Narcolepsy With Cataplexy
13
Seminar www.thelancet.com Vol 369 February 1 0, 2007 499 Narcolepsy with cataplexy Yves Dauvilliers, Isabelle Arnulf, Emmanuel Mignot Narcolepsy with cataplexy is a disabling sleep disorder affecting 0·02% of adults worldwide. It is characterised by severe, irresistible daytime sleepiness and sudden loss of muscle tone (cataplexy), and can be associated with sleep- onset or sleep-offset paralysis and hallucinations, frequent movement and awakening during sleep, and weight gain. Sleep monitoring during night and day shows rapid sleep onset and abnormal, shortened rapid-eye-movement sleep latencies. The onset of narcolepsy with cataplexy is usually during teenage and young adulthood and persists throughout the lifetime. Pathophysiological studies have shown that the disease is caused by the early loss of neurons in the hypothalamus that produce hypocretin, a wakefulness-associated neurotransmitter present in cerebrospinal fluid. The cause of neural loss could be autoimmune since most patients have the HLA DQB1*0602 allele that predisposes individuals to the disorder. Treatment is with stimulant drugs to suppress daytime sleepiness, antidepressants for cataplexy, and γ hydroxybutyrate for both symptoms. Because narcolepsy is an under-reco gnised disease, it is important that general practitioners and other primary health-care workers identify abnormal daytime sleepiness early. Narcolepsy is a disabling sleep disorder characterised by excessive daytime sleepiness and abnormal rapid-eye- movement (REM) sleep manifestations including cataplexy (sudden loss of muscle tone triggered by strong emotions), sleep paralysis, and hypnagogic (sleep-onset) hallucinations and REM periods. 1–4 A century after it was first described, 5,6 narcolepsy is one of the most studied sleep disorders at the molecular level 7–10 since it is useful for investigating REM sleep regulation and the most severe example of sleepiness in human beings, as well as the study of stimulant drugs. Major studies in animal models show that deficient hypocretin transmission causes narcolepsy. 11,12 A striking decrease in hypocretin-1 concentrations in the cerebrospinal fluid (CSF) 11,13 and in the number of hypocretin neurons in post-mortem brain tissue have been reported in narcolepsy patients. 14–17 Additionally, the treatment of narcolepsy has evolved over the past few years with the widespread use of modafinil for daytime sleepiness, newer antidepressants for cataplexy, and γ hydroxybutyrate (sodium oxybate) for both symptoms. Epidemiology From investigations in California in the early 1970s, 18 the prevalence of narcolepsy with cataplexy was estimated at between 0·05% and 0·067% in the USA. In a study of a cohort of 8000 twins from Finland, 0·026% reported daily sleep attacks and at least one episode of muscular weakness per week. 7 Similar results were reported with different methods in more recent studies in Europe, 8 Hong Kong, 9 and MN, USA. 10 The US study also reported an incidence of 0·74 pe r 100 000 inhabit ants per y ear. The prevalence of narcolepsy is higher in Japan 19 and lower in Israel 20 than in Europe and North America. Most studies have found a slight male predominance. The age of onset varies from early c hildhood to the 50s, with a bimodal distribution, including a large peak around 15 years of age and a smaller peak around 36 years (figure 1). 21 More than half of narcoleptic patients report important events in the days or weeks preceding the onset of symptoms. These include a major psychological stress, an abrupt change of sleep schedules, head trauma, and pregnancy. 22 The gap between the emergence of initial symptoms and diagnosis is usually more than 10 years, but this has shortened in some countries with increased awareness about narcolepsy among health-care professionals and the general public. 23 Clinical features Excessive daytime sleepiness In most cases, daytime sleepiness is the first symptom to appear. It is also the most severe symptom and the most frequent cause for consultation. 3,4,21 Daytime sleepiness occurs daily, recurring typically every 2 h, although this can vary widely. Sleepiness is exacerbated when the patient is physically inactive. The sleep episodes have several characteristics: (1) they are often irresistible, despite the individual making desperate efforts to fight the urge to sleep; (2) they are usually short, although their length can vary with environmental factors (eg, the duration can increase with passive activities such as watching television); (3) they are frequently associated with dreaming; and (4) they typically restore normal wakefulness for up to several hours. 24–26 The refreshing value of short naps is of considerable diagnostic value, except in children who are frequently tired on awakening. Severe sleepiness can also lead to unconscious microsleep episodes or lapses. Lancet 2007; 369: 499–511 Neurologie, CHU Montpellier Hôpital Gui-de- Chauliac and INSERM U888, Montpellier-France (Y Dauvilliers MD); Fédération des Pathologies du Sommeil, Hôpital Pitié-Salpêtrière, Assistance Publique-Hôpit aux de Paris, France (I Arnulf MD); National Reference Network for Orphan Diseases (Narcolepsy and Idiopathic Hypersomni a), France (Y Dauvilliers, I Arnulf); and Howard Hughes Medical Institute and Center for Narcolepsy, Stanford University, Palo Alto, CA, USA (Prof E Mignot MD) Correspondence to: Dr Yves Dauvilliers, Service de Neurologie, Hôpital Gui-de- Chauliac, 80 avenue Augustin Fliche, 34295 Montpellier cedex 5, France [email protected] Search strategy and selection criteria We used the term “narcolepsy” for PubMed searches, including articles in all languages. Articles published between 2001 and 2006 (although key articles were included irrespective of publication date), systematic review articles, meta-analyses, and evidence-based guidelines were preferentially selected. As well as this material, this Seminar is based on consultation with experts in the area of narcolepsy, and on feedback from reviewers.
-
Upload
einsteintheotter -
Category
Documents
-
view
12 -
download
0
description
Narcolepsy With Cataplexy- Y. Dauvilliers et al.
Transcript of Narcolepsy With Cataplexy
-
Seminar
www.thelancet.com Vol 369 February 10, 2007 499
Narcolepsy with cataplexyYves Dauvilliers, Isabelle Arnulf, Emmanuel Mignot
Narcolepsy with cataplexy is a disabling sleep disorder a ecting 002% of adults worldwide. It is characterised by severe, irresistible daytime sleepiness and sudden loss of muscle tone (cataplexy), and can be associated with sleep-onset or sleep-o set paralysis and hallucinations, frequent movement and awakening during sleep, and weight gain. Sleep monitoring during night and day shows rapid sleep onset and abnormal, shortened rapid-eye-movement sleep latencies. The onset of narcolepsy with cataplexy is usually during teenage and young adulthood and persists throughout the lifetime. Pathophysiological studies have shown that the disease is caused by the early loss of neurons in the hypothalamus that produce hypocretin, a wakefulness-associated neurotransmitter present in cerebrospinal uid. The cause of neural loss could be autoimmune since most patients have the HLA DQB1*0602 allele that predisposes individuals to the disorder. Treatment is with stimulant drugs to suppress daytime sleepiness, antidepressants for cataplexy, and hydroxybutyrate for both symptoms. Because narcolepsy is an under-recognised disease, it is important that general practitioners and other primary health-care workers identify abnormal daytime sleepiness early.
Narcolepsy is a disabling sleep disorder characterised by excessive daytime sleepiness and abnormal rapid-eye-movement (REM) sleep manifestations including cataplexy (sudden loss of muscle tone triggered by strong emotions), sleep paralysis, and hypnagogic (sleep-onset) hallucinations and REM periods.14 A century after it was rst described,5,6 narcolepsy is one of the most studied sleep disorders at the molecular level710 since it is useful for investigating REM sleep regulation and the most severe example of sleepiness in human beings, as well as the study of stimulant drugs. Major studies in animal models show that de cient hypocretin transmission causes narcolepsy.11,12 A striking decrease in hypocretin-1 concentrations in the cerebrospinal uid (CSF)11,13 and in the number of hypocretin neurons in post-mortem brain tissue have been reported in narcolepsy patients.1417 Additionally, the treatment of narcolepsy has evolved over the past few years with the widespread use of moda nil for daytime sleepiness, newer antidepressants for cataplexy, and hydroxybutyrate (sodium oxybate) for both symptoms.
EpidemiologyFrom investigations in California in the early 1970s,18 the prevalence of narcolepsy with cataplexy was estimated at between 005% and 0067% in the USA. In a study of a cohort of 8000 twins from Finland, 0026% reported daily sleep attacks and at least one episode of muscular weakness per week.7 Similar results were reported with di erent methods in more recent studies in Europe,8 Hong Kong,9 and MN, USA.10 The US study also reported an incidence of 074 per 100 000 inhabitants per year. The prevalence of narcolepsy is higher in Japan19 and lower in Israel20 than in Europe and North America. Most studies have found a slight male predominance.
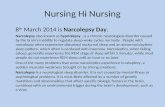
The age of onset varies from early childhood to the 50s, with a bimodal distribution, including a large peak around 15 years of age and a smaller peak around 36 years ( gure 1).21 More than half of narcoleptic patients report important events in the days or weeks preceding the
onset of symptoms. These include a major psychological stress, an abrupt change of sleep schedules, head trauma, and pregnancy.22 The gap between the emergence of initial symptoms and diagnosis is usually more than 10 years, but this has shortened in some countries with increased awareness about narcolepsy among health-care professionals and the general public.23
Clinical featuresExcessive daytime sleepiness In most cases, daytime sleepiness is the rst symptom to appear. It is also the most severe symptom and the most frequent cause for consultation.3,4,21 Daytime sleepiness occurs daily, recurring typically every 2 h, although this can vary widely. Sleepiness is exacerbated when the patient is physically inactive. The sleep episodes have several characteristics: (1) they are often irresistible, despite the individual making desperate e orts to ght the urge to sleep; (2) they are usually short, although their length can vary with environmental factors (eg, the duration can increase with passive activities such as watching television); (3) they are frequently associated with dreaming; and (4) they typically restore normal wakefulness for up to several hours.2426 The refreshing value of short naps is of considerable diagnostic value, except in children who are frequently tired on awakening. Severe sleepiness can also lead to unconscious microsleep episodes or lapses.
Lancet 2007; 369: 499511
Neurologie, CHU Montpellier Hpital Gui-de-Chauliac and INSERM U888, Montpellier-France (Y Dauvilliers MD); Fdration des Pathologies du Sommeil, Hpital Piti-Salptrire, Assistance Publique-Hpitaux de Paris, France (I Arnulf MD); National Reference Network for Orphan Diseases (Narcolepsy and Idiopathic Hypersomnia), France (Y Dauvilliers, I Arnulf); and Howard Hughes Medical Institute and Center for Narcolepsy, Stanford University, Palo Alto, CA, USA (Prof E Mignot MD)
Correspondence to: Dr Yves Dauvilliers, Service de Neurologie, Hpital Gui-de-Chauliac, 80 avenue Augustin Fliche, 34295 Montpellier cedex 5, [email protected]
Search strategy and selection criteria
We used the term narcolepsy for PubMed searches, including articles in all languages. Articles published between 2001 and 2006 (although key articles were included irrespective of publication date), systematic review articles, meta-analyses, and evidence-based guidelines were preferentially selected. As well as this material, this Seminar is based on consultation with experts in the area of narcolepsy, and on feedback from reviewers.
-
Seminar
500 www.thelancet.com Vol 369 February 10, 2007
CataplexyCataplexy is speci c to narcolepsy and is the best diagnostic marker of the disease. It is characterised by a sudden drop of muscle tone triggered by emotional factors, most often by positive emotions such as laughter, repartee, pleasant surprise (eg, seeing friends in the street or scoring a goal), or by anger, but almost never by stress, fear, or physical e ort.3,4,21,27,28 All striated muscles (but not the diaphragm) can be a ected, causing the individual to collapse. Cataplectic attacks are sometimes limited to facial muscles or to the arms or legs, with dysarthria, facial ickering, jaw tremor, head or jaw dropping, dropping of objects, or unlocking of the knees. Clinicians should ask speci cally about these incomplete forms of cataplexy since the patient might not necessarily see them as pathological, given that they remain fully conscious during the episode. Deep tendon re exes are transiently abolished during cataplexy, and the H-re ex is absent.29,30 The duration of cataplexy varies from a split second to several minutes. Its frequency varies from less than one episode per year to several episodes per day. Cataplexy worsens with poor sleep and fatigue. Patients can occasionally have status cataplecticus, which comprises continual cataplectic episodes lasting several hours. This state can occur spontaneously but is more often seen on withdrawal from anticataplectic antidepressant drugs.31 Many neurophysiological and pharmaceutical studies indicate that cataplexy shares common neurophysiological mechanisms with REM sleep atonia.
Associated featuresOther symptoms of dissociated REM sleep in patients with narcolepsy include sleep-related hallucinations and sleep paralysis. These symptoms are present in about 50% of those with the disease,3,21 but can also be seen in people who do not have narcolepsy,32 and thus cannot be used in diagnosis. Hypnagogic or hypnopompic (on awakening) hallucinations can be auditory (eg, the sound of a ringing phone, hearing someone walking on the
stairs), visual (eg, a threatening gure, passing shadows when driving, animals), or somesthetic (eg, an out of body experience, that the person feels like someone is brushing against them). Such hallucinations are sometimes frightening enough that the individual becomes scared of going to bed and resorts to reassuring behaviours such as having their pet sleep in the same room. Even if patients are well aware retrospectively of the nature of these phenomena, some patients report di culty in di erentiating dreams from reality and might occasionally be misdiagnosed as schizophrenic.
Sleep paralysis is an inability to move the limbs or the head or to speak or breathe normally either at sleep onset or on awakening (mainly from REM sleep) despite being mentally awake. It can be associated with hypnagogic hallucinations.33 Sleep paralysis does not usually last long, ie, just a few seconds, but in rare instances can last several minutes. Some patients ask the person sleeping next to them to touch or pinch them, or move their head or limbs, when they are non-responsive to the alarm clock or to a verbal call, thereby putting an end to the symptom.
In the daytime, patients might show automatic behaviourie, automatic continuation of an activity without memory of the event. In these cases, the patient might suddenly say something inappropriate or out of context in a conversation, write something inappropriate or illegible, or might drive to an inappropriate location with no memory of the event. Whether automatic behaviour is caused by microsleep or cognitive impairment when drowsy is unknown.
Narcoleptic patients generally do not spend much time asleep, even at night. Because they are unable to stay awake or asleep for long periods of time, nocturnal sleep is disrupted in a third of patients. Typically, patients fall asleep as soon as they get into bed but they wake up several times during the night. Narcoleptic patients also have higher body-mass indices than those without the disease.34 Some, especially children, gain weight after the onset of narcolepsy.35 Periodic leg movements are also frequent in narcoleptic patients, especially as they get older, but the contribution of these movements to daytime sleepiness remains controversial.36 Sleep-talking and REM sleep behaviour disorders (in which patients physically enact their dreams) have been recorded in a third of patients.37 Depression has also been reported in 1837% of cases.38,39
The general course of narcolepsy is di cult to describe. The order in which symptoms appear varies. In most patients, however, daytime sleepiness is the rst symptom, either on its own or accompanied by cataplexy within a year.21,34 Sleepiness and cataplexy persist throughout life although they often improve after retirement, probably owing to better management of activities, daytime napping, and adjustment of night-time sleep.40 By contrast, nocturnal sleep disturbances usually worsen with age.
Narcolepsy interferes with several aspects of lifethe extent to which it does so depends on its severity.41 The
15 36 550 0 15 36 55 70
Num
ber o
f nar
cole
ptic
patie
nts
France Canada
Age (years)
FemalesMales
Age (years)
Figure 1: Density curves of age at onset distribution for male and female in narcoleptic populations from Montpellier, France, and Montreal, CanadaReprinted, with permission, from reference 21.
-
Seminar
www.thelancet.com Vol 369 February 10, 2007 501
negative social impact of narcolepsy has been extensively studied, highlighting how the disease can impair driving ability, cause car or machine accidents, reduce professional performance leading to people becoming unemployed, changing jobs frequently, or retiring early.4245
Diagnostic criteriaThe diagnosis of narcolepsy with cataplexy is based on excessive daytime sleepiness (occurring almost daily for at least 3 months) and on a history of cataplexy (panel 1).1 Since individuals rarely go into cataplexy in the presence of the clinician, the doctor should refer the patient to a specialist sleep centre to con rm the clinical diagnosis with night-time polysomnography followed by a daytime multiple sleep latency test (MSLT). The aim of the polysomnography is to eliminate other causes of daytime sleepiness (mainly sleep apnoea) and to assess whether the patient has had enough sleep (at least 6 h) before the MSLT. Additionally, polysomnography might show a shortened REM sleep latency (less than 15 minutes) in 40% of cases, a fragmentation in REM sleep with imperfect loss of muscle tone, increased proportions of stage 1 sleep, and a relative augmentation in slow-wave sleep at the end of the night.
The MSLT consists of ve nap times, scheduled at 2-hourly intervals, starting at least 15 h after awakening.46 Each test is stopped after 15 minutes sleep or after 20 minutes if the patient does not fall asleep. A sleep-onset REM period (SOREMP) is de ned as the occurrence of REM sleep within 15 minutes of sleep onset. Since typical patients with narcolepsy frequently have two to ve SOREMPs during MSLT, two or more SOREMPs are needed for the diagnosis. However, in some patients with cataplexy, or in young children and elderly people with narcolepsy, this process does not happen.13,40 MSLT should, in addition, document a mean sleep-onset latency shorter than 8 minutes, although MSLT latency increases with age. Polysomnography and MSLT must be done in patients taking no psychotropic drugs, since these can substantially alter sleep-onset latency and the occurrence of REM sleep. The presence of the human leucocyte antigen (HLA) DQB1*0602 genotype in patients, which is neither sensitive nor speci c in narcolepsy, can only support, not determine, diagnosis. Alternatively, a CSF hypocretin-1 concentration lower than 110 ng/L or a third of mean normal control values could be used as a highly speci c (and de nite) but moderately sensitive criterion.1
Di erential diagnosis Narcolepsy with cataplexy can be confused with other forms of hypersomnolence, such as narcolepsy without cataplexy, sleep apnoea syndrome, idiopathic hyper-somnia, recurrent hypersomnia, hypersomnia associated with depression, and chronic sleep deprivation.2,3,47,48
Sleep apnoea syndrome (de ned by more than ve apnoea or hypopnoea events per hour of sleep) occurs in 24% of men and 9% of women in the general population,
and is associated with daytime sleepiness in 4% of men and 2% of women.49 Sleep apnoea syndrome is a major cause of daytime sleepiness (usually in middle-aged rather than young people), and can confound the MSLT, but never causes cataplexy. It is easily diagnosed with night-time polysomnography. Additionally, asymptomatic sleep apnoea can be present with, but not linked to, narcolepsy. In cases where it is not clear if the two are linked, especially when cataplexy is questionable, treating apnoea rst and re-evaluating symptoms and MSLT afterwards help making the diagnosis of narcolepsy.
Narcolepsy without cataplexy is a new subcategory of narcolepsy, in which patients show all narcoleptic symptoms but cataplexy, and meet identical poly som no-graphy and MSLT criteria to those with cataplexy. Hypocretin de ciency and HLA positivity are less frequent in these patients.13,50,51 Idiopathic hypersomnia, with or without long durations of night-time sleep, can cause daytime sleepiness in young adults and can be di eren-tiated from narcolepsy by the absence of cataplexy, the absence of two or more SOREMPs despite short latencies in MSLT,1 or sleeping for longer than 1112 h during 24-h sleep monitoring. Additionally, patients a ected with idiopathic hypersomnia who sleep for long durations frequently report long-lasting (typically 12 h) and non-refreshing naps that contrast with the short and refreshing naps of narcoleptic patients.52 Patients with recurrent hypersomnia or Kleine-Levin syndrome (rare disorder a ecting mainly teenagers) alternate between weeks or months with severe hypersomnia and behavioural and cognitive problems, followed by weeks or months of normal sleep, behaviour, and cognition.53 Hypersomnia associated with depression is characterised by a low mood, staying in bed for long periods of time, apathy, with no
Panel 1: Criteria for narcolepsy with cataplexy
1 Excessive daytime sleepiness occurring almost daily for at least 3 months.
2 De nite history of cataplexy, de ned as sudden and transient (less than 2 minutes) episodes of loss of muscle tone, generally bilateral, triggered by emotions (usually laughing and joking).
3 Diagnosis should, whenever possible, be con rmed by nocturnal polysomnography (with a minimum of 6 h sleep) followed by a daytime MSLT: Mean daytime sleep latency 8 minutes or shorter, with
two or more sleep onset in REM periods (the time from sleep onset to REM sleep should be less than 15 minutes in at least two naps).
Alternatively, hypocretin-1 concentrations in the cerebrospinal uid 110 ng/L or lower, or a third of mean control values.
4 The hypersomnia is not better explained by another sleep disorder, medical or neurological disorder, mental disorder, medication use, or substance use disorder.
-
Seminar
502 www.thelancet.com Vol 369 February 10, 2007
long periods of sleep during 24-h sleep monitoring.54 In a third of severe depressive episodes, REM sleep latency can be shortened, but SOREMPs are rare.55 Teenagers and young adults can also be sleepy during the daytime as a result of chronic sleep deprivation (when they sleep for shorter periods than usual) or progressive delay in the time they go to bed).1
Narcolepsy is often misdiagnosed as a psychiatric disorder or an epileptic variant. When cataplexy is pre-dominant, narcolepsy can be misdiagnosed as epilepsy (while patients are unconscious), syncope, a drop attack, or a histrionic attack. Pseudonarcolepsy and pseudo-cataplexy are conversion disorders. Some are cases of malingeringwhen individuals seek to receive inappro-priate disability bene t, leave from work, or a prescription of stimulants. Very rarely, cases of isolated cataplexy (mostly familial) without sleepiness or any SOREMP have been reported.
Narcolepsy can also occur as part of other medical disorders, and in these cases is referred to as symptomatic
or secondary narcolepsy.1 These cases can occur with or without cataplexy. Rare cases of secondary cataplexy have been reported in patients with brain lesions (mostly located in the posterior hypothalamus, the mesencephalon, and the pons) caused by tumours, multiple sclerosis, encephalitis, cerebral ischaemia, head trauma, and neurodegeneration.56 Young children with Niemann-Pick disease type C, or patients with muscular dystrophy or Parkinsons disease, can also have symptomatic narcolepsy without cataplexy.57,58
Molecular genetics and pathophysiology Canine model of narcolepsyA natural canine narcolepsy model was identi ed in 1973. Narcoleptic dogs have cataplexy (mainly elicited by the presentation of food), sleepiness, and have SOREMPs. The disease is transmitted as a recessive autosomal trait with complete penetrance in Doberman Pinschers and Labrador Retrievers,59 whereas it is polygenic and determined by environmental factors (sporadic narco-lepsy) in Poodles, Beagles, and other breeds. We discovered in 1999 a mutation in the gene coding for the hypocretin type 2 receptor as the cause of familial canine narcolepsy.11 By contrast, we have not identi ed mutations in hypocretin genes in sporadic canine narcolepsy. Rather, these cases were associated with substantially decreased concentrations of hypocretin-1 in the CSF and in the brain. This nding suggests that sporadic and familial canine narcolepsies have distinct causes, but that both result from decreased hypocretin transmission.60
Hypocretin (orexin)The hypocretin peptides were rst discovered and named in 1998.61 The name hypocretin was derived to re ect the primary localisation of hypocretin-producing cells in the hypothalamus and a sequence similarity with the hormone secretin. Hypocretins 1 and 2 are produced exclusively by a group of several thousand neurons localised in the lateral hypothalamus. These neurons project widely to the olfactory bulb, cerebral cortex, thalamus, hypothalamus, and brainstem, and particularly densely to the locus coeruleus, tuberomamillary nucleus, raphe nucleus, and bulbar reticular formation ( gure 2).62,63 In parallel, endogenous ligands to two orphan receptors with homologous structures had been identi ed and called orexins A and B because of their stimulating e ects on appetite.64 The orexin peptides turned out to be the same as hypocretins. With the discovery of hypocretin involvement in narcolepsy, the presumed role of hypocretin has been refocused on sleep regulation and its interaction with the regulation of energy expenditure. Several animal models with abnormal hypocretin transmission have also been genetically engineered. They all share a similar phenotype including fragmented sleep-wake patterns, behavioural arrests or cataplexy, and premature entrance into REM sleep, similar to that seen in human narcolepsy. These models include pre-prohypocretin gene12 or
Figure 2: Distribution of hypocretin-labelled somas in narcoleptic patients (A) and controls (B), and schematic drawing of hypocretin neuron pathways in the rat brain (C)F=fornix. Inset shows a hypocretin-producing neuron (black dots). Each dot represents a hypocretin-producing cell. Preprohypocretin transcripts are seen in the hypothalamus only in controls. Reprinted, with permission, from reference 63.
-
Seminar
www.thelancet.com Vol 369 February 10, 2007 503
hypocretin receptor-2 gene knockout mice,65 double receptor-1 and receptor-2 knockout mice,65 and hypocretin/ataxin-3 transgene-induced loss of hypocretin neurons in rats and mice.66,67
Studies in human beingsAfter the discovery of the hypocretin 2 receptor gene mutation in narcoleptic dogs, the hypocretin system was also studied in human narcolepsy. The systematic screening of mutations in the hypocretin system was undertaken in patients with cataplexy and SOREMPs, both with and without a family history of narcolepsy, with or without HLA DQB1*0602. So far, we have identi ed only one patient with a mutation in hypocretin-related genes. This patient was atypical, with unusually early onset of narcolepsy and cataplexy at 6 months of age and HLA-DQB1*0602 negativity.14 Additionally, the gene loci for pre-prohypocretin and hypocretin receptors 1 and 2 did not contribute to narcolepsy susceptibility.14,68
Although most cases of human narcolepsy are not caused by hypocretin gene mutations, the genes are involved in the pathophysiology of the disorder. In-situ hybridisation, immunohistochemistry, and radio-immunological assays of peptides in post-mortem brain tissue of narcoleptic patients have identi ed undetectable levels of pre-prohypocretin RNA, hypocretin peptides, and a selective loss of hypocretin neurons.4,14,15 By contrast, melanin-concentrating hormone neurons normally located within the same region were intact. Similar pathological ndings were found in few cases of sporadic canine narcolepsy.61 Hypocretin neurons (and not only hypocretin mRNA) were selectively damaged, since the staining of two markers coexpressed in hypocretin neurons (prodynorphin and neuronal activity-regulated pentraxin) was substantially reduced in the posterior hypothalamus and normal in other brain areas where these polypeptides are not co-localised with hypocretin.16,17 Together with ndings from studies indicating undetectable CSF hypocretin 1 in most cases of human narcolepsy-cataplexy,13,47,50,69 these results suggest that hypocretin de ciency causes most cases of narcolepsy with cataplexy. However, the cause of hypocretin cell death remains unknown. Patients with typical narcolepsy-cataplexy and HLA-DQB1*0602 positivity had no serum or CSF autoantibodies against pre-prohypocretin.7072 The absence of direct evidence of humoral immunity in patients does not, however, exclude the possibility that a transient autoimmune reaction restricted to the CNS could have occurred around disease onset, to disappear shortly thereafter.
Patients with narcolepsy and cataplexy have low concentrations of hypocretin in the CSF, typically below 100 ng/L and most often undetectable with conventional radioimmunoassays.69,73 Several groups of researchers have measured CSF hypocretin 1 concentrations in large groups of healthy individuals and patients with other sleep or neurological disorders ( gure 3). They found
that CSF hypocretin 1 concentrations were almost always above 200 ng/L in controls or individuals with other sleep and neurological disorders. CSF hypocretin 1 con-centrations lower than 110 ng/L had a high (94%) positive predictive value for narcolepsy with cataplexy.13,50,74,75 In rare instances, low CSF hypocretin concentrations outside of narcolepsy were indicative of Guillain-Barr syndrome or previous head trauma.
Measuring CSF hypocretin 1 in clinical practiceSamples are obtained through lumbar puncture during daytime. They must contain a minimum of 500 L CSF and be stored at 80C or in dry ice. CSF hypocretin 1 concentrations can be measured with the commercially available kit for iodine 125 radioimmunoassay (Phoenix Pharmaceuticals, Belmont, CA, USA). Normal values can be established locally with CSF obtained in healthy individuals or in patients with neurological diseases known not to a ect the hypocretin system (eg, mild cognitive impairment, polyneuropathy), after duplicating the measures with a reference centre. Low CSF hypocretin concentrations are highly speci c (99%) and sensitive (8789%) for patients with clear-cut cataplexy and speci c (99%) but not sensitive (16%) for cases with mild, atypical, or absent cataplexy, and for patients with familial or HLA-negative narcolepsy.13,50,74,75 Since diagnosis is generally straightforward in patients with cataplexy, CSF hypocretin 1 is only measured if the usual diagnostic procedures are not su cient. These situations include: (1) equivocal MSLT results; (2) young children (younger than 8 years) who are unable to follow MSLT instructions; (3) individuals already
Day700 Night Typicalcataplexy
Atypicalcataplexy
No cataplexy
600
500
400
300
200
100
0
CSF
hypo
cret
in 1
(ng/
L)
Controls Patients with narcolepsy Patients withidiopathic
hyperinsomnia
Figure 3: CSF hypocretin 1 concentrations in people with narcolepsy with and without cataplexy, in those with idiopathic hypersomnia, and in controlsEach point represents the crude concentration of CSF hypocretin 1 in an individual. Cuto s for normal (>200 ng/L) and low (
-
Seminar
504 www.thelancet.com Vol 369 February 10, 2007
taking psychotropic medications (eg, anticataplectics or stimulants) who are unwilling to stop; (4) individuals who cannot a ord formal sleep testing (eg, those without medical insurance); and (5) individuals with severe or complex psychiatric, neurological, or medical disorders that could compromise the validity of the MSLT results. In these individuals, CSF hypocretin 1 concentrations lower than 110 ng/L or 30% of local normal values are highly indicative of narcolepsy.
HLA genes Narcolepsy-cataplexy is strongly associated with a speci c HLA allele. The main predisposing allele is the DQB1*0602, identi ed in 8595% of patients with narco-lepsy-cataplexy. The presence or absence of the allele is not linked to ethnic origin (table).7679 Furthermore, being homozygous for the HLA DQB1*0602 genotype doubles or quadruples the risk of narcolepsy. In heterozygotes, the relative risk of narcolepsy increases with DQB1*0301 and decreases with DQB1*0501 and DQB1*0601.80,81 This
nding is of interest since only minor variations in the peptide-binding pockets of DQB1*0602 and DQB1*0601 have been recorded ( gure 4).82 In the USA, 12% of Asians, 25% of white people, and 38% of African-Americans in the general population carries HLA-DQB1*0602, but only a small fraction of these have narcolepsy. Additionally, HLA is positive in only 4060% of patients with narcolepsy without cataplexy and in 75% of familial cases of narcolepsy,81,82 indicating that this allele is neither necessary nor su cient to trigger narcolepsy. Accordingly, other non-HLA genes might also confer susceptibility to narcolepsy.78,83,84
Other genetic predisposing factorsMost diseases with a strong HLA association are autoimmune in nature. Several studies have identi ed an association between narcolepsy and immune-related genes, including polymorphisms in the region of the tumour necrosis factor gene and receptor 2 gene,85-88 whereas there was no association between narcolepsy and apolipoprotein E4.89 Although studies of functional polymorphisms a ecting the gene encoding monoamine oxidase A yielded con icting results,90,91 we detected a sexual dimorphism in the functional polymorphism of the gene encoding catechol-O-methyltransferase. This polymorphism also modulated the severity of daytime sleepiness90 and the response of patients to stimulant treatment with moda nil.92 Additionally, a 2004 study has shown positive associations with speci c genomic regions including those encoding the dopamine receptor D2, the -aminobutyric acid receptor -1, and the serotonin receptor 2A.93,94
Familial patternsA genetic predisposition for narcolepsy was suggested in the rst published report of narcolepsy in 1877, where both mother and son were a ected.5 Families with multiple full-blown narcolepsy-cataplexy cases are rare, however, and rarely have more than two a ected individuals.95 12 % of rst-degree relatives are a ected with narcolepsy-cataplexy, which is 1040 times higher than the prevalence in the general population.95 By contrast, families with members who report sleepiness without cataplexy are more common (1030%).96 A genome-wide mapping study has reported
White African-American Japanese
Narcolepsy (n=238) Control (n=146) OR Narcolepsy (n=77) Control (n=243) OR Narcolepsy (n=105) Control (n=698) OR
0102-0602/0102-0602 43 (181%) 3 (21%) 105 18 (234%) 9 (37%) 79 16 (152) 5 (07) 249
0102-0602/X-0301 49 (206%) 4 (27%) 92 12 (156%) 8 (33%) 54 20 (19%) 6 (09%) 271
0102-0602/0101-0501 12 (5%) 2 (14%) 38 5 (65%) 3 (12%) 56 2 (19%) 5 (07%) 27
0102-0602/0103-0601 0 0 0 0 0 0 8 (76%) 15 (21%) 38
0102-0602/other DQB1 109 (458%) 25 (171) 41 37 (481) 56 (23%) 31 59 (56%) 54 (77%) 153
Non 0602/non 0602 25 (105%) 112 (767%) 0 5 (65) 167 (687%) 0 0 613 (978%) 0
Data from reference 81. OR=odds ratio.
Table: Susceptibility e ects of various DQA1-DQB1 allele combinations on narcolepsy, by ethnic origin
66
9
37
3813
26
57
30
Figure 4: DQB1*0602 binding pocketHighlighted residues represent those that di er between DQB1*0602 and DQB1*0601. Reprinted, with permission, from reference 82.
-
Seminar
www.thelancet.com Vol 369 February 10, 2007 505
potential linkage (logarithm-of-odds [LOD] score of 309) to chromosome 4p13-q21 in eight small multiplexes, (multiple members are a ected) Japanese families a ected with narcolepsy-cataplexy.97 In a genome-wide linkage analysis of a large French family with four members a ected by narcolepsy-cataplexy and ten others with isolated recurrent naps, we found evidence for linkage to chromosome 21q (LOD score of 400).98
Environmental factorsSystematic twin studies have not been undertaken for narcolepsy. Only six of 19 published monozygotic pair reports are concordant for narcolepsy-cataplexy,95,99,100 suggesting the in uence of environmental factors. However, most cases are poorly documented at the clinical level. In 2004, we identi ed monozygotic twins who were homozygous for HLA DQB1*0602 but discordant for narcolepsy and CSF hypocretin 1 concentrations.99 An individuals genetic background is therefore not su cient to explain hypocretin de ciency fully. These ndings support a multifactorial model for the development of narcolepsy, with a strong in uence from environmental factors, acting in combination with genetic factors (at least HLA DQB1*0602), possibly triggering an autoimmune process with irreversible damage to the hypocretin system. The nature of the possible environmental trigger is unknown, although onset is frequently associated with various non-speci c ndings such as stressful events.22 Interestingly, recent studies have revealed a March peak and a September trough (in the Northern hemisphere) in the birth pattern of patients with narcolepsy and clear-cut and frequent cataplexy. Therefore, environmental events during early development could in uence narcolepsy severity or the likelihood of developing the disease.101,102
Disease managementMajor advances in the treatment of daytime sleepiness and cataplexy have been made in the past few years. Because narcolepsy has no cure, its management relies on symptomatic therapies. These include stimulants (mostly dopaminergic) for daytime sleepiness and sleep attacks, antidepressants (mostly noradrenergic) for cataplexy and other REM-associated symptoms, and hypnotics for disturbed night-time sleep.24,28,103,104 In 2006, a single drug named sodium oxybate was e ective in controlling daytime sleepiness, cataplexy, and disturbed night-time sleep.105
Treatment of excessive daytime sleepinessModa nil Moda nil is a wakefulness-promoting agent. Although its mechanism of action is unclear, the drug is recommended as a rst-line therapy for narcolepsy for several reasons. First, it is long-acting; second, studies have shown a low potential for abuse, which could be especially important in cases without cataplexy; third, unlike other stimulants, the medication has been
carefully studied in a double-blind placebo-controlled design and shown to be e cacious. A possible dis-advantage of moda nil is its lower e cacy when compared to other amphetamine-like stimulants.
Several studies have outlined its possible action on dopamine, adrenalin, noradrenalin, serotonin, and -aminobutyric acid (GABA) systems.106111 The elimination half-life is 138 h and the maximum concentration is achieved in 24 h. The L-isomer has a shorter half-life than the R-isomer. Randomised studies of 200400 mg per day have shown a signi cant reduction of sleepiness.112114 The
response to moda nil is dependant on the catechol-O-methyltransferase genotype.92 The drug is usually started at a dose of 100200 mg in the morning for 12 weeks, with the possible addition of 100200 mg at lunch, especially when sleepiness recurs in late afternoon. The most common adverse events are mild, including headache (13%), nervousness (8%), and nausea (5%), with no evidence of tolerance. Moda nil can raise concentrations of hepatic cytochrome P450 enzymes and increase the metabolism of oral contraceptives. Thus, a contraceptive containing at least 50 g ethinyloestradiol is recommended for individuals taking moda nil.
Methylphenidate and amphetamines Methylphenidate is a widely used, potent stimulant. It primarily blocks the reuptake of monoamines (mainly dopamine) and, unlike amphetamines, does not inhibit the vesicular monoamine transporter. Clinical experience shows that methylphenidate improves daytime sleepiness in narcolepsy patients at daily doses of 10100 mg.115 The duration of action is 4 h and elimination half-life is 6 h. The short-acting e ect of methylphenidate is useful in cases where moda nil needs to be supplemented at a speci c time of the day, or in situations where maximum alert ness is required (eg, driving). Adverse e ects are similar to those of amphetamines but much less frequent. Long-acting formulations are now available that could be useful in avoiding the roller-coaster changes in alert ness.
Amphetamines have been used for narcolepsy since 1935.116 They promote monoamine (catecholamine but also serotonin) release through multiple mechanisms. All monoamines are a ected, but compared with L-isomers, D-isomers have a larger e ect on dopaminergic trans-mission (versus other monoamines) and are more e ective stimulants. A methylated form (meth-amphetamine) has increased CNS penetration and more potent wakefulness-promoting e ects. At low doses, amphetamines produce a reverse e ux of dopamine (and other monamines) through monoaminergic reuptake sites. At higher doses, they also inhibit vesicular monoamine transporters and monoamine oxidase. Cytotoxicity for dopaminergic neurons can occur at high doses in animals. Ampheta mines are very e ective against sleepiness in narcolepsy but also induce frequent adverse e ects, including irritability, aggressiveness, insomnia, hypertension, and abnormal movements (at
-
Seminar
506 www.thelancet.com Vol 369 February 10, 2007
doses below 60 mg/day). Serious toxic e ects, including anxiety, aggressiveness, and psychotic reactions, can occur at doses above 60 mg/day.117 The potential for drug abuse or tolerance is important, but surprisingly rare, in narcolepsy patients with cataplexy, possibly because of the absence of hypocretin, which has a role in the bodys reward system that can lead to addiction.
Other stimulantsSodium oxybate, taken at night, has been shown to have signi cant stimulant e ects. Other more rarely used stimulants include mazindol, pemoline, and selegiline. Mazindol is an imidazolidine derivative with the ability to block both dopamine and adrenaline reuptake. Elimination half-life is 10 h. Small non-controlled studies have shown signi cant improvements of sleepiness in narcoleptic patients at the optimum daily dose of 23 mg/day.118 Adverse e ects include loss of appetite, dry mouth, nervousness, constipation, and less frequently, nausea, vomiting, headache, dizziness, and tachycardia. Since valvulopathies have developed in obese (non-narcoleptic) individuals who take mazindol in association with fen uramine as an anorexigen,119 a careful cardiological follow-up is recommended. Mazindol has less potential for abuse and tolerance than amphetamines. Pemoline, a weak dopamine reuptake inhibitor of long duration of action, is rarely used today because it occasionally induces hepatotoxicity.120 Selegiline is a complex drug that in-hibits monoamine oxidase B, and is metabolised into amphetamine.121
Treatment for cataplexy and other REM-associated phenomenaSodium oxybate is the only approved treatment for cataplexy in the USA and Europe. Tricyclic antidepressants and more recently selective serotonin and noradrenalin reuptake inhibitors are also widely used and e ective to treat cataplexy. These drugs have been used for decades,122 but their e ect on cataplexy has never been investigated in randomised clinical trials. Drugs that treat cataplexy also reduce hypnagogic hallucinations and sleep paralysis. The anticataplectic e ects of these drugs di er from their antidepressant e ects in the rapid response to them (less than a week); however, rebound cataplexy or status cataplecticus typically occurs if intake is abruptly inter rupted.31
Tricyclic medications include clomipramine (usually 1025 mg, occasionally 75 mg in rare cases of persistent cataplexy), desipramine, imipramine, and protryp-tylin.2,3,28,103 Adverse e ects are frequent: in particular, anticholinergic e ects, but also orthostatic hypotension, anorexia, diarrhoea, weight gain, tiredness, and decreased libido. Serotonin-speci c reuptake inhibitors are e ective, but higher doses than those for tricyclic drugs are often needed ( uoxetine 2060 mg/day, uvoxamine 25200 mg/day, citalopram 2040 mg/day).24,28,103,123 Sexual dysfunction can also be a problem with serotonin-speci c
reuptake inhibitors. Norepinephrine reuptake inhibitors (viloxazine 100 mg/day, reboxetine 210 mg/day, atomoxetine 40100 mg/day) are also e ective against cataplexy with only minor adverse e ects such as headache, dry mouth, hyperhydrosis, constipation, nausea, and dizziness. These compounds are often e ective at lower doses than used for treatment of depression. The dual norepinephrine and serotonin reuptake inhibitor venlafaxine (75300 mg/day) is also e ective against cataplexy, with nausea as the main adverse e ect.2,124126 It is increasingly used as a rst-line therapy against cataplexy, and long-acting formulations are ideal since they are e ective for the whole day. Finally, both mazindol and selegiline have combined anticataplectic and stimulant properties.2 In one study, 13 mg/day of mazindol decreased cataplexy in 85% of patients.127 There is no established behavioural treatment of cataplexy, although patients can learn to avoid situations that trigger cataplexy attacks.
Treatment of disturbed nocturnal sleep Several studies of sodium oxybate have shown a reduction in the number of night-time awakenings with increased slow-wave sleep, making this drug a rst-line treatment for narcoleptic patients with disturbed night-time sleep.128 Clinical experience indicates, however, that regular sleep-wake schedules, benzodiazepines (clonazepam), and related hypnotics (zolpidem, zopiclone and zaleplon) can also alleviate sleep disturbances.2 This bene t should be balanced with the possibility of increasing daytime sleepiness.
Treatment a ecting multiple symptomsSodium oxybate (-hydroxybutyrate [GHB]) is a natural metabolite of -aminobutyrate that acts as a neuro trans-mitter via its own receptors and via the stimulation of GABA-B receptors.129 Previous studies have reported e cacy in managing REM-related symptoms including cataplexy, hypnagogic hallucinations, and sleep paralysis, but also e ectiveness against sleepiness.130 Sodium oxybate has re-emerged in the past few years as a major treatment of narcolepsy. Indeed, it is the only drug that can alleviate all the core symptoms of narcolepsy, including cataplexy, daytime sleepiness, insomnia, and, in some cases, hypnagogic hallucinations.
The drug decreased the number of cataplectic attacks in patients with increasing doses between 3 and 9 g nightly.128 The bene t was signi cant after 4 weeks, at its highest after 8 weeks, and was maintained during long-term (744 months) therapy.131 Patients showed no evidence of tolerance, and unlike for antidepressant-based therapies for cataplexy, interruption of sodium oxybate treatment did not result in a return of cataplexy.
Additionally, sodium oxybate, taken at bedtime and 2540 h later at an optimum dose of 69 g per night, reduced sleepiness and increased alertness in a dose-
-
Seminar
www.thelancet.com Vol 369 February 10, 2007 507
dependent manner in two large placebo-controlled randomised trials.105,128 Despite its elimination half-life of 4060 minutes, its bene t persists much longer. Adverse e ects are dizziness, headache, nausea, and more rarely, pain, depressive mood, enuresis, and sleepwalking. Sodium oxybate can also be used in association with antidepressant or stimulant therapy. Co-administration of sodium oxybate with moda nil was more e ective against daytime sleepiness than each drug alone.105 The addition of sodium oxybate typically allows for the use of lower doses for these ancillary medications.
Patients can be instructed to start at 45 g (225 g before sleeping, 225 g 2 h 30 minutes to 4 h later in the night) for 2 weeks, increasing to 6 g in two equally divided doses over 4 weeks. After a check-up to assess the bene t to risk ratio, the dose can be increased to up to 9 g. Patients should prepare the doses in two small containers before going to bed, to void urine (to avoid enuresis later), and to take the rst dose while in the bed. The second dose can either be taken after a spontaneous awakening (usually) or by using an alarm clock. Sodium oxybate should not be used in conjunction with alcohol. Patients should skip one or two doses if they have drunk any amounts of alcohol.
A major problem with the drug is its non-medical use; it is sometimes used as a mind-altering drug because it produces an uninhibited, slightly euphoric state with transient amnesia. It is also used as a rape drug or for theft. Overdose, often occurring with self-made impure sodium oxybate derivatives and in association with alcohol and other illegal drugs, can be fatal. Additionally, continuous use of high doses can lead to dependence and severe withdrawal symptoms on cessation. For these reasons, the prescription of sodium oxybate is highly controlled in Europe and the USA. It is, however, important to note that when properly used for narcolepsy, there is no evidence for dependence since abrupt cessation of therapy only leads to a slow return of symptoms.
Treatment for other symptomsNarcolepsy patients often report vivid dreams and REM sleep behaviour disorder. On the basis of available information, it is di cult to provide guidelines for the treatment of such symptoms other than recommending conventional medications (clonazepam). Sleep apnoea is more frequent in narcolepsy patients than in the general population, probably because of increased obesity in people with the illness, and should be treated with conventional therapy. It can be di cult to apply continuous positive airway pressure when patients also have disturbed nocturnal sleep. Sodium oxybate can be helpful in these cases, provided ventilation is complied with (the drug is a respiratory depressant). Periodic limb movements in sleep are also more prevalent in narcolepsy than in the general population. However, there is no documented bene t of treating these movements in narcolepsy patients. Depressive patients with narcolepsy can be treated by
antidepressant drugs and psychotherapy.38 Finally, behavioural recommendations, such as regular sleep and wake times and scheduled naps during the day are often helpful, particularly against sleepiness.
Future directionsCurrent research in the area aims to develop new treatments (panel 2),126 and to better understand the physiological role of hypocretin. The cause of hypocretin cell loss is the major unresolved issue in the area. Although an autoimmune cause is likely, a focal in ammatory process targeting hypocretin neurons is so far unproven. Other mechanisms, for example a viral infection or spontaneous neurodegenerative process are also possible. 10% of narcoleptic patients with cataplexy and most patients without cataplexy, without HLA DQB1*0602, or with a family history of the illness have normal CSF hypocretin results, which suggests that factors other than hypocretin de ciency (perhaps downstream of hypocretin neurons) are involved in these cases.
Panel 2: Potential future narcolepsy therapies
Non-hypocretin-based therapyNovel monoamine reuptake inhibitorsAnatomically-targeted dopamine (stimulant) and norepinephrine (anticataplexy) reuptake inhibitors to reduce side-e ects and abuse potential.Novel slow-wave sleep enhancersNovel GABA-B agonists, such as a longer-acting analogues of sodium oxybate; GABA-A subtype speci c compounds (eg, gaboxadol) or GABA reuptake inhibitors (eg, tiagabine)Histaminergic H3 receptor antagonists/inverse agonists Blockade of histamine autoreceptor increases histamine release and reduces sleepiness and cataplexy in animal models. Multiple compounds are being investigated in early clinical trials.
Hypocretin-based therapyHypocretin 1Intravenous, intracisternal, and intranasal administration have not been e ective so far, but extremely high doses might be. Delivering hypocretin 1 intracerebroventricularly is likely to be most e ective.Non-peptide agonistsHigh potential on a medium-term basis; peptide receptor agonists are however often di cult, if not impossible, to make.Hypocretin cell transplantationMight eventually provide a cure; disappointing results in other diseases (graft rejection, low survival rate of implant, and lack of supply for graft availability). These problems might be alleviated with improved stem-cell technology; probably more than 10 years away.Gene therapyPromising but has potentially dangerous side-e ects; could be combined with cell-based therapies.Immune-based therapy.SteroidsIne ective thus far; unlikely to be useful due to late clinical presentation of cell loss.Intravenous immunoglobulinsEquivocal results thus far; generally safe but occasional life-threatening side-e ects.PlasmapheresisEquivocal results thus far; even fewer available data and more invasive than immunoglobulins.
-
Seminar
508 www.thelancet.com Vol 369 February 10, 2007
With improving diagnostic techniques, measurement of plasma (instead of CSF) hypocretin 1 concentrations might be possible and useful for more accurate diagnosis. The prevalence of narcolepsy without cataplexy should also be established. Indeed, evidence that healthy individuals in the Wisconsin sleep cohort have abnormal narcolepsy-like MSLT suggest that the spectrum of the disease might be larger than expected or that MSLT can result in false positives.132
Narcolepsy is genetically complex and environmentally in uenced. HLA is likely to be the major genetic susceptibility factor, but other genes might also have a role. The con rmation of preliminary genetic association studies, the identi cation of new susceptibility genes, of environmental triggering factors, and the study of gene-environment interactions will constitute the major next steps. In sporadic cases, most of susceptibility genes are anticipated to be involved in an autoimmune process targeting hypothalamic hypocretin neurons in conjunction or independent of HLA. The identi cation of mutant genes in narcoleptic families might also be a major step in the identi cation of a genetic variation that contributes to this phenotype. Finally, considering variation in treatment response between individuals, additional pharmacogenomic studies could help design more individualised therapies.
Despite major advances in our understanding of the neurobiological basis of narcolepsy, current treatments all respond to speci c symptoms and are not e ective enough against the disease as a whole. Symptomatic therapies for daytime sleepiness are currently being developed, including an R-isomer of moda nil having a longer duration of action, histamine H3 antagonists, and sodium oxybate formulations or analogues with longer duration of action. The stimulants initially used in narcolepsy are now being tested in several more common diseases with excessive daytime sleepiness (eg, sleepiness refractory to ventilation in sleep apnoea), fatigue, and attention-de cit hyperactivity disorder. Additionally, new antidepressants such as duloxetine, reboxetine, and atomoxetine could also be used for the treatment of cataplexy.
Replacing hypocretin would probably be the ideal therapy. Such manipulations are e ective when administered centrally in hypocretin-de cient mouse models.133 Attempts at using hypocretin-based treatments after peripheral adminis tration have been disappointing, since the peptides do not cross the blood brainbarrier.125,126 Hypocretin-based therapies such as direct use of hypocretin agonists and hypocretin neuron transplantation are currently under investigation in animal models.
Based on the autoimmune hypothesis of narcolepsy, treatments such as intravenous immunoglobulins and plasmapheresis have shown promising results in a few cases, which need to be con rmed in larger series.134136 A limitation of these treatments, however, will be the need to intervene at disease onset (ie, in childhood). Even if
clinical evidence shows that drugs approved in adult patients with narcolepsy are e ective in children, the treatment of narcolepsy in children is still an area in great need of guidelines because of the absence of any approved drug treatment or trial.
ConclusionMajor advances in the past decade have led to improved symptomatic therapies and a better understanding of the pathophysiology of narcolepsy with cataplexy. Although the HLA DQB1*0602 remains the only established genetic risk factor, future approaches could focus on identifying new genetic susceptibility factors and environmental factors that lead to hypocretin neuronal degeneration. This might in turn lead to an understanding of the cause of hypocretin cell death. A better understanding of the prevalence and potential cause of narcolepsy without cataplexy is also needed. Research in this area is likely not only to bene t narcoleptic patients, but may also lead to a better understanding of sleep-regulatory mechanisms, with application in other disease areas.Con ict of interest statementY Dauvilliers and I Arnulf have received honoraria from Cephalon Inc, Orphan Medical, and Bioprojet as investigators, and from UCB Pharma as consultants and for lectures. E Mignot has received honoraria from Cephalon Inc and Orphan Medical for lectures; his laboratory has also received an unrestricted gift from Cephalon Inc to study narcolepsy.
References1 American Academy of Sleep Medicine. The International
Classi cation of Sleep Disorders: diagnostic and coding manual. 2nd edn. Chicago, IL: AASM, 2005.
2 Dauvilliers Y, Billiard M, Montplaisir J. Clinical aspects and pathophysiology of narcolepsy. Clin Neurophysiol 2003; 114: 200017.
3 Overeem S, Mignot E, van Dijk JG, Lammers GJ. Narcolepsy: clinical features, new pathophysiologic insights, and future perspectives. J Clin Neurophysiol 2001; 18: 78105.
4 Scammell TE. The neurobiology, diagnosis, and treatment of narcolepsy. Ann Neurol 2003; 53: 15466.
5 Westphal C. Eigentmliche mit Einschlafen verbundene Anflle. Arch Psychiatr Nervenkr 1877; 7: 63135.
6 Glineau J. De la narcolepsie. Gazette des Hpitaux (Paris) 1880; 53: 62628.
7 Hublin C, Kaprio J, Partinen M, et al. The prevalence of narcolepsy: an epidemiological study of the Finnish Twin Cohort. Ann Neurol 1994; 35: 70916.
8 Ohayon MM, Priest RG, Zulley J, Smirne S, Paiva T. Prevalence of narcolepsy symptomatology and diagnosis in the European general population. Neurology 2002; 58: 182633.
9 Wing YK, Li RH, Lam CW, Ho CK, Fong SY, Leung T. The prevalence of narcolepsy among Chinese in Hong Kong. Ann Neurol 2002; 51: 57884.
10 Silber MH, Krahn LE, Olson EJ, Pankratz VS. The epidemiology of narcolepsy in Olmsted County, Minnesota: a population-based study. Sleep 2002; 25: 197202.
11 Lin L, Faraco J, Li R, et al. The sleep disorder canine narcolepsy is caused by a mutation in the hypocretin (orexin) receptor 2 gene. Cell 1999; 98: 36576.
12 Chemelli RM, Willie JT, Sinton CM, et al. Narcolepsy in orexin knockout mice: molecular genetics of sleep regulation. Cell 1999; 98: 43751.
13 Mignot E, Lammers GJ, Ripley B, et al. The role of cerebrospinal uid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol 2002; 59: 155362.
14 Peyron C, Faraco J, Rogers W, et al. A mutation in a case of early onset narcolepsy and a generalized absence of hypocretin peptides in human narcoleptic brains. Nat Med 2000; 6: 99197.
-
Seminar
www.thelancet.com Vol 369 February 10, 2007 509
15 Thannickal TC, Moore RY, Nienhuis R, et al. Reduced number of hypocretin neurons in human narcolepsy. Neuron 2000; 27: 46974.
16 Crocker A, Espana RA, Papadopoulou M, et al. Concomitant loss of dynorphin, NARP, and orexin in narcolepsy. Neurology 2005; 65: 118488.
17 Blouin AM, Thannickal TC, Worley PF, Baraban JM, Reti IM, Siegel JM. Narp immunostaining of human hypocretin (orexin) neurons: loss in narcolepsy. Neurology 2005; 65: 118992.
18 Dement W, Carskadon M, Ley R. The prevalence of narcolepsy II. Sleep Res 1973; 2: 147.
19 Honda Y. Census of narcolepsy, cataplexy and sleep life among teenagers in Fujisawa city. Sleep Res 1979; 8: 191.
20 Lavie P, Peled R. Narcolepsy is a rare disease in Israel. Sleep 1987; 10: 60809.
21 Dauvilliers Y, Montplaisir J, Molinari N, et al. Age at onset of narcolepsy in two large populations of patients in France and Quebec. Neurology 2001; 57: 202933.
22 Orellana C, Villemin E, Tafti M, Carlander B, Besset A, Billiard M. Life events in the year preceding the onset of narcolepsy. Sleep 1994; 17 (suppl 8): S5053.
23 Morrish E, King MA, Smith IE, Shneerson JM. Factors associated with a delay in the diagnosis of narcolepsy. Sleep Med 2004; 5: 3741.
24 Mullington J, Broughton R. Scheduled naps in the management of daytime sleepiness in narcolepsy-cataplexy. Sleep 1993; 16: 44456.
25 Hood B, Bruck D. A comparison of sleep deprivation and narcolepsy in terms of complex cognitive performance and subjective sleepiness. Sleep Med 2002; 3: 25966.
26 Roehrs T, Zorick F, Wittig R, Paxton C, Sicklesteel J, Roth T. Alerting e ects of naps in patients with narcolepsy. Sleep 1986; 9: 19499.
27 Anic-Labat S, Guilleminault C, Kraemer HC, Meehan J, Arrigoni J, Mignot E. Validation of a cataplexy questionnaire in 983 sleep-disorders patients. Sleep 1999; 22: 7787.
28 Thorpy MJ. Cataplexy associated with narcolepsy: epidemiology, pathophysiology and management. CNS Drugs 2006; 20: 4350.
29 Guilleminault C. Cataplexy. In: Guilleminault C, Dement W, Passouant P, eds. Narcolepsy. New York: Spectrum, 1976: 12543.
30 Overeem S, Reijntjes R, Huyser W, Lammers GJ, van Dijk JG. Corticospinal excitability during laughter: implications for cataplexy and the comparison with REM sleep atonia. J Sleep Res 2004; 13: 25764.
31 Poryazova R, Siccoli M, Werth E, Bassetti CL. Unusually prolonged rebound cataplexy after withdrawal of uoxetine. Neurology 2005; 65: 96768.
32 Ohayon MM. Prevalence of hallucinations and their pathological associations in the general population. Psychiatry Res 2000; 97: 15364.
33 Hishikawa Y, Shimizu T. Physiology of REM sleep, cataplexy, and sleep paralysis. Adv Neurol 1995; 67: 24571.
34 Okun ML, Lin L, Pelin Z, Hong S, Mignot E. Clinical aspects of narcolepsy-cataplexy across ethnic groups. Sleep 2002; 25: 2735.
35 Kotagal S, Krahn LE, Slocumb N. A putative link between childhood narcolepsy and obesity. Sleep Med 2004; 5: 14750.
36 Boivin DB, Lorrain D, Montplaisir J. E ects of bromocriptine on periodic limb movements in human narcolepsy. Neurology 1993; 43: 213436.
37 Nightingale S, Orgill JC, Ebrahim IO, de Lacy SF, Agrawal S, Williams AJ. The association between narcolepsy and REM behavior disorder (RBD). Sleep Med 2005; 6: 25358.
38 Roth B, Nevsimalova S. Depresssion in narcolepsy and hypersommia. Schweiz Arch Neurol Neurochir Psychiatr 1975; 116: 291300.
39 Vandeputte M, de Weerd A. Sleep disorders and depressive feelings: a global survey with the Beck depression scale. Sleep Med 2003; 4: 34345.
40 Dauvilliers Y, Gosselin A, Paquet J, Touchon J, Billiard M, Montplaisir J. E ect of age on MSLT results in patients with narcolepsy-cataplexy. Neurology 2004; 62: 4650.
41 Daniels E, King MA, Smith IE, Shneerson JM. Health-related quality of life in narcolepsy. J Sleep Res 2001; 10: 7581.
42 Broughton R, Ghanem Q, Hishikawa Y, Sugita Y, Nevsimalova S, Roth B. Life e ects of narcolepsy in 180 patients from North America, Asia and Europe compared to matched controls. Can J Neurol Sci 1981; 8: 299304.
43 Kales A, Soldatos CR, Bixler EO, et al. Narcolepsy-cataplexy. II. Psychosocial consequences and associated psychopathology. Arch Neurol 1982; 39: 16971.
44 Findley L, Unverzagt M, Guchu R, Fabrizio M, Buckner J, Suratt P. Vigilance and automobile accidents in patients with sleep apnoea or narcolepsy. Chest 1995; 108: 61924.
45 Beusterien KM, Rogers AE, Walsleben JA, et al. Health-related quality of life e ects of moda nil for treatment of narcolepsy. Sleep 1999; 22: 75765.
46 Carskadon MA, Mitler MM, Roth T. Guidelines for the Multiple Sleep Latency Test (MSLT): a standard measure of sleepiness. Sleep 1986; 9: 51924.
47 Bassetti C, Gugger M, Bischof M, et al. The narcoleptic borderland: a multimodal diagnostic approach including cerebrospinal uid levels of hypocretin-1 (orexin A). Sleep Med 2003; 4: 712.
48 Dauvilliers Y. Di erential diagnosis in hypersomnia. Curr Opin Neurol Neurosciences 2006; 6: 15662.
49 Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med 1993; 328: 123035.
50 Dauvilliers Y, Baumann CR, Carlander B, et al. CSF hypocretin-1 levels in narcolepsy, Kleine-Levin syndrome, and other hypersomnias and neurological conditions. J Neurol Neurosurg Psychiatry 2003; 74: 166773.
51 Bassetti CL. Narcolepsy: selective hypocretin (orexin) neuronal loss and multiple signaling de ciencies. Neurology 2005; 65: 115253.
52 Billiard M, Dauvilliers Y. Idiopathic Hypersomnia. Sleep Med Rev 2001; 5: 34958.
53 Arnulf I, Zeitzer JM, File J, Farber N, Mignot E. Kleine-Levin syndrome: a systematic review of 186 cases in the literature. Brain 2005; 128: 276376.
54 Vgontzas AN, Bixler EO, Kales A, Criley C, Vela-Bueno A. Di erences in nocturnal and daytime sleep between primary and psychiatric hypersomnia: diagnostic and treatment implications. Psychosom Med 2000; 62: 22026.
55 Kupfer DJ. REM latency: a biological marker for primary depressive disease. Biol Psychiatry 1976; 11: 15974.
56 Nishino S, Kanbayashi T. Symptomatic narcolepsy, cataplexy and hypersomnia, and their implications in the hypothalamic hypocretin/orexin system. Sleep Med Rev 2005; 9: 269310.
57 Gibbs JW 3rd, Ciafaloni E, Radtke RA. Excessive daytime somnolence and increased rapid eye movement pressure in myotonic dystrophy. Sleep 2002; 25: 66265.
58 Arnulf I, Konofal E, Merino-Andreu M, et al. Parkinsons disease and sleepiness: an integral part of PD. Neurology 2002; 58: 101924.
59 Mignot E, Wang C, Rattazzi C, et al. Genetic linkage of autosomal recessive canine narcolepsy with a mu immunoglobulin heavy-chain switch-like segment. Proc Natl Acad Sci USA 1991; 88: 347578.
60 Ripley B, Fujiki N, Okura M, Mignot E, Nishino S. Hypocretin levels in sporadic and familial cases of canine narcolepsy. Neurobiol Dis 2001; 8: 52534.
61 de Lecea L, Kildu TS, Peyron C, et al. The hypocretins: hypothalamus-speci c peptides with neuroexcitatory activity. Proc Natl Acad Sci USA 1998; 95: 32227.
62 De Lecea L, Sutcli e JG. The hypocretins and sleep. FEBS J 2005; 272: 567588.
63 Peyron C, Tighe DK, van den Pol AN, et al. Neurons containing hypocretin (orexin) project to multiple neuronal systems. J Neurosci 1998; 18: 999610015.
64 Sakurai T, Amemiya A, Ishii M, et al. Orexins and orexin receptors: a family of hypothalamic neuropeptides and G protein-coupled receptors that regulate feeding behavior. Cell 1998; 92: 57385.
65 Willie JT, Chemelli RM, Sinton CM, et al. Distinct narcolepsy syndromes in Orexin receptor-2 and Orexin null mice: molecular genetic dissection of Non-REM and REM sleep regulatory processes. Neuron 2003; 38: 71530.
66 Hara J, Beuckmann CT, Nambu T, et al. Genetic ablation of orexin neurons in mice results in narcolepsy, hypophagia, and obesity. Neuron 2001; 30: 34554.
67 Beuckmann CT, Sinton CM, Williams SC, et al. Expression of a poly-glutamine-ataxin-3 transgene in orexin neurons induces narcolepsy-cataplexy in the rat. J Neurosci 2004; 24: 446977.
-
Seminar
510 www.thelancet.com Vol 369 February 10, 2007
68 Hungs M, Lin L, Okun M, Mignot E. Polymorphisms in the vicinity of the hypocretin/orexin are not associated with human narcolepsy. Neurology 2001; 57: 189395.
69 Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E. Hypocretin (orexin) de ciency in human narcolepsy. Lancet 2000; 355: 3940.
70 Black JL 3rd, Silber MH, Krahn LE, et al. Analysis of hypocretin (orexin) antibodies in patients with narcolepsy. Sleep 2005; 28: 42731.
71 Black JL 3rd, Avula RK, Walker DL, et al. HLA DQB1*0602 positive narcoleptic subjects with cataplexy have CSF lgG reactive to rat hypothalamic protein extract. Sleep 2005; 28: 119192.
72 Overeem S, Verschuuren JJ, Fronczek R, et al. Immunohistochemical screening for autoantibodies against lateral hypothalamic neurons in human narcolepsy. J Neuroimmunol 2006; 174: 18791.
73 Nishino S, Ripley B, Overeem S, et al. Low cerebrospinal uid hypocretin (Orexin) and altered energy homeostasis in human narcolepsy. Ann Neurol 2001; 50: 38188.
74 Nishino S, Kanbayashi T, Fujiki N, et al. CSF hypocretin levels in Guillain-Barre syndrome and other in ammatory neuropathies. Neurology 2003; 61: 82325.
75 Baumann CR, Bassetti CL. Hypocretins (orexins) and sleep-wake disorders. Lancet Neurol 2005; 4: 67382.
76 Honda Y, Asaka A, Tanaka Y, Juji T. Discrimination of narcolepsy by using genetic markers and HLA. Sleep Res 1983; 12: 254.
77 Billiard M, Seignalet J. Extraordinary association between HLA-DR2 and narcolepsy. Lancet 1985; 1: 22627.
78 Chabas D, Taheri S, Renier C, Mignot E. The genetics of narcolepsy. Annu Rev Genomics Hum Genet 2003; 4: 45983.
79 Mignot E, Lin X, Kalil J, et al. DQB1-0602 (DQw1) is not present in most nonDR2 Caucasian narcoleptics. Sleep 1992; 15: 41522.
80 Pelin Z, Guilleminault C, Risch N, Grumet FC, Mignot E, for the US Moda nil in Narcolepsy Multicenter Study Group. HLA-DQB1*0602 homozygosity increases relative risk for narcolepsy but not disease severity in two ethnic groups. Tissue Antigens 1998; 51: 96100.
81 Mignot E, Lin L, Rogers W, et al. Complex HLA-DR and -DQ interactions confer risk of narcolepsy-cataplexy in three ethnic groups. Am J Hum Genet 2001; 68: 68699.
82 Siebold C, Hansen BE, Wyer JR, et al. Crystal structure of HLA-DQ0602 that protects against type 1 diabetes and confers strong susceptibility to narcolepsy. Proc Natl Acad Sci USA 2004; 101: 19992004.
83 Taheri S, Mignot E. The genetics of sleep disorders. Lancet Neurol 2002; 1: 24250.
84 Tafti M, Maret S, Dauvilliers Y. Genes for normal sleep and sleep disorders. Ann Med 2005; 37: 58089.
85 Hohjoh H, Nakayama T, Ohashi J, et al. Signi cant association of a single nucleotide polymorphism in the tumor necrosis factor-alpha (TNF-alpha) gene promoter with human narcolepsy. Tissue Antigens 1999; 54: 13845.
86 Wieczorek S, Gencik M, Rujescu D, et al. TNFA promoter polymorphisms and narcolepsy. Tissue Antigens 2003; 61: 43742.
87 Wieczorek S, Dahmen N, Jagiello P, Epplen JT, Gencik M. Polymorphisms of the tumor necrosis factor receptors: no association with narcolepsy in German patients. J Mol Med 2003; 81: 8790.
88 Hohjoh H, Terada N, Kawashima M, Honda Y, Tokunaga K. Signi cant association of the tumor necrosis factor receptor 2 (TNFR2) gene with human narcolepsy. Tissue Antigens 2000; 56: 44648.
89 Gencik M, Dahmen N, Wieczorek S, Kasten M, Gencikova A, Epplen JT. ApoE polymorphisms in narcolepsy. BMC Med Genet 2001; 2: 9.
90 Dauvilliers Y, Neidhart E, Lecendreux M, Billiard M, Tafti M. MAO-A and COMT polymorphisms and gene e ects in narcolepsy. Mol Psychiatry 2001; 6: 36772.
91 Koch H, Craig I, Dahlitz M, Denney R, Parkes D. Analysis of the monoamine oxidase genes and the Norrie disease gene locus in narcolepsy. Lancet 1999; 353: 64546.
92 Dauvilliers Y, Neidhart E, Billiard M, Tafti M. Sexual dimorphism of the catechol-O-methyltransferase gene in narcolepsy is associated with response to moda nil. Pharmacogenomics J 2002; 2: 6568.
93 Wieczorek S, Jagiello P, Arning L, Dahmen N, Epplen JT. Screening for candidate gene regions in narcolepsy using a microsatellite based approach and pooled DNA. J Mol Med 2004; 82: 696705.
94 Fehr C, Schleicher A, Szegedi A, et al. Serotonergic polymorphisms in patients su ering from alcoholism, anxiety disorders and narcolepsy. Prog Neuropsychopharmacol Biol Psychiatry 2001; 25: 96582.
95 Mignot E. Genetic and familial aspects of narcolepsy. Neurology 1998; 50 (suppl 1): S1622.
96 Billiard M, Pasquie-Magnetto V, Heckman M, et al. Family studies in narcolepsy. Sleep 1994; 17 (suppl 8): S5459.
97 Nakayama J, Miura M, Honda M, Miki T, Honda Y, Arinami T. Linkage of human narcolepsy with HLA association to chromosome 4p13-q21. Genomics 2000; 65: 8486.
98 Dauvilliers Y, Blouin JL, Neidhart E, et al. A narcolepsy susceptibility locus maps to a 5 Mb region of chromosome 21q. Ann Neurol 2004; 56: 38288.
99 Dauvilliers Y, Maret S, Bassetti C, et al. A monozygotic twin pair discordant for narcolepsy and CSF hypocretin-1. Neurology 2004; 62: 213738.
100 Khatami R, Maret S, Werth E, et al. Monozygotic twins concordant for narcolepsy-cataplexy without any detectable abnormality in the hypocretin (orexin) pathway. Lancet 2004; 363: 1199200.
101 Dauvilliers Y, Carlander B, Molinari N, et al. Month of birth as a risk factor for narcolepsy. Sleep 2003; 26: 66365.
102 Picchioni D, Mignot EJ, Harsh JR. The month-of-birth pattern in narcolepsy is moderated by cataplexy severity and may be independent of HLA-DQB1*0602. Sleep 2004; 27: 147175.
103 Billiard M. Moda nil: pharmacology and therapeutic perspectives. Rev Neurol (Paris) 2003; 159: 12225.
104 Houghton WC, Scammell TE, Thorpy M. Pharmacotherapy for cataplexy. Sleep Med Rev 2004; 8: 35566.
105 Black J, Houghton W, Xyrem International Study Group. Sodium oxybate improves excessive daytime sleepiness in narcolepsy. Sleep 2006; 29: 93946.
106 Lin JS, Hou Y, Jouvet M. Potential brain neuronal targets for amphetamine-, methylphenidate-, and moda nil-induced wakefulness, evidenced by c-fos immunocytochemistry in the cat. Proc Natl Acad Sci USA 1996; 93: 1412833.
107 Lin JS, Roussel B, Akaoka H, Fort P, Debilly G, Jouvet M. Role of catecholamines in the moda nil and amphetamine induced wakefulness, a comparative pharmacological study in the cat. Brain Res 1992; 591: 31926.
108 Mignot E, Nishino S, Guilleminault C, Dement WC. Moda nil binds to the dopamine uptake carrier site with low a nity. Sleep 1994; 17: 43637.
109 Gallopin T, Luppi PH, Rambert FA, Frydman A, Fort P. E ect of the wake-promoting agent moda nil on sleep-promoting neurons from the ventrolateral preoptic nucleus: an in vitro pharmacologic study. Sleep 2004; 27: 1925.
110 Saper CB, Scammell TE. Moda nil: a drug in search of a mechanism. Sleep 2004; 27: 1112.
111 Wisor JP, Eriksson KS. Dopaminergic-adrenergic interactions in the wake promoting mechanism of moda nil. Neuroscience 2005; 132: 102734.
112 Billiard M, Besset A, Montplaisir J, et al. Moda nil: a double-blind multicentric study. Sleep 1994; 17: 10712.
113 US Moda nil in Narcolepsy Multicenter Study Group. Randomized trial of moda nil for the treatment of pathological somnolence in narcolepsy. Ann Neurol 1998; 43: 8897.
114 US Moda nil in Narcolepsy Multicenter Study Group. Randomized trial of moda nil as a treatment for the excessive daytime somnolence of narcolepsy. Neurology 2000; 54: 116675.
115 Mitler MM, Shafor R, Hajdukovich R, Timms RM, Browman CP. Treatment of narcolepsy: objective studies on methylphenidate, pemoline, and protriptyline. Sleep 1986; 9: 26064.
116 Prinzmetal M, Bloomberg W. The use of benzedrine for the treatment of narcolepsy. JAMA 1935; 105: 205154.
117 Auger RR, Goodman SH, Silber MH, Krahn LE, Pankratz VS, Slocumb NL. Risks of high-dose stimulants in the treatment of disorders of excessive somnolence: a case-control study. Sleep 2005; 28: 66772.
118 Alvarez B, Dahlitz M, Grimshaw J, Parkes JD. Mazindol in long-term treatment of narcolepsy. Lancet 1991; 337: 129394.
-
Seminar
www.thelancet.com Vol 369 February 10, 2007 511
119 Ryan DH, Bray GA, Helmcke F, et al. Serial echocardiographic and clinical evaluation of valvular regurgitation before, during, and after treatment with fen uramine or dexfen uramine and mazindol or phentermine. Obes Res 1999; 7: 31322.
120 Honda Y, Hishikawa Y. A long-term treatment of narcolepsy and excessive daytime sleepiness with pemoline (Bentanamin). Curr Ther Res 1980; 27: 42941.
121 Mayer G, Meier-Ewert K. Selegiline hydrochloride treatment in narcolepsya double-blind placebo-controlled study. Clin Neuropharmacol 1995; 18: 30619.
122 Parkes D, Schachter M. Clomipramine and and clonazepam in narcolepsy. Lancet 1979; 2: 108586.
123 Langdon N, Shindler J, Parkes JD, Bandak S. Fluoxetine in the treatment of cataplexy. Sleep 1986; 9: 37173.
124 Smith M, Parkes J, Dahlitz M. Venlafaxine in the treatment of the narcoleptic syndrome. J Sleep Res 1996; 5: 217.
125 Abad VC, Guilleminault C. Emerging drugs for narcolepsy. Expert Opin Emerg Drugs 2004; 9: 28191.
126 Mignot E, Nishino S. Emerging therapies in narcolepsy-cataplexy. Sleep 2005; 28: 75463.
127 Iijima S, Sugita Y, Teshima Y, Hishikawa Y. Therapeutic e ects of mazindol on narcolepsy. Sleep 1986; 9: 26568.
128 US Xyrem Multicenter Study group. A randomized, double blind, placebo-controlled multicenter trial comparing the e ects of three doses of orally administered sodium oxybate with placebo for the treatment of narcolepsy. Sleep 2002; 25: 4249.
129 Maitre M. The gamma-hydroxybutyrate signalling system in brain: organisation and functional implications. Progr Neurobiol 1997; 51: 33761.
130 Lammers GJ, Arends J, Declerck AC, Ferrari MD, Schouwink G, Troost J. Gammahydroxybutyrate and narcolepsy: a double-blind placebo-controlled study. Sleep 1993; 16: 21620.
131 US Xyrem Multicenter Study group. Sodium oxybate demonstrates long-term e cacy for the treatment of cataplexy in patients with narcolepsy. Sleep Med 2004; 5: 11923.
132 Mignot E, Lin L, Finn L, et al. Correlates of sleep-onset REM periods during the Multiple Sleep Latency Test in community adults. Brain 2006; 129: 160923.
133 Mieda M, Willie JT, Hara J, Sinton CM, Sakurai T, Yanagisawa M. Orexin peptides prevent cataplexy and improve wakefulness in an orexin neuron-ablated model of narcolepsy in mice. Proc Natl Acad Sci USA 2004; 101: 464954.
134 Lecendreux M, Maret S, Bassetti C, Mouren MC, Tafti M. Clinical e cacy of high-dose intravenous immunoglobulins near the onset of narcolepsy in a 10year-old boy. J Sleep Res 2003; 12: 34748.
135 Dauvilliers Y, Carlander B, Rivier F, Touchon J, Tafti M. Successful management of cataplexy with intravenous immunoglobulins at narcolepsy onset. Ann Neurol 2004; 56: 90508.
136 Chen W, Black J, Call P, Mignot E. Late-onset narcolepsy presenting as rapidly progressing muscle weakness: response to plasmapheresis. Ann Neurol 2005; 58: 48990.
Narcolepsy with cataplexyEpidemiologyClinical featuresExcessive daytime sleepinessCataplexyAssociated features
Diagnostic criteriaDifferential diagnosisMolecular genetics and pathophysiologyCanine model of narcolepsyHypocretin (orexin)
Studies in human beingsMeasuring CSF hypocretin 1 in clinical practiceHLA genesOther genetic predisposing factorsFamilial patternsEnvironmental factors
Disease managementTreatment of excessive daytime sleepinessModafinilMethylphenidate and amphetaminesOther stimulants
Treatment for cataplexy and other REM-associated phenomenaTreatment of disturbed nocturnal sleepTreatment affecting multiple symptomsTreatment for other symptoms
Future directionsConclusionReferences