Myocardial Infarct Great Ppt!
71
Click here to load reader
-
Upload
boffin2rulez -
Category
Documents
-
view
182 -
download
9
Transcript of Myocardial Infarct Great Ppt!

"Man often becomes what he "Man often becomes what he believes himself to be.believes himself to be.
Mahatma Gandhi
1869-1948, Indian Political Leader

Pathology of Myocardial Infarction:Pathology of Myocardial Infarction:
Dr. Venkatesh M. ShashidharDr. Venkatesh M. ShashidharAssociate Professor & Head of Pathology

Coronary Coronary ArteriesArteries
•Left Coronary A.•L.Anterior Descending•Left Circumflex
•Right Coronary A.
L.CxL.Cx
LADLAD

Coronary Coronary Thrombosis With Thrombosis With InfarctionInfarction

Ischaemic Heart DiseaseIschaemic Heart Disease Etiology – Obstruction to blood flow.
– Most common - Atherosclerosis– increased demand / Obstruction– Ischemia / Infarction.
Angina – Cardiac chest pain.– Stable / Unstable / Variant
Risk factors – (atherosclerosis) – Non Modifiable: Male Sex, Age, Genetic factors. – Modifiable: Hypertension, Diabetes, Smoking, Life
style, Diet (High LDL, Low HDL).

No Q wave - Q waveNo Q wave - Q wave
Why spared?Why spared?

Coronary Atherosclerosis with Thrombosis -(MI)Coronary Atherosclerosis with Thrombosis -(MI)

Coronary AtherosclerosisCoronary Atherosclerosis

IHD Clinical Features:IHD Clinical Features: Angina Pectoris: (no infarction)
– Stable angina, common, Exercise or excitement. stable atherosclerotic narrowing of CA.
– Unstable/crescendo/Preinfarction angina Increasing pain/attacks, less effort/exercise, advanced atheroma prone to complications.
– Prinzmetal variant angina occurs at rest. spasm of coronary arteries (may not be a atheroma).
Acute Myocardial Infarction: Sudden Cardiac Death (SCD): Chronic IHD (Heart failure):

Pathogenesis:Pathogenesis: Obstruction to blood flow.
– Arteriosclerosis, Atheroma, Thrombosis, Embolism, Rupture/hemorrhage.
Diminished coronary perfusion. Ischemic cell injury Chemical mediaters
Chest Pain (Angina) Infarction – Necrosis (MI)
– Inflammation– Granulation tissue– Healing by Fibrous scarring.
Complications: – Acute: Cardiac death, conduction defects, Rupture– Late: CCF, Aneurysm, Infection.

IHD Pathogenesis:IHD Pathogenesis:
Coronary block: <70% - Asympto. >70-75% - Angina 90% - Fixed stenosis
Chronic IHD Plaque change:
– Unstable angina
– Rupture, fissure, ulcer.
> 90% - MI / SCD

Location of IHD / MILocation of IHD / MILAD: 40% to 50%
– anterior left ventricle, anterior septum, and apex circumferentially.
RCA: 30% to 40%– Posterior LV, posterior septum & RV free
wall in some.LCX (Left circumflex): 15% to 20%
– Lateral LV except the apex.
(Read clinical & ECG features for each)

Morphology - Morphology - GrossGross & & MicroscopicMicroscopicTime (approx) GROSS GROSS MICROSCOPYMICROSCOPY
Up to 4 hour None None (loss of glycogen/LDH)
4 - 24 hours Gradually developing pale centre dark mottling at periphery. Oedematous.
Beginning coagulation necrosis contraction bands. Eosinophilia, pyknotic nuclei, Oedema, acute inflammatory cells.
3-7 days Clearly visible Yellow rubbery centre with haemorrhagic border
Obvious necrosis of muscle and plenty of Neutrophils hemorrhage few macrophages & early granulation tissue.
1-3 weeks Infarcted area pale, thin yellow, red gray border. (loss of tissue mass)
Granulation tissue, macrophages prominent capillaries, fibroblasts.
3-6 weeks(permanent)
Small Silvery scar becoming tough and white
Replacement of granulation tissue by dense fibrosis

Myocardial Infarction – 3-7 dayMyocardial Infarction – 3-7 day
Pale centre
Hemorrhagic periphery

Recent MI – 3-7 day. Recent MI – 3-7 day.
Pale centre Hemorrhagic periphery
MI – Papillary M
LV
RV
Papillary Muscle

Myocardial Infarction Myocardial Infarction ? Recent ? old? Recent ? old
1-3wk - Thin wall, white,
thin hemorrhagic periphery

MI - Triphenyl Tetrazolium Cl. Stain forMI - Triphenyl Tetrazolium Cl. Stain for LDH LDH. . old MI old MI recent MI & Hemorrhagerecent MI & Hemorrhage

MI: MI: ?Clinical features,?Clinical features, ? Time, ? Artery ?ECG? Time, ? Artery ?ECG
Acute Post. Infarct: 1-3 Days. Reddish Brown
color Hemorrhagic No significant loss
of muscle mass. Mural thrombus.Complications: H.failure, Rupture,
Tamponade,
Acute- MI
Mural Thrombus
Acute- MI

?Clinical features,?Clinical features, ?Time, ?Artery ?ECG…?Time, ?Artery ?ECG…
Old MI Chronic / old: Weeks to months. Whitish grey scar. Significant loss of
muscle mass – thin wall.
No hemorrhage, thrombus, not dark..
Complications: CCF, aneurysm.

Myocardial Infarction Myocardial Infarction ? time? time
Old & Recent

Normal Myocardium:Normal Myocardium:
Capillary-RBC
My. Neucleus
IC disc

MI 18hr MI 18hr loss of nucleus, contraction bands.loss of nucleus, contraction bands.
C.Bands

MI 18-24 hr MI 18-24 hr loss of nucleus, contaction bands, loss of nucleus, contaction bands, coagulative necrosis.coagulative necrosis.

MI 1day MI 1day loss of nucleus, contraction bands, few loss of nucleus, contraction bands, few neutrophils.neutrophils.
C.Bands
Neutro

MI 2-3 day – MI 2-3 day – Marginal inflammation.Marginal inflammation.
DeadDead LiveLive

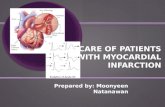
MI 1-2 dayMI 1-2 day Hemorrhage & contraction bands in reperfusion injury.Hemorrhage & contraction bands in reperfusion injury.

MI 1-2 dayMI 1-2 day Hemorrhage & contraction bands in reperfusion injury.Hemorrhage & contraction bands in reperfusion injury.
MI with reperfusion. A Gross and B microscopy: Following streptokinase therapy. (triphenyl tetrazolium chloride-stained transverse section; posterior wall at top.) B, Myocardial necrosis with hemorrhage and contraction bands, visible as hypereosinophilic bands spanning myofibers (arrow).

MI 1-3 day – MI 1-3 day – Plenty of Neutrophils.Plenty of Neutrophils.

MI 1-3 wk – MI 1-3 wk – Granulation tissue, capillaries.Granulation tissue, capillaries.

MI 3-6wk - MI 3-6wk - Scar, inflam, outer viable myocardiumScar, inflam, outer viable myocardium
Live My.Scar.

MI >6-Years - MI >6-Years - Collagen Scar no inflammation.Collagen Scar no inflammation.

Morphology - Morphology - GrossGross & & MicroscopicMicroscopicTime (approx) GROSS GROSS MICROSCOPYMICROSCOPY
Up to 4 hour None None (loss of glycogen)
4 - 24 hours Gradually developing pale centre dark mottling at periphery. Oedematous.
Beginning coagulation necrosis contraction bands. Eosinophilia, pyknotic nuclei, Oedema, acute inflammatory cells.
3-7 days Clearly visible Yellow rubbery centre with haemorrhagic border
Obvious necrosis of muscle and plenty of Neutrophils hemorrhage few macrophages & early granulation tissue.
1-3 weeks Infarcted area pale, thin yellow, red gray border. (loss of tissue mass)
Granulation tissue, macrophages prominent capillaries, fibroblasts.
3-6 weeks(permanent)
Small Silvery scar becoming tough and white
Replacement of granulation tissue by dense fibrosis

Complications: Complications: 75% cases.75% cases.
Acute Complications: Dysfunction, Arrhythmias, Extension of infarction, or
re-infarction Congestive heart failure
(pulm edema) Cardiogenic shock Pericarditis Mural thrombosis, -
embolization Myocardial wall rupture,
tamponade (3-7days) Papillary muscle rupture
Chronic Complications: Ventricular aneurysm CCF – cardiac failure. Mural thrombosis Papillary muscle contraction
– Mitral regurgitation.

Complications of MI:Complications of MI:
A Anterior myocardial rupture . B Rupture ventricular septum C Rupture papillary muscle. D Fibrinous pericarditis (dark, rough) E Thinning and mural thrombus. F aneurysm

MI - RuptureMI - Rupture

MI – 3 days MI – 3 days ? diagnosis? diagnosis

MI – MI – Papillary muscle RupturePapillary muscle Rupture

MI - AneurysmMI - Aneurysm Non contractile Reduced stroke vol. Mural thrombi

Old MI – Ventricular AneurysmOld MI – Ventricular Aneurysm
Aneurysm

Old MI – Ventricular AneurysmOld MI – Ventricular Aneurysm
After an infarct, stretching of collagenous scar causing aneurysmal bulging of the ventricular wall (V).

MI – MI – Rupture & TamponadeRupture & Tamponade

CASE STUDY: 40y diabetic woman - chest pain. P/H Hypertension, 30 pack-year
smoking history. She is on antihypertensives and Statins Had several years ago uncomplicated, myocardial infarct. She had had angina for many years, averaging one bout of angina a
month. Her usual angina lasted 10-15 minutes and was relieved by nitroglycerine. Angioplasty several years ago relieved her symptoms for six months, but eventually exercise-induced angina returned. There were no clinical changes until two weeks prior to her emergency room admission, when she began having daily anginal attacks that lasted 30 minutes or more. In the hour prior to her admission, she had awakened with severe chest pain, nausea, and dyspnea. There had been severe unrelenting pain for 45 minutes, and it had not been relieved by nitroglycerine. Vital signs: HR 105, BP 100/50 (her usual BP was about 155/95), temp. 100 F. She was obese and diaphoretic �(sweating profusely) with pale skin and labored respirations. Rales were heard over both lung fields. An EKG and serial cardiac markers were ordered.
QUESTIONS: ? Differential Diagnosis, ? Further investigations, ? Prognosis, ?
Pathology of Coronary Art. & Myocardium ? Type of Infarct, ? Complications (short term & long term) ? Advice.

"Slow down and enjoy life. It's not only "Slow down and enjoy life. It's not only the scenery you miss by going too fast, you the scenery you miss by going too fast, you also miss the sense of where you are going also miss the sense of where you are going and why."and why."Eddie Cantor1892-1964, Comedian

What is the diagnosis?What is the diagnosis?
1 2 3 4 5
2
14
0
32
1. Acute MI2. Old healed MI3. Atherosclerotic IHD4. Acute on chronic MI5. Bacterial carditis (SBE)

56y, fatigue, Heart - 56y, fatigue, Heart - ? Diagnosis? Diagnosis
A. B. C. D. E.
4 4
9
2
3
A. Acute on Chronic MIB. Atherosclerosis & MI.C. Acute MI only.D. Old MI + aneurysmE. Old MI + rupture.

MI treated, Myocardial Biopsy: Diagnosis?MI treated, Myocardial Biopsy: Diagnosis?
1 2 3 4 5
54
1
10
0
1. Acute MI – 1day. 2. Old MI - 6 wk + Hemorrhage.3. Acute on Chronic MI4. Acute MI + Reperfusion.5. MI 1-3 weeks.

17y male found in cardiac arrest following blow to chest while playing football. Spontaneous recovery following defibrillation. Paramedic ECG strop at the site showed ventricular fibrillation. On arrival at ER X-ray chest & ECG showed no abnormality, Cardiac markers high normal cardiac troponin-1. What is the most likely diagnosis?
1 2 3 4 5
54
1
10
0
1. Hypertrophic cardiomyopathy.2. Myocardial infarction.3. Prinzmetal angina.4. Commotio cordis.5. Long-QT Syndrome.

What is the diagnosis?What is the diagnosis?
1 2 3 4 5
2
14
11
3
1. Healed MI with aneurysm.2. Acute MI with mural
thrombus3. Acute Mi with aneurysm.4. Acute on chronic MI5. Acute MI with bacterial
Infection.

52y chest pain, post mortem Heart 52y chest pain, post mortem Heart (paper arrow) (paper arrow) what is the most likely Cause of death?what is the most likely Cause of death?
1 2 3 4 5
7
1 1
5
7
A. Cardiac tamponadeB. Acute MIC. Ventricular aneurysmD. Mitral incompetenceE. Thromboembolism

Myocardial Biopsy: MI duration?Myocardial Biopsy: MI duration?
1 2 3 4 5
0
4
0
6
11
1. < 4 hours 2. 4-24 hours3. 1-3 days4. 1-3 weeks.5. > 3 weeks.

Myocardial Biopsy: MI duration?Myocardial Biopsy: MI duration?
1 2 3 4 5
1
7
0
2
12
1. < 4 hours 2. 4-24 hours3. 1-3 days4. 1-3 weeks.5. > 3 weeks.

Myocardial Biopsy MI duration?Myocardial Biopsy MI duration?(Blue collagen stain):(Blue collagen stain):
1 2 3 4 5
0 0
15
3
0
1. < 4 hours 2. 4-24 hours3. 1-3 days4. 1-3 weeks.5. > 3 weeks.

52year woman, worst heartburn ever experienced since 8 hours intermittent. Tired for last few days, truble taking deep breath. No pain radiation, initially relieved by antacids, but now not responding to Ranitidine and rest. Hypertension 8 years, Hyperlipidemia 3 years. P/E BP 146/90, Chest X-ray & Troponin normal, ECG 1-2mm ST depression in anterior leads. What is the most likelyosis?
1 2 3 4 5
54
1
10
0
1. Unstable angina (Prinzmetal).2. MI - STEMI3. Pulmonary Embolism.4. MI - Non-STEMI5. GERD (Hyperacidity-esophagitis).

72y M, CCF: Complication shown by arrow?72y M, CCF: Complication shown by arrow?
1 2 3 4 5
14
5
001
1. Endocardial fibrosis2. Old healed MI3. Ventricular Aneurysm4. Mitral incompetence5. Mural thrombosis

62y chronic IHD: ? complication62y chronic IHD: ? complication
1 2 3 4 5
0
15
2
0
2
1. Old Healed MI2. LV Aneurysm3. Mural thrombosis4. Acute on Chronic MI5. Cardiac tamponade.

Myocardial Biopsy: MI duration?Myocardial Biopsy: MI duration?
1 2 3 4 5
8
2
9
2
0
1. < 4 hours 2. 4-24 hours3. 1-3 days4. 1-3 weeks.5. > 3 weeks.

62y chronic CHD: ? complication62y chronic CHD: ? complication
1 2 3 4 5
1
5
8
1
5
1. Old Healed MI2. Old MI +Aneurysm+Thrombus3. Old MI + Mural thrombus4. Acute on Chronic MI5. Acute on Old MI + Thrombus.

Myocardial Biopsy: MI duration?Myocardial Biopsy: MI duration?
1 2 3 4 5
10
6
2
0
2
1. < 4 hours 2. 4-24 hours3. 1-3 days4. 1-3 weeks.5. > 3 weeks.

CPC1.1. – Learning Issues:CPC1.1. – Learning Issues: Atherosclerosis: Etiology / Risk factors, Pathogenesis. Morphology/types – dot, streak, soft, hard, c… Complications :BV / Tissue, Acute/Chronic Lipids – LDL, HDL, ratio, interpretation. Epidemiology & Research in AS*
Ishemic Heart Disease: Angina – types & pathophysiology. Clinical features – LAD, RC, LC – pathological basis. MI – etiology, pathogenesis, gross, micro (time), MI – Complications acute/chronic.

Our progress towards success Our progress towards success begins with a simple begins with a simple
fundamental question...?fundamental question...?
Where am I going...?Where am I going...?

Laboratory DiagnosisLaboratory Diagnosis

Self Study CasesSelf Study Cases & Questions: & Questions:
Nice video of Pathogenesis of Acute MI online:http://pri-med.com/PMO/Home.aspx
(Select “Pathogenesis of Acute MI” from list)

CaseCase
A 42-year-old man presents to your surgery with central chest and left shoulder pain which came on during
his weekly game of squash, lasted for about 20 minutes and was relieved by rest. He is otherwise well but
smokes 25 cigarettes a day.On examination his BP is 140/85 and
pulse rate is 65 and regular. Heart sounds are normal and lung fields are clear on auscultation.

CaseCase
You perform an ECG in your rooms which is normal apart from some LVH.
You refer the patient to the pathology lab for CK-MB and troponin I tests and send the patient home to rest
and await the results. The blood is taken three hours after the onset of pain.
Results: CK-MB = 9 (R.Range <5μg/L)Troponin I = <0.1 (R.Range <0.1μg/L)

Questions:Questions:
Is troponin useful when measured 3 hours after onset of chest pain?
What is the diagnostic utility of measuring CK-MB and troponin I levels at the same time?
What further testing would confirm or rule out an evolving myocardial infarct?
Is the measurement of troponin T likely to provide better diagnostic information?

Case 2:Case 2:
A 58-year-old woman visits your surgery at 7pm with a history of three episodes of chest pain during the day. The first occurred at 8am after her morning swim, and lasted about an hour. The second occurred soon after lunch lasting 30 minutes, and the third episode came on during a walk after dinner and is continuing, although not as severe as initially.
She has no history of chest pain and is otherwise well.

Case 2:Case 2:
Physical examination is unremarkable and the ECG shows ST depression of 1-2mm in the anterior leads.
You call an ambulance and send her to the emergency department.
In the emergency department the ECG is repeated and is unchanged.
Blood is sent to the lab for troponin I level which is reported as 0.6μg/L(Reference Interval = <0.1μg/L)

Questions:Questions:
Is this a significant rise in troponin I or a borderline insignificant result?
Does the troponin I level confirm MI?How should this patient be
investigated?

Case 3:Case 3:
A 35-year-old man presents to your surgery with a two-day history of malaise, fever and intermittent chest pain. He is a non-smoker with no other significant medical history.
The chest pain is described as sharp and pleuritic and is worse on lying flat. He does not complain of dyspnoea, but has felt very tired and lethargic in the past few days and has not been able to exercise as usual.
On examination he is febrile at 37.5°C, BP=105/55, PR= 95/minute and regular. There is a soft early

Case 3:Case 3: systolic murmur at the left sternal edge which you
think is a flow murmur. No added sounds are heard and the lung fields are clear.
An ECG reveals widespread T-wave inversion with poor R-wave progression over the chest leads.
You arrange for the patient to be transported to the nearest emergency department where blood is drawn for troponin and C-reactive protein (CRP) levels.
Results Troponin I = 0.9 (Reference Interval = <0.1μg/L)
CRP = 28 (Reference Interval = 0-3mg/L)

Questions:Questions:
How do you interpret these results in the context of the clinical presentation and ECG?
What further investigations need to be done?
What is the usual indication for CRP measurement?
What other information may CRP provide that is particularly relevant to patients with coronary artery disease?