Musculoskeletal Anatomy - WikispacesRevision+for+ME… · Musculoskeletal Anatomy ... Endochondral...
65
Musculoskeletal Anatomy Revision for MEDI1000 and USMLE Monday October 26th
Transcript of Musculoskeletal Anatomy - WikispacesRevision+for+ME… · Musculoskeletal Anatomy ... Endochondral...
Musculoskeletal Anatomy Revision for MEDI1000 and USMLE
Monday October 26th
Disclaimer
• Jokes may not be funny
• Information is from Moore’s but may have mistakes
• First time lecturing
• PLEASE ASK QUESTIONS

Some General Thoughts on Anatomy • It’s a language. Best learnt through combination of didactic lectures
then self-directed revision.
• Not PBL
• Not 2 hours a week
• Not once off – go home and learn this lecture 9pm – midnight tonight
• 50% of time for 5% of marks
• 20% of knowledge used 80% of the time
• Important in the long-term
• Suggest approach:
• Learn systemic anatomy – start with skeleton • Lectures
• Textbooks
• Anatomy museum
• Then learn regional anatomy
Some hints on the language
• Latin and Greek
• Adjectives matter – vertebra/vertebral, ulna/ulnar, etc
• Plurals matter – ramus communicans / rami communicantes, pelvis/pelves, humerus/humeri, vertebra(e), vas(a), cortex/cortices, foramen/foramina, septum/septa, epididymis/epididymides
• Common terms
• Epi = above, ad = above
• Sub = deep
• Intra = inside, extra = outside
• Infra = below, extra = above
• “__lla” means little, e.g. patella, canalicula, etc
• Parietal = wall
• Viscus / viscera = internal organ (note adj. = splanchnic)
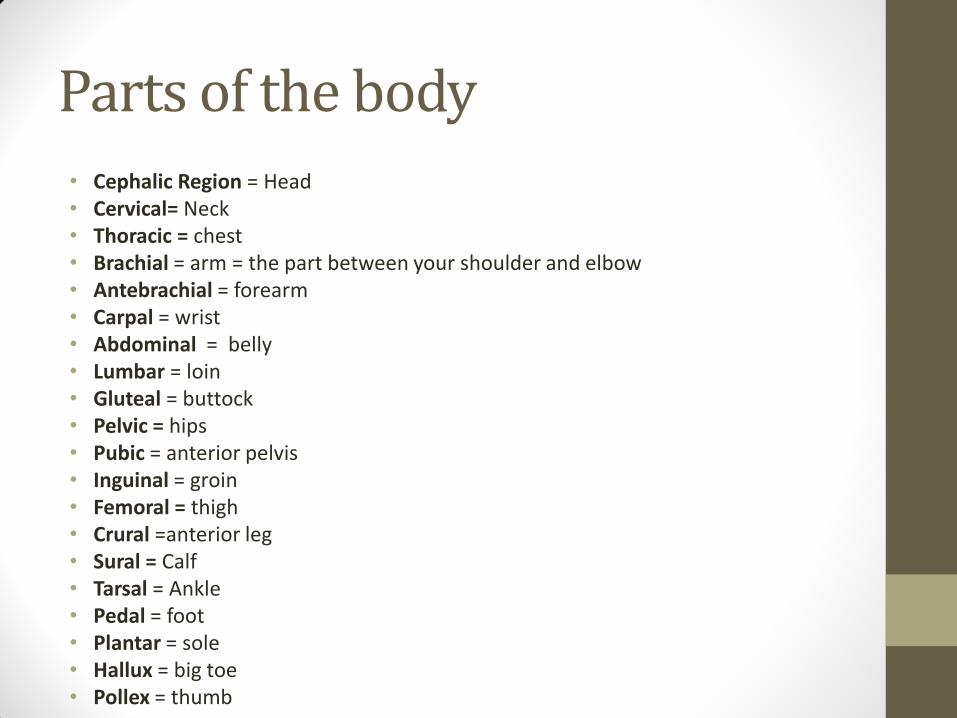
Parts of the body
• Cephalic Region = Head • Cervical= Neck • Thoracic = chest • Brachial = arm = the part between your shoulder and elbow • Antebrachial = forearm • Carpal = wrist • Abdominal = belly • Lumbar = loin • Gluteal = buttock • Pelvic = hips • Pubic = anterior pelvis • Inguinal = groin • Femoral = thigh • Crural =anterior leg • Sural = Calf • Tarsal = Ankle • Pedal = foot • Plantar = sole • Hallux = big toe • Pollex = thumb
A note on eponyms
• Phased out in Terminologia Anatomica system (congress of anatomists)
• Clinicians are not anatomists
• Eponyms are widely used by surgeons
• Good for impressing surgeons
• “The CSF is produced on the roof of the lateral ventricles, it then travels through the foramina of Munro, into the third ventricle, down the aqueduct of Sylvius, into the fourth ventricle, through the foramina of Luschka and the foramen of Magenda, into the subarachnoid space where it circulates around to be absorbed by the granulations of Pacchioni”
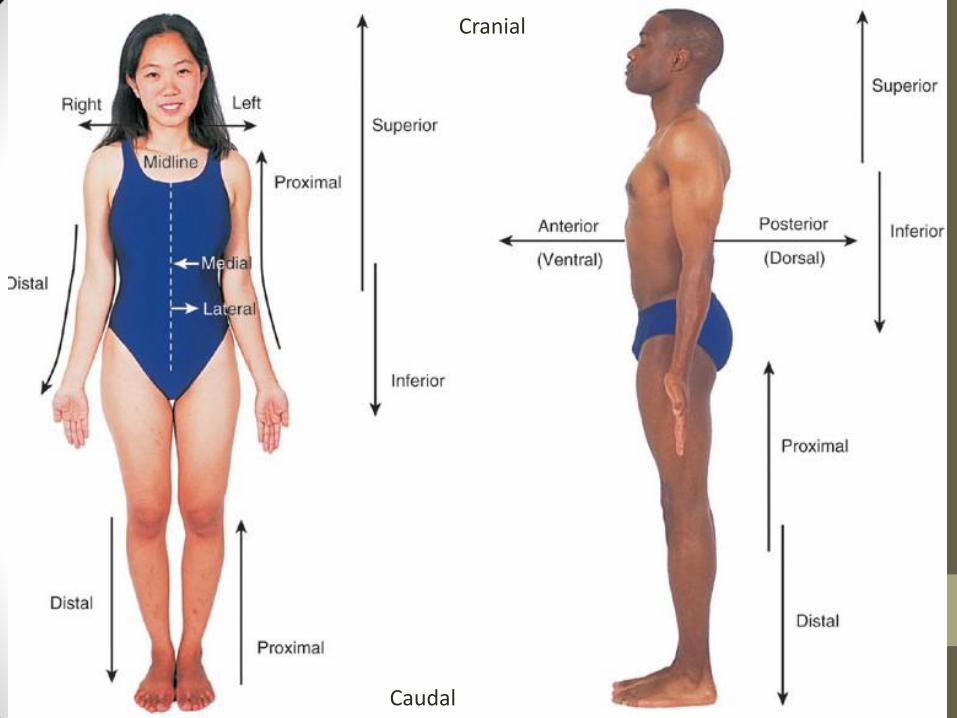
Caudal
Cranial
Osteology
Classification of bones
• By shape
• Long bones (femur, tibia)
• Flat bones (roof of skull, sternum, ribs)
• Sutural (between calvaria)
• Irregular (vertebrae, pelvis)
• Short (carpals, tarsals)
• Sesamoid (inside tendons, e.g. patella)
• Pneumatic (air-filled, e.g. maxilla)
• By gross features
• Compact – periphery of long bones. Thickest in diaphysis (shaft)
• Cancellous / spongy – in epiphyses
Common terms for bony features
• General Elevations or projections • Process – any projection or bump • Ramus – an extension of a bone making an angle with the rest of the structure
• Processes formed where tendons or ligaments attach • Trochanter – a large, rough projection • Tuberosity – a smaller, rough projection • Tubercle – a smaller, rounded projection • Crest – a prominent ridge • Spine – a pointed or narrow process • Head – the expanded articular end of an epiphysis
• Processes formed for articulation with adjacent bones • Neck – narrow connection between epiphysis and diaphysis • Condyle – a smooth, rounded articular process • Trochlea – a smooth, grooved articular process shaped like a pulley • Facet – a small, flat articular surface
• Depressions • Fossa – a shallow depression • Sulcus – a narrow groove
• Openings • Foramen – a rounded passageway for blood vessels or nerves • Canal or Meatus – A passageway through the substance of a bone • Fissure – an elongated cleft • Sinus or Antrum – a chamber within a bone, normally filled with air
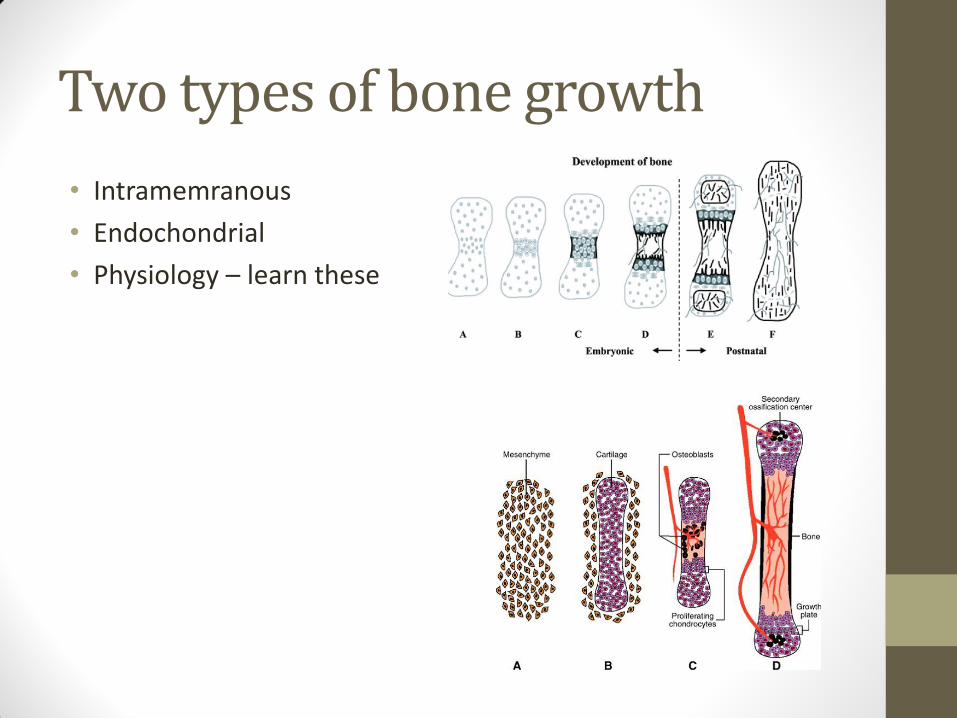
Two types of bone growth
• Intramemranous
• Endochondrial
• Physiology – learn these
Intramembranous ossification - learn at home
• Intramembranous ossification occurs in the flat bones of the skull, the mandible and the clavicle
• Mesenchymal stem cells differentiate into osteochondral progenitor cells and then into osteoblasts, which congregate to form an ossification centre. This is mediated by factors such as TGF-β and FGF. This secreted osteoid (the organic part of the bone matrix) which becomes mineralised and forms bone spicules, which then form trabeculae.
• As trabeculae thicken, the osteoblasts become surrounded by their own bone matrix and become osteocytes
• Bone formation occurs on the inner and outer surfaces of cortical plates of bone
• Red marrow, vessels and nerves infiltrate the medullary cavity of the bone, filling it with haemopoietic bone marrow
Endochondral Ossification – learn at home
• Mesenchymal cells begin to condense and differentiate into chondrocytes. These form a hyaline cartilaginous model of the prospective bone. The cartilage is surrounded by perichondrium, a dense layer of connective tissue, and contains an outer fibrous layer and an inner chondrogenic layer which contain fibroblasts, chondroblasts or chondrocytes as it is undifferentiated.
• Blood vessels invade the centre of the cartilaginous model, bringing osteoblasts with them so that chondrocytes proliferation only takes place at the epiphyses (ends, singular = epiphysis) of the bones.
• Osteoblasts deposit bone matrices, or osteoid, and convert the perichondrium into periosteum to form a bone collar • Note that periosteum covers all bone except the ends of long bone, where it
• Chondrocytes in the shaft of the bone (diaphysis) mineralize the surrounding matrix, undergo hypertrophy then undergo apoptosis once surrounding mineralised bone inhibits their blood supply. This forms a cavity inside the bone while the bone collar provides stability
• The bone is penetrated by a periosteal bud, which contains nutrient arteries, veins, lymphatic, nerve fibres, red marrow elements, osteoblasts and osteoclasts. The site of this penetration remains as the nutrient foramen of long bones.
• The osteoclasts break down the calcified cartilaginous matrix, but osteoid from osteoblasts forms spongy bone. This occurs at the primary ossification centre. These are found in all long bones of the body by the 12th week of development.
• As the primary ossification centre enlarges, osteoclasts breakdown the newly-formed spongy bone to create a marrow cavity • Appositional growth increases the width of the bone. The outer fibrous layer of periosteum contains fibroblasts while
the inner osteogenic layer lays down new bone while osteoclasts increase the size of the medullary cavity from the inside.
• At birth, the diaphysis is completely ossified but the two epiphyses are still cartilaginous. Soon after birth, secondary ossification centres form later as blood vessels invade the epiphyses. Further growth of bones occurs from chondrocytes proliferation at the junction between the metaphysis (neck of long bones) and the epiphyseal plates. Endochondral ossification proceeds on both sides of the plate, and the plate disappears when growth is complete after puberty, when the epiphyses fuse with the diaphysis • Long bones have an epiphyseal plate at each extremity; smaller bones (e.g. the phalanges) only have one. Irregular
bones such as vertebrae have several primary and secondary centres of ossification.
Arthrology
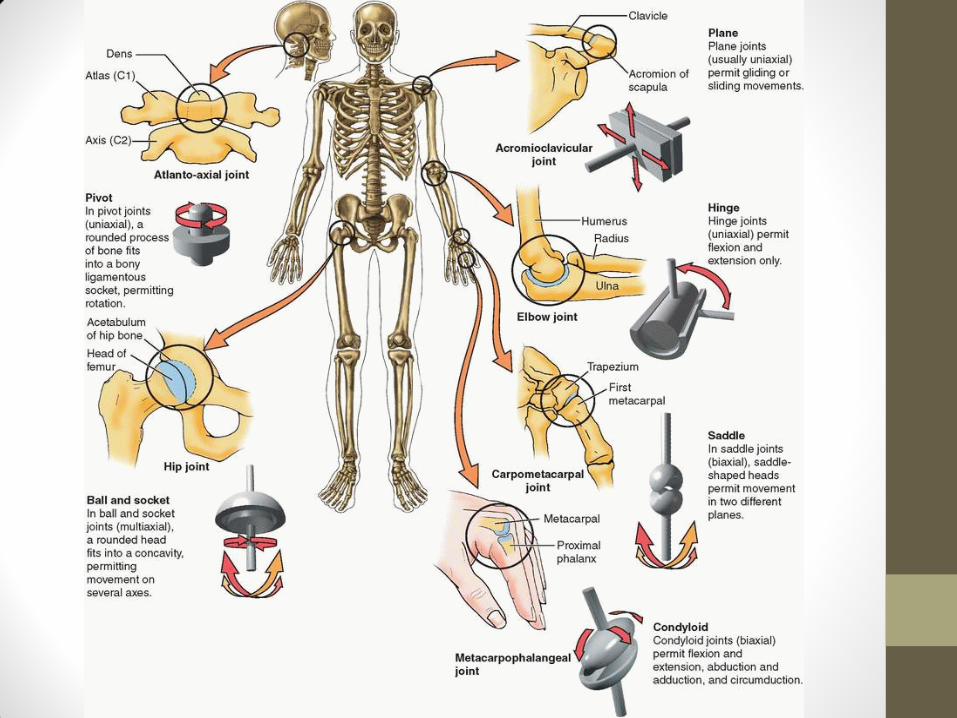
Types of Joint • Synovial – joint capsule, synovial fluid, most common type,
allow free movement. Reinforced by accessory ligaments (extrinsic or intrinsic). If surfaces incongruent – articular disc.
• Plane - e.g. AC joint
• Hinge – uniaxial, collateral ligaments. E.g. DIPJ
• Saddle –Biaxial (Ab/ad, flex/ext + circumduction). E.g. 1st CMCJ
• Condyloid – biaxial but sagittal mvmt > frontal. E.g. MCPJ
• Ball and socket – multi-axial, e.g. Hip
• Pivot – uniaxial rotation. Rounded bone in sleeve or ring. E.g. Radio-ulnar joint
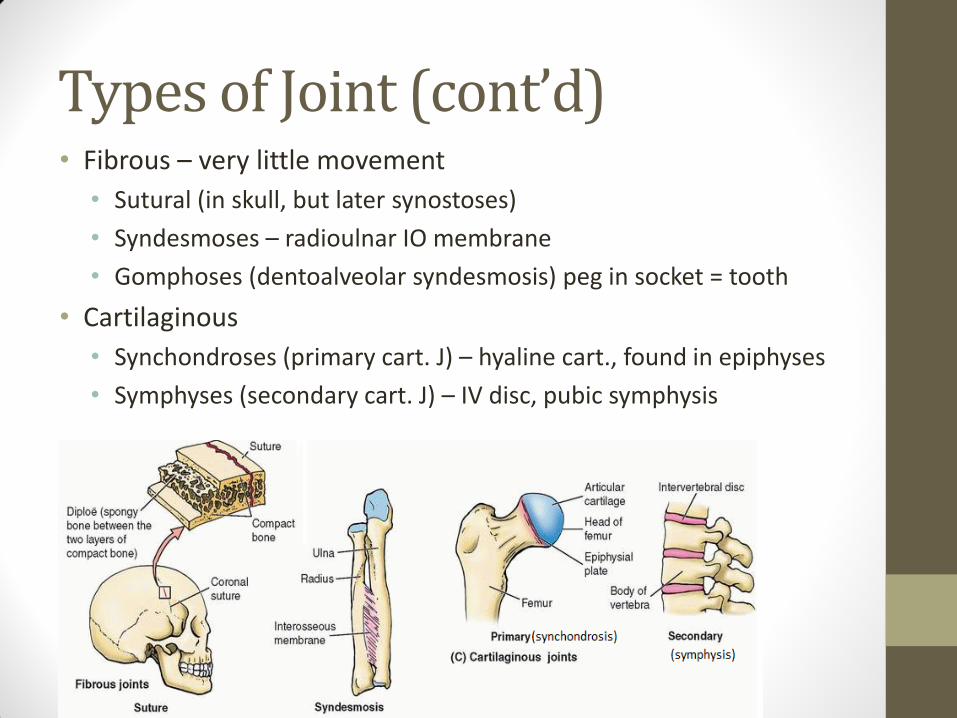
Types of Joint (cont’d) • Fibrous – very little movement
• Sutural (in skull, but later synostoses)
• Syndesmoses – radioulnar IO membrane
• Gomphoses (dentoalveolar syndesmosis) peg in socket = tooth
• Cartilaginous
• Synchondroses (primary cart. J) – hyaline cart., found in epiphyses
• Symphyses (secondary cart. J) – IV disc, pubic symphysis

Myology
General info on muscles
• Takes of 40-50% of body mass
• Basic features
• Myocytes fascicles skeletal muscle
• Connective tissue
• Endomysium (arround each fibre)
• Perimysium (around the fascicle)
• Epimysium (surrounds whole muscle)
• Tendon = muscular attachment to bone (not all muscles have tendons)
• Origin = fixed attachment, usually proximal
• Insertion = attachment to part that moves, usually distal
• Note origin/insertion can swap (e.g. iliopsoas)
Arrangement of Fascicles
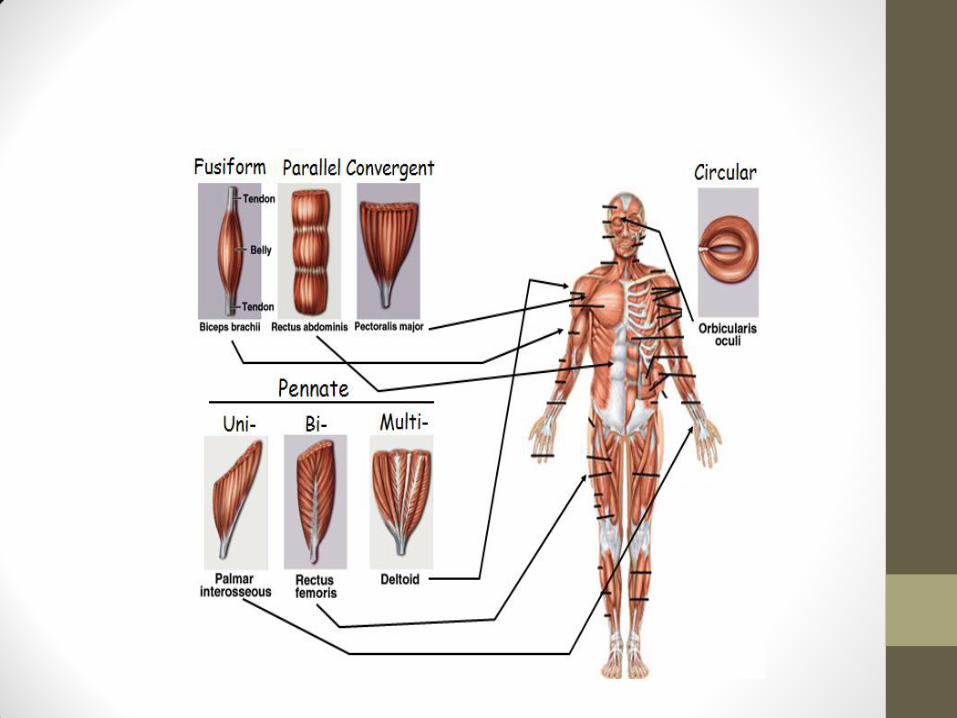
• Parallel – long axes of fascicles run parallel to long axes of muscle. Most muscles
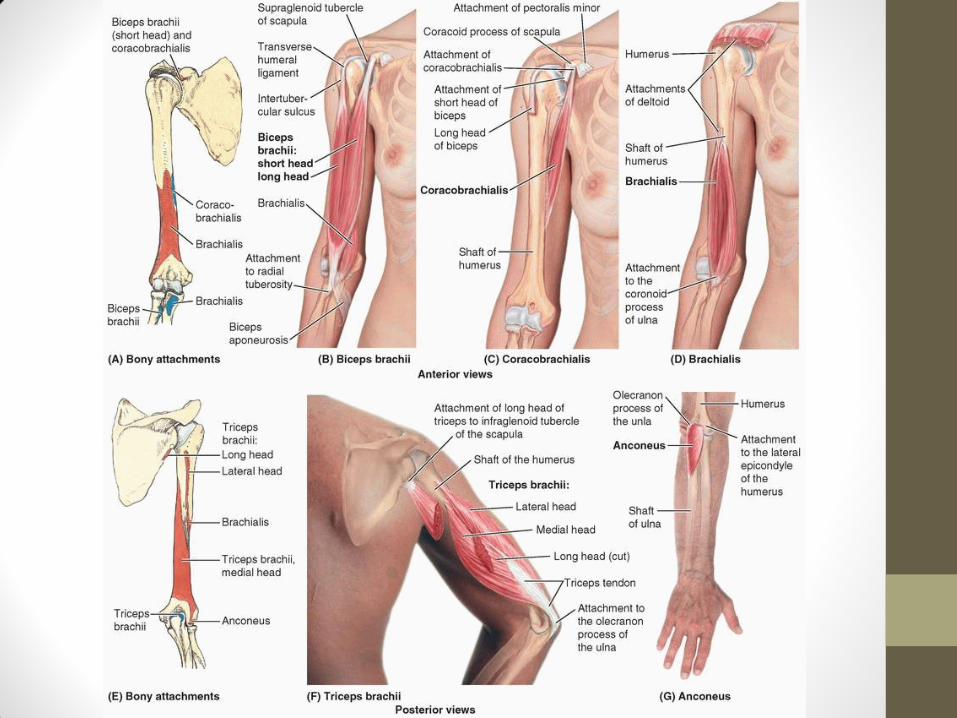
• Fusiform e.g. biceps brachii
• Strap-like e.g. sartorius
• Convergent – wide origin then converge onto tendon, e.g. pectoralis major
• Circular – fascicles arranged in ring. E.g. Orbicularis oculi
• Pennate
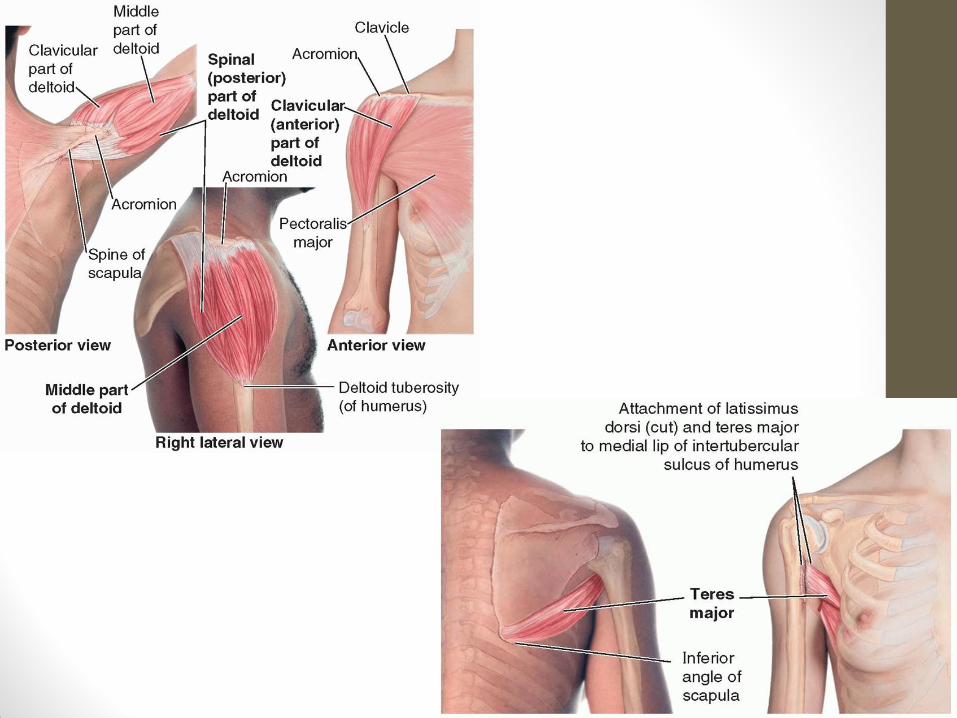
• Multipennate – look like feathers, very strong. E.g. deltoid
• Bipennate - fascicles attach to tendon from both sites e.g. rectus femoris
• Unipennate – fascicles attach from one side, e.g. EDL or palmar interossei
Muscle Contraction
• Range of motion – the more parallel the fasciles, the more the muscles can shorten, the greater ROM (e.g. biceps brachii cf. deltoid)
• Power – depends on number of fibres (multipennate > bipennate)
• Types of contraction • Isotonic (length changes)
• Concentric (shortens)
• Eccentric (lengthens)
• Isometric (no change in length)
• Agonist = prime mover
• Antagonist = opposes the agonist
• Synergist = muscle that helps agonist (e.g. fixators)
Muscle Terminology
• Terms indicate location • Bone attachment – e.g. flexor carpi ulnaris • Relative position – e.g. flexor digitorum superficialis • Intrinsic (origin inside), extrinsic (origin outside) • Supra / infra • Body region – e.g. brachialis, flexor pollicis longus
• Terms indicate action • Flexor / extensor, abductor / adductor, sphincter / dilator, levator /
depressor
• Terms indicate direction • Rectus = straight • Oblique = diagonal • Transverse = transversus
• Terms indicate shape • Trapezoid - trapezius • Rhomboid • Quadrilateral – pronator quadratus • Triangular - deltoid
Muscle Terminology • Terms indicates size
• Large = maximus, magnus, major
• Small = minimus, minor
• Terms indicate length
• Long = longus, longissimus
• Short = brevis
• Terms indicate number of heads
• 2/3/4 heads = bi/tri/quadriceps
Bones of the Upper Limb
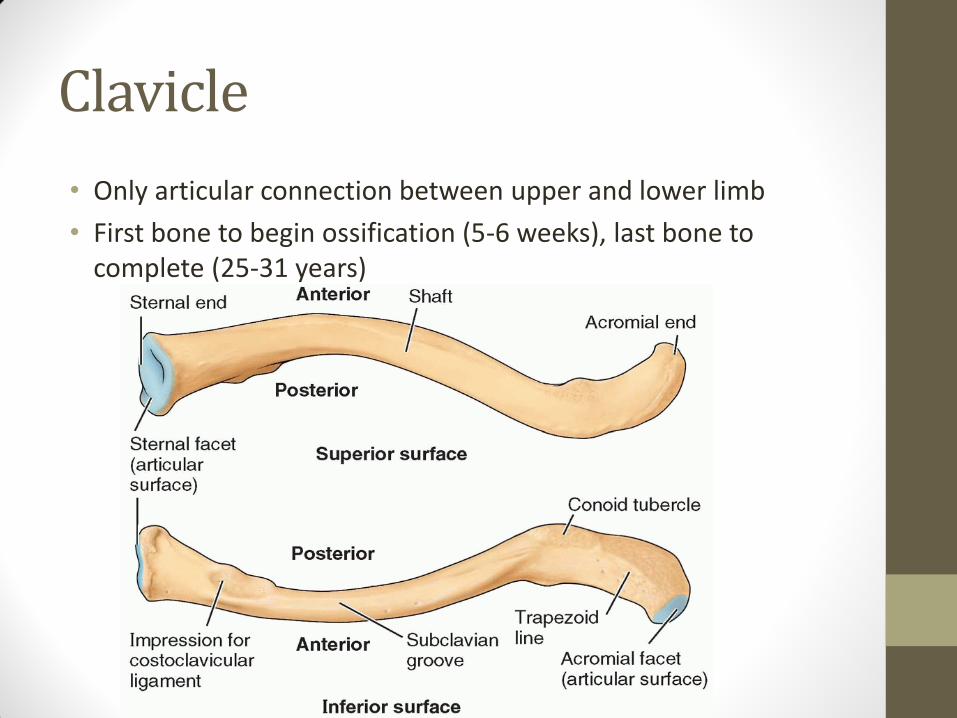
Clavicle
• Only articular connection between upper and lower limb
• First bone to begin ossification (5-6 weeks), last bone to complete (25-31 years)
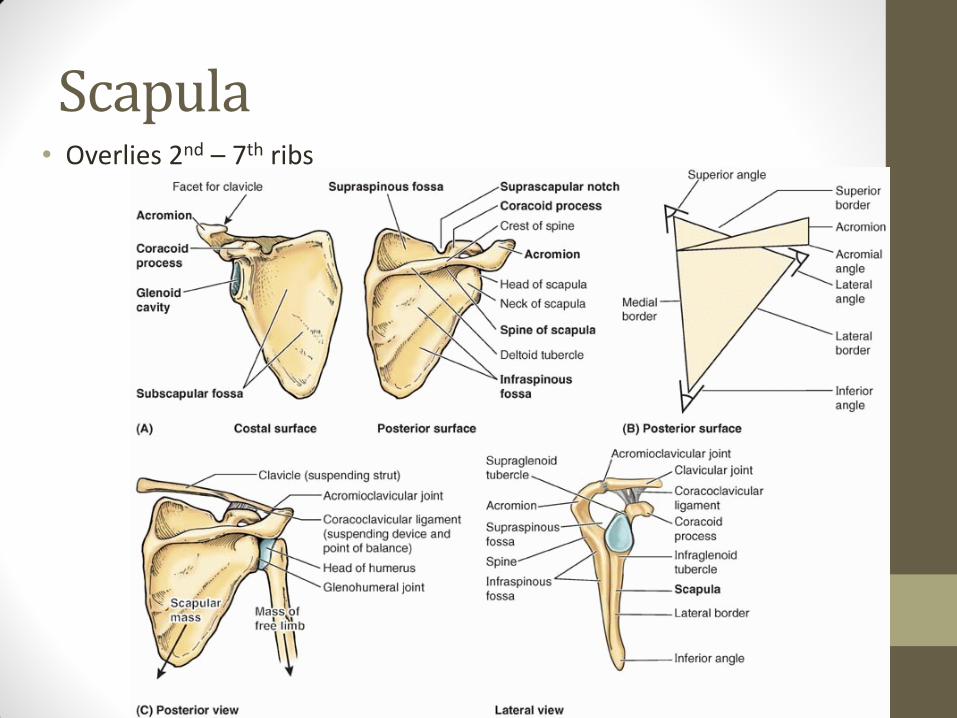
Scapula • Overlies 2nd – 7th ribs
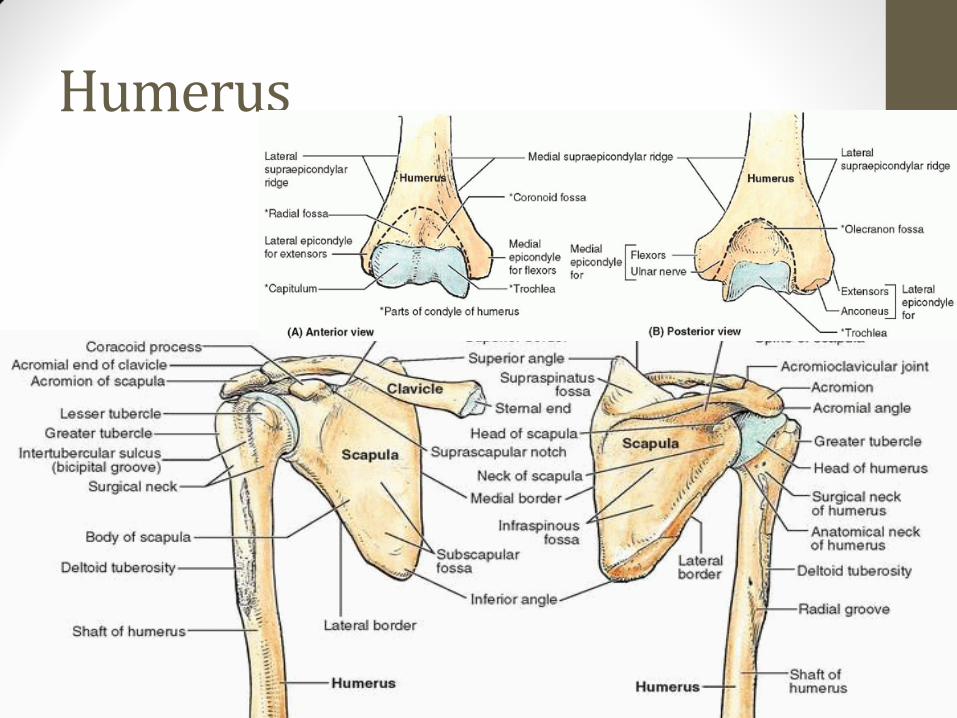
Humerus
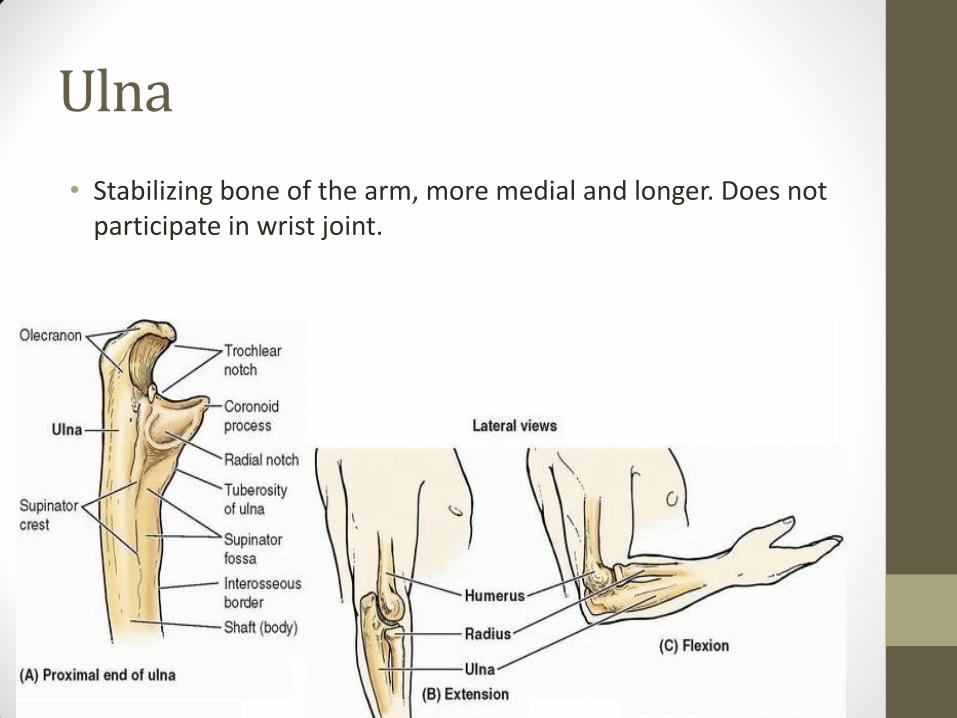
Ulna
• Stabilizing bone of the arm, more medial and longer. Does not participate in wrist joint.
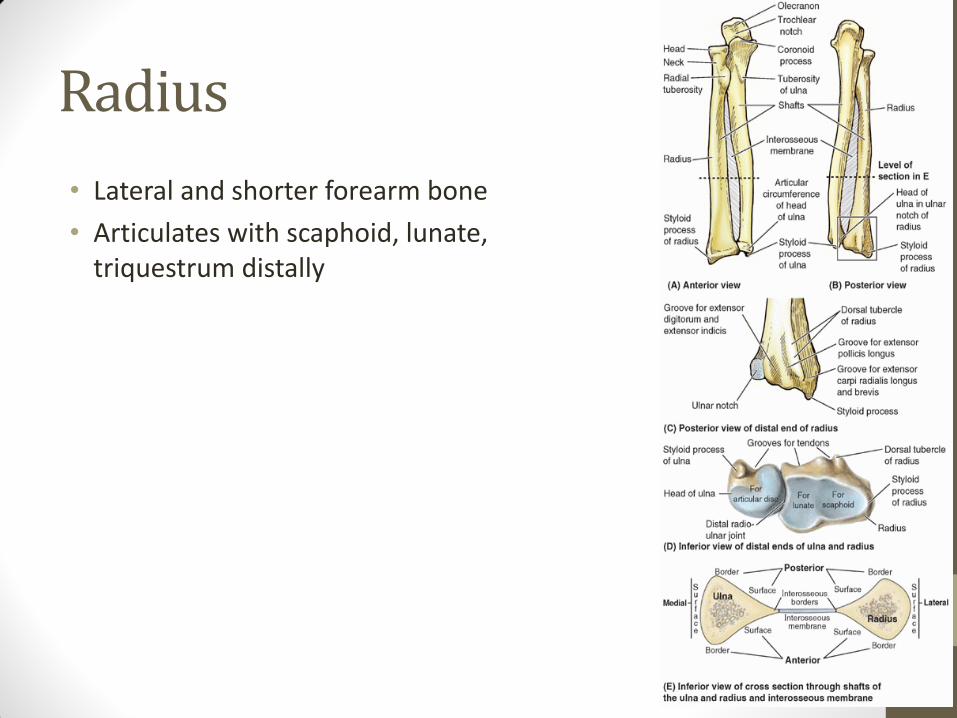
Radius
• Lateral and shorter forearm bone
• Articulates with scaphoid, lunate, triquestrum distally
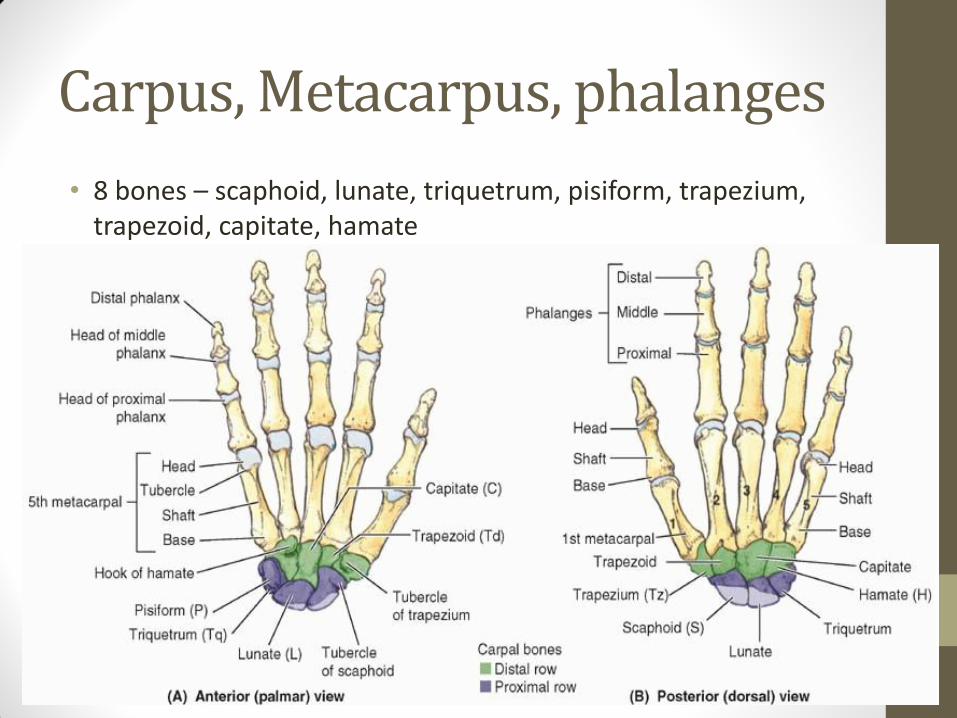
Carpus, Metacarpus, phalanges
• 8 bones – scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, hamate
Metacarpus
• 5 metacarpals – form the palm
• Base
• Head
• Phalanges
• Proximal
• Middle (except 1st)
• Distal
Joints of the Upper Limb
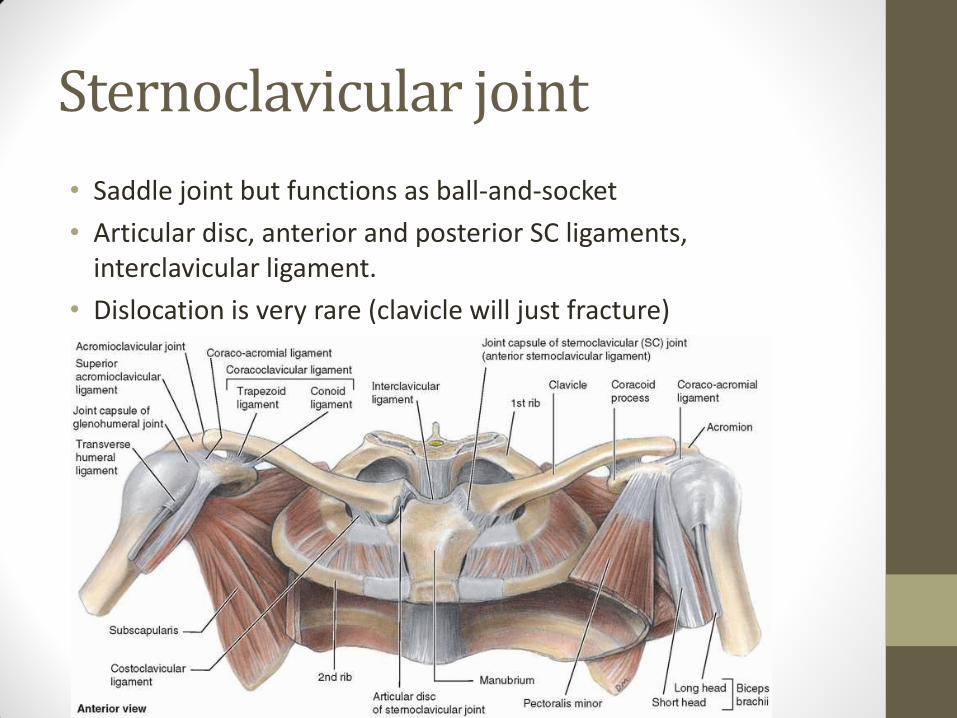
Sternoclavicular joint
• Saddle joint but functions as ball-and-socket
• Articular disc, anterior and posterior SC ligaments, interclavicular ligament.
• Dislocation is very rare (clavicle will just fracture)
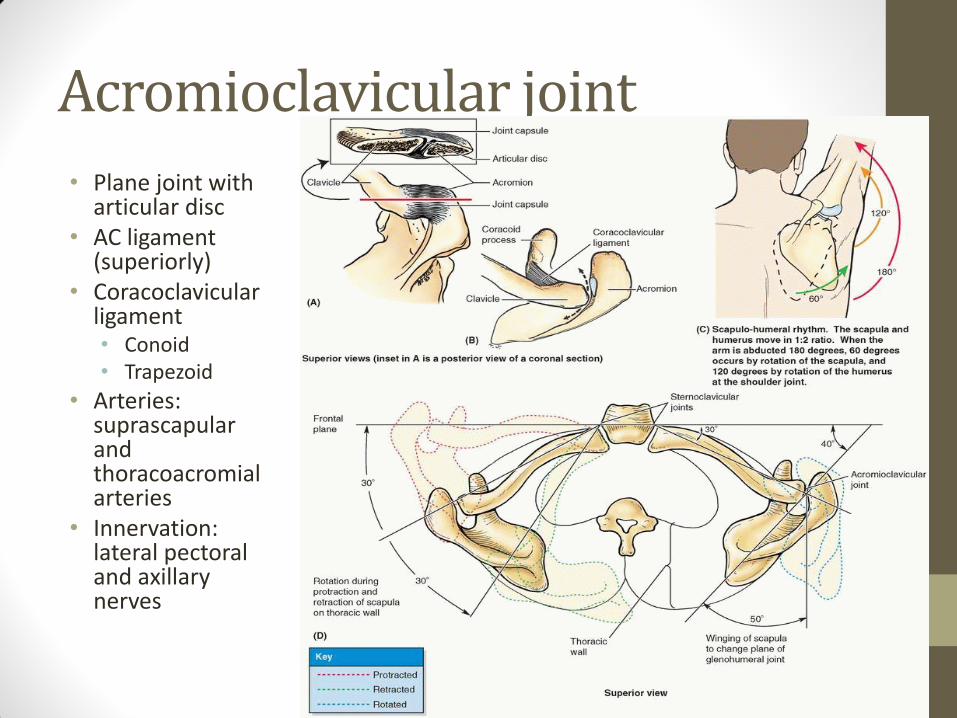
Acromioclavicular joint
• Plane joint with articular disc
• AC ligament (superiorly)
• Coracoclavicular ligament • Conoid • Trapezoid
• Arteries: suprascapular and thoracoacromial arteries
• Innervation: lateral pectoral and axillary nerves
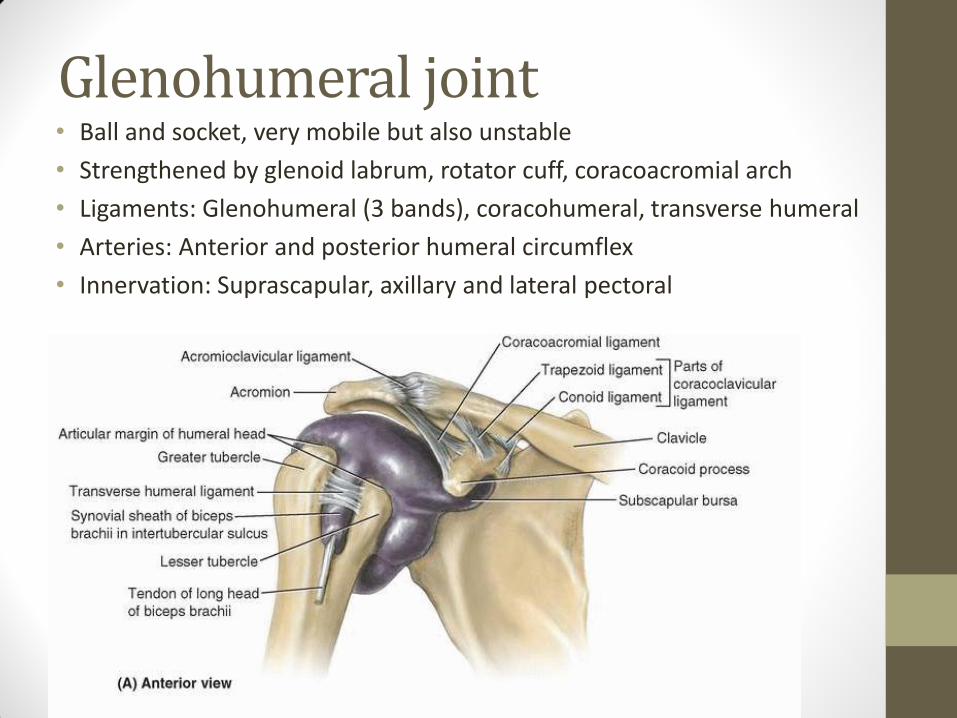
Glenohumeral joint • Ball and socket, very mobile but also unstable
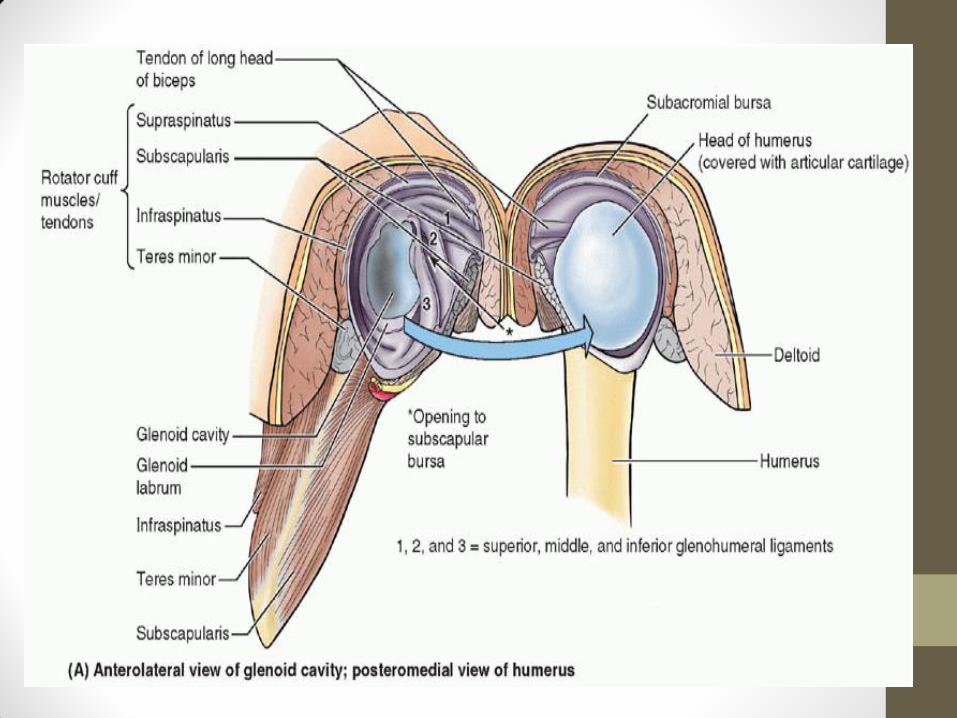
• Strengthened by glenoid labrum, rotator cuff, coracoacromial arch
• Ligaments: Glenohumeral (3 bands), coracohumeral, transverse humeral
• Arteries: Anterior and posterior humeral circumflex
• Innervation: Suprascapular, axillary and lateral pectoral
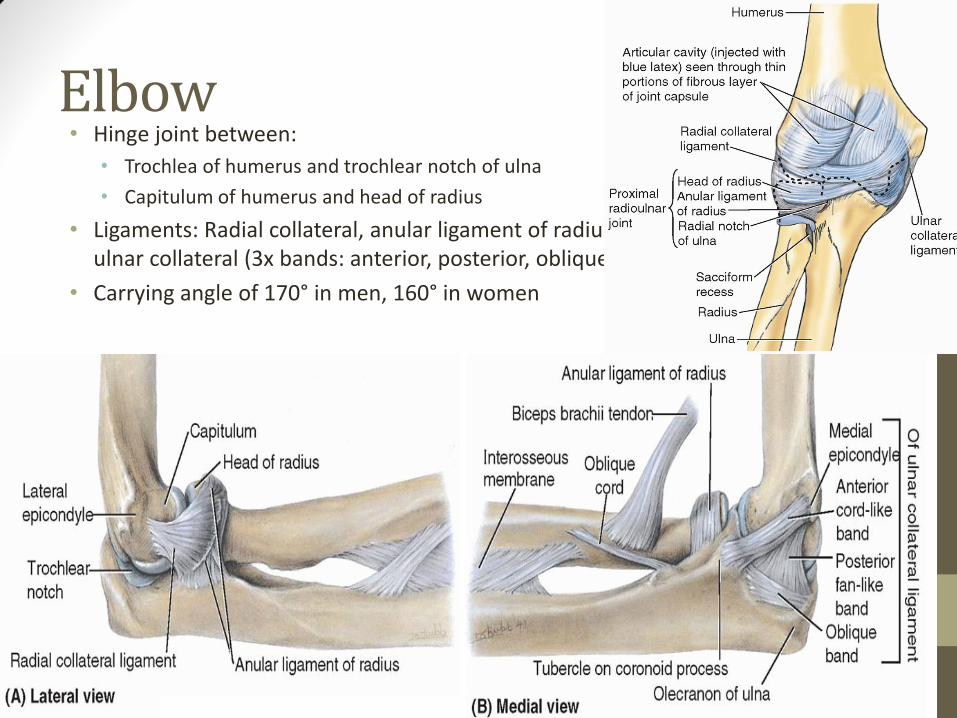
Elbow • Hinge joint between:
• Trochlea of humerus and trochlear notch of ulna
• Capitulum of humerus and head of radius
• Ligaments: Radial collateral, anular ligament of radius, ulnar collateral (3x bands: anterior, posterior, oblique)
• Carrying angle of 170° in men, 160° in women
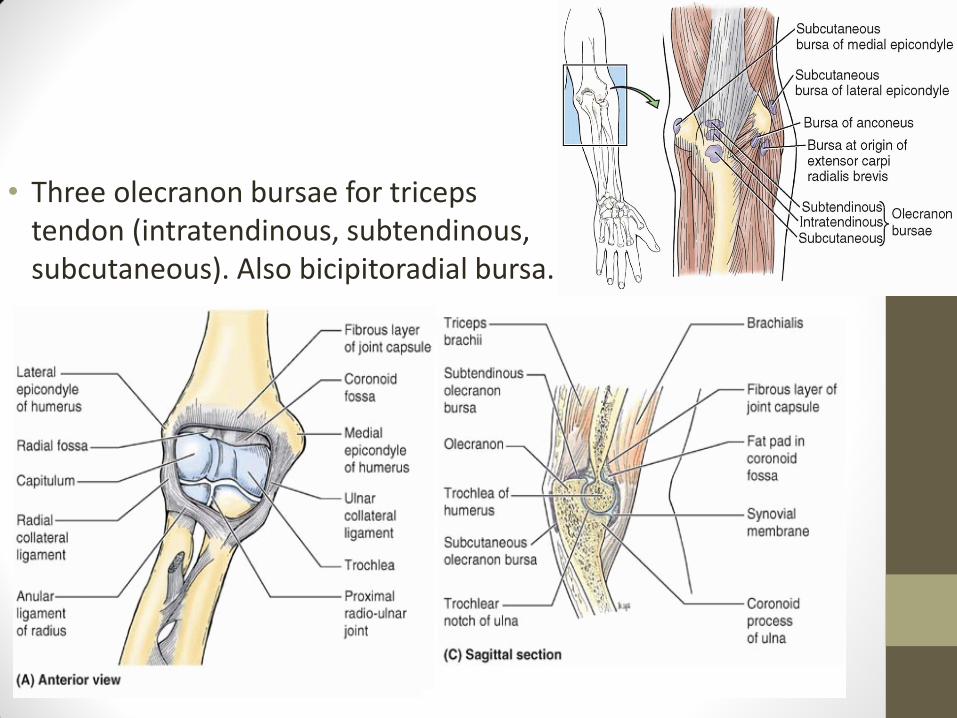
• Three olecranon bursae for triceps tendon (intratendinous, subtendinous, subcutaneous). Also bicipitoradial bursa.
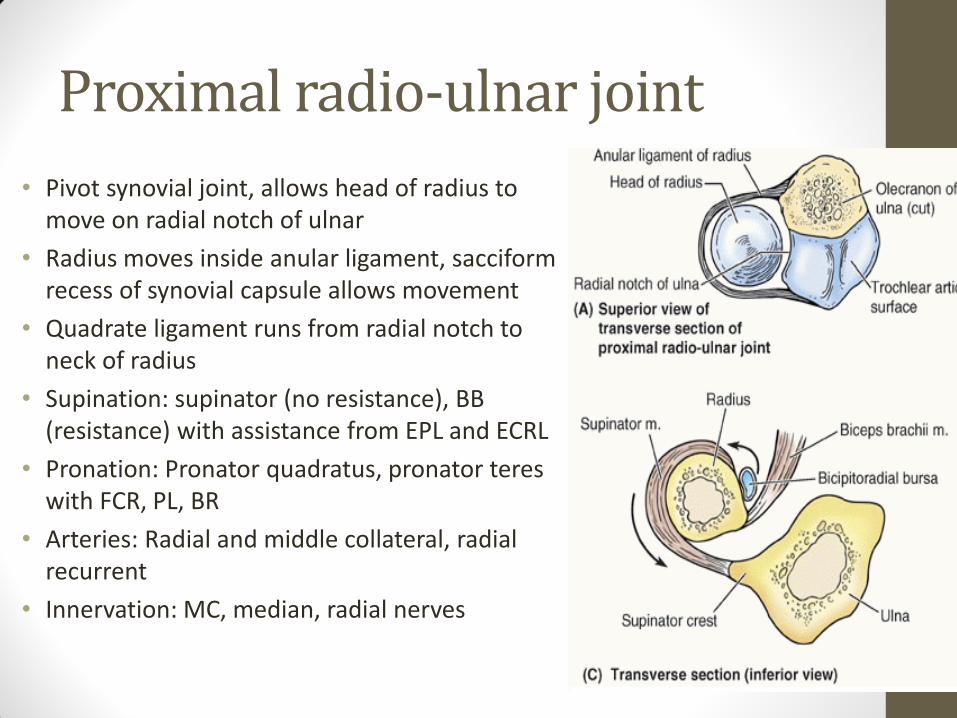
Proximal radio-ulnar joint
• Pivot synovial joint, allows head of radius to move on radial notch of ulnar
• Radius moves inside anular ligament, sacciform recess of synovial capsule allows movement
• Quadrate ligament runs from radial notch to neck of radius
• Supination: supinator (no resistance), BB (resistance) with assistance from EPL and ECRL
• Pronation: Pronator quadratus, pronator teres with FCR, PL, BR
• Arteries: Radial and middle collateral, radial recurrent
• Innervation: MC, median, radial nerves
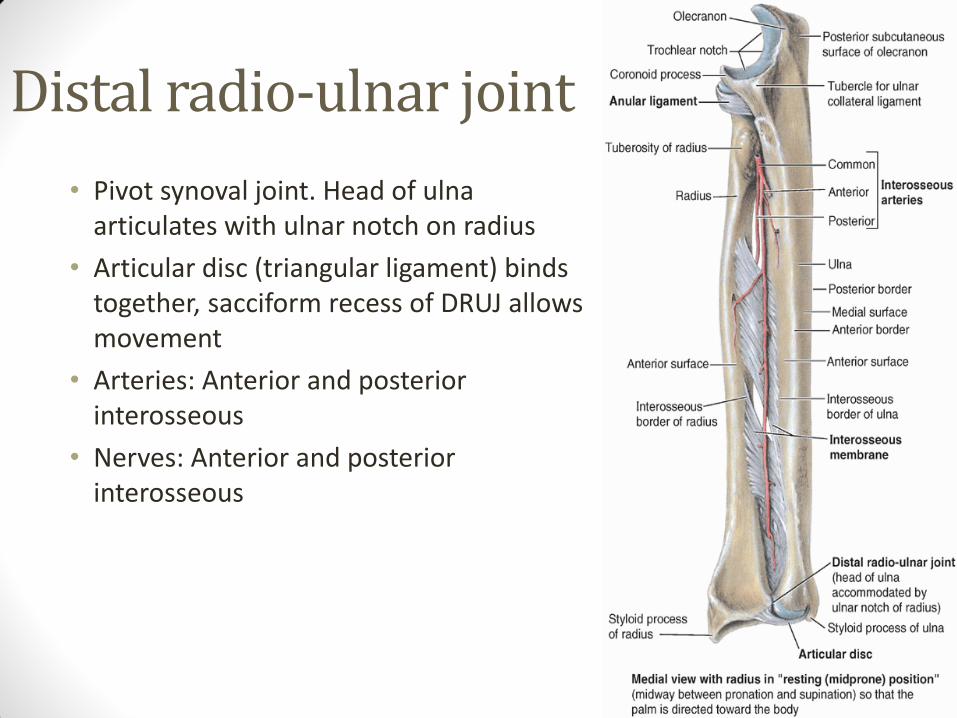
Distal radio-ulnar joint
• Pivot synoval joint. Head of ulna articulates with ulnar notch on radius
• Articular disc (triangular ligament) binds together, sacciform recess of DRUJ allows movement
• Arteries: Anterior and posterior interosseous
• Nerves: Anterior and posterior interosseous
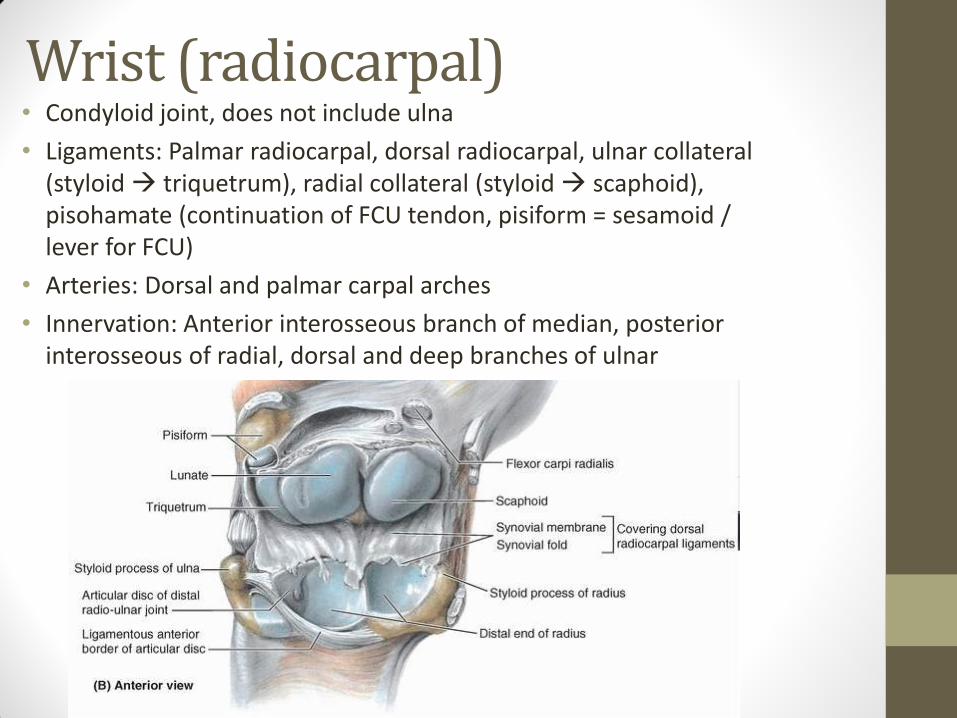
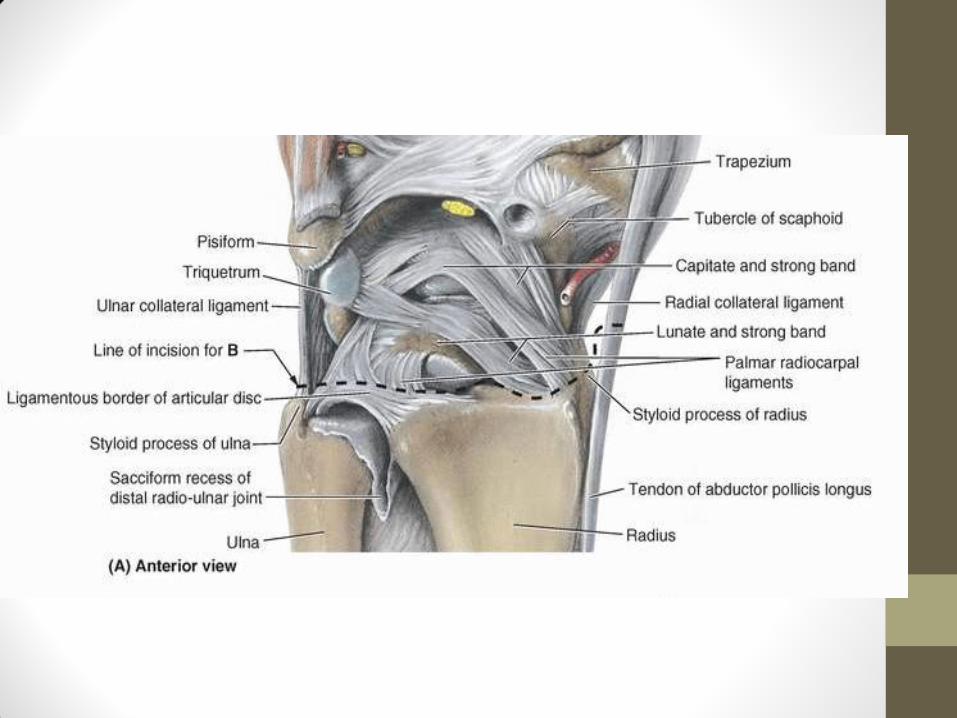
Wrist (radiocarpal) • Condyloid joint, does not include ulna
• Ligaments: Palmar radiocarpal, dorsal radiocarpal, ulnar collateral (styloid triquetrum), radial collateral (styloid scaphoid), pisohamate (continuation of FCU tendon, pisiform = sesamoid / lever for FCU)
• Arteries: Dorsal and palmar carpal arches
• Innervation: Anterior interosseous branch of median, posterior interosseous of radial, dorsal and deep branches of ulnar
Intercarpal and CMC joints
• Intercarpal:
• Plane, synovial joints that interconnect the carpals
• Common articular cavity for intercarpal and CMC joints (except 1st CMCJ)
• Joined by anterior, posterior, interosseous ligaments
• Gliding movements possible
• Flexion at mid-carpal joint (between 1st and 2nd row)
• 1st CMC (thumb): saddle, independent capsule. Articulation between trapezium and base of 1st MC
• 2nd – 5th CMC: plane synovial joints, some flexibility in 4th and 5th.
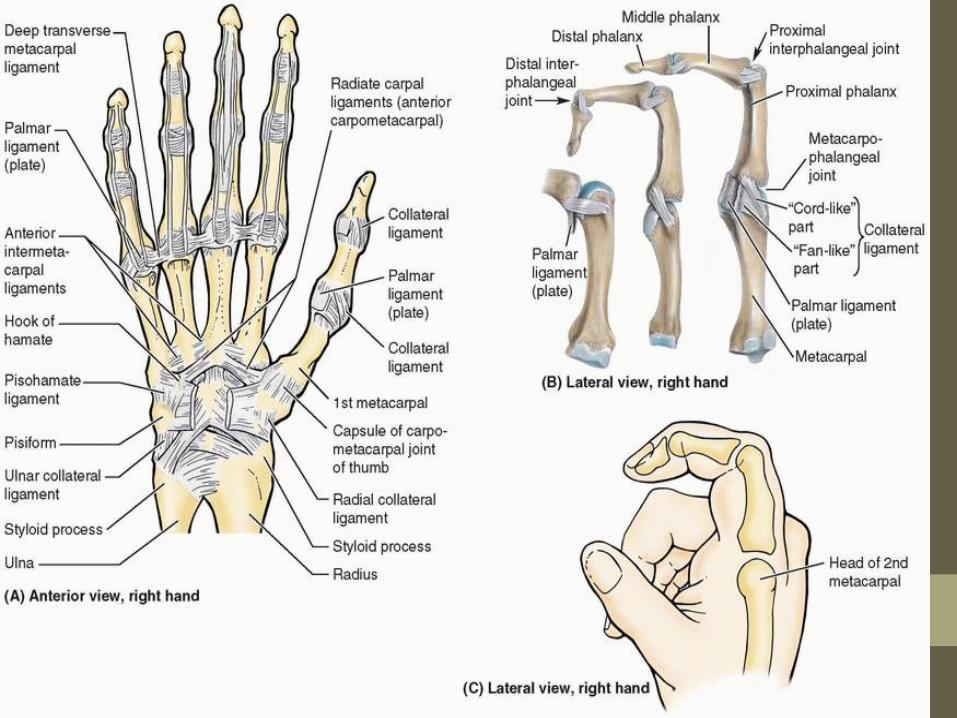
MCP, PIP and DIP joints
• MCP: condyloid joints, allow flexion/extension, abduction/adduction.
• Strengthened by collateral ligaments and palmar ligaments
• IPJ: Hinge, permit flexion and extention only
• Strengthened by collateral ligaments
• Supplied by deep digital arteries and digital nerves
Review Question 1
• Name the 8 carpal bones
• Scaphoid
• Lunate
• Triquetrum
• Pisiform
• Trapezium
• Trapezoid
• Capitate
• Hamate
Muscles of the Upper Limb
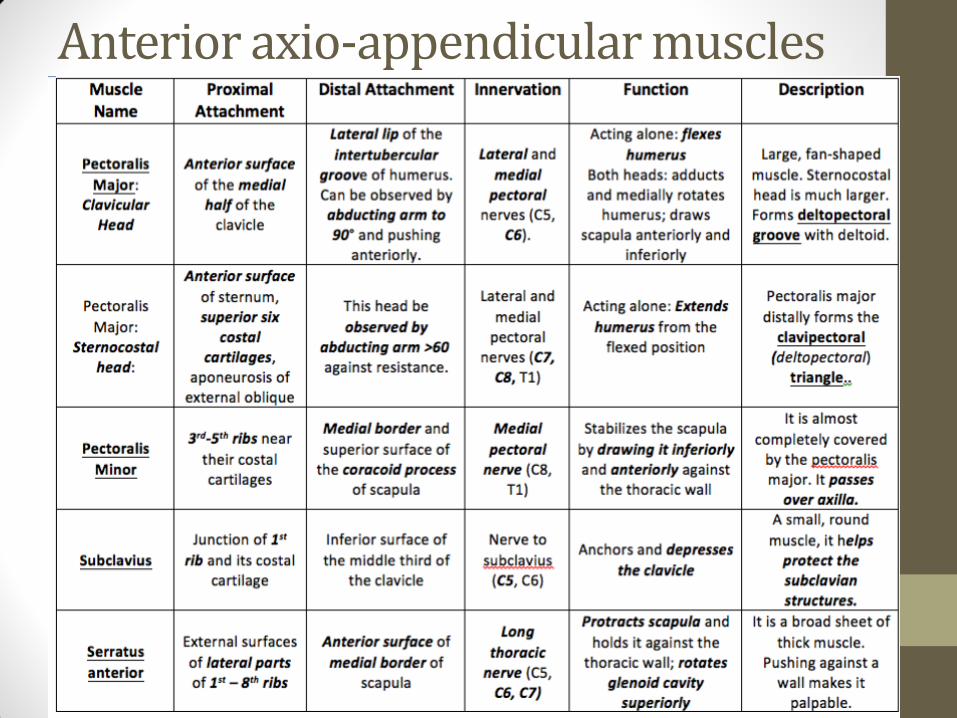
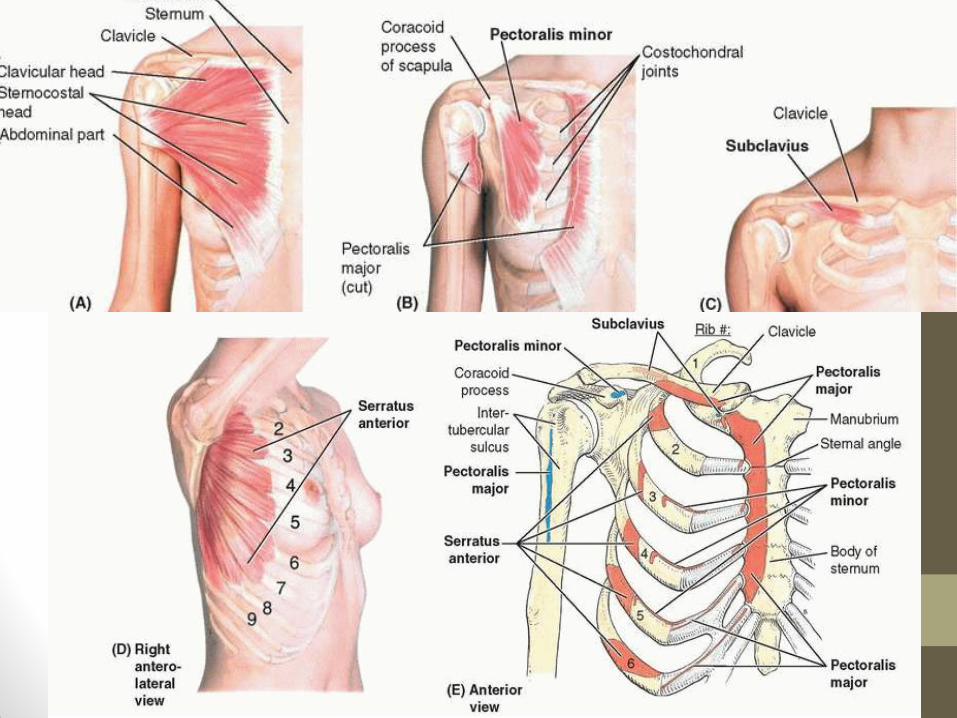
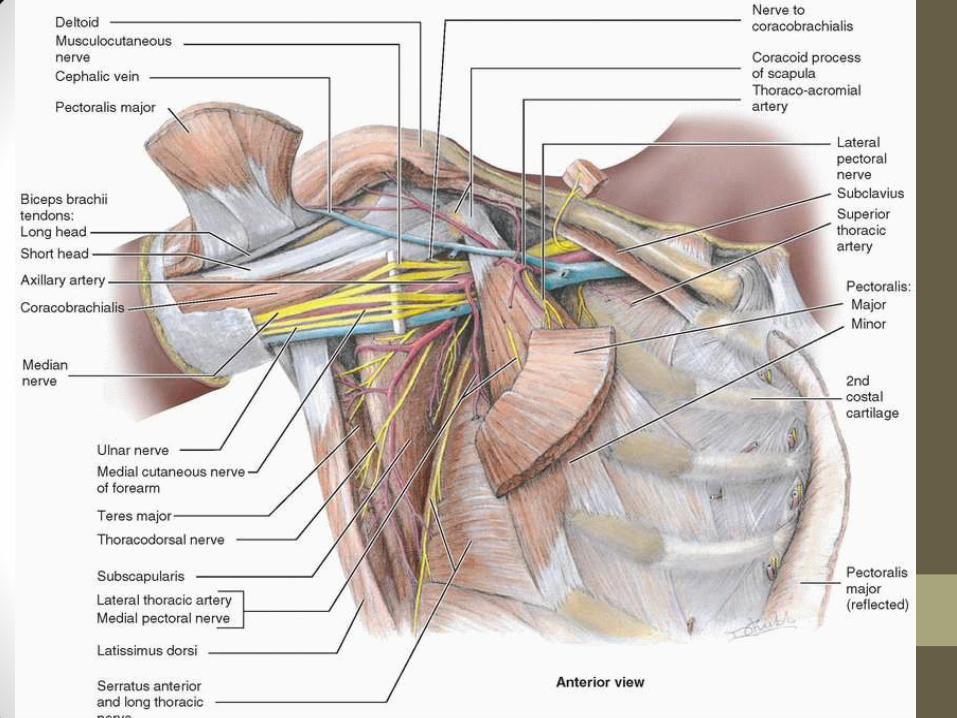
Anterior axio-appendicular muscles
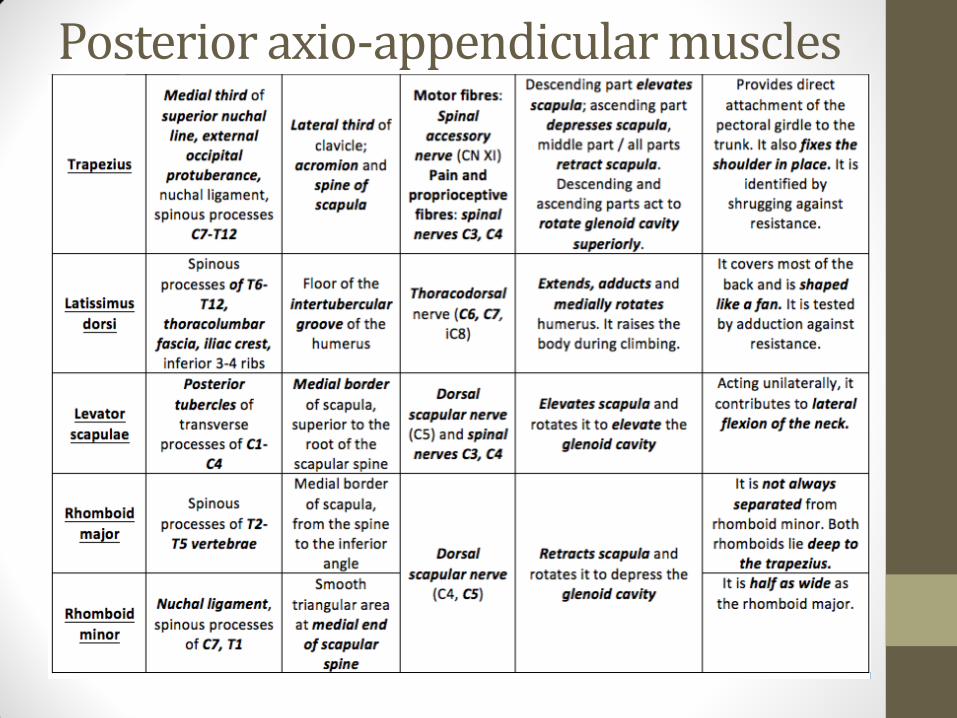
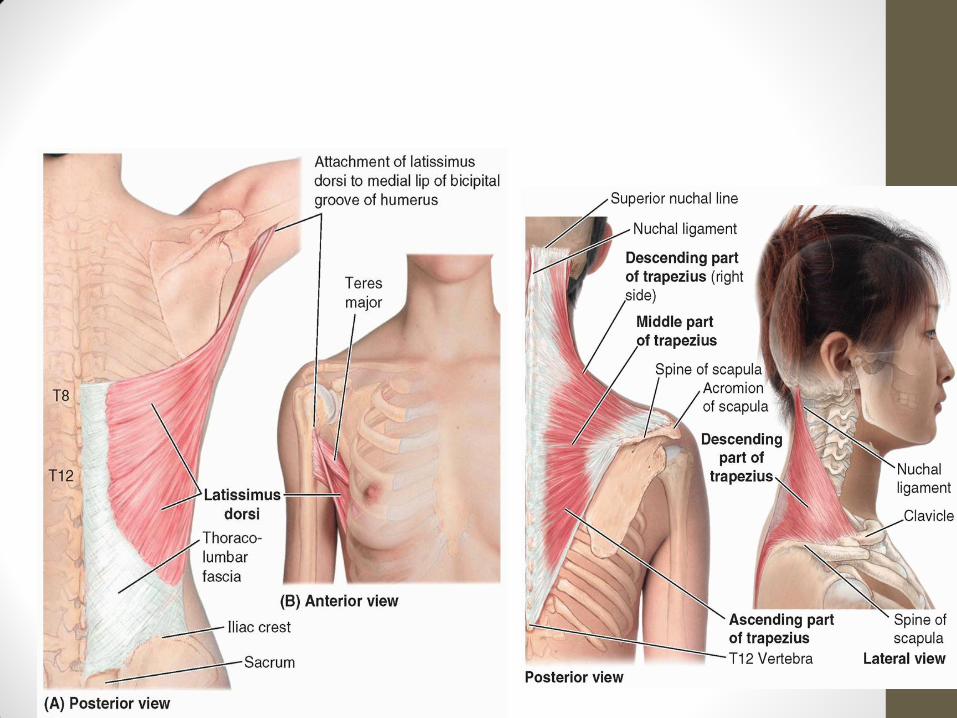
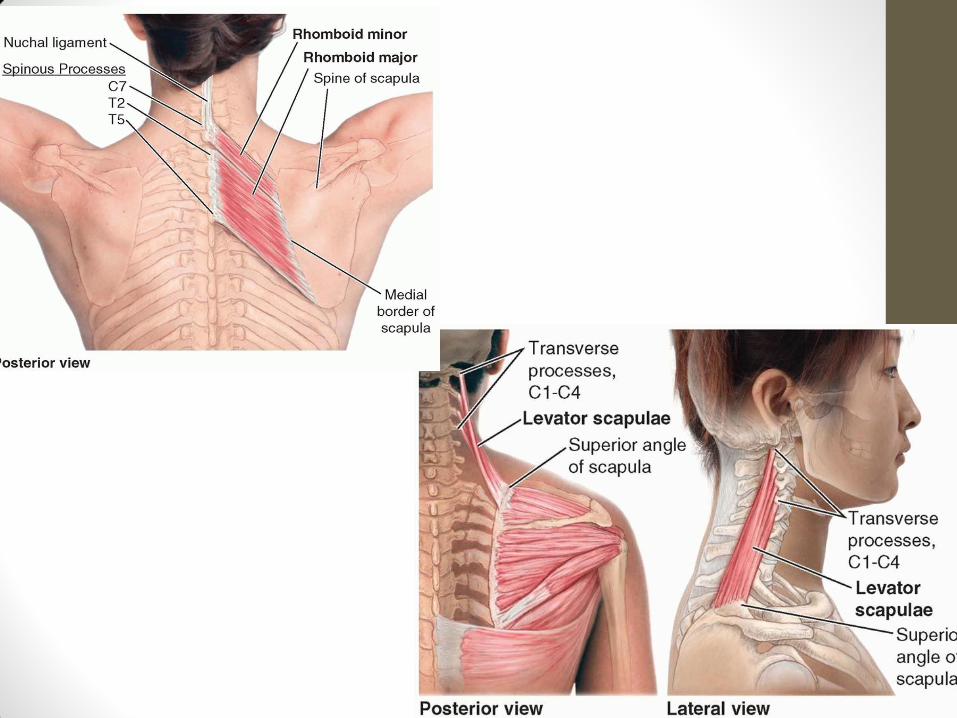
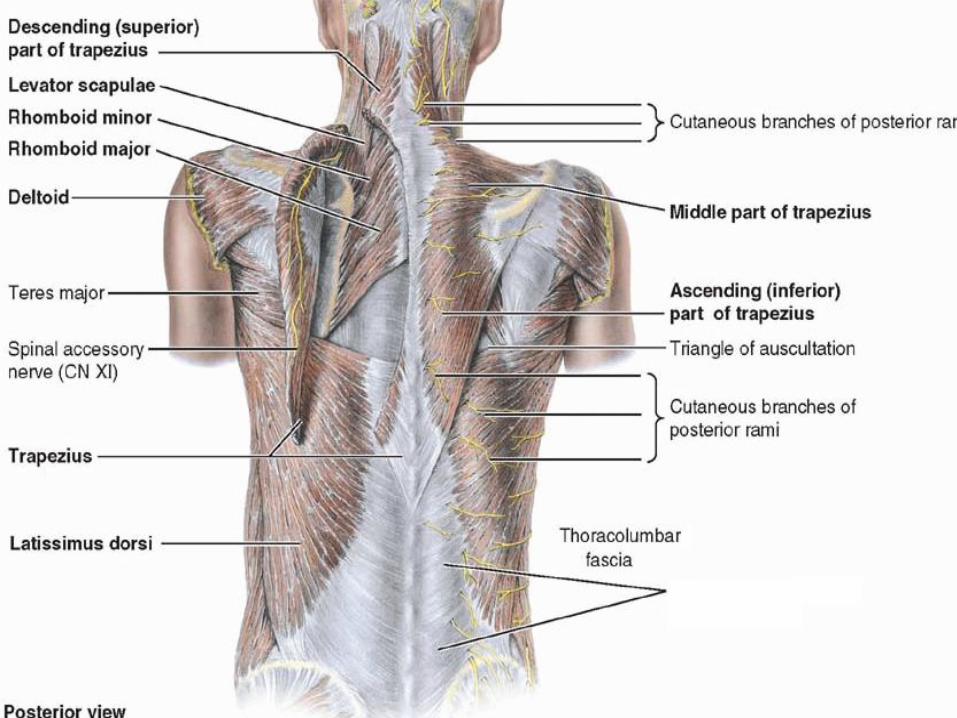
Posterior axio-appendicular muscles
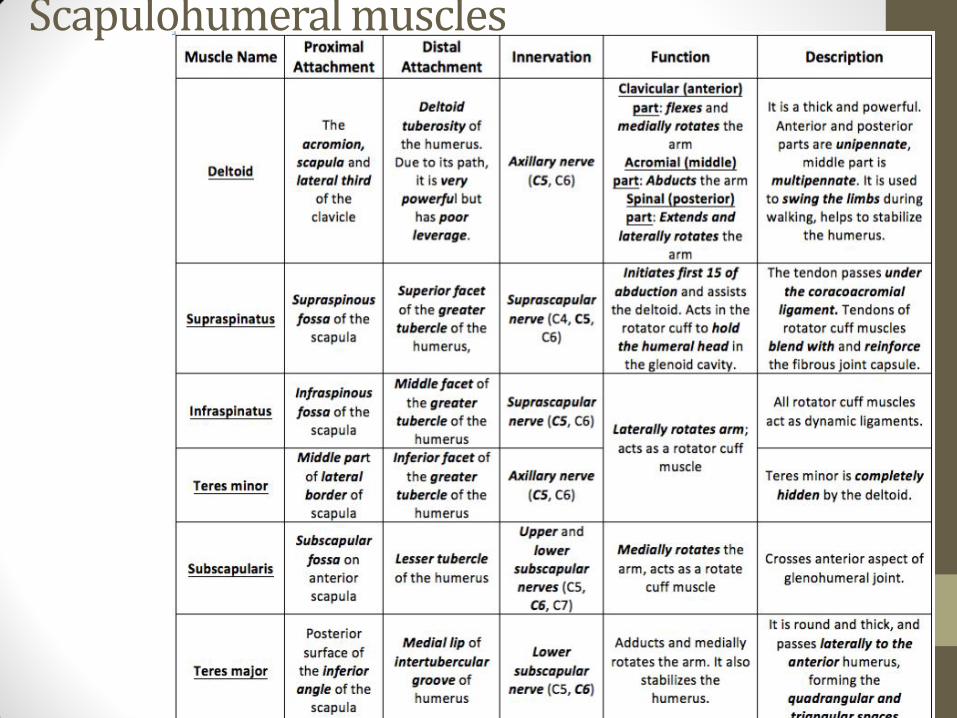
Scapulohumeral muscles