Natural History of Thyroid Nodule
31
Natural History of Thyroid Nodule Xiaohong Wu Department of Endocrinology, First Affiliated Hospital, Nanjing Medical University, Nanjing, China
-
Upload
marcellus-alston -
Category
Documents
-
view
48 -
download
5
description
Natural History of Thyroid Nodule. Xiaohong Wu Department of Endocrinology, First Affiliated Hospital, Nanjing Medical University, Nanjing, China. Thyroid Nodules: the scope of the problem. Palpation: 3% ~ 7% Ultrasonography: 20% ~76% More common in: - PowerPoint PPT Presentation
Transcript of Natural History of Thyroid Nodule

Natural History of Thyroid Nodule
Xiaohong Wu Department of Endocrinology, First Affiliated Hospital,
Nanjing Medical University, Nanjing, China

Thyroid Nodules: the scope of the problem
• Palpation: 3% ~ 7%• Ultrasonography: 20% ~76%• More common in:
elderly persons;
women;
those with iodine deficiency;
those with a history of radiation
exposure.
Endocr Pract. 2010;16(Suppl 1)

Prevalence of Thyroid Incidentalomas in health check-up
ages(year) male/female male(%) female (%) total (%)
10 ~ 22/14 9.1 7.1 8.3
30 ~ 69/61 17.4 23.0 20.0
50 ~ 86/59 39.51) 52.53) 44.82)
≥70 19/10 73.71) 60.03) 69.02)
total 196/144 31.6 36.1 33.5
Note: compared with other ages, 1) P < 0.01, 2) P <0.05, compared with group A、 B, 3) P < 0.05
Wu X, Liu C, et al. Chinese Journal of Practical Internal Medicine, 2005; 25(9):823-824

Prevalence of Thyroid Nodules in Jiangsu Province
ages (year) male female
sample size
cases prevalence sample size
cases prevalence
20-29 242 12 4.96 273 23 8.42
30-39 386 30 7.77 716 109 15.22
40-49 567 63 11.11 1056 196 18.56
50-59 617 105 17.02 1061 328 30.91
60- 552 134 24.28 658 294 44.68
total 2364 344 14.55 3764 950 25.24
Feng C, Liu C, et al. Chinese Journal of Endocrinology and Metabolism. 2011, 27: 492-494
In China, according to a recent community survey in ten cities, thyroid nodules have a prevalence of approximately 18.6%.

Etiology of Thyroid Nodules
Endocr Rev. 2003;24(1):102-32.

Endocr Pract. 2010;16(Suppl 1)

Pat. P.M. Nodular Volume After 6 Years3.1 ml 4.3 ml
6.3 ml

Course of Thyroid Nodules
• What is the long-term course of thyroid nodules?
• What influences growth and function of thyroid nodules?
Questions

Long-Term Follow-up of Thyroid Nodule Growth
109 euthyroid patients with benign thyroid nodules95 women, 14 men; 46,2 ± 12,7 (14 - 73) years
Follow-up of at least 3 years3 - 13 years (median 4,9 years)
Quadbeck B, et al. Exp Clin Endocrinol Diabetes. 2002;110:348-354

Development of Thyroid Nodules
Quadbeck B, et al. Exp Clin Endocrinol Diabetes. 2002;110:348-354

Evaluation of Factors affecting Thyroid Nodules Growth
Quadbeck B, et al. Exp Clin Endocrinol Diabetes. 2002;110:348-354

Evaluation of Factors affecting Thyroid Nodules Growth
Quadbeck B, et al. Exp Clin Endocrinol Diabetes. 2002;110:348-354

Determinants of Nodular Growth
According to the Cox Proportional Harzards Model
There was no significant influence on the growth pattern of thyroid nodules of:
– Age and sex of the patient,– Initial size of the nodule, – Scintigraphic behaviour of the nodule,– TSH-suppression by therapy
Quadbeck B, et al. Exp Clin Endocrinol Diabetes. 2002;110:348-354

Conclusions• The majority of benign thyroid nodules exhibits a slow
growth rate during long-term observation.– After 3 yeras only half of the nodules have significantly increased
in size.
• Thyroid nodules do grow more rapidly than the whole goitre of the same patient.
• The growth rate of thyroid nodules is mainly determined endogeneously rather than by exogenous factors, which show little, if any, infleunce.
Quadbeck B, et al. Exp Clin Endocrinol Diabetes. 2002;110:348-354

How about Thyroid Incidentalomas
Health check-up
Thyroid ultrasonography
Incidentalomas
Clinical evaluation
d>1cm, US-FNA
FT3,FT4,TSH,Tg,Nodule volumes Follow-up
n=323, M/F=196/144
n=144,M/F=62/52
Wu X, Liu C, et al. Chinese Journal of Practical Internal Medicine,2005;25(9):823-824

Four-year Follow-up of Thyroid Incidentalomas
10
36
4014
25
0 10 20 30 40 (%)
di sappeared
decreased
unchanged
i ncreased
Sol i tary tomul ti pl e
Wu X, Liu C, et al. Chinese Journal of Practical Internal Medicine,2005;25(9):823-824

Changes of Thyroid Incidentalomas after Four-year Follow-up
- 1
- 0. 53
- 0. 05
0. 29
- 1
- 0. 8
- 0. 6
- 0. 4
- 0. 2
0
0. 2
0. 4
nodule volume
di sappeared decreased unchanged i ncreased
Wu X, Liu C, et al. Chinese Journal of Practical Internal Medicine,2005;25(9):823-824

Characteristics of 20 included publicationsStudyname Publication year Study design Follow-up Nodule n Criteria of change Change of nodules at endpoint
(percentage change)
Increase No change DecreaseCheung 1989 Cohort 1.5ys 37 NA 19 - -Kuma 1994 Cohort 15ys 134 Not defined 13.5 33.6 52.9
Knudsen 2000 Cohort 2ys 45 Nodule diameter≥ 5mm
2.2 91.1 6.7
Buadbeck 2000 Cohort 5ys 57 Not defined 35 31 24Rago 2001 Cohort 3ys 27 Nodule volume≥30% 11.1 - -
Quadbeck 2002 Cohort 3ys 139 Nodule volume≥30% 61.2 15.8 23
Alexander 2003 Cohort 20m 330 Nodule volume≥15% 39 - -
Wu 2005 Cohort 4ys 100 Nodule volume≥20% 14 40 46
Murat 2006 Cohort 39m 531 Nodule volume≥15% 32 34.9 33.1
Gharib 1987 Case-control 0.5y 25 Failure of any reduction
40 60
Reverter 1992 Case-control 1y 20 Nodule is not reduced or reduced to
50%
85 15
Papini 1993 Case-control 1y 50 Failure of any reduction
74 26
La Rosa 1995 Case-control 1y 22 Nodule is not reduced or reduced to
50%
100 0
Mainini 1995 Case-control 2ys 10 Nodule is not reduced or reduced to
50%
100 0
Lima 1997 Case-control 1y 20 Nodule is not reduced or reduced to
20%
80 20
Papini 1998 Case-control 5ys 41 Nodule is not reduced or reduced to
11.7%
53.7 46.3
Zelmanovitz 1998 Case-control 1y 24 Nodule is not reduced or reduced to
50%
91.7 8.3
Larijani 1999 Case-control 1y 30 Failure of any reduction
60 40
Sakalauskiene 2002 Case-control 0.5y 25 Failure of any reduction
84 16
Wemeau 2002 Case-control 1.5ys 59 Nodule is not reduced or reduced to
20%
69.5 30.5

Forest plot of 9 studies providing the percentage of volume increase for benign thyroid nodules
NOTE: Weights are from random effects analysis
Overall (I-squared = 96.9%, p = 0.000)
Wu 2005
ID
Kuma 1994
Quadbeck 2002
Alexander 2003
Buadbeck 2000
Rago 2001
Knudsen 2000
Cheung 1989
Murat 2006
Study
25.21 (13.12, 37.31)
14.00 (7.20, 20.80)
percentage (95% CI)
13.50 (7.71, 19.29)
61.20 (53.10, 69.30)
39.00 (33.74, 44.26)
35.00 (22.62, 47.38)
11.10 (-0.75, 22.95)
2.20 (-2.09, 6.49)
19.00 (6.36, 31.64)
32.00 (28.03, 35.97)
100.00
11.32
Weight
11.44
11.16
11.49
10.46
10.55
11.57
10.41
11.60
%
25.21 (13.12, 37.31)
14.00 (7.20, 20.80)
percentage (95% CI)
13.50 (7.71, 19.29)
61.20 (53.10, 69.30)
39.00 (33.74, 44.26)
35.00 (22.62, 47.38)
11.10 (-0.75, 22.95)
2.20 (-2.09, 6.49)
19.00 (6.36, 31.64)
32.00 (28.03, 35.97)
100.00
11.32
Weight
11.44
11.16
11.49
10.46
10.55
11.57
10.41
11.60
%
0-69.3 0 69.3

Forest plot of 6 studies providing rate of no-change of the volume for benign thyroid nodules
NOTE: Weights are from random effects analysis
Overall (I-squared = 97.6%, p = 0.000)
Knudsen 2000
Murat 2006
Kuma 1994
Quadbeck 2002
Buadbeck 2000
ID
Wu 2005
Study
41.03 (22.01, 60.06)
91.10 (82.78, 99.42)
34.90 (30.85, 38.95)
33.60 (25.60, 41.60)
15.80 (9.74, 21.86)
31.00 (18.99, 43.01)
percentage (95% CI)
40.00 (30.40, 49.60)
100.00
16.67
17.09
16.71
16.92
16.11
Weight
16.50
%
41.03 (22.01, 60.06)
91.10 (82.78, 99.42)
34.90 (30.85, 38.95)
33.60 (25.60, 41.60)
15.80 (9.74, 21.86)
31.00 (18.99, 43.01)
percentage (95% CI)
40.00 (30.40, 49.60)
100.00
16.67
17.09
16.71
16.92
16.11
Weight
16.50
%
0-99.4 0 99.4

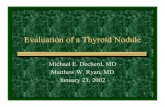
Forest plot of 17 publications providing rate of volume decrease for benign thyroid nodules
NOTE: Weights are from random effects analysis
Overall (I-squared = 97.4%, p = 0.000)
Lima 1997
Larijani 1999
Quadbeck 2002
Buadbeck 2000
Zelmanovitz 1998
Wu 2005
Sakalauskiene 2002
Mainini 1995
Reverter 1992
La Rosa 1995
Papini 1998
Wemeau 2002
Knudsen 2000
ID
Papini 1993
Gharib 1987
Murat 2006
Kuma 1994
Study
25.58 (17.57, 33.60)
20.00 (2.47, 37.53)
40.00 (22.47, 57.53)
23.00 (16.00, 30.00)
24.00 (12.91, 35.09)
8.30 (-2.74, 19.34)
46.00 (36.23, 55.77)
16.00 (1.63, 30.37)
0.10 (-1.86, 2.06)
15.00 (-0.65, 30.65)
0.10 (-1.22, 1.42)
46.30 (31.04, 61.56)
30.50 (18.75, 42.25)
6.70 (-0.60, 14.00)
percentage (95% CI)
26.00 (13.84, 38.16)
60.00 (40.80, 79.20)
33.10 (29.10, 37.10)
52.90 (44.45, 61.35)
100.00
5.08
5.08
6.39
5.95
5.96
6.11
5.52
6.69
5.35
6.70
5.40
5.87
6.36
Weight
5.82
4.85
6.61
6.25
%
25.58 (17.57, 33.60)
20.00 (2.47, 37.53)
40.00 (22.47, 57.53)
23.00 (16.00, 30.00)
24.00 (12.91, 35.09)
8.30 (-2.74, 19.34)
46.00 (36.23, 55.77)
16.00 (1.63, 30.37)
0.10 (-1.86, 2.06)
15.00 (-0.65, 30.65)
0.10 (-1.22, 1.42)
46.30 (31.04, 61.56)
30.50 (18.75, 42.25)
6.70 (-0.60, 14.00)
percentage (95% CI)
26.00 (13.84, 38.16)
60.00 (40.80, 79.20)
33.10 (29.10, 37.10)
52.90 (44.45, 61.35)
100.00
5.08
5.08
6.39
5.95
5.96
6.11
5.52
6.69
5.35
6.70
5.40
5.87
6.36
Weight
5.82
4.85
6.61
6.25
%
0-79.2 0 79.2

How about nodular goiter?• On the basis of cross-sectional data and ultrasonic scanning,
an average annual growth rate of 4.5% in multinodular goiter has been reported---Am J Med 1990;89:602–608
• In the Whickham survey, 20% of the women and 5% of the men who had goiters in the initial survey had no goiter in the follow-up survey, whereas only 4% of the women and none of the men acquired a goiter between the two surveys.
---Clin Endocrinol (Oxf) 1995;43:55–68
• In a 20-yr follow-up study of 11- to 18-yr-old subjects in the southwestern United States, 60% of the 92 subjects who had diffuse goiters initially had spontaneous regression by the age of 30 yr. ---Am J Med 1991;91:363–370

Decreasing frequency of goiter with age
• A fall in lean body mass with age, known to be related to thyroid volume
• A fall with age in IGF-I and GH
• At least in women, the loss of estradiol-mediated increase in proliferation and down-regulation of the NIS gene
Clin Endocrinol (Oxf) 1998;48:701–706J Am Geriatr Soc 1999;47:1238–1243Endocrinology 1999;140:5705–5711

Follow-up of Nontoxic AutonomouslyFunctioning Thyroid Nodules
J Clin Endocrinol Metab 1980;50:1089–1093

Correlation of change in nodule size and function and duration of follow up for nontoxic AFTN
J Clin Endocrinol Metab 1980;50:1089–1093
Increase: 15/159=9.4%No change: 138/159=86.8%
Decrease: 6/159=3.8%
Toxic: 14/159=8.8%

Correlation of function of untreated AFTN with age after varying follow-up periods
J Clin Endocrinol Metab 1980;50:1089–1093
Nodules greater than 3 cm in size at diagnosis carried a 20% risk of developing hyperthyroidism, whereas nodules less than 2.5 cm in size had only a 2-5% risk of developing hyperthyroidism within the same time frame

Correlation of changes in nodule size and function andduration of follow up for nontoxic AFTN from iodine-sufficient
(control) and iodine-deficient (endemic) areas
J Clin Endocrinol Metab 1983;56:283–287

Nontoxic Nodular Goiter
• An incidence of 8-10% of overt hyperthyroidism during a 6- to 12-yr follow-up period corresponding to 0-6% per year. .
• In part, this progression depends on genetic predisposition, somatic mutations in individual nodules, and extrinsic factors such as iodine intake.
Postgrad Med J 1990;66:186–190Clin Nucl Med 1979;4:181–190
J Clin Endocrinol Metab 1980;50:1089–1093J Clin Endocrinol Metab 1983;56:283–287
Acta Endocrinol (Copenh) 1993;128:51–55

• The natural history of thyroid nodule with respect to
growth and function varies and is difficult to predict
in a given patient.
• Most patients need no treatment after malignancy is
ruled out.
• New molecular genetic techniques applied on FNAB
should lead to an increasing understanding of the
pathogenesis of nodular thyroid disease and a better
characterization of phenotypes.
Summary

Acknowledgements
Yingyue Lv
Yili Xu
Xiaojing Wang
Jiayu Zhu
Xiaoyun Liu
Huanhuan Chen
Kuangfeng Xu
Tao Yang
Collaborators:
Yu Duan
Xinhua Ye
Hongjun Lin
Meiping Shen
Wei Liu
Supervisor:
Chao LiuGrants: NSFC(30971404/C140406 and 81070621/H0704) Jiangsu Province key medical personnel project (RC2011068) International Science and technology cooperation (BZ2011042)

Thank you!