
National Survey of Drug -Resistant Tuberculosis in...
47
National Survey of Drug-Resistant Tuberculosis in China Dr. Yanlin Zhao National Centre for Tuberculosis Control and Prevention of China CDC National TB Reference Laboratory , China CDC
Transcript of National Survey of Drug -Resistant Tuberculosis in...

National Survey of Drug-Resistant Tuberculosis in China
Dr. Yanlin Zhao National Centre for Tuberculosis Control and Prevention of
China CDC National TB Reference Laboratory , China CDC
BACKGROUND • China lists as 2nd among the 22 TB high-burden countries. • In 1979, 1984/1985, 1990, 2000, nationwide epidemiological
prevalence survey. • Prevalence survey in 2000 shows 18.6% of initial resistance
and 46.5% acquired resistance. • During 1996~2008, 13 province have taken part in drug-
resistance surveillance organized by WHO/IUATLD . Initial: 14.8%~42.1%; Acquired: 33.7%~66%
• Estimation of MDR-TB in China: 5.0%, 26%

Objectives
1. To interpret the epidemiological status of drug resistant tuberculosis in China
2. To analyze the risk factor for drug resistance occurrence among tuberculosis patients
3. To explore the predominant mycobacterium bacillus biological characteristics in China
4. To understand the micro-evolution of the prevalent strains in China.
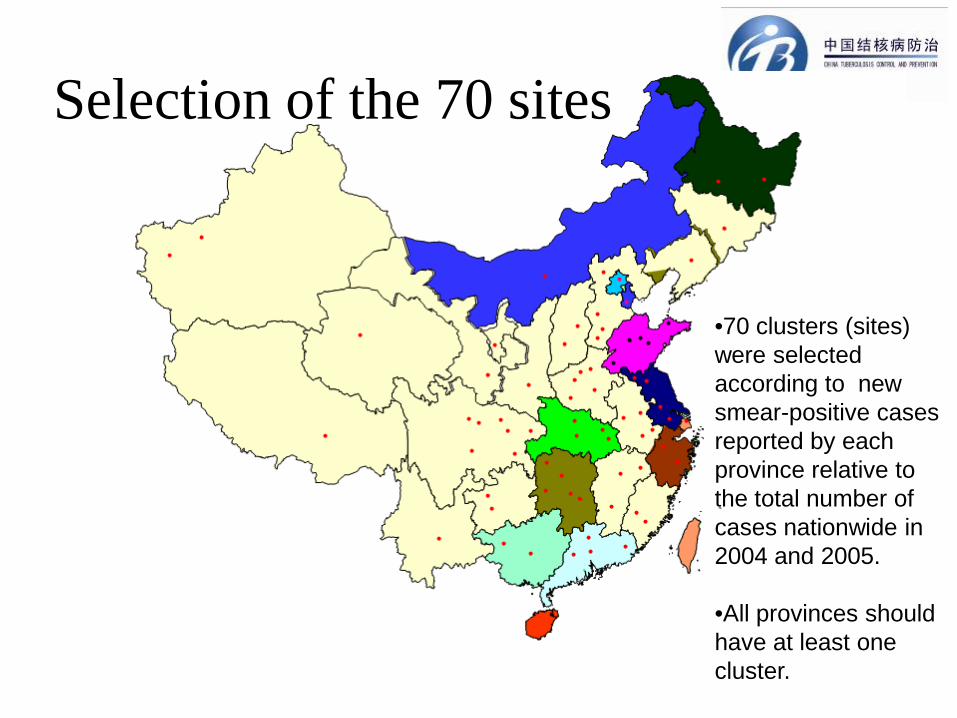
Selection of the 70 sites
•70 clusters (sites) were selected according to new smear-positive cases reported by each province relative to the total number of cases nationwide in 2004 and 2005.
•All provinces should have at least one cluster.
1.70 clusters(counties) from all 31 provinces
2.51 smear positive new cases and 17 smear
positive retreatment cases with newly diagnosed
3. DST(proportion method) against 6 anti-TB
drugs
Method
5 1/29/2013
• Design and preparation
2 Pilots

Design and Preparation
Experience and lessons

Design and preparation
• Training objectives: all persons(about 700 persons) involved in this survey
• Training contents: Interaction method, role play and practice


Resource of reagents and disposables for the
laboratory
Anti-TB baseline survey lauching meeting ( 1st Apr. 2007)
Record files and register book
Logistics
• Monthly report • Newsletter • special email address • special fixed telephone • fixed people 24h response • established reporting and recording feedback machanism
Quality assurrance
• Leader group • Experts panel • Executive office • Standardization of definition • Standardization of methods • Standardization of the parameters of the equipment, reagents and disposals Standardization of the implementation period of the
time

Supervision Supervision for all clusters, Special supports to priority sites( 2 people from central level work in Tibet 3 weeks)

Strain files management

Strain logistic box special vehicle
Consent informs Questionaires

• Panel testing for all persons who are
responsible for DST • Panel testing from Hongkong Supernational
Reference Laboratory
Database of investigation
Data input double blinded input the data by Peking University and 100% recheck by NRL
DST work in NRL
•Lowenstein-Jensen (L-J) media and proportion method was used for DST.
•6 anti-Tb drugs were included: sonazied(INH), Rifampine(RFP),
Streptomycin(SM), Ethembutol(EMB), ofloxacin (Ofx); Kanamycin(Km)
Proficiency test for DST was done to NRL by Hong Kong Super-National reference laboratory .
10% of the isolates were randomly chosen to repeat DST , the outcome was eligible according to WHO’s guideline.
Species identification work in NRL
Selective L-J media method was used.
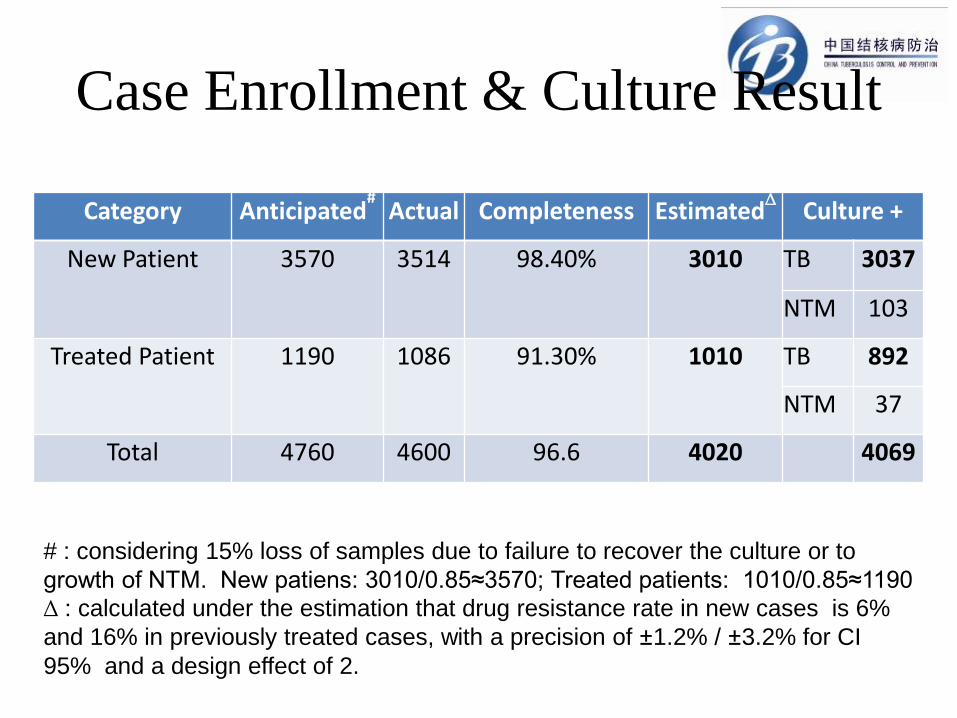
Case Enrollment & Culture Result
Category Anticipated# Actual Completeness Estimated∆ Culture +
New Patient 3570 3514 98.40% 3010 TB 3037
NTM 103
Treated Patient 1190 1086 91.30% 1010 TB 892
NTM 37
Total 4760 4600 96.6 4020 4069
# : considering 15% loss of samples due to failure to recover the culture or to growth of NTM. New patiens: 3010/0.85≈3570; Treated patients: 1010/0.85≈1190 ∆ : calculated under the estimation that drug resistance rate in new cases is 6% and 16% in previously treated cases, with a precision of ±1.2% / ±3.2% for CI 95% and a design effect of 2.
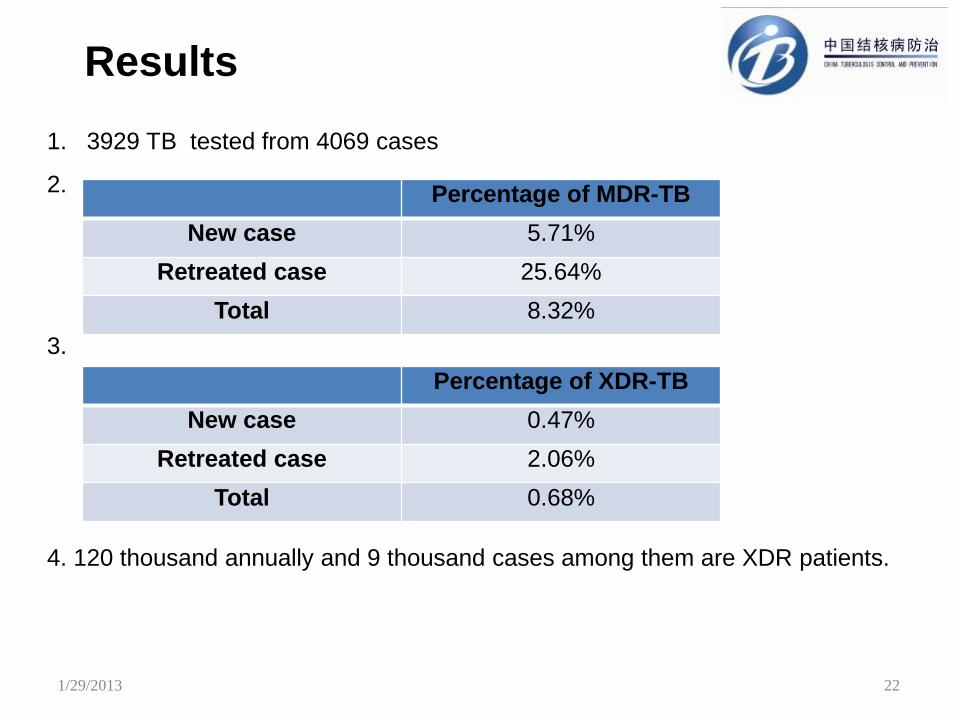
1. 3929 TB tested from 4069 cases
2.
3.
4. 120 thousand annually and 9 thousand cases among them are XDR patients.
Results
22 1/29/2013
Percentage of MDR-TB
New case 5.71%
Retreated case 25.64%
Total 8.32%
Percentage of XDR-TB
New case 0.47%
Retreated case 2.06%
Total 0.68%
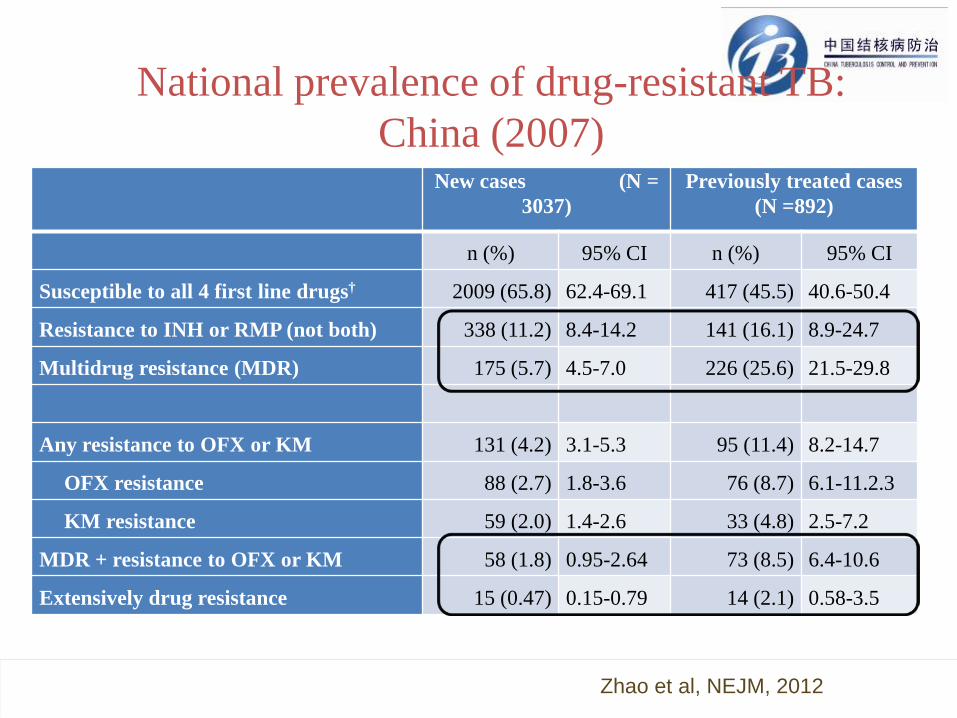
National prevalence of drug-resistant TB: China (2007)
New cases (N = 3037)
Previously treated cases (N =892)
n (%) 95% CI n (%) 95% CI
Susceptible to all 4 first line drugs† 2009 (65.8) 62.4-69.1 417 (45.5) 40.6-50.4
Resistance to INH or RMP (not both) 338 (11.2) 8.4-14.2 141 (16.1) 8.9-24.7
Multidrug resistance (MDR) 175 (5.7) 4.5-7.0 226 (25.6) 21.5-29.8
Any resistance to OFX or KM 131 (4.2) 3.1-5.3 95 (11.4) 8.2-14.7
OFX resistance 88 (2.7) 1.8-3.6 76 (8.7) 6.1-11.2.3
KM resistance 59 (2.0) 1.4-2.6 33 (4.8) 2.5-7.2
MDR + resistance to OFX or KM 58 (1.8) 0.95-2.64 73 (8.5) 6.4-10.6
Extensively drug resistance 15 (0.47) 0.15-0.79 14 (2.1) 0.58-3.5
Zhao et al, NEJM, 2012
January 29, 2013 © 2011 Bill & Melinda Gates Foundation | 24
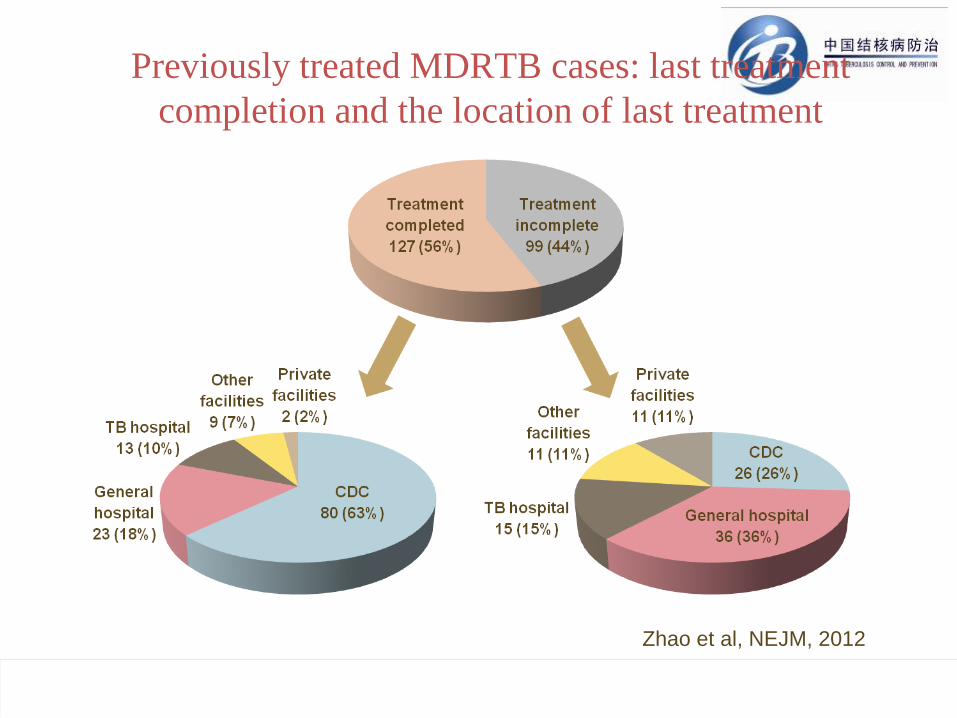
Previously treated MDRTB cases: last treatment completion and the location of last treatment
Zhao et al, NEJM, 2012
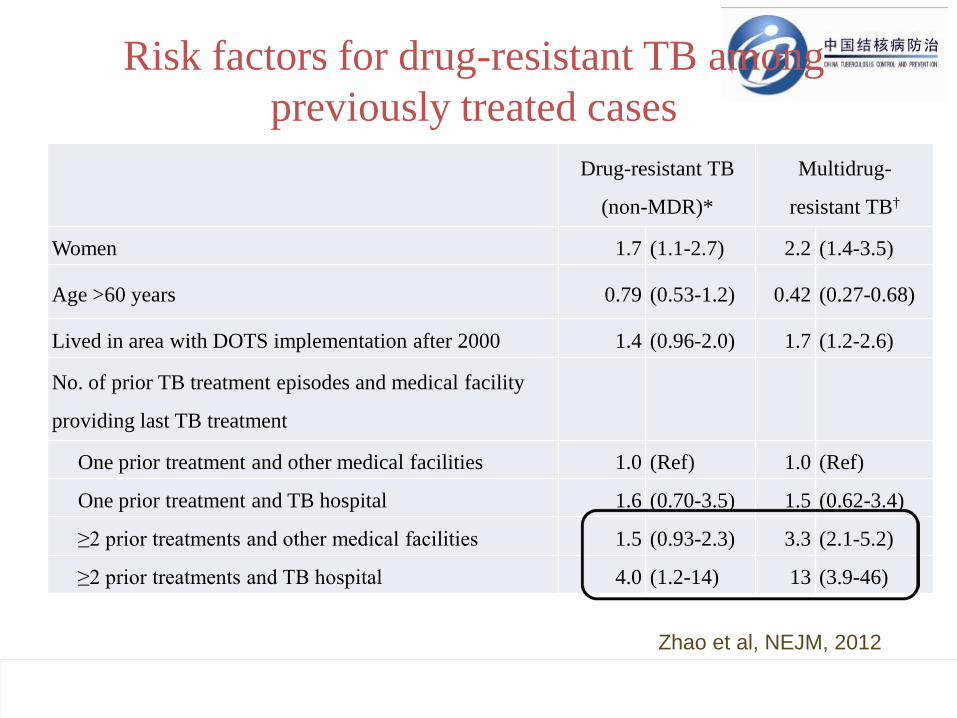
Risk factors for drug-resistant TB among previously treated cases
January 29, 2013 © 2011 Bill & Melinda Gates Foundation | 25
Drug-resistant TB
(non-MDR)*
Multidrug-
resistant TB†
Women 1.7 (1.1-2.7) 2.2 (1.4-3.5)
Age >60 years 0.79 (0.53-1.2) 0.42 (0.27-0.68)
Lived in area with DOTS implementation after 2000 1.4 (0.96-2.0) 1.7 (1.2-2.6)
No. of prior TB treatment episodes and medical facility
providing last TB treatment
One prior treatment and other medical facilities 1.0 (Ref) 1.0 (Ref)
One prior treatment and TB hospital 1.6 (0.70-3.5) 1.5 (0.62-3.4)
≥2 prior treatments and other medical facilities 1.5 (0.93-2.3) 3.3 (2.1-5.2)
≥2 prior treatments and TB hospital 4.0 (1.2-14) 13 (3.9-46)
Zhao et al, NEJM, 2012
Preventing MDRTB: new tools + system change
• Reduce sub-optimal treatment in CDC and hospital system by using treatment regimens based on resistance testing
• Make sure patients starting treatment in hospitals are followed up after discharge till they complete treatment; build linkage between hospital system and CDC system
• Improve treatment provided by TB hospitals: appropriate drug regimens, improved infection control, better follow-up after discharge
• Improve community case-management of patients on treatment (perhaps using adherence technology)
January 29, 2013 © 2011 Bill & Melinda Gates Foundation | 26

Patients evaluated for TB
No MDR
Routine treatment (1st-line drugs)
MDR
CDC system Specialized hospital
Patients evaluated for TB
No MDR M/XDR
M/XDR treatment (2nd-line drugs)
Effective case management in community
Building hospital-CDC collaboration to prevent and treat M/XDR TB

DOTS Program
(in CDC)
Diagnosis • Smear microscopy
Empiric treatment • Standardized regimen
using 1st-line drugs Community case-management
• Self or family members
Innovative
Program (CDC & hospital)
Molecular diagnosis • Rapid dx of TB • Rapid dx of MDR-TB
Treatment based on testing for resistance
• 2nd-line drugs for MDR • 1st-line FDC drugs for
non-MDR Technology-supported case-management
• Use of mobile phone & med monitor
Hospital-CDC collaboration
Quality-assured drugs
Financing model for MDRTB
Incentive model for HCW’s

Risk factors for drug-resistant TB among new cases
January 29, 2013 © 2011 Bill & Melinda Gates Foundation | 29
Drug-resistant TB
(non-MDR)*
Multidrug-
resistant TB†
Women 0.90 (0.74-1.1) 1.5 (1.0-2.1)
Age >60 years 0.88 (0.71-1.1) --- ---
Occupation as non-farmer 1.2 (0.95-1.4) 1.4 (0.97-2.0)
Lived in area with DOTS implementation after 2000 0.85 (0.71-1.0) --- ---
History of treatment with TB drugs and prior TB diagnosis
No treatment (with or without a prior TB diagnosis) 1.0 (Ref) 1.0 (Ref)
Treatment of <1 month and a prior TB diagnosis 1.6 (1.1-2.1) 1.2 (0.65-2.4)
Treatment of any duration and no prior TB diagnosis 1.2 (0.86-1.5) 2.4 (1.5-3.8)
Zhao et al, NEJM, 2012
Preventing drug-resistant TB among new cases
• Who are the patients with no prior diagnosis of TB but given TB drugs? – Likely suspected to have TB and started on TB
drugs – Did not receive a diagnosis of TB because proper
diagnosis not made – Took TB drugs long enough, but improperly,
such that MDRTB developed – Mostly treated in hospital system
• Importance of performing proper diagnosis of TB
January 29, 2013 © 2011 Bill & Melinda Gates Foundation | 30
Implications for new drug R&D • Important to “turn off the tap” of DR-TB
– Current factors causing DR-TB will lead to rapid “loss” of any new drug to resistance
• Urgency in light of new TB drugs becoming available – TMC-207, OPC67683, linozelid
– Need to improve system, adopt new diagnostics, and use new drugs in a rational manner in order to prevent DR-TB
• Level of quinolone resistance has implications for development and use of new
January 29, 2013 © 2011 Bill & Melinda Gates Foundation | 31
Questions continues…
What’s the population structure of the prevalent TB strains in China?
What advantages do they have to become the prevalent strains?
How do the prevalent strains interact with hosts and environment?
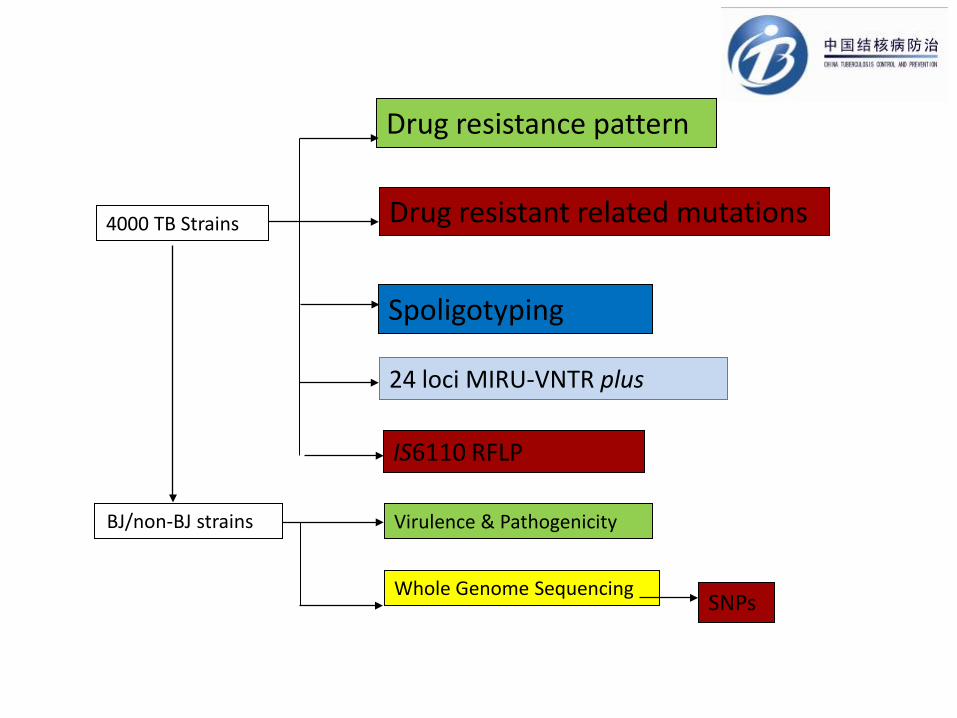
4000 TB Strains
Drug resistance pattern
Drug resistant related mutations
Spoligotyping
24 loci MIRU-VNTR plus
IS6110 RFLP
BJ/non-BJ strains Virulence & Pathogenicity
Whole Genome Sequencing SNPs


Distribution map of different spoligotypes

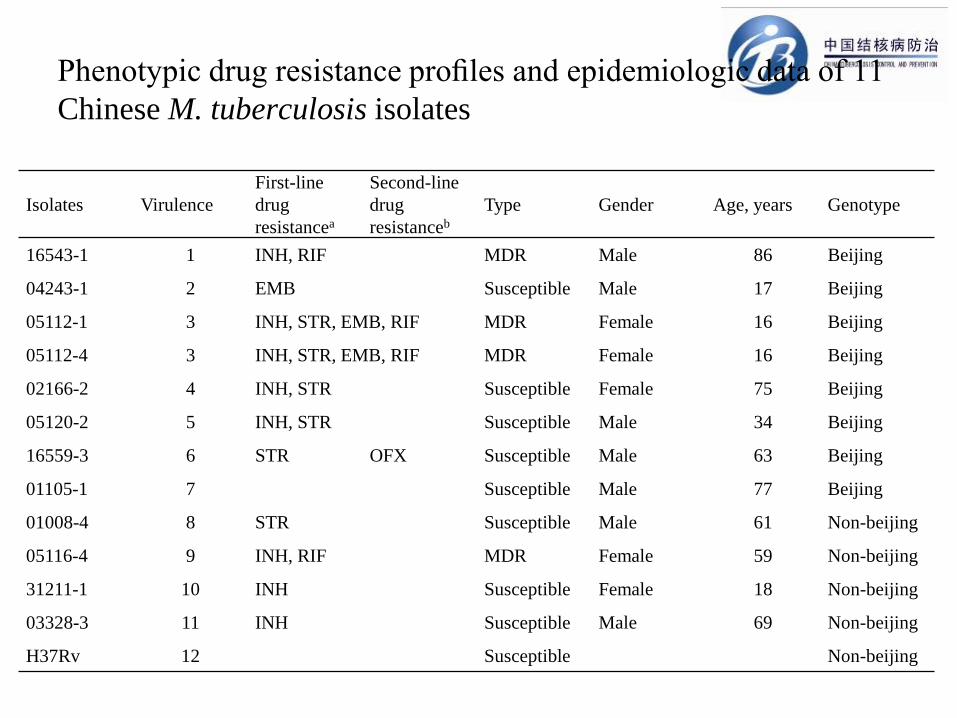
Phenotypic drug resistance profiles and epidemiologic data of 11 Chinese M. tuberculosis isolates
Isolates Virulence First-line drug resistancea
Second-line drug resistanceb
Type Gender Age, years Genotype
16543-1 1 INH, RIF MDR Male 86 Beijing
04243-1 2 EMB Susceptible Male 17 Beijing
05112-1 3 INH, STR, EMB, RIF MDR Female 16 Beijing
05112-4 3 INH, STR, EMB, RIF MDR Female 16 Beijing
02166-2 4 INH, STR Susceptible Female 75 Beijing
05120-2 5 INH, STR Susceptible Male 34 Beijing
16559-3 6 STR OFX Susceptible Male 63 Beijing
01105-1 7 Susceptible Male 77 Beijing
01008-4 8 STR Susceptible Male 61 Non-beijing
05116-4 9 INH, RIF MDR Female 59 Non-beijing
31211-1 10 INH Susceptible Female 18 Non-beijing
03328-3 11 INH Susceptible Male 69 Non-beijing
H37Rv 12 Susceptible Non-beijing
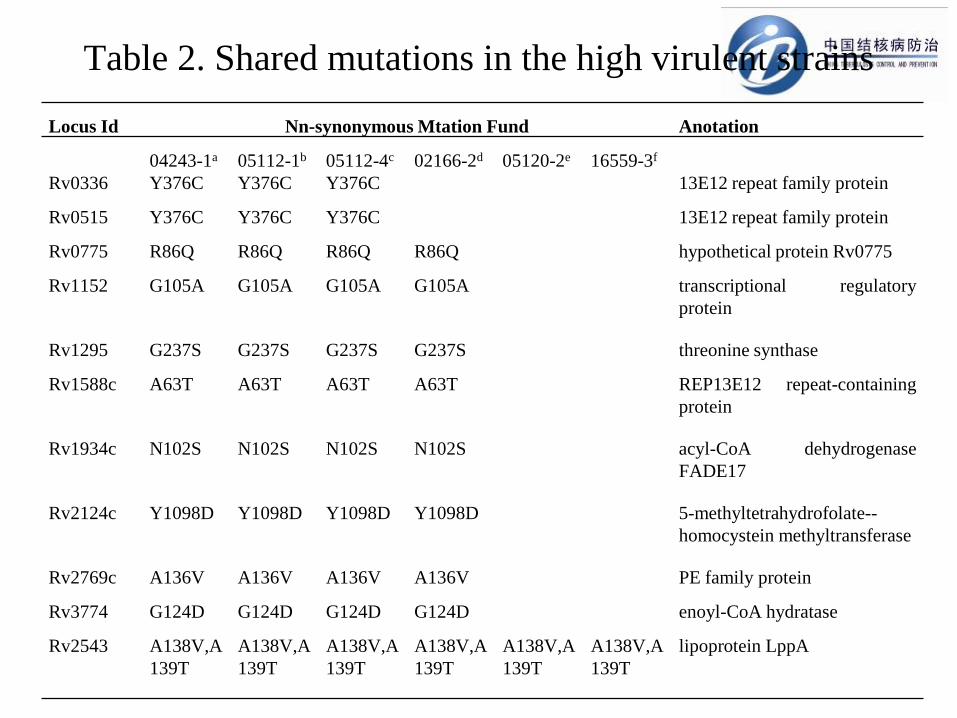
Table 2. Shared mutations in the high virulent strains Locus Id Nn-synonymous Mtation Fund Anotation
04243-1a 05112-1b 05112-4c 02166-2d 05120-2e 16559-3f Rv0336 Y376C Y376C Y376C 13E12 repeat family protein
Rv0515 Y376C Y376C Y376C 13E12 repeat family protein
Rv0775 R86Q R86Q R86Q R86Q hypothetical protein Rv0775
Rv1152 G105A G105A G105A G105A transcriptional regulatory protein
Rv1295 G237S G237S G237S G237S threonine synthase
Rv1588c A63T A63T A63T A63T REP13E12 repeat-containing protein
Rv1934c N102S N102S N102S N102S acyl-CoA dehydrogenase FADE17
Rv2124c Y1098D Y1098D Y1098D Y1098D 5-methyltetrahydrofolate--homocystein methyltransferase
Rv2769c A136V A136V A136V A136V PE family protein
Rv3774 G124D G124D G124D G124D enoyl-CoA hydratase
Rv2543 A138V,A139T
A138V,A139T
A138V,A139T
A138V,A139T
A138V,A139T
A138V,A139T
lipoprotein LppA

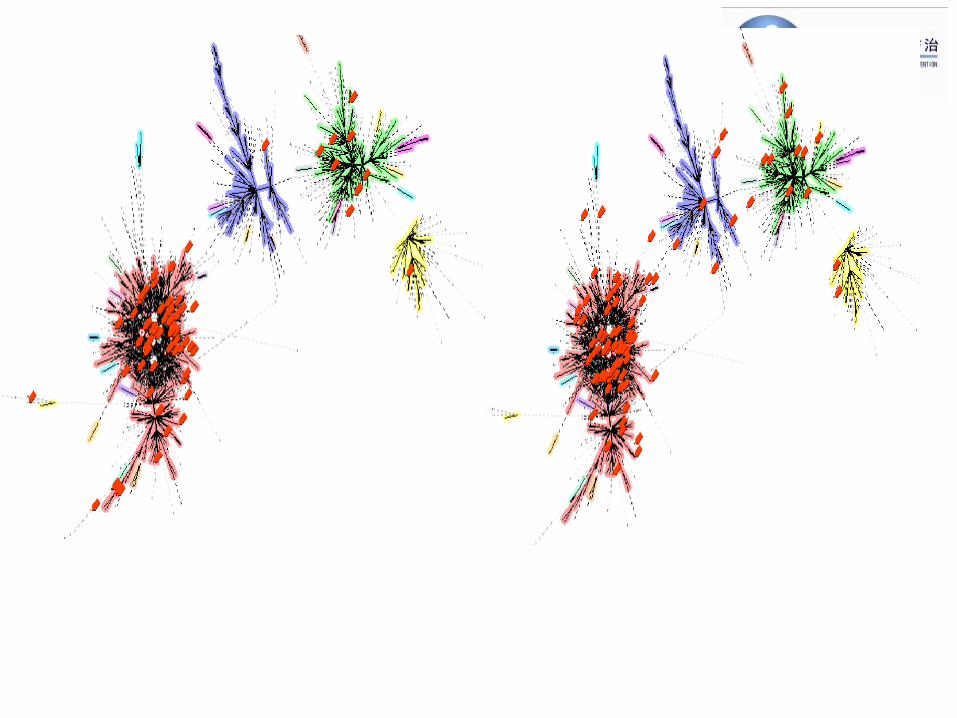
• Position of the 871 non-synonymous SNPs by excluding common SNPs in Beijing genotype and non-Beijing genotype, respectively, Positions are Relative to the M. tuberculosis H37Rv Genome Sequence (From inner to outer: 01008-4, 02166-2, 03232-3, 03328-3, 04243-1, 05112-1, 05112-4, 05116-4, 05120-2, 16559-3, 31211-1, green indicates susceptible strains, cyan indicates MDR strains)

Visible TB distribution model

大气监测数据可视化
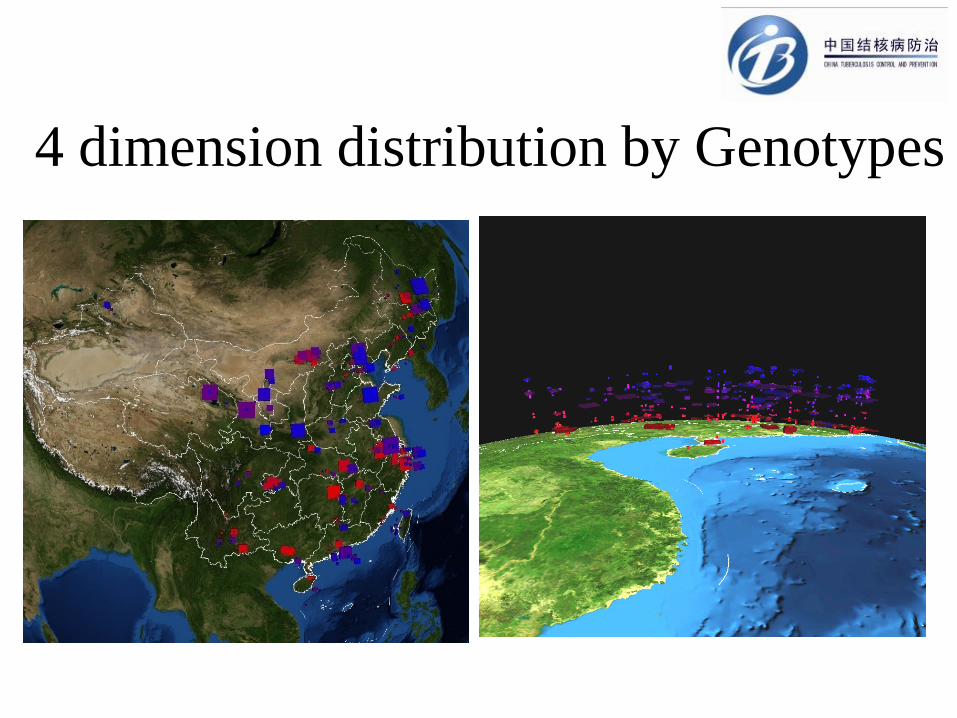
4 dimension distribution by Genotypes

分枝杆菌迁徙可视化效果图

Acknowledgement
people who made efforts and contribution to the survey
Disease Prevention and Control Center of China (CDC)
Beijing Tuberculosis and Thoracic Tumor Institute
Peking Union Medical College of China
Beijing University of China
31 provincial TB dispensary and 70 clusters