Musculoskeletal Imaging and Bone Trauma Edward Smitaman, MD Clinical Assistant Professor University...
74
Musculoskeletal Imaging and Bone Trauma Edward Smitaman, MD Clinical Assistant Professor University of California, San Diego
-
Upload
norman-campbell -
Category
Documents
-
view
216 -
download
2
Transcript of Musculoskeletal Imaging and Bone Trauma Edward Smitaman, MD Clinical Assistant Professor University...

Musculoskeletal Imaging and Bone Trauma
Edward Smitaman, MD
Clinical Assistant Professor
University of California, San Diego

Case #1
• Right hip pain, after motor vehicle accident


Fracture types

Fracture Characterization
• What you really need to notice– Alignment: Needs Reduction– Open (compound) fracture?- Needs surgery– Intra-articular Extension?
• Articular Gap/Depression
– Common associated injuries• Fracture patterns• Associated ligamentous soft tissue injury

Common Fracturesand
Fractures Associations that are Helpful to Know
Case # 2
• 22 year old male with hand pain after punching a wall

Boxer’s Fracture
• Most common type of metacarpal fracture• Must evaluate for intra-articular extension• Must evaluate for angulation and rotational
deformity- determines management• Good history/exam for soft tissue swelling can
be very helpful in picking up subtle fractures

Case # 3
• 24 year old with arm pain after fall

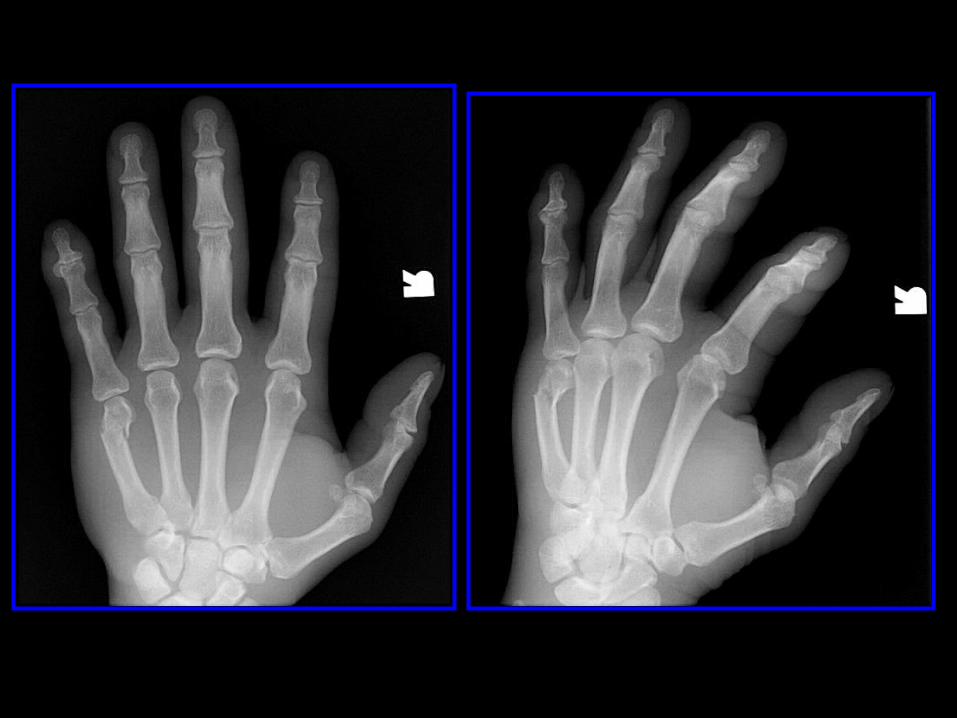
Monteggia Fracture
• Views of the entire forearm and elbow should be obtained to exclude this injury.
• The forearm acts like a bony ring (with ulna and radius fixed at each end by the radioulnar joints)
• A fracture of one bone is uncommon without a second fracture or dislocation of the proximal or distal radio-ulnar joints.

Galleazzi Fracture
Fracture of radiusWith dislocation of distal ulna
Case # 4
• 30 year old male with knee pain after playing soccer

Segond Fracture
• Avulsion fracture of lateral tibial plateau• High Association (>75%) with
– Anterior Cruciate Ligament tear– Medial Mensicus tear– Posterior Cruciate Ligament tear
• Order MRI to assess ligaments of knee and consult ORTHO


Case #4
• 20 year old tennis player with acute onset of ankle pain.


Maisonneuve fracture
• External rotation injury to ankle results in– Disruption of deltoid (medial) ankle ligaments– Disruption of interosseous membrane– Proximal fibular fracture as force exits laterally
• Always image entire tibia/fibula if concerned about ankle syndesmosis
Case #5
• Cassanova is now complaining of back pain

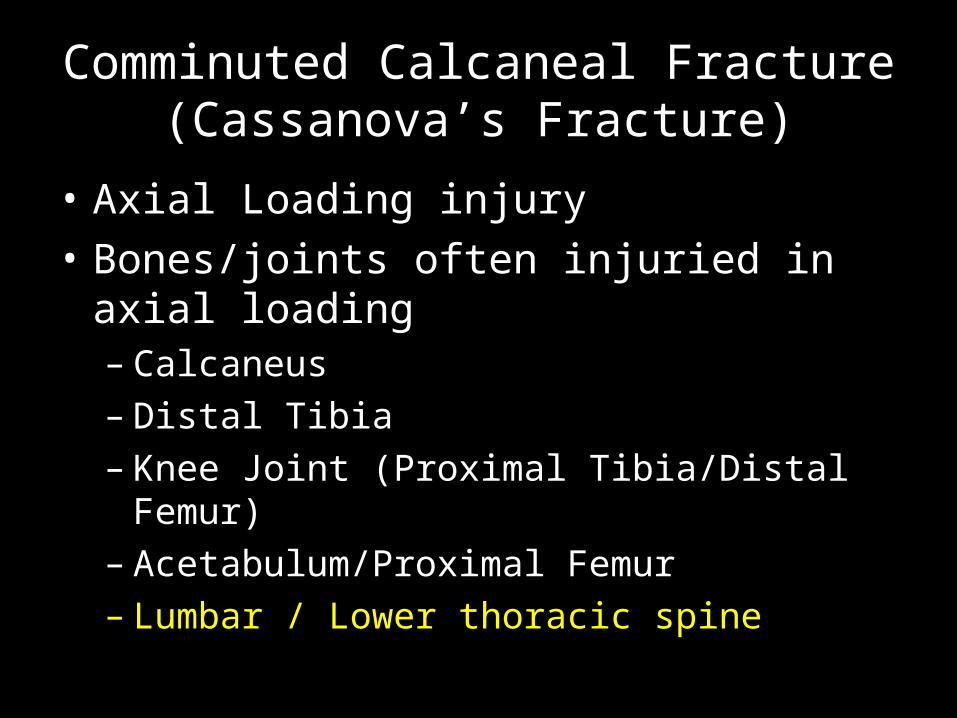
Comminuted Calcaneal Fracture (Cassanova’s Fracture)
• Axial Loading injury• Bones/joints often injuried in axial loading
– Calcaneus– Distal Tibia– Knee Joint (Proximal Tibia/Distal Femur)– Acetabulum/Proximal Femur– Lumbar / Lower thoracic spine

Anatomy

Case #6
• 24 year old male with hand pain after skiing.


Gamekeeper’s Fracture
• Avulsion fracture at insertion of ulnar colateral ligament
• Often managed conservatively (unless fracture fragment is very displaced
• Do NOT obtain stress views– Can convert this lesion into a Stenner lesion-
where adductor apponeurosis gets in the way of the UCL and prevents healing.
• IF DX in question get MRI

Findings Associated with Fractures that are Helpful to Know

Case # 7
• Elbow pain

Elbow Joint Effusion
• Highly associated with boney injury– In adults: Radial head fracture– In children: Supracondylar fracture
• May not always see fracture on initial radiographs, delayed films, CT or MR may be necessary


Case # 8
• Knee pain, status post bicycle accident

Knee Effusion with Lipohemarthrosis
• Joint effusion is non-specific– Trauma– Infection– Inflammatory disease
• Lipohemarthrosis (fat-fluid level)– Very specific for fracture or bone bruise– When present and a fracture is not seen
• Get CT or MR
Pediatric Bone Trauma
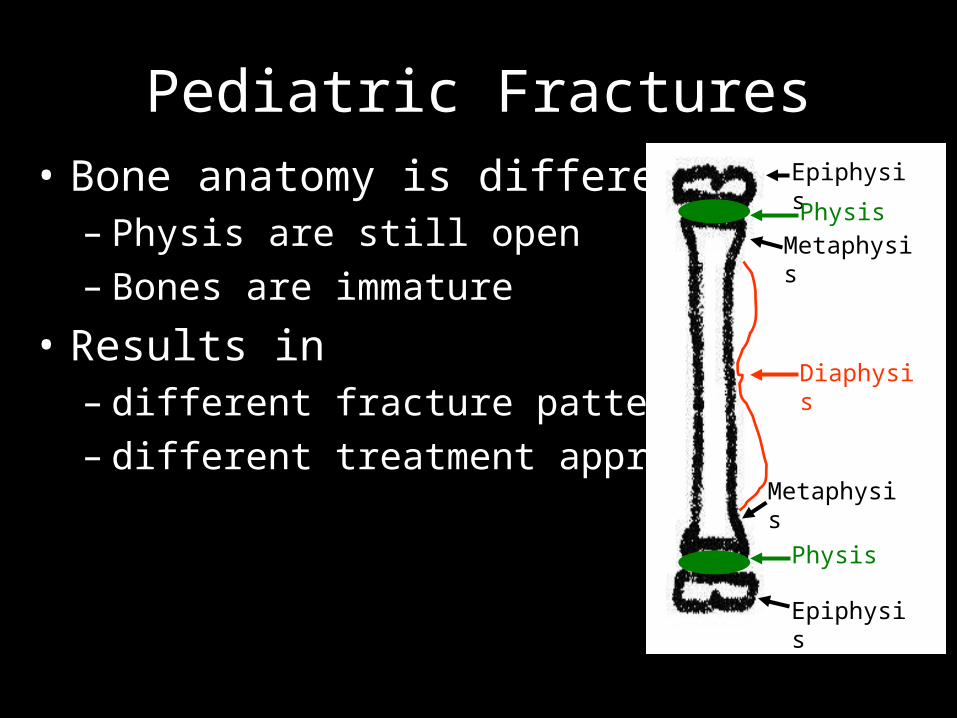
Pediatric Fractures• Bone anatomy is different
– Physis are still open– Bones are immature
• Results in – different fracture patterns – different treatment approaches
Epiphysis
Physis
Metaphysis
Diaphysis
Epiphysis
Physis
Metaphysis

Salter-Harris Physeal Fracture Classification
As Fracture type increases from 1 to 5, prognosis worsens.
Type I fractures will almost always heal with normal bone growth
Type V fracture will virtually always result in abnormal bone growth

Case # 9
• 12 year old male with wrist pain after trauma


Salter Harris Type II
• Most Common Physeal Fracture• Good Prognosis

Case # 10
• 12 year old boy with left hip pain

Hint: Skeletal ageSlipped Capital Femoral Epiphysis

SCFE
Normal Alignment

SCFE• Salter Harris Type I fracture• Presents with:
– Limp and or pain– Pain in hip/groin ~ 85%– Distal thigh or knee pain ~ 15%
• More common in boys: average 13-14 years • Gender: M:F = 2.5:1• Predisposing factors
– Obesity is currently most significant factor – Adolescent growth spurt – Endocrine disorders: Primary hypothyroidism, pituitary dysfunction, etc. – Down syndrome
• Treatment: Surgical Pinning – To prevent further slippage and resultant premature osteoarthritis

Case # 11
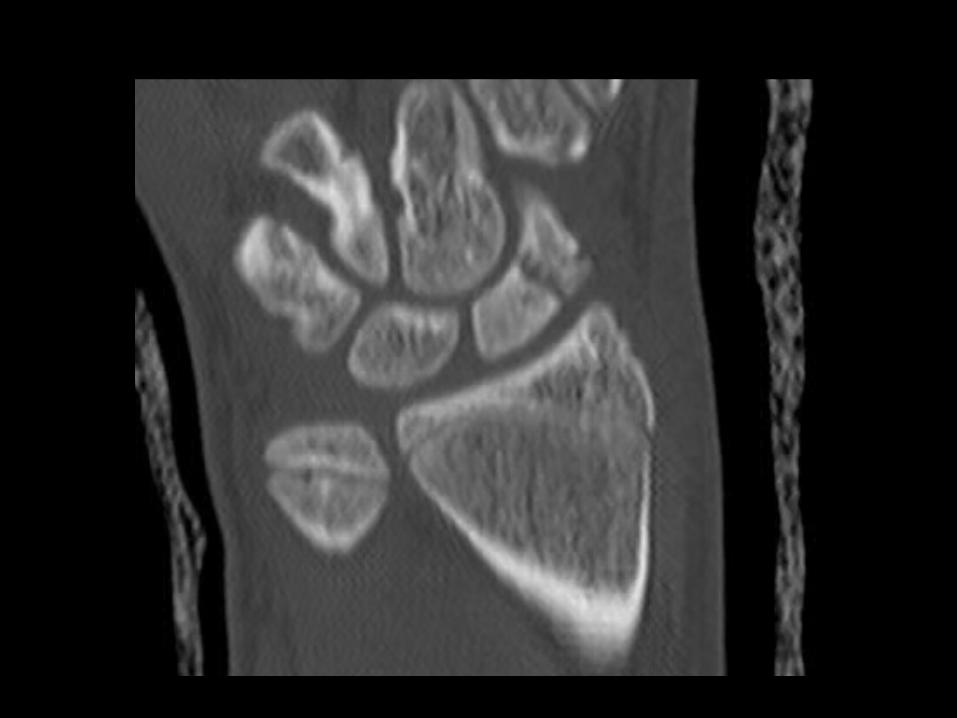
• 14 year old female with wrist pain after playing softball

Buckle Fracture Distal Radius
• A.K.A.– Torus Fracture– Incomplete Fracture
• Common in children because of immature bone strength
• Treatment – Reduction if necessary (often not)– Casting (short term ~ 3-4 wks)


Case # 12
• 15 year old male with wrist pain after falling on an outstretched hand.


Scaphoid Fracture• Transverse fx; 70% middle 1/3 of the waist• Assoc with radial styloid and triquetrial fx and scapholunate
ligament injury• 2-5% not seen on XR. Splint and reimage in 7-10 days or get
MRI• Most frequent malunion is with dorsal apex angulation• 10-15% nonunion• 15-30% develop AVN of proximal pole
– Blood supply to the scaphoid is retrograde• Tx is immobilization; ORIF if unstable or delayed nonunion

Case # 13
• 40 year-old man with knee pain after MVA



Anterior Knee Dislocation
• High impact injury (60% MVA)• Hyperextension injury with tear of posterior
structures• Posterior knee dislocation-direct blow to
proximal tibia• Need to assess for injury to the popliteal
artery-CTA or conventional angiogram• MRI to assess meniscal and ligament injury

Case # 14
• 20 year old man BIBA after MVA


Pelvic Fractures
• Pelvis is a bony ring--must break in 2 places• Superior/Inferior pubic rami• Sacroiliac joints• Open Book--pubic symphysis diastasis• Acetabular Fx


Case # 16
• 48 year-old man fell off a ladder



Odontoid Fracture
• Sudden forward or backward movement of head
• XR: lucent fx line, displacement of the anterior arch of C1, prevertebral soft tissue swelling, can see fx on open mouth view
• CT: need MPRs, axial images can miss fx• Type I: avulsion of dip of dens• Type II: transverse fx at base of dens• Type III: fx extends to body of C2

Case #17
• Left foot pain status post trauma


Lisfranc Fracture-Dislocation
• Lisfranc ligament - from anterolateral aspect of the medial cuneiform to the medial base of the 2nd MT
• Offset TMT joints• Gap at the bases of the 1st and 2nd MTs


Case # 18
• 3 year old male with acute onset of leg pain while running.