MyDentist: Making Children with Autism familiar with ... · II Mariasole Bondioli et al. autism and...
8
MyDentist: Making Children with Autism familiar with Dental Care Mariasole Bondioli 1 , Maria Claudia Buzzi 2 , Marina Buzzi 2 , Maria Rita Giuca 3 , Francesca Pardossi 3 , Susanna Pelagatti 1 , Valentina Semucci 4 , Caterina Senette 2 , Fabio Uscidda 1 , and Benedetta Vagelli 4 1 University of Pisa, Lungarno Pacinotti 43, 56124, Pisa mariasole.bondioli, [email protected], [email protected] 2 IIT-CNR, via Moruzzi 1, 56124 Pisa claudia.buzzi, marina.buzzi, [email protected] 3 Dipartimento di Patologia Chirurgica, Medica, Molecolare e dell’Area Critica, Ambulatorio di Odontoiatria Pediatrica, Ospedale Santa Chiara, Pisa [email protected] [email protected] 4 UFSMIA Pisa, ASL Nordovest, Via Garibaldi, Pisa. [email protected] [email protected] Abstract. Children with autism perceive sensory experiences differ- ently and have problems accepting unknown social contexts. In a dental care setting, there are many strong sound-visual stimuli, which are usu- ally not found in known environments such as home or school. This usually upsets a child with autism, often forcing dentists to administer an anesthetic even to perform normal dental hygiene. In recent years, technology-enhanced systems and apps have been developed to help peo- ple with autism adapt to new contexts and cope with distressing social situations. In this paper, we present a web application (MyDentist) which provides dentists, parents and children with a set of resources to teach children with autism the proper oral procedures at home and correct be- havior during dental visits. MyDentist includes multimodal games and activities to lighten children’s tension and to make them familiar with dental procedures. Games and activities can be personalized according to child’s needs and preferences. Professionals may also take and collect photos and videos during dental visits, making them accessible to parents and caregivers in the private profile of each child. Keywords: autism, web application, dental care, dental anxiety 1 Introduction Autism is a spectrum of neuro-developmental conditions that seriously compro- mise the way people communicate with and relate to other people and their ability to make sense of the world around them. In recent years, attention has been increasingly focused on the use of ICT to help people with autism in differ- ent contexts [14]. This interest is motivated by the rapidly growing prevalence of
Transcript of MyDentist: Making Children with Autism familiar with ... · II Mariasole Bondioli et al. autism and...

MyDentist: Making Children with Autismfamiliar with Dental Care
Mariasole Bondioli1, Maria Claudia Buzzi2, Marina Buzzi2, Maria Rita Giuca3,Francesca Pardossi3, Susanna Pelagatti1, Valentina Semucci4, Caterina
Senette2, Fabio Uscidda1, and Benedetta Vagelli4
1 University of Pisa, Lungarno Pacinotti 43, 56124, Pisamariasole.bondioli, [email protected], [email protected]
2 IIT-CNR, via Moruzzi 1, 56124 Pisaclaudia.buzzi, marina.buzzi, [email protected]
3 Dipartimento di Patologia Chirurgica, Medica, Molecolare e dell’Area Critica,Ambulatorio di Odontoiatria Pediatrica, Ospedale Santa Chiara, Pisa
[email protected] [email protected] UFSMIA Pisa, ASL Nordovest, Via Garibaldi, Pisa.
Abstract. Children with autism perceive sensory experiences differ-ently and have problems accepting unknown social contexts. In a dentalcare setting, there are many strong sound-visual stimuli, which are usu-ally not found in known environments such as home or school. Thisusually upsets a child with autism, often forcing dentists to administeran anesthetic even to perform normal dental hygiene. In recent years,technology-enhanced systems and apps have been developed to help peo-ple with autism adapt to new contexts and cope with distressing socialsituations. In this paper, we present a web application (MyDentist) whichprovides dentists, parents and children with a set of resources to teachchildren with autism the proper oral procedures at home and correct be-havior during dental visits. MyDentist includes multimodal games andactivities to lighten children’s tension and to make them familiar withdental procedures. Games and activities can be personalized accordingto child’s needs and preferences. Professionals may also take and collectphotos and videos during dental visits, making them accessible to parentsand caregivers in the private profile of each child.
Keywords: autism, web application, dental care, dental anxiety
1 Introduction
Autism is a spectrum of neuro-developmental conditions that seriously compro-mise the way people communicate with and relate to other people and theirability to make sense of the world around them. In recent years, attention hasbeen increasingly focused on the use of ICT to help people with autism in differ-ent contexts [14]. This interest is motivated by the rapidly growing prevalence of

II Mariasole Bondioli et al.
autism and by the positive effects of the interaction of people with autism withcomputers and predictable environments [18, 22]. In 2010, the overall prevalenceof ASD (Autistic Spectrum Disorder) measured by the network of Centers forDisease Control and Prevention in the US was 14.7 per 1000 (one in 68) childrenaged 8 years [10]. As a matter of fact, prevalence has increased by more than anorder of magnitude in the past 15 years. At present the only possible interven-tion is based on early diagnosis based on clinical observation (usually, in Italyat around age 1.5/2 years), followed by intensive treatment. Research suggeststhat behavioral programs implemented early and in an intensive manner canbe efficacious in improving cognitive, adaptive, and social–communicative out-comes in young children with ASD [24, 25]. Moreover, autism is characterized bya remarkable heterogeneity on the behavioral level, with substantial individualdifferences [28]. Dental health is a very serious issue for people with autism.In a dental care setting, there are many strong sound-visual stimulations thatare different from those in any other setting. This usually upsets a patient withautism, often forcing dentists to administer an anesthetic in order to carry outdental procedures. However, the positive attitude of people with autism regard-ing technology has been used to simplify oral care with positive results [16, 2].In this paper, we describe MyDentist, a web application designed to supportdental professionals in teaching ASD children to perform proper dental care athome and in dental clinics. The main goal is to train children with autism to takecare of their own oral hygiene and to accept the dental clinic environment andprocedures for prevention procedures, thus drastically reducing dental problems.MyDentist design is based on a three-month study involving ten children withautism, age 6-12 years (age range covering the permanent dentition process) ata public hospital in Pisa [3].The paper is organized as follows. Sec. 2 discusses the related work on experi-ences using ICT to simplify dental care in autism. The requirements emergingfrom the preliminary study are summarized in Sec. 3. Sec. 4 provides an overviewof the application and Sec. 5 concludes.
2 Related work
Several studies in literature underline the positive effects of the daily use ofcomputer-based intervention on different life aspects of ASD people [8, 21, 22,17]. Indeed, to this day, the ICT field has already been widely investigated andexploited in connection with many different educational approaches for ASDpeople. A wide set of digital tools has led to positive reactions in areas such asimproving language, encouraging vocalization and learning appropriate forms ofcommunication [4, 9, 12, 13, 15]. Moreover, many software programs have beendeveloped and tested to facilitate the intervention of therapists and teachersinvolved in the educational path of ASD children. For example, Buzzi et al. [5]presented ABCD SW, a software to support the learning of conceptual matchingabilities using Discrete Trial Training, in which the tutor may personalize eachtraining session.

My dentist III
The literature underlines the good results obtained in learning new skillsusing the video modeling technique [7, 27], augmented reality [6], software to fa-cilitate communication [19] and other different applications favoring interactionand communication between therapists, children and parents in normal or clini-cal context [1, 11] . The important results by the literature related to computerintervention used with ASD people focus on improving autonomy and properlymanage socially stressful situations [7, 20, 26, 23]. Among all the stressful situa-tions in ASD people’s daily life, dental care contexts have rarely been the targetof research intervention mediated by computer. In fact, few studies have at-tempted to explore the full potential of ICT in the domain of dental care. Isonget al. [16] conducted a randomized study with ASD children to test differentanxiety reactions to the dental intervention with or without the introductionof electronic screen media - a DVD reader and Google glass - during the visit.Isong et al. have obtained some results similar to those presented herein, butin their research they do not take into account the reproducibility of the testedapproach and moreover, they did not provide any form of personalization of thematerials. A lack of personalized tools can also be found in the study conductedby Berry [2] in which the researcher proposes a familiarization method basedon some digital tools, such as the reproduction of photos of dental clinics andstaff, and social stories to memorize the important elements of this activity, todistract the children during the dental visits. Unfortunately, even in this case,the possibility of customizing the resources offered to the child is not provided.
To sum up, a wide knowledge of the positive effects of technological interven-tions in the life of people with ASD emerges from the literature, but we identifiedlittle research in the specific field of personalized digital tools to facilitate ASDdental care. Moreover, in most cases, the interest in this domain still focusesonly on the positive results offered by a limited set of digital tools, e.g., videomodeling, without investigating other digital resources that may better involvepatients, such as cognitive games.
3 Participative requirement analysis
We analyzed the problem of using technological support to reduce anxiety andteach various dental care skills during a 3-month study involving ten children 6-12 years old, their parents/caregivers and a team of dentists at the public SantaChiara hospital in Pisa [3]. During this process, we worked with ASD therapistsin a public ASD therapy center (UFSMIA ASL NO Pisa) to select the properactivities to include in MyDentist and determine how they should appear.
In the study, the goal for each child was to learn how to perform proper oralcare at home and how to behave properly during visits at the clinic in order toundergo professional oral hygiene and dental care. The approach followed by themedical team took several visits (the number could vary depending on the child’sresponse) in which the child could explore and get used to the new environmentand to the medical staff. The visits were preceded by an informal meeting withparents/caregivers to explain the goal of the project and to understand the

IV Mariasole Bondioli et al.
special needs of each child. A questionnaire was administered to the caregivers toprofile children’ oral health, dental hygiene habits, sensory disturbances, autismcondition, etc. [3]. During the visits, the dentist (always the same in all the visitsof a given child) worked first on creating a relationship with the child, takinginto account his/her special needs and then gradually moving on to dental careprocedures.
In this process, a very important aid to reducing anxiety was the possibilityof taking pictures and videos during the visits, to be seen there or later at home.Multimedia material recorded during each visit was elaborated in interactivePDF social stories recalling the highlights of each visits. Pictures, videos andthe PDFs were made available to parents/caregivers to be used at home in orderto prepare the child for the next visit. Furthermore, the basic abilities for dentalcare at home were taught using video models and digital activities. In eachvisit, a set of suitable resources for activities reinforcing previous concepts andpreparing the child for the next visit were given to parents and caregivers tobe used at home. Some of them were general, others were personalized to meetindividual child’s needs.
The study with children with autism allowed us to better identify the mostaccepted and suitable digital tools to provide in MyDentist, and how to simplifythe children access to the digital activities, e.g. through a calendar highlightingpast and future dental visits. Furthermore, dentists helped us to improve My-Dentist usability, e.g. the creation/management of pictures and videos related toeach patient and the production of PDF stories that is automatically performedthrough simple guided steps. Additional information on the three-month studycarried out to evaluate if and how using technological support to reduce anxietyand teach dental care skills in ASD children can be found in [3].
4 MyDentist: a web application
MyDentist app is a dynamic Rich Internet Application based on distributed Webarchitecture. Specifically, it is coded in PHP, AJAX and HTML5 and relies ona MySQL database. All the software’s functions are implemented using jQueryand JSON libraries, which enable the creation of abstractions for low-level in-teraction, advanced effects and high-level widgets. The AJAX technology allowsthe efficient and easy exchange of data, so the HTML5 client user interfacesare constantly updated. MyDentist works as a big repository, a ”toolkit” wherematerials are arranged in two main sets: one set includes pre-packaged generalmaterials available for all the children as needed; the other set includes each pa-tient’s materials (dynamically created) containing multimedia collected duringeach visit and classified by visit date.MyDentist provides pre-defined games but also a game-engine that allows to eas-ily create three types of new games using personal resources (photos and images):sequences, puzzles, memories. The game-engine may be used autonomously bythe caregiver with minimal effort through simple wizards.
My dentist V
Two access profiles are available: one for the dentist’s use and the other forchildren and parents. The main tasks of the dentist profile are:
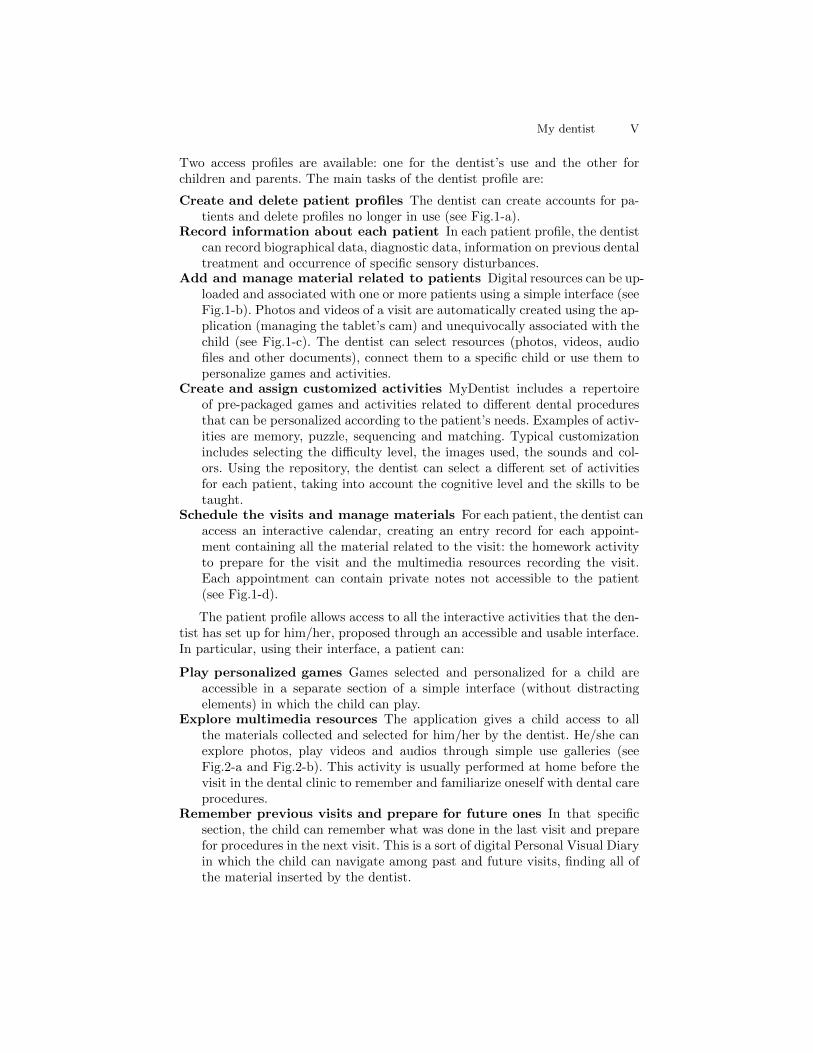
Create and delete patient profiles The dentist can create accounts for pa-tients and delete profiles no longer in use (see Fig.1-a).
Record information about each patient In each patient profile, the dentistcan record biographical data, diagnostic data, information on previous dentaltreatment and occurrence of specific sensory disturbances.
Add and manage material related to patients Digital resources can be up-loaded and associated with one or more patients using a simple interface (seeFig.1-b). Photos and videos of a visit are automatically created using the ap-plication (managing the tablet’s cam) and unequivocally associated with thechild (see Fig.1-c). The dentist can select resources (photos, videos, audiofiles and other documents), connect them to a specific child or use them topersonalize games and activities.
Create and assign customized activities MyDentist includes a repertoireof pre-packaged games and activities related to different dental proceduresthat can be personalized according to the patient’s needs. Examples of activ-ities are memory, puzzle, sequencing and matching. Typical customizationincludes selecting the difficulty level, the images used, the sounds and col-ors. Using the repository, the dentist can select a different set of activitiesfor each patient, taking into account the cognitive level and the skills to betaught.
Schedule the visits and manage materials For each patient, the dentist canaccess an interactive calendar, creating an entry record for each appoint-ment containing all the material related to the visit: the homework activityto prepare for the visit and the multimedia resources recording the visit.Each appointment can contain private notes not accessible to the patient(see Fig.1-d).
The patient profile allows access to all the interactive activities that the den-tist has set up for him/her, proposed through an accessible and usable interface.In particular, using their interface, a patient can:
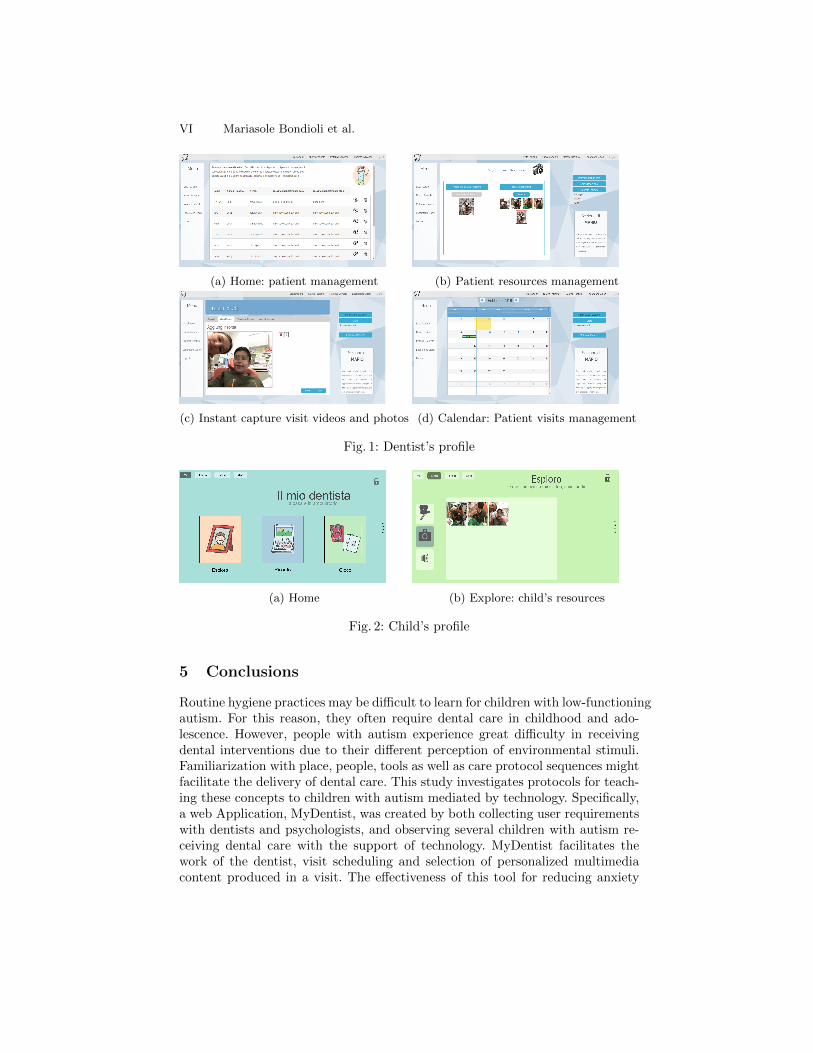
Play personalized games Games selected and personalized for a child areaccessible in a separate section of a simple interface (without distractingelements) in which the child can play.
Explore multimedia resources The application gives a child access to allthe materials collected and selected for him/her by the dentist. He/she canexplore photos, play videos and audios through simple use galleries (seeFig.2-a and Fig.2-b). This activity is usually performed at home before thevisit in the dental clinic to remember and familiarize oneself with dental careprocedures.
Remember previous visits and prepare for future ones In that specificsection, the child can remember what was done in the last visit and preparefor procedures in the next visit. This is a sort of digital Personal Visual Diaryin which the child can navigate among past and future visits, finding all ofthe material inserted by the dentist.
VI Mariasole Bondioli et al.
(a) Home: patient management (b) Patient resources management
(c) Instant capture visit videos and photos (d) Calendar: Patient visits management
Fig. 1: Dentist’s profile
(a) Home (b) Explore: child’s resources
Fig. 2: Child’s profile
5 Conclusions
Routine hygiene practices may be difficult to learn for children with low-functioningautism. For this reason, they often require dental care in childhood and ado-lescence. However, people with autism experience great difficulty in receivingdental interventions due to their different perception of environmental stimuli.Familiarization with place, people, tools as well as care protocol sequences mightfacilitate the delivery of dental care. This study investigates protocols for teach-ing these concepts to children with autism mediated by technology. Specifically,a web Application, MyDentist, was created by both collecting user requirementswith dentists and psychologists, and observing several children with autism re-ceiving dental care with the support of technology. MyDentist facilitates thework of the dentist, visit scheduling and selection of personalized multimediacontent produced in a visit. The effectiveness of this tool for reducing anxiety

My dentist VII
and stress in young patients, facilitating the dental intervention, remains to beconfirmed by objective data coming from future tests involving two sets of ASDchildren (one used as a control group). Technology can have an important role inaccessible teaching and avoiding a distressing intervention. Ambient intelligenceand Internet of Things (IoT) technologies can leverage the burden of work thatdentists face when taking care of children with autism. Future work will defineintelligent dental rooms equipped for facilitating the delivery of dental care tospecial needs patients.
References
1. K.M. Ayres, A. Maguire, and D. McClimon. Acquisition and generalization ofchained tasks taught with computer based video instruction to children withautism. Education and Training in Developmental Disabilities, pages 493–508,2009.
2. S. M. Barry. Improving access and reducing barriers to dental care for childrenwith autism spectrum disorder. PhD thesis, University of Leeds, 2012.
3. M. Bondioli, M. C. Buzzi, M. Buzzi, S. Pelagatti, and C. Senette. Ict to aid dentalcare of children with autism. In Proc. ASSETS 2017, 2017.
4. A. Bosseler and D.W. Massaro. Development and evaluation of a computer-animated tutor for vocabulary and language learning in children with autism. JAutism Dev Disord, pages 653–66, 2003.
5. M. C. Buzzi, M. Buzzi, B. Rapisarda, and M. Tesconi. Teaching low-functioningautistic children: Abcd sw. EC-TEL, 2013.
6. X. Casas, G. Herrera, I. Coma, and M. Fernandez. A kinect-based aug-mented reality system for individuals with autism spectrum disorders. In Proc.GRAPP/IVAPP, pages 440–446, 2012.
7. M. H. Charlop and J. P. Milstein. Teaching autistic children conversational speechusing video modeling. Journal of applied behavior analysis, 22(2):275–285, 1989.
8. SH1 Chen and V. Bernard-Opitz. Comparison of personal and computer-assistedinstruction for children with autism. Ment Retard., pages 368–376, 1993.
9. MB. Coleman-Martin, K. Wolff-Heller, and KL Irvine DF Cihak. Using computer-assisted instruction and the nonverbal reading approach to teach word identifica-tion. Focus Autism Other Dev Disabl, page 80?90, 2005.
10. Centers For Disease Control and Prevention (CDC). Prevalence of autism spectrumdisorder among children aged 8 years – autism and developmental disabilities mon-itoring network, 11 sites, unites states, 2010. MMWR Surveill summ, 63(2):1–21,March 2014.
11. M. Costa, A. Costa, V. Julian, and P. Novais. A task recommendation system forchildren and youth with autism spectrum disorder. pages 87–94, 2008.
12. M. Davis, K. Dautenhahn, C. Nehaniv, and S. Powell. Touch story: towards aninteractive learning environment for helping children with autism to understandnarrative. Designing accessible technology, page 785?792, 2005.
13. S. Faja, E. Aylward, R. Bernier, and G. Dawson. Becoming a face expert: acomputerized face-training program for high-functioning individuals with autismspectrum disorders. Dev Neuropsychol, pages 1–24, 2008.
14. T. R. Goldsmith and L. A. LeBlanc. Use of technology in interventions for childrenwith autism. Journal of Early and Intensive Behavior Intervention, 2004.
VIII Mariasole Bondioli et al.
15. J. Hailpern, K. Karahalios, and Jn. Halle. Creating a spoken impact: encouragingvocalization through audio visual feedback in children with asd. Proceedings ofCHI, pages 453–462, 2009.
16. I. A. Isong, S. R. Rao, C. Holifield, D. Iannuzzi, E. Hanson, J. Ware, and L. P.Nelson. Addressing dental fear in children with autism spectrum disorders: arandomized controlled pilot study using electronic screen media. 53(3):230–237,2014.
17. R. Jordan. Computer assisted education for individuals with autism. AutismeFrance 3rd International Conference, 1995.
18. K. M. Kapp. The gamification of learning and instruction: Game-based methodsand strategies for training and education. Pfeifer, San Francisco, CA, 2012.
19. G. De Leo and G. Leroy. Smartphones to facilitate communication and improvesocial skills of children with severe autism spectrum disorder: special educationteachers as proxies. In Proceedings of the 7th international conference on Interac-tion design and children, pages 45–48. ACM, 2008.
20. D. Moore, Y. Cheng, P. McGrath, and N.J. Powell. Collaborative virtual environ-ment technology for people with autism. Focus on autism and other developmentaldisabilitie, 20(4):231–243, 2005.
21. M. Moore and S. Calvert. Brief report: Vocabulary acquisition for children withautism: Teacher or computer instruction. Journal of Autism and DevelopmentalDisorders, 2000.
22. D. Murray. Autism and information technology: therapy with computers. InS. Powell and R. Jordan, editors, Autism and learning: a guide to good practice.,pages 100—-117. David Fulton, London, 1997.
23. L.M. Passerino and L.M.C. Santarosa. Autism and digital learning environments:Processes of interaction and mediation. Computers & Education, 51(1):385–402,2008.
24. D. Reichow. Overview. J. Autism Dev. Disor., 2011.25. S. Rogers and K. Wallace. Intervention for infants and toddlers with autism spec-
trum disorders. In D.G. amaral, G Dawson, and D.H. Geschwind, editors, AutismSpectrum Disorders, pages 1081–1094. Oxford University Press, New York, 2011.
26. M.L. Da Silva, D. Goncalves, T. Guerreiro, and H. Silva. A web-based applicationto address individual interests of children with autism spectrum disorders. ProcediaComputer Science, 14:20–27, 2012.
27. L. Tereshko, R. MacDonald, and W.H. Ahearn. Strategies for teaching childrenwith autism to imitate response chains using video modeling. Research in AutismSpectrum Disorders, 4(3):479–489, 2010.
28. G. Vivanti, M. Prior, K. Williams, and C. Dissanayake. Predictors of outcomes inautism early intervention: why don’t we know more? Frontiers in Pediatrics, 2,2015.