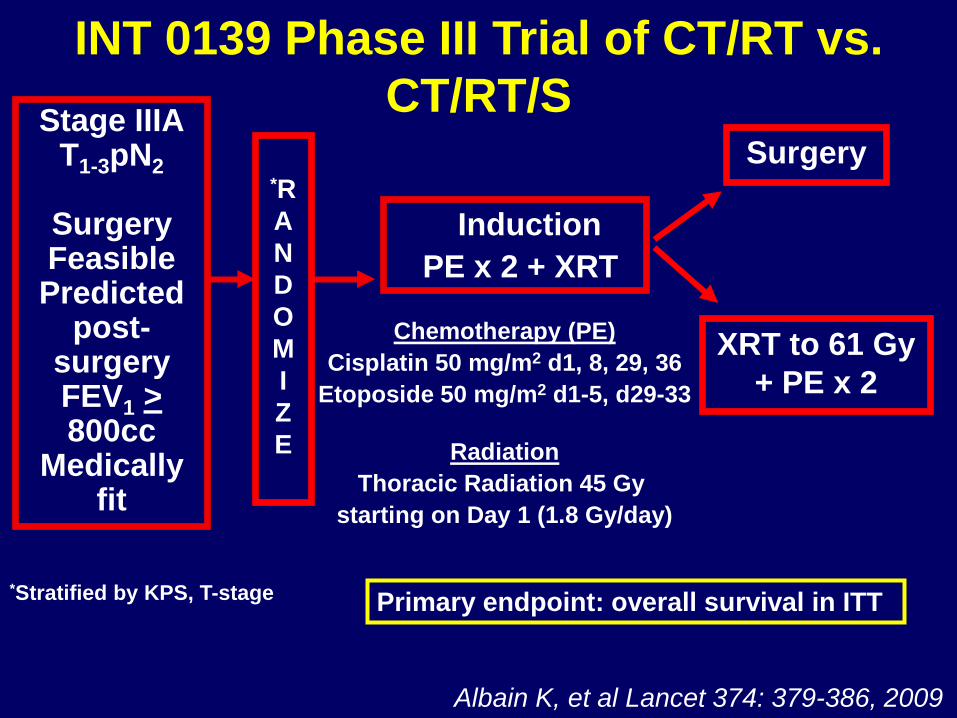
INT 0139 Phase III Trial of CT/RT vs. CT/RT/S
Albain K, et al Lancet 374: 379-386, 2009
Chemotherapy (PE) Cisplatin 50 mg/m2 d1, 8, 29, 36
Etoposide 50 mg/m2 d1-5, d29-33
Radiation Thoracic Radiation 45 Gy
starting on Day 1 (1.8 Gy/day)
Induction PE x 2 + XRT
Surgery
XRT to 61 Gy + PE x 2
Stage IIIA T1-3pN2
Surgery Feasible Predicted
post-surgery FEV1 > 800cc
Medically fit
*R A N D O M I Z E
*Stratified by KPS, T-stage Primary endpoint: overall survival in ITT

INT 0139 PFS Favors Tri-Modality Arm
Months from Randomization
/
/ / / / / / / / / / / / / / / / / / / / / / / / / 0
25
50
75
100
0 12 24 36 48 60
/
/ / / / / / / / / / / / / / / / / / / / / / / / / % A
live
with
out P
rogr
essi
on
CT/RT/S CT/RT 5-yr Median PFS (mo) 12.8 10.5 5-yr PFS Rate 22.4% 11.1%
CT/RT/S N=202
CT/RT N=194
HR 0.77, p=0.017
Albain K, et al Lancet 374: 379-386, 2009

INT 0139 Overall Survival %
Aliv
e
Months from Randomization
HR 0.87 p=0.24
0
25
50
75
100
0 12 24 36 48 60
CT/RT/S N=202
CT/RT N=194
Albain K, et al Lancet 374: 379-386, 2009
CT/RT/S CT/RT
5-yr Median OS (mo) 23.6 22.2 5-yr OS Rate 27.2% 20.3%

Chemo-XRT (n=179)
ChemoXRT-Surgery (n=177)
Induction ChemoXRT 0 0
30 days Post-operative period - 10 (5%)
Consolidation ChemoRT
4 (2%) -
Other 0 6 (3%)
Total 4 (2%) 16 (8%)
INT 0139 Deaths
Deaths on surgery arm mostly occurred in pneumonectomy patients (14 of the 16 pts).
26% (n=14/54) of all pneumonectomy cases died; mostly from ARDs and respiratory failure.
Albain K, et al Lancet 374: 379-386, 2009

Months from Randomization
% A
live
0
25
50
75
100
0 12 24 36 48 60
/
/ /
/ / / /
/ /
/
CT/RT/S N=38
CT/RT N= 42
p = NS
INT 0139 OS by Pneumonectomy vs. CT/RT
CT/RT/S CT/RT Median OS (mo) 18.9 29.4
3 yr OS 36% 45% 5 yr OS 22% 24%
Albain K, et al Lancet 374: 379-386, 2009

INT 0139 OS by Lobectomy vs CT/RT %
Aliv
e
0
25
50
75
100
Months from Randomization 0 12 24 36 48 60
/ / / / / / / / / / / / / /
/ / / / / / / / /
CT/RT/S N=57
CT/RT N=74 p = 0.002
CT/RT/S CT/RT Median OS (mo) 33.6 21.7
5 yr OS 36% 18%
Albain K, et al Lancet 374: 379-386, 2009

Summary: INT 0139
• Neoadjuvant chemo-radiation before surgery improves PFS but not OS over definitive chemo-radiation in stage IIIA (T1-3 pN2) NSCLC patients.
• There was a trend towards increased 5-year OS rates with the tri-modality arm.
• N0 status at surgery predicts for greater 5-yr survival; i.e. down-staging is associated with improved survival.
Albain K, et al Lancet 374: 379-386, 2009

Summary: INT 0139
• No significant differences in toxicity beyond increased esophagitis in the chemo-radiation alone arm.
• In patients that require a pneumonectomy, neoadjuvant chemo-radiation is associated with a high risk of post-operative death (26%).
• At this time, can safely consider neoadjuvant chemo-radiation in very good PS patients who can receive a lobectomy.

S9900: Treatment Schema
Stage IB-IIIA
(excluding N2)
R
A
N
D
O
M
I
Z
E
Paclitaxel and Carboplatin x 3 cycles
Surgery
Surgery
Stratify by stage IB/IIA vs IIB/IIIA
Pisters ASCO 2007 Abs #7520
N = 336

Overall Survival by Treatment Arm (median F/U 53 mo)
HR=0.81 [0.60-1.10], p=0.19
0%
20%
40%
60%
80%
100%
0 24 48 72 96 Months After Registration
Median 3 year 5 year
Preop 75 mos 62% 50%
Control 46 mos 57% 43%
Per
cent
Sur
viva
l
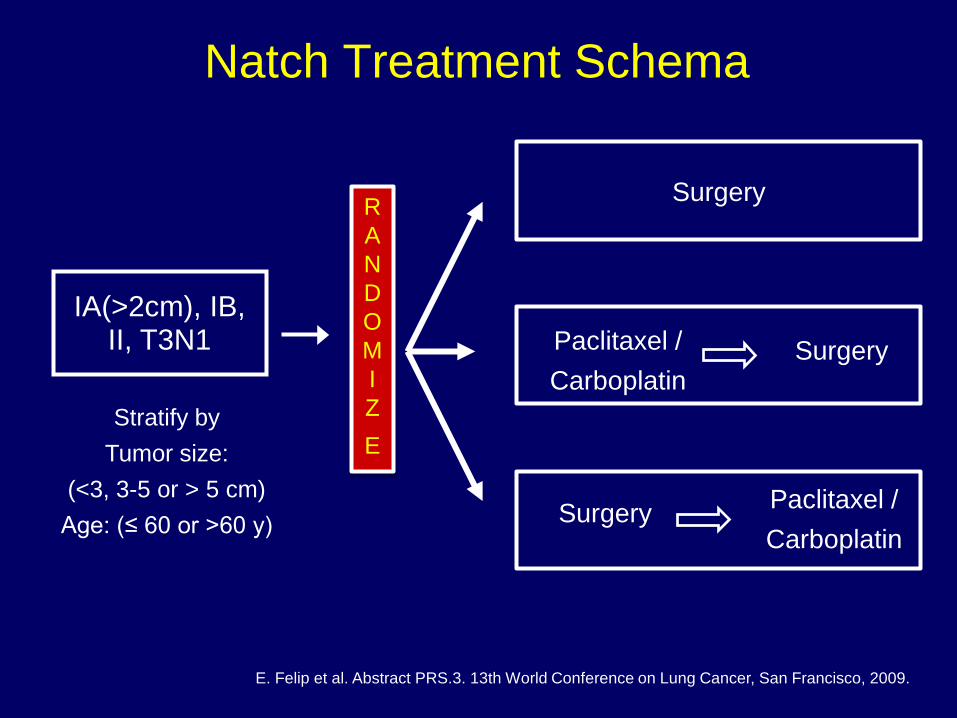
Natch Treatment Schema
Stratify by Tumor size:
(<3, 3-5 or > 5 cm) Age: (≤ 60 or >60 y)
Surgery
Surgery Paclitaxel / Carboplatin
Surgery Paclitaxel / Carboplatin
IA(>2cm), IB, II, T3N1
R A N D O M I Z E
E. Felip et al. Abstract PRS.3. 13th World Conference on Lung Cancer, San Francisco, 2009.

Overall Survival by Arm
At risk:
Surgery 168 131 105 72 40 27
ADJ CT 161 121 90 65 40 29
PREOP CT 165 131 99 71 45 31
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 1 2 3 4 5 6 Time (years)
Pro
babi
lity
Surgery ADJ CT PREOP CT (N=210) (N=210) (N=199) Events 109 102 99 Median OS 48.8 50.3 55.2 3-year OS 58.6% 58.4% 59.2% 5-year OS 44% 45.5% 46.6% ADJ CT vs Surgery: HR=0.99 (0.75 to 1.3); P=0.93 PREOP CT vs Surgery: HR=0.96 (0.84 to 1.1); P=0.56
E. Feip et al. Abstract PRS.3. 13th World Conference on Lung Cancer, San Francisco, 2009.

Post Operative Radiotherapy (PORT) Following Complete Resection
Meta-analysis of 9 Trials in 2128 Pts
• Adverse effect of postoperative radiotherapy on survival (p=0.001) with a hazard radio of 1.21, a 21% relative increased death risk. Survival decreased from 55% to 48% at 2 years.
• Adverse effect greatest for Stage I/II, N0-N1
• No adverse effect with Stage III, N2 Lancet 1998; 352:257

Treatment Options for Unresectable Stage III NSCLC



Phase III Randomized Study of Induction Chemotherapy Followed by CT/XRT vs. CT XRT Alone in Unresectable NSCLC (CALGB 39801)
• 366 stage III pts entered between 10/98 – 5/02 • Goal: To show a 40% ↑ in median survival: 13 to 18 mo. CT/XRT CT → CT/XRT # of Pts. 182 184 Gr 3/4 ANC (%) 11/4 21/6 Gr 3 anemia (%) 5 11 Gr 3/4 esoph. (%) 30/1 28/7 MS (mo.) 12 14 p =.3 2 yr. Surv. (%) 29 31 Vokes et al, JCO 2007

Efficacy
Median OS time 22.7 months 2-year survival rate 49.3%
Blumenschein et al. JCO 2011
Median PFS 12 months 2-year progression-failure rate 55.2%

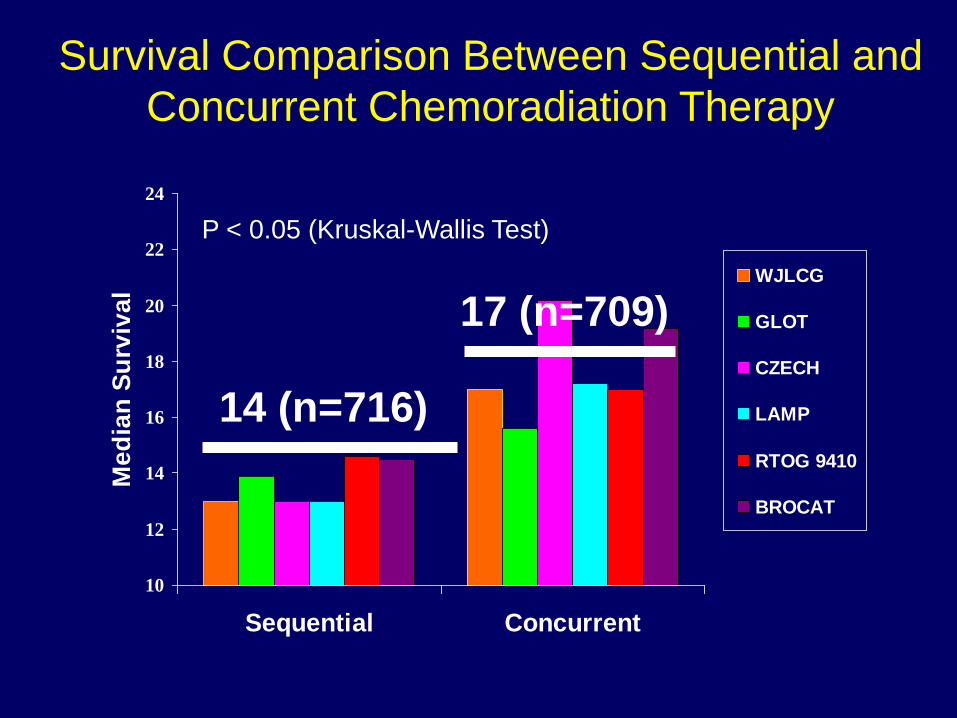
Concurrent vs. Sequential CT/RT (RTOG 9410)
• RX: SEQ: CIS/VINB x 2 → 60 Gy RT D50 Con QD RT: Cis/Vinb x 2/60 Gy RT D1 Con BID RT: Cis/Oral Etop/69.6 Gy BID RT D1 P-value Gr 3/4 Arm MST 4-yr Surv vs SEQ Esophagitis SEQ 14.6 mo 12% 4% Con QD RT 17.0 mo 21% 0.046 25% Con BID RT 15.2 mo 17% 0.296 47% WJ Curran, et al, ASCO 2003
10
12
14
16
18
20
22
24
Sequential Concurrent
Med
ian
Surv
ival
WJLCG
GLOT
CZECH
LAMP
RTOG 9410
BROCAT
14 (n=716)
17 (n=709)
Survival Comparison Between Sequential and Concurrent Chemoradiation Therapy
P < 0.05 (Kruskal-Wallis Test)

0
5
10
15
20
25
30
Sequential Concurrent
% E
soph
agiti
s (G
3/4) WJLCG
GLOT
CZECH
LAMP
RTOG 9410
BROCAT
Early Toxicity Comparison between Sequential and Concurrent Chemoradiation Therapy
4%
23%

SWOG 9504 - Therapy for Stage IIIB (T4 or N3) NSCLC
• Therapy: PE x 2/XRT → Docetaxel x 3 P - 50 mg/m2 d1,8,29,36 E - 50 mg/m2 d1-5 & 29-33 XRT d1 45 Gy + 16 Gy Boost D 75 mg/m2 cycle 1, 100 mg/m2 cycles 2, 3
• No. of pts - 83 • Major toxicity - neutropenia • Overall Response 63% (4% CR) • Median Survival 26 mo. • 1 & 2 yr Survival 76% and 53%
Gandara et al, 9th World Conference on Lung Cancer

SWOG 9504 Update: Concurrent Chemoradiotherapy with consolidation
Docetaxel in Stage IIIB NSCLC
• Rx: P 50 mg/m2 d 1, 8, 29 & 36; E – 50 mg/m2 d1-5, 29- 33, current RT d1 61 Gy (1.8-2.0 Gy/d) followed by consolidation Doc 75-100 mg/m2 q 21d x 3 • 83 patients • Results N Med. Surv. (mo.) 5-yr. (%) T4N0-1 31 32 29 T4N2 27 26 37 N3 25 16 20
Gandara et al, ASCO 2005

RANDOMIZE
HOG LUN 01-24
Concurrent Consolidation CisP/VP-16/RT Docetaxel
Concurrent: CisP/VP-16/RT

Stage arm=Arm CD Stage lllB
Overall Survival By Stage For only the 143 randomized patients with stage and survival data
Survival Distribution Function
1.00
0.75
0.50
0.25
0.00 20 25 50 75 100 200 175 150 125
Weeks since registration
Cox proportional hazards Stage p=0.6606 Arm p=0.8768 Stage*Arm p=0.9004
SWOG 9504

RTOG 0617: Conventional vs. High Dose RT +/- C225
R A N D O M I Z E
XRT: 60 Gy Carbo-paclitaxel
+/- cetuximab
XRT: 74 Gy Carbo-paclitaxel
+/- cetuximab
Carbo-paclitaxel X 2 cycles
A total 500 pts have been accrued.
The high-dose XRT 74 Gy arms have been
closed due to lack of OS benefit on May
2011.

Conclusion: Resectable IIIA Consider XRT after surgical
resection for improved local-regional control. Then adjuvant cisplatin-doublet based chemo.
Microscopic pN2
Surgery after chemoradiation improves PFS but not OS in
excellent PS patients. DO NOT consider pre-op
chemoradiation in patients who require a pneumonectomy.
ChemoXRT + Surgery
Unclear whether preoperative or adjuvant chemo is better.
Recommend multi-modality Tx. Clinical N2

Conclusion: Unresectable III
Stage IIIA/IIIB
Concurrent chemo-radiation is standard of care. Chemo regimen should be platinum-doublet based. Role of induction chemo versus consolidation chemo is unclear. - SWOG 9504 had high survival results in IIIB pts; yet, HOG LUN phase III study did not show a survival benefit for consolidation docetaxel .

Optimal: “Systemic + Local”
Monoclonal antibodies (e.g. HER-2
-neu)
Gene Therapy
? Novel Chemo
CT ? Timing
? Surgery ? 3-D
Conformal RT
? Altered Fx
Hypoxic Cytotoxins (e.g. tirapazamine)
Angiogenesis Inhibitors
Radioprotectors (e.g. amifostine)
Goals = ↓ Distant Failure ↓ Local Failure
↑ Survival → Quality and Quantity (QOL)


















