
National Treatment Guidelines for Malaria in …...including coma (Glasgow coma scale < 11, Blantyre...
56
National Treatment Guidelines for Malaria in Cambodia December 2014 Kingdom of Cambodia Nation Religion King
Transcript of National Treatment Guidelines for Malaria in …...including coma (Glasgow coma scale < 11, Blantyre...

National Treatment Guidelines
for Malaria in CambodiaDecember 2014
Kingdom of CambodiaNation Religion King


National Treatment Guidelines for Malaria in Cambodia i
1. PREFACE
Malaria, which has plagued humankind since ancient times, continues to be one of the most important and devastating infectious diseases in the world. Half of the world’s population, roughly 3.4 billion people, living in 104 countries are at risk of contracting the disease, with an estimated 207 million cases and 627,000 malaria deaths in 2012 (World Malaria Report, 2013). In Cambodia, despite the limited areas of the country where transmission occurs, an estimated 8.6 million people live in malaria endemic areas. In the past few years, we have made remarkable strides in controlling malaria. The number of recorded malaria deaths dropped from 93 in 2011 to 45 in 2012 and further to only 12 in 2013. Similarly the total number of malaria cases dropped from 62,690 in 2012 to 45,533 in 2013. However, Cambodia’s gains in malaria control are threatened by the emergence and spread of artemisinin resistance, originally detected along the Thai-Cambodia border. Reduced efficacy of artemisinin combination therapies (ACTs) has now been documented in several additional provinces. To successfully implement the National Strategic Plan for Elimination of Malaria (NSPEM) by 2025 supported and approved by Samdech Akak Moha Sena Badei Techo HUN SEN, Prime Minister of Cambodia, it is imperative that every malaria control intervention be implemented with the highest degree of coverage and quality. Selection and spread of drug resistant malaria strains will occur more rapidly with inappropriate treatment regimens, inadequate patient adherence, and use of substandard quality pharmaceuticals. Accordingly, the Ministry of Health (MOH) is publishing this revised version of the National Treatment Guidelines for Malaria, incorporating updated information presented at National Malaria Drug Policy meetings held in December 2013 and January 2014. These meetings gathered experts and key stakeholders from the Ministry of Health, WHO, academic and international partners to consider the latest malaria surveillance and research findings including Therapeutic Efficacy Studies (TES) to refine and improve existing treatment guidelines.
These guidelines are designed for doctors and staff at each level of the public health framework (referral hospital, health center and health post), the military, police, and private sectors as well as community level workers to provide uniform and quality malaria case management. The goals espoused in these guidelines are threefold. First, the MOH seeks to further aggressively reduce malaria morbidity and mortality as it approaches malaria

ii National Treatment Guidelines for Malaria in Cambodia
pre-elimination. Second, by optimizing drug regimens and extending case management to follow up with patients in high risk areas to ensure successful cure, we aim to reduce the impact of resistant malaria strains and preserve our current arsenal of malaria treatments. Third, more comprehensive diagnostic testing is encouraged to accurately diagnose and treat a larger proportion of malaria cases. Achieving the triple aims of “Test, Treat, and Track” is critical as we execute Cambodia’s National Malaria Elimination Strategy.
In the 2014 version of the Malaria National Treatment Guidelines, the Ministry of Health now recommends the following changes to the existing national treatment guidelines:
• Substitution of artesunate-mefloquine for selected provinces where DHA-piperaquine is currently used and failing to achieve acceptable cure rates. • Replacing co-blistered artesunate-mefloquine previously used in Cambodia with a fixed dose combination (FDC). • Prioritize directly observed therapy (DOT) and documentation of cure as an essential part of case management.• Enhancing timely surveillance to inform drug treatment policy.• Reducing primaquine dosing to block P. falciparum malaria transmission to be consistent with the 2012 WHO guidelines on transmission and amending P. vivax radical cure.
The main aim of this publication is to provide all those involved in the management of malaria in different sectors and levels with clear and practical guidelines for the early diagnosis and prompt and appropriate treatment of malaria.
The Ministry of Health would like to recognize for strong effort being made by National Center for Parasitology Entomology and Malaria Control (CNM) and to thank President’s Malaria Initiative (PMI), WHO and other stakeholders for their assistance in updating this new edition.
National Treatment Guidelines for Malaria in Cambodia iii
2. GOALS AND OBJECTIVES OF THE NATIONAL MALARIA CONTROL PROGRAMME
Goal: To move towards pre-elimination of malaria across Cambodia with special efforts to contain artemisinin resistant P.falciparum malaria.
Objectives: 1. To improve access to early malaria diagnosis and treatment services. 2. To decrease drug pressure for selection of artemisinin resistant malaria parasites.3. To improve access to preventive measures and specifically prevent transmission of artemisinin resistant malaria parasites.4. To increase community awareness and behavior change among the population at risk. 5. To provide effective management (including information systems and surveillance) and coordination.
Broad Aims of Malaria Case ManagementTo cure infection and reduce morbidity and mortalityTo reduce the infectious reservoir
Specific Objectives of Malaria Case ManagementEarly detection and prompt effective treatment to cure the infection and prevent
progression to severe disease Proper management of severe disease to prevent deathPrevent drug resistance Reduce malaria transmission
Components of Malaria Case Management▪ Prompt parasitological diagnosis ▪ Treatment with effective drugs▪ Referral (and pre-referral treatment when indicated) ▪ Counseling and Follow up of patient▪ Issues related to diagnosis: policy and quality assurance▪ Drugs: supply and management; safety (pharmacovigilance), quality (regulation
issues) and therapeutic efficacy

iv National Treatment Guidelines for Malaria in Cambodia
3. TABLE OF CONTENTS
1 PREFACE ............................................................................................................. i
2 GOALS AND OBJECTIVES OF THE NATIONAL MALARIA ........... CONTROL PROGRAMME ........................................................................... iii
3 TABLE OF CONTENTS ................................................................................ iv
4 ABBREVIATIONS AND ACRONYMS ....................................................viii
5 GLOSSARY ........................................................................................................ ix
6 INTRODUCTION.............................................................................................1
7 COMPARISON BETWEEN 2012 and 2014 CAMBODIA NATIONAL MALARIA TREATMENT GUIDELINES ..................................................1
7.1 Recommendations changed from the 2012 Cambodia National Treatment Guidelines .............................................................................................................1
7.2 Recommendations unchanged from the 2012 Cambodia National Malaria Treatment Guidelines ..........................................................................................2
8 EVALUATION OF PATIENTS WITH POSSIBLE MALARIA .............. 3
8.1 Taking a patient history ......................................................................................3
8.2 Malaria Diagnosis: When to perform a diagnostic test? ................................ 4
8.3 Malaria diagnosis: rapid diagnostic tests vs. microscopy ............................... 5
8.4 Evaluating for uncomplicated vs. severe malaria ............................................6
9 REFERRAL OF MALARIA PATIENTS ......................................................9
9.1 Rectal artesunate pre-referral treatment for severe malaria .......................... 9
10 TREATMENT OF UNCOMPLICATED MALARIA ..............................11
10.1 Principles .............................................................................................................11
10.2 First Line Treatment for Uncomplicated P. falciparum, vivax, ovale and ... malariae species ..................................................................................................11
10.3 DHA+PPQ dosing ...........................................................................................12
10.4 Artesunate + mefloquine FDC dosing ..........................................................13
10.5 Mefloquine adverse effects and contraindications .......................................13
10.6 Second-line treatment for uncomplicated P. falciparum malaria ...............14
10.7 Use of Malarone® in Cambodia for use in special situations ....................15

National Treatment Guidelines for Malaria in Cambodia v
10.8 Additional considerations for treating uncomplicated malaria ...................15
10.9 Drug resistance, treatment failures, and strategies to reduce transmission of resistant parasites ...............................................................................................16
10.10 How to manage potential treatment failure ...................................................17
10.11 Follow up of uncomplicated P. Falciparum malaria ....................................18
10.12 Primaquine indications .....................................................................................18
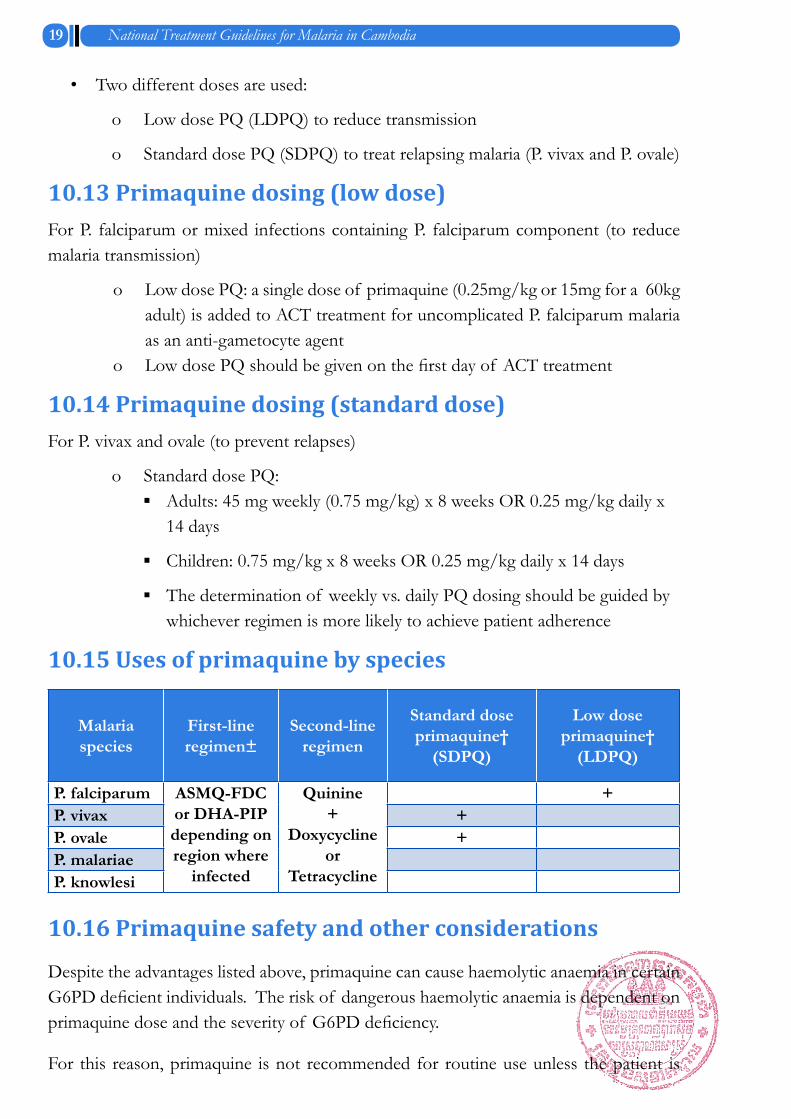
10.13 Primaquine dosing (low dose) .........................................................................19
10.14 Primaquine dosing (standard dose) .................................................................19
10.15 Uses of primaquine by species ........................................................................19
10.16 Primaquine safety and other considerations..................................................19
11 TREATMENT OF UNCOMPLICATED MALARIA IN INFANTS ...... AND CHILDREN ...........................................................................................20
12 TREATMENT OF UNCOMPLICATED MALARIA IN PREGNANT WOMEN ............................................................................................................21
12.1 First line treatment ............................................................................................21
12.2 Lactating women ...............................................................................................22
13 TREATMENT OF SEVERE MALARIA ...................................................22
13.1 Treatment objectives .........................................................................................22
13.2 Clinical assessment ............................................................................................22
13.3 Differential diagnosis of severe malaria .........................................................23
13.4 Urgent initial treatment steps ..........................................................................23
13.5 First line treatment of severe malaria in adults and children .....................23
13.6 Preparation of artesunate for IV or IM administration ..............................24
13.7 Alternative first line treatment: IM artemether .............................................24
13.8 Recommended dosing for IM artemether in adults and children ..............28
13.9 Second line treatment for severe malaria .......................................................28
13.10 Pre-referral treatment for severe malaria with rectal artesunate ................30
13.11 Dosing of pre-referral AS suppositories .......................................................30
13.12 General management of severe malaria .........................................................30
14 Clinical and adjunctive treatment for severe malaria ...................................32
14.1 Parasitological monitoring in severe malaria .................................................33

vi National Treatment Guidelines for Malaria in Cambodia
14.2 Treatment of severe malaria in pregnant women .........................................33
15 MALARIA DIAGNOSIS AND TREATMENT IN COMMUNITY ....... (VMW/MMW) AND PRIVATE SECTOR .................................................34
15.1 Village Malaria Worker (VMW)/Mobile Malaria Worker (MMW) ............34
15.2 PRIVATE SECTOR .........................................................................................35
16 DIRECLY OBSERVED THERAPY (DOT) ..............................................35
17 QUALITY OF ANTIMALARIAL MEDICINES ......................................36
18 SCREENING OF PREGNANT WOMEN ...............................................36
19 CHEMOPROPHYLAXIS ...............................................................................36
20 REFERENCES .................................................................................................37
21 Annex A ..............................................................................................................38

National Treatment Guidelines for Malaria in Cambodia vii
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Odd
ar
Mea
nche
y20
1359
452
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Snou
l (K
ratie
)20
1196
4
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Paili
n20
1076
294
2009
9238
4
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Prea
h V
ihea
r20
1383
655
2011
974
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Rata
naki
ri20
1397
635
2010
100
4
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Batta
mba
ng20
1269
403
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Kam
pong
T
hom
2012
100
604
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Purs
at20
1355
955
2012
9124
420
1183
423
Loca
tion
Year
Cur
e ra
te
DP
(%)
NRe
f
Kam
pong
Sp
eu20
1210
022
420
1089
2
Not
es (R
ef.)
1.
Not
PC
R co
rrec
ted
2.
Lon
C., e
t a l
ASM
TH a
bstra
ct 1
3-L-
B-36
64, p
rese
nted
at N
ovem
ber 2
013
ASM
TH, W
ash
DC.
AC
P R
59%
bas
ed o
n IT
T an
alys
is3.
Le
ang
R, E
ffica
cy o
f D
HA
-PIP
for t
he tr
eatm
ent o
f U
ncom
plic
ated
PF
Mal
aria
in C
ambo
dia,
2012
4.
WH
O/C
NM
5.
Fairh
urst
, US
NIH
, unp
ublis
hed
data
6.
Mal
aria
J. 2
013
Sep
23;1
2:34
3
DH
A-p
iper
aqui
ne c
ure
rate
s by
pro
vinc
es in
Cam
bodi
a
viii National Treatment Guidelines for Malaria in Cambodia
4. ABBREVIATIONS AND ACRONYMS
ACT Artemisinin-based Combination TherapyAS ArtesunateAS+MQ FDC Artesunate plus Mefloquine Fixed-Dose CombinationBW Body WeightCNM National Center for Parasitology, Entomology and Malaria ControlCQ ChloroquineDHA+PPQ Dihydroartemisinin plus Piperaquine FDH Former District HospitalG6PD Glucose-6-Phosphate DehydrogenaseHC Health CenterHP Health PostHRP2 Histidine-Rich Protein 2IC50 Concentration Providing 50% InhibitionIV IntravenousIM IntramuscularMIC Minimum Inhibitory ConcentrationMMW Mobile Malaria WorkerMQ MefloquineOD Operational DistrictPCR Polymerase Chain ReactionPMI President’s Malaria InitiativePQ PrimaquineRCT Randomized Controlled TrialRDT Rapid Diagnostic TestRH Referral HospitalVMW Village Malaria WorkerWHO World Health Organizationdl Deciliterh Hourµl Microliterkg Kilogrammg Milligramml Millilitermmol Milimolmm Hg Millimeter of mercury

National Treatment Guidelines for Malaria in Cambodia ix
5. GLOSSARY
Artemisinin-based Combination Therapy (ACT): A combination of artemisinin or one of its derivatives with an antimalarial or antimalarials of a different class.
Asexual cycle: The life-cycle of the malaria parasite in host from merozoite invasion of red blood cells to schizont rupture (merozoite→ ring stage → trophozoite→ schizont→ merozoites). Duration approximately 48 h in Plasmodium falciparum, P. ovale and P. vivax; 72 h in P. malariae.
Asexual parasitemia: The presence in host red blood cells of asexual parasites. The level of asexual parasitemia can be expressed in several different ways: the percentage of infected red blood cells, the number of infected cells per unit volume of blood, the number of parasites seen in one microscopic field in a high-power examination of a thick blood film, or the number of parasites seen per 200–1000 white blood cells in a high power examination of a thick blood film.
Cerebral malaria: Severe P. falciparum malaria with cerebral manifestations, usually including coma (Glasgow coma scale < 11, Blantyre coma scale < 3). Malaria with coma persisting for > 30 min after a seizure is considered to be cerebral malaria.
Combination treatment (CT): A combination of two or more different classes of antimalarial medicines with unrelated mechanisms of action.
Cure: Elimination of the symptoms and asexual blood stages of the malaria parasite that caused the patient or caregiver to seek treatment.
Drug resistance: The World Health Organization (WHO) defines resistance to antimalarials as the ability of a parasite strain to survive and/or to multiply despite the administration and absorption of a medicine given in doses equal to or higher than those usually recommended but within the tolerance of the subject, provided drug exposure at the site of action is adequate. Resistance to antimalarials arises because of the selection of parasites with genetic mutations or gene amplifications that confer reduced susceptibility.
Gametocytes: Sexual stages of malaria parasites present in the host red blood cells.
Hypnozoites: Persistent liver stages of P. vivax and P. ovale malaria that remain dormant in host hepatocytes for an interval (most often 3–45 weeks) before maturing to

x National Treatment Guidelines for Malaria in Cambodia
hepatic schizonts. These then burst and release merozoites, which infect red blood cells. Hypnozoites are the source of relapses.
Mass drug administration (MDA): The practice of treating a whole population within a given geographical area, irrespective of the presence of symptoms and withoutdiagnostic testing.
Monotherapy: Antimalarial treatment with a single medicine (either a single active compound or a synergistic combination of two compounds with related mechanism of action).
Plasmodium: A genus of protozoan vertebrate blood parasites that includes the causal agents of malaria. Plasmodium falciparum, P. malariae, P. ovale and P. vivax cause malaria in humans. Human infections with the monkey malaria parasite, P. knowlesi have also been reported from forested regions of South-East Asia.
Pre-erythrocytic development: The life-cycle of the malaria parasite when it first enters the host. Following inoculation into a human by the female anopheline mosquito, sporozoites invade parenchyma cells in the host liver and multiply within the hepatocytes for 5–12 days, forming hepatic schizonts. These then burst liberating merozoites into the bloodstream, which subsequently invade red blood cells.
Radical cure: In P. vivax and P. ovale infections only, this comprises a cure as defined above plus prevention of relapses by killing hypnozoites.
Rapid diagnostic test (RDT): An antigen-based stick, cassette or card test for malaria in which a coloured line indicates that plasmodial antigens have been detected.
Recrudescence: The recurrence of asexual parasitemia after treatment of the infection with the same infection that caused the original illness. This results from incomplete clearance of parasitemia due to inadequate or ineffective treatment. It is, therefore, different to a relapse in P. vivax and P. ovale infections, and it differs from a new infection or re-infection (as identified by molecular genotyping in endemic areas).
Recurrence: The recurrence of asexual parasitemia following treatment. This can be caused by a recrudescence, a relapse (in P. vivax and P. ovale infections only) or a new infection.
Relapse: The recurrence of asexual parasitemia in P. vivax and P. ovale malaria deriving

National Treatment Guidelines for Malaria in Cambodia xi
from persisting liver stages. Relapse occurs when the blood stage infection has been eliminated but hypnozoites persist in the liver and mature to form hepatic schizonts. After variable intervals of weeks to months, the hepatic schizonts burst and liberate merozoites into the bloodstream.
Ring stage: Young usually ring-shaped intra-erythrocytic malaria parasites, before malaria pigment is evident under microscopy.
Schizonts: Mature malaria parasites in host liver cells (hepatic schizonts) or red blood cells (erythrocytic schizonts) that are undergoing nuclear division. This process is called schizogony.
Selection pressure: Resistance to antimalarials emerges and spreads because of the selective survival advantage that resistant parasites have in the presence of antimalarials to which they are resistant. Selection pressure describes the intensity and magnitude of the selection process; the greater the proportion of parasites in a given parasite population exposed to concentrations of an antimalarial that allows proliferation of resistant, but not sensitive parasites, the greater the selection pressure.
Severe anemia: Haemoglobin concentration of < 5 g/100 ml (haematocrit< 15%).
Severe falciparum malaria: Acute falciparum malaria with signs of severity and/or evidence of vital organ dysfunction.
Sporozoites: Motile malaria parasites that are infective to humans, inoculated by a feeding female anopheline mosquito. The sporozoites invade hepatocytes.
Transmission intensity: The intensity of malaria transmission measured by the frequency with which people living in an area are bitten by anopheline mosquitoes carrying sporozoites. This is often expressed as the annual entomological inoculation rate (EIR), which is the number of inoculations of malaria parasites received by one person in one year.
Uncomplicated malaria: Symptomatic infection with malaria parasitemia without signs of severity and/or evidence of vital organ dysfunction.

1 National Treatment Guidelines for Malaria in Cambodia
6. INTRODUCTION
Despite considerable progress in reducing both the morbidity and mortality of the disease, efficacy of first line antimalarial drug regimens is compromised by resistance to the artemisinin combination therapies. As of 2014, no feasible replacement regimens, capable of producing reliable cure rates on a countrywide basis, are currently available. This edition of the Cambodia National Treatment Guidelines for Uncomplicated and Severe Malaria has subsequently been developed to keep pace with the changing efficacy of antimalarial drugs in Cambodia and are based on the best available evidence.
7. COMPARISON BETWEEN 2012 and 2014 CAMBODIA NATIONAL MALARIA TREATMENT GUIDELINES
7.1 Recommendations changed from the 2012 Cambodia National Treatment Guidelines
• Since 2012, reduced efficacy of antimalarial treatments against P. falciparum has been measured in several areas in Cambodia. Because treatment responses may vary by geography, specific first-line regimens also vary by geography.
• DHA-piperaquine, while still recommended for use in certain provinces/operational districts (OD), is no longer the only recommended first line antimalarial treatment.
• For uncomplicated P. falciparum, new fixed dose combination (FDC) formulation of artesunate-mefloquine will be introduced in certain locations.
• Because treatment responses may vary from one year to the next, specific first-line treatment for P. falciparum are listed in Annex 1: “Province/OD specific P. falciparum treatment regimens”

National Treatment Guidelines for Malaria in Cambodia 2
7.2 Recommendations unchanged from the 2012 Cambodia National Malaria Treatment Guidelines
• Parasitological confirmation by microscopy or alternatively by RDTs is recommended in all patients suspected of malaria before treatment is started.
• Treatment solely on the basis of clinical suspicion should only be considered when a parasitological diagnosis is not accessible.
• Artemisinin-based combination therapies (ACTs) are the recommended treatments for uncomplicated P. falciparum malaria.
• Oral artemisinin and its derivatives should not be used as monotherapy for uncomplicated malaria.
• Second-line antimalarial treatment consists of quinine plus tetracycline or doxycycline for 7 days.
• Treatment of uncomplicated P. falciparum malaria in special risk groups: o First trimester of pregnancy: oral quinine for 7 days, with ACT indicated only
if quinine is not immediately available. o ACTs known to be effective in the region. o Lactating women: standard antimalarial treatment (including ACTs) except
for primaquine and tetracycline. o Infants and young children: ACTs for first-line treatment in infants and
young children with attention to accurate dosing and ensuring the administered dose is retained.
• Severe malaria: after rapid clinical assessment and confirmation of the diagnosis, full doses of parenteral antimalarial treatment should be started without delay with whichever effective antimalarial is first available
o For adults, children and infants, IV artesunate is first line treatment; intramuscular artemether is an acceptable alternative if parenteral artesunate is not available
o If complete treatment of severe malaria is not possible, patients should be given pre-referral treatment and referred immediately to an appropriate facility for further treatment.
o Patients should be given pre-referral treatment and referred immediately

3 National Treatment Guidelines for Malaria in Cambodia
8. EVALUATION OF PATIENTS WITH POSSIBLE MALARIA
8.1 Taking a patient history
Taking a patient history will help to determine whether a patient may have malaria, but the only way to be sure that a patient has malaria is if he/she has a positive diagnostic test. This is known as “confirmed” malaria. However, as malaria incidence decreases in Cambodia, it is important to diagnose and treat every possible malaria case even if many patients must be tested. In addition, P. falciparum malaria in Cambodia can be difficult to treat because of resistance to certain drugs. It is important to use the proper drugs to treat P. falciparum malaria for two reasons. First, inappropriate treatment can allow drug resistance to spread more rapidly, possibly making current treatments ineffective. Second, using the right drugs will ensure that patients are completely cured. For these reasons, patients diagnosed with a second P. falciparum malaria infection within a 28 day period should be referred to a referral hospital (or former district hospital) or health center/post and treated with second line agent. When evaluating potential malaria cases, providers should take a medical history by asking the questions listed in the table below.
Table 8.1: Questions to ask when evaluating for suspected malaria
Question Reason
In the past one month, have you had any risk factors for malaria such as travel to the forest, not using a bednet in areas with known malaria cases?
These risk factors place a patient at higher risk of having malaria
Have you recently travelled from an area without malaria to one where there is?
These patients are at higher risk of both getting malaria and getting sicker once they contract it
Have you had malaria in the past 28 days?
Patients with recent malaria may have failed treatment and may require retreatment with a second line agent
If you had malaria in the last 28 days what medicines did you take?
This will help determine if the patient really had malaria and avoid retreating with the same medicines

National Treatment Guidelines for Malaria in Cambodia 4
Have you had any symptoms such as fever, chills, and/or sweats?
These are typical malaria symptoms, but patients can still have malaria without having these symptoms
Have you had other signs that could point to malaria such as headache, nausea, vomiting, or diarrhoea?
These symptoms are less typical, but could be a sign the patient has malaria
Are you, or could you be pregnant? (If the patient is a young female)
Pregnant women are at risk of malaria complications and should be treated with medicines which are safe in pregnancy
Do you have any allergies to medi-cines?
Medicine allergies can be dangerous, even life threatening. Patients who have previously had lip or throat swelling or difficulty breathing after taking medicines should avoid taking those medicines.
8.2 Malaria Diagnosis: When to perform a diagnostic test?Prompt diagnosis of malaria is an important part of malaria case management. Diagnosis includes two components: first, providers must assess malaria risk in order to determine whether a patient may have “suspected” malaria based on symptoms or risk factors. Secondly, patients with “suspected” malaria should be confirmed to have malaria with a parasitological diagnosis. Obtaining a parasitological diagnosis has the following advantages:
• Improved patient care
• Identification of parasite negative patients who might have another disease
• Preventing the unnecessary use of antimalarial drugs
• Improved malaria case detection and reporting
• Confirmation of treatment failures
Recent data show that many patients may have malaria without the typical symptoms of fevers, chills or sweating. In fact, because some patients acquire immunity to malaria, patients may not exhibit symptoms at all even though they have a malaria infection.
It is therefore necessary to test patients even if they don’t have typical symptoms.
To determine who should be tested for malaria, providers should evaluate malaria risk based on epidemiological risk factors in addition to symptoms. Such risk factors include having a recent malaria infection, travel to the forest, recent arrival in a malaria endemic area, and living or working around other patients with confirmed malaria.
5 National Treatment Guidelines for Malaria in Cambodia
Box 8.1: Criteria for malaria diagnostic testing
Patients should be suspected to have malaria based on risk factors and physical symptoms. Consider testing if: They have one of the following:
• Fever• Chills• Sweats
ORTwo of the following:• Headache• Nausea• Vomiting• Diarrhoea• Travel to the forest in the past month• Confirmed malaria in the past 28 days• Travel to a malaria endemic area from a non-endemic area• Live or work around others with a recently confirmed malaria diagnosis
8.3 Malaria diagnosis: rapid diagnostic tests vs. microscopy
• Two laboratory methods are routinely used to diagnose malaria in field settings: microscopic examination of thick and thin stained blood films and rapid diagnostic tests. Quality assured microscopic examination of thick and thin stained blood films remains the gold standard for diagnosing malaria in field settings. Microscopy based diagnosis can provide information on mixed infections and level of parasite burden. In addition, microscopy can be used to follow patient treatment response over the course of time. Because of the high degree of technical skill needed to perform microscopy, rapid diagnostic tests (RDT) can be used in certain settings so that treatments can be given more quickly. If RDTs are used, it is important to use a test that differentiates between P. falciparum and P. vivax malaria.
• The choice of microscopy vs. RDT is based on many factors. Microscopy can be useful to determine species and quantitate parasite burden. The main disadvantage of microscopy is the requirement for a high degree of technical skill

National Treatment Guidelines for Malaria in Cambodia 6
to assure accurate results. The use of RDTs, however, allows diagnosis to occur at the community level so that treatment can be given more quickly and at greater convenience for patients.
• Parasitological diagnosis should be made, within two hours of the patient presenting for care.
• RDT manufacturer recommendations should be followed.
• Unless the patient has signs of severe malaria, treatment should NOT be started prior to confirming malaria with a positive diagnostic test.
• If a suspected malaria patient has signs of severe malaria, it is permissible to treat for malaria while awaiting the results of a confirmatory test.
• In severe malaria, blood films are preferred over RDT as they have the added advantage of following up response to treatment.
8.4 Evaluating for uncomplicated vs. severe malaria Patients with malaria are classified as having either uncomplicated or severe malaria. This distinction is significant because patients with severe malaria are at greater risk for complications (including death), and are not treated with the same medicines as patients with uncomplicated malaria. When evaluating malaria patients, providers should rapidly assess patients to determine if they meet criteria for severe malaria so that a decision can be made to administer appropriate treatment. Although all malaria species can cause severe malaria, P. falciparum is most associated with severe disease.
Many symptoms of malaria, especially fevers, chills and sweats, are also shared with diseases such as meningitis, encephalitis, typhoid fever, pneumonia, septicemia (blood poisoning), dengue hemorrhagic fever or pre-ecclampsia (in pregnant women). Providers should remember that many of the signs and symptoms of severe malaria may also indicate the presence of another serious disease. Patients may turn out to have one of these potentially serious diseases, either instead of malaria, or in addition to malaria. For this reason, patients with signs or symptoms of severe malaria should be sent as quickly as possible to a referral hospital where they can get proper treatment.

7 National Treatment Guidelines for Malaria in Cambodia
Box 8.2: Signs and symptoms of severe malaria
Clinical signs/symptoms• Impaired consciousness or unarousable coma• Prostration, i.e. generalized weakness so that the patient is unable walk or sit up without assistance• Failure to feed• Multiple convulsions – more than two episodes in 24 h• Deep breathing, respiratory distress (acidotic breathing)• Circulatory collapse or shock, systolic blood pressure < 70 mm Hg in adult and < 50 mm Hg in children• Clinical jaundice plus evidence of other vital organ dysfunction• Anuria or oliguria ( Urine output < 400 ml/24h) • Haemoglobinuria• Abnormal spontaneous bleeding• Pulmonary oedema (radiological)
Laboratory signs of severe malaria• Hypoglycaemia (blood glucose < 2.2 mmol/l or < 40 mg/dl)• Metabolic acidosis (plasma bicarbonate < 15 mmol/l)• Severe normocytic anaemia (Hb< 5 g/dl, packed cell volume < 15%)• Hyperparasitaemia (> 2%/100 000/μl in low intensity transmission areas or > 5% or 250 000/µl in areas of high stable malaria transmission intensity)• Hyperlactataemia (lactate > 5 mmol/l)• Renal impairment (serum creatinine> 265 µmol/l).
In patients with signs/symptoms of severe malaria:• It is ALWAYS PREFERRED to make a blood smear• However, treatment should be started immediately if testing is not readily available• At village or community level, treat with rectal artesunate before referral • Because patients can have malaria with another serious disease, it is acceptable to treat patients with severe symptoms with both antimalarial drugs and antibiotics if response is not seen with antimalarial treatment alone

National Treatment Guidelines for Malaria in Cambodia 8
Figure 1: Flow chart for malaria diagnosis and treatment
Definition of Suspected Malaria CaseONE of the following: Fevers, chills or sweats
OR TWO of the following: Headache, nausea, vomiting, diarrhea, forest travel,
confirmed malaria in the past six weeks, travel to malaria endemic area from non-endemic, or living/working around others with confirmed malaria
Perform diagnostic test (microscopy or RDT)Evaluate for signs of severe malaria
(See Box 13.1 Clinical, laboratory and radiological signs of severe malaria and Blantyre/Modified Glasgow
coma scale)
Positive test withsevere malaria signs: If IV AS or IM AM available treat for severe malariaIf not available, give rectal artesunate and refer (see Figure 2: Referral patterns & required treatment capabilities by health facility type “Recommended Referral Patterns by Facility Type”)
Positive test without severe malaria signs: Treat for uncomplicated malariaObserve first dose, DOT for remainder of treatment if possible
Negative test with severe malaria signs: If malaria still suspected, treat as test (+) for malaria, look for other causes of illness and refer to RH/FDH
Negative testWithout severe malaria signs:Consider other illnesses; if patient at high risk for malaria, retest in 1-2 days
If P. falciparum or mixed infection with Pf and known G6PD non-deficient, give primaquine: 0.25mg/kg or 15 mg x 1 dose
If P. vivax or ovale and known G6PD non-deficient, give primaquine:
• 15 mg X 14d (0.25 mg/kg) or
• 45 mg (0.75 mg/kg) weekly X 8 weeks
9 National Treatment Guidelines for Malaria in Cambodia
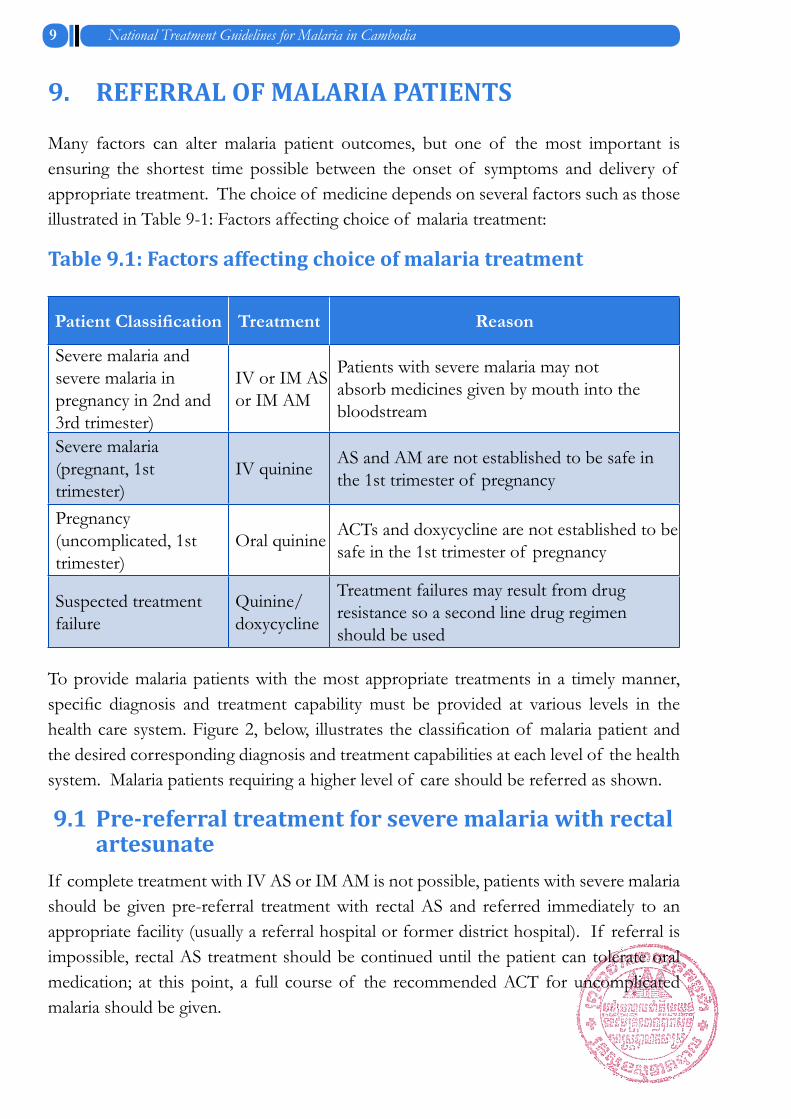
9. REFERRAL OF MALARIA PATIENTS
Many factors can alter malaria patient outcomes, but one of the most important is ensuring the shortest time possible between the onset of symptoms and delivery of appropriate treatment. The choice of medicine depends on several factors such as those illustrated in Table 9-1: Factors affecting choice of malaria treatment:
Table 9.1: Factors affecting choice of malaria treatment
Patient Classification Treatment Reason
Severe malaria and severe malaria in pregnancy in 2nd and 3rd trimester)
IV or IM AS or IM AM
Patients with severe malaria may not absorb medicines given by mouth into the bloodstream
Severe malaria (pregnant, 1st trimester)
IV quinine AS and AM are not established to be safe in the 1st trimester of pregnancy
Pregnancy (uncomplicated, 1st trimester)
Oral quinine ACTs and doxycycline are not established to be safe in the 1st trimester of pregnancy
Suspected treatment failure
Quinine/ doxycycline
Treatment failures may result from drug resistance so a second line drug regimen should be used
To provide malaria patients with the most appropriate treatments in a timely manner, specific diagnosis and treatment capability must be provided at various levels in the health care system. Figure 2, below, illustrates the classification of malaria patient and the desired corresponding diagnosis and treatment capabilities at each level of the health system. Malaria patients requiring a higher level of care should be referred as shown.
9.1 Pre-referral treatment for severe malaria with rectal artesunateIf complete treatment with IV AS or IM AM is not possible, patients with severe malaria should be given pre-referral treatment with rectal AS and referred immediately to an appropriate facility (usually a referral hospital or former district hospital). If referral is impossible, rectal AS treatment should be continued until the patient can tolerate oral medication; at this point, a full course of the recommended ACT for uncomplicated malaria should be given.

National Treatment Guidelines for Malaria in Cambodia 10
Figure2: Referral patterns & required treatment capabilities by health facility types
• Registered private outlets providing health services should only provide treatment to uncomplicated malaria among ≥ 5Y and Non-pregnancy. All others should be referred to the above MoH facilities as appropriate
• Health facilities under ministry of national defense (MOND) and national police should use the same treatments as at MoH public sector facilities
Referral and FD HospitalsReceive from private sector, HC/HP and VMW/MMWs:• Severe• Uncomplicated pregnant women in 1st trimester• Suspected treatment failure(TF)
Referral Hospitals and Former District HospitalsPatient classification Required treatment capacity Severe RDTs and microscopy ACTs
Quinine (oral for 1st trimester pregnancies and 2nd line treatment;
Quinine IV for severe pregnant)
Doxycycline (2nd line treatment)IV AS or IM artemether
Uncomplicated, including 1st trimester pregnancy Children < 5
Suspected TF
VMW/MMWsRefer to RH/FDH
• Severe • Suspected TFRefer to HC/HP or RH/FDH• Uncomplicated pregnant women in 1st trimester
Health Centers/postsReceive from private sector, VMW/MMWs:
• Uncomplicated pregnant women in 1st trimester• <5 Y from PPs
Refer to Referral and FDHs
• Severe malaria• Suspected TF
Health Centers and Health PostsPatient classification Required treatment capacity Uncomplicated, including 1st trimester pregnancy
RDTs and microscopyACTsQuinine (oral for 1st trimester pregnancies and 2nd line treatment)Doxycycline/Tetracycline (2nd line treatment)Pre-referral rectal AS for severe cases
Children < 5
VMW/MMWsPatient classification Required treatment capacity
Uncomplicated, except 1st trimester pregnancy
RDTs +/- microscopy ACTsPre-referral rectal AS for severe cases
Children < 5

11 National Treatment Guidelines for Malaria in Cambodia
10. TREATMENT OF UNCOMPLICATED MALARIA
10.1 PrinciplesMalaria parasites infect the body through the bite of an infected mosquito by passing through the liver, and entering the blood stream. Some malaria species (vivax and ovale) form sleeping forms in the liver (hypnozoites), which can cause malaria relapses weeks or months after the initial infection. Malaria parasites in the blood stream cause malaria symptoms and can be passed to others when mosquitoes bite patients and ingest the form of malaria parasite that reproduces in mosquitoes (gametocytes). Malaria medicines reduce malaria incidence in three ways: first, by killing forms in the blood that cause symptoms, second by killing hypnozoites, and third, by killing gametocytes so that they cannot reproduce in the mosquito. As Cambodia makes progress towards reducing malaria throughout the country, malaria treatments will focus on killing malaria at each of these points in its lifecycle by using primaquine to kill hypnozoites and gametocytes and DHA-PIP/ASMQ-FDC for other malaria parasite stages in the blood.
The National Malaria Programme recommendations for treatment regimens for all malaria species are based on the principles:• First line treatment regimens will be those with expected maximum efficacy against P. falciparum. Treatment for other malaria species will be the same as that for P. falciparum• Treatments may differ by geographical area and are determined by resistance data. See Annex A: • Patients with P. vivax and ovale with non-deficient G6PD status should be treated with primaquine to prevent relapse. • Treatment of uncomplicated malaria will only be initiated after a parasitological diagnosis.
10.2 First Line Treatment for Uncomplicated P. falciparum, vivax, ovale and malariae speciesAs in the past, current first line treatments for uncomplicated P. falciparum malaria are guided by treatment responses as measured by therapeutic efficacy studies or other drug resistance data. The first and second line treatments and dosing for P. falciparum malaria are also used for P. vivax, P. ovale, or P. malariae species. P. falciparum treatments for malaria include either dihydroartemisinin-piperaquine (DHA + PPQ) or artesunate-mefloquine (ASMQ). The artesunate-mefloquine formulation recommended by CNM

National Treatment Guidelines for Malaria in Cambodia 12
is a “fixed dose combination” (FDC) and will be used instead of the loose artesunate and mefloquine tablets previously used in Cambodia. Use of the FDC formulation will simplify dosing and likely reduce side effects compared to giving artesunate and mefloquine separately.
• 1st line treatment: o Dihydroartemisinin-piperaquine (DHA + PPQ)
ORo Artesunate + mefloquine (A+M) Fixed Dose Combination (FDC)
• The choice of DHA +PPQ or A+M FDC depends on region where malaria was acquired• 2nd line treatment:
o quinine + doxycycline/tetracycline, regardless of where infection was acquired
10.3 DHA+PPQ dosingDHA-piperaquine is a fixed dose combination with tablets containing 40 mg of dihydroartemisinin and 320 mg of piperaquine. The target dose is 2-4 mg/kg/day dihydroartemisinin and 20 mg/kg/day piperaquine for 3 days.
Table 10.1: DHA + PPQ daily dosing for uncomplicated malaria
Weight (kg) Age (years)Number of Tablets
Day 1 Day 2 Day 3 Total
5≤w<10 3 months ≤a<1 year ½ ½ ½ 1 ½
10≤w<19 1 year ≤ a < 5 years 1 1 1 3
19≤w<30 5 years ≤a < 10 years 1 ½ 1 ½ 1 ½ 4 ½
30≤w<40 10 years ≤a <15 years 2 2 2 6
40≤w<60 15 years+ 3 3 3
≥ 60 kg 15 years++ 4 4 4 12
9

13 National Treatment Guidelines for Malaria in Cambodia
10.4 Artesunate + mefloquine FDC dosing
The CNM recommended fixed dose combination is available in a tablet form containing 25 mg AS + 50 mg mefloquine (small tablets) or 100 mg artesunate + 200 mg mefloquine (large tablets). The target dose of 4 mg/kg/day artesunate and 6 mg/kg/day of meflo-quine should be given once a day for 3 days:
Table 10.2: Artesunate + mefloquine FDC daily dosing for uncomplicated malaria
Patient weight
(kg)
Number of artesunate-mefloquine
tablets (25 mg artesunate + 50 mg mefloquine)
Total # tablets
(ASMQ 25/50 mg
Number of artesunate-mefloquine
tablets (100 mg artesunate + 200 mg mefloquine)
Total # tablets
(ASMQ 100/200
mg)
Day 1 Day 2 Day 3 Total/3days Day 2 Day 2 Day 3 Total/
3days
5-<9 1 1 1 3
9-<18 2 2 2 6
18-<30 1 1 1 3
>30 2 2 2 6
10.5 Mefloquine adverse effects and contraindications• Mefloquine is a component of artesunate-mefloquine FDC. Mefloquine adverse effects include:
o Nausea, vomiting, abdominal pain, poor appetite, diarrohea o Headache, dizziness, loss of balance, sleep disorders, abnormal dreams.
• AS+MQ should be avoided in patients with psychiatric disorders• AS+MQ should be avoided in patients who received mefloquine in the past 4 weeks

National Treatment Guidelines for Malaria in Cambodia 14
10.6 Second-line treatment for uncomplicated P. falciparum malaria
10.6.1 Quinine-doxycycline/tetracycline dosing
The second line treatment for all species of uncomplicated malaria is quinine + doxycy-cline/tetracycline. This regimen must be taken for 7 days to achieve desired cure rates so it is important to explain to patients the importance of adhering to a complete 7 day regimen.
• Quinine: o Adult and paediatric dose is 10 mg/kg X 3 times daily X 7 dayso Quinine has a bitter taste--for small children, tablets can be crushed and mixed with a solution of water and sugar
• Doxycycline: o Adults: 100 mg twice daily X 7 dayso Children: 2mg/kg twice daily X 7 days (only for children > 8 years).
• For adults and children over 8 years: tetracycline may be substituted for doxycycline. Tetracycline is dosed at 8.3 mg/kg X 3X daily (25 mg/kg/day).
Table 10.3: Quinine-doxycycline dosage
Age Weight (kg)
Number of tablets
Quinine (300mg) Doxycycline (100mg)
Dose/8h Total/day Total/
7days
Total/ day (single dose)
Total/ 7days
< 6 month < 7 ¼ ¾ 5 ¼ - -
≥ 6 m - 2 years 7-15 ½ 1 ½ 10 ½ - -
≥ 2-<8 years 16-30 1 3 21 - -
≥8-<15 years 31-40 1 ½ 4 ½ 31 ½ 1
≥ 15 years > 40 2 6 42 2
7
14

15 National Treatment Guidelines for Malaria in Cambodia
Table 10.4: Quinine-tetracycline dosing
Age Weight (kg)
Number of tablets
Quinine (300mg) Tetracycline (250mg)
Dose/8h Total/ day
Total/ 7days Dose/8h Total/
day Total/ 7days
< 6 month < 7 ¼ ¾ 5 ¼ - - -
≥ 6 m - 2 years 7-15 ½ 1 ½ 10 ½ - - -
≥ 2-<8 years 16-30 1 3 21 - - -
≥ 8-<15 years 31-40 1 ½ 4 ½ 31 ½ 1¼ 4¼ 31¼
≥ 15 years > 40 2 6 42 2 6 42
10.6.2 Doxycycline/tetracycline contraindicationsDoxycycline and tetracycline are contraindicated in pregnancy and children < 8 years old. Children < 8 years requiring second line treatment should be treated with 7 days of quinine without doxycycline or tetracycline.
10.7 Use of Malarone® in Cambodia for use in special situationsMalarone® will be registered in Cambodia for use in special situations and only by special permission by the national malaria control program (CNM). Because of concerns for resistance, Malarone is only recommended in combination with another antimalarial drug such as artesunate.
10.8 Additional considerations for treating uncomplicated malaria
• To assure accurate dosing, it is preferable to use weight to assure correct dosing. If no scale is available, treat according to patient’s age.• Providers should explain to patients:
o The importance of adhering to the medications given, and that patients should complete their entire course even if they feel better.o Possible side effects, such as headache, dizziness, nausea, vomiting, diarrhoea, or loss of appetite. Many of these symptoms can be caused by malaria as well.
• If a patient has taken quinine, providers should wait at least 12 hours before treating with ASMQ.• Providers should observe patient for one hour after taking medicine to assure

National Treatment Guidelines for Malaria in Cambodia 16
patient doesn’t vomit medicine.• Fever is common in malaria. Using antipyretics (fever reducing medicine such as
paracetamol) will not only reduce patient discomfort, but also reduce the likelihood that patients will vomit their medicine. In addition to antipyretics, patients can be cooled by using fanning and sponging with cloths soaked in cool water.
10.9 Drug resistance, treatment failures, and strategies to reduce transmission of resistant parasitesIn Cambodia, most patients can be successfully cured. Patients with recurrent symptoms after a recent malaria diagnosis and treatment may have a new infection, a different disease, or a treatment failure. Treatment failures occur when malaria parasites are not completely cleared from the body and return later to cause a second infection. Treatment failures can occur for a variety of reasons including inadequate levels of antimalarial drug in the blood stream where they exert their effect.1
• Treatment failures can result from incomplete adherence (i.e. the patient did not take all the required doses) • Poor quality medicine, or poor absorption of drug into the blood stream • Resistance of parasites to antimalarial treatment (In Cambodia, there is widespread resistance to many drugs, including ACTs)
Drug resistance is more likely to develop when patients are not completely cured, thus it is important to detect treatment failures and treat them appropriately. This will help ensure that currently available treatment remains effective.The continued use of a medicine to which parasites are partially resistant will encourage the selection of resistant parasites and their transmission. After treatment, gametocyte densities are higher in patients with resistant parasites than sensitive parasites and recrudescent infections are associated with higher rates of gametocyte carriage than primary infections. The cumulative effect of incompletely cured infections is the generation of more gametocytes capable of malaria transmission. Gametocytes with resistant genes are also more infectious to mosquitoes, producing higher parasite densities in the mosquito. Therefore, providers have a special role to ensure that drug resistance is prevented as shown in Box 10.1

17 National Treatment Guidelines for Malaria in Cambodia
Box 10.1: How providers can prevent drug resistance from worsening
Providers should: • Be aware that the continued use of a failing regimen will selectively increase the selection of resistant parasites and hasten their spread• Treat malaria patients as early as possible with an effective antimalarial (ACT)• Use only high quality unexpired drugs from approved sources• Explain to patients that malaria parasites may still remain in the body even after they feel better, so it is important to take all recommended doses. DOT is encouraged! • If possible, use patient weight instead of age to determine correct dosing• Encourage patients to take medicines with food• Encourage patients to return for care if their malaria symptoms do not improve or worsen• Use second line medication (quinine based regimens) for treatment failures. Refer if necessary
10.10 How to manage potential treatment failureIn Cambodia, P. Falciparum malaria cases reoccurring within 28 days of a previous malaria P. falciparum treatment are likely due to treatment failure. This can occur even after a patient is apparently cured and free of symptoms. If a patient is confirmed to have a second P. Falciparum diagnosis within 28 days, providers should consider the possibility of treatment failure. In this case providers should:
• Carefully question that patient to determine if the correct antimalarial medicine was given and whether the patient took all recommended doses. • If an incorrect medication was given, retreat with the correct regimen according to the region where malaria was acquired. • If the patient’s adherence is doubtful, or if the patient recalls vomiting any dose within one hour, treat again with the correct first line regimen. • If the patient adhered to the correct treatment regimen, treatment with second line therapy (quinine-doxycycline/tetracycline).• If P. falciparum malaria is confirmed later than 28 days from a prior P. falciparum treatment, treat as a new P. falciparum diagnosis with the recommended first-line agent.

National Treatment Guidelines for Malaria in Cambodia 18
10.11 Follow up of uncomplicated P. Falciparum malariaAll P. falciparum malaria should be monitored for clinical response to malaria treatment. Because of heightened concern over drug resistant P. falciparum, CNM will identify certain health centres or referral (former district) hospitals where microscopy is available to participate in intensified parasitological follow up of P. falciparum cases. Those areas will follow up patients for adequate parasitological responses as summarized in Box 10.2 below.
Box 10.2: Summarized recommendations on parasitological follow up of P. falciparum infections
CNM will coordinate and monitor, as part of surveillance, a 28 days parasitological follow up in selected provinces. These activities consist of:• Prepare blood film on the third day after treatment (D3) to confirm the negativity of the slide or the change of the parasitemia density compared to the first day (D0)• If the parasitemia decreased on the third day after treatment (D3), make another slide on day 7 (D7) to confirm parasite clearance
• If the parasitemia increases on D3 after treatment, refer the patient to the nearest referral hospital, where he/she will be treated with second line treatment• Where feasible, obtain follow up slides at D28 to confirm whether or not the treatment has been successful.• Recurrent parasitemia should be treated as specified in section 10.10 “How to manage potential treatment failure”• RDTs are not suitable to assess parasitological response after treatment. They often remain positive up to and even after D14, even when malaria parasites are not present by microscopy.
CNM will direct the collection of P. falciparum malaria samples at regular intervals in certain provinces in order to identify drug resistance markers. This information will help guiding future malaria drug policy.
10.12 Primaquine indicationsPrimaquine plays a unique role in malaria treatment because of its ability to kill hypnozoites and prevent P. vivax and ovale relapses. In addition, primaquine at lower doses than used to kill hypnozoites may also prevent malaria transmission by killing gametocytes.
• Primaquine is recommended by the World Health Organization (WHO) for falciparum malaria to reduce transmission, and to eradicate dormant malaria forms (hypnozoites) of relapsing malaria species (P. vivax and P. ovale).
19 National Treatment Guidelines for Malaria in Cambodia
• Two different doses are used:
o Low dose PQ (LDPQ) to reduce transmission
o Standard dose PQ (SDPQ) to treat relapsing malaria (P. vivax and P. ovale)
10.13 Primaquine dosing (low dose)For P. falciparum or mixed infections containing P. falciparum component (to reduce malaria transmission)
o Low dose PQ: a single dose of primaquine (0.25mg/kg or 15mg for a 60kg adult) is added to ACT treatment for uncomplicated P. falciparum malaria as an anti-gametocyte agent
o Low dose PQ should be given on the first day of ACT treatment
10.14 Primaquine dosing (standard dose)For P. vivax and ovale (to prevent relapses)
o Standard dose PQ: ▪ Adults: 45 mg weekly (0.75 mg/kg) x 8 weeks OR 0.25 mg/kg daily x
14 days
▪ Children: 0.75 mg/kg x 8 weeks OR 0.25 mg/kg daily x 14 days
▪ The determination of weekly vs. daily PQ dosing should be guided by whichever regimen is more likely to achieve patient adherence
10.15 Uses of primaquine by species
Malaria species
First-line regimen±
Second-line regimen
Standard dose primaquine†
(SDPQ)
Low dose primaquine†
(LDPQ)
P. falciparum ASMQ-FDC or DHA-PIP depending on region where
infected
Quinine +
Doxycycline or
Tetracycline
+P. vivax +P. ovale +P. malariaeP. knowlesi
10.16 Primaquine safety and other considerations
Despite the advantages listed above, primaquine can cause haemolytic anaemia in certain G6PD deficient individuals. The risk of dangerous haemolytic anaemia is dependent on primaquine dose and the severity of G6PD deficiency.
For this reason, primaquine is not recommended for routine use unless the patient is

National Treatment Guidelines for Malaria in Cambodia 20
determined to be G6PD non-deficient, or with special permission from CNM.
Box 10.3: Primaquine Safety
• Primaquine can cause haemolysis in patients with G6PD deficiency and should be stopped if signs of haemolysis occur (yellowish eyes/skin or brown or dark yellow urine)
• Primaquine should not be given to children under one year, pregnant or nursing women unless the breastfeeding infant is determined not to be G6PD deficient
• Primaquine causes abdominal discomfort when taken on an empty stomach; it should always be taken with food. Patients should be instructed on the clinical signs of haemolysis, anaemia and jaundice and to check their urine and seek medical care in case of suspected haemolysis.
• Primaquine should only be administered if the patient’s G6PD status is known or with special permission from CNM
11. TREATMENT OF UNCOMPLICATED MALARIA IN INFANTS AND CHILDREN
Because children can deteriorate more quickly than adults, it is particularly important that young children and infants receive diagnosis and treatment for suspected malaria without delay. In addition to the symptoms typical for adults with malaria, the following symptoms are also seen in children:
• Nausea, vomiting and sometimes diarrhoea• Algid syndrome: crying and restlessness in infant and young child, headache in
older ones, often associated with an acute and distend abdomen (which might simulate a surgical abdomen)
• Neurological syndrome: drowsiness, confusion, meningismus, evocative of encephalitis
• Splenomegaly is common and might be associated to hepatomegaly• Broncho-tracheal signs: cough is common with sometimes a labial herpes (which
might be confusing)First line treatment and special considerations in children: First line malaria treatment for children is the same as adults. However, because dosing based on body weight are included in the section 10.3. It is important to determine the body weight in infants and young children to determine correct dosing.

21 National Treatment Guidelines for Malaria in Cambodia
• First line malaria treatment in infants and children is the same as for adults• It is especially important to use the correct dose in infants and children• Dosing should be based on the patient’s weight (see Annex A)• Both DHA-piperaquine and ASMQ FDC are available in smaller paediatric formulations. These smaller formulations should be used.
12. TREATMENT OF UNCOMPLICATED MALARIA IN PREGNANT WOMEN
Pregnant women with malaria are at a higher risk than other patients of developing complications of malaria. Pregnant women have the additional risk or increased risk of premature delivery, congenital infection, low birth weight and still birth. Hypoglycaemia, anaemia and pulmonary oedema are common complications of malaria in pregnant women. Because most antimalarial treatments are not well studied in pregnant women, the choice of treatment must be carefully chosen, especially in the first trimester of pregnancy when the foetus is most susceptible to the potential side effects of antimalarial drugs. Fortunately, several malaria drugs are considered safe in pregnancy, including quinine. For this reason, it is especially important that pregnant women receive early diagnosis and appropriate treatment.
As shown below, first line treatments differ in pregnant women depending on the gestational age of pregnancy at the time malaria is diagnosed. While treatment in the 2nd and 3rd trimester of pregnancy is the same as for non-pregnant patients, quinine should be used in women in the 1st trimester of pregnancy. Because many women do not know they are pregnant while in the 1st trimester, it is important that providers actively question women of child-bearing age whether they might be pregnant.
Because of the special requirements and risk of complications, all pregnant women diagnosed with malaria should be referred as shown in Figure 2: Referral patterns and required treatment capabilities by health facility type.
12.1 First line treatmentQuinine is safe for pregnant women in all three trimesters. Since there is insufficient data to support the use of ASMQ and DHA + PPQ in the first trimester, these regimens should only be used in the second and third trimesters unless quinine is unavailable. First line treatment of uncomplicated P. falciparum, vivax, ovale, or malariae in pregnant women are as follows:
• Quinine is first line treatment for pregnant women in the first trimester• DHA-PIP and ASMQ are safe for pregnant women in second and third trimesters• Quinine must be given for seven days to achieve satisfactory cure rates• Doses are the same as used for non-pregnant patients (see section 10 TREATMENT OF UNCOMPLICATED MALARIA

National Treatment Guidelines for Malaria in Cambodia 22
• Doxycycline and tetracycline are contraindicated in pregnancy and in children <8 years of age
12.2 Lactating womenOnly small amounts of antimalarials enter the breast milk of lactating women, so the first line treatment for malaria in lactating women is the same as for non-breastfeeding women. However, because of the small risk of G6PD related haemolysis in infants, breastfeeding women should not be treated with primaquine unless the breast fed infant is determined not to be G6PD deficient.
In breastfeeding women, tetracycline and doxycycline must also be avoided because of the potential effect on the infant’s bones and teeth.
13. TREATMENT OF SEVERE MALARIASevere malaria is most commonly caused by infection with P. falciparum, although P. vivax can also cause also cause severe malaria. A fifth human malaria, P. knowlesi, is found mostly on the Indonesian island of Borneo, but cases have been reported elsewhere in Southeast Asia.
The risk is or progression from uncomplicated malaria to severe disease is increased if treatment is delayed, in children, in pregnant women, patients with HIV/AIDS, and in patients who have undergone splenectomy.
Therefore, the most important aspect of treating severe malaria is recognizing the disease early and providing prompt treatment. Since treatment for severe malaria requires parental treatment and stockage of IV artesunate (or IM artemether), providers must weigh the benefits of transferring patients to referral centers carrying these drugs against the risk of delaying treatment.
13.1 Treatment objectivesThe main objective of treating severe malaria is to prevent the patient from dying, while secondary objectives are prevention of disabilities and prevention of malaria recrudescence. The mortality of untreated severe malaria (particularly cerebral malaria) is thought to approach 100%, but with prompt, effective antimalarial treatment and supportive care, the mortality rate falls significantly. Death from severe malaria can occur within hours of presentation for care, so it is essential that treatment with a highly effective antimalarial is begun as soon as possible.
13.2 Clinical assessmentSevere malaria is a medical emergency, so providers should examine patients for signs and symptoms of severe malaria including a assessing the patient’s coma score (see Box 13.1). The Glasgow coma scale is suitable for adults, and the Blantyre coma score can be used for children, including those who have not learned to speak. Although these criteria are

23 National Treatment Guidelines for Malaria in Cambodia
useful for strictly defining severe malaria, from a practical perspective, providers should generally apply a low threshold for treating patients with IV artesunate (or acceptable alternative as defined in section 13.5, below).
13.3 Differential diagnosis of severe malariaProviders should be aware of the overlap in severe symptoms of malaria and other potential fatal infectious diseases. Fevers, chills and sweats, can also result from meningitis, encephalitis, typhoid fever, pneumonia, septicaemia (blood poisoning), dengue haemorrhagic fever or pre-ecclampsia (in pregnant women). Patients may turn out to have one of these potentially serious diseases which may occur in combination with malaria. For this reason, patients with signs or symptoms of severe malaria should be sent as quickly as possible to a referral hospital where they can get proper treatment. Unconscious patients should have a lumbar puncture for cerebrospinal fluid analysis to exclude bacterial meningitis.
13.4 Urgent initial treatment stepsBecause severe malaria is a medical emergency, initiating early treatment interventions is a high priority. The following steps should be prioritized:
• If patient is unconscious, ensure an open airway and assess for breathing and circulation while assessing patient for other severe signs. Start other resuscitative measures immediately• Establish IV access• Weigh patient so that medicines, including antimalarials and fluids, can be given. If a scale is not immediately available, estimate patient weight • Measure blood glucose levels. Correct hypoglycemia if present• Treat convulsions in seizing patients
13.5 First line treatment of severe malaria in adults and childrenIn Cambodia, intramuscular artemether has traditionally been used for severe malaria. IM artemether is given as a single daily dose for period of 5-7 days, depending on when the patient can transition treatment to oral antimalarials. However because of concern over the unpredictable absorption of IM artemether, IV or IM artesunate are also recommended as first line treatments. Artesunate, given intravenously is the only agent proven to
• Give parenteral antimalarial agents in the treatment of severe malaria for a minimum of 24h, even if the patient is able to tolerate oral medication earlier.• Calculate the doses based on mg/kg of body weight. All patients should be weighed; if this is not possible, the patient’s weight should be estimated.• Treatment doses of AS or AM are as follows:
o Artesunate 2.4 mg/kg BW IV or IM given on admission (time = 0), then at

National Treatment Guidelines for Malaria in Cambodia 24
12 h and 24 h, then once a day is the recommended treatment. Artesunate doses for IV and IM are the same, but should be diluted into different volumes of normal saline or 5% dextrose
o IM artemether is an acceptable alternative if IV or IM artesunate are not options. Artemether dosing is 3.2 mg/kg IM given on admission then 1.6 mg/kg BW per day
• When the patient can swallow, discontinue IV AS and give primaquine and full 3-day oral dose of DHA-PIP or A+M FDC, depending on region where infection was acquired.• Do not give ASMQ in patients recovering from cerebral malaria if there is a chance of neuropsychiatric reaction (give DHA-piperaquine instead).
13.6 Preparation of artesunate for IV or IM administrationAfter initial clinical assessment, providers should move quickly to prepare artesunate for IV dosing by:
• Based on measured or estimated weight, determine the number of artesunate vials needed for the initial dose. Although dosing by intravenous route is preferred, artesunate can also be given by intramuscular injection.
• Artesunate vials contain 60 mg powered drug and must be first activated by dissolving in bicarbonate, then diluted before dosing.
• Dissolve powdered artesunate by adding 1 ml bicarbonate directly to the artesunate vial. Artesunate is not stable in water or acidic pH, so it should not be reconstituted in water or other diluent. Use the full content of bicarbonate vial to ensure artesunate solution reaches desired pH.
• Further dilute dissolved (activated artesunate) in either normal saline or 5% dextrose. The appropriate volume of diluent varies depending on whether it will be given by IV or IM route of administration. Add 5 ml of diluent for IV dosing; 2 ml of diluent for IM dosing.
• Shake vial(s) until dissolved. Solution will be cloudy, but should clear in approximately 2 minutes. Discard if not clear.
• Depending on whether dosing will be by IV or IM routes, refer to section 13.5 and Table 13 1 (IV) and Table 13 2 (IM) to determine appropriate volume for injection
• Infuse artesunate intravenously by slow bolus (3-4 ml/minute)• Dose to be given should be rounded up to the next nearest whole number of
milliliters (ml) to be injected. For example, if a patient requires only 4.3 ml, round up to 5 ml.
• Discard any unused solution if not used within one hour of preparation. This includes remaining portions of vials not required for dosing
• Preparation a fresh vial or set of vials for each dose

25 National Treatment Guidelines for Malaria in Cambodia
Blantyre coma scale (for children who can’t speak)
ScoreEye movements:• Directed (e.g., follows mother’s face 1• Not directed 0Verbal response:• Appropriate cry 2• Moan (“gémissements”) or inappropriate cry 1• None 0Best motor response:• Localizes painful stimulus± 2• Withdraw limb from pain* 1• Non-specific or absent response 0Total 0 to 5±Rub knuckles on patient’s sternum or above patient’s eyebrow.* Firm horizontal pressure on thumbnail bed with a pencilA state of unarousable coma is reached at a score of <3. This scale can be used repeatedly to assess improvement or deterioration.
Modified Glasgow coma scale (for adults and children who can speak) ScoreEye opening:• Spontaneous 4• To speech 3• To pain 2• Never 1Best verbal response:• Oriented 5• Confuse 4• Inappropriate words 3• Incomprehensible sounds 2• None 1Best motor response:• Obeys commands 5• Localizes pain1 4• Flexion to pain2 3• Extension to pain 2• None 1Total 3 to 14
Box 13.1: Clinical, laboratory and radiological signs of severe malaria andBlantyre/ModifiedGlasgowcomascale
Clinical signs/symptoms• Impaired consciousness or unarousable coma• Prostration, i.e. Generalized weakness so that the patient is unable walk or sit up without assistance• Failure to feed• Multiple convulsions – more than two episodes in 24 h• Deep breathing, respiratory distress (acidotic breathing)• Circulatory collapse or shock, systolic blood pressure <70 mm Hg in adult; <50 mm Hg in children• Clinical jaundice plus evidence of other vital organ dysfunction• Oliguria (<400 ml/24 H), Hemoglobinuria• Abnormal spontaneous bleeding• Pulmonary edema (Confirmed by radiology)
Laboratory/radiological signs of severe malaria• Hypoglycemia (blood glucose < 2.2 mmol/l or < 40 mg/dl)• Metabolic acidosis (plasma bicarbonate< 15 mmol/l)• Severe normocytic anemia (Hb< 5 g/dl, packed cell volume < 15%)• Hemoglobinuria• Hyperparasitemia (> 2%/100 000/μl in low intensity transmission areas or > 5% or 250 000/µl in areas of high stable malaria transmission intensity)• Hyperlactatemia (lactate > 5 mmol/l)• Renal impairment (serum creatinine > 265 µmol/l)• Pulmonary edema

National Treatment Guidelines for Malaria in Cambodia 26
Table 13.1: IV artesunate treatment for severe malaria
Recommended antimalarial regimen
Dosing by weight and day
Follow up + comments
Weight (kg)
Day 1 doses(ml diluted
AS)
Two doses, 12 hours
apart
Day 2- 7(ml diluted AS)
On day 2, give dose 24 hours after 1st dose
IV artesunate:• Each vial contains 60 ml artesunate powder
• Dissolve AS powder in 1 ml 5% sodium bicarbonate
• Dilute with 5 ml of 5% dextrose or normal saline and give dose (in ml) shown immediately by IV bolus
• DO NOT USE WATER AS DILUENT
• Each vial of AS prepared this way contains 10 mg/ml
• Give at least 24 hours of IV or IM treatment even if patient can tolerate oral treatment earlier
6-<7 2 (each dose) 2 • When patient can take oral: give full 3 days course of first line regimen for region (either DHA-piperaquine or ASMQ FDC)
• Do not give ASMQ in patients recovering from cerebral malaria if there is a chance of neuropsychiatric reaction (give DHA-piperaquine instead).
7-<10 3 3
11-<14 4 4
14-<17 5 5
17<26 6 6
26-<30 7 7
30-<34 8 8
34-<38 9 9
38--<42 10 10
42-<46 11 11
46-<51 12 12
51<54 13 13
55-<59 14 14
59-<63 15 15
63-<67 16 16
67-<71 17 17
71-<75 18 18
≥75 24 24

27 National Treatment Guidelines for Malaria in Cambodia
Table 13.2: IM artesunate treatment for severe malaria
Recommended antimalarial regimen
Dosing by weight and day
Follow up + commentsWeight
(kg)
Day 1 doses(ml diluted
AS)
Two doses, 12 hours
apart
Day 2- 7(ml diluted
AS)
On day 2, give dose 24 hours after
1st dose
IV artesunate:
• Each vial contains 60 ml artesunate powder
• Dissolve AS powder in 1 ml 5% sodium bicarbonate
• Dilute with 2 ml of 5% dextrose or normal saline and give dose (in ml) shown immediately by IV bolus
• DO NOT USE WATER AS DILUENT
• Each vial of AS prepared this way contains 20 mg/ml
• Give at least 24 hours of IV or IM treatment even if patient can tolerate oral treatment earlier
6-<7 1 (each dose) 1
• When patient can take oral: give full 3 days course of first
line regimen for region (either DHA-
piperaquine or ASMQ FDC)
• Do not give ASMQ in patients recovering from
cerebral malaria if there is a chance of
neuropsychiatric reaction (give
DHA-piperaquine instead).
7-<10 2 2
11-<14 2 2
14-<17 3 3
17<26 3 3
26-<30 3 3
30-<34 4 4
34-<38 5 5
38--<42 5 5
42-<46 6 6
46-<51 6 6
51<54 7 7
55-<59 7 7
59-<63 8 8
63-<67 8 8
67-<71 9 9
71-<75 9 9
≥75 10 10
13.7 Alternative first line treatment: IM artemetherIntramuscular artemether with its simple once-a-day regimen and ease of administration is an

National Treatment Guidelines for Malaria in Cambodia 28
acceptable alternative to IV or IM artesunate. However, artemether formulation is oil-based and may be inadequately or erratically absorbed after intramuscular injection in severely ill patients.
13.8 Recommended dosing for IM artemether in adults and childrenGive single dose of Artemether IM 3.2 mg/kg body weight on the Day 1 and then single dose of 1.6 mg/ kg bodyweight daily from Day 2 to Day 5 to the maximum of total five doses.
Table 13.3: Recommended IM artemether dosing in adults and children
Patient Weight (Kg)
Day 1 Day 2 to Day 5
Artemether (mg/kg)
No. of ampules
Artemether (mg/kg)
No. of ampules
50 3.2 2 1.6 125 3.2 1 1.6 ½
12.5 3.2 ½ 1.6 ¼
13.9 Second line treatment for severe malariaAlthough IV/IM artesunate and IM artemether are preferred over IV quinine for severe malaria, the most important factor in treating severe malaria is reducing the time to treatment. If IV artesunate is unavailable, IV quinine is an acceptable second treatment and should not be withheld. The maintenance dose of quinine (10 mg salt/kg body weight) is administered at 8-h intervals, starting 8 h after the first dose. The formulation available in Cambodia is quinine dihydrochloride
Rapid administration of quinine is unsafe. Each dose of parenteral quinine must be administered as a slow, rate-controlled infusion (usually diluted in 5% dextrose and infusedover 4 h). The infusion rate should not exceed 5 mg salt/kg body weight per hour.
• If you cannot weigh the patient, estimate his/her weight.• Always use a 10% dextrose infusion as quinine can cause hypoglycemia.• If Doxycycline is not available, substitute/replace with tetracycline.• Doxycycline and tetracycline should not be used for children under 8 years old.To make dextrose 10%: add 50 ml of dextrose 50% to 500 ml of dextrose 5% for infusion.• Start oral treatment when the patient regain consciousness and can swallow.
Important notes about quinine:
- One ampoule of 2 ml contains 600 mg of quinine dihydrochloride.- In case of a renal failure (if the patient passes only a small amount of dark urine

29 National Treatment Guidelines for Malaria in Cambodia
and appears well hydrated), reduce after 24 hours the dose of quinine by 50%, i.e. quinine 5 mg/kg in an 8-hour infusion, 3 times per 24 hours.
- If haemoglobinuria occurs, DO NOT STOP or REDUCE QUININE. If anemia is severe, transfuse. While quinine commonly causes hypoglycaemia in pregnant women, it is safe for fetuses.
- Mild side-effects are common, notably cinchonism (tinnitus, hearing loss, dizziness, nausea, uneasiness, restlessness and blurring of vision)
- Hypoglycaemia is the most serious and frequent adverse side-effect.
Box 13.2: Recommended IV quinine treatment protocol
D1 (day of admission)1st infusion:500 ml dextrose 10% + quinine dihydrochloride10 mg/kg over 4 hours (40 drops/minute)2nd infusion (given over 8 hours); 8 hours after 1st infusion:500 ml dextrose 10% + quinine 10 mg/kg over 8 hours (20 drops/minute)3rd infusion(given over 8 hours); 8 hours after 2nd infusion):500 ml dextrose 10% + quinine 10 mg/kg over 8 hours(20 drops/minute)
D2Give 3 infusions at 8-hours intervals, identical to the 3rd infusion of D1:
500 ml dextrose 10% + quinine 10 mg/kg (20 drops/minute)
From D3 to D7If the patient has regained consciousness and is able to take oral tablets:STOP THE INFUSION
• Give quinine 10mg/kg x 3 times per day (every 8 hours) to complete a 7 days course• Doxycycline/tetracycline100mg for adult x 2 time per day (every 24 hours) to complete 7 days course
If the patient has not recovered from coma:• Give drugs and infusions as on D2

National Treatment Guidelines for Malaria in Cambodia 30
13.10 Pre-referral treatment for severe malaria with rectal artesunateIf complete treatment with IV AS or IM AM is not possible, patients with severe malaria should be given pre-referral treatment with rectal AS and referred immediately to an appropriate facility (usually a referral hospital or former district hospital). If referral is impossible, rectal AS treatment should be continued until the patient can tolerate oral medication; at this point, a full course of the recommended ACT for uncomplicated malaria should be given.
13.11 Dosing of pre-referral AS suppositoriesHealth workers and volunteers such as village malaria workers and mobile malaria workers play an important role in recognizing symptoms of malaria and initiating early treatment after a positive diagnosis. Another important role of VMWs/MMWs is to recognize the danger signs of severe malaria that can threaten the life of children and adults. Although the best treatment for severe malaria is intravenous artesunate, pre-referral treatment allows the first dose of medicine to be given earlier. This is significant since the risk of death is greatest in the first 24 hours after diagnosis and patients often delay seeking treatment. It is crucial to begin treatment severe malaria before patients are referred.
The 10 mg/kg body weight single dose of artesunate suppository should be administered rectally as soon as the presumptive diagnosis of severe malaria is made.
Table 13.4: Pre-referral AS dosing
Weight (kg) Age (years) Total dose Artesunate suppository used (mg)
No. of suppositories
≤ 5 3 m ≤ -<1 yr 50 50 1>5≤ 10 1 yr ≤ -< 5 yrs 100 50 2>10≤ 20 5 yrs ≤ -< 14 yrs 200 200 1>20≤ 40
>15 yrs 400 200 2>40≤ 60 600 200 3
If an artesunate suppository is expelled from the rectum within 30 min of insertion, a second suppository should be inserted and, especially in young children, the buttocks should be held together for 10 min to ensure retention of the rectal dose of artesunate.Before referring, fill out the referral form including dosage and timing of drug given.
13.12 General management of severe malariaThe following measures should be taken for all patients with clinically diagnosed or suspected severe malaria:
• Make a rapid clinical assessment, with special attention to the general condition and level of consciousness, blood pressure, rate and depth of respiration and
31 National Treatment Guidelines for Malaria in Cambodia
pallor. Assess neck stiffness and examine for rash to exclude alternative diagnoses.• Admit the patient to an acute illness ward or room; or next to the nurses’ station in
a general ward for close monitoring. However if indicated and available, admit the patient to an intensive care unit.
• Make a rapid initial check of the blood glucose level, correct hypoglycaemia if present, and then monitor frequently for hypoglycemia.
• If possible, examine the optic fundi. Retinal whitening, vascular changes or haemorrhages, if present, will help diagnosis. The examination will rarely reveal papilloedema, which is a contraindication to a lumbar puncture
• Treat seizures with a benzodiazepine (intravenous diazepam, midazolam or lorazepam). If a seizure episode persists longer than 10min after the first dose, give a second dose of a benzodiazepine (diazepam, midazolam or lorazepam).
• If parasitological confirmation of malaria is not readily feasible, make a blood film and start treatment for severe malaria on the basis of the clinical presentation.
• Provide good nursing care. This is vital, especially if the patient is unconscious• Pay careful attention to the patient’s fluid balance in severe malaria in order to avoid
over- or underhydration. • Make sure to look for other treatable causes of coma. Meningitis should be excluded
by lumbar puncture. If lumbar puncture is contraindicated or not feasible, the patient should receive presumptive antibiotic treatment.
• Look for and manage any other complicating or associated infections.• Record urine output, and look for the appearance of brown or black urine
(haemoglobinuria) or oliguria, which may indicate acute kidney injury.• Monitor the therapeutic response, both clinical and parasitological, by regular
observation and blood films.• Monitor the core temperature (preferably rectal), respiratory rate and depth, pulse,
blood pressure and level of consciousness regularly. These observations will allow• Identification of complications such as hypoglycemia, metabolic acidosis (indicated
by the presence or development of deep breathing), pulmonary edema and hypotensive shock. In children, a capillary refill time of > 2s, often associated with other signs of impaired perfusion, defines a high-risk group that should be monitored closely.
• Reduce high body temperatures (> 39°C) by administering paracetamol as an antipyretic. Tepid sponging and fanning may make the patient comfortable.
• Carry out regular laboratory evaluation of erythrocyte volume fraction (hematocrit) or hemoglobin concentration, glucose, urea or creatinine and electrolytes.
• Avoid drugs that increase the risk for gastrointestinal bleeding (aspirin, corticosteroids).

National Treatment Guidelines for Malaria in Cambodia 32
14. CLINICAL AND ADJUNCTIVE TREATMENT FOR SEVERE MALARIA
Clinical care of a severe malaria patient relies on a daily clinical examination, looking for the clinical improvement of the patient compared to admission day. Various adjunctive treatments are recommended to manage severe malaria patients as follows:
Table 14.1: Adjunctive treatments for severe malaria
Condition Management
Coma
Maintain airway. Place patient on his/her side. Remove dentures. Exclude other treatable causes of coma such as hypoglycemia, bacterial meningitis Assess and monitor coma by using the modified Glasgow coma scale for adults or Blantyre coma scale for children. Consider lumbar puncture if cause of coma is not clear
HyperpyrexiaAdminister tepid sponging, fanning or cooling blanket and antipyretic drugs. Paracetamol is preferred over nephrotoxic drugs such as non-ste-roidal anti-inflammatory agents.
HypoglycemiaCheck blood glucose at least every 4 hours. Hypoglycaemia should be sus-pected and treated presumptively in any patient that deteriorates suddenly. Correct hypoglycaemia with glucose containing infusion
Severe anemia Transfuse with screened fresh whole blood
Acute pulmonary edemaProp patient up to 45º by elevating head of bed or using pillows. Give supplementary oxygen. Intubate and use mechanical ventilation for life threatening hypoxemia.
Acute renal failureExclude and treat other causes of renal failure. Avoid NSAIDs and check fluid balance. If available, use haemodialysis or peritoneal dialysis for life threatening renal failure.
Spontaneous bleeding/
coagulapathy
Give vitamin K injection if available. Consider transfusion with blood
products which can reduce coagulopathy such as fresh whole blood, cryo-
precipitate, fresh frozen plasma and platelets.
Metabolic acidosis Exclude or treat hypoglycaemia, septicemia. If severe, consider dialysis.
ShockSuspect septicemia, take blood for cultures; give parenteral broad-spec-
trum antimicrobials, correct haemodynamic disturbances.

33 National Treatment Guidelines for Malaria in Cambodia
14.1 Parasitological monitoring in severe malariaDespite the documented existence of artemisinin resistant P. falciparum uncomplicated malaria cases throughout Southeast Asia, at the time that these guidelines are written, there has not been a clearly demonstrated case of artemisinin/artesunate resistance in severe P. falciparum malaria. Aside from the question of resistance, even if given the correct malaria medication for severe malaria, patients may not respond to treatment.
The best way to monitor patient response is to conduct at least daily blood smears to calculate parasite burden and provide appropriate supportive care.
• All patients with severe malaria should have a daily blood slide performed until there are 2 consecutive negative slides.• All patients should have a blood film on D7 to assure that malaria parasites have cleared. • Consider substituting IV quinine if parasite response is not adequate. • The finding of gametocytes alone (i.e. no asexual form) on a D7 blood slide should not be considered a sign of poor parasitological response or treatment failure; no special treatment is needed.
14.2 Treatment of severe malaria in pregnant womenSevere malaria in pregnancy is associated with much higher mortality rates and carries the risk of congenital malaria, low birth weight and fetal death. Antimalarial treatment, either by infusion of IM injection, should be given to pregnant women with severe malaria as soon as possible after diagnosis. Despite this, the most overriding factor in treating pregnant women with severe malaria is to administer whichever drug (artesunate, artemether or quinine) is most readily available in pregnant women with severe symptoms.
• For pregnant patients in the 2nd or 3rd trimester:o IV or IM artesunate or artemether should be given without delay to women in the 2nd or 3rd trimester of pregnancy and is preferred over IV quinine (see dosing for IV/IM artesunate and IM artemether, see section 13, “ TREATMENT OF SEVERE MALARIA”o Continue IV or IM treatment for a minimum of 24 hours. o When the patient can take oral medicines, discontinue IV/IM treatment (after a minimum of 24 hours, and administer full 3 days course either DHA+PPQ or AS+MQ FDC depending on region where malaria was acquired.
• For patients in the 1st trimester of pregnancyo Quinine is safe in the first trimester,o If the patient is unsure whether she is in the 1st or 2nd trimester of pregnancy it is acceptable to give IV or IM artesunate because of the risk of hygoglycemia associated with quinineo When the patient can take oral medicine, give quinine

National Treatment Guidelines for Malaria in Cambodia 34
15. MALARIA DIAGNOSIS AND TREAMTNET IN COMMUNITY (VMW/MMW) AND PRIVATE SECTOR
15.1 Village Malaria Worker (VMW)/Mobile Malaria Worker (MMW)Decision Chart for malaria diagnosis and treatment
Malaria is suspected in the following features/conditions:1. Has a typical malaria symptom: Fever + Chill + Sweating (3 major signs) or2. Has periodic fever: Fever occuring at repeated cycle every day or3. Has one of the major signs or other minor signs or4. Has stayed or crossed a malaria endemic area in the last month
RDT/MICROSCOPY TEST
TEST (+) TEST (-)
Pf/Pv/Mix
Simple Malaria
Follow NTG for simple malaria
treatment
Refer toHP/HC/FDH for malar-
ia treatment
Refer to HP/HC/FDH fro treatment of other diseases
Severe malaria * or malaria in 1st trimester pregnancy*
or patient took anti-malaria drug in the past month**
* Severe malaria or first trimester pregnancy or unknown age of pregnancy must be referred to public health facility
** If patient took anti-malaria drug in the past month, this patient must be referred to public health facility

35 National Treatment Guidelines for Malaria in Cambodia
15.2 PRIVATE SECTORCambodia’s “National Strategic Plan for Elimination of Malaria 2011-2025” calls for the gradual prohibition of all antimalarials through the private sector outlets. Accordingly, after December 2015, CNM will allow treatment by private sector only in registered outlets. This ban will be carefully considered as CNM moves from control to elimination.
It is understood that patients will continue to seek care in private sector outlets, and these cases threaten to undermine the success of pre-elimination efforts if not closely monitored and supported. Therefore the ban on treatment at private facilities will be prioritized in areas implementing pre-elimination activities. Registered private outlets which can assure directly observed therapy and establish reliable referral systems will be permitted to continue functioning.
Regardless, registered private sector outlets at the community level are only permitted to treat uncomplicated, non-pregnant patients and those older than five years of age and must report caseload data to the public sector.
All other patients must be referred to the nearest appropriate public sector as shown in Figure 2: “Referral patterns and required treatment capabilities by health facility type”.
Responsibility of health care system in malaria case management
Clinical Manifestations
Health service where treatment is indicated
RH/FDH HC/HP VMW/MMW Private***
Uncomplicated malaria Yes Yes Yes Yes
Malaria in pregnancy Yes Yes Yes Refer to public sector
Malaria in children under 5 years old Yes Yes Yes Refer to public
sector
Severe and complicated malaria Yes Artesunate Suppository & Refer
*** Ban on sale of all anti -malarial drugs in private sector after 2015
16. DIRECLY OBSERVED THERAPY (DOT)Drug resistant malaria can be caused when patients do not take all of their medicines, increasing the chance that malaria is not completely cured. Where feasible, patients should be observed taking all of their medicines. In order of descending priority: DOT should be implemented for:
National Treatment Guidelines for Malaria in Cambodia 36
• All doses of first line treatments to treat acute blood stages, according to these guidelines. In most cases this means observing 3 daily doses of ACT treatments. • First three days’ dosing for second line therapy (quinine-doxycycline)• If patient’s G6PD status is known, low dose PQ for all P. falciparum cases• If patient’s G6PD status is known, standard dose PQ to prevent P. vivax and P. ovale relapses
Patients should be observed taking their antimalarial medication and for one hour after each dose to ensure they tolerate the medication well without vomiting
17. QUALITY OF ANTIMALARIAL MEDICINESArtemisinin and its derivatives are inherently unstable, causing breakdown of the active components, especially under the tropical conditions common on Cambodia. This emphasizes the need to store ACTs and other antimalarial medicines under proper conditions and to ensure that medicines are replaced before their expiration date.
Counterfeit antimalarial tablets and ampoules containing no or minimal amounts of active pharmaceutical ingredients are also a major problem in some areas. These issues may lead to under-dosage, and may result in fatal delays in appropriate treatment. Substandard quality and incomplete dosages have the potential to lead to a failure in cure with a 3 day regimen leading to the mistaken impression of resistance. Simultaneously this may also be contributing to the actual development of resistance by delivering suboptimal dosing.
18. SCREENING OF PREGNANT WOMEN• In high prevalence areas, consideration should be given to screening pregnant
women during ante-natal visits. The frequency of ANC screenings should be determined by local malaria epidemiology and logistical factors
• In high prevalence areas, consideration should be given to community level (VMW based) screening of pregnant women during 2nd and 3rd trimester of pregnancy.
19. CHEMOPROPHYLAXIS • Because malaria transmission remains relatively low in Cambodia, CNM does not recommend the routine use of chemoprophylaxis, although mosquito avoidance and use of personal protective measures are warranted. • Travelers may wish to refer to resources at the US Centers for Disease Control and Prevention for further information (http://www.cdc.gov/malaria/travelers/).

37 National Treatment Guidelines for Malaria in Cambodia
20. REFERENCESDrugs for Neglected Diseases Initiative. (2012, Sept). Fixed-dose combination of
Artesunate and Mefloquine: a new effective tool in the fight against malaria. Retrieved from http://www.dndi.org/images/stories/pdf_products/ASMQ/ASMQ%20FDC%20scientific%20document.pdf
Dondorp A, et al. South East Asian Quinine Artesunate Malaria Trial (SEAQUAMAT) group ; Artesunate versus quinine for Treatment of severe falciparum malaria: A randomized trial. Lancet, 366(9487), 717-725.
Dundorp A, et al. Artesunate vs. quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open label randomized clinical trial. Lancet, 376(9753), 1647-57.
Medicines for Malaria Venture. (2013). Injectable artesunate tool kit. Retrieved from Medicines for Malaria Venture: http://www.mmv.org/sites/default/files/uploads/docs/access/Injectable_Artesunate_Tool_Kit/InjectableArtesunate_userguideEN.pdf
National Malaria Center. (2012). Retrieved from National Treatment Guidelines for Malaria, Kingdom of Cambodia: http://www.cnm.gov.kh/index.php?action=ID106
Newman. (2013, October). Implementation of Low Dose Primaquine as a Gametocytocide in sub-Saharan Africa . Retrieved from Global Health Sciences: http://globalhealthsciences.ucsf.edu/sites/default/files/content/ghg/mei-primaquine-report.pdf
World Health Organization. (2010). Guidelines for the treatment of malaria. Second edition. Retrieved from http://www.who.int/malaria/publications/atoz/9789241547925/en/
World Health Organization. (2012). Single dose Primaquine as a gametocytocide in Plasmodium falciparum malaria. Retrieved from http://www.who.int/malaria/pq_updated_policy_recommendation_en_102012.pdf
World Health Organization. (2012). WHO Evidence Review Group: The Safety and Effectiveness of Single Dose Primaquine as a P. falciparum gametocytocide. Retrieved from http://www.who.int/malaria/mpac/sep2012/primaquine_single_dose_pf_erg_meeting_report_aug2012.pdf?ua=1
World Health Organization. (2013, Apr). Management of severe malaria – A practical handbook. Third edition. Retrieved from http://apps.who.int/iris/bitstream/10665/79317/1/9789241548526_eng.pdf?ua=1

National Treatment Guidelines for Malaria in Cambodia 38
21. A
nnex
ATa
ble
A1: R
ecom
men
ded
trea
tmen
t reg
imen
s fo
r un
com
plic
ated
P. f
alci
paru
m m
alar
ia
Mal
aria
D
iagn
osis
Reg
ion
Infe
ctio
n A
cqui
red
whe
re
drug
s w
ork
Rec
omm
ende
d an
timal
aria
l re
gim
en
Rec
omm
ende
d D
ose
(RH
/FD
H,H
C/H
P, V
MW
/M
MW
)Fo
llow
up
+
com
men
ts
Wei
ght (
kg)
Day
1D
ay 2
Day
3If
a p
atie
nt re
turn
s with
sym
p-to
ms,
it m
ay b
e a
diff
eren
t dise
ase
or th
e pa
tient
did
not
take
the
treat
men
t app
ropr
iate
ly (i
nade
-qu
ate
abso
rptio
n or
inco
mpl
ete
treat
men
t).If
the
patie
nt’s
com
plia
nce
is do
ubtfu
l, th
en re
-trea
t with
sam
e re
gim
enIf
pat
ient
was
com
plia
nt a
nd
com
es b
ack
befo
re th
e 28
th d
ay
afte
r tre
atm
ent,
give
qui
nine
+
doxy
/tet
racy
clin
eIf
the
patie
nt re
turn
s afte
r the
28
th d
ay a
fter t
reat
men
t with
a
new
mal
aria
dia
gnos
is tre
at w
ith
the
sam
e re
gim
en
Repe
at P
Q d
osin
g fo
r eac
h ne
w
mal
aria
dia
gnos
is
Firs
t lin
e tre
atm
ent:
Unc
ompl
icat
ed
P. fa
lcip
arum
or
mix
ed in
fect
ion
(ie c
onta
inin
g P.
falc
ipar
um +
se
cond
spec
ies)
Cur
rent
ly
sugg
este
d: P
ailin
, Ba
ttam
bang
, O
ddar
Mea
nche
y, Pr
eah
Vih
ear,
Purs
at, …
ASM
Q-fi
xed
dose
co
mbi
natio
n (F
DC
)
AS:
12
mg/
kg/3
day
sM
Q: 2
5 m
g/kg
/3 d
ays
1 sm
all t
able
t: 25
mg
AS
and
50 m
g M
Q1
1 la
rge
tabl
et: 1
00 m
g A
S an
d 20
0 m
g M
Q
In g
ener
alA
S: 4
mg/
kgM
Q: 8
mg/
kgA
S: 4
mg/
kgM
Q: 8
mg/
kgA
S: 4
mg/
kgM
Q: 8
mg/
kg
5-<
91
smal
l tab
1
smal
l tab
1 sm
all t
ab
9-<
182
smal
l tab
s 2
smal
l tab
s2
smal
l tab
s
19-<
30 k
g1
larg
e ta
b 1
larg
e ta
b1
larg
e ta
b
>30
kg
2 la
rge
tabs
2
larg
e ta
bs2
larg
e ta
bs
All
othe
rs (e
xcep
t Pa
ilin,
Bat
tam
-ba
ng, O
ddar
M
eanc
hey,
Prea
h V
ihea
r Pur
sat)
DH
A-P
IP
DH
A: 2
-4 m
g/kg
/3
days
PIP:
20
mg/
kg/3
day
s
1 Ta
blet
: 40
mg
DH
A
and
320
mg
PIP
5-<
101/
2 ta
b1/
2 ta
b1/
2 ta
b
10-<
191
tab
1 ta
b1
tab
19-<
301
½ ta
bs1
½ ta
bs1
½ ta
bs
30-<
402
tabs
2 ta
bs2
tabs
40-<
603
tabs
3 ta
bs3
tabs
≥60
4 ta
bs4
tabs
4 ta
bs
Unc
ompl
icat
ed
P.fa
lcip
arum
All
Low
dos
e Pr
imaq
uine
(fo
r tra
nsm
issio
n bl
ocki
ng)
1 ta
blet
: 15
mg
<10
No
dosin
g gi
ven
• Prim
aqui
ne (l
ow d
ose)
, to
be
used
onl
y if
safe
ty st
udy
confi
rmed
• Spe
cial
per
miss
ion
from
CN
M
10-2
5¼
tab
(3.7
5 m
g) g
iven
on
D1
20-<
50½
tab
(7.5
mg)
giv
en o
n D
1
≥50
kg
1 ta
b (1
5 m
g) g
iven
on
D1

39 National Treatment Guidelines for Malaria in CambodiaTa
ble
A2: R
ecom
men
ded
first
line
trea
tmen
t of u
ncom
plic
ated
P.v
ivax
, ova
le o
r m
alar
ae m
alar
ia
Mal
aria
Dia
gnos
isR
egio
n In
fect
ion
Acq
uire
d
Rec
omm
ende
d an
timal
ar-
ial r
egim
en
Rec
omm
ende
d D
ose
(RH
/FD
H, H
C/H
P, V
MW
/MM
W)
Follo
w u
p +
com
men
ts
Wei
ght (
kg)
Day
1D
ay 2
Day
3
Trea
tmen
t is s
ame
as fo
r P.
falcip
arum
mala
ria
Firs
t lin
e tre
atm
ent:
Unc
ompl
icat
ed
P. v
ivax
, ova
le, o
r m
alar
iae
(Firs
t lin
e tre
atm
ent)
All
DH
A-P
IP
DH
A: 2
-4 m
g/kg
/3 d
ays
PIP:
20
mg/
kg/3
day
s
1 Ta
blet
: 40
mg
DH
A a
nd
320
mg
PIP
5-<
101/
2 ta
b1/
2 ta
b1/
2 ta
b
10-<
191
tab
1 ta
b1
tab
19-<
301
½ ta
bs1
½ ta
bs1
½ ta
bs
30-<
402
tabs
2 ta
bs2
tabs
40-<
603
tabs
3 ta
bs3
tabs
≥60
4 ta
bs4
tabs
4 ta
bs
Ant
irela
pse
or a
n-ti-
hypn
ozoi
te tr
eat-
men
t:P.
viv
ax o
r ova
le o
nly
All
Prim
aqui
ne (f
or ra
dica
l tre
at-
men
t)
1 ta
blet
: 15
mg
<10
No
dosin
g gi
ven
Prim
aqui
ne is
use
d to
kill
sle
epin
g m
alar
ia fo
rms i
n th
e liv
er (“
hypn
ozoi
tes”
) th
at c
an re
laps
e w
eek/
mon
ths a
fter t
he in
itial
in
fect
ion
It is
use
d if
pat
ient
G6P
D
stat
us is
kno
wn
to b
e no
r-m
al. I
n pr
actic
e, th
e 14
day
s tre
atm
ent i
s pre
fera
ble
≥10
0.25
mg/
kg x
14
days
OR
0.75
mg/
kg w
eekl
y x
8 w
eeks

National Treatment Guidelines for Malaria in Cambodia 40
Tabl
e A3
: Rec
omm
ende
d se
cond
line
trea
tmen
t of u
ncom
plic
ated
P. f
alci
paru
m, v
ivax
, ova
le a
nd m
alar
ae m
alar
ia
Mal
aria
D
iagn
osis
Reg
ion
Infe
ctio
n A
cqui
red
Rec
omm
ende
d an
timal
aria
l re
gim
enA
geW
eigh
t (K
g)
Num
ber o
f ta
blet
sFo
llow
up
+
com
men
ts
Qui
nine
(300
mg)
Dox
ycyc
line
(100
mg
Dos
e/
8hTo
tal/
day
Tota
l/7d
ays
Tota
l/da
y (S
ingl
e do
se)
Tota
l/7d
ays
Seco
nd li
netre
atm
ent:
All
Qui
nine
+D
oxyc
yclin
eQ
uini
ne: 1
0 m
g/kg
X
3 tim
es d
aily
X 7
day
sD
oxyc
yclin
e:• A
dults
: 200
mg
daily
X
7 d
ays
• >8-
14 y
ears
: 2m
g/kg
tw
ice
daily
X 7
day
s • ≤
8 ye
ars,
preg
nant
w
omen
: C
ontra
-in
dica
ted
< 6
mon
ths
<7
1/4
3/4
5 1/
4
Qui
nine
m
ust b
e gi
ven
for
7 da
ys fo
r cu
re
≥ 6
mon
ths-
2
year
s7-
151/
21
1/2
10 1
/2
>2
year
s-8
year
s16
-30
13
21
> 8
-<15
yea
rs31
-40
1 1/
24 1/2
31 1
/21
7
≥ 1
5 ye
ars
>40
26
422
14
Qui
nine
+Te
trac
yclin
e
Qui
nine
: 10
mg/
kg X
3
times
dai
ly X
7 d
ays
Tetra
cycl
ine:
• Adu
lts a
nd c
hild
ren:
8.
3 m
g/kg
X 3
tim
es
daily
X 7
day
s • ≤
8 ye
ars,
preg
nant
w
omen
: C
ontra
-in
dica
ted
Qui
nine
(300
mg)
Tetr
acyc
line
(250
mg)
Dos
e /8
hTo
tal
/day
Tota
l/7
days
Dos
e/8
hTo
tal
/day
Tota
l/7
days
< 6
mon
ths
<7
1/4
3/4
5 1/
4
≥ 6
mon
ths-
2
year
s7-
151/
21 1/2
10 1
/2
>2
year
s-8
year
s16
-30
13
21
> 8
-<15
yea
rs31
-40
1 1/
24 1/2
31 1
/21
1/2
4 1/
231
1/2
≥ 1
5 ye
ars
>40
26
422
642
Unc
ompl
icat
ed
P. o
vale
or
viva
xA
llPr
imaq
uine
(for
radi
cal
treat
men
t) 1
tabl
et: 1
5 m
g
< 1
0 N
o do
sing
giv
enSe
e co
mm
ent
at T
able
A2
≥10
0.25
mg/
kg x
14
days
OR
0.7
5 m
g/kg
wee
kly
x 8
wee
ks

41 National Treatment Guidelines for Malaria in Cambodia
Tabl
e A4
: Rec
omm
ende
d tr
eatm
ent r
egim
en fo
r un
com
plic
ated
mal
aria
in p
regn
ancy
Mal
aria
Dia
gnos
isR
egio
n In
fect
ion
Ac-
quire
dR
ecom
men
ded
an
timal
aria
l reg
-imen
R
ecom
men
ded
dose
Preg
nant
wom
en
(unc
ompl
icat
ed, fi
rst
trim
este
r)A
ll Q
uini
ne su
lfate
alo
ne
Qui
nine
Tetra
cycl
ine
and
do
xycy
clin
e ar
e
cont
rain
dica
ted
in
preg
nanc
y
Preg
nant
wom
en
(unc
ompl
icat
ed, 2
nd a
nd 3
rd
trim
este
rs)
Follo
w
reco
mm
enda
tion
for
unco
mpl
icat
ed
mal
aria
acc
ordi
ng
to re
gion
ASM
Q F
DC
or D
HA
-PIP
Follo
win
g do
sing
re
com
men
ded
abov
e


Copy right by National Center for Malaria Control, Parasitology and Entomology (CNM)
Corner Street 92, Trapaing Svay Village, Sangkat Phnom Penh Thmey, Khan Sen Sok
E-mail: [email protected]:www.cnm.gov.kh

![Severe Malaria: North American Perspective...aggressively. The Glasgow coma scale in adults and Blantyre coma scale in children is useful for determining the level of impaired consciousness.[1]](https://static.fdocuments.in/doc/165x107/5e6c4948e97f9a3cc14d24a1/severe-malaria-north-american-perspective-aggressively-the-glasgow-coma-scale.jpg)









![Can the Assessment of Malaria Severity be Simplified for ... · The status of consciousness was assessed using Blantyre coma scale [22] and the revised Glasgow coma scale (scores](https://static.fdocuments.in/doc/165x107/5aef9dfb7f8b9a572b8e61ec/can-the-assessment-of-malaria-severity-be-simplified-for-status-of-consciousness.jpg)




![Can the Assessment of Malaria Severity be Simplified for ......The status of consciousness was assessed using Blantyre coma scale [22] and the revised Glasgow coma scale (scores 3](https://static.fdocuments.in/doc/165x107/5e6c4945e97f9a3cc14d248d/can-the-assessment-of-malaria-severity-be-simplified-for-the-status-of-consciousness.jpg)
