Musculoskeletal MRI. Goals ► What types of MR studies are available for evaluation of the...
81
Musculoskeletal Musculoskeletal MRI MRI
-
Upload
amanda-pierce -
Category
Documents
-
view
214 -
download
0
Transcript of Musculoskeletal MRI. Goals ► What types of MR studies are available for evaluation of the...

Musculoskeletal MRI Musculoskeletal MRI
GoalsGoals
►What types of MR studies are available What types of MR studies are available for evaluation of the musculoskeletal for evaluation of the musculoskeletal system?system?
►Considerations when ordering a studyConsiderations when ordering a study Remember one of the roles of the radiologist Remember one of the roles of the radiologist
is as consultant to work with you in is as consultant to work with you in determining the best study for the patient’s determining the best study for the patient’s needs (it’s in the job description)… talk to needs (it’s in the job description)… talk to them!them!
►Most common pathologies for which MSK Most common pathologies for which MSK MRI is performedMRI is performed

Exam TypesExam Types
►MRI without contrastMRI without contrast Most commonMost common Evaluation of ligaments, tendons, occult Evaluation of ligaments, tendons, occult
fracture, cartilagefracture, cartilage►MRI with contrastMRI with contrast
Evaluation of bone or soft tissue tumor, Evaluation of bone or soft tissue tumor, osteomyelitis, abscessosteomyelitis, abscess
►MR ArthrogramMR Arthrogram Evaluation of labrum, intercarpal Evaluation of labrum, intercarpal
ligamentsligaments
Body PartBody Part
►When ordering any study must have a ddx When ordering any study must have a ddx in mind, particularly with MRI (not a in mind, particularly with MRI (not a screening tool) screening tool)
►Cannot perform an MRI of a whole Cannot perform an MRI of a whole extremity (time, pt motion, protocol issues) extremity (time, pt motion, protocol issues)
►Must identify part to be imaged – be Must identify part to be imaged – be specificspecific A joint, a bone (prox, mid, distal), a muscle A joint, a bone (prox, mid, distal), a muscle
(origin, belly, insertion)(origin, belly, insertion)►Must have plain radiographMust have plain radiograph

Most Common IndicationsMost Common Indications
► Occult fx or stress fxOccult fx or stress fx► Early osteonecrosis – in pt with risk factors & pain, Early osteonecrosis – in pt with risk factors & pain,
known AVN of one hipknown AVN of one hip► Osteomyelitis – plain film is insensitive Osteomyelitis – plain film is insensitive (30-50% loss of bone (30-50% loss of bone
density) density) BUT necessary for MRI interpretation, nucs has BUT necessary for MRI interpretation, nucs has poor resolutionpoor resolution
► Osteochondral lesion – evaluate stabilityOsteochondral lesion – evaluate stability► Ligament/tendon injury – knee, shoulder, ankle > Ligament/tendon injury – knee, shoulder, ankle >
other jtsother jts► Bone tumor – MUST HAVE X-RAY 1Bone tumor – MUST HAVE X-RAY 1stst, imperative in , imperative in
providing ddx on MRI (dx on x-ray, determine extent providing ddx on MRI (dx on x-ray, determine extent on MR)on MR)
► Soft tissue mass/muscle injurySoft tissue mass/muscle injury

Considerations when ordering Considerations when ordering an MRIan MRI
► Joint replacement in joint of interest – don’t do itJoint replacement in joint of interest – don’t do it► Pacemaker – don’t do itPacemaker – don’t do it► Claustrophobia - sedationClaustrophobia - sedation► Unable to hold still/follow instructions – sedationUnable to hold still/follow instructions – sedation► Metal in area of interest (susceptibility artifact) – Metal in area of interest (susceptibility artifact) –
consult radiologist, may vary technique or consult radiologist, may vary technique or recommend another study recommend another study
► Metal not in area of interest ie. orbits (motion, Metal not in area of interest ie. orbits (motion, overheating)overheating)
► If you only remember one thing, remember this:If you only remember one thing, remember this: cannot do a PE protocol chest CT without contrastcannot do a PE protocol chest CT without contrast

Metal ArtifactMetal Artifact
Small metal foreign body results in large area of signal void.
Metal or gas = black hole.

General PrinciplesGeneral Principles
►Fluid, edema, inflammation is bright on T2Fluid, edema, inflammation is bright on T2►Fat is bright on T1 & T2 (can have fat sat)Fat is bright on T1 & T2 (can have fat sat)►Blood is often bright on T1Blood is often bright on T1►Tendons & ligaments are black on all Tendons & ligaments are black on all
sequencessequences►Cartilage is bright on T2Cartilage is bright on T2►Muscle is intermediate in signalMuscle is intermediate in signal

Pelvis & Hip – Normal Pelvis & Hip – Normal AnatomyAnatomy
► Joints – sacroiliac, pubic symphysis, hipsJoints – sacroiliac, pubic symphysis, hips►Tendons – iliopsoas, gluteal, hamstrings, Tendons – iliopsoas, gluteal, hamstrings,
rectus femorisrectus femoris►Bursa – trochanteric, iliopsoasBursa – trochanteric, iliopsoas►Bones – evaluate for bone marrow Bones – evaluate for bone marrow
replacing process (MM, mets), AVN, occult replacing process (MM, mets), AVN, occult or stress fxor stress fx
►Acetabular labrum – need intra-articular Acetabular labrum – need intra-articular gadoliniumgadolinium
Femoral Head OsteonecrosisFemoral Head Osteonecrosis
► Groin painGroin pain► Many predisposing factors: trauma (fem neck Many predisposing factors: trauma (fem neck
fx, dislocation), steroids, SLE, sickle cell dz, fx, dislocation), steroids, SLE, sickle cell dz, pancreatitis, alcohol abuse, Gaucher’s dzpancreatitis, alcohol abuse, Gaucher’s dz
► Increased risk of contralateral AVN, must Increased risk of contralateral AVN, must evaluate other side, most sensitive study is evaluate other side, most sensitive study is MRIMRI
► MRI:MRI: Early – bone marrow edemaEarly – bone marrow edema Later – geographic area of abnormal signal in the Later – geographic area of abnormal signal in the
anterosuperior femoral head; double line sign on T2anterosuperior femoral head; double line sign on T2 Even later – subchondral collapse, femoral head Even later – subchondral collapse, femoral head
collapse, degenerative joint dzcollapse, degenerative joint dz

Femoral Head OsteonecrosisFemoral Head Osteonecrosis

the other hip – 40% bilateralthe other hip – 40% bilateral
Anterior and superior femoral head
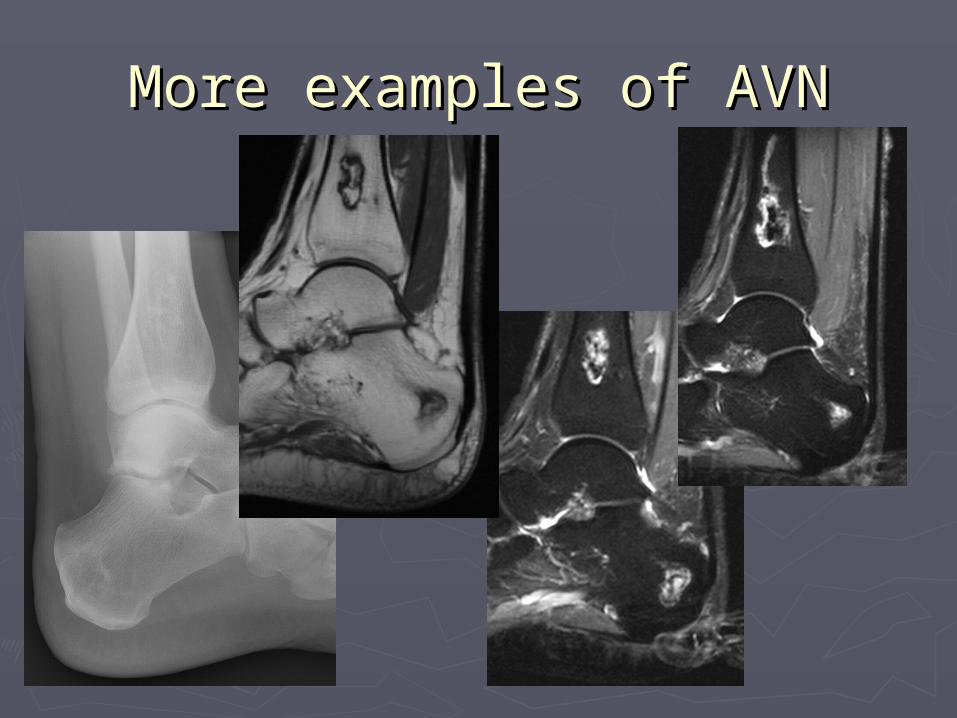
More examples of AVNMore examples of AVN

and more…and more…
Triple line sign?
Labral TearLabral Tear
► Clicking, locking, pain with pivoting/twistingClicking, locking, pain with pivoting/twisting► Traumatic (young), degenerative (older) or Traumatic (young), degenerative (older) or
assoc. with femoroacetabular impingement assoc. with femoroacetabular impingement (middle-aged)(middle-aged)
►MRI:MRI: Anterosuperior or posterosuperiorAnterosuperior or posterosuperior Linear high T2 signalLinear high T2 signal Loss of triangular morphologyLoss of triangular morphology Paralabral cystParalabral cyst
►MR arthrogram most sensitive study – MR arthrogram most sensitive study – contrast fills tearcontrast fills tear
Knee – Normal AnatomyKnee – Normal Anatomy
►Anterior & posterior cruciate ligamentsAnterior & posterior cruciate ligaments►Medial & lateral menisciMedial & lateral menisci►Medial collateral ligamentMedial collateral ligament►Lateral ligamentous complex (lateral Lateral ligamentous complex (lateral
collateral, iliotibial band, biceps collateral, iliotibial band, biceps femoris)femoris)
►Extensor mechanismExtensor mechanism►Normal variant (discoid meniscus)Normal variant (discoid meniscus)
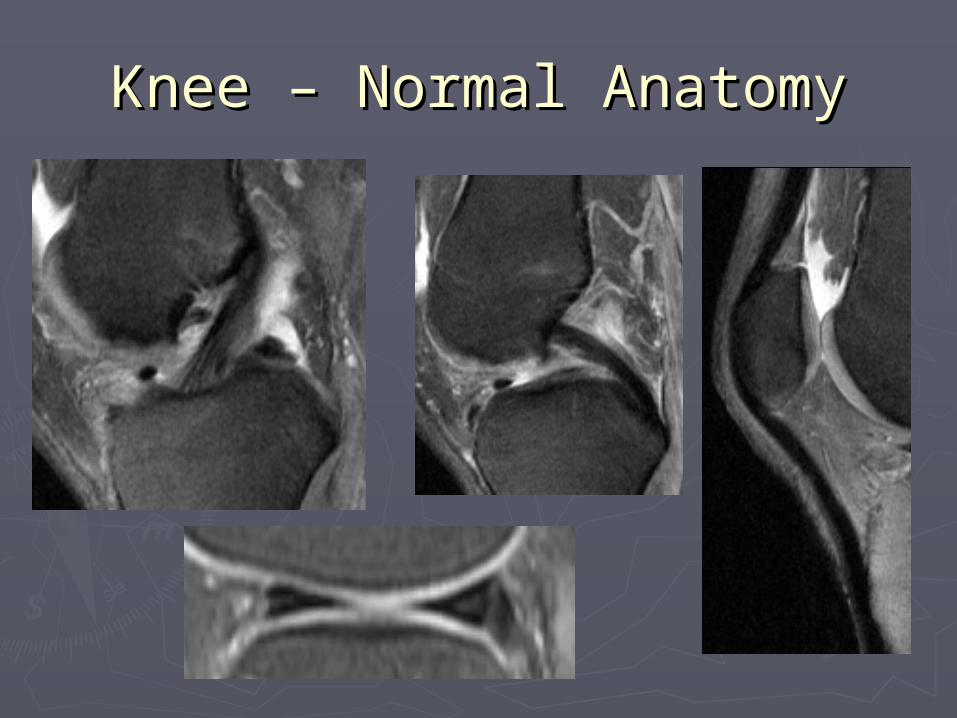
Knee – Normal AnatomyKnee – Normal Anatomy

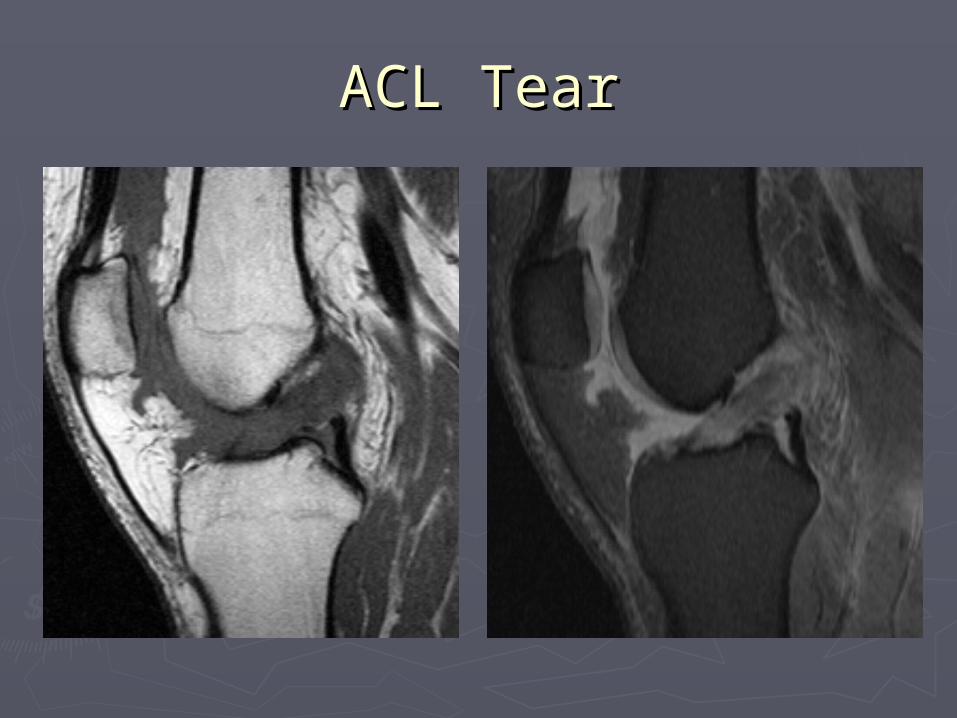
ACL TearACL Tear
► Sports injury, rapid stopping/starting/pivoting Sports injury, rapid stopping/starting/pivoting (skiing, soccor, football, basketball etc), anterior (skiing, soccor, football, basketball etc), anterior drawer sign on PEdrawer sign on PE
► MRI:MRI: Disruption of fibers, high signal on T2Disruption of fibers, high signal on T2 Pivot-shift contusionsPivot-shift contusions Anterior translation of tibia relative to femurAnterior translation of tibia relative to femur
► Associated with MCL and medial meniscus injury – Associated with MCL and medial meniscus injury – O’Donahue’s unhappy triadO’Donahue’s unhappy triad
► Associated with Segond fx (avulsion of mid third Associated with Segond fx (avulsion of mid third lateral capsular ligament from lateral tibial plateau)lateral capsular ligament from lateral tibial plateau)
ACL TearACL Tear
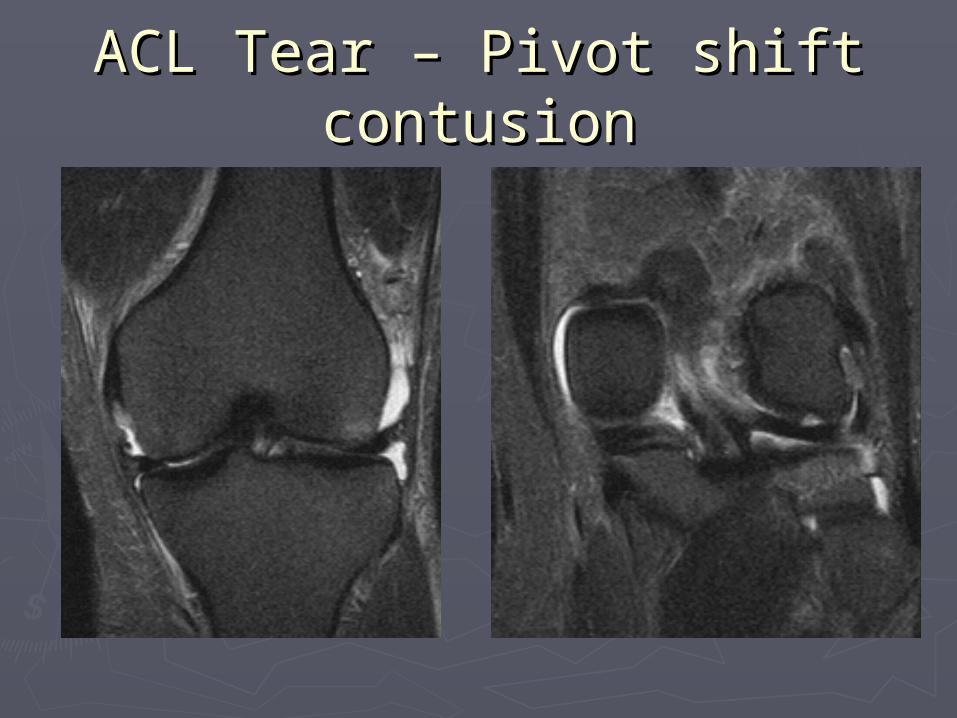
ACL Tear – Pivot shift ACL Tear – Pivot shift contusioncontusion
PCL TearPCL Tear
►Dashboard injury of flexed knee, Dashboard injury of flexed knee, posterior drawer sign on PEposterior drawer sign on PE
►MRI:MRI: Disruption of fibers/thickened fibersDisruption of fibers/thickened fibers Abnormal high T2 signalAbnormal high T2 signal Avulsion at insertion on posterior tibiaAvulsion at insertion on posterior tibia

PCL TearPCL Tear

Meniscal TearMeniscal Tear
► Joint line tenderness, Joint line tenderness, clicking, lockingclicking, locking
►MRI:MRI: High T2 signal in the High T2 signal in the
meniscus extending to meniscus extending to the articular surfacethe articular surface
longitudinal, radial, longitudinal, radial, flap (flipped), oblique, flap (flipped), oblique, bucket-handlebucket-handle
Parameniscal cystParameniscal cyst

Oblique Undersurface Tear w/ Oblique Undersurface Tear w/ Parameniscal CystParameniscal Cyst

Bucket-handle TearBucket-handle Tear
►Medial > lateralMedial > lateral►Diminutive Diminutive
meniscusmeniscus► Inner edge of Inner edge of
meniscus is meniscus is displaced medially displaced medially into notchinto notch
►Double PCL signDouble PCL sign

Bucket-handle TearBucket-handle Tear
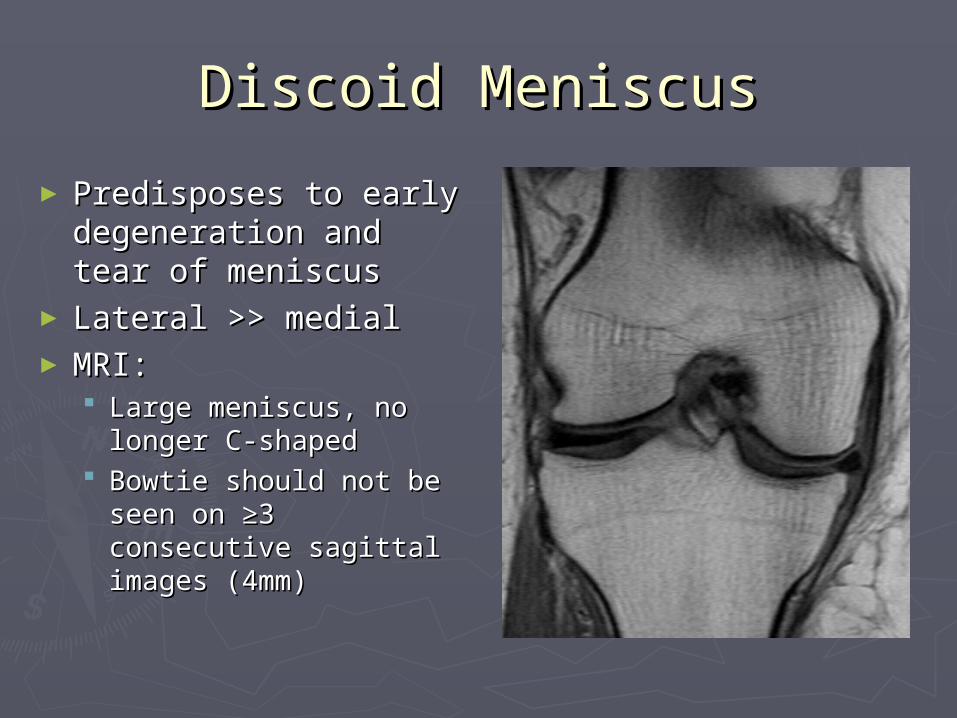
Discoid MeniscusDiscoid Meniscus
► Predisposes to early Predisposes to early degeneration and degeneration and tear of meniscustear of meniscus
► Lateral >> medialLateral >> medial► MRI:MRI:
Large meniscus, no Large meniscus, no longer C-shapedlonger C-shaped
Bowtie should not be Bowtie should not be seen on ≥3 seen on ≥3 consecutive sagittal consecutive sagittal images (4mm)images (4mm)

Discoid MeniscusDiscoid Meniscus

Medial Collateral Ligament Medial Collateral Ligament TearTear
►Valgus stressValgus stress►Complete or partial tears affecting Complete or partial tears affecting
superficial and/or deep fiberssuperficial and/or deep fibers►MRI:MRI:
Disruption of fibers with thickening & Disruption of fibers with thickening & abnormal high signalabnormal high signal
►Associated with ACL & medial meniscal Associated with ACL & medial meniscal tears tears
►Pellegrini-Stieda lesion – ossification at Pellegrini-Stieda lesion – ossification at origin of MCL indicative of old tearorigin of MCL indicative of old tear
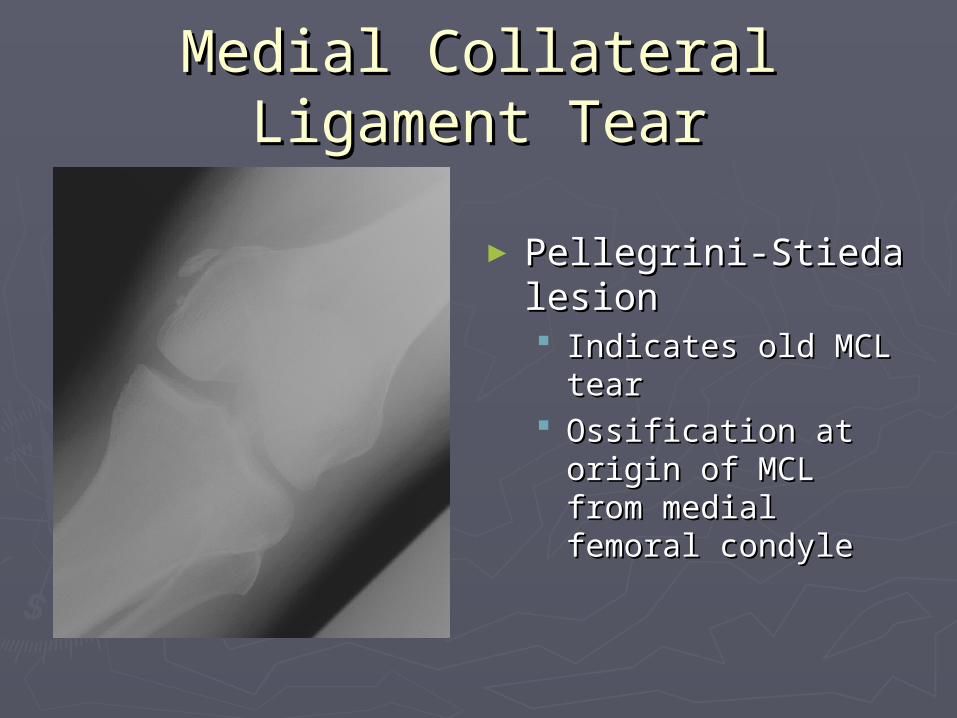
Medial Collateral Ligament Medial Collateral Ligament TearTear
► Pellegrini-Stieda Pellegrini-Stieda lesionlesion Indicates old MCL Indicates old MCL
teartear Ossification at origin Ossification at origin
of MCL from medial of MCL from medial femoral condylefemoral condyle

Acute on chronic MCL tearAcute on chronic MCL tear

Patellar Tendon TearPatellar Tendon Tear
►Partial or completePartial or complete►Most commonly in proximal third of Most commonly in proximal third of
tendon at inferior pole of patellatendon at inferior pole of patella►Plain film: Plain film:
patella altapatella alta
►MRI: MRI: Disruption of fibers, thickening & abn signalDisruption of fibers, thickening & abn signal Fluid-filled gap, hemorrage or granulation Fluid-filled gap, hemorrage or granulation
tissuetissue

Patellar Tendon TearPatellar Tendon Tear

Patellar Tendon TearPatellar Tendon Teardifferent patientdifferent patient
Jumper’s Knee Jumper’s Knee (Patellar Tendinosis)(Patellar Tendinosis)
► Repetitive traumaRepetitive trauma►MRI:MRI:
Proximal third of patellar tendon (posterior Proximal third of patellar tendon (posterior fibers)fibers)
Early – edema in peritenonEarly – edema in peritenon Later - thickening & edema (inc T2)Later - thickening & edema (inc T2) Even later – partial or complete tearEven later – partial or complete tear +/- reactive osteitis in lower pole patella (edema)+/- reactive osteitis in lower pole patella (edema) Reactive edema in adjacent fat padReactive edema in adjacent fat pad

Jumper’s KneeJumper’s Knee

Jumper’s KneeJumper’s Knee
Osteochondral LesionOsteochondral Lesion
► Young male, 50% have h/o traumaYoung male, 50% have h/o trauma► Lateral aspect of medial femoral condyle, talar Lateral aspect of medial femoral condyle, talar
dome, capitellumdome, capitellum► Plain film: area of sclerosis or bone/cartilage Plain film: area of sclerosis or bone/cartilage
fragment in situ or defect with loose body in jointfragment in situ or defect with loose body in joint► MRI necessary to determine stability and guide MRI necessary to determine stability and guide
treatment (stable-heal spontaneously, unstable-treatment (stable-heal spontaneously, unstable-surgery)surgery)
► MRI:MRI: Fragment composed of hyaline articular cartilage and Fragment composed of hyaline articular cartilage and
underlying subchondral boneunderlying subchondral bone Unstable if fluid between fragment and donor site on T2Unstable if fluid between fragment and donor site on T2

OCDOCD

OCDOCD
Ankle – Normal AnatomyAnkle – Normal Anatomy
► Joints – tibiotalar, distal tibiofibular, subtalar Joints – tibiotalar, distal tibiofibular, subtalar (ant, middle, post), intertarsal(ant, middle, post), intertarsal
► Tendons – flexor (tibialis posterior, digitorum Tendons – flexor (tibialis posterior, digitorum longus, hallucis longus), extensor (tibialis longus, hallucis longus), extensor (tibialis anterior, hallucis longus, digitorum), peroneus anterior, hallucis longus, digitorum), peroneus (longus, brevis), Achilles(longus, brevis), Achilles
► Ligaments – medial (deltoid), lateral Ligaments – medial (deltoid), lateral (talofibular, talocalcaneal), syndesmotic, Lis-(talofibular, talocalcaneal), syndesmotic, Lis-FrancFranc
►Muscles, bones, plantar fasciaMuscles, bones, plantar fascia► Normal Variants – plantaris, accessory soleusNormal Variants – plantaris, accessory soleus

Tarsal CoalitionTarsal Coalition
► Lack of segmentation of two tarsal bonesLack of segmentation of two tarsal bones► Most commonly calcaneonavicular or talocalcaneal Most commonly calcaneonavicular or talocalcaneal
(middle subtalar joint)(middle subtalar joint)► 20% bilateral; pain, flat foot20% bilateral; pain, flat foot► Cartilaginous, fibrous, osseousCartilaginous, fibrous, osseous► Plain film: anteater sign, continuous C sign, talar Plain film: anteater sign, continuous C sign, talar
beak, pes planusbeak, pes planus► MRI: MRI:
Cartilaginous, fibrous or bony bridge between 2 tarsal Cartilaginous, fibrous or bony bridge between 2 tarsal bonesbones
Fibrous/cartilaginous - JSN, irregularity, sclerosis, bone Fibrous/cartilaginous - JSN, irregularity, sclerosis, bone marrow edemamarrow edema
Bony – continuity of bone marrow and cortexBony – continuity of bone marrow and cortex
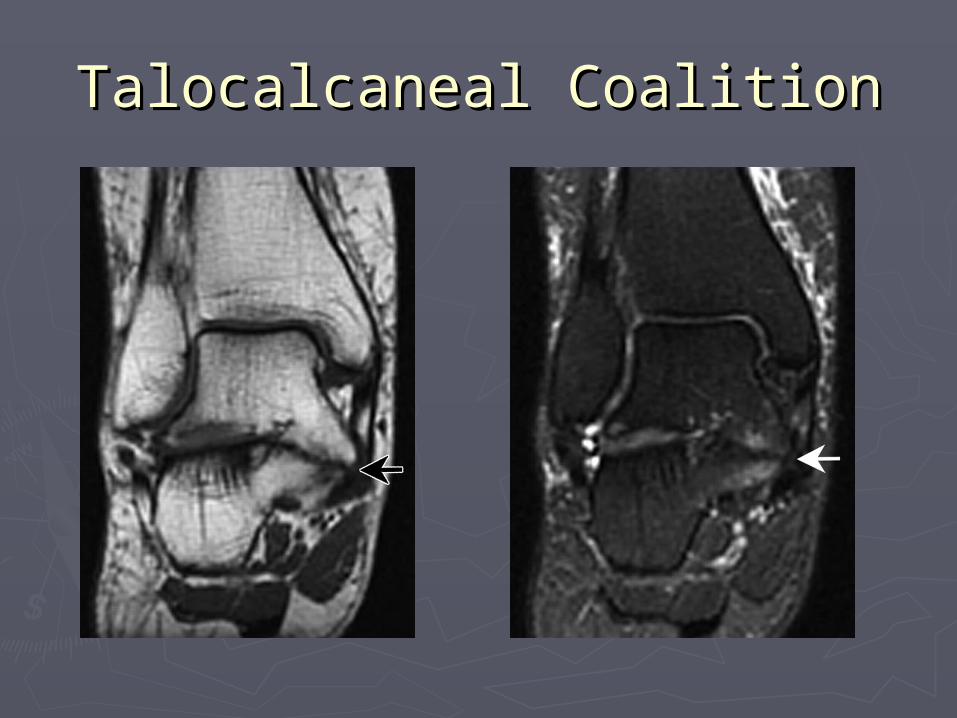
Talocalcaneal CoalitionTalocalcaneal Coalition
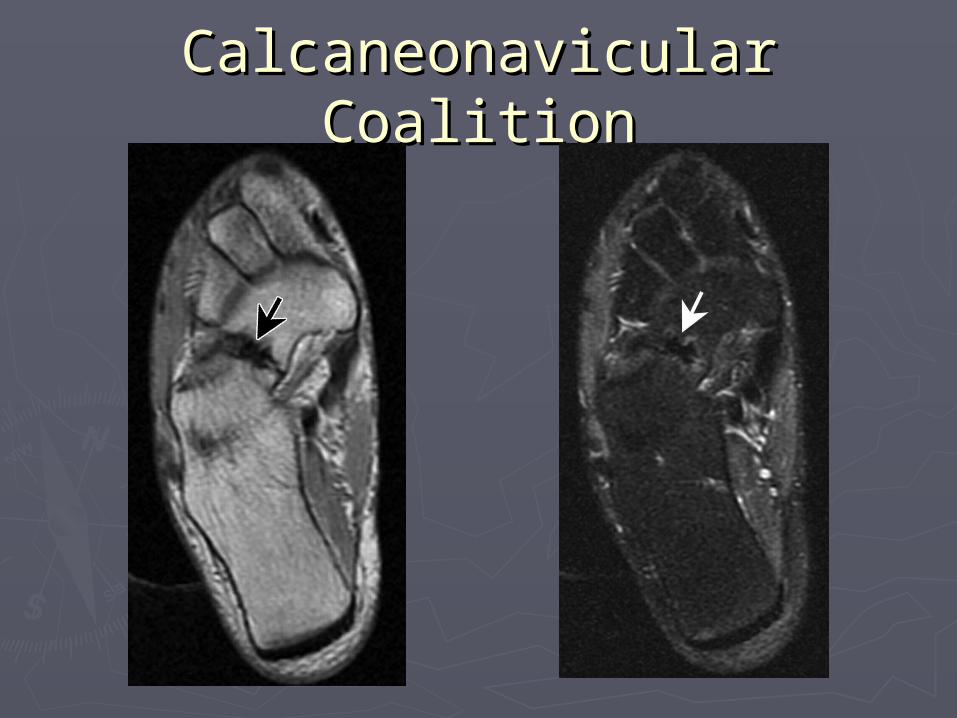
Calcaneonavicular CoalitionCalcaneonavicular Coalition

Calcaneonavicular CoalitionCalcaneonavicular Coalition

Accessory Soleus MuscleAccessory Soleus Muscle
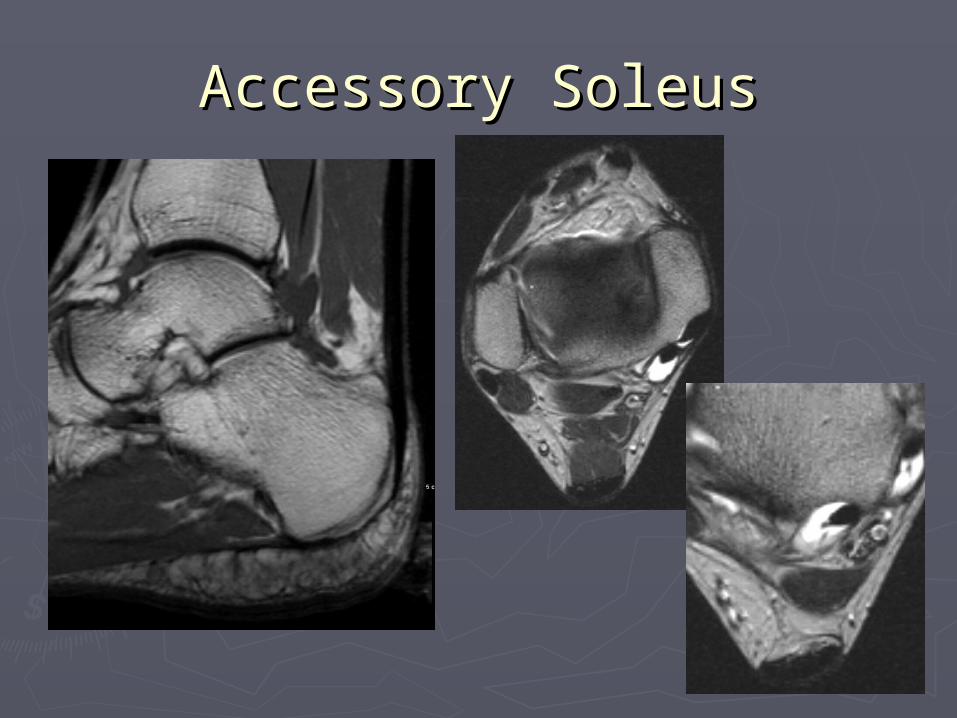
Accessory SoleusAccessory Soleus

… … and OCDand OCD
Stable or unstable?
Peroneus Brevis Split TearPeroneus Brevis Split Tear
►Peroneus brevis is normally round and Peroneus brevis is normally round and anterior to longusanterior to longus
►Tear most commonly at level of lateral Tear most commonly at level of lateral malleolusmalleolus
►MRI:MRI: C-shaped tendonC-shaped tendon Longitudinal split, peroneus longus may Longitudinal split, peroneus longus may
be interposed between two subtendonsbe interposed between two subtendons +/- fluid in tendon sheath (tenosynovitis)+/- fluid in tendon sheath (tenosynovitis)

Peroneus Brevis Split TearPeroneus Brevis Split Tear
Tom
Dick
Harry
Achilles
Peroneustendons
Talar dome

Stress FractureStress Fracture► 2 types of stress fractures:2 types of stress fractures:
1.1. Fatigue fx – normal bone under abnormal stress (young Fatigue fx – normal bone under abnormal stress (young marathon runner, military recruit etc…)marathon runner, military recruit etc…)
2.2. Insufficiency fx – abnormal bone under normal stress Insufficiency fx – abnormal bone under normal stress (elderly osteopenic female, steroids etc…)(elderly osteopenic female, steroids etc…)
► Characteristic locations: 3Characteristic locations: 3rdrd metatarsal, tibial metatarsal, tibial diaphysis, calcaneus, medial aspect femoral neck, diaphysis, calcaneus, medial aspect femoral neck, sacrumsacrum
► Plain film: Plain film: Cortical bone – periosteal rxn and/or endosteal thickeningCortical bone – periosteal rxn and/or endosteal thickening Cancellous bone - ill-defined sclerosisCancellous bone - ill-defined sclerosis
► MRI: MRI: Low signal line on T1Low signal line on T1 High signal bone marrow edema on T2High signal bone marrow edema on T2 Calcaneus – trabecular fractures perpendicular to long axisCalcaneus – trabecular fractures perpendicular to long axis

Stress FractureStress Fracture

Stress FractureStress Fracture

Stress FractureStress Fracture

Brachial Plexus – Normal Brachial Plexus – Normal AnatomyAnatomy
►Ventral nerve roots of C5, C6, C7, C8 & Ventral nerve roots of C5, C6, C7, C8 & T1T1
►Coarse between anterior & middle Coarse between anterior & middle scalene muscles, under clavicle, over scalene muscles, under clavicle, over 11stst rib, adjacent to subclavian artery rib, adjacent to subclavian artery (post & sup)(post & sup)
►Normal MRI appearance:Normal MRI appearance: Fascicles well-defined with intervening fatFascicles well-defined with intervening fat
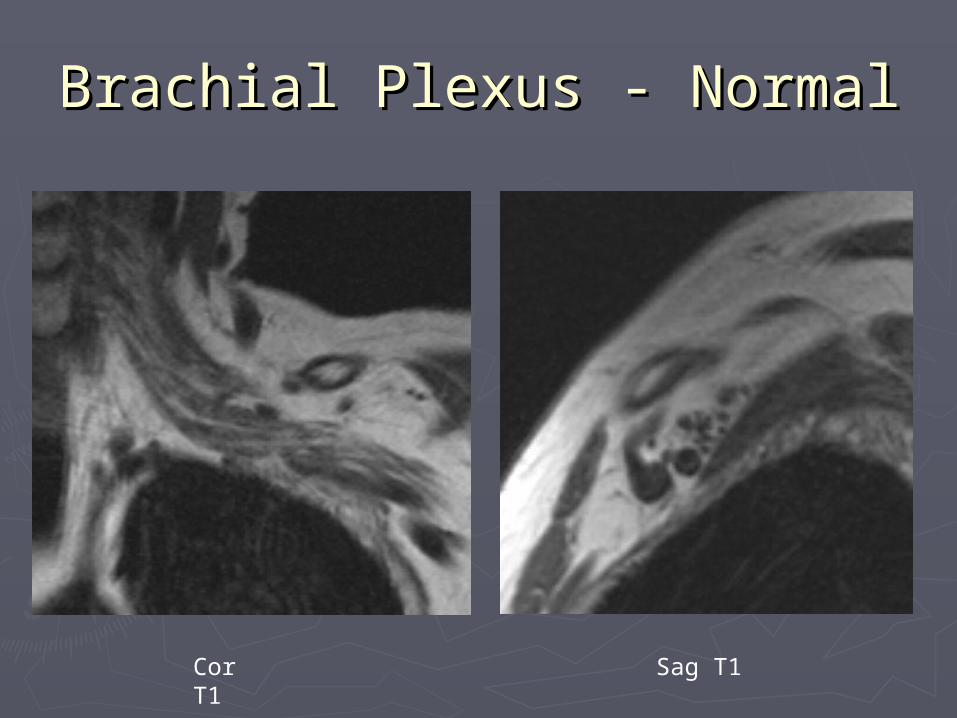
Brachial Plexus - NormalBrachial Plexus - Normal
Cor T1 Sag T1
Brachial PlexopathyBrachial Plexopathy
► Pain in the shoulder radiating down armPain in the shoulder radiating down arm► Etiologies: radiation >60 Gy(breast, lung Etiologies: radiation >60 Gy(breast, lung
ca), metastatic disease (via axillary ca), metastatic disease (via axillary lymphatics), direct invasion by tumor lymphatics), direct invasion by tumor (Pancoast’s, lymphoma), direct trauma, (Pancoast’s, lymphoma), direct trauma, stretch injurystretch injury
►MRI:MRI: Thickened fascicles with obliteration of the Thickened fascicles with obliteration of the
intervening fat planesintervening fat planes Well-defined massWell-defined mass
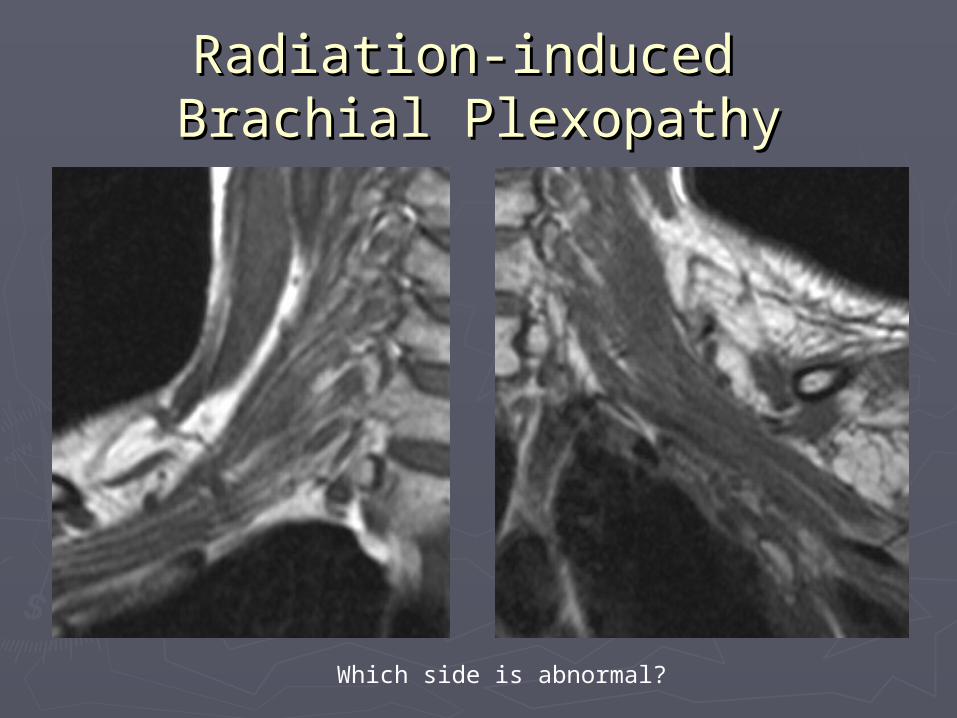
Radiation-induced Radiation-induced Brachial PlexopathyBrachial Plexopathy
Which side is abnormal?

Radiation-induced Radiation-induced Brachial PlexopathyBrachial Plexopathy
►Which number Which number corresponds to the corresponds to the brachial plexus?brachial plexus?
►What are the other What are the other 2 structures?2 structures?
Subclavian artery
Subclavian vein
1
2
3

Brachial Plexus MetastasisBrachial Plexus Metastasis
Cor & Sag T1

Brachial Plexus MetastasisBrachial Plexus Metastasis
Subclavian artery
Vein
Mass
Pre and post-contrast cor T1 with fat sat
Shoulder – Normal AnatomyShoulder – Normal Anatomy
► Rotator cuffRotator cuff► Long head of the biceps brachialis tendon – Long head of the biceps brachialis tendon –
intertubercular and intracapsular portionsintertubercular and intracapsular portions► AC joint/impingementAC joint/impingement►Glenoid labrum – triangular low signal on all Glenoid labrum – triangular low signal on all
sequences, serves to deepen glenoid fossa sequences, serves to deepen glenoid fossa thereby stabilizing GH joint, attachment site thereby stabilizing GH joint, attachment site of long head of bicepsof long head of biceps Myxoid degeneration, labral tear (alphabet soup), Myxoid degeneration, labral tear (alphabet soup),
Bankart lesionBankart lesion Best evaluated with MR arthrographyBest evaluated with MR arthrography
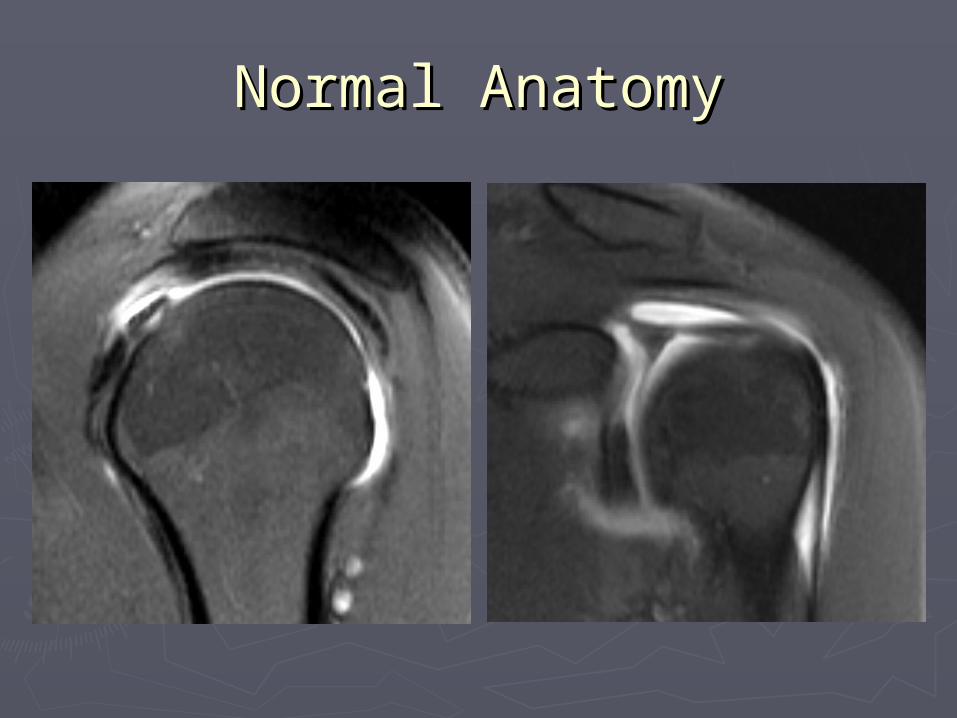
Normal AnatomyNormal Anatomy

Rotator Cuff TearRotator Cuff Tear► Supraspinatus, infraspinatus, teres minor, Supraspinatus, infraspinatus, teres minor,
subscapularissubscapularis► Pts > 40 yo, insidious onset of painPts > 40 yo, insidious onset of pain► Spectrum: tendinopathy, partial and full thickness tearSpectrum: tendinopathy, partial and full thickness tear► Etiology: degeneration (age, overuse, impingement), Etiology: degeneration (age, overuse, impingement),
trauma, collagen vascular diseasetrauma, collagen vascular disease► MRI:MRI:
Tendinopathy – thickened tendon, increased signal on PD, Tendinopathy – thickened tendon, increased signal on PD, intermed on T2intermed on T2
Partial tear – increased signal on T2, defect does not extend Partial tear – increased signal on T2, defect does not extend through cuffthrough cuff
Complete tear – increased signal defect on T2 extending Complete tear – increased signal defect on T2 extending through RC from articular surface to bursal surface; fluid in through RC from articular surface to bursal surface; fluid in subacromial/subdeltoid bursasubacromial/subdeltoid bursa
Chronic tear – muscle atrophyChronic tear – muscle atrophy
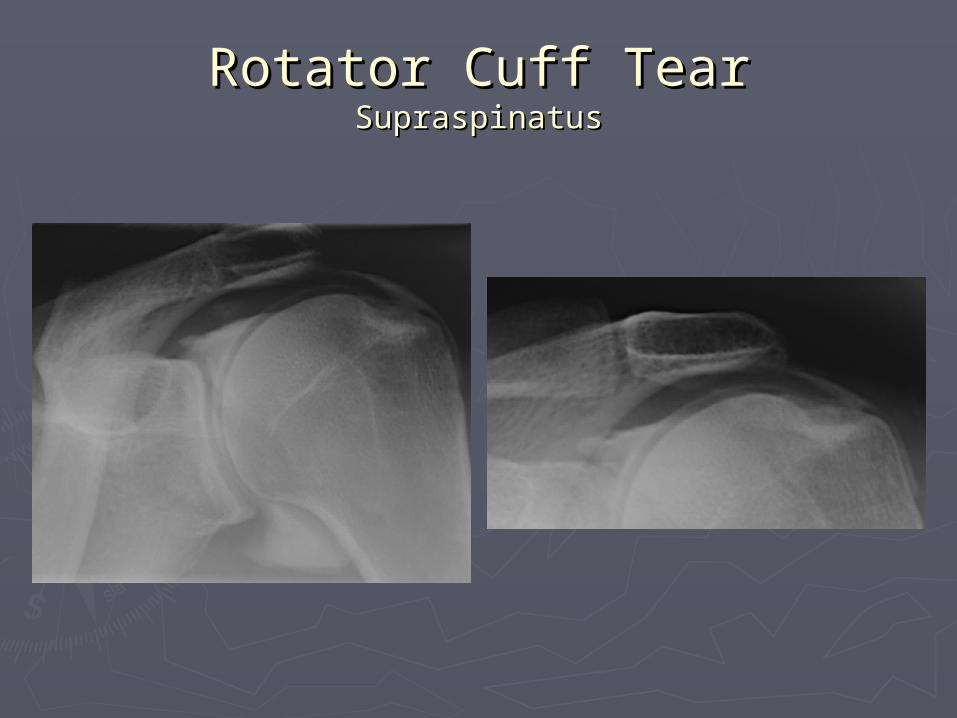
Rotator Cuff TearRotator Cuff TearSupraspinatusSupraspinatus
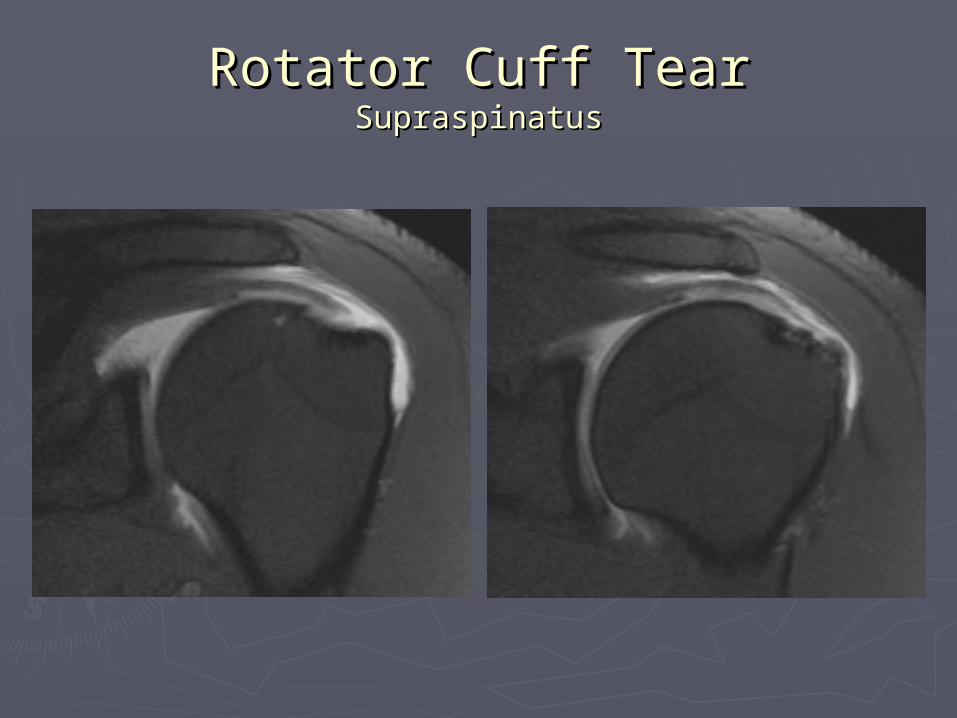
Rotator Cuff TearRotator Cuff TearSupraspinatusSupraspinatus

Supraspinatus TendinopathySupraspinatus Tendinopathy
► Underlying Underlying degenerated tendon as degenerated tendon as evidenced by evidenced by thickening and thickening and abnormal signalabnormal signal

Labral TearLabral Tear
► Young pts <40 yo, pain, instabilityYoung pts <40 yo, pain, instability► Best evaluated with MR arthrogramBest evaluated with MR arthrogram► MRI:MRI:
Linear high T2 signal within substance of labrumLinear high T2 signal within substance of labrum Diffuse high signal (crush injury)Diffuse high signal (crush injury) Absent or small labrumAbsent or small labrum Detached labrumDetached labrum
► Mimics:Mimics: Undercutting of articular cartilage between labrum and Undercutting of articular cartilage between labrum and
glenoidglenoid Interposed synovial recess (sulcus)Interposed synovial recess (sulcus) Sublabral foramen/hole (detached anterosuperior labrum)Sublabral foramen/hole (detached anterosuperior labrum)

Labral TearLabral Tear

Labral Tear?Labral Tear?
►NONO► Undercutting of Undercutting of
cartilage between cartilage between labrum & glenoidlabrum & glenoid
► Interposed synovial Interposed synovial sulcussulcus
► Contrast follows Contrast follows contour of glenoid contour of glenoid (points medially)(points medially)

Hillsach’s and Bankart Hillsach’s and Bankart LesionsLesions
►History of anterior shoulder dislocationHistory of anterior shoulder dislocation►Hillsach’s – impaction fracture of posterior Hillsach’s – impaction fracture of posterior
superior humeral head superior humeral head ► Bankart – anterior inferior labral avulsion w/ Bankart – anterior inferior labral avulsion w/
rupture of periosteum, many variants rupture of periosteum, many variants ► Bony Bankart – fracture of anterior glenoidBony Bankart – fracture of anterior glenoid►MRI:MRI:
Impaction fracture of posterosuperior humeral Impaction fracture of posterosuperior humeral head (not round on 1head (not round on 1stst three axial images) three axial images)
Anterior labral tear or variant (best evaluated Anterior labral tear or variant (best evaluated with arthrography)with arthrography)
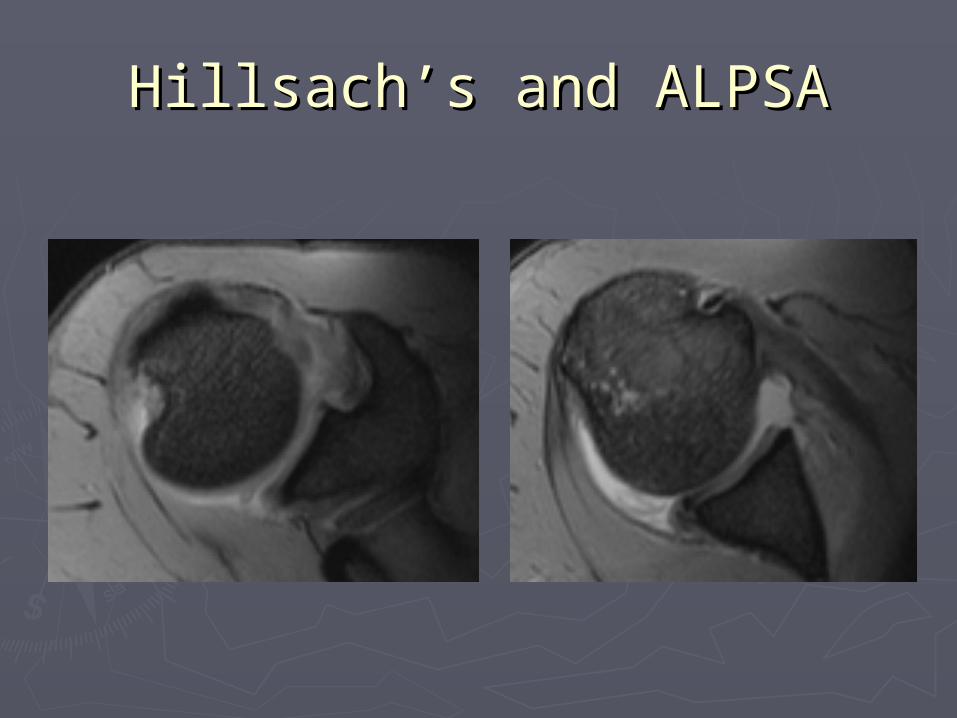
Hillsach’s and ALPSAHillsach’s and ALPSA
Elbow – Normal AnatomyElbow – Normal Anatomy
►Tendons – biceps, brachialis, triceps, Tendons – biceps, brachialis, triceps, common flexor and extensor originscommon flexor and extensor origins
►Ligaments – ulnar and radial collateralLigaments – ulnar and radial collateral► Joints – elbow, proximal radioulnarJoints – elbow, proximal radioulnar►Olecranon bursaOlecranon bursa

Olecranon BursitisOlecranon Bursitis
► Painless mass following acute direct trauma Painless mass following acute direct trauma or recurrent trauma; assoc with systemic dzor recurrent trauma; assoc with systemic dz
►Distension of olecranon bursa (synovial sac) Distension of olecranon bursa (synovial sac) with fluidwith fluid
►MRI:MRI: In superficial soft tissues adjacent to olecranon In superficial soft tissues adjacent to olecranon
process and triceps insertionprocess and triceps insertion mm – cm in sizemm – cm in size High signal on T2, possible rim enhancementHigh signal on T2, possible rim enhancement +/- hemorrhagic debris+/- hemorrhagic debris

Olecranon BursitisOlecranon Bursitis

Lateral EpicondylitisLateral Epicondylitis
► Insidious onset of lateral elbow pain with activityInsidious onset of lateral elbow pain with activity► Overuse syndrome – repetitive varus stressOveruse syndrome – repetitive varus stress► Chronic tendinopathy at common extensor Chronic tendinopathy at common extensor
origin, predominantly involving the extensor origin, predominantly involving the extensor carpi radialis brevis tendoncarpi radialis brevis tendon Partial avulsion with scar formationPartial avulsion with scar formation
► Plain film: normal or spur at lateral epicondylePlain film: normal or spur at lateral epicondyle► MRI:MRI:
Thickening of tendon with increased signal on T1 & Thickening of tendon with increased signal on T1 & T2T2
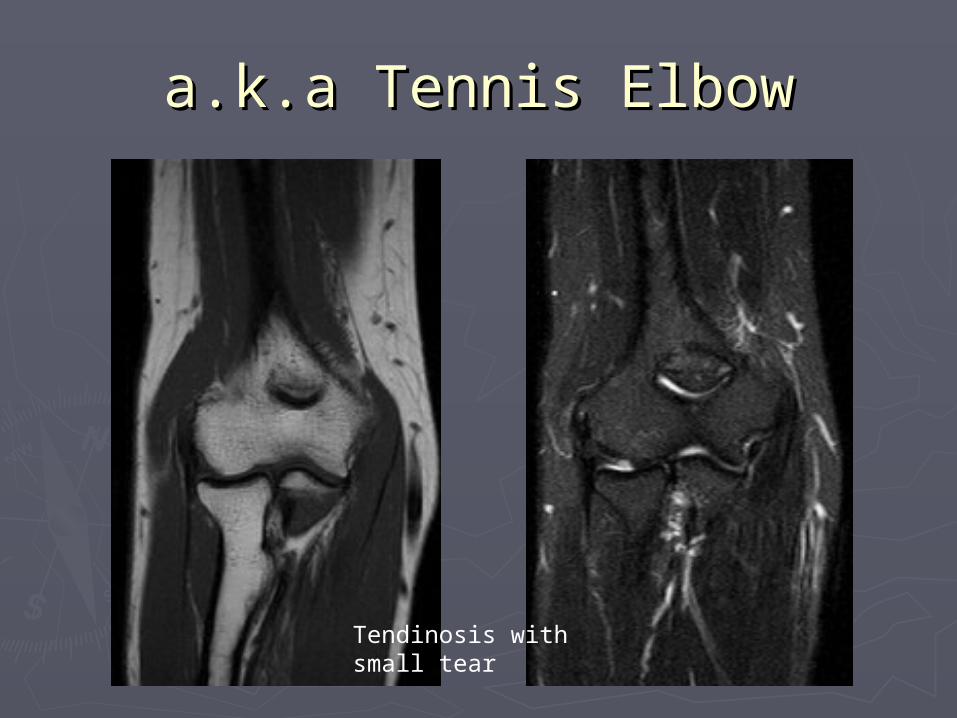
a.k.a Tennis Elbowa.k.a Tennis Elbow
Tendinosis with small tear

Lateral EpicondylitisLateral Epicondylitis
Involves both deep and superficial fibers of extensor carpi radialis longus

Wrist – Normal AnatomyWrist – Normal Anatomy
►Bones – distal radius & ulna, carpus, Bones – distal radius & ulna, carpus, MT’sMT’s
► Joints – DRUJ, radiocarpal, intercarpalJoints – DRUJ, radiocarpal, intercarpal►Tendons – flexor & extensor Tendons – flexor & extensor ►Nerves – median & ulnar Nerves – median & ulnar ►Ligaments – intercarpal (instability) Ligaments – intercarpal (instability) ►Masses – most common ganglion cystMasses – most common ganglion cyst
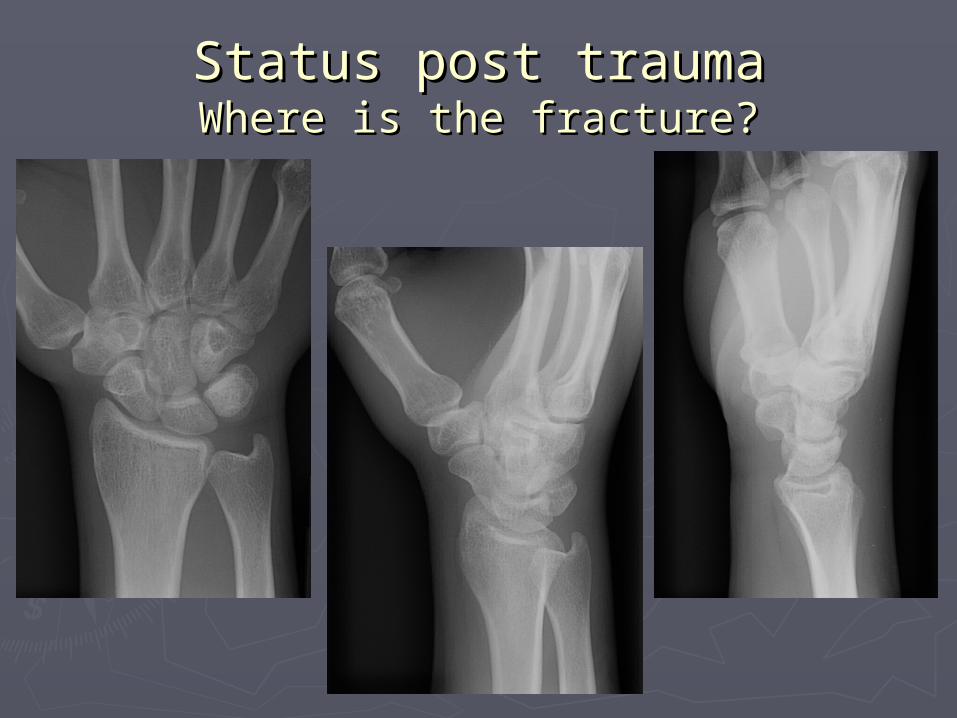
Status post traumaStatus post traumaWhere is the fracture?Where is the fracture?
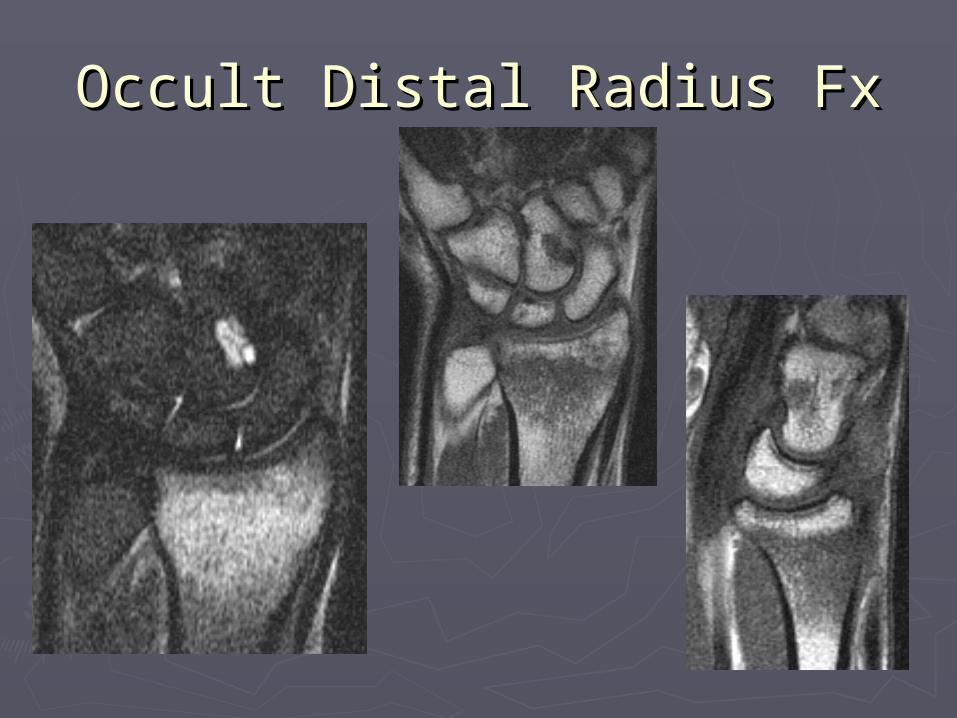
Occult Distal Radius FxOccult Distal Radius Fx