Nation = 15,648 FacilitiesMichigan = 433 FacilitiesLansing = 190 FacilitiesDetroit = 186...
118
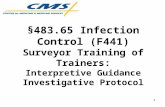
Nation = 15,648 Facilities Michigan = 433 Facilities Lansing = 190 Facilities Detroit = 186 Facilities Gaylord = 57 Facilities F441 – Infection Control* 37% F441 – Infection Control* 47% F441 – Infection Control 47% F323 - Accidents 51% F441 – Infection Control 46% F371 – Sanitary Conditions* 35% F323 – Accidents* 40% F371 – Sanitary Conditions 43% F441 – Infection Control 48% F371 – Sanitary Conditions 46% F323 – Accidents* 29% F371 – Sanitary Conditions* 38% F323 - Accidents 38% F371 – Sanitary Conditions 30% F226 – Policy & Procedure on Abuse 25% F309 – Quality of Care* 25% F329 – Unnecessary Drugs* 28% F329 – Unnecessary Drugs 37% F309 – Quality of Care 23% F465 – Other Environmental Conditions 23% F329 – Unnecessary Drugs* 23% F309 – Quality of Care* 25% F309 – Quality of Care 29% F226 – Policy & Procedure on Abuse 22% F431 – Control, Labeling & Storage of Drugs 21% F431 – Control, Labeling & Storage of Drugs* 20% F226 – Policy & Procedure on Abuse 24% F314 – Pressure Sores 26% F329 – Unnecessary Drugs 22% F329 – Unnecessary Drugs 21% F279 – Comprehensive Care Plans 19% F314 – Pressure Sores 21% F226 – Policy & Procedure on Abuse 25% F314 – Pressure Sores 19% F309 – Quality of Care 12% F241 – Dignity 16% F431 – Control, Labeling & Storage of Drugs* 19% F332 – Medication Errors 5% or greater 24% F465 – Other Environmental Conditions 18% F314 – Pressure Sores 9% F514 – Clinical Records 15% F465 – Other Environmental Conditions 18% F431 – Control, Labeling & Storage of Drugs 21% F431 – Control, Labeling & Storage of Drugs 18% F323 - Accidents 9% F282 – Services by Qualified 14% F332 – Medication 16% F465 – Other Environmental 18% F332 – Medication 13% F332 – Medication 2%
-
Upload
parker-siner -
Category
Documents
-
view
215 -
download
1
Transcript of Nation = 15,648 FacilitiesMichigan = 433 FacilitiesLansing = 190 FacilitiesDetroit = 186...

Nation = 15,648 Facilities Michigan = 433 Facilities Lansing = 190 Facilities Detroit = 186 Facilities Gaylord = 57 Facilities
F441 – Infection Control*
37% F441 – Infection Control*
47% F441 – Infection Control
47% F323 - Accidents 51% F441 – Infection Control
46%
F371 – Sanitary Conditions*
35% F323 – Accidents* 40% F371 – Sanitary Conditions
43% F441 – Infection Control
48% F371 – Sanitary Conditions
46%
F323 – Accidents* 29% F371 – Sanitary Conditions*
38% F323 - Accidents 38% F371 – Sanitary Conditions
30% F226 – Policy & Procedure on Abuse
25%
F309 – Quality of Care*
25% F329 – Unnecessary Drugs*
28% F329 – Unnecessary Drugs
37% F309 – Quality of Care 23% F465 – Other Environmental Conditions
23%
F329 – Unnecessary Drugs*
23% F309 – Quality of Care*
25% F309 – Quality of Care 29% F226 – Policy & Procedure on Abuse
22% F431 – Control, Labeling & Storage of Drugs
21%
F431 – Control, Labeling & Storage of Drugs*
20% F226 – Policy & Procedure on Abuse
24% F314 – Pressure Sores 26% F329 – Unnecessary Drugs
22% F329 – Unnecessary Drugs
21%
F279 – Comprehensive Care Plans
19% F314 – Pressure Sores 21% F226 – Policy & Procedure on Abuse
25% F314 – Pressure Sores 19% F309 – Quality of Care 12%
F241 – Dignity 16% F431 – Control, Labeling & Storage of Drugs*
19% F332 – Medication Errors 5% or greater
24% F465 – Other Environmental Conditions
18% F314 – Pressure Sores 9%
F514 – Clinical Records 15% F465 – Other Environmental Conditions
18% F431 – Control, Labeling & Storage of Drugs
21% F431 – Control, Labeling & Storage of Drugs
18% F323 - Accidents 9%
F282 – Services by Qualified Persons
14% F332 – Medication Errors 5% or greater
16% F465 – Other Environmental Conditions
18% F332 – Medication Errors 5% or greater
13% F332 – Medication Errors 5% or greater
2%

Michigan QTR 1st 2nd 3rd 4th
Rolling data – CASPER file March 2014 June 2014 September 2014
December 2014
Infection Control – F441 48% 47% 47%
Accidents – F323 44% 40% 40%
Sanitary Conditions – F371 39% 37% 40%
Unnecessary Drugs – F329 36% 33% 28%
Quality of Care – F309 23% 25% 25%
P&P on Abuse – F226 21% 23% 24%
Pressure Sores – F314 22% 21% 21%
Control, Labeling & Storage of Drugs – F431 18% 19% 19%
Other Environmental Conditions – F465 22% 20% 18%
Medication Errors 5% or greater – F332 18% 16%
Comprehensive Care Plan – F279 18%

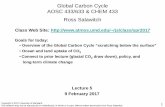
Partnership to Improve Dementia Care in Nursing HomesAntipsychotic Drug use in Michigan’s Nursing Homes trend updateQuarterly Prevalence of Antipsychotic Use for Long-Stay Residents
Source – CMS Quality Measure, based on MDS 3.0 Data
*Rank – lower = better
2011Q2
2011Q3
2011Q4
2012 Q1
2012 Q2
2012 Q3
2012 Q4
2013 Q1
2013 Q2
2013 Q3
2013 Q4
2014 Q1
2014 Q2
Rank in 2014Q2
16.2%
16.0%
16.4%
16.4%
15.8%
16.0%
15.5%
14.9%
14.4%
14.1%
13.9%
13.7%
13.4%
2

Infection Control - F441483.65 The facility must establish and maintain an
Infection Control Program designed to provide a safe, sanitary and comfortable environment and to help prevent the development and transmission of disease and infection.
(a) The facility must establish an Infection Control Program under which it –
1. Investigates, controls, and prevents infections in the facility;2. Decides what procedures, such as isolation, should be applied to an individual
resident; and 3. Maintains a record of incidents and corrective actions related to infections.

Infection Control - F441(b) Preventing Spread of Infection
1. When the Infection Control Program determines that a resident needs isolation to prevent the spread of infection, the facility must isolate the resident.
2. The facility must prohibit employees with a communicable disease or infected skin lesions from direct contact with residents or their food, if direct contact will transmit the disease.
3. The facility must require staff to wash their hands after each direct resident contact for which hand washing is indicated by accepted professional practice
(c) Personnel must handle, store, process and transport linens so as to prevent the spread of infection.

Infection Control - F441Overview
Infections result in an estimated 150,000 to 200,000 hospital admissions per year. When a nursing home resident is hospitalized with a primary
diagnosis of infection, the death rate can reach as high as 40%.
An effective facility-wide infection prevention and control program can help contain costs and reduce adverse consequences.
Critical aspects include:• Recognizing and managing infections at the time of a resident’s
admission to the facility and throughout their stay
• Following recognized infection control practices while providing care.

Infection Control - F441Program Development and Oversight
Involves: Establishing goals and priorities for the program Planning and implementing strategies to achieve the goals
• Identify the staff’s roles and responsibilities• Develop, train, and implement infection control policies and procedures
Monitoring the implementation of the program – includes infection control practices• Document the tracking/analyzing outbreaks of infection including the actions taken
to resolve related problems• Define and manage appropriate health initiative – influenza and pneumonia
immunizations, tuberculosis screening• Manage food safety, pest control, waste disposal and employee health and hygiene
Responding to errors, problems or other identified issues

Infection Control - F441Policy and Procedures
Policies and procedures are reviewed periodically and revised as needed to conform to current standards of practice or to address specific facility concerns.
Establish the program’s expectations and parameters - i.e.; • Specify the use of standard precautions facility-wide and use of transmission-based
precautions when indicated• Define the frequency and nature of surveillance activities• Require staff to use accepted hand hygiene after each direct resident contact for which hand
hygiene is indicated• Prohibit direct resident contact by an employee who has an infected skin lesion or
communicable disease. Procedures guide the implementation of the policies and performance of
specific tasks – i.e.;• How to identify and communicate information about residents with potentially transmissible
infectious agents

Infection Control - F441Policy
Policies and procedures are reviewed periodically and revised as needed to conform to current standards of practice or to address specific facility concerns.
Establish the program’s expectations and parameters - i.e.; • Specify the use of standard precautions facility-wide and use of transmission-based
precautions when indicated• Define the frequency and nature of surveillance activities• Require staff to use accepted hand hygiene after each direct resident contact for
which hand hygiene is indicated• Prohibit direct resident contact by an employee who has an infected skin lesion or
communicable disease.

Infection Control - F441 Procedures
Procedures guide the implementation of the policies and performance of specific tasks – i.e.;
• How to identify and communicate information about residents with potentially transmissible infectious agents
• How to obtain vital signs for a resident on contact precautions and what to do with the equipment after its use
• Essential steps and considerations (including choosing agents) for performing hand hygiene

Infection Control - F441Surveillance
Essential elements of a surveillance system include: Use of standardized definitions and listings of the symptoms of infection
- http://www.apic.org/Professional-Practice/Practice-Resources/Definitions-Surveillance
Use of surveillance tools such as infection surveys and data collection templates
Walking rounds throughout the facility Identification of segments of the resident populations at risk for infection Identification of the processes or outcomes selected for surveillance Statistical analysis of data that can uncover an outbreak Feedback of results to the primary caregivers so they can assess the
residents for signs of infection.

Infection Control - F441Process Surveillance
Determines whether the facility - Minimizes exposure to a potential source of infection Uses appropriate hand hygiene prior to and after all procedures Ensures that appropriate sterile techniques are followed when indicated Uses personal protective equipment when indicated Ensures that reusable equipment is appropriately cleaned, disinfected or
reprocessed Uses single-use medication vials and other single use items
appropriately

Infection Control - F441Outcome Surveillance
Consists of – Collecting/documenting data on individual cases and comparing the
collected data to standard written definitions (criteria) of infections.• Reports describe the types of infections• Descriptive documentation provides the facility with summaries of the observed staff
practices and/or the investigation of the causes of an infection or trends
The IP (Infection Preventionist) or other designated staff reviews data to detect clusters and trends such as antibiotic orders, antibiotic susceptibility profiles, medication regimen review reports, physician progress reports and transfer summaries of newly admitted residents.• All residents are monitored for current infections and infection risks• Review of outcome data helps the facility to identify the number of residents who
develop infections within the nursing home.

Infection Control - F441Education
Both initial and ongoing infection control education help staff comply with infection control practices.
Essential topics of infection control training include: Routes of disease transmission Hand hygiene Sanitation procedures MDROs (multi-drug resistant organisms)
• Because of increases in MDROs, review of the use of antibiotics (including comparison of prescribed antibiotics with available susceptibility reports) is a vital aspect of the prevention and control program
Transmission-based precaution techniques Federally required OSHA education

Infection Control - F441Preventing the Spread
Modes of transmission include - Contact Droplet Airborne

Infection Control - F441Factors of the Spread
Individual Corticosteroids and chemotherapy Decreased function of the heart, lungs and kidneys Decreased/absent cough reflex, thinning skin, decreased tear production,
vascular insufficiency, impaired immune function Coexisting chronic diseases – diabetes, cancer, COPD, anemia
Institutional Pathogen exposure in shared communal living space – handrails &
equipment Common air circulation Transfer of residents to and from hospitals or other settings Improper hand hygiene, improper glove use, improper food handling

Infection Control - F441Factors of the Spread
Direct transmission (Person to Person) Contaminated hands of staff are often implicated Examples include (but not limited to) - MRSA, VRE, and Influenza
Indirect transmission Resident care devices – thermometers or glucose monitoring devices Clothing, uniforms, lab coats etc., i.e. – MRSA, VRE, Clostridium difficile Toilets and bedpans, i.e. – salmonella, shigella, E. coli, norovirus and C-diff.
Reducing and/or preventing infections through indirect contact requires the decontamination (cleaning, sanitizing, or disinfecting) of resident equipment, medical devices, and the environment.

Infection Control - F441Factors of the Spread
Critical items – equipment must be sterile when used such as needles, intravenous catheters, indwelling urinary catheter.s
Semi-critical items – equipment that require meticulous cleaning followed by high-level disinfection tx or sterilized such as thermometers, podiatry equipment, electric razors.
Non-critical items – equipment that require low level disinfection by cleaning periodically and after visible soiling with an EPA disinfectant detergent or germicide such as stethoscopes, blood pressure cuffs, over-bed tables.
Single dose/single use equipment is an alternative to sterilizing medical instruments. They must be discarded after use and are never used for more than one resident.

Infection Control - F441Factors of the Spread
Single dose/single use medications – must not be used for multiple residents due to the risk of spreading infections diseases.
Medications labeled as single-use or single dose by manufacturers typically lack antimicrobial preservatives and once a SDV is entered, the contents can support the growth of micro-organisms.
The risk of infection transmission associated with using SDVs for multiple residents is well documented, with evidence accumulated from the investigation of multiple outbreaks.
Administering drugs from on SDV to multiple residents without adhering to USP standards is not acceptable.

Infection Control - F441Factors of the Spread
Insulin Pens are designed to permit self-injection and are intended for single-person use, using a new needle for each injection.
Insulin pens are designed to be used multiple times by a single resident only and must never be shared.
Insulin pens must be clearly labeled with the resident’s name or other identifiers to verify that the correct pen is used for the correct resident.
Policy and procedures and staff education should be provided when facility’s use insulin pens.
If it is discovered that insulin pens are shared between residents, the facility’s plan of correction should include notification of the local health department.

Infection Control - F441Linens
It is important that all potentially contaminated linen be handled with appropriate measures to prevent cross-transmission.
If the facility handles all used linen as potentially contaminated (i.e., using standard precautions), no additional separating or special labeling of the linen is recommended.
No special precautions (double bagging) or categorizing is recommended for linen originating in isolation rooms.
Double bagging of linen is only recommended if the outside of the bag is visibly contaminated or is observed to be wet through to the outside of the bag.
Leak-resistant bags are recommended for linens contaminated with blood or body substances.
For the routine handling of contaminated laundry, minimum agitation is recommended to avoid the contamination of air, surfaces, and persons.
It is important that laundry areas have hand washing facilities and products (PPE) available for workers to wear while sorting linens.
It is recommended that damp linen is not left in machines overnight.

Infection Control - F441Linens
The CDC recommends leaving washing machines open to air when not in use to allow the machine to dry completely and to prevent growth of microorganisms in wet, potentially warm environments.
Laundry detergents used within facilities are not required to have state anti-microbial claims. Facilities should closely follow manufacturer’s instructions for laundry detergents used.
CMS and CDC have determined that ozone cleaning systems are acceptable methods of processing laundry. Ozone cleaning systems also should be used per manufacturer’s instructions.
An effective way to destroy microorganisms in laundry items is through hot water washing at temps about 160 degrees Fahrenheit (F) for 25 minutes.
Alternatively, low temp washing at 71-77 degrees F plus a 125-part-per-million (ppm) chlorine bleach rinse has been found to be effective and comparable to high temperature wash cycles.

Infection Control - F441Linens
Laundry washing within facilities typically occurs in a low water temperature environment. Many laundry items are composed of materials that cannot withstand a chlorine bleach rinse and remain intact.
A chlorine beach rinse is not required for all laundry items processed in low temperature washing environments due to the availability of modern laundry detergents that are able to produce hygienically clean laundry without the presence of chlorine beach.
However, a chlorine bleach rinse may still be used for laundry items composed of materials such as cottons.

Infection Control - F441Linens
Hot water washing at temps greater than 160 degrees F for 25 minutes and low temp washing at 71 to 77 degrees F with a 125 ppm chlorine bleach rinse continue to be effective ways to wash laundry.
If a facility chooses to process laundry using a hot water temp environment, the temp maintained for 25 minutes should be at or about 160 degrees F.
Facilities are not required to maintain a record of water temps during laundry processing cycles.
Facilities are required to follow manufacturer’s instructions for all material involved in laundry processing.
Facilities should consider resident’s individual needs (allergies) when selecting methods for processing laundry.

Infection Control - F441Linens
If linen is sent off to a professional laundry, the facility should obtain an initial agreement that stipulate the laundry will be hygienically cleaned and handled to prevent recontamination from dust and dirt during loading and transport.
An ozone laundry cleaning system is a method which may require a professional laundry service. The facility will need to obtain such an agreement.
Whether laundry processing is completed within or outside the facility, facilities should have written policies & procedures which should include training for staff who will handle linens and laundry.

Infection Control - F441Linens
Regarding standard mattresses and pillows
- patches for tears and holes in mattress covers do not provide an impermeable surface over a mattress – therefore it is recommended that mattress covers with tears/holes be replaced.
- And it is recommended that moisture resistant mattress covers be cleansed and disinfected between residents with an EPA approved germicidal detergent to help prevent the spread of infections and fabric mattress covers be laundered in a hot water laundry cycle between residents.

Infection Control - F441Recognizing and Containing Outbreaks
It is important that facilities know how to recognize and contain infectious outbreaks. An outbreak is typically one or more of the following:
• One case of an infection that is highly communicable;
• Trends that are 10% higher than the historical rate of infection for the facility that may reflect an outbreak or seasonal variation and therefore warrant further investigation; or
• Occurrence of three or more cases of the same infection over a specified length of time on the same unit or other defined areas.

Infection Control - F441MDRO’s
MDRO’s found in facilities include (but not limited to)
MRSA – Methicillin resistant staphylococcus aureusVRE – Vancomycin resistant enterococcusC. Diff - Clostridium difficile
Transmission-based precautions are employed for residents who are actively infected with a MDRO.

Infection Control - F441MDRO’s
Staphylococcus is a common cause of infections in hospitals and nursing homes and increasingly in the community.
Common sites of MRSA colonization include the rectum, perineum, skin and nares.
Colonization may precede or endure beyond an acute infection.
MRSA is transmitted (most commonly) by person to person and on inanimate objects (i.e. stethoscopes etc)
*MRSA infection is commonly treated with vancomycin – which, in turn can lead to increased enterococcus antibiotic resistance.

Infection Control - F441MDRO’s
C. Difficile is an organism which normally lives benignly in the colon in spore form.
When antibiotic use eradicates normal intestinal flora, the organism may become active and produce a toxin that causes symptoms such as diarrhea, abdominal pain, and fever.
More severe cases can lead to additional complications such as intestinal damage and severe fluid loss. Treatment options include stopping the antibiotics and starting specific anticlostridial antibiotics such as metronidazole (flagyl) or oral vancomycin.
Contact precautions are instituted for residents with symptomatic C. difficile infection.

Infection Control - F441Intravascular devices
Devices such as central venous catheters, PICC lines, dialysis catheters etc. may increase the risk for local and systemic infections.
Surveillance consistently includes all residents with vascular access to reduce risk for infection. What does this mean? Observation of the insertion sites
Observation of the dressing changes
Observation for use of appropriate PPE and hand hygiene during the care and tx of residents with venous catheters.
Review of medical record for evidence of infection

Infection Control – F441
Surveyor Investigative Protocol
Observations Linens handled in manner to prevent contamination Employees with cold symptoms, infections or open lesions
on hands are prohibited from contact with resident(s) & food Adherence to infection control practices – use of PPE Hand hygiene and use of gloves when indicated Availability of gloves and products to perform hand hygiene Residents with S&S of infections Cleaning and disinfecting practices

Infection Control – F441
Surveyor Investigative Protocol
Interview(s) of Direct care staff concerning;
• Whether they are aware of and have reported any signs/symptoms exhibited by the resident that may be associated with an infection
• Whether they have been instructed on any special precautions that are applicable to a resident on transmission based precautions
• How staff know which residents are covered by transmission-based precautions and, what specific actions are required for each type of transmission based precautions.

Infection Control – F441
Surveyor Investigative ProtocolRecord Review
Resident’s medical record reveals an evaluation of factors which may increase the risk of infection (i.e. – urinary catheters, trache tube etc.) and if an infection is present, documentation indicating potential causes/contributing factors
Resident’s plan of care includes interventions to prevent transmission of infection when applicable
Surveillance records reflect pertinent data – date of infection, sign/symptoms meet criteria of infection, treatment ordered, precautions implemented, date resolved, review of antibiotic appropriateness/effectiveness
Infection control policies meet current professional standards of practice and are defined by departments i.e. – nursing, dietary, laundry

Infection Control - 441
Criteria for Compliance
This is determined if the program/facility demonstrates; Ongoing surveillance, recognition, investigation and control of infections to
prevent the onset and the spread of infection; Practices to reduce the spread of infection and control of transmission-
based precautions; Practices and process consistent with infection prevention and prevention
of cross-contamination (i.e. -catheter care etc.); That it uses records of incidents to improve its infection control processes
and outcomes by taking corrective action; Processes and procedures to identify and prohibit employees with a
communicable disease or infected skin lesions from direct contact with residents or their food;
Consistent adherence with appropriate hand hygiene practices; Handling, storage, processing and transporting of linens so as to prevent
the spread of infection.

Infection Control - 441
Deficiency CategorizationSeverity Level 2 - indicates noncompliance that results in a resident outcome of no more than minimal discomfort and/or has the potential to compromise the resident’s ability to maintain or reach his or her highest practicable level of well being. The potential exists for greater harm to occur if interventions are not provided.
The facility failed to ensure that their staff demonstrates proper hand hygiene between residents to prevent the spread of infections. The staff administered medications to a resident via a gastric tube and while wearing the same gloves, proceeded to administer oral medications to another resident. The staff did not remove the used gloves and wash or sanitized their hands between residents.The facility failed to implement a surveillance program including the investigation of infections or attempt to distinguish facility-acquired infections from community-acquired infections.The facility identified issues related to staff infection control practice but failed to identify the cause and institute measures to correct the problem

Infection Control - 441
Deficiency Categorization
Severity Level 3 - indicates noncompliance that results in actual harm that is not immediate jeopardy.
The facility routinely sent urine cultures of asymptomatic residents with indwelling catheters, putting residents with positive cultures on antibiotics, resulting in two residents acquiring antibiotic-related colitis and significant weight loss.
The facility failed to institute internal surveillance for adherence to hand washing procedures or pertinent reminders to staff regarding appropriate respiratory precautions during an influenza outbreak resulting in additional cases of influenza in residents on another, previously unaffected unit or section of the facility.

Infection Control - 441
Deficiency Categorization
Severity Level 4 – immediate jeopardy is a situation… likely to result in serious injury, harm, impairment, or death to a resident AND requires immediate correction etc.
The facility failed to restrict a staff member with a documented open, draining and infected skin lesion that was colonized with MRSA from working without adequately covering the area, resulting in MRSA transmission and infection of one or more residents under that staff person’s care.
The facility failed to investigate, document surveillance of and try to contain an outbreak of gastrointestinal illness among residents; as a result, additional resident became ill.

Infection Control - 441Summary Statement of Deficiency
On …. at 4:06pm, facility staff nurse (A) was observed using an ultra trak ultimate glucometer to place a blood tinged test strip into the device for a serum blood glucose reading for resident #20. Upon leaving resident #20’s room, staff nurse (A) failed to disinfect the glucometer and placed it back into the treatment cart. Then staff nurse (A) went to resident #21’s room. Taking out the same glucometer used for resident #20 serum glucose measurement from the treatment cart, staff nurse (A) then inserted a blood tinged test strip into the glucometer for a serum glucose measurement. After use of the glucometer, staff nurse (A) then placed the glucometer into the top right drawer of the treatment care without disinfecting it.
At 4:25pm (same date), staff nurse (A) removed the same ultra trak ultimate glucometer from the treatment cart use for resident #21 and place a blood tinged test strip into it for measuring resident #3’s serum glucose level. Staff nurse (A) failed to sanitize this glucometer prior to and after use on resident #3.

Infection Control - 441Summary Statement of Deficiency
An observation of pericare for Resident #X on x/xx/xx at 3:00pm Certified Nurse Aide (CNA) entered with Resident #X into her room. CNA did not wash hands prior to applying gloves before transferring Resident #X into her bed. When Resident #X was in bed, CNA, with same gloves on, checked Resident #X’s brief to check if Resident #X was soiled. CNA stated that Resident #X would need to be changed. CNA then with same gloved hands, proceeded to Resident #X’s closet to retrieve a clean brief. CNA removed gloves and left the room without washing hands to get washcloths. CNA returned to room without washing hand to and applied clean gloves, filled wash basin, and retrieved Resident#4’s body wash from her bedside stand. CNA placed the wash basin directly on Resident #X’s bedside table….CNA removed gloves, and without washing hands, applied clean gloves and proceeded to clean Resident #X back side. Once Resident #X pericare was complete and a clean brief applied, CNA went across room and with gloved hand turned on air conditioner for room….

Infection Control - 441Summary Statement of Deficiency
…during an observation of the dressing change to Resident #x’s right heel on X/XX/XX at X:XX pm, Assistant Director of Nursing was observed with gloved hands to remove the dressing from Resident #X’s right heel, then, with her right gloved hand, reached into her left pocket to get a measuring tool to measure Resident #X’s heel ulcer.

Infection Control - 441Summary Statement of Deficiency
…An interview was conducted with the Director of Nursing (DON) on 7/23/14 at 9:00am, pertaining to the Infection Control Program. A review of the Infection Control Program documentation from April 2013 through July XX, 2014 revealed:1) No “Employee Infection Logs” 2) No documentation showing employee illnesses were monitored and
compared with resident infections in the monthly summaries3) No monthly summaries showing infection control information
gathered had been analyzed with appropriate recommendations to prevent the potential spread of infectious organisms.
4) The maps of the facility showing the locations of residents with infections by color-coding was not consistently completed to include all of the infections…

Let’s take a pause here for any questions or comments regarding the Infection Control tag – F441

Accidents – F323483.25 (h)(1)(2) The facility must ensure that the resident remains as free from accident hazards as is possible; and
each resident receives adequate supervision and assistance devices to prevent accidents.
The intent of this requirement is to ensure the facility provides an environment that is free from accident hazards over which the facility has control and provides supervision and assistive devices to each resident to
prevent avoidable accidents. This includes: Identifying, evaluating and analyzing hazards and risks
Implementing interventions to reduce the hazards and risks Monitoring for effectiveness and modifying interventions as necessary

Accidents – F323Definitions
“Accident” – refers to any unexpected or unintentional incident which may result in injury or illness to a resident. (This does not include adverse outcomes that are a direct consequence of treatment or care that is provided in in accordance with current standards of practice, i.e. drug side effects).
“Avoidable Accident” – means that an accident occurred because the facility failed to identify environmental hazards and individual resident risk of an accident including the need for supervision, and/or failed to implement intervention, including adequate supervision, consistent with a resident’s needs, goals, plan of care and current standards of practice in order to reduce the risk of an accident and/or failed to monitor for effectiveness and modify interventions as necessary.
“Unavoidable Accident” – means that an accident occurred despite facility efforts to identify, evaluate and analyze the hazards and risks, and to implement interventions to reduce the hazards and risks, and to monitor for effectiveness and modify interventions as necessary.

Accidents – F323
“Assistance Device” or “Assistive Device” – refers to any item (handrails, grab bars, transfer lifts, canes, wheelchairs etc.) that is used by, or in the care of a resident to promote, supplement, or enhance the resident’s function and/or safety.
“Fall” – refers to unintentionally coming to rest on the ground, floor, or other lower level, but not as a result of an overwhelming external force i.e. – resident pushes another resident. An episode where a resident lost their balance and would have fallen, if not for staff intervention, is considered a fall. A fall without injury is still a fall. Unless there is evidence suggesting otherwise, when a resident is found on the floor, a fall is considered to have occurred.
“Hazards” – refer to element of the resident environment that have the potential to cause injury or illness.

Accidents – F323Definitions
“Free of accident hazards as is possible” – refers to being free of accident hazards over which the facility has control.
“Supervision/Adequate Supervision” – refers to an intervention and means of mitigating the risk of an accident.
Facilities are obligated to provide adequate supervision to prevent accidents.

Accidents – F323Overview
Numerous and varied accident hazards exist in everyday life.
It is important that all facility staff understand the facility’s responsibility, as well as their own, to ensure the safest environment possible for residents.
The facility is responsible for providing care to residents in a manner that helps promote quality of life. This includes respecting residents’ rights to privacy,
dignity and self determination, and their right to make choices about significant aspects of their life in the facility.
The responsibility to respect resident’s choices is balanced by considering the potential impact of these choices on other individuals and the facility’s
obligation to protect the residents from harm.

Accidents – F323Identification of Hazards and Risks
Identification of Hazards and Risks - sources may include;
Quality assurance activities Environmental rounds MDS/CAAs data Medical history and physical exam Individual observation
This information is to be documented and communicated across all disciplines.

Accidents – F323Evaluation and Analysis
Evaluation and Analysis - may include;
Considering the severity of hazards The immediacy of risk Trends such as time of day, location etc.

Accidents – F323Implementation of Interventions
Implementation of Interventions which are consistent with relevant standards of care including evidence-based practices – process includes;
Communicating the interventions to all relevant staff Assigning responsibility Developing or revising policies and procedures Providing training as needed Repairing devices/equipment Documenting interventions Ensuring the interventions are put into place.

Accidents – F323Monitoring and Modification
Monitoring and Modification – processes include; Ensuring that interventions are implemented correctly and consistently Evaluating the effectiveness of interventions* Modifying or replacing interventions as needed Evaluating the effectiveness of new interventions

Accidents – F323Supervision
Supervision is an intervention and a means of mitigating accident risk.
Facilities are obligated to provide adequate supervision to prevent accidents.
What is adequate supervision?It is defined by type and frequency, based on the individual resident’s assessed
needs, and identified hazards in the resident environment.
Adequate supervision may vary from resident to resident and from time to time for the same resident. Tools or items such as personal alarms can help to
monitor a resident’s activities, but they do not eliminate the need for adequate supervision.

Accidents – F323Supervision & Resident Smoking
NFPA 101, the Life Safety Code - 19.7.4 reads, “…shall include not less than the following provisions:
1) Smoking shall be prohibited in any room, ward, or individual enclosed space where flammable liquids, combustible gases, or oxygen is used or stored and in any other hazardous location, and such areas shall be posted with signs that read NO SMOKING or shall be posted with the international symbol for no smoking.
2) In health care occupancies where smoking is prohibited and signs are prominently placed at all major entrances, secondary signs with language that prohibits smoking shall not be required.
3) Smoking by patients classified as not responsible shall be prohibited.4) The requirement of 19.7.4(3) shall not apply where the patient is under direct
supervision.5) Ashtrays of noncombustible material and safe design shall be provided in all areas
where smoking is permitted.6) Metal containers with self-closing cover devices into which ashtrays can be emptied
shall be readily available to all areas where smoking is permitted.

Accidents – F323Supervision & Resident to Resident Altercations
Assess, Care Plan, Implement, Monitor, and Evaluate
Certain situations or conditions may increase the potential for altercations; A history of aggressive behaviors including striking out, verbal outbursts, or
negative interactions with other resident(s). Behavior that tends to disrupt or annoy others such as constant crying,
yelling, calling out for help, making negative remarks, restlessness, repetitive behaviors, taking items that do not belong to them, going into others’ rooms, drawers, or closets, and undressing in inappropriate areas.
Although these behaviors may not be aggressive in nature, they may precipitate a negative response from others, resulting in verbal, physical, and/or emotional harm.

Accidents – F323Supervision & Resident to Resident Altercations
Possible interventions that could address potential/actual negative interactions include; Providing safe supervised areas for unrestricted movement Eliminating or reducing underlying causes of distressed behavior such as
boredom and pain Monitoring environmental influences such as temperatures, lighting and noise
levels Evaluating staffing assignments to ensure consistent staff who are more familiar
with the resident and who thus may be able to identify changes in a resident’s condition and behavior
Evaluating staffing levels to ensure adequate supervision* Ongoing staff training and supervision, including how to approach a resident
who may be agitated, combative, verbally or physically aggressive and how/when to obtain assistance in managing a resident with behavior symptoms

Accidents – F323Resident Risks and Environmental Hazards
In order to be considered hazardous, an element of the resident environment must be accessible to a vulnerable resident.
Resident vulnerability is based on risk factors including the individual resident’s functional status, medical condition, cognitive abilities, mood, and health treatments such as medications.
Resident vulnerability to hazards may change over time – hence, ongoing assessment helps to identify when elements pose hazards to a resident.

Accidents – F323Environmental Hazards
Improper actions or omissions by staff can create hazards in the building/grounds, environment, and/or with devices and equipment, i.e. – Fire doors that have been propped open Disabled locks or latches Nonfunctioning alarms Buckled or badly torn carpets, cords on floors, irregular walking surfaces Improper storage and access to toxic chemicals Exposure to unsafe heating unit surfaces and/or water temperatures Furniture that is not appropriate for a resident – chairs/beds that are too
low/high or unstable as to present a fall hazard Lighting that is either inadequate or so intense as to create a glare Devices such as pumps, ventilators, assistive devices may be hazardous
when they are defective, disabled, or used in a manner that is not per manufacturer’s recommendations or current standards of practice*

Accidents – F323Resident Vulnerabilities
Falls - contributing factors can include;
Environmental hazards Underlying medical conditions Medication side effects Lower extremity weakness Balance disorders Poor grip strength Functional and cognitive impairment Visual deficits

Accidents – F323Resident Vulnerabilities
Proper actions following a fall include:
Ascertaining if there were injuries and providing needed treatment; Determining what may have caused or contributed to the fall; Addressing the factors for the fall; Revising the resident’s plan of care and/or facility practices as need

Accidents – F323Unsafe Wondering or Elopement
…is random or repetitive locomotion.
It may be goal-directed such as searching for something like an exit or it may be aimless.
The non-goal-directed wandering requires a response in a manner that address both safety issues and an evaluation to identify root caused to the degree possible.
Moving about the facility aimlessly may indicate that the resident is frustrated, anxious, bored, hungry or depressed.

Accidents – F323Unsafe Wondering or Elopement
Unsafe wandering may occur when the resident at risk enters and area that physically hazardous or that contains potential safety hazards such as chemical, tools, equipment or out an exit door.
Elopement occurs when a resident leaves the premises or a safe area without authorization and/or any necessary supervision to do so.
A resident who leaves a safe area may be at risk of or has the potential to experience heat or cold exposure, dehydration and/or other medical complications, drowning or being struck by a motor vehicle.
Resident’s who are at risk for wandering should have interventions in their care plan to mitigate the risk.
The facility’s disaster and emergency preparedness plan should include a plan to locate a missing resident.

Accidents – F323Physical Plant Hazards
For a material to pose a safety hazard to a resident, it must be;
Toxic, caustic, or allergenic; Accessible and available in a sufficient amount to cause harm
Examples of materials that may pose a hazard to a resident could include; Chemicals used by the facility staff in the course of their duties
(housekeeping) and chemicals/or materials brought into the resident environment by staff, other residents or visitors;
Drugs and therapeutic agents; Plants and other “natural” materials found in the resident environment

Accidents – F323Physical Plant Hazards – Water temperature
Many residents in long-term care facilities have conditions that may put them at increased risk for burns, for example;
Decreased skin thickness Decreased skin sensitivity Peripheral neuropathy Decreased agility/reaction time Decreased cognition Decreased mobility Decreased ability to communicate

Accidents – F323Water Temperature Time required for a
3rd degree burn to occur
155°F 1 sec
148°F 2 sec
140°F 5 sec
133°F 15 sec
127°F 1 min
124°F 3 min
120°F 5 min

Accidents – F323Thermal burns
First-degree burns involve the top layer of skin such as a minor sunburn. These may present as red and painful to touch and the skin may show
mild swelling.
Second-degree burns involve the first two layers of skin. These may present as deep reddening of the skin, pain, blisters, glossy
appearance from leaking fluid, and possible loss of some skin.
Third-degree burns penetrate the entire thickness of the skin and permanently destroy tissue.
These present as loss of skin layers, often painless, dry and leathery skin (pain may be caused by presence of 1st & 2nd degree burns in the area surrounding the 3rd degree tissue damage).
Skin may appear charred or have patches that appear white, brown or black.

Accidents – F323Electrical Safety
Extension cords should not be used to take the place of adequate wiring in a facility.
If extension cords are used, the cords should be properly secured and not be place overhead, under carpets or rugs, or anywhere that the cord can cause trips, falls, or overheat.
Extension cords should be connected to only one device to prevent overloading of the circuit.
The cord itself should be of a size and type for the expected electrical load and made of material that will not fray or cut easily.
Electrical cords including extension cords should have proper grounding if required and should not have any grounding devices removed or not used if required.

Accidents – F323
Power strips may not be used as a substitute for adequate electrical outlets in a facility.
Power strips are not designed to be used with medical devices in patient care areas. Please read CMS S&C memo: 14-46-LSC regarding categorical waiver for power strips use in patient care areas.
Precautions needed if power strips are used include; Installing internal ground fault and over-current protection devices Preventing cords from becoming tripping hazards Using power strips that are adequate for the number and types of devices
used.
Electric blankets and heating pads Should not be tucked in or squeezed – constriction can cause the internal wires to break. Manufacturer’s instructions for use should be followed closely.

Accidents – F323Assistive Devices/Equipment Hazards
Training of staff, residents, family members and volunteers on the proper use of assistive devices/equipment is crucial to prevent accident.
Communicate clearly the approaches identified in the care plan to all staff, including temporary staff.
NOTE – The Safe Medical Devices Act of 1990 (SMDA) requires nursing home to report deaths, serious illness, and injuries associated with the use of medical devices to manufacturers and the Food and Drug Administration.

Accidents – F323Mobility devices include items such as canes, standard and rolling walkers, manual and powered wheelchairs.
Factors that may be associated with an increased accident risk related to mobility devices include; Resident condition Personal fit and device condition Staff practices
Mechanical assistive devices for transferring a resident include items such as total body lifts, sit-to-stand devices and transfer/gait belts.
Factors that may influence a resident’s risk of an accident during a transfer may include; Staff availability Resident abilities Staff training

Accidents – F323Devices with Entrapment Risks
Residents most at risk for entrapment may include –
those who are frail or elderly and/or;
those who have conditions such as • Agitation• Delirium• Confusion• Pain• Uncontrolled body movement• Hypoxia• Fecal impaction• Acute urinary retention

Accidents – F323
Entrapment may occur when a resident is caught between the mattress and bed rail or in the bed rail itself.
Resident beds must have proper fitting mattresses and when side rails are applied, they need also to be sturdy without wide spaces between the bars.
The use of a specialty air-filled mattress or a therapeutic air-filled bed may also present an entrapment risk that is different from rail entrapment with a regular mattress.
Precautions may include following manufacturer equipment alerts and increasing supervision.

Accidents– F323
Surveyor Investigative Protocol
Expect the SA to use this protocol when;
A sampled resident is at risk for (or who has a history of) accidents, falls, or unsafe wandering/elopement
A sampled resident is a risk to create a risk to others
When hazards/risks have been identified

Accidents– F323
The survey team is expected to make observations for and investigate potential hazards. This includes: Accessibility of chemicals, toxics or other hazards such as housekeeping
chemicals/supplies, medications, sharp utensils, and smoking materials; Environmental conditions such as unstable or slippery floor surfaces,
loose hand rails, excessive water temperatures, electrical hazards, insufficient or excessive light, arrangement of living spaces, obstacles in corridors, unsupervised access into or egress out of the facility, low or loose toile seats, defective or nonfunctioning beds;
Staff responses to verbal calls for help and alarms and response to potential/actual hazards such as cleaning of spilled liquids in a resident care area
Assistive devices (mechanical lifts etc.) that are defective or not used properly (according to manufacturer’s specifications

Accidents– F323
The survey team is expected to conduct interviews to determine the relationship between the resident’s risk and hazards.
Resident, family and/or responsible party; To identify if they had reported or help identify the resident’s risk for an
accident or hazard How and when staff responded to a hazard once it was identifiedStaff; To determine if they were aware of planned interventions to reduce a
resident’s risk for an avoidable accident If they reported potential resident risks or environmental hazards to the
supervisor according the facility policy If they are aware of and follow facility procedures correctly to remove or
reduce hazards.

Accidents– F323
The survey team is expected to conduct record review of the resident assessment instrument * to determine if the facility identified a risk(s), evaluated/analyzed the risk(s), implement interventions to try to prevent accidents and monitor/modify interventions as needed. Risk factors such as;
Unsafe wandering, elopement, ingesting nonfood items, altercations Hearing, visual, and sensory impairments Impaired physical functioning, balance or gait problems Diagnoses/conditions that could relate to safety awareness or safety
practices such as dementia, Parkinson’s, seizure disorder, vertigo, postural hypotension
Use of physical restraints and/or other devices that might limit movement Medications such as antidepressants, anticholinergics, diuretics,
psychotropics History of falls

Accidents– F323
Surveyor Investigative Protocol
The survey team is expected to conduct record review of the resident’s plan of care to determine if the facility developed interventions based on the risks and if the plan was modified as needed based on the response, outcomes, and needs of the resident.
If it is found that a resident has had an accident, the surveyor is expected to determine if the accident is the result of; An order not being followed; and/or A care need was not being addressed; and/or A plan of care not being implemented

Accidents – F323
Criteria for ComplianceFor the resident who has had an accident or was assessed at risk for an avoidable accident, the facility is in compliance if staff have: Identified the hazards and risks based on the facility’s assessment of both the
resident and the environment (including need for supervision and/or assistive devices);
Evaluated/analyzed the hazards/risks; Implemented interventions consistent with resident’s needs and current standards
of practice; Provided assistive devices consistent with the resident’s assessed needs Properly deployed and maintained resident specific equipment – lifts, canes,
wheelchairs etc. Provided a safe environment such as monitoring for chemicals, wet floors, and trip
hazards Operated equipment in accordance with manufacturers recommendations Provided and maintain a secure environment to prevent negative outcomes for
residents who exhibit unsafe wandering Monitored the effectiveness of the interventions and modified the interventions as
necessary, in accordance with current standards of practice.

Accidents - F323
Deficiency CategorizationSeverity Level 2 - indicates noncompliance that results in a resident outcome of no more than minimal discomfort and/or has the potential to compromise the resident’s ability to maintain or reach his or her highest practicable level of well being. The potential exists for greater harm to occur if interventions are not provided.
Bruising, minor skin abrasions, and rashes; Pain that does not impair normal activities; 1st degree burn; Medical evaluation or consultation may or may not have been necessary, and
tx such as first aid may been required; Fall(s) which resulted in no more than minimal harm because the facility had
additional established measure(s) that limited the injury or potential for injury; Unsafe wandering and/or elopement which resulted in no more than minimal
harm because of established measures that limited the resident’s exposure to hazards, i.e.-resident with Alzheimer’s left locked unit but found quickly unharmed on another unit.

Accidents - F323
Deficiency CategorizationSeverity Level 3 - indicates noncompliance that results in actual harm and can include but may not be limited to clinical compromise, decline, or the resident’s ability to maintain and/or reach their highest practicable well-being. Examples of compromise include:
Short-term disability; Pain that interfered with normal activities; 2nd degree burn; Fracture or other injury that may require surgical intervention and does not result
in significant decline in mental and/or physical functioning; Medical evaluation was necessary, and tx beyond first aid was required; Fall(s) that resulted in actual harm such as short-term disability, pain that
interfered with normal activities, fx or other injury that may require surgical intervention and does not result in significant decline in mental and/or physical functioning and the facility had established measure or practices to limit the resulting impact;
Unsafe wandering and/or elopement that resulted in actual harm and the facility had established measure or practices to limit the resulting impact.

Accidents - F323
Deficiency CategorizationSeverity Level 4 – immediate jeopardy condition; examples of negative outcomes that occurred or have the potential to occur as a result might include:
Esophageal damage due to ingestion of corrosive substances; Loss of consciousness related to head injuries; 3rd degree burn, or a 2nd degree burn covering a large surface area; Fracture or other injury that may require surgical intervention and results in significant
decline in mental and/or physical functioning; Electric shock due to use of unsafe or improperly maintained equipment; Entrapment Fall(s) with fracture or other injury that may require surgical intervention and/or
significant decline in functioning and the facility had no established measure(s) or practice(s) or ineffective measure(s) that would have prevented the fall or limited the resident’s injury
Unsafe wandering and/or elopement – resident leaves facility or locked unit unnoticed and sustained or had potential to sustain serious injury, impairment, harm or death and the facility had no established (or ineffective) measure(s) or practices(s), that would have prevented or limited the resident’s exposure to hazards

Accidents – F323Summary Statement of Deficiency
….Resident #XXX was observed sleeping in a low bed with a bed alarm in place. The ADON stated, “Resident #XXX has a history of falls and fracture of the nose….The resident’s minimum data set…dated 5/13/14 revealed that the resident’s cognition was severely impaired and required extensive assistance for most activities of daily living…the MDS noted that the resident had a history of falls and balance was unsteady, only able to stabilize with human assistance moving from seated to standing position and surface to surface transfers…Review of unplanned occurrence report dated 7/xx/13…revealed “resident calling for help. Observed resident lying on the floor near the foot of her bed…states she wanted to go to bed…The interdisciplinary post fall summary revealed…does not use call light, does not always ask for assist or wait for assistance. Staff heard alarm sounding and resident calling for help. Intervention: Recommend asking resident after dinner when she would like to go to bed to meet her bedtime preference and continue with alarms….Review of unplanned occurrence report dated 9/xx/13…resident yelling for help, alarm sounding, observed resident on floor…Preventative measures and/or corrective action: Resident to be put in carefoam chair for a nap after lunch, resident to stay in hallway…

Accidents – F323Summary Statement of Deficiency
…review of unplanned occurrence report dated 10/xx/13…revealed resident fell forward out of wheelchair as a staff member began to move her chair through the dining room doorway…preventative measures …assist to and from dining room. Assure resident sitting safely in wheelchair when assisting from the dining room….IDT met and concurred that not only does resident need assist in and out of dining room but assure she is sitting safely in wheelchair when assisting her. The ADON was queried as to what took place as stated, “they (staff) were assisting her out of the dining room. She went forward in her chair. Sometimes she scoots up and tries to stand”. When queried as to if staff was educated on ensuring the resident is sitting properly in chair before attempting to assist resident from the dining room, the ADON stated, “No, we didn’t feel that the staff did anything wrong. They were to assist her.”

Accidents – F323Summary Statement of Deficiency
…Review of unplanned occurrence report date 1/xx/14…revealed that resident was observed sitting on the floor mat on side of her bed. The post fall intervention was for the resident to be “up in carefoam chair. Naps to be in carefoam chair in hallway for monitoring.” The ADON was queried as to why resident was not in a carefoam chair for her after lunch nap at the time of the fall, and she stated, “That’s a problem. That was a previous intervention. I am not sure why it was not implemented….Review of unplanned occurrence report dated 2/xx/14 revealed resident found sitting on floor bedside bed. Preventative measures and/or corrective actions taken: when alarm sounds and resident at side of bed, get resident up in chair…Review of unplanned occurrence report dated 4/xx/14 revealed bed alarm sounding…resident sitting on the floor…Stated “I don’t know what happened. I was turning, turning, turning…” Preventative measures taken: ordered a winged mattress.

Accidents – F323Summary Statement of Deficiency
…Review of unplanned occurrence report dated 4/xx/14 revealed “called to dining room by activities aide. Resident observed on floor face down with chair alarm sounding…”during activities, writer called down…observed resident lying on right side face down on floor with blood coming out and from her nose…pain verbalized from resident on right lower extremity…resident has fractured nose from fall…conclusion from investigation:…fall happened after group activities was over. Activity assistant in dining room-not close enough to prevent fall….staff interview revealed “…didn’t see fall. I heard the fall. I was talking to (another resident and resident husband) and I heard the thump. Did you hear the alarm sounding? After I heard the thump…”…On 5/xx/14..the ADON stated, “there was no CNA education for the fall…(when staff assisted the resident out of the dining room). We felt there was no need for education…there is no documentation as to whether the bed was in low position or the mat in place for the incident on 2/xx/14 and no documentation as to why the resident had not been in the carefoam chair as ordered (incident on 1/xx/14)….”

Let’s take a pause here for any questions or comments regarding the
Accident tag – F323

Sanitary Conditions - F371483.35(i)(1)(2) The facility must procure food from sources approved or considered satisfactory by Federal, State or local authorities and store,
prepare, distribute and serve food under sanitary conditions
Nursing home residents risk serious complications from food-borne illness
as a result of their compromised health status.

Sanitary Conditions - F371
CMS recognizes the U.S. Food and Drug Administration’s (FDA) Food Code and the Centers
for Disease Control and Prevention’s (CDC) food safety guidance as national standards to procure, store, prepare, distribute and serve food in long
term care facilities in a safe and sanitary manner.
http://www.michigan.gov/documents/mdard/MI_Modified_2009_Food_Code_396675_7.pdfhttp://www.ntis.gov/products/food-code.aspx

Sanitary Conditions – F371
Epidemiological outbreak data repeatedly identify five major risk factors related to employee behaviors and preparation practices in food service establishments as contributing to food-borne illness:
•Improper holding temperatures•Inadequate cooking, such as undercooking raw shell eggs•Contaminated equipment•Food from unsafe sources, and•Poor personal hygiene

Sanitary Conditions - F371
Types of Food ContaminationBiological – pathogenic bacteria, viruses, toxins, and spores
Chemical – glass and oven cleaners, soaps, and insecticides.
Physical – foreign objects (staples, fingernails, jewelry, hair, glass, metal shavings from can openers, or pieces of bones) that may inadvertently enter the food.

Sanitary Conditions – F371Factors which may influence bacteria growth
Certain foods are considered more hazardous than other and are called “potentially hazardous foods (PHF) or Time/Temperature Controlled for Safety (TCS)” food (i.e. ground beef, poultry, chicken, seafood, cut melon, unpasteurized eggs, milk, yogurt and cottage cheese)
Time in conjunction with temperature controls of the food is critical. The longer food remains in the danger zone, the greater the risks for growth of harmful pathogens. Bacteria multiply rapidly in a moist environment in the danger zone. Freezing does not kill bacteria. Rapid death of most bacteria occurs at 165 degrees Fahrenheit (F) or above.

Sanitary Conditions - F371Other risk factors contributing of foodborne illness
Poor personal hygiene – employee health and hygiene are significant factors in preventing foodborne illness (e.g. – Norovirus)
Proper hand washing techniques and exclusion of infectious workers from handling food are critical in prevention
Bare hand contact with foods is prohibited. Staff should have access to proper hand washing facilities with available
soap (regular or anti-microbial), hot water, and disposable towels and/or heat/air drying methods.
Gloved hands are considered a food contact surface that can get contaminated or soiled. Failure to change gloves between tasks can contribute to cross-contamination.
Dietary staff must wear hear restraints – hairnet, hat, and/or beard restraint.
Nails are to be kept clean and neat

Sanitary Conditions - F371
Food from unsafe sources – those that are not approved or considered satisfactory by Federal, State, and local authorities.
Nursing homes are not permitted to use home-prepared or home-preserved (canned or pickled) foods for service to residents.
All residents have the right to accept food brought by any visitor for any resident.
Dry food storage – the focus of protection is to keep the items free from contaminants.
Recommended that foods stored in bins (i.e. four or sugar) be removed from their original packaging.
Keep food off the floor and clear of ceiling sprinklers, sewer/waste disposal pipes.

Sanitary Conditions – F371
Refrigerated storage – PHF/TCS foods must be maintained at or below 41 degrees F (unless otherwise specified by law). Prudent practices include:
Monitoring food temps and functioning of the refrigeration equip. daily and at routine intervals during all hours of operation
Placing hot food in containers (i.e. shallow pans) that permit food to cool rapidly
Separating raw animal foods (i.e. beef, fish, lamb, pork, poultry) from each other and storing raw meats on shelves below fruits, vegetables or other ready-to-eat foods
Labeling, dating, and monitoring refrigerated food, including, but not limited to leftovers, so it is used by its use-by day, or frozen (where applicable) or discarded.

Sanitary Conditions – F371Safe food preparation can reduce the risk of a foodborne illness
Cross-contamination can occur when harmful substance or disease-causing microbes are transferred to food by hands, food contact surfaces, sponges, cloth towels, or utensils that are not cleaned after touching raw food and then touch ready-to-eat goods.
Additional ways to help prevent cross-contamination include: Between uses, store towels/cloths used for wiping surfaces during the
kitchen’s daily operation in containers filled with sanitizing solution at the appropriate concentration per the manufacturer’s specifications.
Wash and sanitize cutting boards made of acceptable materials (e.g. hardwood, acrylic) and food processors, blenders, preparation tables, knife blades, can openers and slicers between uses.

Sanitary Conditions – F371Thawing foods properly can reduce the risk of a foodborne illness
Thawing frozen foods is often the first step in food prep.
Recommended methods to safely thaw frozen foods include: In a refrigerator, in a drip-proof container, and in a manner that prevents
cross-contamination. (anybody remember what that looks like?) Completely submerging the item under cold water, at a temp of 70
degrees F or below, and the water is running fast enough to agitate and float off loose ice particles.
Using microwave to thaw the item then cooking and serving immediately.
Thawing as part of a continuous cooking process.

Sanitary Conditions – F371 Final Cooking Temperatures
can reduce the risk of a foodborne illness
Foods should reach the following internal temperatures: Poultry and stuffed foods – 165 degrees (°) Fahrenheit (F) Ground meet (beef, pork), ground fish and eggs held for service – 155 ° F Fish and other meats – 145 ° F Unpasteurized eggs when cooked to order in response to resident
request and to be eaten promptly after cooking must be cooked until all parts of the egg are completely firm.
When cooking raw animal foods in the microwave, foods should be rotated and stirred during the cooking process so that all parts of the food are heated to a temp of at least 165 ° F and allowed to stand covered for at least 2 minutes after cooking to obtain temp equilibrium.
Fresh, frozen or canned fruits/vegetables – 135 ° F.

Sanitary Conditions - F371Reheating foods properly
can reduce the risk of a foodborne illness
The PHF/TCS food that is cooked and cooled must be reheated so that all parts of the food reach an internal temperature of 165 ° F for at least 15 seconds before holding for hot service.
Ready-to-eat foods that require heating before consumption are best taken directly from a sealed container (secured against the entry of micro’s) or an intact package from an approved food processing source and heated to at least 135 ° F for holding for hot service.
Note – using the steam table to reheat food is unacceptable since it does not bring the food to the proper temperature within acceptable timeframes.

Sanitary Conditions – F371
Cooling foods properlycan reduce the risk of a foodborne illness
Foods that have been cooked and held at improper temperatures promote the growth of disease-causing microorganisms that may have survived the cooking process (i.e. – spore-formers)
Cooked potentially hazardous foods that are subject to time and temperature control for safety are best cooled rapidly within 2 hours, from 135 to 70 ° F, and within 4 more hours to the temp of approx. 41° F.
The total time for cooling from 135 to 41 ° F should not exceed 6 hours.

Sanitary Conditions - F371Foods with “modified consistently”
can increase the risk of a foodborne illness
When pureed, ground, or diced food drop into the danger zone (below 135° F), the mechanically altered food must be reheated to 165° F for 15 seconds.

Sanitary Conditions - F371Pooled Eggs
can increase the risk of a foodborne illness
The facility should crack only enough eggs for immediate service in response to a resident’s request or as an ingredient immediately before baking.
Salmonella infections associated with unpasteurized eggs cans be prevented by using pasteurized shell eggs or be substituted for raw eggs in the preparation of foods that will not be thoroughly cooked (i.e. Caesar dressing, Hollandaise sauces, egg fortified beverages, ice cream and French toast)
Waivers to allow undercooked unpasteurized eggs for resident preference are not acceptable.
Pasteurized shell eggs are available and allow for safe consumption of undercooked eggs.

Sanitary Conditions – F371Food Service and Distribution also is a
factor in the development of a foodborne illness
Food safety requires consistent temperature control from the tray line to transport and distribution to prevent contamination (i.e. – covering food items).
The length of time needed to transport trays is more critical when the food is simply covered and transported in open or closed carts without a heated or cooled environment.
The maximum length of time that foods can be held on a steam table is a total of 4 hours. Monitoring of the temperature by food service workers while food is on the steam table is essential.
Foods may be reheated (only once) to 165 ° F. Reheated foods are best discarded if not eaten within two hours after
reheating.

Sanitary Conditions – F371 Food Service and Distribution also is a
factor in the development of a foodborne illness
Potential food handling problems/risks associated with food distribution include:
Staff distributing trays without first properly washing their hands. Serving food to residents after collecting soiled plates and food waste,
without proper hand washing. Food / Snacks left on trays or countertops beyond safe time and/or
temperature requirements Food / Snacks left in refrigerators beyond safe “use by” dates – including
foods that been opened but were not labeled Food / Snacks stored in open containers, without covers which allow for
potential cross-contamination Foods not maintained at safe temperature levels in refrigerators.

Sanitary Conditions – F371 Potential food handling problems/risks associated with food distribution - continued
Nursing homes with gardens are compliant with the food procurement requirements as long as the facility has and follows policies and procedures for maintaining the gardens.
If residents take prepared foods with them out of the facility (i.e. – bag lunches for resident attending dialysis, clinics, or day treatment programs etc.), the foods must be handled and prepared for them with the same safe and sanitary approached used during primary food prep in the facility.
Contamination risks associated with ice and water handling practices include staff who use poor hygiene, fail to wash hands adequately, or handle ice with their bare hands and failure to keep ice machines drained, cleaned and sanitized as needed/according to manufacturer’s specifications.

Sanitary Conditions – F371 Equipment and Utensil cleaning factors in the development of a foodborne illness
Machine Washing and Sanitizing
High Temp Dishwashing (heat sanitization)• Wash: 150 – 165 ° F• Final rinse: 180 ° F; or 165 ° F for a stationary rack, single
temperature machine
Low Temp Dishwashing (chemical sanitization)• Wash: 120 ° F• Final rinse: 50 ppm (parts per million) hypochlorite (chlorine) on
dish surface in final rinse.

Sanitary Conditions – F371 Equipment and Utensil cleaning factors in the development of a foodborne illness
Manual washing and Sanitizing
First step – through washing using hot water and detergent after food particles have been scraped.
Second step – rinsing with hot water to remove all soap residues.
Third step – sanitizing with either hot water or a chemical solution maintained at the correct concentration, based on periodic testing, and for the effective contact time according to manufacturer’s guidelines.• Hot water - at least 171 ° F for 30 seconds, or• Chlorine – 50-100 ppm minimum with 10 second contact time• Iodine – 12.5 ppm minimum with 30 second contact time• QAC space (Quaternary) – 150-200 ppm concentration and contact time per
manufacturer’s instructions.

Sanitary Conditions – F371 Equipment and Utensil cleaning factors in the development of a foodborne illness
Cleaning Fixed Equipment
When cleaning equipment that cannot readily be immersed in water such as mixers and slicers, the removable parts are washed and sanitized and non-removable parts are cleaned with detergent and hot water, rinsed, air-dried and sprayed with a sanitizing solution at the correct concentration.
Service area wiping cloths are cleaned and dried, or placed in a chemical sanitizing solution of appropriate concentration.

Sanitary Conditions - F371
Surveyor Investigative Protocol
Observations
Food procurement procedures
Food preparation procedures
Service of food during and after meal times
Storage of food

Sanitary Conditions - F371Interview(s) of:
Staff who performs the task about the procedures they follow to procure, store, prepare, distribute, and serve food
Dietary supervisor or dietician concerning:•Practice for dealing with employees who come to work coughing, sneezing, diarrhea, vomiting or with open wounds.
•How the facility identifies problems with time & temperature control of PHF/TCS foods and what are the processes to address those problems.
•Whether the facility and follows a cleaning schedule for the kitchen and food service equipment.
•If there is a problem with equipment, how staff informs maintenance and follows up to see if the problem is corrected
•Is the facility aware of current CDC and FDA nursing home egg handling and preparation policies and does the facility have written egg storage and preparation policies that honor resident preferences safely.

Sanitary Conditions - F371
Review of records:
Any facility documentation such as P&P’s related to compliance with food sanitation and safety. Determine if the food service employees have received relevant training
Food temperature records from tray line, refrigerator/freezer dishwasher temp records
Maintenance records such as work orders and manufacturer’s specifications
Facility infection control surveillance records for foodborne illness and actions related to suspected or confirmed outbreaks of GI illnesses.
The policies and procedures for maintaining nursing home gardens

Sanitary Conditions - F371
Criteria for Compliance
This is determined if staff;
Procures, stores, handles, prepares, distributes, and serve food to minimize the risk of foodborne illness.
Maintains PHF/TCS foods at safe temperatures, cools food rapidly, and prevents contamination during storage.
Cooks food to the appropriate temperature and holds PHF/TCS at or below 41 °F (for cold foods) or at or above 135 °F (for hot foods).
Utilizes proper hand washing and personal hygiene practices to prevent food contamination; and
Maintains equipment and food contact surfaces to prevent food contamination.

Sanitary Conditions - F371
Deficiency Categorization
Severity Level 2 - indicates noncompliance that results in a resident outcome of no more than minimal discomfort and/or has the potential to compromise the resident’s ability to maintain or reach his or her highest practicable level of well being. The potential exists for greater harm to occur if interventions are not provided.
Food service workers sliced roast port on the meat slicer. The meat slicer was not washed, rinsed, and sanitized after usage. The facility failed to educate and train staff on how to clean and sanitize all kitchen equipment.
During the initial tour of the kitchen, two food service workers were observed on the loading dock. One was smoking and the other was emptying trash. Upon returning to the kitchen, they proceeded to prepare food without washing their hands.

Sanitary Conditions - F371
Deficiency Categorization
Severity Level 3 - indicates noncompliance that results in actual harm that is not immediate jeopardy. The negative outcome can include but may not be limited to clinical compromise, decline, or the resident’s inability to maintain and/or reach his/her highest practicable level of well-being.
Outbreak of nausea and vomiting occurs in the facility related to the inadequate sanitizing of dishes and utensils;
Episode of food poisoning occurs because facility had an event in which tuna, chicken, and potato salads served in bulk were not kept adequately chilled and were still left out for eating after 5 hours

Sanitary Conditions - F371
Deficiency Categorization
Severity Level 4 – immediate jeopardy is a situation in which the facility’s noncompliance with one or more requirements has allowed/caused/resulted in or is likely to result in serious injury, harm, impairment, or death to a resident AND requires immediate correction, as the facility either created the situation or allowed the situation to continue by failing to implement preventive or corrective measures.
A roast (raw meat) thawing on a plate in the refrigerator had bloody juices overflowing and dripping onto uncovered salad greens on the shelf below. The contaminated salad greens were not discarded and were used to make salad for the noon meal.The facility had a recent outbreak of Norovirus after the facility allowed a food worker who was experiencing vomiting and diarrhea to continue preparing food. Observations and interviews indicate that other food services staff with GI illnesses are also permitted to prepare food.

Sanitary Conditions - F371
Summary Statement of Deficiency
On x/xx/xx at xx:xx a.m., during the initial tour of the kitchen with the Certified Dietary Manager (CDM) “C”, the small bucket of quaternary ammonia (QUAT) disinfectant solution stored in the dish machine room and used to clean food preparation surfaces was tested for the concentration level of the solution by Dietary Service Aide (DS) “H”. According to the test strip color when compared to the color chart on the test strip container, the concentration of the solution was less than 200 ppm (parts per million). DSA “H” stated the concentration should be at least 200 ppm to be effective. A second bucket under the steam table near the stove also tested with less than 200 ppm concentration of the disinfectant.

Sanitary Conditions - F371
Summary Statement of Deficiency
On x/xx/xx at xx:xx p.m., the small bucket the QUAT disinfectant solution stored in the food preparation room and used to clean food preparation surfaces was tested for the concentration level of the solution by Cook “D”. According to the test strip color when compared to the color chart on the test strip container, the concentration of the solution was less than 150 ppm. Cook “D” stated the concentration should be at least 150-300 ppm to be effective . During the same observation and interview, Cook “D” stated the disinfectant solution had been prepared at about 10:00 a.m. when she started her shift. Cook “D” stated the solution should be changed every 2 hours or when there was a lot of debris in it. On x/xx/xx at 2:47 p.m. on the same day CDM “C” provided the facility policy “Cleanliness & Sanitation…” for “sanitizer solution” dated x/xx/xx which reflected QUAT sanitizer must be mixed to 200 ppm and changed when dirty, cold or every 2 hours.

Sanitary Conditions - F371
Summary Statement of DeficiencyOn x/xx/xx at xx:xx p.m., a small cup of coleslaw in the holding refrigerator in the kitchenette next to the dining room was tested and found to be at 53 degrees Fahrenheit. Dining Services Aide “F” stated she had just put the coleslaw in the refrigerator after removing it from a resident’s place setting at a table in the dining room. DSA “F” stated the coleslaw had been put at a resident’s place at a table in the dining room at approximately xx:xx a.m. and when the resident did not come for lunch, the coleslaw was removed from the table, covered with plastic wrap, dated x/xx and put in the refrigerator for use the same day. DSA “F” stated she usually put the salad of the day out on the tables at the beginning of the dining service (11:30 a.m.) The coleslaw was at a table in the dining room unprotected from contamination for approximately 45 minutes and above the safe holding temperature of 41 degrees Fahrenheit according to the Food and Drug Association…209 Food Code…then, returned to the refrigerator for potential use later the same day.

Questions / Comments