51st International Conference on Nursing and Primary Healthcare
Insert name of presentation on Master Slide
National Primary Care Conference
15 November 2018
#PrimaryCare18
Insert name of presentation on Master Slide
Transforming Access – reflections on progress across Wales
15 November 2018
#PrimaryCare18

Insert name of presentation on Master Slide
Community Pharmacy
15 November 2018
Dylan Jones
#PrimaryCare18

Community Pharmacy Independent Prescriber








72 94 107 163 128 129 140 117 105 139 112 150 159 229 112 153 118 155 1500
2
4
6
8
10
12
14
16
18
20
0
50
100
150
200
250
Da
ys
Pro
vid
ed
Co
nsu
lta
tio
ns
Service availability and consultation numbersDec 2016 to Jun 2018

Cardiac1%
CNS1%
Injury2%GI
3%Nasal
3%
Eye4% UTI
5%
Other5%
Musculo7%
Ear11%
Mouth13%
Skin20%
Respiratory25%
Condition type (Dec 2017 to Jun 2018)

GP Pharm Total GP Pharm Total GP Pharm Total
Consultation
Impact
(Yr 1 v Yr 2)
GP Impact
(Yr 1 v Yr 2)
Consultation
Impact
(Yr 1 v Yr 3)
GP Impact
(Yr 1 v Yr 3)
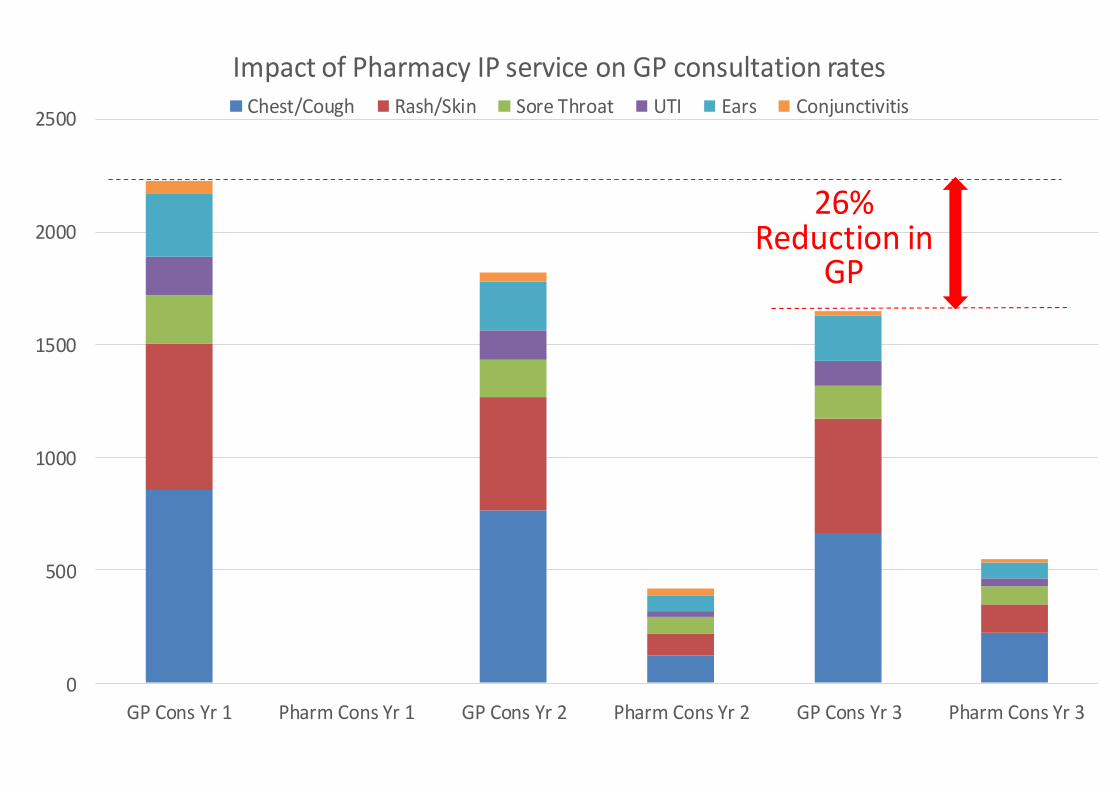
Chest/Cough 857 0 857 766 123 889 663 221 884 4% -11% 3% -23%
Rash/Skin 644 0 644 499 94 593 509 126 635 -8% -23% -1% -21%
Sore Throat 219 0 219 167 78 245 144 80 224 12% -24% 2% -34%
UTI 169 0 169 129 21 150 112 37 149 -11% -24% -12% -34%
Ears 282 0 282 220 71 291 199 72 271 3% -22% -4% -29%
Conjunctivitis 57 0 57 36 31 67 21 15 36 18% -37% -37% -63%
Total 2228 0 2228 1817 418 2235 1648 551 2199 0% -18% -1% -26%
Search strategy amended from previous searches to more accurately capture variety of data recording methods used by all prescribers.
All data periods from 1st Dec to 30th May
Dec 15 to May 16 (Yr 1) Dec 16 to May 17 (Yr 2)
Condition
Dec 17 to May 18 (Yr 3)
GP Practice on average seeing 26% less patients for these conditions Over 33% for some conditions now being seen at the pharmacy
0
500
1000
1500
2000
2500
GP Cons Yr 1 Pharm Cons Yr 1 GP Cons Yr 2 Pharm Cons Yr 2 GP Cons Yr 3 Pharm Cons Yr 3
Impact of Pharmacy IP service on GP consultation ratesChest/Cough Rash/Skin Sore Throat UTI Ears Conjunctivitis
26% Reduction in
GP
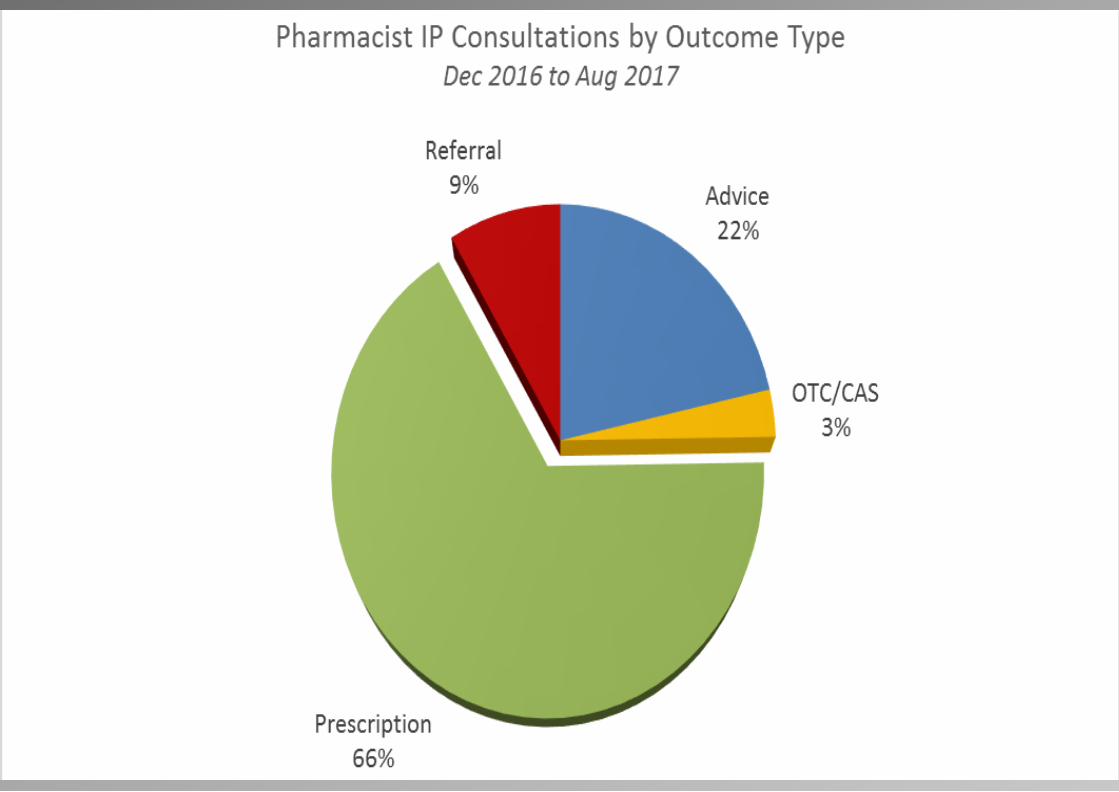
Consultation Outcomes
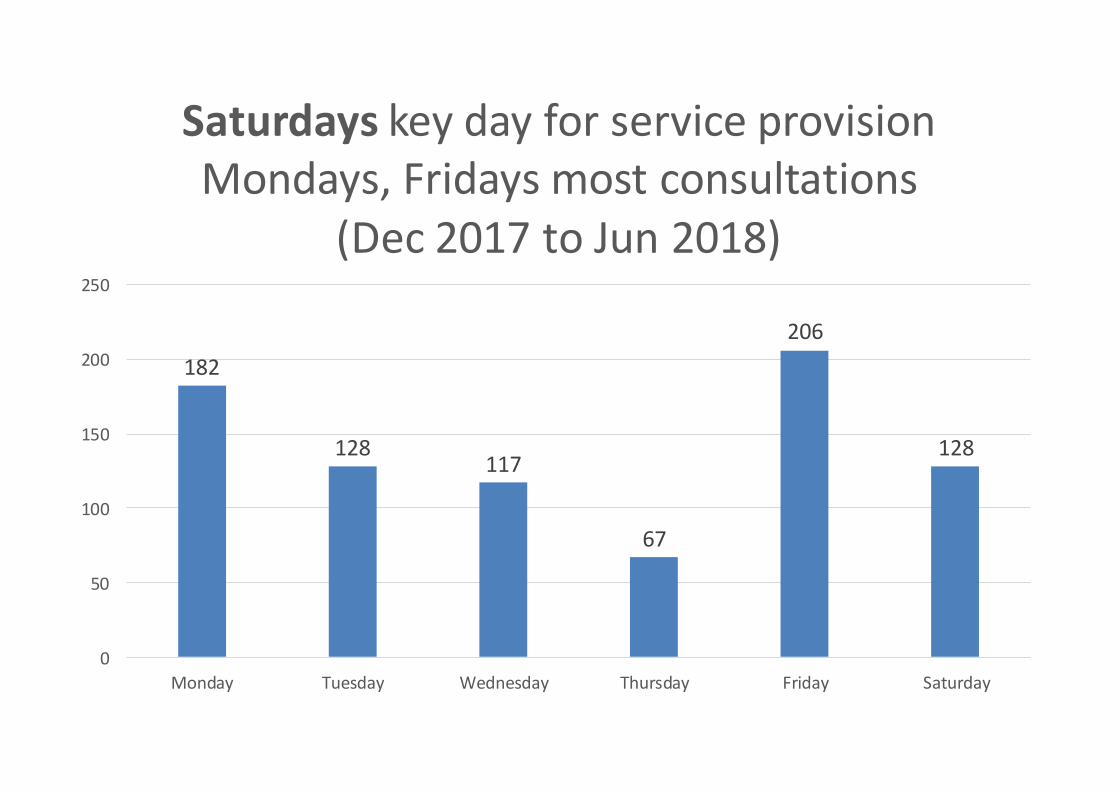
182
128117
67
206
128
0
50
100
150
200
250
Monday Tuesday Wednesday Thursday Friday Saturday
Saturdays key day for service provision Mondays, Fridays most consultations
(Dec 2017 to Jun 2018)
Examples of consultations
“Very useful service in the event of the doctors’ surgery being busy. The pharmacist was very knowledgeable, friendly and put me at ease.”



It’s not a pharmacy service…
…it’s coordinated primary health care that patients access at a pharmacy.
Insert name of presentation on
Master Slide
Community Optometry
15 November 2018
Andy Britton
#PrimaryCare18
From PEARS to WECS
Dropping a vowel but picking up more work in a
community setting
Andy Britton, Optometrist, Haverfordwest
Committed to excellence in eye care
Something old – the service before
• PEARS – Primary Eye Acute Referral Service - Optometry Led
• WEHE’s – Wales Eye Health Examination – Optometry Led
• The Wales Low Vision Service – Optometry Led
• Diabetic Retinopathy Screening – non Optometry Led
• Glaucoma Monitoring – non Optometry Led
Sheen NJ, Fone D, Phillips CJ, Sparrow JM, Pointer JS & Wild JM. Novel optometrist-led all Wales primary
eye-care services: evaluation of a prospective case series. Br J Ophthalmol.2009, 93 (4) 435-438.
A WECS / EHEW is
born!
Providing the people of Wales with:
• Eye health examinations
• Further investigations
• Follow-up services
Enhanced
Scheme
Evaluation
Project (ESEP)
How does the new service work?
• Accreditation by Wales Optometry Post Grad Education Centre
• List of accredited practices
• Three types of appointment
eye health examination
further investigations following a sight test
follow-ups to an eye health examination
• Banded fee structure commensurate with time taken
and level of skill
• In built clinical audit – Data at last!
Welsh Government Together for
Health – an Eye Care Plan for
Wales 2013-2018
Moving services where appropriate to a
community setting
Using primary care professionals to deliver eye
care services
Expanding the role of primary care based
optometrists
But What Does It Mean?
Smoking Cessation
Post Cataract Community Follow Ups
OHT and Suspect Glaucoma Monitoring
WECS/EHEW Triaging
IT Connectivity across all Practices
Local, Primary Care Based Funding
Independent Prescribing
Joint Working
Post cataract follow-up appointments in
the community: Aneurin Bevan UHB
RESULT
Over 1,600 hospital appointments per year
were saved in the past year
Follow-up appointments in the
community for patients who have
glaucoma: Aneurin Bevan UHB
RESULT
1,698 appointments freed up in hospital eye
clinic in a 4 month period
What do the patients think?
Patient satisfaction results for the glaucoma
follow-up scheme:
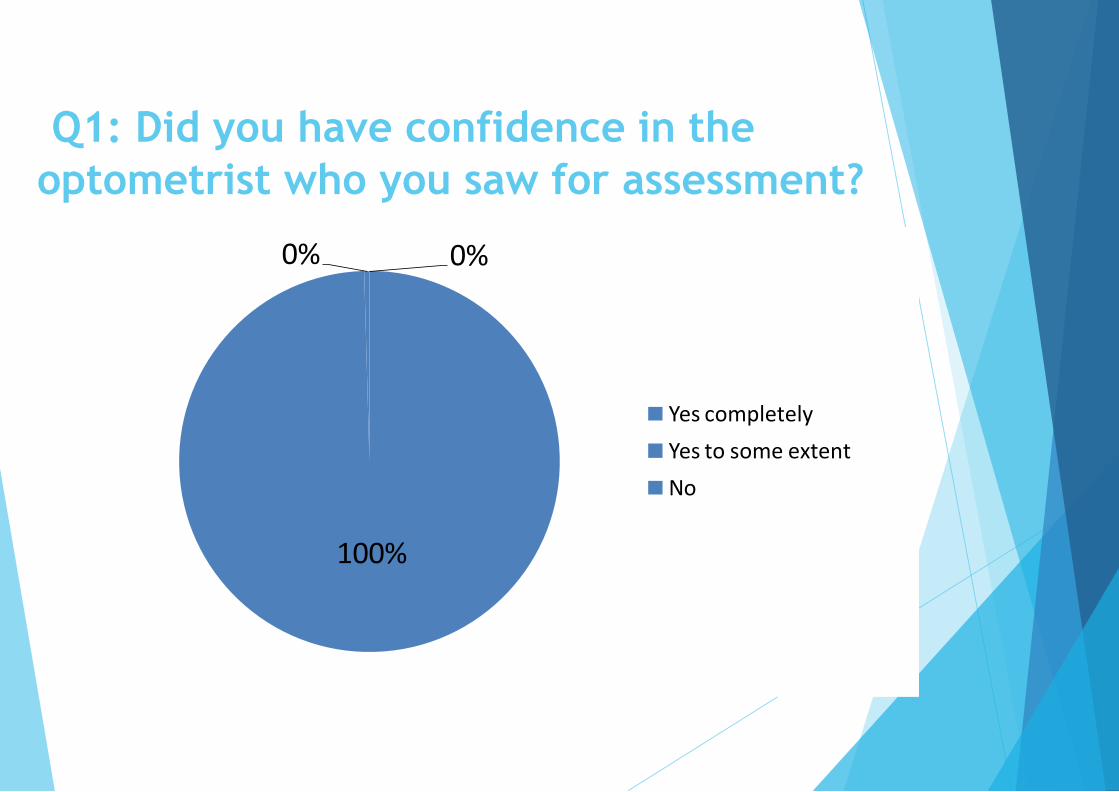
Q1: Did you have confidence in the
optometrist who you saw for assessment?
100%
0% 0%
Yes completely
Yes to some extent
No
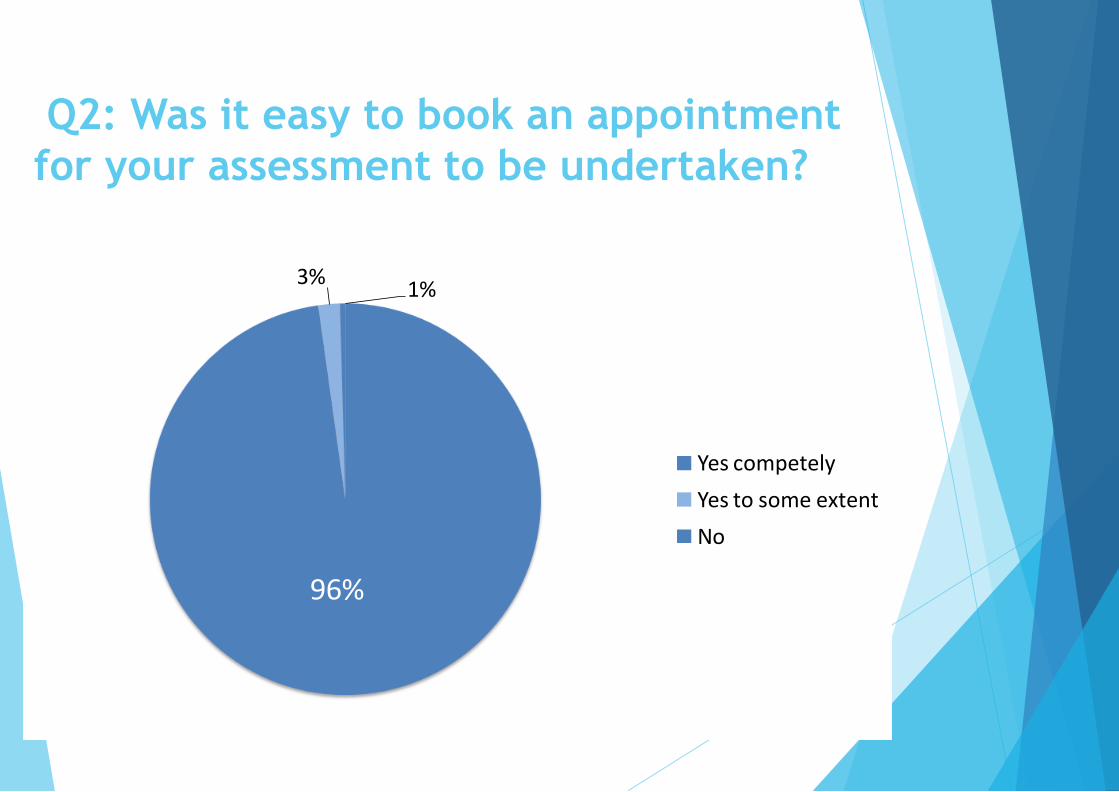
Q2: Was it easy to book an appointment
for your assessment to be undertaken?
96%
3%1%
Yes competely
Yes to some extent
No
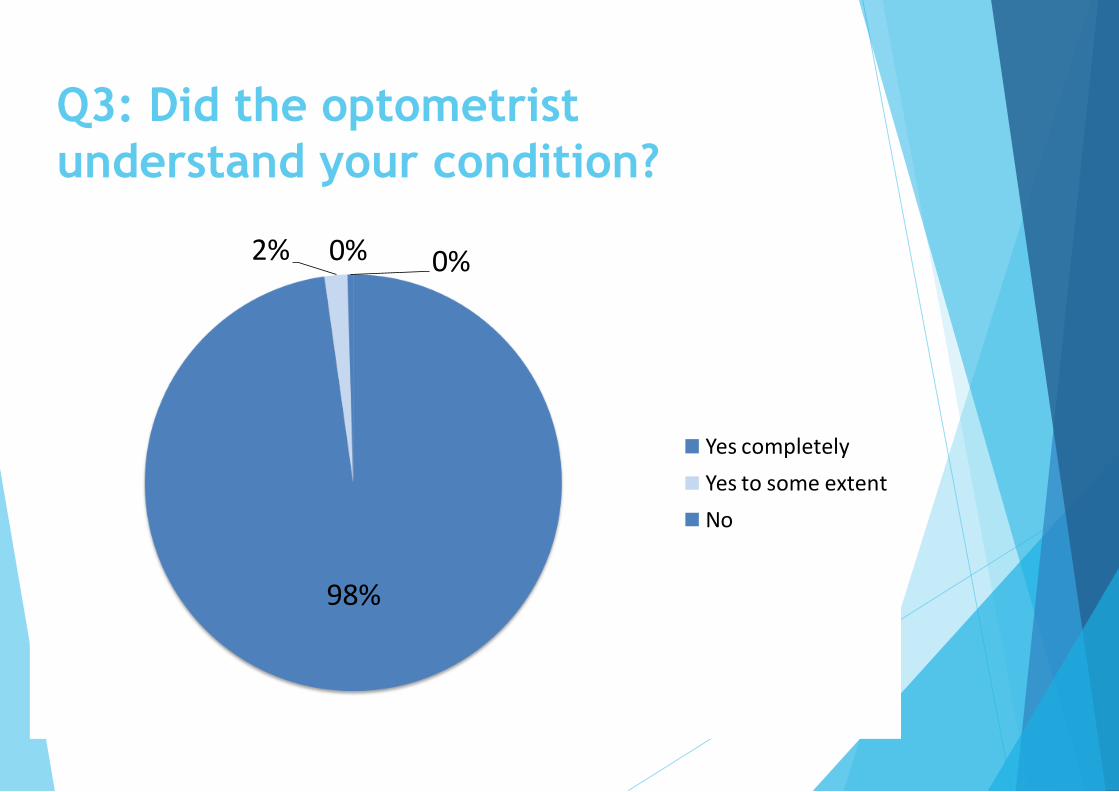
Q3: Did the optometrist
understand your condition?
98%
2% 0%0%
Yes completely
Yes to some extent
No

Q4: Was the optometry practice
accessible?
85%
10%5%
Yes easier than hospital
Yes as easy as the hospital
No it was harder than the hospital
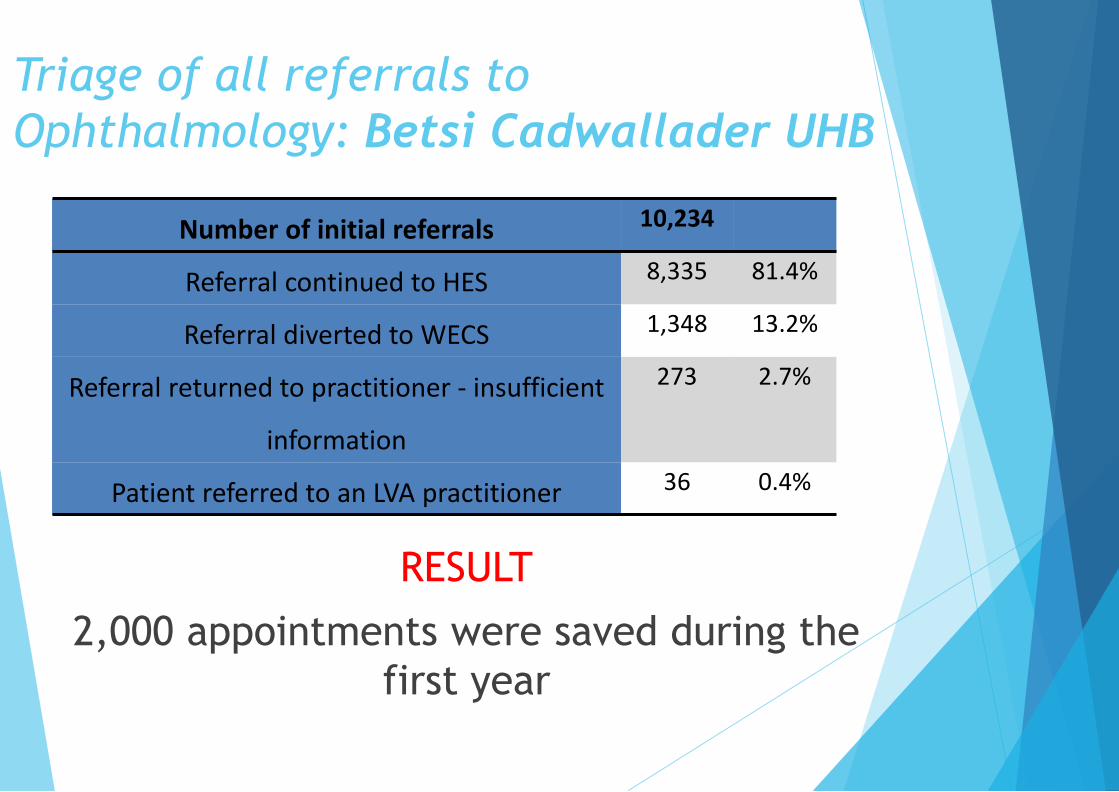
Triage of all referrals to
Ophthalmology: Betsi Cadwallader UHB
RESULT
2,000 appointments were saved during the
first year
Number of initial referrals 10,234
Referral continued to HES 8,335 81.4%
Referral diverted to WECS 1,348 13.2%
Referral returned to practitioner - insufficient
information
273 2.7%
Patient referred to an LVA practitioner 36 0.4%
What this means for patients in Wales
Skills and equipment are in place
Close to people’s homes
Better access for patients
NO waiting lists and NO workforce shortages
First port of call for eye problems
Avoid unnecessary referral to hospital eye
services
But What Does It Mean?
Smoking Cessation
Post Cataract Community Follow Ups
OHT and Suspect Glaucoma Monitoring
WECS Triaging
IT Connectivity across all Practices
Local, Primary Care Based Funding
Independent Prescribing
Joint Working
Specsavers Haverfordwest
The story so far…
Acquired the practice in 2006
Started gradual program of equipment upgrade
• Networked Fundus Camera £25K
• Hospital Standard Visual Fields Machine £14K
• Hospital Standard Tonometry £1K
• Pachymetry £1K
• Networked Optical Coherence Topography £40K
• Alongside program of improved eye examination equipment
Phoropters £36k
Digital Test Charts £12K
Improved Non contact tonometers £12K
Frequency Doubling Field Machines £8K
Disabled accessible consulting rooms £20K
All in all almost £200,000 of equipment investment in 12yrs…

A new hope
We outgrew our existing business because of the amount of
work that we could see being required to be delivered in
primary care…
Belief that delivery of primary care services HAS to be at the
heart of the professional offering…
Cue a £500,000 relocation to purpose built brand new
practice where we could put primary eyecare at the centre
of what we do……
Its not all about the toys….
Professional development is key
Job satisfaction
Recruitment
Higher qualifications / professional kudos
Ability to deliver services to the standards
demanded by the Royal College of
Ophthalmologists, General Optical Council and
College of Optometrists
Independent prescribing
Higher Glaucoma Qualifications
Medical Retina Qualifications

Warm and fluffy...
We make a difference
Brain Tumours
Strokes
Retinal Detachment
Reassurance
We are accessible
Let work together
Cluster Working
Work with the clusters to improve health and
healthcare outcomes
Mutual respect
Prescription requests
Training
Guidance
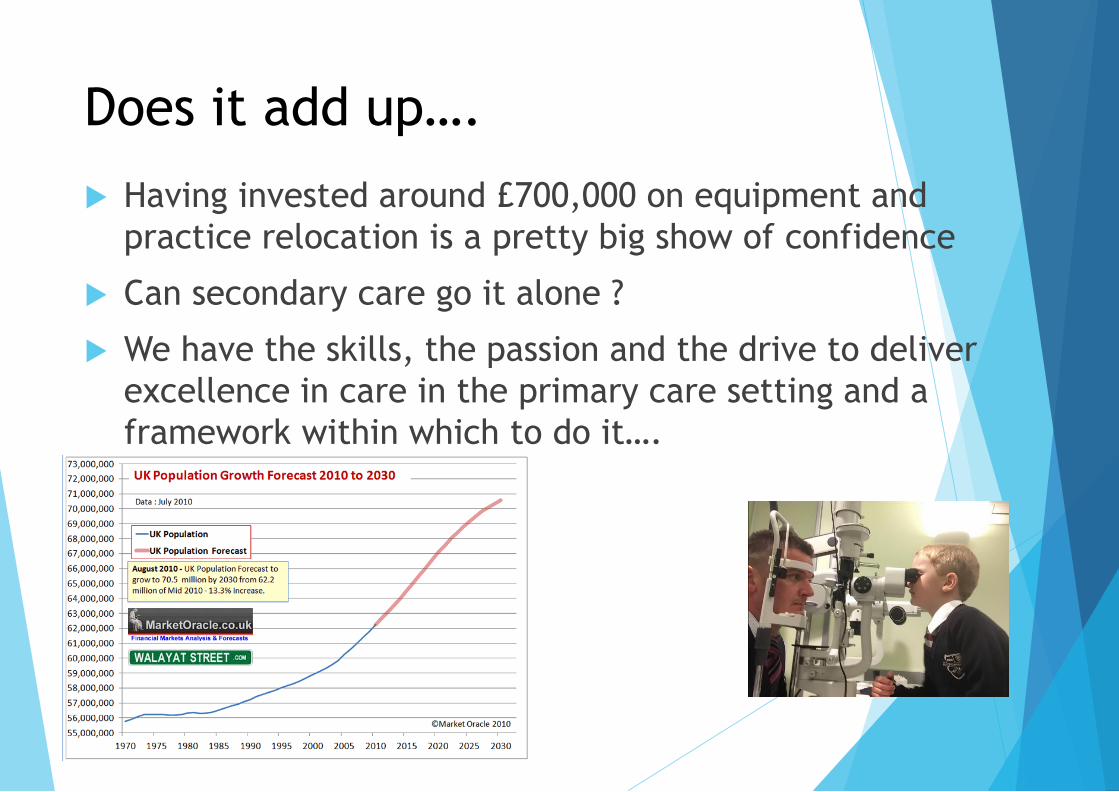
Does it add up….
Having invested around £700,000 on equipment and
practice relocation is a pretty big show of confidence
Can secondary care go it alone ?
We have the skills, the passion and the drive to deliver
excellence in care in the primary care setting and a
framework within which to do it….

The Future Is Bright
..................................
Insert name of presentation on Master
Slide
General Dental Services
15 November 2018
Richard Jones
#PrimaryCare18
NHS General Dental ServicesOpportunities for Change
Richard Jones
BDS (Wales) PG Cert Med Ed
Brief History of NHS Dental contracts since 2006
• Pre 2006 dentists were paid on an ‘item of service’ basisi.e. paid for what they did – no limits and Registration
• 2006 units of dental activity [UDAs] introduced, banding and capping activity
dentists contracted to complete a specified number of UDAs per year
• UDA definitions flawed:e.g. same payment no matter how many patient visits needed to complete a course of treatment
Negative impact of 2006 contract
• Immediate visible consequences:• 900,000 less UK patients seen in first 18 months; with less complex
treatment provided• Exodus of disillusioned GDPs from NHS care
• Closed contracts stopped/limited capacity to ‘grow’ services
• Professional de-motivation/disengagement resulting from:• variation of >50% different UDA rates paid to practices• “Claw back” for under performance• Banding inequities provided barriers to treating high need patients
• Consequences:• complex or high need patients referred to secondary care or Community
Dental service• Primary Care dentists de-skilled – on a TREADMILL
Response
2008 the Parliamentary Health Select Committee investigation found
UDAs were unfit for purpose and sought alternative contract models
• Welsh Dental Pilots Programme instigated• 8 practices tested removal of UDA for adults or children
• 2011 two Pilots remained adult based and children only • Eastside and Belgrave Dental Centres, Swansea
• Removes UDAs focuses on quality, access and prevention
• Clinical freedom to best suit demographics

Belgrave Dental Centre
Instant Advantages
• Clinical Freedom without UDA
• Care pathways based on:• Risk• Need• Prudent health care • Co-production
• Flexibility for LHB seeking responsive services, e.g. • Asylum seekers, HMP support
• Urgent access offered a risk based care plan
Skill Mix
Freedom to really apply:
• Enhanced skill mix usage
• Prevention Better oral Health and evidence based toolkit
• Treating patients on risk and need: Red/Amber/Green
• Working at top of competencies
All ↑ increase capacity to see more patients
Janice -one of twoOral Health Educators
Positive Feedback
“First time in 30 years I really understand how to look after my mouth”
“having one child with dental pain and decay ,I now Feel confident I know how to look after my children’s dental Heath as well as my own!”
“ I am Happy for you to refer me for help”

2016: Dental Contract hit buffers or reached a crossroad?
• Pilots were to end – no prospect of new UK contract
• Belgrave faced reversion to UDA basis… but
WG review was positive:• Good patient feedback• increased access• Application of prudent healthcare principles• No impact on patient income
ABMU (only) supported continuing the 2 sites
as prototype and would continue to:
• work with practices to spread learning
• innovate in skill mix and combating health inequalities
So what about our sister practice ?
Our second practice (from 2013), left behind with:
• UDAs
• High needs population
• Frustration attempting to treat based on targets not need , risk , coproduction and prudent healthcare principles
• Retention issues - Young performers disillusioned with system
• Clawback from missing targets due to trying to treat a high needs population under current GDS contract and low UDA rate.
However...2017 - Contract Reform!
• WAG keen to drive learning from pilots & prototypes
• Need for evidence based data on risk and need
• Positive support from ABMU
• Phase 1: • 10% UDA reduction for collection of ACORN data
• ACORN also collected in 2 prototype sites
• Phase 2: higher percentage of UDA target reduced informed by phase 1
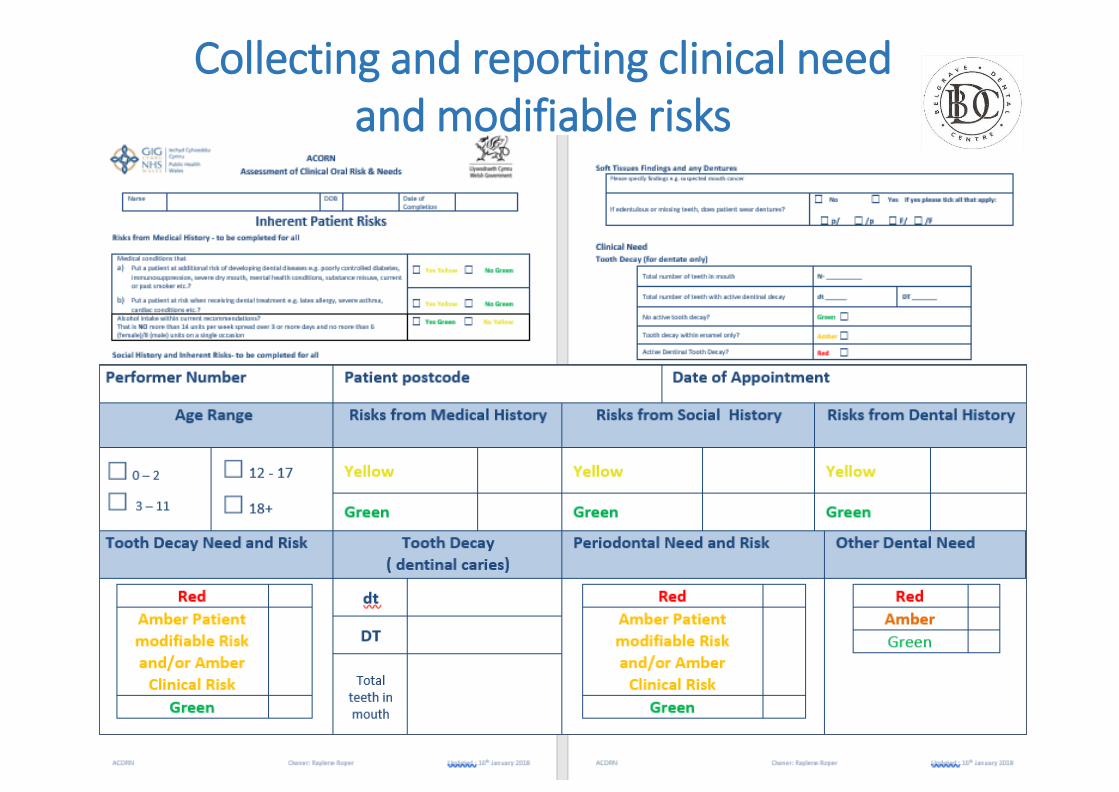
Collecting and reporting clinical need and modifiable risks
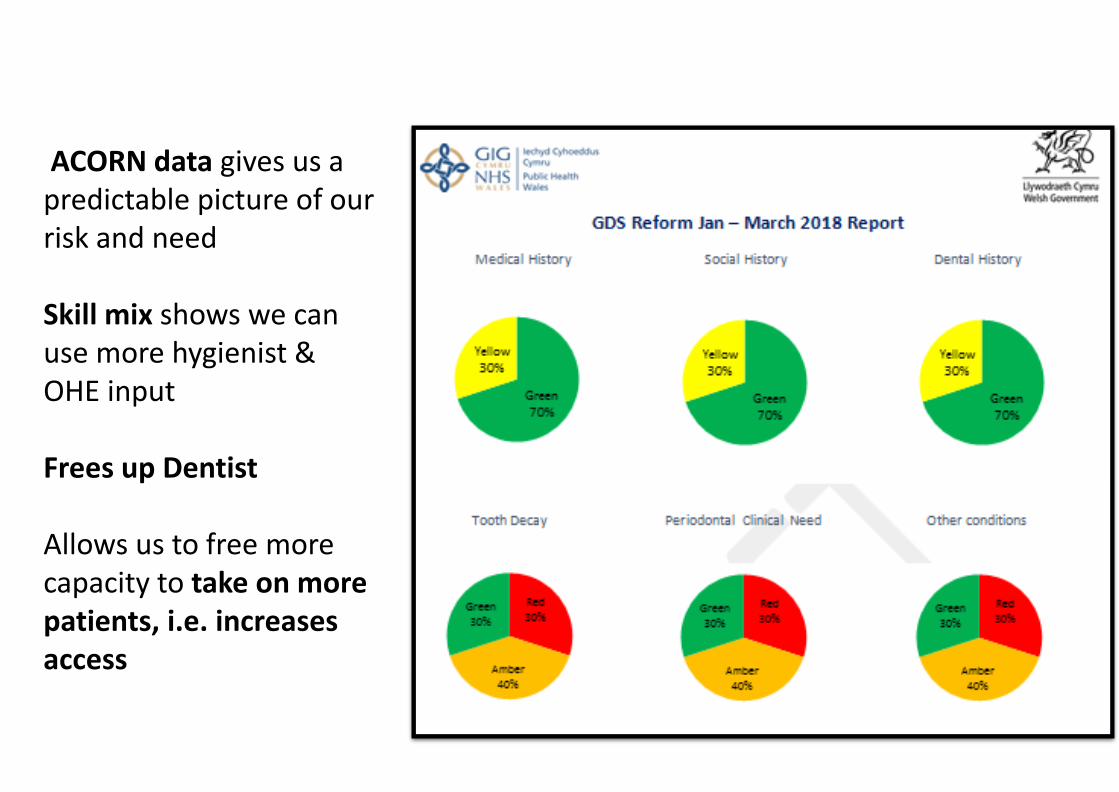
ACORN data gives us a predictable picture of our risk and need
Skill mix shows we can use more hygienist & OHE input
Frees up Dentist
Allows us to free more capacity to take on more patients, i.e. increases access

General Dental Practitioner Fellowship Scheme
• ABMU has developed, now piloting, a dental Fellowship which upskills Dentists, Pontardawe dental practice awarded first fellow
• With understanding from our ACORN our hygienist enables us to release our dentist to be upskilled
• Fellow focus is currently endodontics (MSc), possible opportunities in developing into a recognised Dentist with Enhanced Skills (DES)
• Currently with a 4 year waiting list within restorative dentistry’s secondary care service, pathway will help relieve pressure
• Actively involve patients
• Increase patient access to NHS dentistry
• Make more effective use of current resources
• Facilitate a preventive and prudent healthcare approach to care in more dental practices
• Provide opportunity for more specialised service provision in primary care which would relieve the burden on secondary care services
By supporting our practices ABMU has allowed us to not only meet such criteria but be a pace setter for its Formation
Aims to:
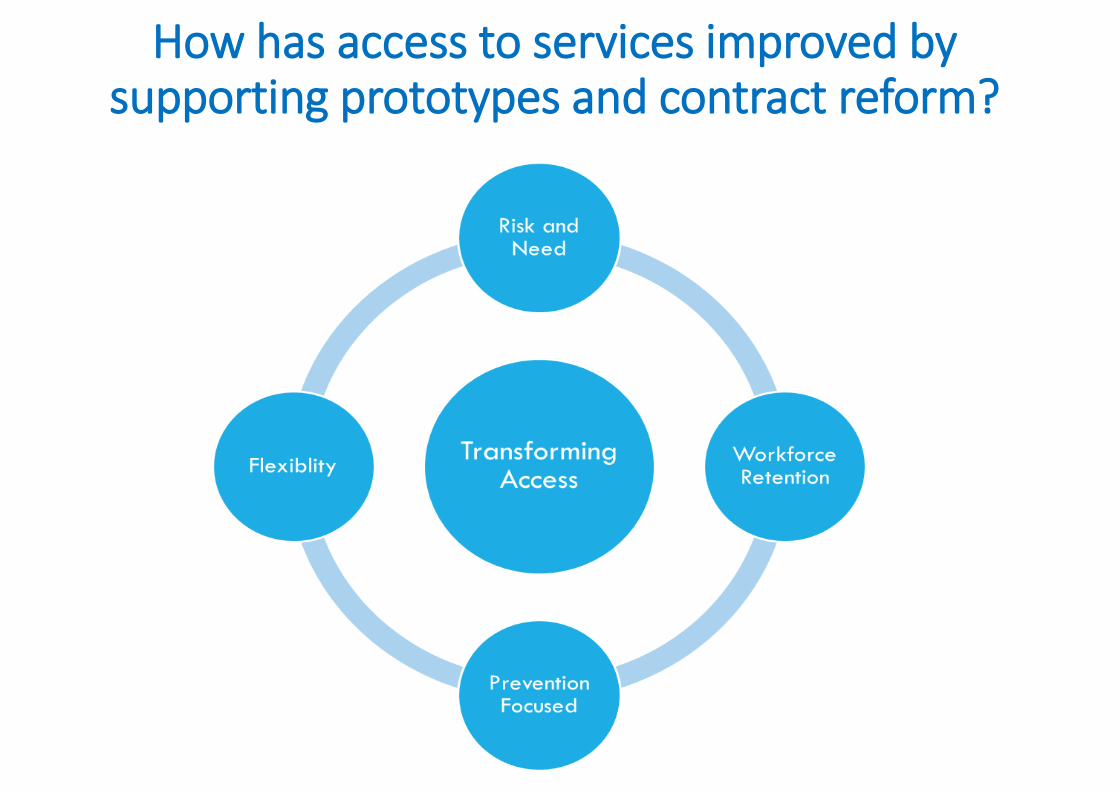
How has access to services improved by supporting prototypes and contract reform?
Future opportunities for innovation /access
• Multi-professional links
• Cluster working
• Community based projects
• Improved pathways supporting secondary care and community services
• http://www.youtube.com/watch?v=J55jlxR3nMY
Insert name of presentation on
Master Slide
General Practice
15 November 2018
Dr Gaynor Thomas
#PrimaryCare18

Dr. Gaynor Thomas
• Prudent Health Care
• ‘only do what only you can do’
• Access
• GP workload
• Recruitment
• Retention


GP
Clinical personal assistants
Maximize use of clinical team
Pharmacists
Common ailments scheme
Dentists
Opticians

• GPNs backbone of general practice
• Highly skilled
• Highly valued
• Inspirational role models
• 33.4% of GPN are due to retire by 2020
• Average age of GPN in Cwm Taf is 45
• ATP scheme, which was developed in 2009 in Yorkshire.
• 10% of the undergraduates that pass through the primary care placements have been recruited into general practice
Hub and spoke model
Hub
Spoke
Spoke
Spoke
Spoke
Spoke
Spoke
Undergraduate nurse placements
• 6 week placement in year 2
• 12 week consolidation placement in year 3
• High quality placement
• Inter-professional learning
Nurse mentors
• Each practice to have two nurse mentors
• Each nurse to become signing off mentor
• Nurse Mentor Support Workshop
GPN Ready Scheme
• Newly qualified nurses/return to work
• 2 year career training and education path
• Practice apply to Hub
• Discussion around role and training
• Advertise for nurse
• Incentivised scheme

Timeline
Year 2
6 week placement
Year 3
12 week consolidation
block
Newly qualified nurse
GPN ready scheme
2 years
Fully trained Practice Nurse
Student Feedback
• High level of satisfaction
• University evaluation top 5% of placements
• Improved awareness of role
• Opportunity to learn new skills
Nurse Feedback
• Initial apprehension
• Enjoy placements
• Renewed enthusiasm for teaching
• Shared learning between mentors
• Retain current workforce
Future
• Hubs at heart of training and education
• Run by primary care for primary care
• Network of practices with training expertise
• Provide the infrastructure to train all future workforce
Insert name of presentation on Master Slide
National Primary Care Conference
15 November 2018
#PrimaryCare18