Nasopharyngeal Carcinoma in Children: Comparison of Conventional and Intensity-Modulated...
9
CLINICAL INVESTIGATION Head and Neck NASOPHARYNGEAL CARCINOMA IN CHILDREN: COMPARISON OF CONVENTIONAL AND INTENSITY-MODULATED RADIOTHERAPY SIDDHARTHA LASKAR, M.D.,* GAURAV BAHL, M.D.,* MARYANN MUCKADEN, M.D.,* SURESH K. PAI, M.D., y TEJPAL GUPTA, M.D.,* SHRIPAD BANAVALI, M.D., y BRIJESH ARORA, D.M., y DAYANAND SHARMA, D.R.P., z PURNA A. KURKURE, M.D., y MUKTA RAMADWAR, M.D., x SEETHALAXHMI VISWANATHAN, M.D., x VENKATESH RANGARAJAN, D.N.B., { SAJID QURESHI, M.S., k DEEPAK D. DESHPANDE,PH.D., z SHYAM K. SHRIVASTAVA, M.D.,* AND KETAYUN A. DINSHAW, F.R.C.R.* Departments of *Radiation Oncology, y Medical Oncology, z Medical Physics, x Pathology, { Bio-Imaging, and k Surgical Oncology, Tata Memorial Hospital, Mumbai, India Purpose: To evaluate the efficacy of intensity-modulated radiotherapy (IMRT) in reducing the acute toxicities associated with conventional RT (CRT) in children with nasopharyngeal carcinoma. Patients and Methods: A total of 36 children with nonmetastatic nasopharyngeal carcinoma, treated at the Tata Memorial Hospital between June 2003 and December 2006, were included in this study. Of the 36 patients, 28 were boys and 8 were girls, with a median age of 14 years; 4 (11%) had Stage II and 10 (28%) Stage III disease at presentation. All patients had undifferentiated carcinoma and were treated with a combination of chemotherapy and RT. Of the 36 patients, 19 underwent IMRTand 17 underwent CRT. Results: After a median follow-up of 27 months, the 2-year locoregional control, disease-free, and overall survival rate was 76.5%, 60.6%, and 71.3%, respectively. A significant reduction in acute Grade 3 toxicities of the skin (p = 0.006), mucous membrane (p = 0.033), and pharynx (p = 0.035) was noted with the use of IMRT. The median time to the development of Grade 2 toxicity was delayed with IMRT (skin, 35 vs. 25 days, p = 0.016; mucous-membrane, 39 vs. 27 days, p = 0.002; and larynx, 50 vs. 28 days, p = 0.009). The duration of RT significantly influenced disease-free survival on multivariate analysis (RT duration >52 days, hazard ratio = 5.49, 95% confidence interval, 1.14–26.45, p = 0.034). The average mean dose to the first and second planning target volume was 71.8 Gy and 62.5 Gy with IMRT compared with 66.3 Gy (p = 0.001) and 64.4 Gy (p = 0.046) with CRT, respectively. Conclusion: The results of our study have shown that IMRT significantly reduces and delays the onset of acute tox- icity, resulting in improved tolerance and treatment compliance for children with nasopharyngeal carcinoma. Also, IMRT provided superior target coverage and normal tissue sparing compared with CRT. Ó 2008 Elsevier Inc. Nasopharynx, Carcinoma, Pediatric, Intensity-modulated radiotherapy, IMRT, Radiotherapy. INTRODUCTION Pediatric nasopharyngeal carcinoma (PNPC) is a rare disease that accounts for <1% of all childhood malignancies (1–4). Although the treatment guidelines for PNPC have evolved from those established for adults, it must be emphasized that PNPC is a distinct entity. The close association with World Health Organization (WHO) Type III (undifferenti- ated) histologic features and the high incidence of locore- gionally advanced disease have dictated the need for special considerations in the treatment of these children. Many previously reported studies on PNPC, including one from our institute, have documented the benefit of combined radiotherapy (RT) and chemotherapy compared with RT alone (5–9). Furthermore, a few reports have demonstrated a significant survival advantage for patients receiving a total RT dose of >66 Gy (2, 5, 6, 10–12). However, high radiation doses are associated with both acute and late treatment-re- lated adverse effects, leading to frequent treatment interrup- tions and an increased incidence of late morbidities. Intensity-modulated RT (IMRT) has gained popularity in the treatment of head-and-neck cancers in adults. According to the experiences with the use of IMRT for adults with naso- pharyngeal carcinoma (NPC) (13–17), it is expected that im- plementation of IMRT for PNPC would also translate into improved outcome with reduced treatment-related toxicities. In an attempt to define the role of this modality in the Reprint requests: Siddhartha Laskar, M.D., Department of Radi- ation Oncology, Tata Memorial Hospital, Dr. Ernest Borges Road, Parel, Mumbai 400 012, India. Tel: (+91) 22-2417-7167; Fax: (+91) 22-2414-6937; E-mail: [email protected] Conflict of interest: none. Received Dec 6, 2007, and in revised form Jan 13, 2008. Accepted for publication Jan 15, 2008. 728 Int. J. Radiation Oncology Biol. Phys., Vol. 72, No. 3, pp. 728–736, 2008 Copyright Ó 2008 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/08/$–see front matter doi:10.1016/j.ijrobp.2008.01.032
-
Upload
siddhartha-laskar -
Category
Documents
-
view
215 -
download
2
Transcript of Nasopharyngeal Carcinoma in Children: Comparison of Conventional and Intensity-Modulated...

CLINICAL INVESTIGATION Head and Neck
NASOPHARYNGEAL CARCINOMA IN CHILDREN: COMPARISON OFCONVENTIONAL AND INTENSITY-MODULATED RADIOTHERAPY
SIDDHARTHA LASKAR, M.D.,* GAURAV BAHL, M.D.,* MARYANN MUCKADEN, M.D.,*
SURESH K. PAI, M.D.,y TEJPAL GUPTA, M.D.,* SHRIPAD BANAVALI, M.D.,y BRIJESH ARORA, D.M.,y
DAYANAND SHARMA, D.R.P.,z PURNA A. KURKURE, M.D.,y MUKTA RAMADWAR, M.D.,x
SEETHALAXHMI VISWANATHAN, M.D.,x VENKATESH RANGARAJAN, D.N.B.,{ SAJID QURESHI, M.S.,k
DEEPAK D. DESHPANDE, PH.D.,z SHYAM K. SHRIVASTAVA, M.D.,* AND KETAYUN A. DINSHAW, F.R.C.R.*
Departments of *Radiation Oncology, yMedical Oncology, zMedical Physics, xPathology, {Bio-Imaging, and kSurgical Oncology,Tata Memorial Hospital, Mumbai, India
Purpose: To evaluate the efficacy of intensity-modulated radiotherapy (IMRT) in reducing the acute toxicitiesassociated with conventional RT (CRT) in children with nasopharyngeal carcinoma.Patients and Methods: A total of 36 children with nonmetastatic nasopharyngeal carcinoma, treated at the TataMemorial Hospital between June 2003 and December 2006, were included in this study. Of the 36 patients, 28were boys and 8 were girls, with a median age of 14 years; 4 (11%) had Stage II and 10 (28%) Stage III diseaseat presentation. All patients had undifferentiated carcinoma and were treated with a combination of chemotherapyand RT. Of the 36 patients, 19 underwent IMRT and 17 underwent CRT.Results: After a median follow-up of 27 months, the 2-year locoregional control, disease-free, and overall survivalrate was 76.5%, 60.6%, and 71.3%, respectively. A significant reduction in acute Grade 3 toxicities of the skin (p =0.006), mucous membrane (p = 0.033), and pharynx (p = 0.035) was noted with the use of IMRT. The median time tothe development of Grade 2 toxicity was delayed with IMRT (skin, 35 vs. 25 days, p = 0.016; mucous-membrane, 39vs. 27 days, p = 0.002; and larynx, 50 vs. 28 days, p = 0.009). The duration of RT significantly influenced disease-freesurvival on multivariate analysis (RT duration >52 days, hazard ratio = 5.49, 95% confidence interval, 1.14–26.45,p = 0.034). The average mean dose to the first and second planning target volume was 71.8 Gy and 62.5 Gy withIMRT compared with 66.3 Gy (p = 0.001) and 64.4 Gy (p = 0.046) with CRT, respectively.Conclusion: The results of our study have shown that IMRT significantly reduces and delays the onset of acute tox-icity, resulting in improved tolerance and treatment compliance for children with nasopharyngeal carcinoma.Also, IMRT provided superior target coverage and normal tissue sparing compared with CRT. � 2008 ElsevierInc.
Nasopharynx, Carcinoma, Pediatric, Intensity-modulated radiotherapy, IMRT, Radiotherapy.
Int. J. Radiation Oncology Biol. Phys., Vol. 72, No. 3, pp. 728–736, 2008Copyright � 2008 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/08/$–see front matter
doi:10.1016/j.ijrobp.2008.01.032
INTRODUCTION
Pediatric nasopharyngeal carcinoma (PNPC) is a rare disease
that accounts for <1% of all childhood malignancies (1–4).
Although the treatment guidelines for PNPC have evolved
from those established for adults, it must be emphasized
that PNPC is a distinct entity. The close association with
World Health Organization (WHO) Type III (undifferenti-
ated) histologic features and the high incidence of locore-
gionally advanced disease have dictated the need for
special considerations in the treatment of these children.
Many previously reported studies on PNPC, including one
from our institute, have documented the benefit of combined
radiotherapy (RT) and chemotherapy compared with RT
Reprint requests: Siddhartha Laskar, M.D., Department of Radi-ation Oncology, Tata Memorial Hospital, Dr. Ernest Borges Road,Parel, Mumbai 400 012, India. Tel: (+91) 22-2417-7167; Fax:(+91) 22-2414-6937; E-mail: [email protected]
72
alone (5–9). Furthermore, a few reports have demonstrated
a significant survival advantage for patients receiving a total
RT dose of >66 Gy (2, 5, 6, 10–12). However, high radiation
doses are associated with both acute and late treatment-re-
lated adverse effects, leading to frequent treatment interrup-
tions and an increased incidence of late morbidities.
Intensity-modulated RT (IMRT) has gained popularity in
the treatment of head-and-neck cancers in adults. According
to the experiences with the use of IMRT for adults with naso-
pharyngeal carcinoma (NPC) (13–17), it is expected that im-
plementation of IMRT for PNPC would also translate into
improved outcome with reduced treatment-related toxicities.
In an attempt to define the role of this modality in the
Conflict of interest: none.Received Dec 6, 2007, and in revised form Jan 13, 2008.
Accepted for publication Jan 15, 2008.
8

IMRT for nasopharyngeal carcinoma in children d S. LASKAR et al. 729
management of PNPC, we prospectively reviewed our expe-
rience and compared our results with those of children treated
using conventional RT (CRT) during the same period.
PATIENTS AND METHODS
Patient characteristicsA total of 36 children with nonmetastatic PNPC were treated at
the Tata Memorial Hospital (Mumbai, India) between June 2003
and December 2006. The patient age at presentation ranged from
5 to 18 years (median, 14). Of the 36 patients, 28 were boys and 8
were girls (male/female ratio, 3.5:1). Most (92%) presented with
cervical lymphadenopathy. Other common presenting symptoms
were nasal obstruction or discharge (64%), epistaxis (44%), and
headache (25%). The initial staging evaluation included a complete
history and physical examination, endoscopy and biopsy, complete
blood count determination, liver and renal function tests, chest
X-ray, and computed tomography (CT) or magnetic resonance im-
aging of the head-and-neck region. CT scans of the abdominopelvis
or chest, bone scans, and positron emission tomography scans
were done when clinically indicated. Patients underwent clinically
staging according to the American Joint Committee on Cancer stag-
ing system (6th edition) (18). Only 4 patients (11%) had Stage II dis-
ease at presentation. Table 1 lists the demographic features of the
patient population. The histopathologic review was done by experi-
Table 1. Patient characteristics
Characteristic CRT IMRT
Gender (n)Male 14 14Female 3 5
Age (y)#14 9 12>14 8 7
Tumor volume (cm3)#70 7 13>7 10 6
T stage (n)T1 0 2T2a 3 2T2b 1 7T3 5 4T4 8 4
N stage (n)N1 2 4N2 4 8N3a 10 7N3b 1 0
Overall stage (n)I 0 0IIA 0 0IIB 1 3III 3 7IVA 2 2IVB 11 7
Response to neoadjuvant chemotherapy (n)CR/PR 8 9SD/PD 9 10
Abbreviations: CRT = conventional radiotherapy; IMRT = inten-sity-modulated RT; CR = complete response; PR = partial response;SD = stable disease; PD = progressive disease.
enced pathologists at our institute, who classified the tumors accord-
ing to the WHO system. All 36 children had the undifferentiated
(WHO Type III) variant of PNPC.
Treatment detailsAll children were treated with a radical intent using a combina-
tion of chemotherapy and RT. The chemotherapy regimen con-
sisted of a combination of cisplatin (20 mg/m2 on Days 1–5),
bleomycin (10 U on Days 1 and 8), and methotrexate (50 mg/m2
on Days 1 and 8), with each cycle repeated after 4 weeks (5). A
total of four cycles of chemotherapy were administered, two before
(neoadjuvant) and two after (adjuvant) RT. RT, either IMRT (n =
19) or CRT (n = 17), was initiated 3–4 weeks after completion of
the second cycle of chemotherapy. The choice of RT technique
was the treating physician’s decision and was determined by logis-
tic factors.
Target volume delineationThe gross tumor volume included the gross disease in the naso-
pharynx as determined from the CT and endoscopic findings. Posi-
tron emission tomography-CT images were not used for target
volume delineation or treatment planning. Grossly positive lymph
nodes were included in this volume. The clinical target volume
(CTV) included the gross tumor volume and adjacent areas consid-
ered to contain potential microscopic disease. Three CTVs were de-
fined. CTV1 included the nasopharyngeal primary, retropharyngeal
lymph node region, and lymph node levels with positive nodes.
CTV2 was a concentric volume that completely encompassed the
entire CTV1 and included the pterygoid fossae, parapharyngeal
space, inferior sphenoid sinus, skull base, and posterior third of
the nasal cavity and maxillary sinuses. The CTV2 also included
the high-risk lymph node levels, which were defined as the next ech-
elon of lymph nodes beyond the grossly involved nodes. Finally,
CTV3 consisted of the low-risk lymph node levels, defined as those
distal to the high-risk lymph nodes. The planning tumor volumes
(PTV1, PTV2, and PTV3) were defined according to the three
CTVs. A margin of 5 mm was allowed around each CTV to generate
the respective PTV. The PTVs were restricted to 4 mm within the
skin (body) contour.
Critical normal structures, including the brain stem, spinal cord,
optic nerves and chiasm, pituitary, parotid glands, inner ears, eyes,
and temporal lobes, were outlined. The planning organ-at-risk vol-
umes were generated for the spinal cord and brainstem and defined
as 3 mm larger in all directions than the corresponding structure.
Treatment planning and dose specificationsOf the 36 patients, 17 were treated with CRT using the standard
three-phase shrinking-field technique to the target volumes, as de-
scribed in our previous publication (5). A total dose of 70.2 Gy
was delivered in daily fractions of 1.8 Gy, 5 d/wk. The spinal
cord was shielded after 45 Gy, and the posterior cervical lymphatic
chains were treated with 6–12-MeV electrons. Involved neck nodes
received about 59.4–66.6Gy.
For the 19 patients treated with IMRT, treatment plans were gen-
erating using the Varian Cadplan Plus (n = 5) or Eclipse, version
7.4.1 (n = 14) treatment planning system. Treatment was delivered
on a Varian (2100 CD or 6 Ex) linear accelerator with dynamic mul-
tileaf collimators using the sliding window technique with 6-MV
photons.
The three PTVs, PTV1, PTV2, and PTV3, were planned to re-
ceive 70.2 Gy in 33 fractions at 2.13 Gy/fraction, 59.4 Gy in 33 frac-
tions at 1.8 Gy/fraction, and 52.8 Gy in 33 fractions at 1.6 Gy/

730 I. J. Radiation Oncology d Biology d Physics Volume 72, Number 3, 2008
Table 2. Prognostic factors for clinical outcome
Treatment response LRC DFS OS
Prognostic factors n CR rate (%) p 2-y (%) p 2-y (%) p 2-y (%) p
Gender 0.172 0.094 0.116 0.338Male 28 75.0 67.68 50.45 64.42Female 8 100 100 87.50 87.50
Age (y) 0.418 0.309 0.331 0.440#14 21 85.7 81.48 64.96 85.56>14 15 73.3 70.62 59.26 65.45
Maximal tumor diameter (cm) 0.394 0.005 0.004 0.243#6 22 86.4 95.45 84.78 84.01>6 14 71.4 48.70 32.14 58.37
Tumor volume (cm3) 0.120 0.008 0.006 0.065#70 20 90.0 95.00 84.38 88.21>70 16 68.8 49.72 33.04 54.48
T stage 0.067 0.199 0.040 0.533T1-T2 15 93.3 86.15 78.32 84.41T3 9 77.8 87.50 77.78 76.20T4 12 66.7 50.00 25.93 55.90
N stage 0.402 0.042 0.042 0.444N1-N2 18 88.9 94.44 81.16 81.48N3 18 72.2 58.96 38.27 60.33
Overall stage 0.209 0.109 0.147 0.277II-III 14 92.9 92.86 77.92 84.42IV 22 72.7 63.35 45.01 61.00
RT technique 0.219 0.201 0.477 0.641CRT 17 70.6 68.28 55.76 66.74IMRT 19 89.5 84.21 67.54 80.81
Response to neoadjuvantchemotherapy
0.408 0.206 0.050 0.029
CR/PR 17 88.2 86.88 79.64 92.31SD/PD 19 73.7 64.74 42.80 54.32
Acute toxicity during RT 0.005 0.002 0.007 0.151Grade 1-2 23 95.7 92.31 78.30 84.85Grade 3-4 13 53.8 51.28 34.62 53.95
Total RT duration (d) 0.021 0.001 0.001 0.111#52 20 95.0 100.0 88.41 87.40>52 16 62.5 49.20 33.90 57.80
Abbreviations: LRC = locoregional control; DFS = disease-free survival; OS = overall survival; other abbreviations as in Table 1.
fraction, respectively. Treatment was delivered once daily, five frac-
tions weekly. The mean, minimal, and maximal doses for the PTVs
were recorded, along with the percentage of volume receiving <93%
and >110% of the prescribed dose. For the critical normal organs
with serially arranged functional subunits (brain stem, spinal cord,
optic nerves and chiasm) the dose to 5% and 10% of the volume
was recorded. For other normal organs, the mean dose and dose to
50% and 80% of the volume were documented.
Plans for each treatment phase were generated on the treatment
planning system and then combined to obtain the dose–volume
data. The dose–volume histograms from these retrospectively gen-
erated plans were then analyzed and compared with those obtained
for the patients treated with IMRT.
Reviews and follow-upAcute RT-related toxicities were documented according to the
Radiation Therapy Oncology Group guidelines. At each follow-up
visit, a complete physical examination (including endoscopy if re-
quired) was performed. A post-therapy positron emission tomogra-
phy-CT scan was obtained for all patients at 3 months after treatment
completion. Late radiation effects were evaluated and scored
according to the Radiation Therapy Oncology Group/European Or-
ganization for Research and Treatment of Cancer late effects scale.
Quantitative measurement of unstimulated whole mouth saliva us-
ing the spit method was done at each follow-up visit to determine
the grade of xerostomia. A pure-tone audiogram, an ophthalmologic
evaluation, and dental checkup were done on the second follow-up
visit and then yearly.
Statistical analysisAcute and late toxicities, the response to treatment, locoregional
control (LRC), disease-free survival (DFS), and overall survival
(OS) were the endpoints reviewed in this study. The disease status
for all surviving children was updated as of June 2007. Responses
were documented as defined by the WHO criteria (18). Univariate
and multivariate analyses were performed for evaluation of the prog-
nostic factors. Dosimetric data, including the mean, median, mini-
mal, and maximal dose, or dose to percentage of the volume of
various organs, were compared for both treatment types using the
Student t test. Acute RT toxicities among the two treatment groups
were compared using the chi-square test.

IMRT for nasopharyngeal carcinoma in children d S. LASKAR et al. 731
RESULTS
After a median follow-up of 27 months (range, 4–42), 24
patients (69%) were alive and without disease, 4 (11%)
were alive with disease, 7 (20%) had died of disease, and 1
had died of adjuvant chemotherapy-related febrile neutrope-
nia. The complete response rate at therapy completion was
80.6%. The 2-year LRC, DFS, and OS rate was 76.53%,
60.69%, and 71.36%, respectively.
Prognostic factorsOn univariate analysis, children with lesions >6 cm in the
maximal diameter on the initial CT scan had a significantly
Table 3. Multiple covariate Cox regression analysis for prognostic factors
LRC DFS OS
Variable p HR 95% CI p HR 95% CI p HR 95% CI
Tumor volume >70 cm3 — — — — — — — — —Stage T4 — — — 0.024 3.80 1.19–12.11 — — —Stage N3 — — — — — — — — —Grade 3-4 acute toxicity 0.048 8.75 1.02–75.11 — — — — — —RT duration >52 d — — — 0.034 5.49 1.14–26.45 — — —No response to neoadjuvant
chemotherapy— — — — — — 0.053 7.28 0.98–59.33
Abbreviations: HR = hazard ratio; CI = confidence interval; RT = radiotherapy; other abbreviations as in Table 2.
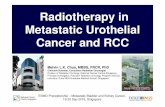
Fig. 1. Locoregional control (LRC) stratified by prognostic factors (Kaplan-Meier method). (A) Tumor volume, (B) nodalstage, (C) total radiotherapy (RT) duration, and (D) grade of acute radiotherapy toxicity.

732 I. J. Radiation Oncology d Biology d Physics Volume 72, Number 3, 2008
poor outcome. The LRC and DFS rate for these two groups
was 48.70% vs. 95.45% (p = 0.005) and 32.14% vs.
84.78% (p = 0.004), respectively. Other patient-related fac-
tors that had a statistically significant influence on survival
included tumor volume $70 cm3 (LRC, 49.72% vs.
95.0%, p = 0.008; DFS, 33.04% vs. 84.38%, p = 0.006),
Stage N3 (LRC, 58.96% vs. 94.44%, p = 0.042; DFS,
38.27% vs. 81.16%, p = 0.042), and T stage (Table 2 and
Fig. 1). The DFS rate was 78.32% for those with Stage T1
and T2 tumors, 77.78% for those with Stage T3, and
25.93% for those with Stage T4 disease (p = 0.040). How-
ever, none of these patient-related prognostic factors signifi-
cantly affected the OS. On multivariate analysis, only T stage
(Stage T4, hazard ratio = 3.80, 95% confidence interval,
1.19–12.11, p = 0.024) retained statistical significance for
DFS (Table 3).
Acute toxicityTreatment with IMRT significantly reduced the incidence
of Grade 3 toxicity of the skin (p = 0.006), mucous membrane
(p = 0.033), and pharynx and esophagus (p = 0.035; Table 4).
Furthermore, Grade 2 acute xerostomia (salivary gland,
31.6% vs. 88.2%, p = 0.002) and Grade 2 dysphagia (pharynx
and esophagus, 42.0% vs. 94.1%, p = 0.010) were signifi-
Table 4. Acute RT toxicities
IMRT CRT
Toxicity n % n % p
SkinGrade $2 16 84.2 17 100 0.136Grade $3 1 5.3 8 47.1 0.006
Mucous membraneGrade $2 15 78.9 17 100 0.066Grade $3 3 15.8 9 52.9 0.033
LarynxGrade $2 10 53.6 13 76.5 0.095Grade $3 2 10.5 6 35.3 0.114
Pharynx and esophagusGrade $2 8 42.0 16 94.1 0.010Grade $3 2 10.5 7 41.2 0.035
Salivary glandGrade $2 6 31.6 15 88.2 0.002
Abbreviations as in Table 1.
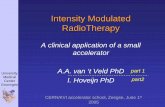
cantly less in children treated with IMRT. The median time
from starting RT to the development of Grade 2 toxicity
was considerably delayed in children treated with IMRT
compared with the interval in those treated with CRT (skin,
35 vs. 25 days, p = 0.016; mucous membrane, 39 vs. 27
days, p = 0.002; larynx, 50 vs. 28 days, p = 0.009). The me-
dian time to the development of Grade 2 acute xerostomia
and Grade 2 dysphagia was 32 days (95% confidence inter-
val, 25.28–38.72) and 27 days (95% confidence interval,
24.35–29.65), respectively, for patients receiving CRT. The
median had not yet been reached for the patients treated
with IMRT (Table 5 and Fig. 2). Six children treated with
CRT lost >15% of their body weight during the RT course
and required nutritional support in the form of nasogastric
tube feeding. None of the children receiving IMRT did so.
Furthermore, 5 patients treated with CRT required an inter-
ruption in their treatment of >5 days because of Grade 3 or
greater RT-induced acute toxicity. For 2 patients receiving
CRT, treatment was concluded at 66.6 Gy instead of the
planned 70.2 Gy because of the severe toxicity and poor gen-
eral condition. None of the children treated with IMRT re-
quired a treatment interruption or dose reduction. The
median time required to complete RT was 52 days (49 for
IMRT and 54 for CRT). Eleven patients (65%) treated with
CRT required more than the median of 52 days to complete
the RT course compared with only 5 (26%) of the children
who received IMRT (p = 0.020, chi-square test).
Treatment-related outcomeAt the analysis, locoregional failure had developed in 7 pa-
tients. The failure was at the primary site (nasopharynx) in 5
of these children and at a neck nodal region in the other 2. The
sites of locoregional failures in all these patients were com-
pletely within the RT portals scheduled to receive 70 Gy.
Six children developed distant metastasis (one of whom
also had locoregional failure). The site of metastasis was
the liver in 3 children and bone in the other 3.
Of the 36 patients, 17 (47.2%) responded well to the
neoadjuvant chemotherapy (complete response or partial
response) and had a significantly better outcome com-
pared with the 19 (52.8%) who did not (stable disease
or progressive disease). The DFS and OS rates for these
two groups were 79.64% vs. 42.80% (p = 0.050) and
92.31% vs. 54.32% (p = 0.029), respectively. No
Table 5. Median time to development of Grade 2 toxicity after starting RT
IMRT CRT
Toxicity Median time (d) 95% CI Median time (d) 95% CI p
Skin 35 32.87–37.13 25 21.77–28.23 0.016Mucous membrane 39 28.65–43.35 27 24.35–29.65 0.002Larynx 50 47.76–53.23 28 21.90–34.05 0.009Pharynx and esophagus NR — 27 24.35–29.65 <0.001Salivary gland NR — 32 25.28–38.72 <0.001
Abbreviations: CI = confidence interval; NR = not reached; other abbreviations as in Table 1.

IMRT for nasopharyngeal carcinoma in children d S. LASKAR et al. 733
significant difference was found in the LRC, DFS, or OS
rate for patients treated with IMRT vs. CRT (Table 2).
However, the total RT duration and the grade of acute
toxicity influenced the final outcome (Fig. 1). The com-
plete response rate (95.0% vs. 62.5%, p = 0.021), LRC
rate (100% vs. 46.2%, p = 0.001), and DFS rate
(88.4% vs. 33.9%, p = 0.001) were significantly superior
Days after starting Radiation Therapy
56494235282114
Gra
de I
I A
cute
Ski
n T
oxic
ity F
ree
Stat
us
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Days after starting Radiation Therapy
56494235282114
Gra
de
II M
uco
siti
s F
ree
Sta
tus
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
Days after starting Radiation Therapy
7063564942352821
Gra
de
II A
cute
Xer
ost
om
ia F
ree
Sta
tus
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
IMRT: Median 39 days
(95% CI: 28.6 – 43.3)
Conventional RT:
Median 27 days
(95% CI: 24.3 – 29.6) B
P = 0.016
IMRT: Median not reached
Conventional RT:
Median 32 days
(95% CI: 25.3 – 38.7) C
P <0.001
IMRT: Median 35 days
(95% CI: 32.8 – 37.1)
Conventional RT:
Median 25 days
(95% CI: 21.8 – 28.3) A
P = 0.016
Fig. 2. Median time to development of Grade 2 toxicity after start-ing radiotherapy (intensity-modulated radiotherapy [IMRT] vs. con-ventional RT). (A) Acute skin toxicity, (B) mucositis, and (C) acutexerostomia. CI = confidence interval.
for the children who completed RT in #52 days (Table 2).
The total RT duration retained statistical significance
for DFS when entered in the multivariate analysis with
the other prognostic factors (RT duration >52 days, haz-
ard ratio = 5.49, 95% confidence interval, 1.14–26.45,
p = 0.034; Table 3).
Late toxicityIn this report, we have detailed our early results, and a de-
tailed analysis of late toxicity will be done after longer fol-
low-up. At the analysis, the most frequent late toxicity
documented was xerostomia. The greatest grade for patients
treated with CRT was Grade 1 in 6, Grade 2 in 9, and Grade
3 in 2. In contrast, the highest grade for patients undergoing
IMRT was Grade 0 in 2, Grade 1 in 14, and Grade 2 in 3.
Subcutaneous fibrosis (Grade 2) was reported in 5 patients
treated with CRT and 2 children treated with IMRT. A total
of 5 children (IMRT, n = 1; CRT, n = 4) developed sensory-
neural hearing loss for higher frequencies (4,000 Hz). This
was symptomatic in 2 patients and discovered only on the
follow-up pure tone audiogram for the other 3. One child
treated with IMRT developed a superonasal visual field def-
icit, as determined by perimetry on the second follow-up
visit.
Dose–volume analysisThe IMRT and CRT plans were compared using dose–vol-
ume histograms (Table 6). Although the prescription dose
was 70.2 Gy to PTV1 and 59.4 Gy to PTV2, the average
mean dose to PTV1 was 71.8 Gy and 62.5 Gy to PTV2
with IMRT vs. 66.3 Gy (p = 0.001) and 64.4 Gy (p =
0.046) with CRT. IMRT resulted in superior target coverage,
with only 0.9% of PTV1 and 1.64% of PTV2 receiving <93%
of the prescribed dose. However, with CRT, the gross tumor
received an average of 4 Gy less than the prescribed dose.
Furthermore, 5.3% of PTV1 received <93% of the prescribed
dose. Using IMRT, on average, 1.15% of the PTV1 received
>110% of the prescribed dose; however, no amount of the
PTV1 treated with CRT received >110% of the prescribed
dose.
Superior sparing of almost all critical structures occurred
with the use of IMRT. The dose to the parotid glands, spinal
cord, optic chiasm, inner ears, and brain stem was signifi-
cantly greater with CRT (Table 6). The mean dose to the pa-
rotid glands was 37.17 Gy (right) and 39.44 Gy (left) using
IMRT vs. 57.31 Gy and 56.82 Gy with CRT, respectively.
However, the use of IMRT did not result in significant spar-
ing of the optic nerves or pituitary gland (Table 6).
DISCUSSION
It has been well established that a combination of RT and
chemotherapy can be considered the standard of care for
treatment of PNPC (4–6). The Rare Cancer Network study
on PNPC reported that a radiation dose of >66 Gy resulted
in a significantly better outcome (LRC rate of 90% vs.
73%, p = 0.01) (6). Similarly, in a previous report from our

734 I. J. Radiation Oncology d Biology d Physics Volume 72, Number 3, 2008
Table 6. Dose–volume statistics derived from dose–volume histograms
Variable IMRT CRTDifference between
means 95% CI p
PTV1Mean dose (Gy) 71.80 (67.7–74.8) 66.27 (64.6–69.4) 5.53 4.46–6.60 0.001Minimal dose (Gy) 55.92 (43.1–64.0) 51.84 (42.0–58.0) 4.08 0.42–8.59 0.074Maximal dose (Gy) 77.23 (70.6–83.5) 72.25 (68.6–75.0) 4.98 2.45–7.50 0.001Volume receiving <93%
of prescribed dose (%)0.94 (0.02–2.70) 5.30 (1.6–16.2) 4.30 2.04–6.67 0.020
Volume receiving >110%of prescribed dose (%)
1.15 (0.00–5.60) 0 1.15 0.265–2.04 0.014
PTV2Mean dose (Gy) 62.53 (57.9–67.2) 64.43 (62.2–66.8) 1.89 0.03–3.76 0.046Minimal dose (Gy) 47.66 (35.6–54.3) 44.19 (38.9–49.8) 3.47 0.12–6.84 0.043Maximal dose (Gy) 72.42 (68.1–80.1) 69.12 (65.8–72.5) 3.30 0.40–6.20 0.030Volume receiving <93%
of prescribed dose (%)1.64 (0.03–6.20) 4.05 (2.0–8.1) 2.40 1.01–3.78 0.005
Brain stemMean dose (Gy) 32.01 (15.4–47.9) 49.32 (39.7–59.40) 17.31 11.4–23.2 0.000Dose to 5% volume (Gy) 48.85 (31.1–59.8) 55.95 (44.0–69.10) 7.10 2.05–12.15 0.010Dose to 10% volume (Gy) 46.07 (30.0–57.0) 50.43 (40.0–66.0) 4.36 0.37–9.00 0.070
Spinal cordMean dose (Gy) 35.16 (25.0–46.5) 47.73 (40.1–53.4) 12.58 8.81–16.34 0.000Dose to 5% volume (Gy) 44.87 (37.9–53.0) 55.56 (48.0–64.7) 10.69 7.30–14.08 0.000Dose to 10% volume (Gy) 42.77 (34.0–49.1) 51.05 (43.0–66.3) 8.27 4.76–11.78 0.000
ChiasmMean dose (Gy) 24.01 (2.8–61.9) 36.71 (6.9–64.5) 6.00 0.45–24.9 0.043Dose to 5% volume (Gy) 28.91 (2.9–67.9) 45.24 (12.0–68.8) 6.47 3.1–29.5 0.017Dose to 10% volume (Gy) 27.01 (2.8–67.3) 38.93 (8.9–66.1) 6.36 1.06–24.90 0.071
Right optic nerveMean dose (Gy) 17.94 (1.8–39.4) 25.77 (7.1–57.7) 7.33 2.9–17.64 0.160Dose to 5% volume (Gy) 26.73 (2.3–59.1) 32.52 (12.0–68.1) 5.79 6.5–18.12 0.350Dose to 10% volume (Gy) 24.17 (2.1–53.1) 28.14 (8.9–65.4) 3.96 8.0–15.9 0.500
Left optic nerveMean dose (Gy) 17.66 (1.7–59.3) 24.74 (8.4–55.8) 7.07 4.51–18.67 0.222Dose to 5% volume (Gy) 23.63 (2.2–53.2) 32.87 (16.0–64.5) 9.24 2.7–21.21 0.125Dose to 10% volume (Gy) 21.20 (2.1–57.8) 26.76 (10.3–61.1) 5.55 6.9–18.05 0.371
Right parotidMean dose (Gy) 37.17 (19.6–55.0) 57.31 (31.1–62.2) 20.14 9.3–23.4 0.000Dose to 50% volume (Gy) 34.78 (16.0–55.7) 52.76 (25.0–63.6) 17.97 11.1–26.8 0.000Dose to 80% volume (Gy) 26.20 (10.6–44.8) 47.13 (25.0–57.0) 20.90 13.23–28.62 0.000
Left parotidMean dose (Gy) 39.44 (19.4–50.0) 56.82 (23.0–63.9) 17.38 7.1–20.9 0.000Dose to 50% volume (Gy) 38.12 (15.3–49.6) 54.25 (23.0–63.9) 16.13 7.9–22.3 0.000Dose to 80% volume (Gy) 27.70 (10.4–42.0) 47.00 (20.0–58.5) 19.30 12.2–26.39 0.000
Right inner earMean dose (Gy) 40.83 (19.0–67.3) 53.90 (43.5–66.1) 13.07 6.40–19.75 0.000Dose to 50% volume (Gy) 39.09 (18.7–65.4) 54.11 (43.3–67.4) 15.02 8.56–21.67 0.000Dose to 80% volume (Gy) 29.19 (15.4–43.5) 48.84 (39.7–57.2) 19.65 13.59–25.70 0.000
Left inner earMean dose (Gy) 39.50 (15.3–61.2) 54.43 (42.4–68.2) 14.93 8.17–21.64 0.000Dose to 50% volume (Gy) 38.47 (16.1–61.9) 55.21 (44.3–68.4) 16.73 10.13–23.33 0.000Dose to 80% volume (Gy) 31.00 (14.9–44.8) 49.40 (37.4–60.2) 18.40 12.65–24.16 0.000
PituitaryMean dose (Gy) 31.00 (2.2–57.4) 38.10 (18.6–66.9) 7.10 5.69–19.89 0.265Dose to 50% volume (Gy) 31.20 (2.0–58.7) 39.47 (19.0–66.4) 8.26 4.27–20.81 0.188Dose to 80% volume (Gy) 26.38 (2.0–48.4) 30.41 (12.0–53.6) 4.02 6.52–14.58 0.431
Abbreviations: CI = confidence interval; PTV = planning target volume; other abbreviations as in Table 1.
institute, we found a significant survival advantage with radi-
ation doses >66 Gy (DFS rate, 68% vs. 40%, p = 0.020; OS
rate, 73% vs. 46%, p = 0.012) (5). However, acute and late
normal tissue toxicity remains an area of concern when esca-
lating radiation doses in the pediatric population.
Intensity-modulated RT allows for the delivery of high
doses to the target while sparing the surrounding critical
structures and offers a significant advantage compared with
CRT in improving the therapeutic ratio. Furthermore, the de-
crease in acute normal tissue toxicity with IMRT improves

IMRT for nasopharyngeal carcinoma in children d S. LASKAR et al. 735
patient compliance to RT, with resultant improvement in lo-
cal disease control. In the series reported by Lee et al. (13),
the 4-year estimate of locoregional progression-free and
overall survival was 98%, and 88% respectively, and Zhao
et al. (19), reported a LRC rate of 96.7% for their patients
treated using IMRT.
We compared the results of 19 children treated using
IMRT with the results of 17 children treated using CRT dur-
ing the same period. The tumor-related prognostic factors
that influenced the outcome included the initial tumor vol-
ume, T stage, and N stage. Patients with a good response
to neoadjuvant chemotherapy (complete response or partial
response) had a superior DFS (p = 0.050) and OS (p =
0.029) compared with those who did not (stable disease or
progressive disease). No statistically significant difference
was found in the LRC, DFS, or OS rates for children treated
with IMRT vs. CRT. However, we did document a signifi-
cant reduction in the incidence of acute Grade 3 toxicity
and a considerable prolongation in the median time to the
onset of Grade 2 toxicity with IMRT. Of the children treated
with CRT, 10 (59%) developed Grade 3 or greater acute tox-
icity compared with only 3 (16%) of those treated with
IMRT. Furthermore, although most of the children treated
with CRT developed Grade 2 acute toxicity by approxi-
mately the fourth week of RT, the onset of these reactions
was delayed almost to the last week of RT for patients re-
ceiving IMRT. As a result, frequent treatment interruptions
were required for the patients treated with CRT, leading to
prolongation in the total RT duration. Concurring with the
published data, we found the total RT duration to be a signif-
icant predictor of outcome. Children who completed RT
within the median time of 52 days had a LRC rate of
100% compared with a rate of 49.2% for those requiring
>52 days (p = 0.001).
To our knowledge, the present study is the first large series
reporting on the feasibility and outcome on the use of IMRT
for children with nasopharyngeal cancer. IMRT allows for
delivery of a greater total dose and dose per fraction to the tar-
get volume, while maintaining low doses to the adjacent crit-
ical structures (Table 6).
The acute toxicity of CRT is augmented by the addition of
chemotherapy and at times can become quite severe. The pro-
longation of RT because of toxicities leads to a reduction in
the biologic efficacy of RT, compromising the probability of
local disease control. Lee et al. (20) reported that in adult pa-
tients with NPC treated using RT alone, the risk of local fail-
ure increased by 5.9% for each day the treatment was
prolonged. In the present study, we found the use of IMRT
to be safe and effective in the pediatric age group. The use
of IMRT resulted in a significant reduction in the incidence
of Grade 3 acute toxicity, delayed the onset of Grade 2 toxic-
ity, resulting in a reduction in the total time required to de-
liver RT compared with CRT. We also found that the
response to neoadjuvant chemotherapy and the total RT du-
ration are important prognostic factors for survival in chil-
dren with PNPC.
This study, because it was prospective nonradomized
study comparing IMRT and CRT, had the inherent defi-
ciencies of not being a prospective randomized comparison.
Thus, imbalances were present between the two treatment
groups in terms of adverse prognostic factors such as tumor
volume and disease stage. In view of the relatively short
follow-up of 27 months, we primarily focused on the re-
sponse rates, acute toxicities, and early results of disease
control in this review. IMRT seems to be an effective mo-
dality for the treatment of PNPC with a significant reduc-
tion in normal tissue toxicity without compromising
disease control.
REFERENCES
1. Deutsch M, Mercado R, Parsons JA. Cancer of the nasopharynxin children. Cancer 1978;41:1128–1133.
2. Ingersoll L, Woo SY, Donaldson S, et al. Nasopharyngealcarcinoma in young: A combined M.D. Anderson and Stan-ford experience. Int J Radiat Oncol Biol Phys 1990;19:881–887.
3. Pao WJ, Hustu HO, Douglass EC, et al. Paediatric nasopharyn-geal carcinoma: Long-term follow-up of 29 patients. Int JRadiat Oncol Biol Phys 1989;7:299–305.
4. Ayan I, Kaytan E, Ayan N. Childhood nasopharyngeal car-cinoma: From biology to treatment. Lancet Oncol 2003;4:13–21.
5. Laskar S, Sanghavi V, Muckaden MA, et al. Nasopharyngealcarcinoma in children: Ten years experience at the Tata Memo-rial Hospital, Mumbai. Int J Radiat Oncol Biol Phys 2004;58:189–195.
6. Ozyar E, Selek U, Laskar S, et al. Treatment results of 165 pe-diatric patients with non-metastatic nasopharyngeal carcinoma:A Rare Cancer Network study. Radiother Oncol 2006;81:39–46.
7. Uzel O, Yoruk SO, Sahinler I, et al. Nasopharyngeal carcinomain childhood: Long term results of 32 patients. Radiother Oncol2001;58:137–141.
8. Selek U, Ozyar E, Ozyigit G, et al. Treatment results of 59young patients with nasopharyngeal carcinoma. Int J PediatrOtorhinolaryngol 2005;69:201–207.
9. Ayan I, Altun M. Nasopharyngeal carcinoma in children: Retro-spective review of 50 patients. Int J Radiat Oncol Biol Phys1996;35:485–492.
10. Jenkins DT, Anderson JR, Jereb B, et al. Nasopharyngeal car-cinoma—A retrospective review of patients less than thirtyyears of age: A report from Children’s Cancer Study Group.Cancer 1981;47:360–366.
11. Serin M, Erkal H, Elhan AH, et al. Nasopharyngeal carcinomain childhood and adolescence. Med Pediatr Oncol 1998;31:498–505.
12. Ahern V, Jenkin D, Banerjee D, et al. Nasopharyngeal carci-noma in the young. Clin Oncol 1994;6:24–30.
13. Lee N, Xia P, Quivey JM, et al. Intensity-modulated radiother-apy in the treatment of nasopharyngeal carcinoma: An updateof the UCSF experience. Int J Radiat Oncol Biol Phys 2002;53:12–22.
14. Kam M, Teo P, Chau R, et al. Treatment of nasopharyngealcarcinoma with intensity modulated radiotherapy: The HongKong experience. Int J Radiat Oncol Biol Phys 2004;60:1440–1450.

736 I. J. Radiation Oncology d Biology d Physics Volume 72, Number 3, 2008
15. Wolden SL, Chen WC, Pfister DG, et al. Intensity-modulatedradiation therapy for nasopharynx cancer: Update of the Memo-rial Sloan-Kettering experience. Int J Radiat Oncol Biol Phys2006;64:57–62.
16. Lu TX, Mai WY, The BS, et al. Initial experience using inten-sity-modulated radiotherapy for recurrent nasopharyngeal carci-noma. Int J Radiat Oncol Biol Phys 2004;58:682–687.
17. Greene FL, Page DL, Fleming ID, et al. AJCC cancer stagingmanual. 6th ed. New York: Springer; 2002.
18. World Health Organization. WHO handbook for reporting re-sults of cancer treatment. Geneva: World Health OrganizationOffset Publication No. 48; 1979.
19. Zhao C, Han F, Lx Lu, et al. Intensity modulated radiotherapyfor local-regional advanced nasopharyngeal carcinoma. AiZheng 2004;23:1532–1537.
20. Lee AW, Chan DK, Fowler JF, et al. Effect of time, dose andfractionation on local control in nasopharyngeal carcinoma.Radiother Oncol 1995;36:24–31.