Musculoskeletal Considerations of the Rib Cage. Objectives Review of anatomy – True rib pair has...
40
Musculoskeletal Considerations of the Rib Cage
-
Upload
kallie-cantrill -
Category
Documents
-
view
216 -
download
0
Transcript of Musculoskeletal Considerations of the Rib Cage. Objectives Review of anatomy – True rib pair has...

Musculoskeletal Considerations of the Rib Cage
Objectives
• Review of anatomy– True rib pair has 10 joints.
• Discuss common structural dysfunction which can cause pain with breathing.
• Discuss cardiopulmonary dysfunction which can cause mechanical dysfunction within the rib cage.

RIB SOMATIC DYSFUNCTION
• Rib dysfunctions are grouped into two categories:– Respiratory rib dysfunctions
• Happens during breathing
– Structural rib dysfunctions• Happens with rib itself or with movement.
• Treat thoracic spine for rotational dysfunctions in extension or flexion before treating the rib dysfunctions– Thoracic spine fixes rib issues commonly
PRINCIPLES OF DIAGNOSIS• After you assess the thoracic contour and evaluate
symmetry/asymmetry:– Symmetry, humps with flexion, breathing, rib mobility, springing on
ribs, measuring volume.– Rule of three: T1-T3 rib at level of transver, T3: ½ below
T10: whole level, T11: ½ level, T12:
-Evaluate the rib angle, should gradually move laterally
• With the patient supine, push on the lateral aspect of the ribs.
• Resistance to this pushing force indicates rib restriction.

PRINCIPLES OF DIAGNOSIS
• You can evaluate rib motion without the patient actively breathing.
• Simply passively move the ribs into exhalation and inhalation.
• Remember: “Down in front, up in back” (flexion) for exhalation and “Up in front, down in back” for inhalation (extension).
• Palpate posteriorly for tenderness/tissue change at the rib angle.
• Palpate anteriorly; look for anterior counterstrain points.

MECHANICAL CONSIDERATIONS
On inhalation, the thoracic A-P curve flattens, on exhalation it increases. 1. An extended thoracic area should be associated with inhalation dysfunction in ribs. 2. A flexed thoracic area should be associated
with exhalation dysfunction in ribs.3. Sometimes, an atypical pattern rib dysfunction
exists with reversal of the pattern.

Diaphragm
• Manual muscle test of the diaphragm– Push belly up, and we then give resistance to push
it back in.• When breathing is compromised, then the
diaphram forgets its posture role, and focuses just on breathing.
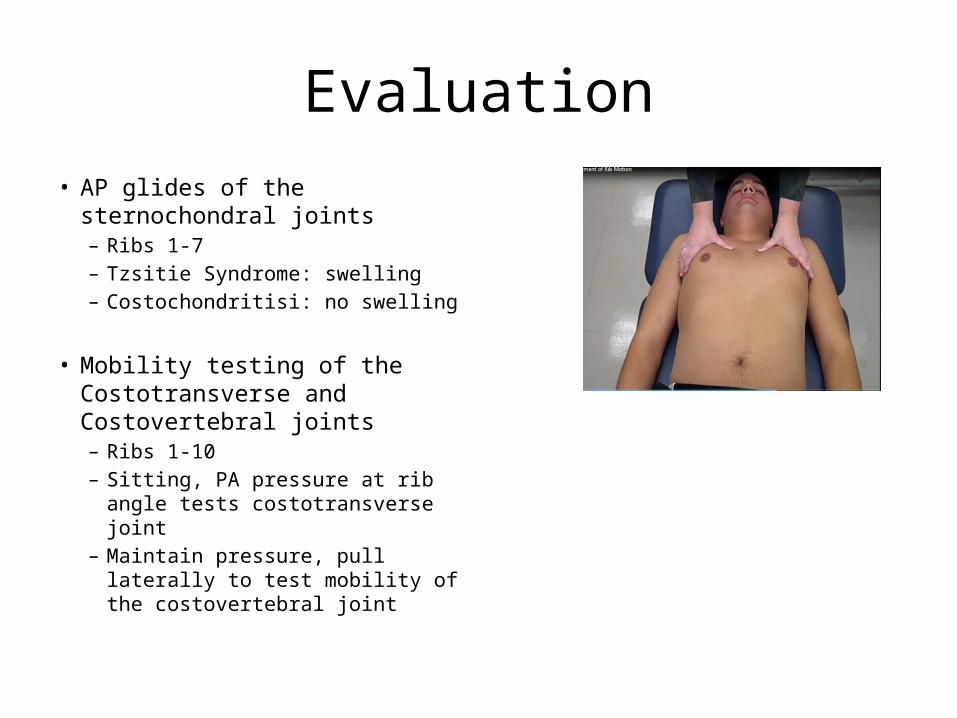
Evaluation• AP glides of the sternochondral
joints– Ribs 1-7– Tzsitie Syndrome: swelling– Costochondritisi: no swelling
• Mobility testing of the Costotransverse and Costovertebral joints– Ribs 1-10– Sitting, PA pressure at rib angle
tests costotransverse joint– Maintain pressure, pull laterally to
test mobility of the costovertebral joint
Evaluation
• Rib Angles• Changes in AP symmetry• Inferior border for
sharpness• Changes in intercostal
spaces• Hypertonicity and
tenderness• Changes with flexion or
extension of the spine
• Sharp angle/edge, means that it is a rotational injury

Evaluation
• Cervical Rotation/Lateral Flexion Test (CRLF) for Diagnosis of Superiorly subluxed first rib
• Patient supine or sitting• PT maximally rotates head
to one side, then laterally flexes head
• Rotate head to left and laterally flex, are testing the right first rib mobility
• Rotate head to the right, then left scalenes and SCM are tight then flexing asses the left 1st rib

Evaluation
Pump handle breathing • Can be assessed in sitting or supine• Place hands on anterior chest• Ask patient to breathe in and out • Assess rib movement
Bucket handle breathing• Can be assessed in sitting or supine• Place hands on lateral chest wall• Ask patient to breathe in and out • Assess rib movement
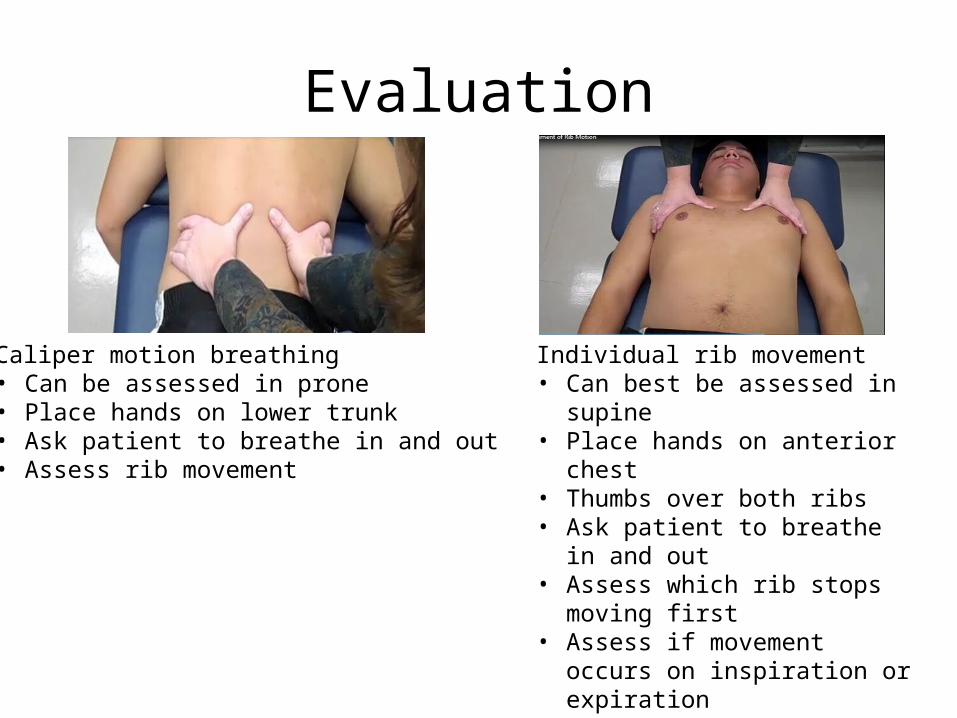
Evaluation
Caliper motion breathing • Can be assessed in prone• Place hands on lower trunk• Ask patient to breathe in and out • Assess rib movement
Individual rib movement• Can best be assessed in supine• Place hands on anterior chest • Thumbs over both ribs• Ask patient to breathe in and out • Assess which rib stops moving first• Assess if movement occurs on
inspiration or expiration• Key Rib: need to t(x) this rib, the 1st
superior rib that does not move compared to the other side in inhalation. In exhalation it is the 1st inferior rib that does not move.

Key Rib
• Restriction in rib mobility secondary to one of the below:– Non-neutral vertebral dysfunction: ERS (not able to
exhale) or FRS (not able to inhale) at that level (90%)– A structural rib dysfunction– A respiratory rib dysfunctionRib vs. Facet – Rib dysfunction: pain will wrap around the body– Facet dysfunction: pain will shoot straight through the
body
STRUCTURAL RIB CLASSIFICATION(Greenman)
• Anterior Rib Subluxation Diagnosis:– Rib angle tender– Rib angle less prominent posteriorly– Prominence of anterior portion of rib – Marked motion restriction for both inhalation and exhalation
• Posterior Rib Subluxation Diagnosis:– Rib angle tender– Rib angle more prominent posteriorly– Anterior portion of rib less prominent– Marked motion restriction for both inhalation and exhalation

Anterior Rib Subluxation

Posterior Rib Subluxation
• Superior 1st Rib Subluxation Diagnosis:– Palpation of superior aspect of 1st rib shows
dysfunctional side to be 5-6mm cephalic compared to other side
– Marked tenderness of superior aspect of first rib– Restriction primarily during Exhalation– Positive Cervical Rotation Lateral Flexion Test

Superior First Rib

If First Rib Treatment Fails
• T1 is dysfunction – check for non-neutral dysfunctions – ERS or FRS
• T2 is laterally flexed and won’t allow T1 to return to normal position
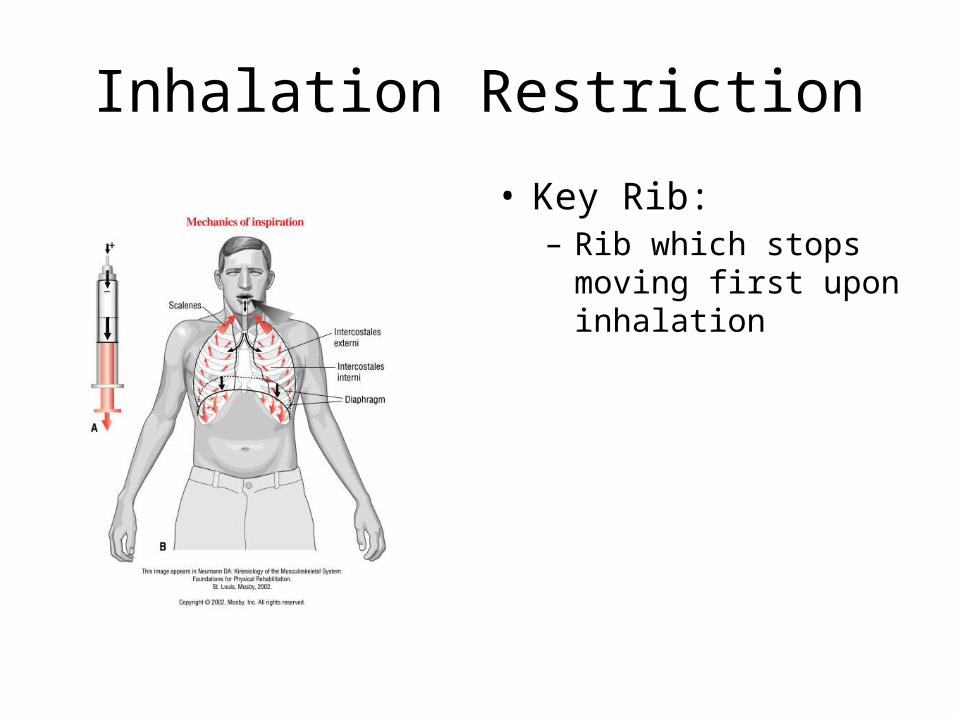
Inhalation Restriction
• Key Rib:– Rib which stops moving
first upon inhalation

Treatment of Inhalation RestrictionsRibs 1-2Key Muscle: Scalenes

Laterally Flexed 2nd rib
• Evaluate: – Acute tenderness to
palpation of pect minor– Positive neural tension
signs– Failed first rib treatment
• Treatment:– Patient supine with arm
outstretched in median nerve neural tension position
– Patient’s head in flexion sidebending away and rotation away from side of dysfunction
– Elbow is flexed and extended
– PT will put pressure on second rib
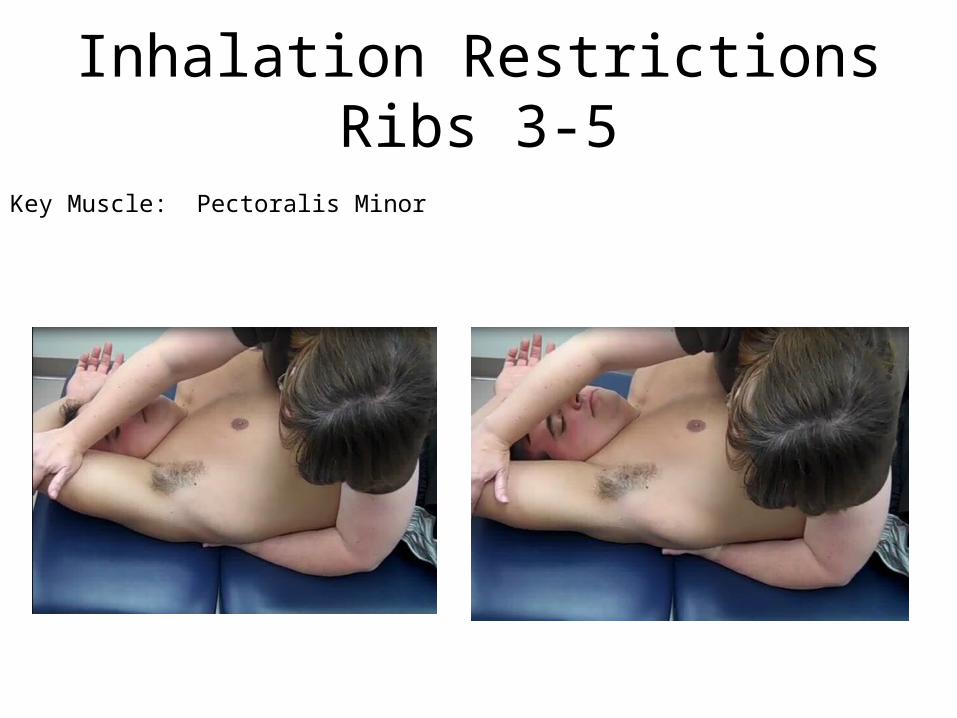
Inhalation Restrictions Ribs 3-5
Key Muscle: Pectoralis Minor
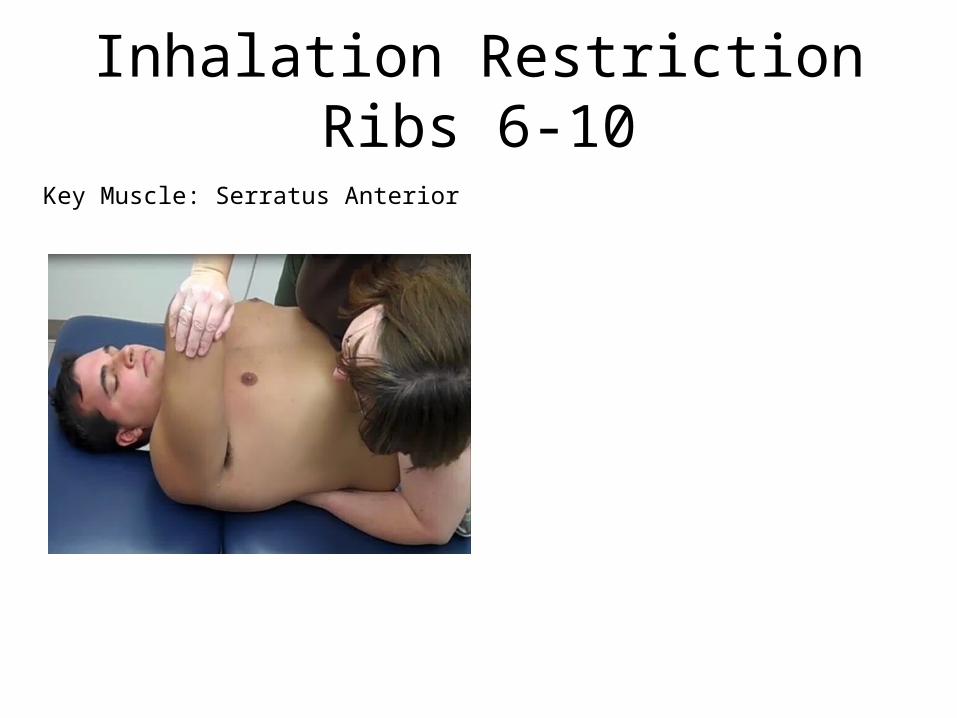
Inhalation Restriction Ribs 6-10
Key Muscle: Serratus Anterior
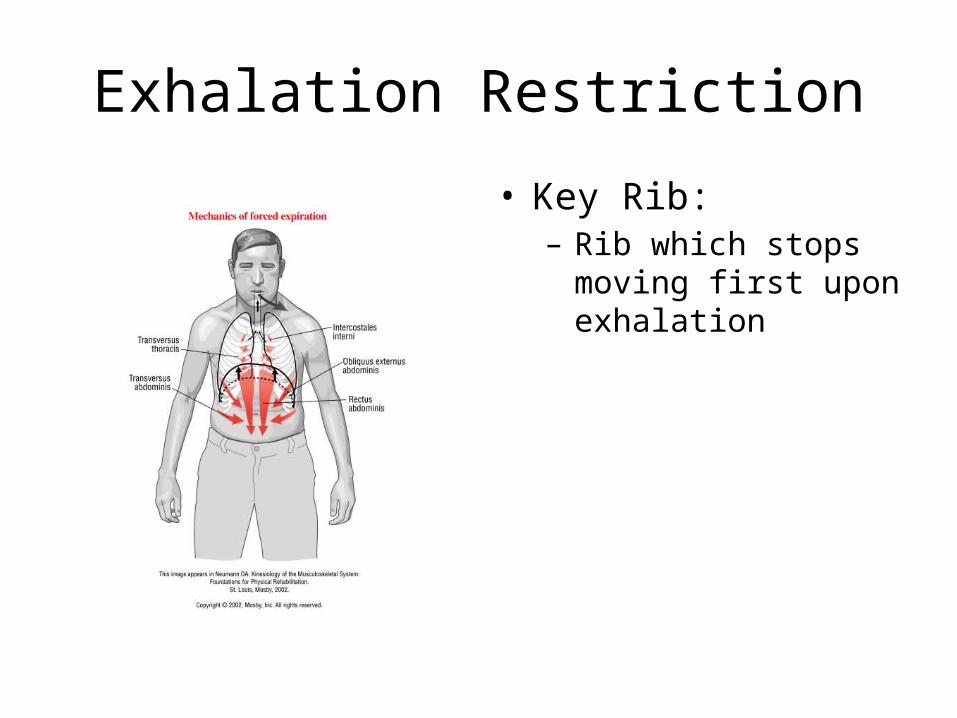
Exhalation Restriction
• Key Rib:– Rib which stops moving
first upon exhalation

Exhalation Restriction
Trunk is placed in Flexion, SidebendingOn restricted side.
-Can place a wedge or lift of table to help

Inhalation restriction ribs 11-12
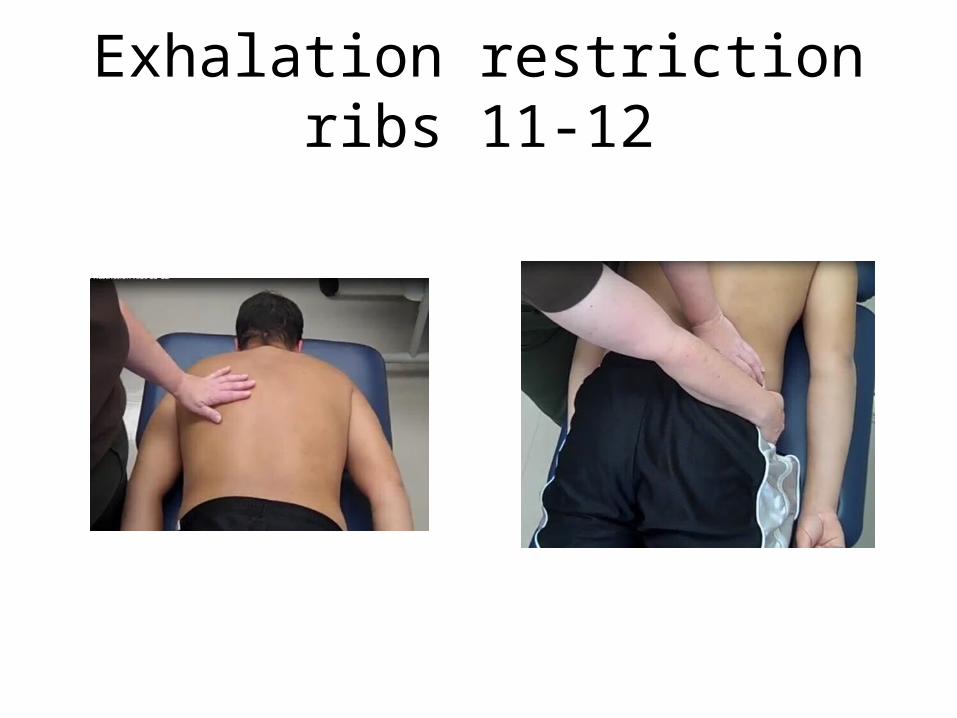
Exhalation restriction ribs 11-12

Limiting factors to Rib motions
• Muscular attachments contributing to respiratory dysfunctions:– Scalenes to ribs 1-2– External & Internal intercostals– Pectoralis minor ribs 3-5– Serratus anterior ribs 3-9– Diaphragm to inner surface ribs 6-12– Quadratus lumborum to rib 12
• Ligamentous strain – Costo-transverse & costo-vertebral articulations
• Chondral dysfunction• Thoracic vertebral dysfunction

Insert slides
Manual Therapy in the Treatment of Patients with Cardiovascular and Rib
Dysfunctions
M uscles of the Spine and Thorax
Text
Diaphragm

Teitze’s Syndrome and Costochondritis
Acute Care Examples of Patients with Rib Dysfunctions
• Post Surgical– Sternotomy– Thoracic incisions from CABG, valve replacement
and chest tube placements– Spinal surgeries– Abdominal incisions from any organ surgery and
PEG tube placements/ostomy– Mastectomy– Tracheostomy
Sternotomy
• Full Median Sternotomy: central incision through the length of the sternum– Standard approach for a CABG
• Partial Median Sternotomy: central incision from sternal notch to ribs 4,5– Common in surgeries of the heart valves


Partial Stenotomy

Breathing Disorders• Exacerbations of Disease
– COPD– MS– Pneumonia
• Neuromusculoskeletal Dysfunctions– CVA
• Depressed on one side
– Trauma to the spine, ribs, pelvis with or without surgical procedures
• Mechanical Rib Dysfunctions
– Amputation with co-morbidities of cardiopulmonary disorders

• What effects would scoliosis have on rib cage movement? – Convexity of Left: rib smaller, humps up and
laterally being squished. • What would happen to breathing if a rib
separation occurred at an intercostal joint?– Can’t pull rib below it, with it when you breath in.
Pain with breathing, pt will hold rib and breath away from separation.