NATURAL WAYS TO STOP TMJ CLICKING, GRINDING AND PAIN · together to form the temporomandibular...
16
NATURAL WAYS TO STOP TMJ CLICKING, GRINDING AND PAIN DR. JASON NITZSCHE
Transcript of NATURAL WAYS TO STOP TMJ CLICKING, GRINDING AND PAIN · together to form the temporomandibular...

NATURAL WAYS TO STOP TMJ CLICKING, GRINDING
AND PAIN
DR. JASON NITZSCHE
TABLE OF CONTENTS
INTRODUCTION 2
TEMPOROMANDIBULAR JOINT DISORDER OVERVIEW 3
THE HEAD, NECK AND JAW 5 The Head and Spine 5 The Upper Cervical Spine 5 The3Highways:Nerveflow,Bloodflow,CSFflow 6 IMPROVING TMJ FUNCTION 8 Evaluation11 ReportandInitalCorrection11 Follow-up 12
CONCLUSION 13 TMJRelatedResearch 14
2
Thankyoufordownloadingthise-book.Itismyhopethatyouwilldiscoverpracticalandactionableinformationtohelpyoufindhopeandhealing.MynameisDr.JasonNitzsche,andIhavebeenhelpingpeoplewithtemporomandibularjointdisorders(TMJ)findnaturalanddrug-freereliefformanyyears. MostpeoplecannotappreciatethedevastatingimpactofTMJ.Temporomandibularjointdisordersdisrupteveryaspectoflifeoftencausingpainwithanymouthmovementincludingeating,talking,yawningandmore.
Manypeoplewhohavesomeformofillnessorchronicpainthathasplaguedthemforyearshavehadnumerousdoctors’visitsandpromises,oftenwithoutlong-termresults.Unfortunately,thereisnomagicpotionorpillthatwillsimplyhealyou.Therealizationofthishasledmanypeopletoourdoor.
Theprocessofgettingwellrequiresadoctorthatiswillingtogettothecauseoftheillnessand/orpainandnotjustmasktheproblemwithmeds;adoctorthatunderstandshowtoreverseyearsofdegeneration;andlastly,adoctorthatcancreateasuccessplanincorporatingALLofthefundamentalfacetsofhealthcare,notjustone.TRUEhealinghasoccurredwhenyougetyourbodybacktotheplaceitoncewas(ormaybeevenbetter)beforeyouacquiredthetroublesyouhavetoday!Yes,thatispossiblebutittakeshardworkandconsistency.
Thefundamentalsofuppercervicalcarere–empowerthenervoussystemsothatyoucanhealproperly.Itistrulya“miracle”systemwhendonetoitsfullestpotentialbutitisnotenoughtocreatefullhealth.Fullhealthrequirestheadoptionofaproactivehealthcaremodel;doingwhatittakestogethealthyandstayhealthy,notjusttreatingsymptoms.Thisincludesanervoussystemfreeofinterference,goodnutrition,regularexerciseandplentyofrest.Thisrecipewillremovetheobstacleof“nohope”.ItisasuccesssystemthathealstheONLYeffectiveway...fromthe“insideout”.Thisiswhatwewillbegintoexploreinthise-book.
Thise-bookisforeducationalpurposesonly.Beforebeginninganewdietorexerciseroutine,pleaseconsultaphysician.Thisbookmaynotbereproducedinanypartwithouttheexpresswrittenpermissionoftheauthor.
INTRODUCTION
Thelowerjawisconnectedtotheskullbythetemporomandibularjoints(TMJ)whicharelocatedinfrontofeachear.Thesearecomplicatedjointswhichallowthelowerjawtoopen,close,slideandrotate.Onanaverage,theTMJisusedover5000timeseachdaywhenwechew,swallow,yawn,smile,laugh,eatandspeak! Ifyouhaveevernoticedaclickingsoundwhenyouchew–thenyouarelikelyexperiencingsymptomsofTMJ.Surprisingly,alargenumberoftheadultpopulationisaffectedbythis–anywherebetween20-30%,usuallythosebetweentheagesof20and40.Itismorecommonforwomentosufferfromthisthanmen.
TMJpainismainlycausedduetodamagetothejointitself.Themostcommoncauseistraumatothejaworupperneck,whichleadstoimmensepainanddysfunctioneitherimmediatelyaftertheinjuryorsometimelater.Headandneckinjuriesincludingsportsinjuries,caraccidents,anddentalworkmaybethereasonforthetraumaandresultingTMJdisorder.Otherthingslikeexcessivegumchewing,teethclenching,nailbiting,consistentlyholdingaphonebetweenyourshoulderandthesideoftheheadandotherrepetitivetraumaarepotentialthreatsaswell.TMJcanaffectoneorbothjointsandthesymptomscanvaryfrommildtosevereandfrompersontoperson.
SignsofTMJinclude:
• Clicking,grinding,poppingorothernoisesinthejoint• Painwithorwithoutchewing• Lockingofthejaw• Toothache• Facialand/orneckpain• Headaches• Earaches• Tinnitus(ringingintheears)• Cloggedorstuffyear
3
TEMPOROMANDIBULAR JOINTDISORDEROVERVIEW

Thesesymptomsarefrequentlycausedbythejointbeingoutofalignmentandcanbearesultofmusclefibrousbands(scarliketissues)inthejawmusclesthatcanoccurduetoteethclenchingorgrindingandpoorpostureaswell.Thesymptomscomeaboutwhenmusclestenseupcausingtheskullandlowerjawtopullclosertogetherandendupmisaligned,puttingpressureonthejoint,tearingorstretchingligamentsandcompressingthediscwhichpullsitoutofposition(acommonoccurrenceinwhiplashinjuries).Insomecasesthisleadstojointdegeneration,whenthediscwearsaway,causingthebonestorubagainstandirritatethenerves.
4
5
THEHEAD,NECKANDJAWInordertounderstandtemporomandibularjointdisorders,onehastounderstandwherethejawlives:theheadandneck.
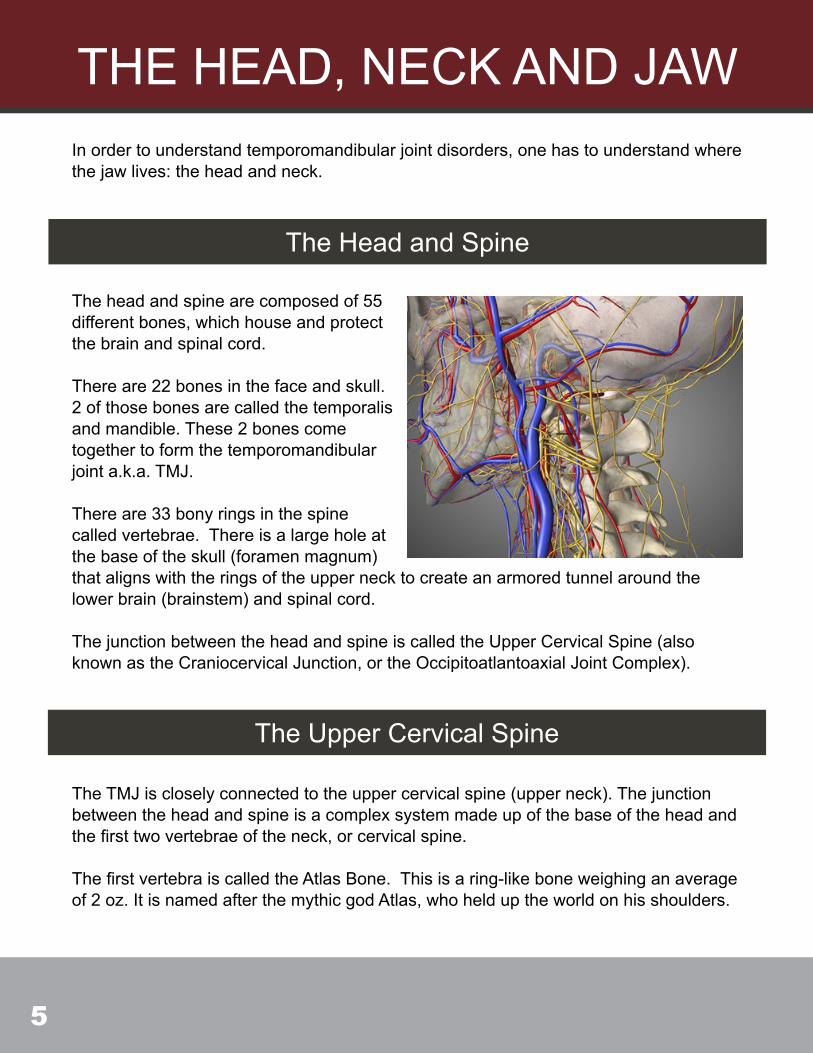
Theheadandspinearecomposedof55differentbones,whichhouseandprotectthebrainandspinalcord.
Thereare22bonesinthefaceandskull.2ofthosebonesarecalledthetemporalisandmandible.These2bonescometogethertoformthetemporomandibularjointa.k.a.TMJ.
Thereare33bonyringsinthespinecalledvertebrae.Thereisalargeholeatthebaseoftheskull(foramenmagnum)thatalignswiththeringsoftheuppernecktocreateanarmoredtunnelaroundthelowerbrain(brainstem)andspinalcord.
ThejunctionbetweentheheadandspineiscalledtheUpperCervicalSpine(alsoknownastheCraniocervicalJunction,ortheOccipitoatlantoaxialJointComplex).
The Head and Spine
TheTMJiscloselyconnectedtotheuppercervicalspine(upperneck).Thejunctionbetweentheheadandspineisacomplexsystemmadeupofthebaseoftheheadandthefirsttwovertebraeoftheneck,orcervicalspine.
ThefirstvertebraiscalledtheAtlasBone.Thisisaring-likeboneweighinganaverageof2oz.ItisnamedafterthemythicgodAtlas,whohelduptheworldonhisshoulders.
The Upper Cervical Spine
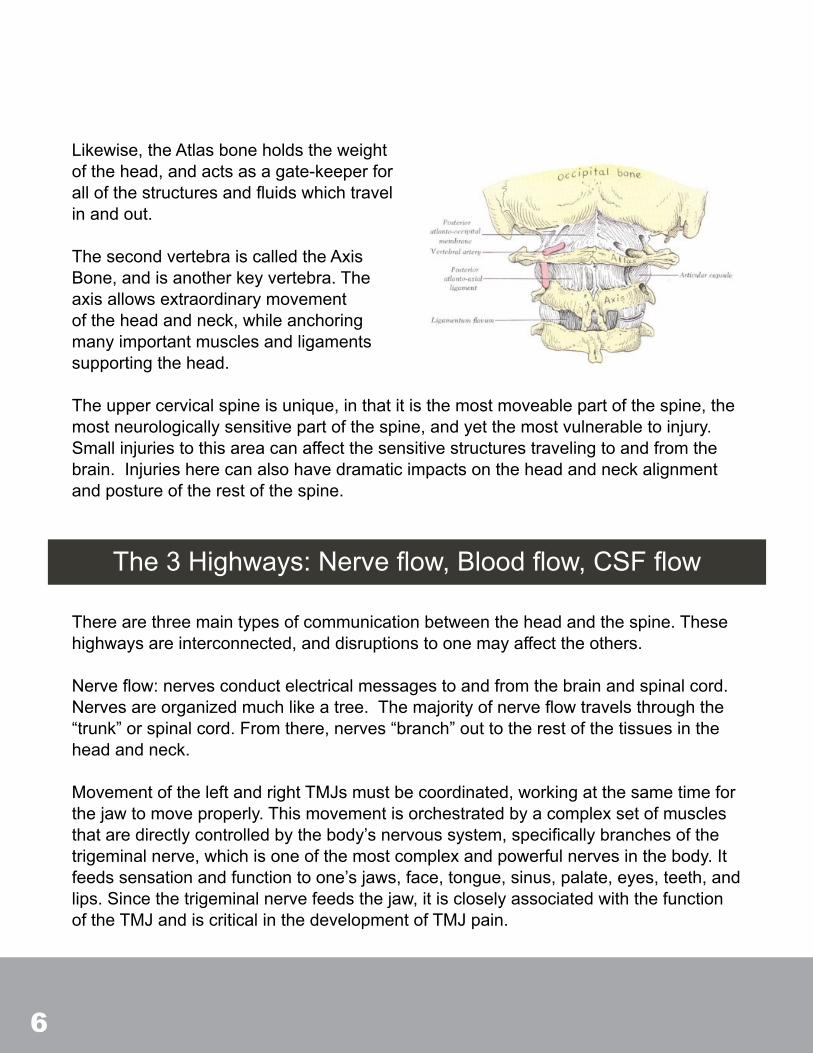
Likewise,theAtlasboneholdstheweightofthehead,andactsasagate-keeperforallofthestructuresandfluidswhichtravelinandout. ThesecondvertebraiscalledtheAxisBone,andisanotherkeyvertebra.Theaxisallowsextraordinarymovementoftheheadandneck,whileanchoringmanyimportantmusclesandligamentssupportingthehead.
Theuppercervicalspineisunique,inthatitisthemostmoveablepartofthespine,themostneurologicallysensitivepartofthespine,andyetthemostvulnerabletoinjury.Smallinjuriestothisareacanaffectthesensitivestructurestravelingtoandfromthebrain.Injuriesherecanalsohavedramaticimpactsontheheadandneckalignmentandpostureoftherestofthespine.
Therearethreemaintypesofcommunicationbetweentheheadandthespine.Thesehighwaysareinterconnected,anddisruptionstoonemayaffecttheothers. Nerveflow:nervesconductelectricalmessagestoandfromthebrainandspinalcord.Nervesareorganizedmuchlikeatree.Themajorityofnerveflowtravelsthroughthe“trunk”orspinalcord.Fromthere,nerves“branch”outtotherestofthetissuesintheheadandneck.
MovementoftheleftandrightTMJsmustbecoordinated,workingatthesametimeforthejawtomoveproperly.Thismovementisorchestratedbyacomplexsetofmusclesthataredirectlycontrolledbythebody’snervoussystem,specificallybranchesofthetrigeminalnerve,whichisoneofthemostcomplexandpowerfulnervesinthebody.Itfeedssensationandfunctiontoone’sjaws,face,tongue,sinus,palate,eyes,teeth,andlips.Sincethetrigeminalnervefeedsthejaw,itiscloselyassociatedwiththefunctionoftheTMJandiscriticalinthedevelopmentofTMJpain.
The3Highways:Nerveflow,Bloodflow,CSFflow
6
7
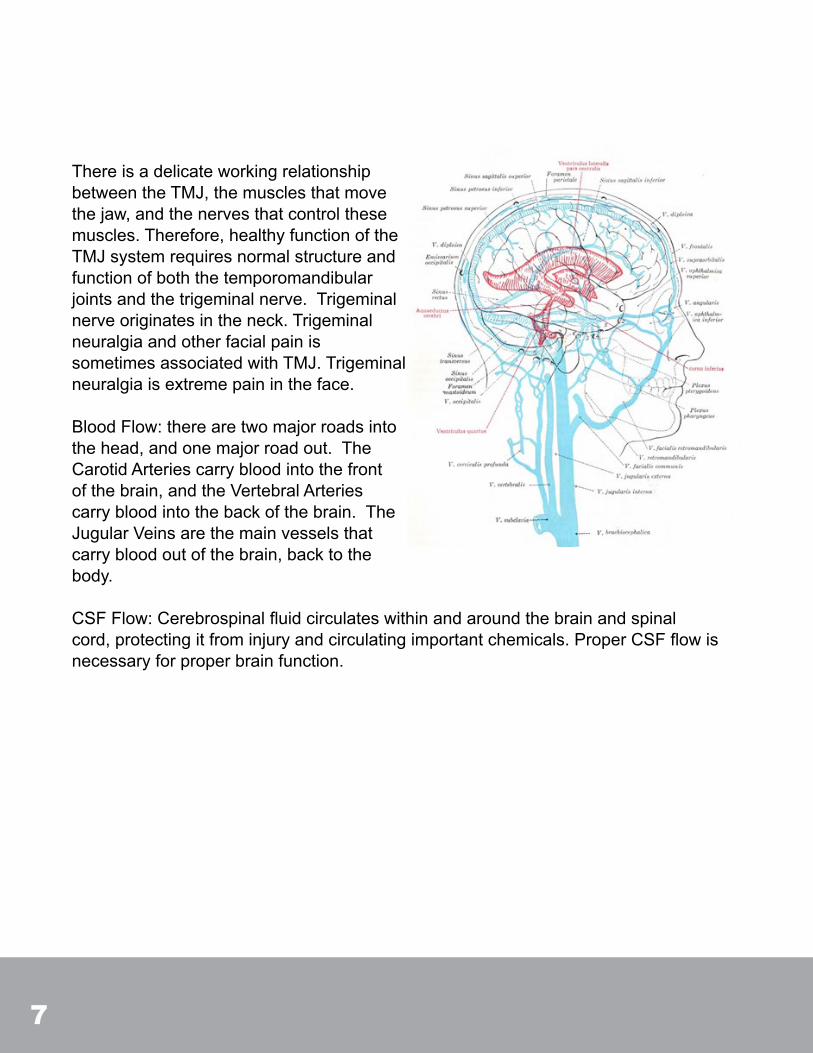
ThereisadelicateworkingrelationshipbetweentheTMJ,themusclesthatmovethejaw,andthenervesthatcontrolthesemuscles.Therefore,healthyfunctionoftheTMJsystemrequiresnormalstructureandfunctionofboththetemporomandibularjointsandthetrigeminalnerve.Trigeminalnerveoriginatesintheneck.TrigeminalneuralgiaandotherfacialpainissometimesassociatedwithTMJ.Trigeminalneuralgiaisextremepainintheface.
BloodFlow:therearetwomajorroadsintothehead,andonemajorroadout.TheCarotidArteriescarrybloodintothefrontofthebrain,andtheVertebralArteriescarrybloodintothebackofthebrain.TheJugularVeinsarethemainvesselsthatcarrybloodoutofthebrain,backtothebody.
CSFFlow:Cerebrospinalfluidcirculateswithinandaroundthebrainandspinalcord,protectingitfrominjuryandcirculatingimportantchemicals.ProperCSFflowisnecessaryforproperbrainfunction.

8
OneoftheprimarycausesofTMJistrauma(motorvehicleaccidents,sportsinjuries,dentalwork,etc.).Restorationofnormaltemporomandibularjoint(TMJ)functionmustbemadevianormalizationofneurologicalcontroloverthemusclesthatgoverntheTMJ.Abnormalneuralinputfromthecentralnervoussystemduetouppercervicaljointdysfunction(fromtraumaticinjury)canresultinabnormalTMJmusclecoordination.Followingthetraumatotheuppercervicalspineandtemporomandibularjoint,symptomscanbetriggeredimmediatelyorcantakemonthsoryearstodevelop.
Itisimportanttoreversethetrauma-inducedupperneckinjury;therebyreducingirritationtothenervesinthebrainstemandspinalcordthatcontrolneuromuscularfunctioninthefaceandjaw.WhilemanyTMJsufferersrecallspecifictraumassuchasheadinjuries,autoaccidentsorfalls,somedonot.Anevaluationisnecessaryineachindividual’scasetoassesswhetheranuppercervicalinjuryispresentandwhetherbenefitfromuppercervicalcarecanbeachieved.
TheAtlasvertebra,alsoknownasC1isthetopboneinthespine.Thisisthebonewheretheheavyheadrests.ThejointbetweentheAtlasandtheskullcanfrequentlybecomedamagedandmisalignedduetoheadandneckinjuries.Oncethepositionofthisupperneckandskullareahasbeenalteredcompensationswilldevelopbothbelowandabovethearea.
AbovetheAtlasmisalignment,theTMJwillfrequentlybeaffected.Astheheadtiltstoonesidemorepressurewillbeappliedtoonesideofthejaw.Thelongerthismisalignmentistherethemorelikelytherewillbefacialasymmetry,painandothersymptoms.
Belowthearea,themusclesaroundtheshoulderswillbegintopullunevenlyleadingtoatiltingoftheshouldergirdle.Frequently,you’llbeabletovisualizethiswhenyoulookinthemirror.Oneshoulderwillbenoticeablyhigherthantheother.
IMPROVINGTMJFUNCTION

9
Continuingdownthespinethemuscleswillcontinuetobeimbalancedasaresultofthemisalignmentintheupperneckandthechangeintheheadposition.
Thiswillleadtoasimilartiltingofthehippositionleadingtounevenhips.Andeventuallyachangeinweightdistributionwheremoreoftheweightwillbeononeleg,frequentlyleadingtounevenwearpatternsontheshoes.
Asmallgroupofclinicalresearchers,biophysicists,PhDs,andspecializedchiropractorshavefocusedonunderstandingthechangesassociatedwithchangestotheheadandneckinthosesufferingwithtemporomandibularjointdisordersandcorrectingthem. Usingthelatestinimagingtechnology,physics,andbiomechanics,auniquetechniquehasbeendevelopedtodetect,andcorrect,changestotheheadandneckresponsibleforalteredheadandneckpostureandtrigeminalnervefunction. ThetechniqueiscalledUpperCervicalCare.Itisexceptionallysafe,gentle,andnon-invasive.Itdoesnotseektotreattemporomandibularjointdisorders,ratherfocusesonrestoringhead,neckandbodyposture,toimprovenervefunctionandrestoreproperalignmentofthejawjoints.However,theresultshavebeenoverwhelminglypositive.
Researchhasshownagreaterthan85%improvementinthosesufferingwithTMJfollowingUpperCervicalCare.TheUpper
10
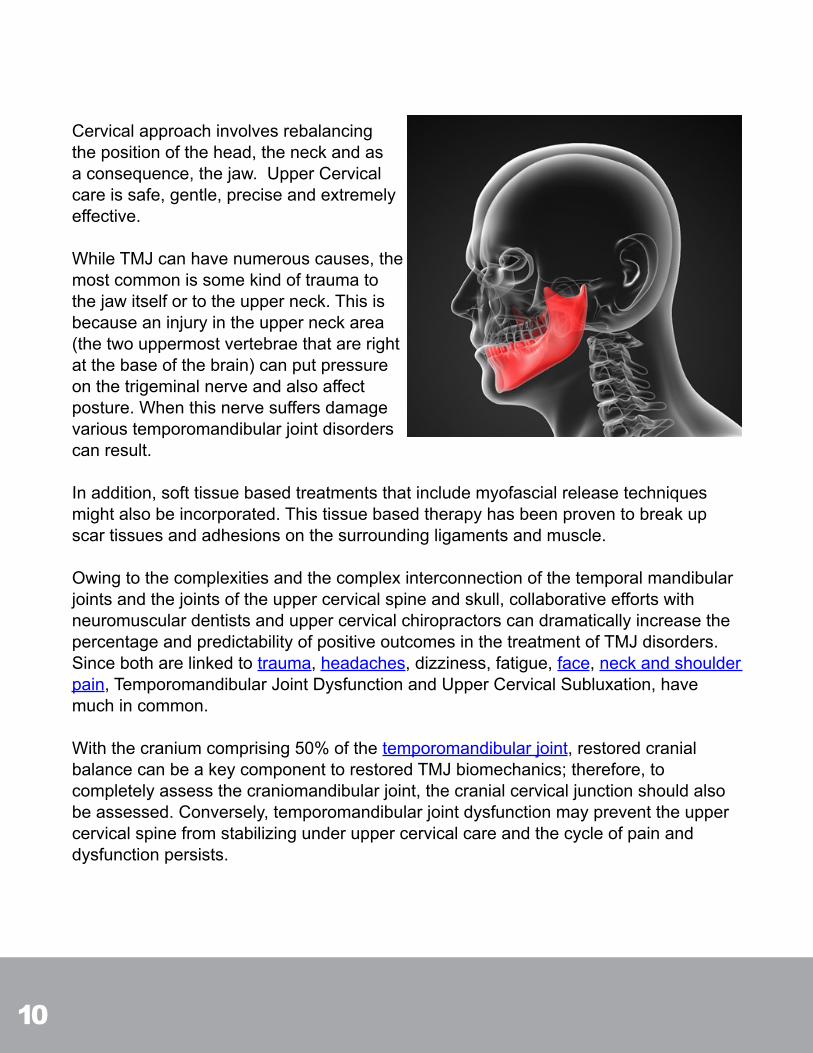
Cervicalapproachinvolvesrebalancingthepositionofthehead,theneckandasaconsequence,thejaw.UpperCervicalcareissafe,gentle,preciseandextremelyeffective.
WhileTMJcanhavenumerouscauses,themostcommonissomekindoftraumatothejawitselfortotheupperneck.Thisisbecauseaninjuryintheupperneckarea(thetwouppermostvertebraethatarerightatthebaseofthebrain)canputpressureonthetrigeminalnerveandalsoaffectposture.Whenthisnervesuffersdamagevarioustemporomandibularjointdisorderscanresult.
Inaddition,softtissuebasedtreatmentsthatincludemyofascialreleasetechniquesmightalsobeincorporated.Thistissuebasedtherapyhasbeenproventobreakupscartissuesandadhesionsonthesurroundingligamentsandmuscle.
Owingtothecomplexitiesandthecomplexinterconnectionofthetemporalmandibularjointsandthejointsoftheuppercervicalspineandskull,collaborativeeffortswithneuromusculardentistsanduppercervicalchiropractorscandramaticallyincreasethepercentageandpredictabilityofpositiveoutcomesinthetreatmentofTMJdisorders.Sincebotharelinkedtotrauma,headaches,dizziness,fatigue,face,neckandshoulderpain,TemporomandibularJointDysfunctionandUpperCervicalSubluxation,havemuchincommon.
Withthecraniumcomprising50%ofthetemporomandibularjoint,restoredcranialbalancecanbeakeycomponenttorestoredTMJbiomechanics;therefore,tocompletelyassessthecraniomandibularjoint,thecranialcervicaljunctionshouldalsobeassessed.Conversely,temporomandibularjointdysfunctionmaypreventtheuppercervicalspinefromstabilizingunderuppercervicalcareandthecycleofpainanddysfunctionpersists.
11
Evaluation
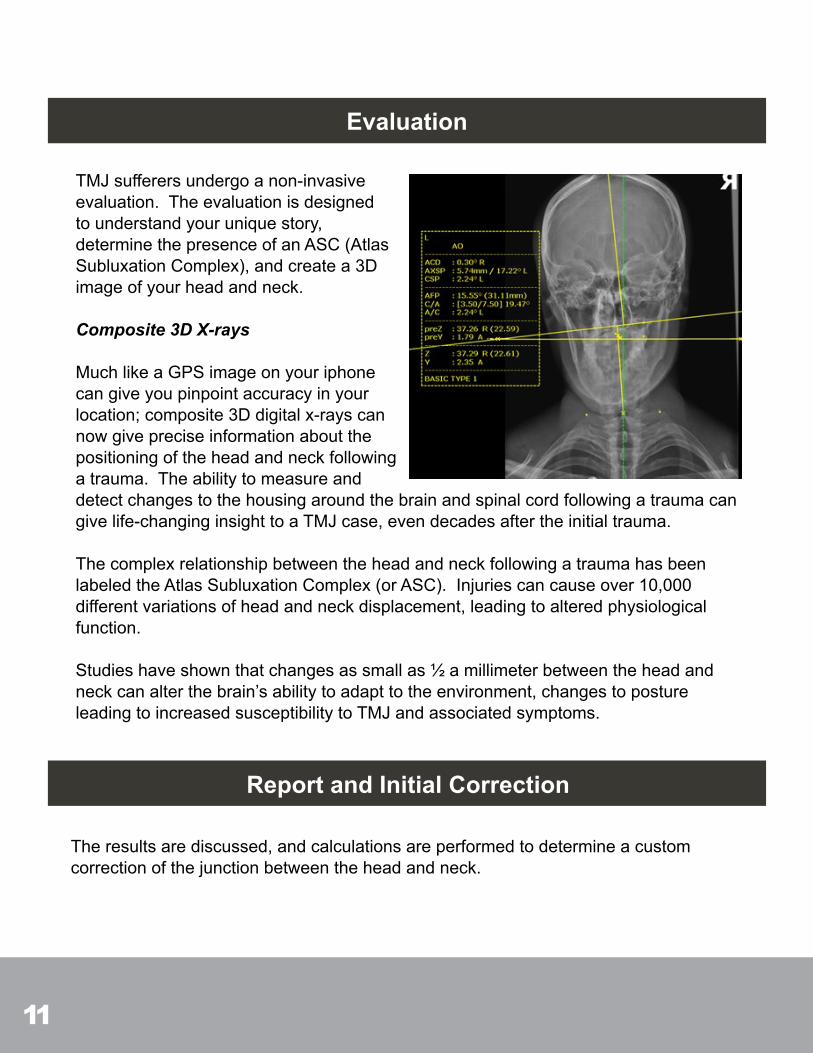
TMJsufferersundergoanon-invasiveevaluation.Theevaluationisdesignedtounderstandyouruniquestory,determinethepresenceofanASC(AtlasSubluxationComplex),andcreatea3Dimageofyourheadandneck.
Composite 3D X-rays
MuchlikeaGPSimageonyouriphonecangiveyoupinpointaccuracyinyourlocation;composite3Ddigitalx-rayscannowgivepreciseinformationaboutthepositioningoftheheadandneckfollowingatrauma.Theabilitytomeasureanddetectchangestothehousingaroundthebrainandspinalcordfollowingatraumacangivelife-changinginsighttoaTMJcase,evendecadesaftertheinitialtrauma.
ThecomplexrelationshipbetweentheheadandneckfollowingatraumahasbeenlabeledtheAtlasSubluxationComplex(orASC).Injuriescancauseover10,000differentvariationsofheadandneckdisplacement,leadingtoalteredphysiologicalfunction.
Studieshaveshownthatchangesassmallas½amillimeterbetweentheheadandneckcanalterthebrain’sabilitytoadapttotheenvironment,changestopostureleadingtoincreasedsusceptibilitytoTMJandassociatedsymptoms.
Report and Initial Correction
Theresultsarediscussed,andcalculationsareperformedtodetermineacustomcorrectionofthejunctionbetweentheheadandneck.

12
Follow-up
Thecorrectionisanextremelylightandgentleadjustmentthatfeelsmuchlikeadoctortakingsomeone’spulseonthesideoftheneck.Thecorrectionissogentle,itissafelyperformedoninfantsandbabies.
Composite3DX-raysareretakentoensureapropercorrectionhasbeenperformed.Theindividualoftendoesnotfeelachangeimmediatelyfollowingthefirstcorrection.
Theindividualoftenreturnsduringaninitial12-weekperiodtoassessforpropercorrection,monitortissuehealing,andmeasuretheprogressofthesymptoms.
Unlikedrugsandmedications,theuppercervicaltechniquedoesnottreatorsuppressthesymptomsassociatedwithTMJ.Theuppercervicalprocedureisdesignedtoimprovethebiomechanicsofthehousingaroundthebrainandspinalcord:theheadandneck.
Theimprovedbiomechanicsoftenimprovestheadaptabilityofthebrainandspinalcord,andindividualsoftenshowdramaticimprovementintheirsymptoms.
Wehaveseenover85%improvementinthefrequencyandseverityofTMJsymptomsthroughuppercervicalcare.TheclinicalsoworkswithintegrativeprofessionalsincludingNeuromuscularDentists,Neuroopthamologists,andCraniosacralTherapistsformorecomplicatedTMJcases.

13
CONCLUSIONTMJcanbeasourceofimmenseanxietyinyourlife.Itisextremelydifficulttolivewithpainorothersymptomseverytimeyoumoveyourjaw.AfterreadingthiseBook,youshouldbeabletodeterminepossibletriggersthatresultinaTMJdysfunction. Whileeliminatingtriggerscanbeimportantitismuchmoreimportanttoaddresstheunderlyingcauseofthecondition.Anuppercervicalcorrectiveprocedureisfocusedoncorrectingacommonunderlyingcauseoftemporomandibularjointdisorders.Whenproperpostureandalignmentisrestoredtothehead,neckandjawasaresultofanupperneckcorrectiveprocedure,manyofthetriggerswillceasetoaffectyou.
Thankyouforreadingthise-bookandifyouwouldliketospeakwithmepersonallyinmyCalgaryofficeaboutyourTMJcall407-578-2225orjustclickthebuttonbelow:
BeWell, Dr.JasonNitzsche ClinicDirector OrlandoSpineCenter http://www.gentlespinecare.com/ 407-578-2225

14
• Eriksen,Kirk.UpperCervicalSubluxationComplex–ACompleteReviewofChiropracticandMedicalLiterature.Philadelphia:Lippincott,WilliamsandWilkins,2004.Print.
• JournalofManipulativeandPhysiologicalTherapeutics2003Sep;26(7):421-5.• JournalofOrofacialPain2003summer;17(3):224-36.• FriedmanMH,WeisbergJ.Thecraniocervicalconnection:aretrospectiveanalysisof300whiplash
patientswithcervicalandtemporomandibulardisorders.Cranio2000Jul;18(3):163-7.• O’ShaughnessyT.Craniomandibular/temporomandibular/cervicalimplicationsofaforcedhyper-
extension/hyper-flexionepisode(ie,whiplash).FunctOrthod1994Mar-Apr;11(2):5-10,12.• McKayDC,ChristensenLV.Whiplashinjuriesofthetemporomandibularjointinmotorvehicle
accidents:speculationandfacts.JOralRehabil1998Oct;25(10):731-46.• KolbinsonDA,EpsteinJB,BurgessJA.Temporomandibulardisorders,headaches,andneckpain
aftermotorvehicleaccidents:apilotinvestigationofpersistenceandlitigationeffects.JProsthetDent1997Jan;77(1):46-53.
• GarciaRJr,ArringtonJA.Therelationshipbetweencervicalwhiplashandtemporomandibularjointinjuries:anMRIstudy.Cranio1996Jul;14(3):233-9.
• KronnE.TheincidenceofTMJdysfunctioninpatientswhohavesufferedacervicalwhiplashinjuryfollowingatrafficaccident.JOrofacPain1993Spring;7(2):209-13.
• PressmanBD,ShellockFG,SchamesJ.MRimagingoftemporomandibularjointabnormalitiesassociatedwithcervicalhyperextension/hyperflexion(whiplash)injuries.JMagnResonImaging1992Sep-Oct;2(5):569-74.
• EpsteinJB.Temporomandibulardisorders,facialpain,andheadachefollowingmotorvehicleaccidents.JCanDentAssoc1992Jun;58(6):488-9,493-5.
• BurgessJ.SymptomscharacteristicsinTMDpatientsreportingblunttraumaand/orwhiplashinjury.JCraniomandibDisord1991Fall;5(4):251-7.
• MannheimerJ,AttanasioR,CinottiWR.Cervicalstrainandmandibularwhiplash:effectsuponthecraniomandibularapparatus.ClinPrevDent1989Jan-Feb;11(1):29-32.
• TrosterL.Temporomandibulardisorders:culpritoraccompliceofthepost-traumaticmyofascialpaindysfunctionsyndrome?Aphysicaltherapist’sperspective.AlphaOmegan1998Oct;91(3):25-30.
• FerrariR,LeonardMS.Whiplashandtemporomandibulardisorders:acriticalreview.JAmDentAssoc1998Dec;129(12):1739-45.
• BergmanH,AnderssonF,IsbergA.Incidenceoftemporomandibularjointchangesafterwhiplashtrauma:aprospectivestudyusingMRimaging.AJRAmJRoentgenol1998Nov;171(5):1237-43.
• HowardRP,BowlesAP,GuzmanHM.Head,neck,andmandibledynamicsgeneratedbywhiplash.AccidAnalPrev1998Jul;30(4):525-34.
TMJ RELATED RESEARCH
15
• HowardRP,HatsellCP,GuzmanHM.Temporomandibularjointinjurypotentialimposedbythelow-velocityextension-flexionmaneuver.JOralMaxillofacSurg1995Mar;53(3):256-62;discussion263.
• ProbertTC,WiesenfeldD,ReadePC.Temporomandibularpaindysfunctiondisorderresultingfromroadtrafficaccidents-anAustralianstudy.IntJOralMaxillofacSurg1994Dec;23(6Pt1):338-41.
• LevandoskiRR.Mandibularwhiplash.PartII.Anextensionflexioninjuryofthetemporomandibularjoints.FunctOrthod1993Mar-Apr;10(2):45-51.
• BradyC,TaylorD,O’BrienM.Whiplashandtemporomandibularjointdysfunction.JIrDentAssoc1993;39(3):69-72.
• HeiseAP,LaskinDM,GervinAS.Incidenceoftemporomandibularjointsymptomsfollowingwhiplashinjury.JOralMaxillofacSurg1992Aug;50(8):825-8.
• KirkWSJr.WhiplashasabasisforTMJdysfunction.JOralMaxillofacSurg1992Apr;50(4):427-8.• CapursoU,PerilloL,FerroA.Cervicaltraumainthepathogenesisofcranio-cervico-mandibular
dysfunction.MinervaStomatol1992Jan-Feb;41(1-2):5-12.• BedruneB,JammetP,ChossegrosC.Temporomandibularjointpain-dysfunctionsyndromeafter
whiplashinjury.Medico-legalproblemsincommonlaw.RevStomatolChirMaxillofac1992;93(6):408-13.
• WeinbergS,LapointeH.Cervicalextension-flexioninjury(whiplash)andinternalderangementofthetemporomandibularjoint.JOralMaxillofacSurg1987Aug;45(8):653-6.
• MosesAJ,SkoogGS.CervicalwhiplashandTMJ.BasalFacts1986;8(2):61-3.• ErnestEA3rd.TheorthopedicinfluenceoftheTMHapparatusinwhiplash:reportofacase.GenDent
1979Mar-Apr;27(2):62-4.• RoydhouseRH.Whiplashandtemporomandibulardysfunction.Lancet1973Jun16;1(7816):1394-5.• Neckpainanddisabilityoutcomesfollowingchiropracticuppercervicalcare:aretrospectivecase
series.RochesterRP.JCanChiroprAssoc.2009ug;53(3):173-85.http://www.ncbi.nlm.nih.gov/pubmed/19714232