Napoleon: 1769 - 1821. Which Napoleon would you want as a ruler? Napoleon Crossing the Alps.

Page 1 of 32
GERMAN INTERGROUP RECOMMENDATIONS ON THE DIAGNOSTIC
AND THERAPEUTIC MANAGEMENT OF
ACUTE PROMYELOCYTIC LEUKEMIA (APL)
Version: Final V3.0
30.06.2015
Page 2 of 32
Steering committee:
Prof. Dr. U. Platzbecker
Dresden, for the SAL group Universitätsklinikum Carl Gustav Carus Technische Universität Dresden Medizinische Klinik und Poliklinik I Fetscherstr. 74 01307 Dresden, e‐mail: uwe.platzbecker@uniklinikum‐dresden.de
PD Dr. E. Lengfelder
Mannheim, for the AML‐CG group Universitätsklinikum Mannheim der Universität Heidelberg III. Medizinische Klinik Hämatologie und Internistische Onkologie Theodor‐Kutzer‐Ufer 1‐3 68167 Mannheim, e‐mail: [email protected]
Prof. Dr. R. F. Schlenk
Ulm, for the AML‐SG group Universitätsklinikum Ulm Klinik für Innere Medizin III Albert‐Einstein‐Allee 23 89081 Ulm, e‐mail: Richard.Schlenk@uniklinik‐ulm.de
Review committee:
Prof. Dr. M. Bornhäuser
PD Dr. Ch. Röllig
Prof. Dr. G. Ehninger
Universitätsklinikum Carl Gustav Carus Dresden
Medizinische Klinik und Poliklinik 1
Prof. Dr. H. Serve Klinikum der J.W. Goethe‐Universität, Medizinische Klinik II
Prof. Dr. H. Döhner
Prof. Dr. K. Döhner
Universitätsklinikum Ulm
Klinik für Innere Medizin III
Prof. Dr. M. Lübbert Universitätsklinikum Freiburg, Medizinische Klinik 1
Prof. Dr. U. Germing Heinrich‐Heine Universität Düsseldorf
Klinik für Hämatologie, Onkologie u. Klinische Immunologie
Prof. Dr. D. Niederwieser Universitätsklinikum Leipzig
Abteilung für Hämatologie und Internistische Onkologie
Prof. Dr. W. Hiddemann
Prof. Dr. K. Spiekermann
Klinikum der Universität München, Campus Großhadern Medizinische Klinik und Poliklinik III
Prof. Dr. A. Ganser Klinik für Hämatologie und Onkologie, Medizinische Hochschule Hannover
Prof. Dr. T. Büchner
Prof. Dr. W. Berdel
Universitätsklinikum Münster
Medizinische Klinik A
Prof. Dr. F. Lo‐Coco University of Tor Vergata Rome, Italy
Page 3 of 32
Glossary
AML acute myeloid leukemia
APL acute promyelocytic leukemia
aPTT activated partial prothrombin
time
Ara‐C cytarabine
ATO arsenic trioxide
ATRA all‐trans retinoic acid
BMP Bone marrow puncture
CD cluster of differentiation
CR complete remission
CRF Case report forms
CRm molecular complete remission
DIC disseminated intravascular
coagulation
FAB French‐American‐British
classification
FISH fluorescence in‐situ
hybridization
Gpt gigaparticles
hCR hematological complete
remission
ITD internal tandem duplication
MRD minimal residual disease
NUMA nuclear mitotic apparatus
OS overall survival
PML‐
RAR promyelocytic retinoid acid
receptor
POX peroxidase
QoL/
QLQ
quality of life/ quality of life
questionnaire
RDM molecular resistant disease
RT‐PCR reverse transcriptase
polymerase chain reaction
HSCT hematopoietic stem cell
transplantation
WBC white blood counts
WHO World Health Organization
Page 4 of 32
TABLE OF CONTENT
1 DIAGNOSTIC AND THERAPEUTIC MANAGEMENT OF PATIENTS WITH APL ................................ 5
1.1 Definition of APL ............................................................................................................... 5
1.2 Diagnostics of APL ............................................................................................................ 5
1.3 Therapeutic approaches in APL ......................................................................................... 6 1.3.1 ATRA-based induction therapy ...................................................................................................... 6 1.3.2 Consolidation therapy ................................................................................................................... 7 1.3.3 Maintenance therapy ..................................................................................................................... 7 1.3.4 Treatment of minimal residual disease (MRD) or relapse ............................................................. 7 1.3.5 ATO in APL ................................................................................................................................... 8
1.4 Intergroup guidelines for the treatment of APL ................................................................. 8 1.4.1 Treatment recommendation for high-risk APL (WBC >10 Gpt/l at initial diagnosis) according to
AIDA ............................................................................................................................................ 11 1.4.1.1 Induction therapy (high-risk APL)5 .......................................................................................................... 11 1.4.1.2 Consolidation therapy (high-risk APL) ..................................................................................................... 11 1.4.1.3 Maintenance therapy (high-risk APL) ...................................................................................................... 13 1.4.1.4 Dose modifications ................................................................................................................................... 14
1.4.2 Treatment recommendation for non-high-risk APL (WBC ≤10 Gpt/l at initial diagnosis) according to AIDA ....................................................................................................................... 14
1.4.2.1 Induction therapy ...................................................................................................................................... 14 1.4.2.2 Consolidation therapy ............................................................................................................................... 15 1.4.2.3 Maintenance therapy ................................................................................................................................. 16 1.4.2.4 Dose modifications ................................................................................................................................... 16
1.4.3 Treatment recommendation for non-high-risk APL (WBC ≤10 Gpt/l at initial diagnosis) according to the APL0406 study .................................................................................................. 17
1.4.3.1 Induction therapy ...................................................................................................................................... 17 1.4.3.2 Consolidation therapy ............................................................................................................................... 18 1.4.3.3 Dose modifications ................................................................................................................................... 19
1.4.4 Salvage therapy ........................................................................................................................... 19 2 SUPPORTIVE MANAGEMENT OF APL ..................................................................................... 20
2.1 Treatment of leukocytosis .............................................................................................. 20
2.2 Treatment of coagulopathy............................................................................................. 20
2.3 Differentiation syndrome (formerly “ATRA syndrome”) .................................................. 21
2.4 Pseudotumor cerebri with ATRA therapy ........................................................................ 21
2.5 Hepatotoxicity with ATO/ATRA ....................................................................................... 21
2.6 QT prolongation with ATO therapy ................................................................................. 22
3 EVALUATION OF RESPONSE ................................................................................................... 23
3.1 Hematological remission criteria ..................................................................................... 23
3.2 Molecular remission criteria ........................................................................................... 23
4 DIAGNOSTIC EXAMINATION PROGRAM ................................................................................ 24
5 LITERATURE .......................................................................................................................... 27
Page 5 of 32
1 DIAGNOSTIC AND THERAPEUTIC MANAGEMENT OF PATIENTS WITH APL
1.1 Definition of APL
Acute promyelocytic leukemia (APL) is considered a rare disease with estimated 200 to 300
newly‐diagnosed cases per year in Germany. According to the FAB classification APL is
designated as"M3 leukemia" and assigned to the WHO defined type of AML with recurrent
cytogenetic abnormalities, "acute promyelocytic leukemia with t(15;17)(q22;q12),
(PML/RARα) and variants". Detection of PML‐RARα fusion is carried out by conventional
cytogenetics including fluorescence in situ hybridization (FISH) and/or RT‐PCR. Alternative
fusion partners are the zinc finger (PLZF), the nucleophosmin gene (NPM), the nuclear
mitotic apparatus (NUMA) or the STAT5b gene. These fusion partners may be of therapeutic
relevance, e.g. for the sensitivity to all‐trans‐retinoic‐acid (ATRA), which does not exist with
the involvement of the PZLF gene [t(11;17)(q23;q21)].
APL is often clinically characterized by the presence of coagulative abnormalities1, including
disseminated intravascular coagulation (DIC), hyperfibrinolysis and unspecific proteolysis.
In up to 45 % of cases mutations of the FLT3 gene with an internal tandem duplication (ITD)
of the juxtamembranous domain and point mutations in the tyrosine kinase domain II can be
detected2, although their independent prognostic impact has not been demonstrated. Both
mutations are correlated with higher leukocyte counts while a FLT3‐ITD mutation is
associated with the M3v subtype and the S‐type PML/RARαprotein.
In addition to age, the most important prognostic factor is the leucocyte count at diagnosis
which divides patients into a high risk (> 10 Gpt / l) and a non‐high‐risk group ( 10 Gpt / l). Through use of a risk‐guided therapeutic approach the outcome of patients within both
groups including risk of relapse has become almost comparable3‐5.
1.2 Diagnostics of APL
The vast majority of APL cases mostly display a characteristic abnormal hypergranulation of
blasts6‐8. The nuclei of the cells vary in shape and size, being often bilobulated and kidney‐
shaped. Cytoplasm of the cells is completely filled with densed and partially condensed
granulation. In some cells the cytoplasm is filled with dust granulation. Cells with
characteristic bundles of Auer rods are found in the bone marrow or in the peripheral blood,
the so called Faggot‐cells. The M3v, however, contains fewer cells with hypergranulations or
bundles of Auer rods. Hypergranulated promyelocytes strongly react with POX, SSB und
chloracetate esterase. The expression of CD33, CD117 and absence of HLA‐DR and CD34 on
the surface of APL blasts is characteristic of the disease.
The t(15;17) translocation and the respective PML‐RARfusion transcript are diagnostically conclusive and represent definitive hallmarks of APL diagnosis7‐9. According to the current
WHO classification cases with specific cytogenetic and molecular genetic aberrations e.g.
t(15;17)(q22;q11‐12) resulting in the fusion transcript PML/RAR‐ are classified as AML
independently of the percentage of blasts in the bone marrow and peripheral blood9.
Page 6 of 32
The molecular analysis for the detection of the promyelocytic retinoic acid receptor (PML‐
RAR ) fusiongene is carried out by a reverse transcriptase‐polymerase chain reaction (RT‐
PCR). This method provides a fast and a highly sensitive verification of the initial diagnosis
and of minimal residual disease (MRD) in the course of APL therapy. The results of several
independent studies have shown that a positive detection of PCR transcripts for PML‐RAR hybrid gene during cytomorphological remission within consolidation cycles is a predictive
factor for an early hematological recurrence, whereas an abiding negative PCR in the bone
marrow is usually associated with long‐term survival and cure after therapy (also in patients
with relapse)10;11.
1.3 Therapeutic approaches in APL
APL disease must be classified as an emergency with immediate initiation of supportive
therapy. In the case of morphological and clinical suspicion of APL, therapy must be started
immediately before a genetic diagnosis is available because of the potential lethal
complications and the possibility of a curative therapy. Prior to therapy a bone marrow and
blood diagnostic is essential. First‐line treatment recommendations differ for patients of the
high‐risk group and the non‐high‐risk group according to the Sanz Score which are defined as
follows5:
WBC in high‐risk group WBC in non‐high‐risk group
> 10 Gpt / l 10 Gpt / l
1.3.1 ATRA‐based induction therapy
Anthracycline and Ara‐C‐based combination chemotherapy were used until the 1980s and
complete remission rates (CR) of up to 80 % were achieved. However, disease recurrences
were observed in two thirds of the patients. Furthermore, this therapy was associated with a
high rate of early death due to toxicity and bleeding12‐15.
The introduction of all‐trans retinoic acid (ATRA) significantly changed therapeutic success in
APL patients. ATRA causes differentiation of abnormal promyelocytes to mature neutrophils
in vitro and in vivo. Complete remission rates were achieved with single agent ATRA in up to
80‐90 % of newly‐diagnosed and relapsed patients with APL16‐21. Furthermore, ATRA rapidly
alleviates the disturbed coagulation cascade. However, the accelerated differentiation to
mature neutrophils often induces a rapid increase of leukocytes. In fact, in 15‐20 % of
patients an ATRA‐ or better “differentiation‐syndrome” can occur which is associated with a
high mortality rate22‐25.
The duration of remission with single agent ATRA therapy however was often not
enduring16;17. Therefore, concepts with combined and concomitant administration of ATRA
and intensive chemotherapy were explored26;27. These studies consistently showed a higher
CR rate (>95 %) compared to conventional chemotherapy as well as prolonged remission
Page 7 of 32
duration in either randomized or historical comparisons28‐37. The most widely used
combination for induction therapy irrespective of APL risk is the combination of ATRA plus
Idarubicin (AIDA).
1.3.2 Consolidation therapy
Molecular remissions can be achieved in more than 90 % of patients if at least two
anthracycline‐containing consolidation therapies are used. Therefore, this is considered the
present therapeutic standard for all patients with APL in CR after induction chemotherapy38.
There is no comparative study on the efficacy of ATRA in addition to chemotherapy during
consolidation. However, historical comparisons have demonstrated that incorporation of
ATRA contributed to improved outcome27;39.
The role of Ara‐C in APL has long been controversial. However, comparative cohort studies in
high‐risk patients (WBC > 10 Gpt / l) show a clearly positive effect with a significant higher
remission rate, better disease‐free and overall survival rate in favour of Ara‐C‐based therapy
during consolidation6;27;35.
1.3.3 Maintenance therapy
In the European APL‐93 study it was shown that a three‐fold maintenance therapy with
ATRA, 6‐mercaptopurine and methotrexate results in a lower recurrence rate, especially in
patients with high white blood cell count at diagnosis. However, this study did not differ
between patients according to the PCR‐status after consolidation31. Furthermore, no
advantage of maintenance therapy in patients who tested negative after consolidation was
observed by the Italian GIMEMA group40. Therefore, maintenance therapy is based on a
relatively low level of evidence. Despite these controversial results, maintenance therapy is
still included in the most ATRA‐plus‐chemotherapy‐based protocols.
Due to the high cure rate with ATRA and chemotherapy in APL, there is no indication for
hematopoietic stem cell transplantation (HSCT) in patients who are in first molecular
remission after completion of consolidation therapy.
1.3.4 Treatment of minimal residual disease (MRD) or relapse
Despite successful first‐line treatment approximately 10‐15 % of patients relapse. In case of
persistence of minimal residual disease (MRD) with PML/RARa detection or molecular or
hematological relapse, treatment with arsenic trioxide (ATO) +/‐ ATRA for induction and
consolidation therapy is the treatment of choice. This should be followed by further post
consolidation therapy. Autologous HSCT after high‐dose therapy probably contributes to the
stabilization of remission, provided that PML/RARα is negative by PCR in the autologous
graft and in the patient bone marrow prior to transplantation41‐46. In patients not achieving
clearance of MRD by conventional therapy including ATO an allogeneic HSCT should be
considered.
Page 8 of 32
1.3.5 ATO in APL
ATO is the most effective single agent in APL47. ATO acts via complex mechanism in APL that
is not yet fully explained. At a high concentration (0.5 to 2.0 μmol/l) ATO induces apoptosis
in vitro, while at lower concentrations (0.1 to 0.5 μmol/l) it induces partial differentiation of
leukemic promyelocytes through PML/RARα degradation and inhibits angiogenesis48‐51.
ATO is licensed for the treatment of relapsed and refractory APL in the USA and
Europe44;45;52‐58 and can achieve remission rates in up to 90 % of patients. Concerning its
toxicity profile, ATO is usually well tolerated and its use is associated with a series of
manageable adverse events (hyperleucocytosis, increase of liver enzymes, APL
differentiation syndrome, prolongation of the QT interval59). Most of the adverse events
mentioned above are usually mild and manageable44;58.
The antileukemic efficiency of ATO is increased when combined with ATRA. ATO as single
agent is able to induce durable molecular remission after two cycles in the majority of
patients treated for disease recurrence57. Results of various studies conducted with ATO as
single agent or combined with ATRA for newly diagnosed APL patients reported CR rates of
86‐95 %, molecular remission rates after two cycles of 76‐100 % and survival rates of 86‐
88 %, with significantly better responses being obtained in patients with non‐high risk
disease as compared to high‐risk patients60‐64. Recent data of the APL0406 – Intergroup
Study (GIMEMA – AML‐SG/SAL) showed that ATO plus ATRA is at least as effective as AIDA‐
based therapy as first‐line treatment in non‐high risk APL patients65. In particular, early
mortality was almost absent in the experimental treatment arm combining ATO and ATRA. In
addition, the results of a recent published randomized trial evaluating ATO in first‐line
therapy during consolidation demonstrated that ATO further reduced the risk of recurrence
and improved survival66.
1.4 Intergroup guidelines for the treatment of APL
APL is a highly curable malignancy. Once regarded as the most aggressive and rapidly fatal
human leukemia, APL has become over the past 2 decades a curable disease, with more than
80% of patients now being long‐term survivors. However, treatment of APL is still
challenging, in particular during induction therapy, and high rates of cure can only be
achieved in centers with well trained staff. Therefore, treatment in highly specialized and
experienced centers is mandatory including standardized procedures. The recommendations
on APL diagnostics and therapy of newly diagnosed and relapsed APL are based on national
(http://www.dgho‐onkopedia.de/de/onkopedia/leitlinien/akute‐promyelozytaere‐
leukaemie) and European (ELN) guidelines38 (http://www.leukemia‐
net.org/content/leukemias/aml/apl/apl_recommendations/index_eng.html).
The detailed German intergroup treatment guidelines are provided below (Figure 1) and
depend on the leukocyte counts at initial diagnosis (see 1.3).

Page 9 of 32
FIGURE 1: OVERVIEW OF TREATMENT RECOMMENDATIONS FOR NEWLY DIAGNOSED APL
Page 10 of 32
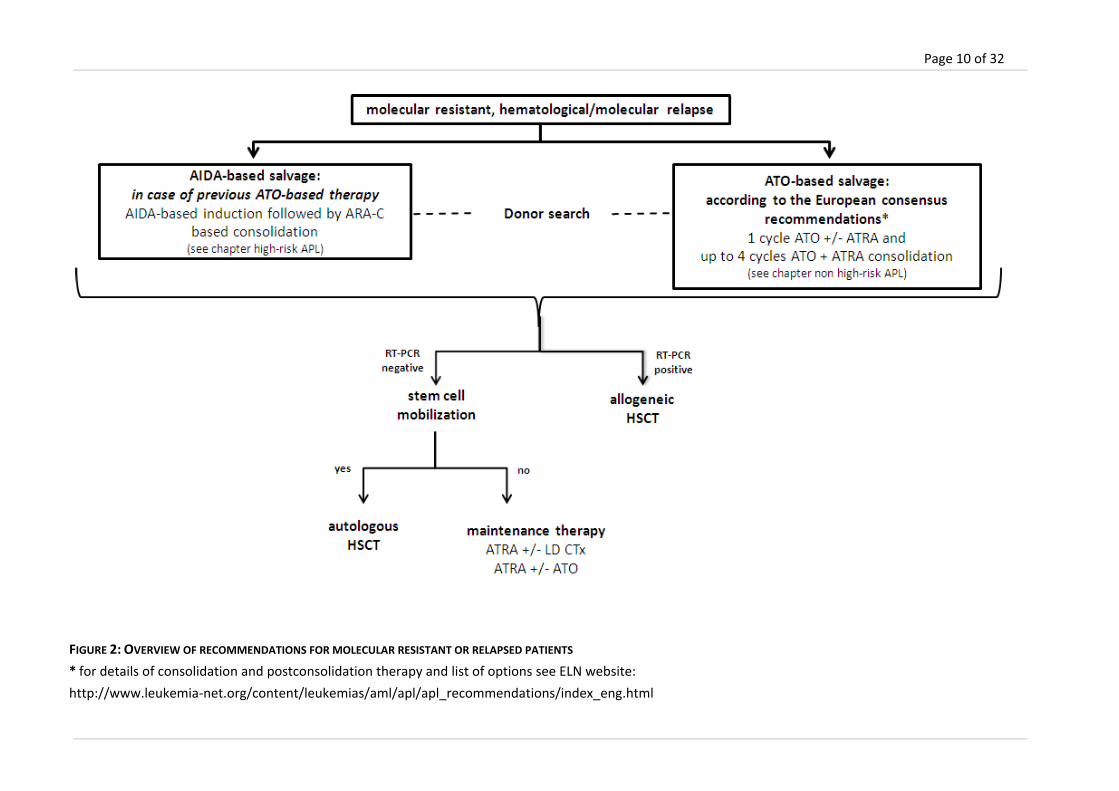
FIGURE 2: OVERVIEW OF RECOMMENDATIONS FOR MOLECULAR RESISTANT OR RELAPSED PATIENTS
* for details of consolidation and postconsolidation therapy and list of options see ELN website:
http://www.leukemia‐net.org/content/leukemias/aml/apl/apl_recommendations/index_eng.html

Page 11 of 32
1.4.1 Treatment recommendation for high‐risk APL (WBC >10 Gpt/l at initial diagnosis)
according to AIDA
1.4.1.1 INDUCTION THERAPY (HIGH‐RISK APL)5
Standard induction therapy ‐ high‐risk APL
Drug Dose Route Administration Comments
ATRA 45 mg/m2 p.o. in two
single
doses
daily until CR, max. 60 days;
doses will be rounded‐up to next
10 mg increment
Idarubicin 12 mg/m2 i.v. day 1, 3, 5, 7 only 3 days in elderly and comorbid
patients
prophylaxis of APL differentiation syndrome with prednisone 0.5 mg / kg / day p.o. from
day 1 of ATO application to the end of induction therapy and possibly hydroxyurea (see
2.1) when leucocytes further raise up to > 10 Gpt / l
bone marrow puncture on day 28
induction therapy should be terminated on the basis of morphological criteria (if CR or
CRi is reached on day 28)
in case of not achieving CR or CRi on day 28, ATRA therapy should be continued up to
max. day 60 until terminal differentiation is reached; this should be accompanied by
serial bone marrow assessments to definitively demonstrate CR
cytogenetic and molecular assessment at the end of induction therapy has no value in
case of CR. Molecular responses should be assessed after consolidation only
1.4.1.2 CONSOLIDATION THERAPY (HIGH‐RISK APL)
After achieving a hematological CR after induction therapy, 3 courses of ATRA plus
chemotherapy are intended. Start of consolidation cycles is considered after hematological
recovery with neutrophils ≥ 1.0 Gpt / l and platelets ≥ 100 Gpt / l. In case of morphological
CR and regenerated blood counts, consolidation therapy should be started within 4 weeks
after documented CR. Each course of therapy should be initiated at hematological recovery
from the previous course. The PCR status after the end of consolidation is an important
stratification parameter for the subsequent therapy.
Page 12 of 32
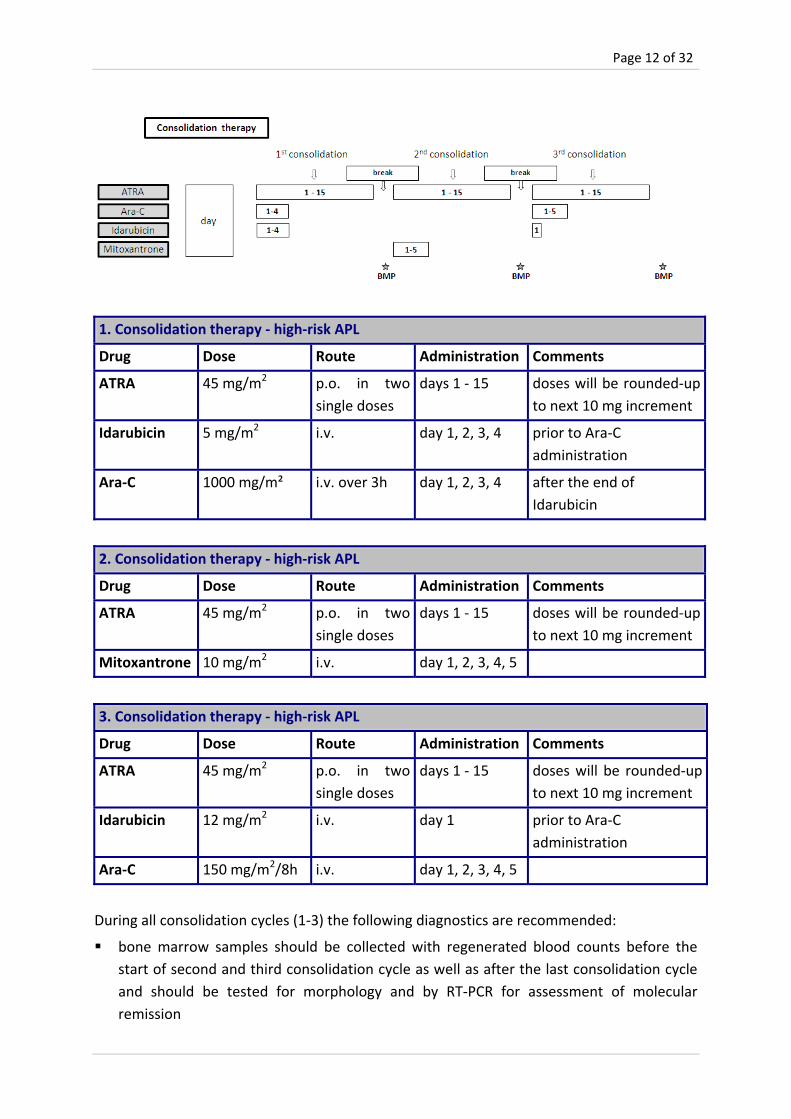
1. Consolidation therapy ‐ high‐risk APL
Drug Dose Route Administration Comments
ATRA 45 mg/m2 p.o. in two
single doses
days 1 ‐ 15 doses will be rounded‐up
to next 10 mg increment
Idarubicin 5 mg/m2 i.v. day 1, 2, 3, 4 prior to Ara‐C
administration
Ara‐C 1000 mg/m² i.v. over 3h day 1, 2, 3, 4 after the end of
Idarubicin
2. Consolidation therapy ‐ high‐risk APL
Drug Dose Route Administration Comments
ATRA 45 mg/m2 p.o. in two
single doses
days 1 ‐ 15 doses will be rounded‐up
to next 10 mg increment
Mitoxantrone 10 mg/m2 i.v. day 1, 2, 3, 4, 5
3. Consolidation therapy ‐ high‐risk APL
Drug Dose Route Administration Comments
ATRA 45 mg/m2 p.o. in two
single doses
days 1 ‐ 15 doses will be rounded‐up
to next 10 mg increment
Idarubicin 12 mg/m2 i.v. day 1 prior to Ara‐C
administration
Ara‐C 150 mg/m2/8h i.v. day 1, 2, 3, 4, 5
During all consolidation cycles (1‐3) the following diagnostics are recommended:
bone marrow samples should be collected with regenerated blood counts before the
start of second and third consolidation cycle as well as after the last consolidation cycle
and should be tested for morphology and by RT‐PCR for assessment of molecular
remission

Page 13 of 32
patients without molecular remission at the end of the entire consolidation program will
be considered as molecularly resistant (see 1.4.4)
Intracranial prophylaxis before each consolidation cycle is not recommended in general, but
may be considered in high risk patients, according to local guidelines.
1.4.1.3 MAINTENANCE THERAPY (HIGH‐RISK APL)
The clinical benefit of maintenance therapy is of lower evidence according to recent
studies28;33;40 and should be initiated only in patients who are in a molecular remission (PML‐
RARα‐negative in the bone marrow).
The start of maintenance therapy is one month (up to a maximum of 3 months) after
consolidation therapy if neutrophils are ≥ 1.0 Gpt / l and platelets are 100 Gpt / l. The duration of maintenance therapy is a total period of 2 years. During this time, patients
receive 7 courses with 6‐mercaptopurine and methotrexate (each lasting 3 month) and 6
courses of ATRA for 15 days.
The last cycle ends with the administration of 6‐mercaptopurine and methotrexate.
Maintenance therapy – high‐risk APL
Drug Dose Route Administration Comments
6‐Mercaptopurine 50 mg/m2 p.o. daily (day 1‐91)
followed by 15
days of rest
for 7 cycles; rounded
down to the nearest
10 mg increment
Methotrexate 15 mg/m2 i.m./p.o. once weekly for
91 days followed
by 15 days of rest
for 7 cycles
ATRA 45 mg/m2 p.o. in two
single doses
daily for 15 days
(prior to day 1 or
after day 91)
every 3 month for a
total of 6 cycles;
during ATRA therapy
treatment break of
6‐MP und MTX
Consider cotrimoxazol as pneumocystis prophylaxis
Page 14 of 32
bone marrow samples should be collected with regenerated blood counts at the
beginning of each maintenance cycle as well as after the last maintenance cycle and
should be tested for morphology and by RT‐PCR for assessment of molecular remission
1.4.1.4 DOSE MODIFICATIONS
Dose modifications of ATRA and conventional chemotherapeutic agents (mitoxantrone, ida‐
rubicine, methothrexate and 6‐mercaptopurine) should be performed according to the
SMPC.
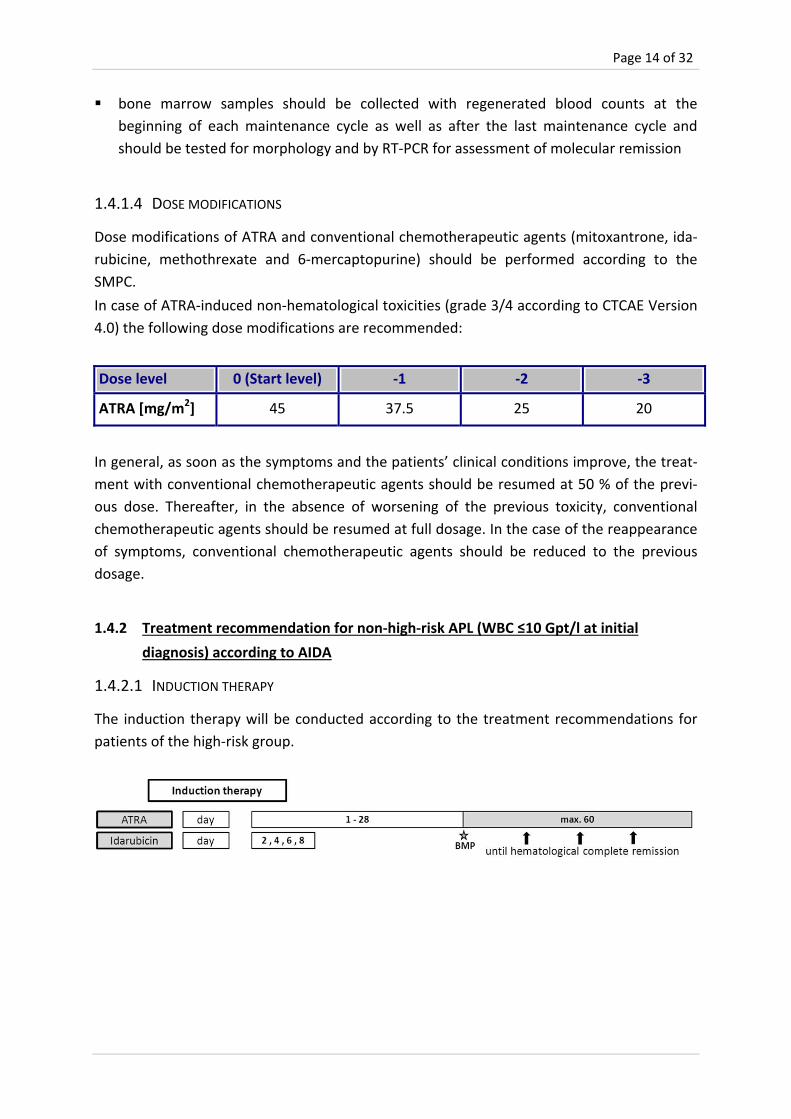
In case of ATRA‐induced non‐hematological toxicities (grade 3/4 according to CTCAE Version
4.0) the following dose modifications are recommended:
Dose level 0 (Start level) ‐1 ‐2 ‐3
ATRA [mg/m2] 45 37.5 25 20
In general, as soon as the symptoms and the patients’ clinical conditions improve, the treat‐
ment with conventional chemotherapeutic agents should be resumed at 50 % of the previ‐
ous dose. Thereafter, in the absence of worsening of the previous toxicity, conventional
chemotherapeutic agents should be resumed at full dosage. In the case of the reappearance
of symptoms, conventional chemotherapeutic agents should be reduced to the previous
dosage.
1.4.2 Treatment recommendation for non‐high‐risk APL (WBC ≤10 Gpt/l at initial
diagnosis) according to AIDA
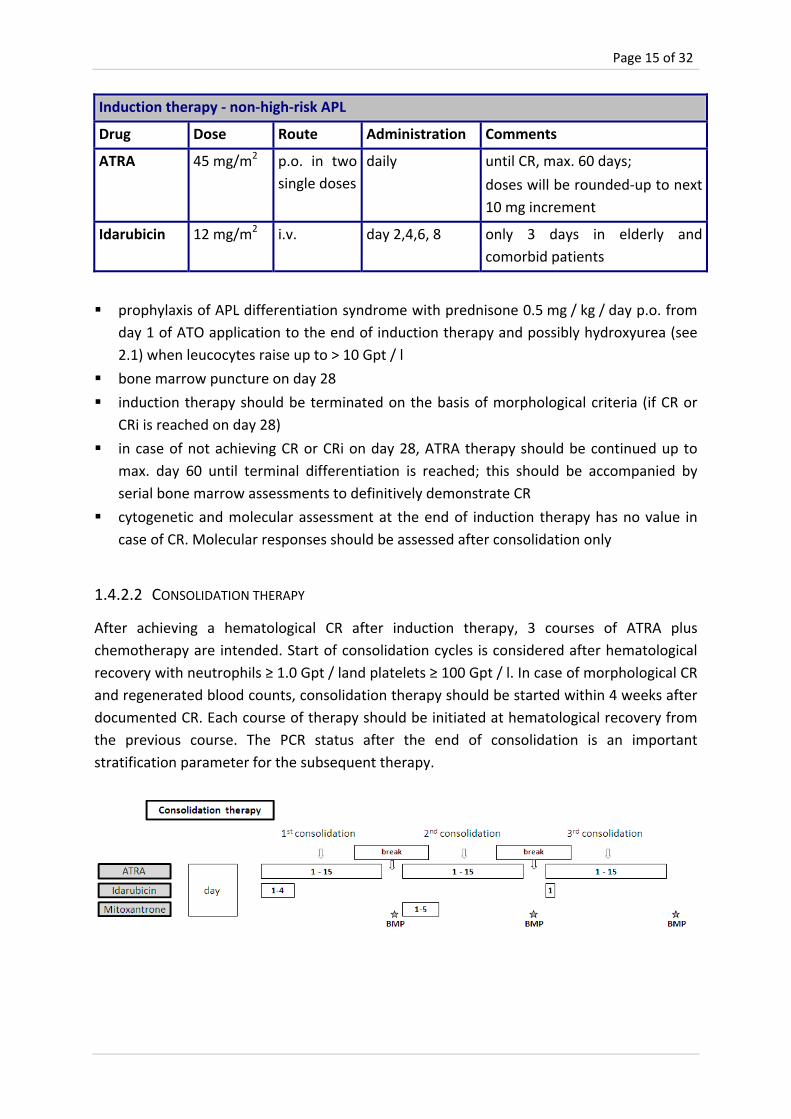
1.4.2.1 INDUCTION THERAPY
The induction therapy will be conducted according to the treatment recommendations for
patients of the high‐risk group.
Page 15 of 32
Induction therapy ‐ non‐high‐risk APL
Drug Dose Route Administration Comments
ATRA 45 mg/m2 p.o. in two
single doses
daily until CR, max. 60 days;
doses will be rounded‐up to next
10 mg increment
Idarubicin 12 mg/m2 i.v. day 2,4,6, 8 only 3 days in elderly and
comorbid patients
prophylaxis of APL differentiation syndrome with prednisone 0.5 mg / kg / day p.o. from
day 1 of ATO application to the end of induction therapy and possibly hydroxyurea (see
2.1) when leucocytes raise up to > 10 Gpt / l
bone marrow puncture on day 28
induction therapy should be terminated on the basis of morphological criteria (if CR or
CRi is reached on day 28)
in case of not achieving CR or CRi on day 28, ATRA therapy should be continued up to
max. day 60 until terminal differentiation is reached; this should be accompanied by
serial bone marrow assessments to definitively demonstrate CR
cytogenetic and molecular assessment at the end of induction therapy has no value in
case of CR. Molecular responses should be assessed after consolidation only
1.4.2.2 CONSOLIDATION THERAPY
After achieving a hematological CR after induction therapy, 3 courses of ATRA plus
chemotherapy are intended. Start of consolidation cycles is considered after hematological
recovery with neutrophils ≥ 1.0 Gpt / land platelets ≥ 100 Gpt / l. In case of morphological CR
and regenerated blood counts, consolidation therapy should be started within 4 weeks after
documented CR. Each course of therapy should be initiated at hematological recovery from
the previous course. The PCR status after the end of consolidation is an important
stratification parameter for the subsequent therapy.

Page 16 of 32
1. Consolidation therapy – non‐high‐risk APL
Drug Dose Route Administration Comments
ATRA 45 mg/m2 p.o. in two
single doses
days 1 ‐ 15 doses will be rounded‐up to
next 10 mg increment
Idarubicin 5 mg/m2 i.v. day 1, 2, 3, 4
2. Consolidation therapy – non‐high‐risk APL
Drug Dose Route Administration Comments
ATRA 45 mg/m2 p.o. in two
single doses
days 1 ‐ 15 doses will be rounded‐up to
next 10 mg increment
Mitoxantrone 10 mg/m2 i.v. day 1, 2, 3, 4, 5
3. Consolidation therapy – non‐high‐risk APL
Drug Dose Route Administration Comments
ATRA 45 mg/m2 p.o. in two
single doses
days 1 ‐ 15 doses will be rounded‐up to
next 10 mg increment
Idarubicin 12 mg/m2 i.v. day 1
During all consolidation cycles (1‐3) the following diagnostics are recommended:
bone marrow samples should be collected with regenerated blood counts before the
start of second and third consolidation cycle as well as after the last consolidation cycle
and should be tested for morphology and by RT‐PCR for assessment of molecular
remission
patients without molecular remission at the end of the entire consolidation program will
be considered as molecular resistant (see 1.4.4)
An intracranial prophylaxis before each consolidation cycle is not recommended in general.
1.4.2.3 MAINTENANCE THERAPY
Maintenance therapy is provided in section 1.4.1.3
1.4.2.4 DOSE MODIFICATIONS
Dose modifications are provided in section 1.4.1.4.

Page 17 of 32
1.4.3 Treatment recommendation for non‐high‐risk APL (WBC ≤10 Gpt/l at initial
diagnosis) according to the APL0406 study
Recently, the APL0406 study provided evidence that the combination of ATO and ATRA is at
least as effective as the AIDA regimen65, while sparing mainly hematological toxicity. In fact,
there was even an improvement in survival with the ATO/ATRA arm. Therefore, this regimen
was included here since physicians might consider it for their patients although ATO has only
marketing authorization in the EU for relapsed APL.
1.4.3.1 INDUCTION THERAPY
Induction therapy ‐ non‐high‐risk APL
Drug Dose Route Administration Comments
ATO 0.15 mg/kg i.v. over 2 h daily starting on day 1; until CR, max. 60
days
ATRA 45 mg/m2 p.o. in two
single doses
daily starting on day 1; until CR, max. 60
days;
doses will be rounded‐up to next
10 mg increment
prophylaxis of APL differentiation syndrome with prednisone 0.5 mg / kg / day p.o. from
day 1 of ATO application to the end of induction therapy and possibly hydroxyurea (see
2.1) when leucocytes raise up to > 10 Gpt / l
bone marrow puncture on day 28
induction therapy should be terminated on the basis of morphological criteria (if CR or
CRi is reached on day 28)
in case CR or CRi is not achieved by day 28, ATO/ATRA therapy should be continued up to
max. day 60 until terminal differentiation is reached; this should be accompanied by
serial bone marrow assessments to definitively demonstrate CR
cytogenetic and molecular assessment at the end of induction therapy has no value in
case of CR. Molecular responses should be assessed after consolidation only
Page 18 of 32
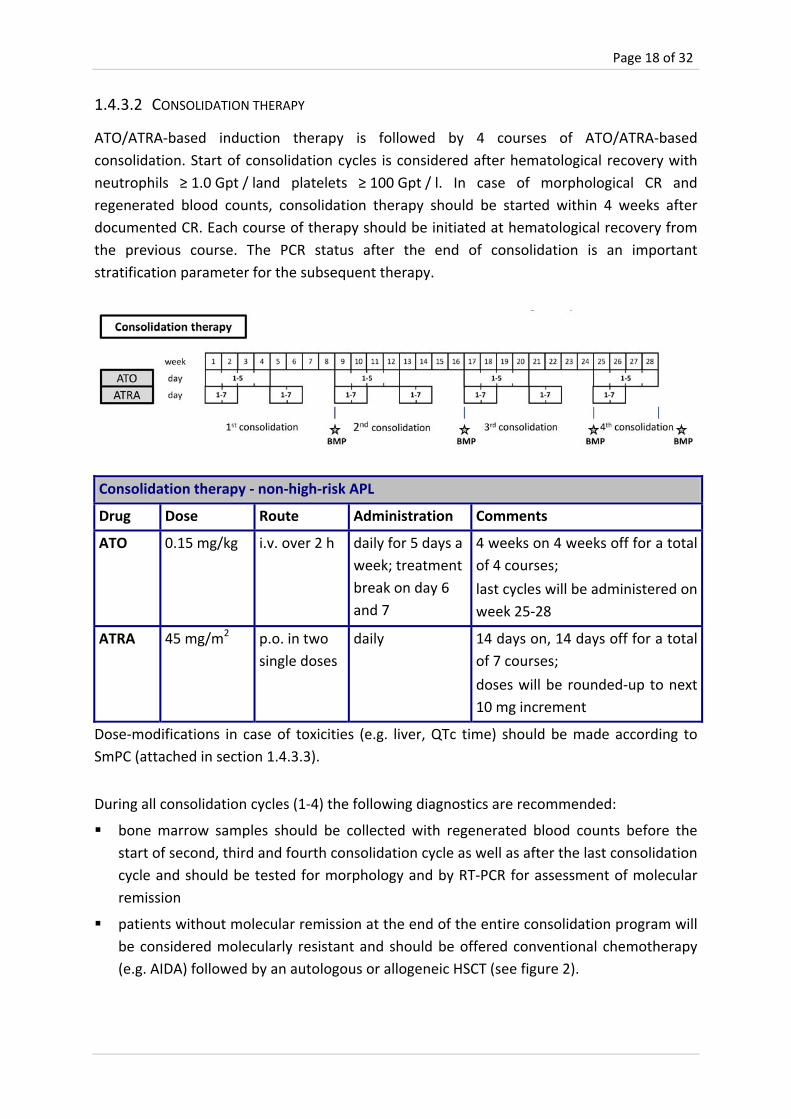
1.4.3.2 CONSOLIDATION THERAPY
ATO/ATRA‐based induction therapy is followed by 4 courses of ATO/ATRA‐based
consolidation. Start of consolidation cycles is considered after hematological recovery with
neutrophils ≥ 1.0 Gpt / land platelets ≥ 100 Gpt / l. In case of morphological CR and
regenerated blood counts, consolidation therapy should be started within 4 weeks after
documented CR. Each course of therapy should be initiated at hematological recovery from
the previous course. The PCR status after the end of consolidation is an important
stratification parameter for the subsequent therapy.
Consolidation therapy ‐ non‐high‐risk APL
Drug Dose Route Administration Comments
ATO 0.15 mg/kg i.v. over 2 h daily for 5 days a
week; treatment
break on day 6
and 7
4 weeks on 4 weeks off for a total
of 4 courses;
last cycles will be administered on
week 25‐28
ATRA 45 mg/m2 p.o. in two
single doses
daily 14 days on, 14 days off for a total
of 7 courses;
doses will be rounded‐up to next
10 mg increment
Dose‐modifications in case of toxicities (e.g. liver, QTc time) should be made according to
SmPC (attached in section 1.4.3.3).
During all consolidation cycles (1‐4) the following diagnostics are recommended:
bone marrow samples should be collected with regenerated blood counts before the
start of second, third and fourth consolidation cycle as well as after the last consolidation
cycle and should be tested for morphology and by RT‐PCR for assessment of molecular
remission
patients without molecular remission at the end of the entire consolidation program will
be considered molecularly resistant and should be offered conventional chemotherapy
(e.g. AIDA) followed by an autologous or allogeneic HSCT (see figure 2).
Page 19 of 32
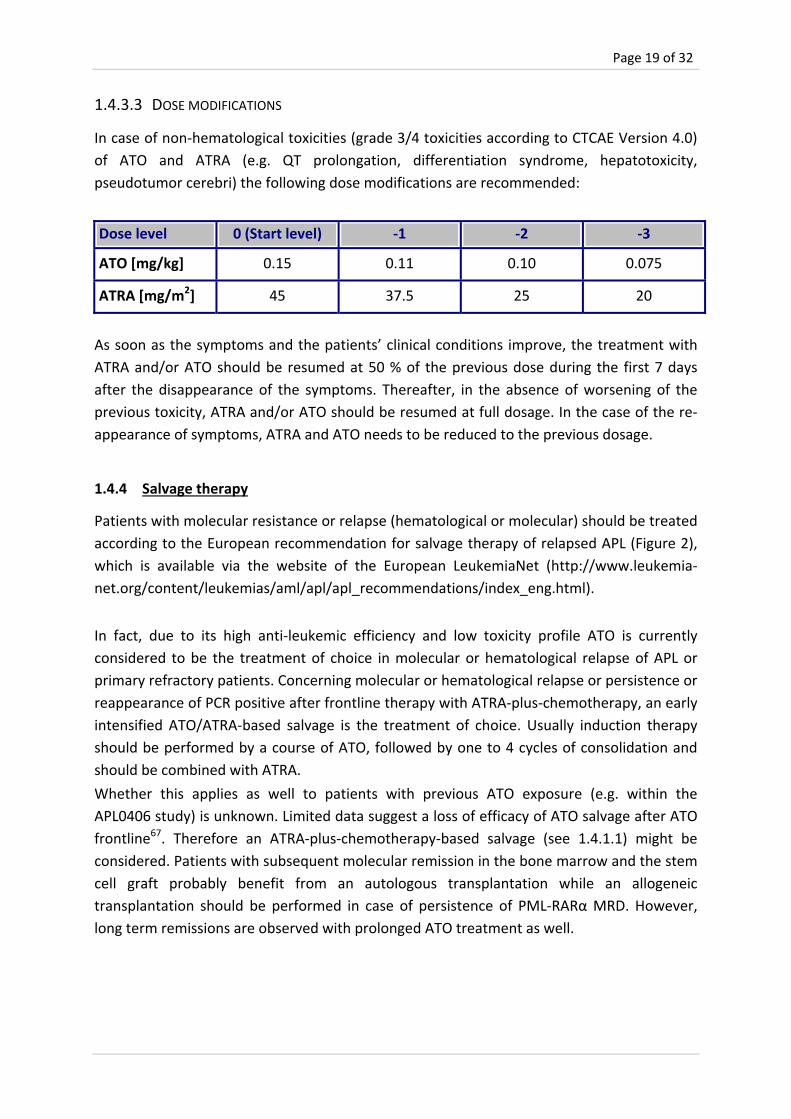
1.4.3.3 DOSE MODIFICATIONS
In case of non‐hematological toxicities (grade 3/4 toxicities according to CTCAE Version 4.0)
of ATO and ATRA (e.g. QT prolongation, differentiation syndrome, hepatotoxicity,
pseudotumor cerebri) the following dose modifications are recommended:
Dose level 0 (Start level) ‐1 ‐2 ‐3
ATO [mg/kg] 0.15 0.11 0.10 0.075
ATRA [mg/m2] 45 37.5 25 20
As soon as the symptoms and the patients’ clinical conditions improve, the treatment with
ATRA and/or ATO should be resumed at 50 % of the previous dose during the first 7 days
after the disappearance of the symptoms. Thereafter, in the absence of worsening of the
previous toxicity, ATRA and/or ATO should be resumed at full dosage. In the case of the re‐
appearance of symptoms, ATRA and ATO needs to be reduced to the previous dosage.
1.4.4 Salvage therapy
Patients with molecular resistance or relapse (hematological or molecular) should be treated
according to the European recommendation for salvage therapy of relapsed APL (Figure 2),
which is available via the website of the European LeukemiaNet (http://www.leukemia‐
net.org/content/leukemias/aml/apl/apl_recommendations/index_eng.html).
In fact, due to its high anti‐leukemic efficiency and low toxicity profile ATO is currently
considered to be the treatment of choice in molecular or hematological relapse of APL or
primary refractory patients. Concerning molecular or hematological relapse or persistence or
reappearance of PCR positive after frontline therapy with ATRA‐plus‐chemotherapy, an early
intensified ATO/ATRA‐based salvage is the treatment of choice. Usually induction therapy
should be performed by a course of ATO, followed by one to 4 cycles of consolidation and
should be combined with ATRA.
Whether this applies as well to patients with previous ATO exposure (e.g. within the
APL0406 study) is unknown. Limited data suggest a loss of efficacy of ATO salvage after ATO
frontline67. Therefore an ATRA‐plus‐chemotherapy‐based salvage (see 1.4.1.1) might be
considered. Patients with subsequent molecular remission in the bone marrow and the stem
cell graft probably benefit from an autologous transplantation while an allogeneic
transplantation should be performed in case of persistence of PML‐RARα MRD. However,
long term remissions are observed with prolonged ATO treatment as well.

Page 20 of 32
2 SUPPORTIVE MANAGEMENT OF APL
APL is an acute vital threat to the patient often caused by a severe plasma coagulation
disorder that can be increased by the introduction of conventional therapy68.
2.1 Treatment of leukocytosis
Guidelines for administering hydroxyurea in patients who develop sustained leukocytosis
(>10 x 109/l) after initiation of therapy are detailed below:
Hydroxyurea should be continued at a given dose to keep the WBC count <10 x 109/l and
subsequently tapered.
Recommendation for initiation of hydroxyurea:
WBC 10 – 50 x 109/l 500 mg four times a day
WBC > 50 x 109/l 1000 mg four times a day
2.2 Treatment of coagulopathy
The pathogenesis of hemorrhagic complications of APL is complex and in particular includes
factors of blood coagulation and fibrinolysis. The coagulopathy is biochemically conspicuous
manifesting as a severe hypofibrinogenemia, increased levels of fibrin degradation products,
a prolonged prothrombin time, a prolonged partial thromboplastin and thrombin time and
thrombocytopenia.
It must be noted that the combination with ATRA can result in a reversion of the clotting
disorder into a thrombophilic constellation with thromboembolic complications.
Administration of fibrinogen (2 g i.v.) is recommended if fibrinogen levels are below 1 g / l. In
case of unavailability of pure fibrinogen preparation, a substitution with fresh frozen plasma
(FFP) is indicated. We recommend to keep platelet counts around 30‐50 Gpt / l in the initial
phase of therapy and Hb‐values should be maintained at > 8 g/dl.
Treatment with tranexamic acid (antifibrinolytic agent such as cyklopkapron® 3 x 1000 mg
i.v. / d), fibrin‐stabilizing factor (Factor XIII, e.g. Fibrogammin® 1250 E) and AT III (e.g.
Cybernin® HS) at values below 50 % of normal range can be considered individually although
not supported by randomized trials69. The prophylactic administration of heparin has no
proven benefit.

Page 21 of 32
2.3 Differentiation syndrome (formerly “ATRA syndrome”)
During treatment with all‐trans retinoic acid (ATRA) and ATO a differentiation syndrome can
develop rapidly. It´s diagnosis should be clinically established by the presence of at least
three of the following signs, but it is suspected already at presence of only one symptom:
weight gain
respiratory distress
unexplained fever
interstitial pulmonary infiltrates
pleural or pericardial effusions with or without leukocytosis
No single sign or symptom may be considered per se as diagnostic for the syndrome. The
release of cytokines leads to this syndrome, which can become fatal if untreated. Prophylaxis
with prednisone is recommended.
In case of diagnosis of an APL differentiation syndrome the administration of APL therapy
should be stopped in time. Early transfer of patients to an ICU for improved monitoring of
vital signs should be considered. Immediate administration of dexamethasone (10 mg) i.v.
every 12 hours for at least 3 days should be started at the first suspicion and a concomitant
diuretic therapy are recommended until the disappearance of symptoms and signs. As soon
as the patients’ clinical condition improve and the symptoms have disappeared and the WBC
count is sustainably lowered to <10 x 109/l, the APL treatment with ATRA and/or ATO can be
resumed at 50 % of the previous dose during the first 7 days. Thereafter in the absence of
worsening of the previous toxicity, ATRA and/or ATO might be resumed at full dosage. In the
case of the reappearance of symptoms, ATRA and ATO will be reduced at the previous
dosage.
2.4 Pseudotumor cerebri with ATRA therapy
Particularly in younger patients a "pseudotumor cerebri" may occur during ATRA therapy,
manifesting by headaches, nausea, vomiting and blurred vision. It is recommended to
discontinue ATRA treatment temporarily and to administer opiates. As soon as the
symptoms and the patients’ clinical conditions improve, the treatment with ATRA will be
resumed at 50 % of the previous dose during the first 7 days after the amelioration of
pseudotumor cerebri. Thereafter, in the absence of worsening of the previous toxicity, ATRA
should be resumed at full dosage.
2.5 Hepatotoxicity with ATO/ATRA
Hepatotoxicity requires temporary suspension of ATRA and/or ATO. As soon as serum
bilirubin and/or SGOT and/or alkaline phosphatase have been reduced to < 4 times the
normal upper level, the treatment with ATRA and/or ATO will be resumed at 50 % of the
Page 22 of 32
previous dose during the first 7 days. Thereafter, in the absence of worsening of the
previous toxicity, ATRA and/or ATO should be resumed at full dosage.
2.6 QT prolongation with ATO therapy
Prolongation of the QT interval in the ECG has been observed during treatment with ATO.
This can lead to ventricular tachycardia (torsade de pointes) with a fatal outcome. In this
context, possible interaction with other drugs that prolong the QT interval must also be
taken into account. For this reason, close monitoring of the ECG and of the electrolytes is
necessary during treatment with ATO. In particular, the Mg++ and K+ levels should always be
kept in the high‐normal range, taking in consideration possible concomitant treatments that
deplete electrolyte levels (e.g. amphotericin B, furosemide etc.). In ECG the QT interval is
represented by the QRS complex, the ST segment and the T wave. Its measurement starts
from the deepest point of Q wave to the end of T wave. This interval greatly depends on the
heart rate and several formulas have been proposed to adjust the QT interval for heart rate
in order to obtain the corrected QT interval (QTc); however, no one of these proposed
formulas is satisfactory. Despite that, data from medical literature indicate that one of the
most simple method for adjusting the QT interval for heart rate is the Fridericia formula:
QTc = QT/cube root of RR
For increased accuracy, the QT interval should be measured on serial ECGs and several
successive beats and averaged for each ECG. The averaged QT value obtained should be
used in the above formula in which all measurement must be expressed in msec (i.e.: 0,470
sec=470msec). Applying this formula, a QTc interval > 500 msec must be considered
prolonged (both genders).
ATO should be discontinued together with any medication known to prolong the QTc
interval and electrolytes should be repleted. The time between discontinuing ATO and
normalization of the QTc interval may be several days. Once QTc is normalized, resume ATO
at 0.075 mg/Kg (50%) for the first 7 days, and then if no further prolongation occurs, resume
at 0.11 mg/Kg for a second week. Thereafter, if no prolongation occurs, resume ATO at full
dose.
Page 23 of 32
3 EVALUATION OF RESPONSE
For the evaluation of treatment response the following hematological and molecular
remission criteria are used as basis for the documentation sheet (CRF).
3.1 Hematological remission criteria
Hematological complete remission (CR)70
5 % blasts without atypical promyelocytes in the bone marrow
Neutrophils 1,0 Gpt/l
platelets 100 Gpt/l
Hematological incomplete remission (CRi)
5 % blasts without atypical promyelocytes in the bone marrow
Neutrophils < 1,0 Gpt/l
platelets < 100 Gpt/l
Non‐Response
≥ 5 % blasts and atypical promyelocytes up to 60 days after beginning of induction
therapy
Hematological Relapse
After a pre‐existing documented morphological CR there is a relapse if:
0,1 Gpt/l of blasts in the peripheral blood
percentage of blasts / atypical promyelocytes > 10 % in the bone marrow at any time
during follow‐up
meningeosis leucemica
bioptic verifiable extramedullary relapse
3.2 Molecular remission criteria
Molecular Complete Remission (CRm)
absence of the PML‐RAR hybrid transcript by RT‐PCR in bone marrow samples
Molecular Resistant Disease (RDm)
persistence of PML‐RAR hybrid transcript in the bone marrow cells at the end of the
last consolidation cycle
it should be always confirmed in two consecutive bone marrow samples taken 2
weeks apart
Page 24 of 32
Molecular relapse
conversion from RT‐PCR negative to positive PML‐RAR hybrid transcript in the bone marrow samples collected at any time after the 3rd consolidation cycle or
recurrent PML‐RARPCR‐positivity of two successive bone marrow samples in
distance of 2‐4 weeks after the last consolidation therapy
conversion/ relapse should be always confirmed in two consecutive bone marrow
samples taken 2 weeks apart
4 DIAGNOSTIC EXAMINATION PROGRAM
The general diagnosis of APL is based on the local standards. Close monitoring of the
following lab parameters should be carried out especially during induction therapy: Quick,
PTT, fibrinogen, hemoglobin, leukocytes, neutrophils, platelets, ATIII, factor XIII and D‐
dimers (depending on the severity of the bleeding disorders up to three times daily).
An ECG, echocardiographic examination (ejection fraction and valve abnormalities) is
recommended before each induction therapy and after completion of treatment.
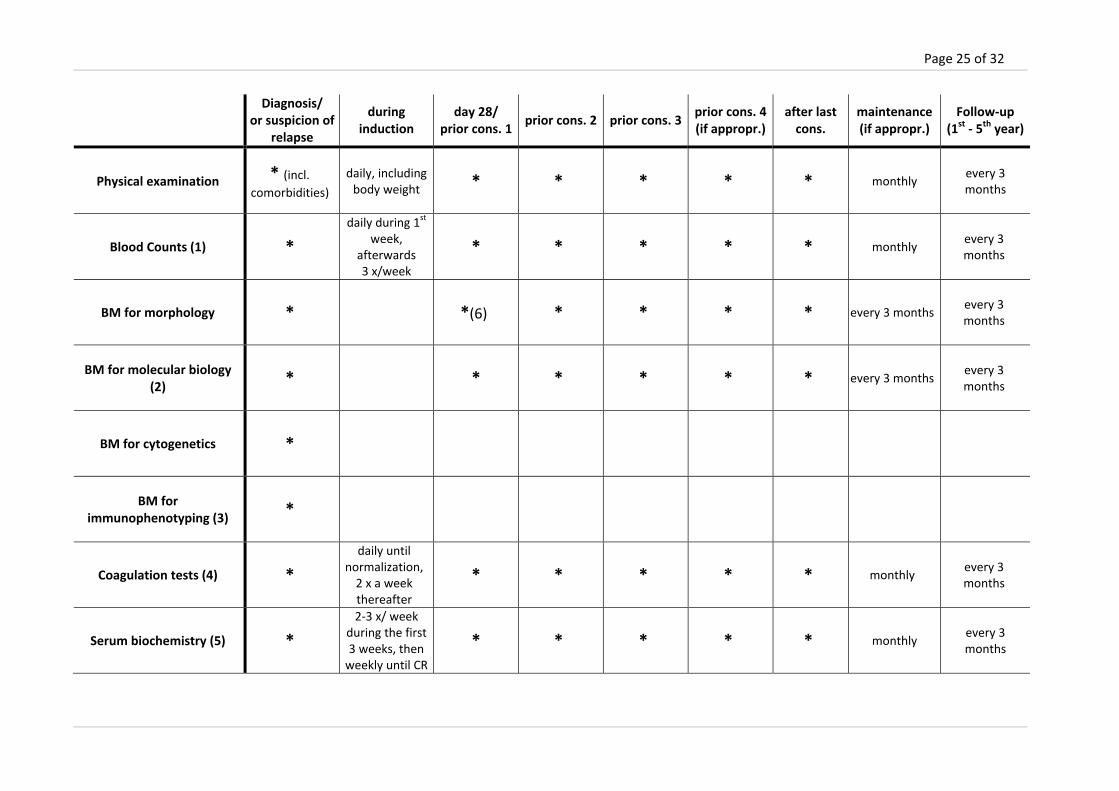
Diagnostic examination schedule
Molecular analyses (PCR) and morphological analyses of the bone marrow and peripheral
blood are recommended
at initial diagnosis
after induction
prior to the second and following consolidation therapy
after the last consolidation therapy
quarterly during maintenance therapy
after therapy quarterly during a 5 year follow‐up from the start of therapy
suspicion of relapse
Cytogenetic and immunophenotype analyses should be performed at the initial diagnosis
and in suspicion of relapse.
For patients with a relapsed APL an equal sample collection is also recommended.
A detailed diagnostic examination schedule is below‐mentioned.
Page 25 of 32
Diagnosis/
or suspicion of relapse
during induction
day 28/ prior cons. 1
prior cons. 2 prior cons. 3prior cons. 4(if appropr.)
after last cons.
maintenance(if appropr.)
Follow‐up (1st ‐ 5th year)
Physical examination * (incl. comorbidities)
daily, including body weight * * * * * monthly
every 3 months
Blood Counts (1) *
daily during 1st
week, afterwards 3 x/week
* * * * * monthly every 3 months
BM for morphology * *(6) * * * * every 3 monthsevery 3 months
BM for molecular biology (2)
* * * * * * every 3 monthsevery 3 months
BM for cytogenetics *
BM for immunophenotyping (3)
*
Coagulation tests (4) *
daily until normalization, 2 x a week thereafter
* * * * * monthly every 3 months
Serum biochemistry (5) *
2‐3 x/ week during the first 3 weeks, then weekly until CR
* * * * * monthly every 3 months
Page 26 of 32
Diagnosis/
or suspicion of relapse
during induction
day 28/ prior cons. 1
prior cons. 2 prior cons. 3prior cons. 4(if appropr.)
after last cons.
maintenance(if appropr.)
Follow‐up (1st ‐ 5th year)
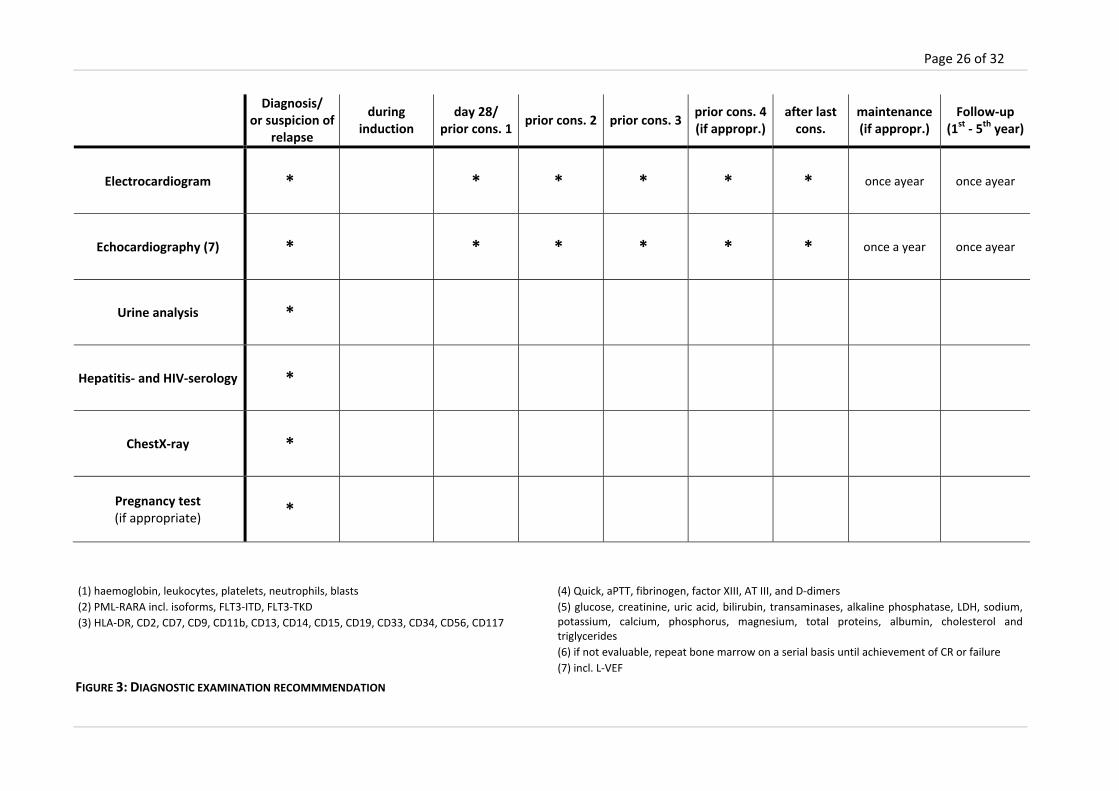
Electrocardiogram * * * * * * once ayear once ayear
Echocardiography (7) * * * * * * once a year once ayear
Urine analysis *
Hepatitis‐ and HIV‐serology *
ChestX‐ray *
Pregnancy test (if appropriate)
*
(1) haemoglobin, leukocytes, platelets, neutrophils, blasts
(2) PML‐RARA incl. isoforms, FLT3‐ITD, FLT3‐TKD
(3) HLA‐DR, CD2, CD7, CD9, CD11b, CD13, CD14, CD15, CD19, CD33, CD34, CD56, CD117
(4) Quick, aPTT, fibrinogen, factor XIII, AT III, and D‐dimers
(5) glucose, creatinine, uric acid, bilirubin, transaminases, alkaline phosphatase, LDH, sodium, potassium, calcium, phosphorus, magnesium, total proteins, albumin, cholesterol and triglycerides
(6) if not evaluable, repeat bone marrow on a serial basis until achievement of CR or failure
(7) incl. L‐VEF
FIGURE 3: DIAGNOSTIC EXAMINATION RECOMMMENDATION
Page 27 of 32
5 LITERATURE Reference List
1. Tallman MS, Kwaan HC. Reassessing the Hemostatic Disorder Associated with Acute Promyelocytic Leukemia. Blood 1992;79:543‐553.
2. Thiede C, Steudel C, Mohr B et al. Analysis of FLT3‐activating mutations in 979 patients with acute myelogenous leukemia: association with FAB subtypes and identification of subgroups with poor prognosis. Blood 2002;99:4326‐4335.
3. Lo‐Coco F, Avvisati G, Vignetti M et al. Front‐line treatment of acute promyelocytic leukemia with AIDA induction followed by risk‐adapted consolidation for adults younger than 61 years: results of the AIDA‐2000 trial of the GIMEMA Group. Blood 2010;116:3171‐3179.
4. Sanz MA, Lo‐Coco F. Modern Approaches to Treating Acute Promyelocytic Leukemia. Journal of Clinical Oncology 2011;29:495‐503.
5. Sanz MA, Lo Coco F, Martin G et al. Definition of relapse risk and role of nonanthracycline drugs for consolidation in patients with acute promyelocytic leukemia: a joint study of the PETHEMA and GIMEMA cooperative groups. Blood 2000;96:1247‐1253.
6. Ades L, Sanz MA, Chevret S et al. Treatment of newly diagnosed acute promyelocytic leukemia (APL): a comparison of French‐Belgian‐Swiss and PETHEMA results. Blood 2008;111:1078‐1084.
7. Bennett JM, Catovsky D, Daniel MT et al. Proposals for Classification of Acute Leukemias. British Journal of Haematology 1976;33:451.
8. Bennett JM, Catovsky D, Daniel MT et al. Variant Form of Hypergranular Promyelocytic Leukemia‐(M3). British Journal of Haematology 1980;44:169.
9. Harris NL, Jaffe ES, Diebold J et al. World Health Organization classification of neoplastic diseases of the hematopoietic and lymphoid tissues: Report of the Clinical Advisory Committee Meeting ‐ Airlie House, Virginia, November 1997. Journal of Clinical Oncology 1999;17:3835‐3849.
10. Burnett AK, Grimwade D, Solomon E, Wheatley K, Goldstone AH. Presenting white blood cell count and kinetics of molecular remission predict prognosis in acute promyelocytic leukemia treated with all‐trans retinoic acid: Result of the randomized MRC trial. Blood 1999;93:4131‐4143.
11. Mandelli F, Diverio D, Avvisati G et al. Molecular remission in PML/RAR alpha‐positive acute promyelocytic leukemia by combined all‐trans retinoic acid and Idarubicin (AIDA) therapy. Blood 1997;90:1014‐1021.
12. Cunningham I, Gee TS, Reich LM et al. Acute Promyelocytic Leukemia ‐ Treatment Results During A Decade at Memorial Hospital. Blood 1989;73:1116‐1122.
13. Fenaux P, Pollet JP, Vandenbosschesimon L et al. Treatment of Acute Promyelocytic Leukemia ‐ A Report of 70 Cases. Leukemia & Lymphoma 1991;4:239‐248.
Page 28 of 32
14. Head DR, Kopecky KJ, Willman C, Appelbaum FR. Treatment Outcome with Chemotherapy in Acute Promyelocytic Leukemia ‐ the Southwest‐Oncology‐Group (Swog) Experience. Leukemia 1994;8:S38‐S41.
15. Rodeghiero F, Avvisati G, Castaman G, Barbui T, Mandelli F. Early Deaths and Antihemorrhagic Treatments in Acute Promyelocytic Leukemia ‐ A Gimema Retrospective Study in 268 Consecutive Patients. Blood 1990;75:2112‐2117.
16. Castaigne S, Chomienne C, Daniel MT et al. All‐Trans Retinoic Acid As A Differentiation Therapy for Acute Promyelocytic Leukemia .1. Clinical‐Results. Blood 1990;76:1704‐1709.
17. Chen ZX, Xue YQ, Zhang R et al. A Clinical and Experimental‐Study on All‐Trans Retinoic Acid‐Treated Acute Promyelocytic Leukemia Patients. Blood 1991;78:1413‐1419.
18. Chomienne C, Ballerini P, Balitrand N et al. All‐Trans Retinoic Acid in Acute Promyelocytic Leukemias .2. Invitro Studies ‐ Structure‐Function Relationship. Blood 1990;76:1710‐1717.
19. Degos L, Chomienne C, Daniel MT et al. Treatment of 1St Relapse in Acute Promyelocytic Leukemia with All‐Trans Retinoic Acid. Lancet 1990;336:1440‐1441.
20. Huang ME, Ye YC, Chen SR et al. Use of All‐Trans Retinoic Acid in the Treatment of Acute Promyelocytic Leukemia. Blood 1988;72:567‐572.
21. Warrell RP, Frankel SR, Miller WH et al. Differentiation Therapy of Acute Promyelocytic Leukemia with Tretinoin (All‐Trans‐Retinoic Acid). New England Journal of Medicine 1991;324:1385‐1393.
22. Fenaux P, Castaigne S, Chomienne C, Dombret H, Degos L. All Trans‐Retinoic Acid Treatment for Patients with Acute Promyelocytic Leukemia. Leukemia 1992;6:64‐66.
23. Frankel SR, Eardley A, Heller G et al. All‐Trans‐Retinoic Acid for Acute Promyelocytic Leukemia ‐ Results of the New‐York Study. Annals of Internal Medicine 1994;120:278‐286.
24. Frankel SR, Eardley A, Lauwers G, Weiss M, Warrell RP. The Retinoic Acid Syndrome in Acute Promyelocytic Leukemia. Annals of Internal Medicine 1992;117:292‐296.
25. Warrell RP, Maslak P, Eardley A et al. Treatment of Acute Promyelocytic Leukemia with All‐Trans‐Retinoic Acid ‐ An Update of the New‐York Experience. Leukemia 1994;8:929‐933.
26. Fenaux P, Chastang C, Chevret S et al. A randomized comparison of all transretinoic acid (ATRA) followed by chemotherapy and ATRA plus chemotherapy and the role of maintenance therapy in newly diagnosed acute promyelocytic leukemia. Blood 1999;94:1192‐1200.
27. Sanz MA. Risk‐adapted treatment of acute promyelocytic leukemia with AIDA derived regimens: The Pethema experience. Annals of Hematology 2006;85:98‐99.
28. de Botton S, Dombret H, Sanz M et al. Incidence, clinical features, and outcome of all trans‐retinoic acid syndrome in 413 cases of newly diagnosed acute promyelocytic leukemia. Blood 1998;92:2712‐2718.
Page 29 of 32
29. Fenaux P, Castaigne S, Dombret H et al. All‐Trans‐Retinoic Acid Followed by Intensive Chemotherapy Gives A High Complete Remission Rate and May Prolong Remissions in Newly Diagnosed Acute Promyelocytic Leukemia ‐ A Pilot‐Study on 26 Cases. Blood 1992;80:2176‐2181.
30. Fenaux P, Chastang C, Chomienne C, Degos L. Tretinoin with Chemotherapy in Newly‐Diagnosed Acute Promyelocytic Leukemia. Lancet 1994;343:1033.
31. Fenaux P, Ledeley MC, Castaigne S et al. Effect of All Transretinoic Acid in Newly‐Diagnosed Acute Promyelocytic Leukemia ‐ Results of A Multicenter Randomized Trial. Blood 1993;82:3241‐3249.
32. Fenaux P, Wattel E, Archimbaud E et al. Prolonged Follow‐Up Confirms That All‐Trans‐Retinoic Acid Followed by Chemotherapy Reduces the Risk of Relapse in Newly‐Diagnosed Acute Promyelocytic Leukemia. Blood 1994;84:666‐667.
33. Kanamaru A, Takemoto Y, Tanimoto M et al. All‐Trans‐Retinoic Acid for the Treatment of Newly‐Diagnosed Acute Promyelocytic Leukemia. Blood 1995;85:1202‐1206.
34. Tallman MS, Andersen JW, Schiffer CA et al. All‐trans‐retinoic acid in acute promyelocytic leukemia. New England Journal of Medicine 1997;337:1021‐1028.
35. Lengfelder E, Haferlach C, Saussele S et al. High dose ara‐C in the treatment of newly diagnosed acute promyelocytic leukemia: long‐term results of the German AMLCG. Leukemia 2009;23:2248‐2258.
36. Lengfelder E, Hanfstein B, Haferlach C et al. Outcome of elderly patients with acute promyelocytic leukemia: results of the German Acute Myeloid Leukemia Cooperative Group. Annals of Hematology 2013;92:41‐52.
37. Schlenk RF, Germing U, Hartmann F et al. High‐dose cytarabine and mitoxantrone in consolidation therapy for acute promyelocytic leukemia. Leukemia 2005;19:978‐983.
38. Sanz MA, Grimwade D, Tallman MS et al. Management of acute promyelocytic leukemia: recommendations from an expert panel on behalf of the European LeukemiaNet. Blood 2009;113:1875‐1891.
39. Lo‐Coco F, Avvisati G, Vignetti M et al. Front‐line treatment of acute promyelocytic leukemia with AIDA induction followed by risk‐adapted consolidation for adults younger than 61 years: results of the AIDA‐2000 trial of the GIMEMA Group. Blood 2010;116:3171‐3179.
40. Avvisati G, Lo‐Coco F, Paoloni FP et al. AIDA 0493 protocol for newly diagnosed acute promyelocytic leukemia: very long‐term results and role of maintenance. Blood 2011;117:4716‐4725.
41. Lo Coco F, Diverio D, Avvisati G et al. Therapy of molecular relapse in acute promyelocytic leukemia. Blood 1999;94:2225‐2229.
42. Meloni G, Diverio D, Vignetti M et al. Autologous bone marrow transplantation for acute promyelocytic leukemia in second remission: Prognostic relevance of pretransplant minimal residual disease assessment by reverse‐transcription polymerase chain reaction of the PML/RAR alpha fusion gene. Blood 1997;90:1321‐1325.

Page 30 of 32
43. Sanz MA. Treatment of Acute Promyelocytic Leukemia. American Society of Hematology Education Program 2006147‐155.
44. Shen ZX, Chen GQ, Ni JH et al. Use of arsenic trioxide (As2O3) in the treatment of acute promyelocytic leukemia (APE) .2. Clinical efficacy and pharmacokinetics in relapsed patients. Blood 1997;89:3354‐3360.
45. Soignet SL, Maslak P, Wang ZG et al. Complete remission after treatment of acute promyelocytic leukemia with arsenic trioxide. New England Journal of Medicine 1998;339:1341‐1348.
46. Thomas X, Dombret H, Cordonnier C et al. Treatment of relapsing acute promyelocytic leukemia by all‐trans retinoic acid therapy followed by timed sequential chemotherapy and stem cell transplantation. Leukemia 2000;14:1006‐1013.
47. Lengfelder E, Hofmann WK, Nowak D. Impact of arsenic trioxide in the treatment of acute promyelocytic leukemia. Leukemia 2012;26:433‐442.
48. Chou WC, Dang CV. Acute promyelocytic leukemia: recent advances in therapy and molecular basis of response to arsenic therapies. Current Opinion in Hematology 2005;12:1‐6.
49. Miller WH, Schipper HM, Lee JS, Singer J, Waxman S. Mechanisms of action of arsenic trioxide. Cancer Research 2002;62:3893‐3903.
50. Roboz GJ, Dias S, Lam G et al. Arsenic trioxide induces dose‐ and time‐dependent apoptosis of endothelium and may exert an antileukemic effect via inhibition of angiogenesis. Blood 2000;96:1525‐1530.
51. Shao WL, Fanelli M, Ferrara FF et al. Arsenic trioxide as an inducer of apoptosis and loss of PML/RAR alpha protein in acute promyelocytic leukemia cells. Journal of the National Cancer Institute 1998;90:124‐133.
52. Au WY, Lie AKW, Chim CS et al. Arsenic trioxide in comparison with chemotherapy and bone marrow transplantation for the treatment of relapsed acute promyelocytic leukaemia. Annals of Oncology 2003;14:752‐757.
53. Lazo G, Kantarjian H, Estey E et al. Use of arsenic trioxide (AS(2)O(3)) in the treatment of patients with acute promyelocytic leukemia ‐ The M. D. Anderson experience. Cancer 2003;97:2218‐2224.
54. Niu C, Yan H, Yu T et al. Studies on treatment of acute promyelocytic leukemia with arsenic trioxide: Remission induction, follow‐up, and molecular monitoring in 11 newly diagnosed and 47 relapsed acute promyelocytic leukemia patients. Blood 1999;94:3315‐3324.
55. Raffoux E, Rousselot P, Poupon J et al. Combined treatment with arsenic trioxide and all‐trans‐retinoic acid in patients with relapsed acute promyelocytic leukemia. Journal of Clinical Oncology 2003;21:2326‐2334.
56. Shigeno K, Naito K, Sahara N et al. Arsenic trioxide therapy in relapsed or refractory Japanese patients with acute promyelocytic leukemia: Updated outcomes of the phase II study and postremission therapies. International Journal of Hematology 2005;82:224‐229.
Page 31 of 32
57. Soignet SL, Frankel SR, Douer D et al. United States multicenter study of arsenic trioxide in relapsed acute promyelocytic leukemia. Journal of Clinical Oncology 2001;19:3852‐3860.
58. Zhang P, Wang SY, Hu XH. Arsenic trioxide treated 72 cases of acute promyelocytic leukemia. Chinese Journal of Hematology 1996;17:58‐62.
59. Sanz MA, Lo‐Coco F. Arsenic Trioxide. American Journal of Cancer 2006;5:183‐191.
60. Estey E, Garcia‐Manero G, Ferrajoli A et al. Use of all‐trans retinoic acid plus arsenic trioxide as an alternative to chemotherapy in untreated acute promyelocytic leukemia. Blood 2006;107:3469‐3473.
61. George B, Mathews V, Poonkuzhali B et al. Treatment of children with newly diagnosed acute promyelocytic leukemia with arsenic trioxide: a single center experience. Leukemia 2004;18:1587‐1590.
62. Ghavamzadeh A, Alimoghaddam K, Ghaffari SH et al. Treatment of acute promyelocytic leukemia with arsenic trioxide without ATRA and/or chemotherapy. Annals of Oncology 2006;17:131‐134.
63. Shen ZX, Shi ZZ, Fang J et al. All‐trans retinoic acid/AS(2)O(3) combination yields a high quality remission and survival in newly diagnosed acute promyelocytic leukemia. Proceedings of the National Academy of Sciences of the United States of America 2004;101:5328‐5335.
64. Mathews V, George B, Lakshmi KM et al. Single‐agent arsenic trioxide in the treatment of newly diagnosed acute promyelocytic leukemia: durable remissions with minimal toxicity. Blood 2006;107:2627‐2632.
65. Lo‐Coco F, Avvisati G, Vignetti M et al. Retinoic Acid and Arsenic Trioxide for Acute Promyelocytic Leukemia. New England Journal of Medicine 2013;369:111‐121.
66. Powell BL, Moser B, Stock W et al. Arsenic trioxide improves event‐free and overall survival for adults with acute promyelocytic leukemia: North American Leukemia Intergroup Study C9710. Blood 2010;116:3751‐3757.
67. Ghavamzadeh A, Alimoghaddam K, Rostami S et al. Phase II Study of Single‐Agent Arsenic Trioxide for the Front‐Line Therapy of Acute Promyelocytic Leukemia. Journal of Clinical Oncology 2011;29:2753‐2757.
68. Lo‐Coco F. ED in APL: tip of the iceberg? Blood 2011;118:1188‐1189.
69. Avvisati G, Buller HR, Tencate JW, Mandelli F. Tranexamic Acid for Control of Hemorrhage in Acute Promyelocytic Leukemia. Lancet 1989;2:122‐124.
70. Cheson BD, Cassileth PA, Head DR et al. Report of the National Cancer Institute‐Sponsored Workshop on Definitions of Diagnosis and Response in Acute Myeloid‐Leukemia. Journal of Clinical Oncology 1990;8:813‐819.

Page 32 of 32
Further Literature
Link, H. Akute Promyelozytenleukämie: APL; M3‐Leukämie. ONKODIN 2008
http://www.onkodin.de/zms/content/e2/e51675/e53188/e54107/index_ger.html
Lengfelder, E.; Platzbecker, U.; Niederwieser, D.; Schlenk, R. F.; Wörmann, B.
Leitlinie Akute Promyelozyten Leukämie, Dokumentenstand Februar 2012
http://www.dgho‐onkopedia.de/de/onkopedia/leitlinien/akute‐promyelozytaere‐leukaemie
European PROMYSE registry for relapsed APL http://www.leukemia‐net.org/content/leukemias/aml/apl/apl_recommendations/index_eng.html