Myocardial Ischemia: Concepts in Management Topics in Clinical Medicine February 14, 2007.
16
Myocardial Ischemia: Concepts in Management Topics in Clinical Medicine February 14, 2007
-
Upload
melinda-lynch -
Category
Documents
-
view
214 -
download
0
Transcript of Myocardial Ischemia: Concepts in Management Topics in Clinical Medicine February 14, 2007.

Myocardial Ischemia: Concepts in Management
Topics in Clinical Medicine
February 14, 2007

Familiar Concepts
• Determinants of myocardial ischemia
• Making the diagnosis – clinical and laboratory investigation
• Prognosis should determine treatment

Historical Notes
Errors in judgment must occur in the practice of an art which consists largely in balancing probabilities.
Sir William Osler, 1882
The capacity to make effective use of today’s diagnostic…technology depends in large measure on the accuracy with which the physician can perceive the dangers to the patient at that particular moment…The ability to forecast with reasonable accuracy is one of the most important things a doctor can do.
Walsh McDermott, 1982

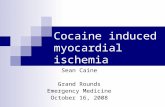
Prognosis in Chronic Ischemic Heart Disease
Severity
Time in Years
DeathTRANSITION
ZONE
STEMI
NSTEMI
UAP
SCA
AB
C

Familiar Concepts
• Determinants of myocardial ischemia
• Determinants of myocardial oxygen supply Oxygen-carrying capacity Coronary flow
• Determinants of myocardial oxygen demand Heart rate Wall tension (~ systolic pressure) Contractility

Familiar Concepts
• Determinants of myocardial ischemia• Making the diagnosis – clinical and laboratory
investigation– Typical angina (definite)
• Substernal discomfort, quality, duration
• Provoked by exertion or emotion
• Relieved by rest or TNG
– Atypical angina (probable) – 2 of above
– Non-specific chest pain – 1 or none

Pretest Likelihood of CAD
Age Men Women Men Women Men Women
30-39 4 2 34 12 76 26
40-49 13 3 51 22 87 55
50-59 20 7 65 31 93 73
60-69 27 14 72 51 94 86
Non-Specific Atypical Typical

Pretest Likelihood of CAD at Catheterization
Age Men Women Men Women Men Women
30-39 4 2 34 12 76 26
40-49 13 3 51 22 87 55
50-59 20 7 65 31 93 73
60-69 27 14 72 51 94 86
Non-Specific Atypical Typical

Familiar Concepts• Determinants of myocardial ischemia• Making the diagnosis – clinical and laboratory
investigation• Prognosis should determine treatmentDuke Treadmill Score
Time in minutes =- 5 x mm ST depression =
0 = none- 4 x angina index 1 = angina, not limiting
2 = limiting anginaTotal score =
Score Risk Group Annual Mortality
> 5 Low 0.25%
-10 to +4 Intermediate 1.25%
< -11 High 5.25%

Why do we treat angina?
• Prevent Death
• Prevent MI
• Reduce Symptoms
• ASA and Anti-anginal Therapy• Beta-blocker and Blood Pressure• Cigarette Smoking and Cholesterol• Diet and Diabetes• Education and Exercise

New Concepts
• Unusual presentations
• Acute treatment in myocardial infarction – how and where to open the artery
• Secondary prevention after myocardial infarction
• Women

MI - Secondary Prevention• BP control (<140/90; <130/80 if diabetes or renal
failure; pre-hypertension)• Lipids – LDL < 100, (optional < 70) but statin in
all; If TG 200-499 – bring non-HDL cholesterol to < 130 – fibrate** or niacin; If TG >500, use fibrate** or niacin first, then treat LDL; ** watch for myopathy – keep statin dose low
• Beta-blocker• Anti-platelet therapy – ASA 75-162 (325 x 1
month if stent); clopidogrel 75 mg/d• ACEi; ARB, esp if intolerant • Aldosterone blockade if EF <40%, DM, CHF

• Smoking Cessation
• Diet - <7% saturated fat, <200 mg cholesterol, stanol/sterol, viscous fiber, fish
• Physical Activity – 30 min 7/wk
• Weight management – waist circumference
• Diabetes control – HbA1c < 7
MI - Secondary Prevention


How to Keep Up
• Online – e.g., Harrison’s Online
• Guidelines – specialty societies– www.americanheart.org

Class IBenefit>>Risk
Treatment SHOULD be performed/administered
Class IIaBenefit>>Risk
Additional studies with focused objectives needed
IT IS REASONABLE to administer
Class IIbBenefit Risk
Additional studies with broad objectives needed;
IT IS NOT UNREASONABLE to administer treatment
Class IIIRisk Benefit
No additional studies neededProcedure/Treatment should NOT be performed/administered SINCE IT IS NOT HELPFUL AND MAY BE HARMFUL
Level A
Multiple (3-5) population risk strata evaluated*
Consistency of direction and magnitude of effect
•Recommendation that procedure or treatment is useful/effective•Sufficient evidence from multiple randomized trials or meta-analyses
•Recommendation in favor of treatment or procedure being useful/effective•Some conflicting evidence from multiple randomized trials or meta-analyses
•Recommendation's usefulness/efficacy less well established•Greater conflicting evidence from multiple randomized trials or meta-analyses
•Recommendation that procedure or treatment not useful/effective and may be harmful•Sufficient evidence from multiple randomized trials or meta-analyses
Level B
Limited (2-3)population risk strata evaluated*
•Recommendation that procedure or treatment is useful/effective•Limited evidence from single randomized trial or non-randomized studies
•Recommendation in favor of treatment or procedure being useful/effective•Some conflicting evidence from single randomized trial or non-randomized studies
•Recommendation’s usefulness/efficacy less well established•Greater conflicting evidence from single randomized trial or non-randomized studies
•Recommendation that procedure or treatment not useful.effective and may be harmful•Limited evidence from single randomized trial or non-randomized studies
Level C
Very Limited (1-2) population risk strata evaluated*
•Recommendation that procedure or treatment is useful/effective•Only expert opinion, case studies, or standard-of-care
•Recommendation in favor of treatment or procedure being useful/ effective•Only diverging expert opinion, case studies, or standard-of-care
•Recommendation’s usefulness/efficacy less well established•Only diverging expert opinion, case studies, or standard-of-care
•Recommendation that procedure or treatment not useful/effective and may be harmful•Only expert opinion, case studies, or standard-of-care
Es
tima
te of C
erta
inty
(Prec
isio
n)
of T
reatm
ent E
ffect
Classification of Recommendations and Levels of EvidenceSize of Treatment Effect