




Muscular System Anatomy and Physiology. Muscular System Functions Movement is the primary function...
114
Muscular System Anatomy and Physiology
-
Upload
alisha-park -
Category
Documents
-
view
223 -
download
4
Transcript of Muscular System Anatomy and Physiology. Muscular System Functions Movement is the primary function...

Muscular System
Anatomy and Physiology
Muscular System Functions
• Movement is the primary function of the muscular system.
• All of this movement (running, chewing, stomach churning etc.) is accomplished through muscle contraction. Muscles pull, they never push.




Other Muscular System Functions
• Holding organs in place. (i.e. Rectus Abdominis)
• Generating heat for warmth.
• Protection • Cushioning.

Skeletal Muscle Tissue
• These muscle cell fibers (muscle cells) are multinucleated.• They can be up to 30 cm in length.• The bands seen in this picture indicate where the myosin and actin fibers overlap
each other• Contraction is voluntary and quick.• Contraction is triggered by nervous system• They are enveloped and anchored to connective tissue.

Smooth Muscle tissue
• Smooth - involuntary, 1 nuclei per cell, no striations, slow rate of contraction
• Found in arterial vessel walls, intestinal walls, alveoli walls

Cardiac Muscle Tissue
• Cardiac Muscle tissue
• Involuntary, 1 or 2 nuclei per cell, intercalated disks (D), striated, quick contraction
• Found only in the Heart
• The heart begins beating from the end of the third week of embryonic development.

Cardiac Muscle Tissue• This is a high power
(400X) view of cardiac tissue.
• See if you can spot the intercalated discs.
• This tissue looks different from skeletal muscle tissue. (Look for branching)
• If cardiac muscle cells are removed from the heart and kept alive in a culture dish they continue to contract rhythmically.
• In the living person the rhythm of the individual cardiac cells is set by the nerve supply to the heart.

Skeletal Muscle Structure• The muscle
fiber is analogous to a muscle cell.
• The cells are arranged in bundles called fasicles.
• The fasicles are arranged in bundles to form a muscle.
• Muscles are arranged together in groups (quadriceps, hamstrings).


• A sarcomere is a contracting unit of a muscle cell fiber.
• There will be hundreds of these repeating units in each muscle cell fiber.
• The striations are caused by the overlapping myosin and actin myofibrils.

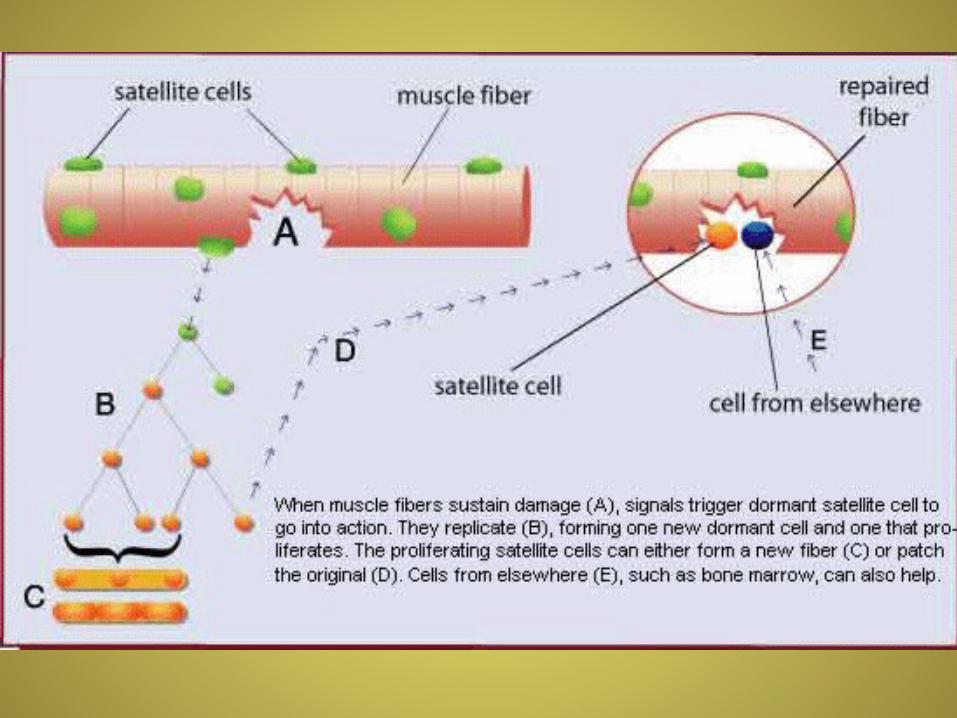
Satellite Cells
New muscle cells form from undifferentiated precursor cells called satellite cells.
This is a way for muscle cells to repair themselves.
Once you are an adult muscle cell fibers cease to multiply.
As a person ages muscle tissue atrophies and is replaced by connective tissue.

A motor unit is a group of muscle cell fibers that are activated by a single neuron.They vary dramatically in size from two to several thousand muscle fibers.
A muscle like the biceps brachii may contain thousands of motor units.

Myoneural Cleft
• Nerve impulses reaching this gap release acetycholine to carry the impulse to the muscle cell fibers
• Acetylcholine causes depolarization of the muscle cell membrane.
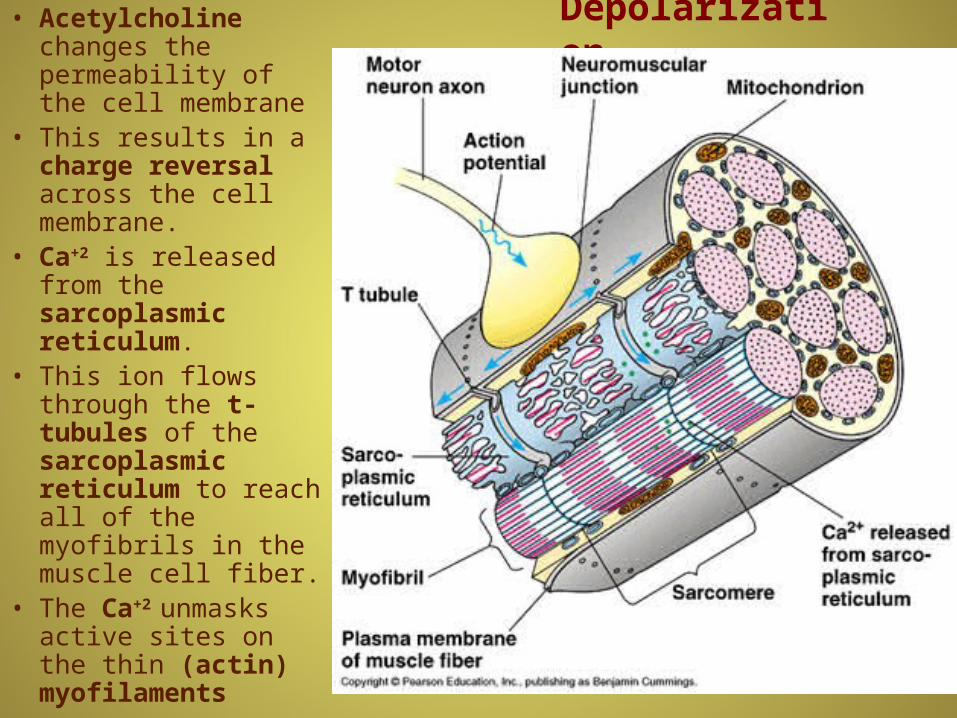
Depolarization• Acetylcholine changes the permeability of the cell membrane
• This results in a charge reversal across the cell membrane.
• Ca+2 is released from the sarcoplasmic reticulum.
• This ion flows through the t-tubules of the sarcoplasmic reticulum to reach all of the myofibrils in the muscle cell fiber.
• The Ca+2 unmasks active sites on the thin (actin) myofilaments



Simple Twitch
• A single depolarization produces a single contraction (simple twitch)
• The strength of a contraction (strength gradation) depends on how many motor units are stimulated.
• Muscles responsible for fine control (i.e. eye movement) have many more motor units.
• A muscle fiber stimulated several times, quickly, produces a sustained (tetanic) contraction.

All Vertebrates have two distinct muscle types of skeletal muscle fibers

ATP
• Utilized as a source of energy muscle cell contraction
• Consists of an organic body plus a tail composed of three phosphate groups.
• The last two phosphate groups are attached by high energy bonds which are readily formed and broken

Creatine phosphate is a long term phosphate storage molecule. It allows for a rapid conversion of ADP to ATP

Acetylcholine• acetylcholine (ACh) is made from acetyl CoA and choline
• ACh is stored in synaptic vesicles
• Nerve impulse releases ACh
• ACh binds to and activates receptor sites.
• ACh is enzymatically broken down by acetylcholinesterase (AChE) located in the synapse.
• Acetylcholine is the neurotransmitter at neuromuscular junctions, synapses in the autonomic nervous system, and at synapses in several parts of the nervous system.


Myoglobin
• Red pigment found in most muscles.
• Stores some O2 for use in muscle contraction.
• Allows muscle to work aerobically for a longer time.


• Energy supply comes from glucose• If broken down aerobically, it yields 36 ATP’s and CO2 and HOH• This process happens slowly.• If not enough O2 is available, glucose broken down anaerobically. • This essentially just splits the glucose molecule in half generating 2 ATP’s and
Lactic acid.• This process happens quickly.

Isotonic Exercise
• This is exercise that involves movement.
• This type of exercise leads to an increase in the supply of blood (number of capillaries) to that muscle and the heart muscle as well.
• This allows the muscle to receive more oxygen and therefore go into oxygen debt later.
Isometric Exercise
• This is exercise without movement.
• Great tension is applied to the muscles.
• This results in increased muscle strength and size.
• It does not increase that muscles or the heart’s vascularity.
• It does burn calories and lower cholesterol.

Muscle Strength and Muscle Power
• Muscle Strength is directly proportional to muscle size.
• The larger a muscle the greater its strength.
• Weightlifters tear muscle cell fibers while they are lifting.
• The muscle cell fibers repair themselves and get larger (hypertrophy) by increasing the number of myofibrils they have.
• Muscle power is the amount of work/time.
• Muscle power is related to how fast the contraction can be accomplished.

Spinach will not make you super strong!

A radioactive Spider bite will not make you super strong!
There is no evidence that being born on another planet will give you super strength.

Being an Amazon does not give you super strength!

Having artificial robotic parts will not make you super strong!

Muscle Atrophy• Muscles respond to use and non-use.
• When a muscle is not used or cannot be used it atrophies and gets smaller.
• Unused muscles can lose as much as 50% of their mass in a month.
• Polio is a viral disease that attacks the nerves in various parts of the body.
• It can lead to paralysis (President Franklin Roosevelt).
• It is now very rare in the US thanks to the Polio vaccine.

Polio• Polio (also called poliomyelitis)
is a contagious, viral disease.
• Historically, it was devastating and has plagued people since ancient times.
• It was virtually eliminated from the Western hemisphere in the second half of the 20th century.
• Its most extensive outbreak occurred in the first half of the 1900s.
• At the height of the polio epidemic in 1952, nearly 60,000 cases with more than 3,000 deaths were reported in the United States alone.
• This is an electron image of a polio virus.

Polio types• In about 95% of cases there are no
symptoms (asymptomatic polio). • In the 4% to 8% of cases in which
there are symptoms (symptomatic polio), the illness appears in three forms.
• A mild form, abortive polio (sickness is limited to flu-like symptoms such as mild upper respiratory infection, diarrhea, fever and sore throat.
• A more serious form associated called nonparalytic polio (1% to 5% show neurological symptoms such as sensitivity to light and neck stiffness)
• A severe, debilitating form called paralytic polio (this occurs in 0.1% to 2% of cases)
Paralytic Polio
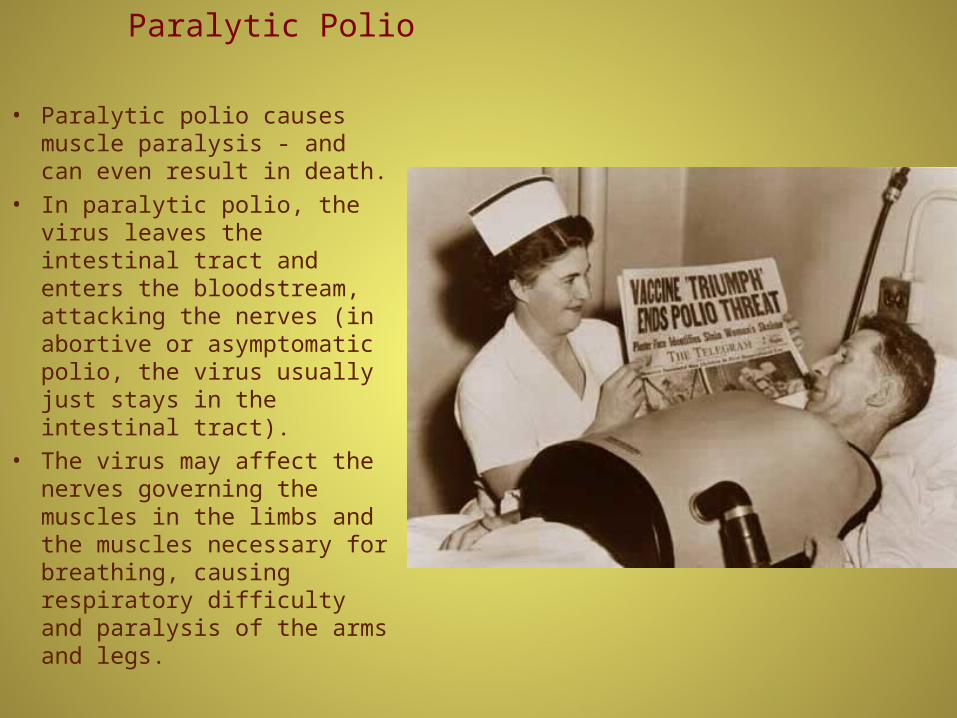
• Paralytic polio causes muscle paralysis - and can even result in death.
• In paralytic polio, the virus leaves the intestinal tract and enters the bloodstream, attacking the nerves (in abortive or asymptomatic polio, the virus usually just stays in the intestinal tract).
• The virus may affect the nerves governing the muscles in the limbs and the muscles necessary for breathing, causing respiratory difficulty and paralysis of the arms and legs.

Contagiousness
• Polio is transmitted primarily through the ingestion of material contaminated with the virus found in stool (poop).
• Not washing hands after using the bathroom and drinking contaminated water were common culprits in the transmission of the disease.

Prevention
• In the US, it's recommended that children have four doses of inactivated polio vaccination (IPV) between the ages of 2 months and 6 years.
• By 1964, the oral polio vaccine (OPV), developed by Albert Sabin, had become the recommended vaccine.
• OPV allowed large populations to be immunized because it was easy to administer, and it provided "contact" immunization.
• This meant that an unimmunized person who came in contact with a recently immunized child might become immune, too.
• The problem with OPV was that, in very rare cases, paralytic polio could develop either in immunized children or in those who came in contact with them.
• The person in the photo is Dr. Jonas Salk developer of the IPV vaccine.

Immunization changes
• Since 1979 (when wild polio was eliminated in the US), the 10 or so cases per year of polio in this country were traced to OPV.
• IPV is a vaccine, made from killed virus, that stimulates the immune system of the body (through production of antibodies) to fight the virus if it comes in contact with it. IPV cannot cause polio.
• In an effort to eradicate all polio, including those cases associated with the vaccine, the Centers for Disease Control and Prevention (CDC) decided to make IPV the only vaccine given in the United States.
• Currently, the CDC and American Academy of Pediatrics (AAP) recommend three spaced doses of IPV given before the age of 18 months, and an IPV booster given between the ages of 4 to 6, when children are entering school.

Original Treatment
• At the height of the epidemic, the standard treatment involved placing a patient with paralysis of the breathing muscles in an "iron lung" - a large machine that actually pushed and pulled the chest muscles to make them work.
• The damaged limbs were often kept immobilized because of the confinement of the iron lung.
• In countries where polio is still a concern, ventilators and some iron lungs are still used.
• Historically, home treatment for paralytic polio and abortive polio with neurological symptoms wasn't sufficient.

Sister Kenny
• Australian born Sister Kenny came to the US in 1940 to help in the treatment of Polio.
• Her method advocated the use of hot packs and consistent movement of the affected limbs by hand.
• This was in direct contrast to the accepted medical practice of keeping the limbs still.
• She was allowed to present her findings at the University of Minnesota.
• Her methods dropped the paralysis rate fro 85% to 15%.
Sister Kenny Institute• In 1942, Kenny established the Sister Kenny Institute in Minneapolis.
• Because of the controversy surrounding her theories, the National Foundation for Infantile Paralysis never supported the Institute.
• They did fund both the training of Kenny therapists in at the University of Minnesota and the staffing of therapists in polio wards.
• The Sister Kenny Institute is now part of Abbott Northwestern Hospital in Minneapolis.
• It is devoted to the rehabilitation of people who suffer from physical limitations because of disease injury, or pain.
• Sister Kenny's methods are still a part of rehabilitative therapy around the world.

Duration
• Although the acute illness usually lasts less than 2 weeks, damage to the nerves lasts a lifetime.
• In the past, some patients with polio never regained full use of their limbs, which would appear withered.
• Those who did fully recover might go on to develop post-polio syndrome (PPS) as many as 30 to 40 years after contracting polio.
• In PPS, the damage done to the nerves during the disease causes an acceleration of the normal, gradual weakness due to aging.

Jack Nicklaus had a mild
form of Polio as a boy.

Alan Alda contracted polio when he was 7. He was given the Sister Kenny treatment and was able to recover almost all of his ability to
move.

Mia Farrow survived polio when she was 5.
The Future of Polio
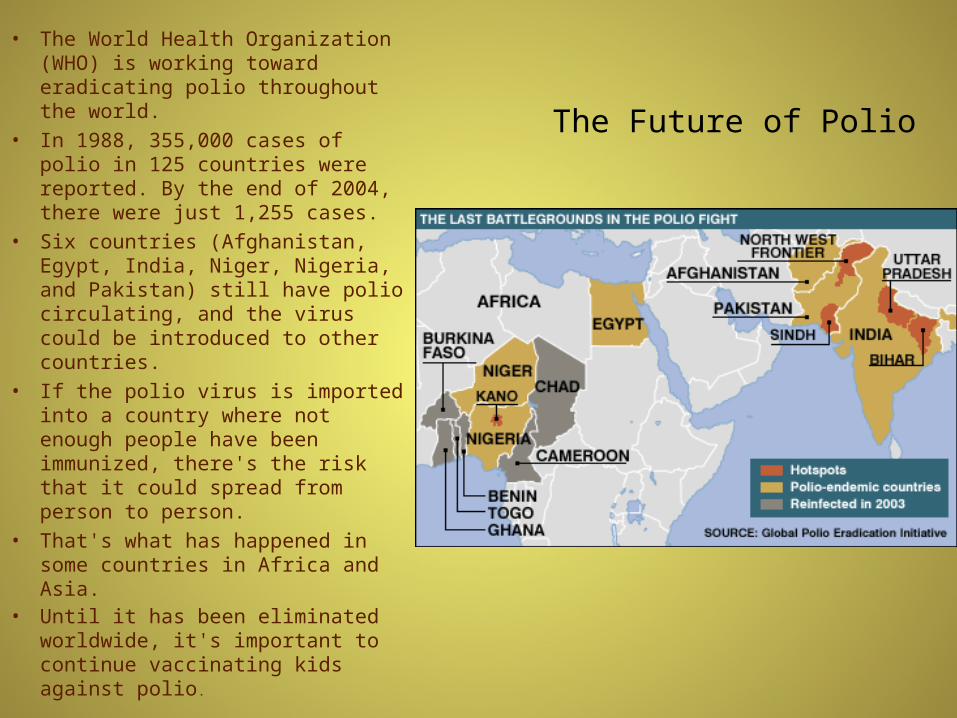
• The World Health Organization (WHO) is working toward eradicating polio throughout the world.
• In 1988, 355,000 cases of polio in 125 countries were reported. By the end of 2004, there were just 1,255 cases.
• Six countries (Afghanistan, Egypt, India, Niger, Nigeria, and Pakistan) still have polio circulating, and the virus could be introduced to other countries.
• If the polio virus is imported into a country where not enough people have been immunized, there's the risk that it could spread from person to person.
• That's what has happened in some countries in Africa and Asia.
• Until it has been eliminated worldwide, it's important to continue vaccinating kids against polio.
Oxygen Debt
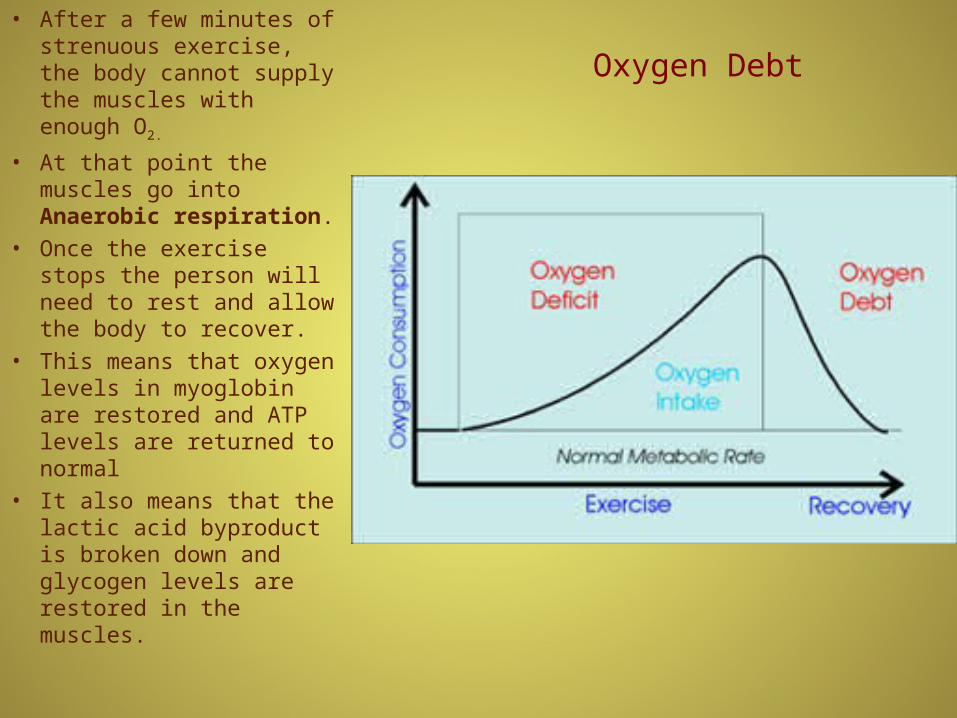
• After a few minutes of strenuous exercise, the body cannot supply the muscles with enough O2.
• At that point the muscles go into Anaerobic respiration.
• Once the exercise stops the person will need to rest and allow the body to recover.
• This means that oxygen levels in myoglobin are restored and ATP levels are returned to normal
• It also means that the lactic acid byproduct is broken down and glycogen levels are restored in the muscles.

Muscle factoids
• 600 or so muscles in the body.
• 40% of body weight. (skeleton is 20%)
• Muscles can contract only 45% of their length. So the longer the muscle the more contraction is possible!
• Origins generally broader than insertions.
• Limbs of the body taper toward the ends with the muscles located far away from the fingers and toes.
• In some cases muscles cross 2 joints which allows them to do two jobs with one contraction.

Gross Anatomy
• The origin of a muscle is the attachment point that is not moved.
• The insertion of a muscle is the attachment point that is moved.
• The middle of the muscle is often referred to as the belly of the muscle.

Muscle Antagonists
• Muscles are arranged in opposing pairs.
• This allows one member of a pair to undo what the other does.
• It also permits fine motor control and smoother arm movement.
• In this example the triceps brachii undoes the action of the biceps brachii.

Synergists
• Many muscles are not directly responsible for a movement.
• Instead they help maintain joint stability during a movement.
• These muscles are called synergists.
• They are often found by the hip and the shoulder.
• The Gluteus medius plays an important role in stabilizing the trunk in the upright position when the opposite foot leaves the ground as in walking and running.

Prime Movers
• Prime movers are responsible for a main body movement.
• The Gastrocnemius functions in flexing the foot.
• It allows people to stand on their tip-toes.
• It attaches to the calcaneus bone via the achilles tendon.
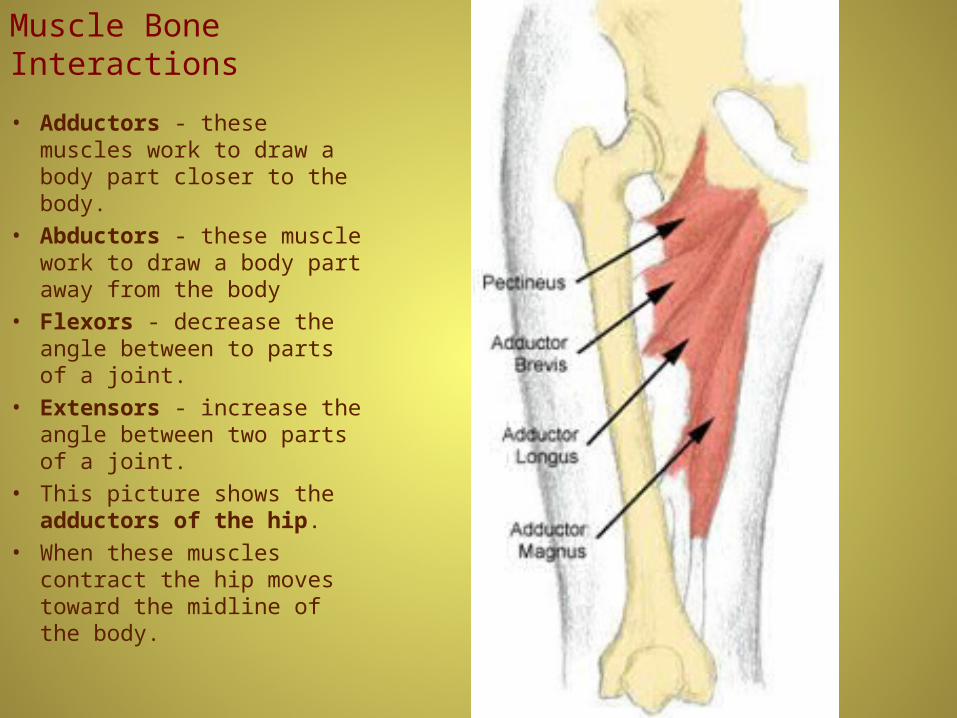
Muscle Bone Interactions
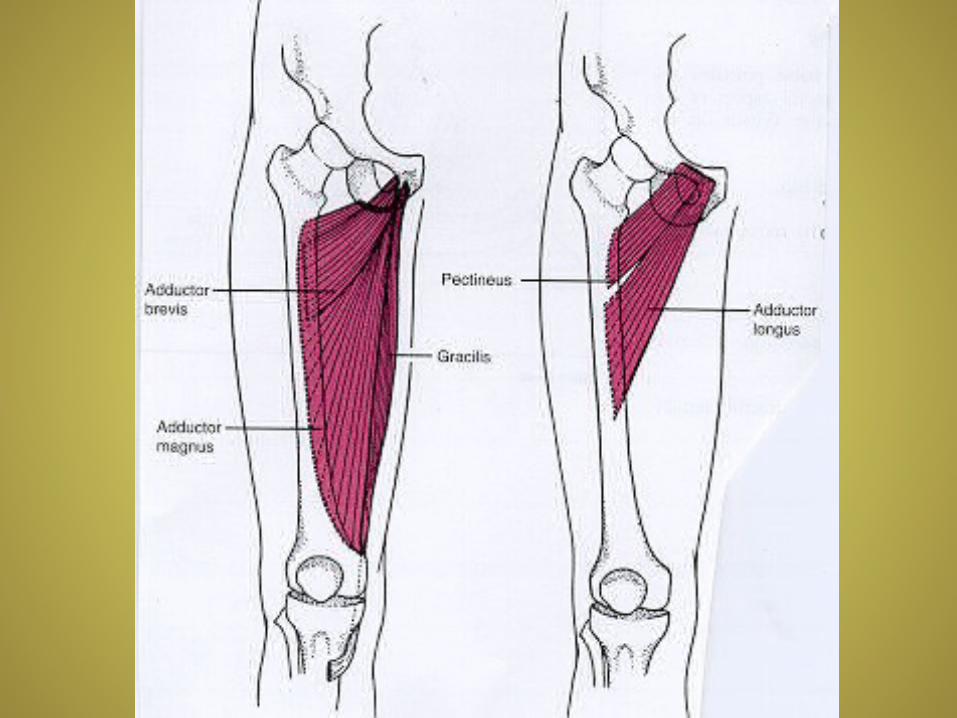
• Adductors - these muscles work to draw a body part closer to the body.
• Abductors - these muscle work to draw a body part away from the body
• Flexors - decrease the angle between to parts of a joint.
• Extensors - increase the angle between two parts of a joint.
• This picture shows the adductors of the hip.
• When these muscles contract the hip moves toward the midline of the body.
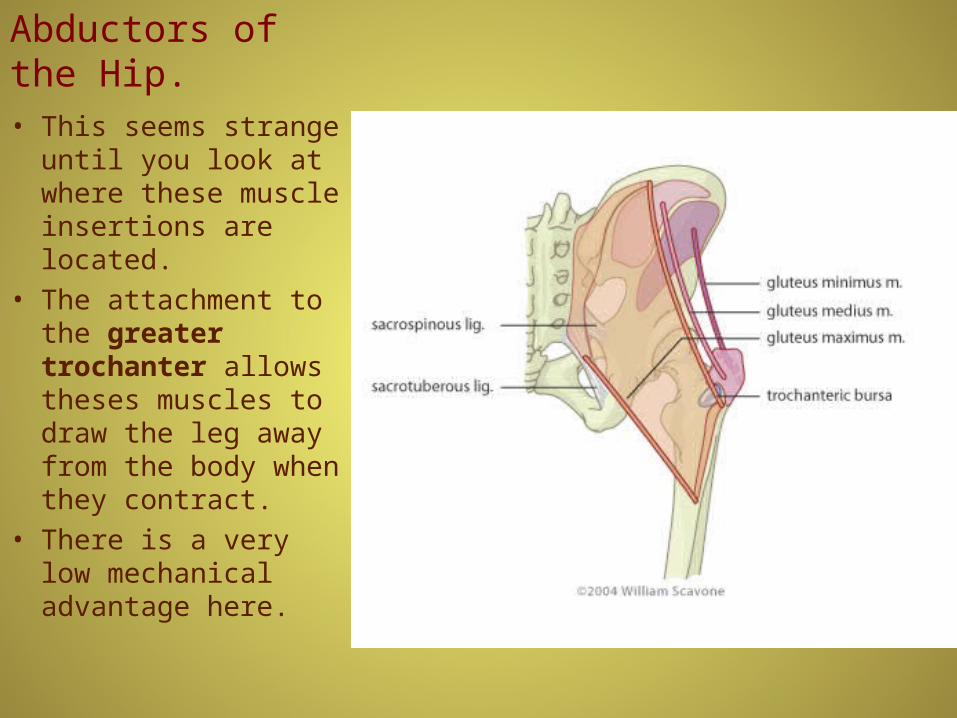
Abductors of the Hip.
• This seems strange until you look at where these muscle insertions are located.
• The attachment to the greater trochanter allows theses muscles to draw the leg away from the body when they contract.
• There is a very low mechanical advantage here.
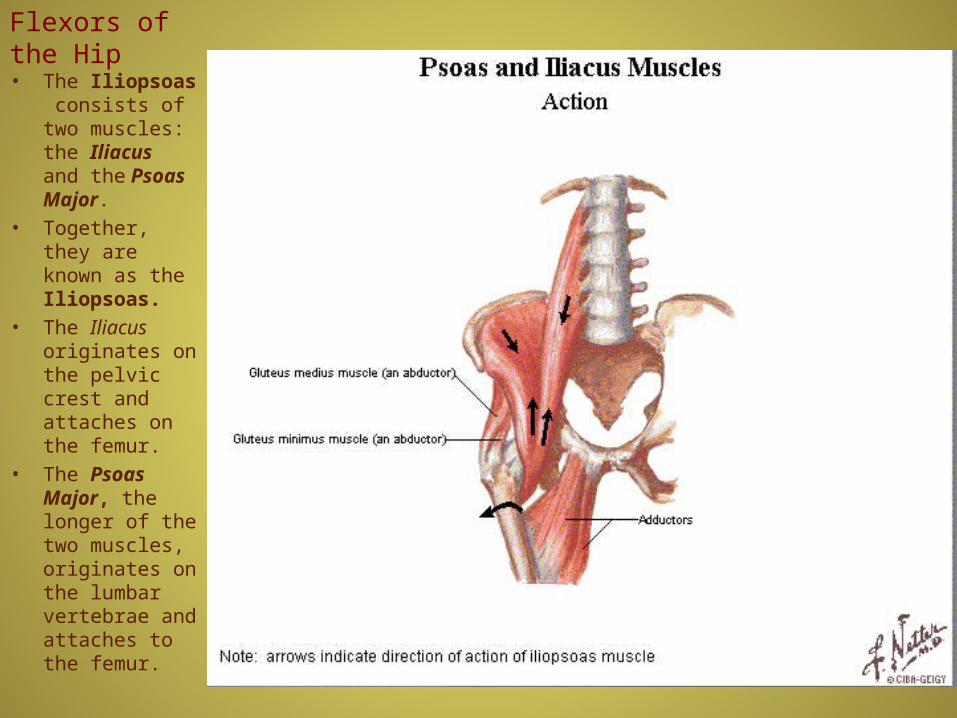
Flexors of the Hip
• The Iliopsoas consists of two muscles: the Iliacus and the Psoas Major.
• Together, they are known as the Iliopsoas.
• The Iliacus originates on the pelvic crest and attaches on the femur.
• The Psoas Major, the longer of the two muscles, originates on the lumbar vertebrae and attaches to the femur.
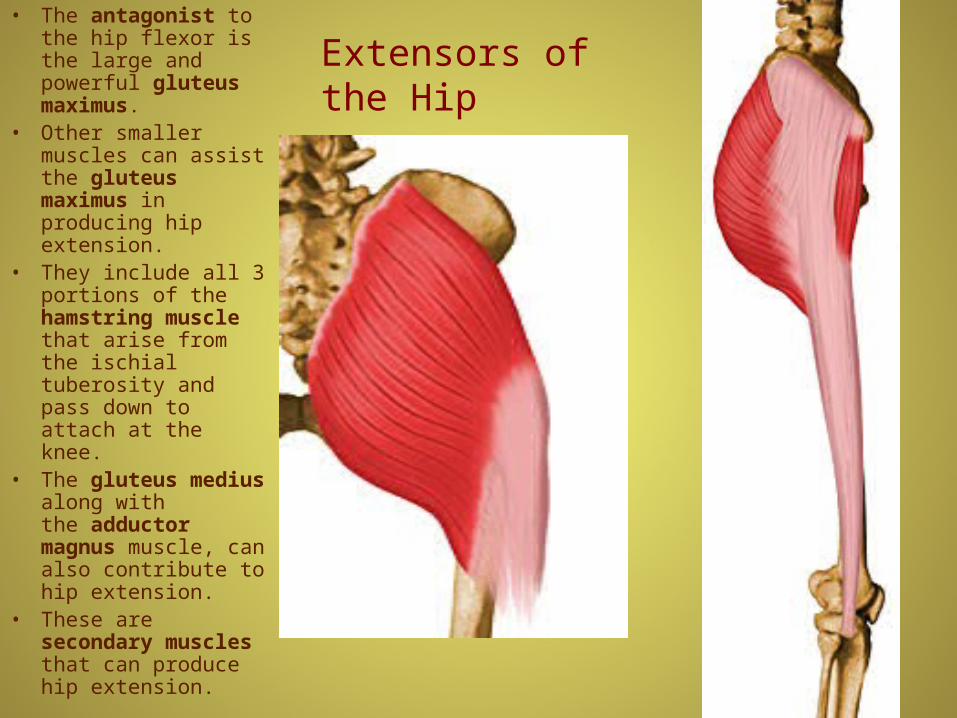
Extensors of the Hip• The antagonist to the
hip flexor is the large and powerful gluteus maximus.
• Other smaller muscles can assist the gluteus maximus in producing hip extension.
• They include all 3 portions of the hamstring muscle that arise from the ischial tuberosity and pass down to attach at the knee.
• The gluteus medius along with the adductor magnus muscle, can also contribute to hip extension.
• These are secondary muscles that can produce hip extension.

Quadriceps• The quadriceps
“muscle” is actually a group of four large muscles that merge just above the knee.
• These muscles are the prime movers in the extension of the knee.
• The also help to stabilize the knee.
• It is these muscles that people work hard to strengthen after knee surgery.
• The Rectus femoris is the only one of the group that crosses the hip joint as well as the knee.
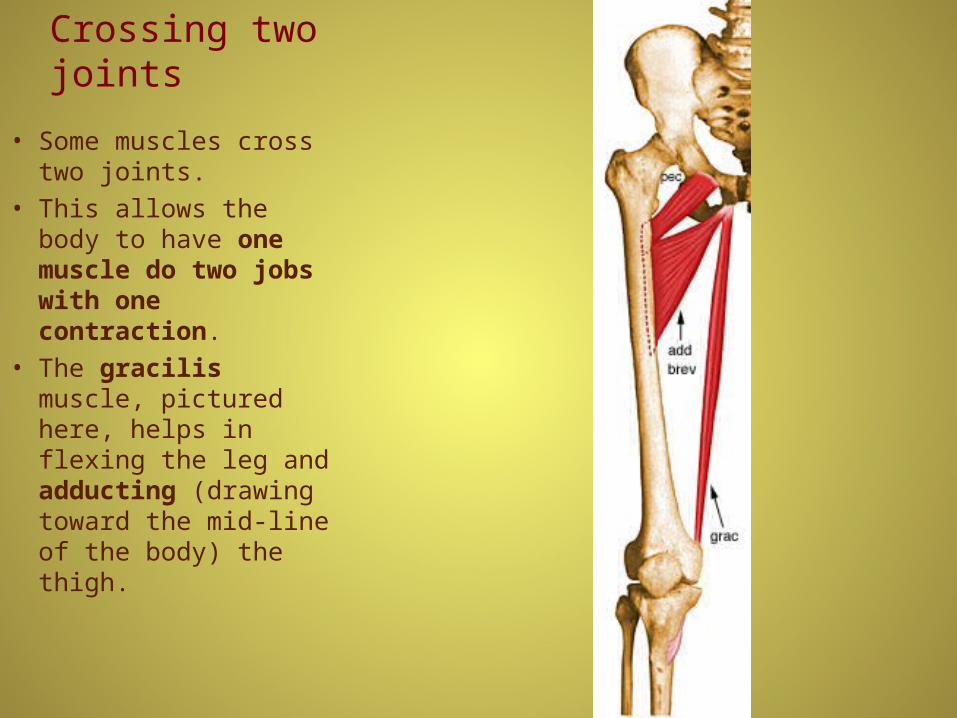
Crossing two joints
• Some muscles cross two joints.
• This allows the body to have one muscle do two jobs with one contraction.
• The gracilis muscle, pictured here, helps in flexing the leg and adducting (drawing toward the mid-line of the body) the thigh.

Another double crosser
• The Sartorius muscle is another muscle that crosses two joints.
• With one contraction it helps to flex the knee and the thigh at the hip.
• It also abducts and laterally rotates the thigh.
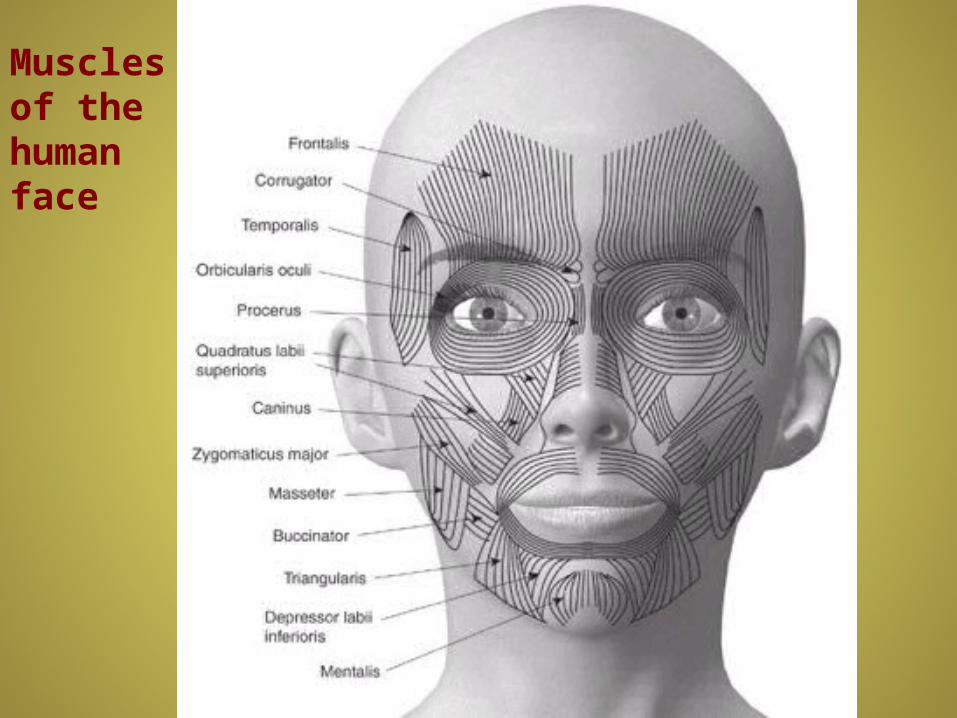
Muscles of the human face

Muscle Tone
• Muscle tone is the constant state of partial muscle contraction that many muscles have.
• This is especially important in muscles like the rectus abdominus in which one of its functions is to hold the abdominal organs in place.
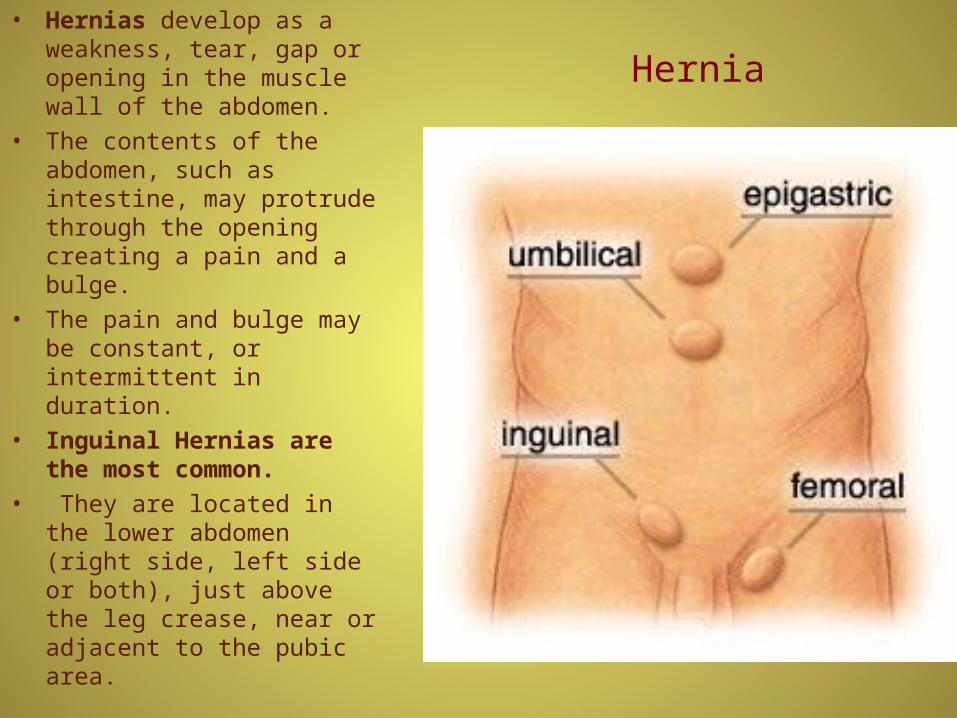
Hernia
• Hernias develop as a weakness, tear, gap or opening in the muscle wall of the abdomen.
• The contents of the abdomen, such as intestine, may protrude through the opening creating a pain and a bulge.
• The pain and bulge may be constant, or intermittent in duration.
• Inguinal Hernias are the most common.
• They are located in the lower abdomen (right side, left side or both), just above the leg crease, near or adjacent to the pubic area.
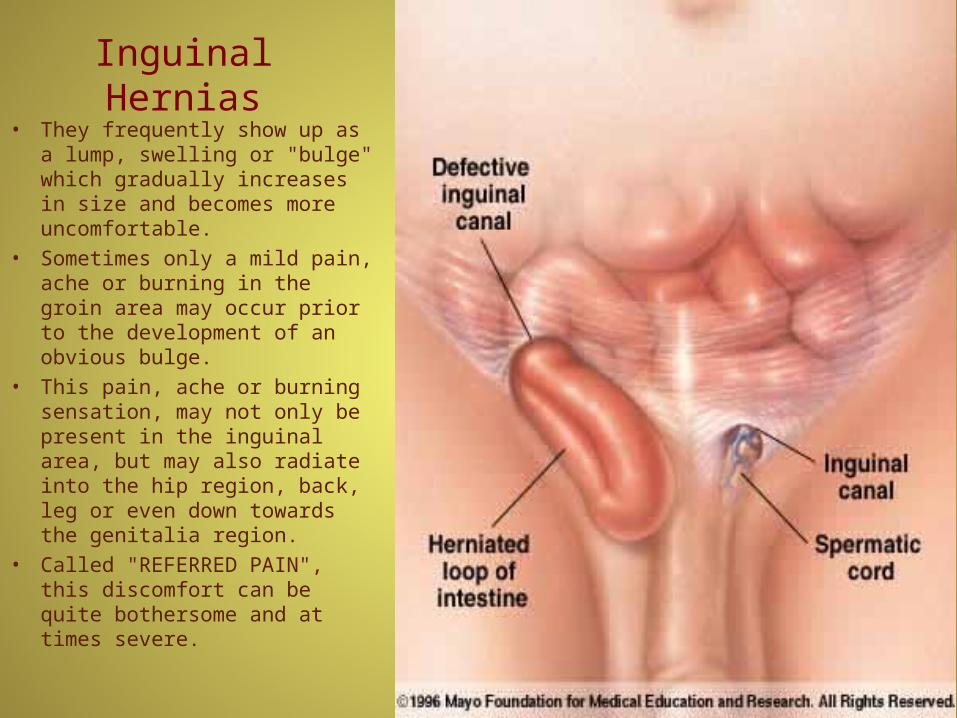
Inguinal Hernias
• They frequently show up as a lump, swelling or "bulge" which gradually increases in size and becomes more uncomfortable.
• Sometimes only a mild pain, ache or burning in the groin area may occur prior to the development of an obvious bulge.
• This pain, ache or burning sensation, may not only be present in the inguinal area, but may also radiate into the hip region, back, leg or even down towards the genitalia region.
• Called "REFERRED PAIN", this discomfort can be quite bothersome and at times severe.

Hernia Repair
• A sterile mesh is carefully placed under the hernia defect.
• The mesh covers not only the hernia, but also reinforces an area of ever-present thinned and weaken tissue that surrounds all hernias.
• The Myopectineal Orifice, is fully supported in this approach.
• The sterile mesh acts as a "lattice", "growth bed" or "scaffolding" for new tissue growth.
• Growth will not only continue to 'heal' the defect further with time, but will go on to allow full incorporation of the mesh, safely and comfortably, into the muscle wall itself.
• The mesh is thin, pliable and flexible and the patient is totally unaware of its presence.
• Activity is not limited after hernia surgery.

Muscle strain
• Muscle strain or muscle pull or even a muscle tear implies damage to a muscle or its attaching tendons.
• You can put undue pressure on muscles during the course of normal daily activities, with sudden, quick heavy lifting, during sports, or while working

Muscle Strain cont.• The tearing of the muscle can also damage small blood vessels, causing local bleeding (bruising) and pain.
• Most muscle strains can be treated with the RICE protocol. RICE stands for Rest, Ice, Compression, and Elevation.
• Rest: You may need to use crutches to avoid putting weight on a strained leg.
• Ice: Do not apply ice directly to the skin, but you can use cold packs for 20 minutes at a time, several times a day.
• Compression: To prevent additional swelling and blood loss, wear an elastic compression bandage.
• Elevation: To minimize swelling, keep your leg up higher than your heart.
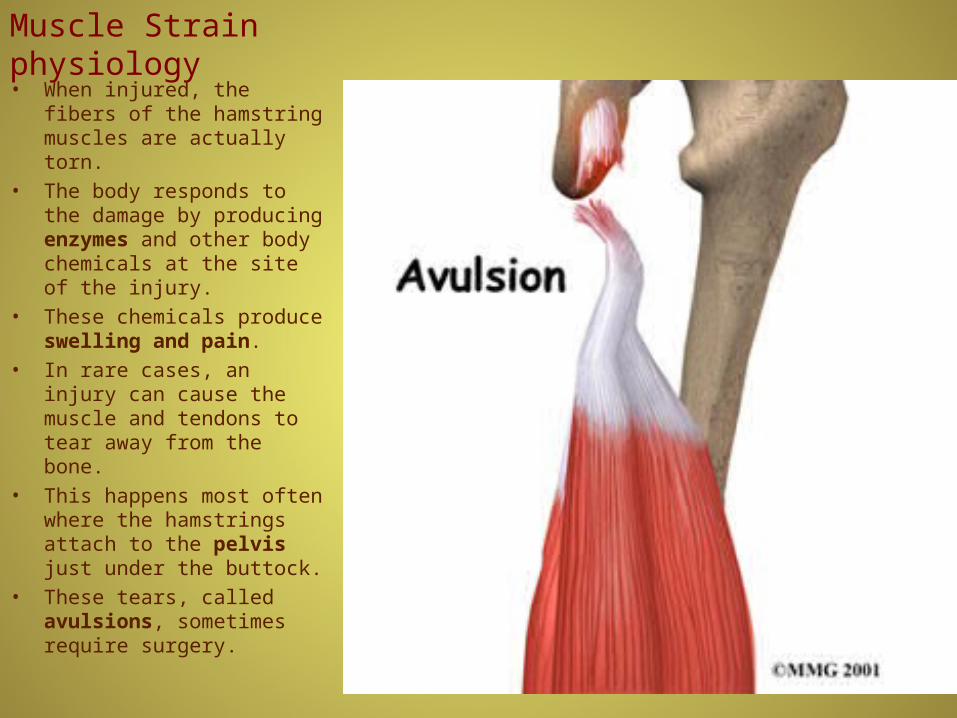
Muscle Strain physiology
• When injured, the fibers of the hamstring muscles are actually torn.
• The body responds to the damage by producing enzymes and other body chemicals at the site of the injury.
• These chemicals produce swelling and pain.
• In rare cases, an injury can cause the muscle and tendons to tear away from the bone.
• This happens most often where the hamstrings attach to the pelvis just under the buttock.
• These tears, called avulsions, sometimes require surgery.
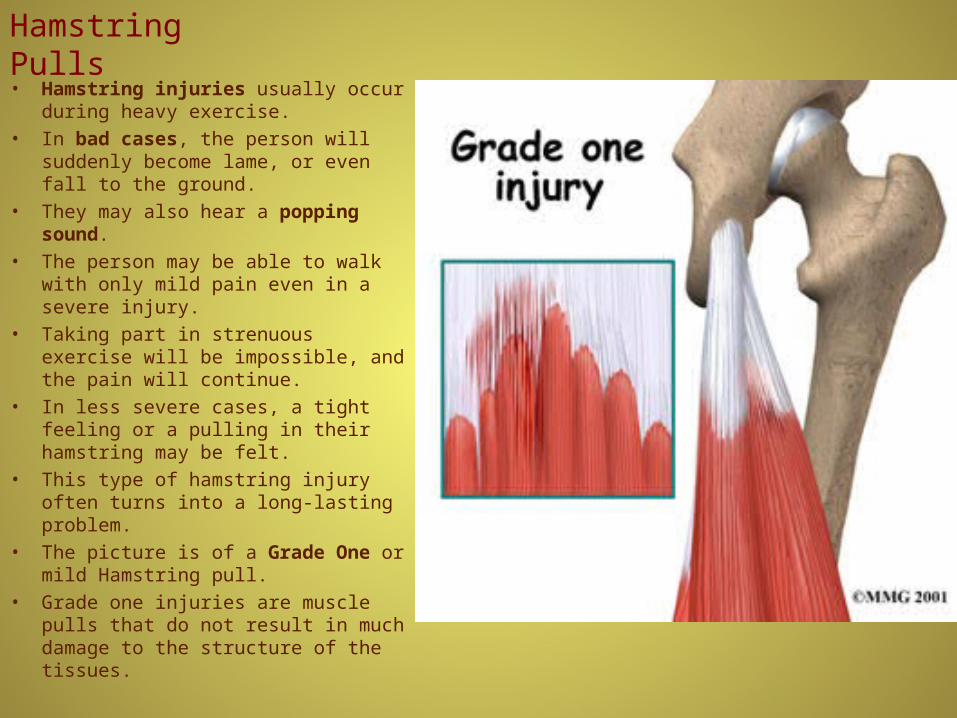
Hamstring Pulls
• Hamstring injuries usually occur during heavy exercise.
• In bad cases, the person will suddenly become lame, or even fall to the ground.
• They may also hear a popping sound.
• The person may be able to walk with only mild pain even in a severe injury.
• Taking part in strenuous exercise will be impossible, and the pain will continue.
• In less severe cases, a tight feeling or a pulling in their hamstring may be felt.
• This type of hamstring injury often turns into a long-lasting problem.
• The picture is of a Grade One or mild Hamstring pull.
• Grade one injuries are muscle pulls that do not result in much damage to the structure of the tissues.
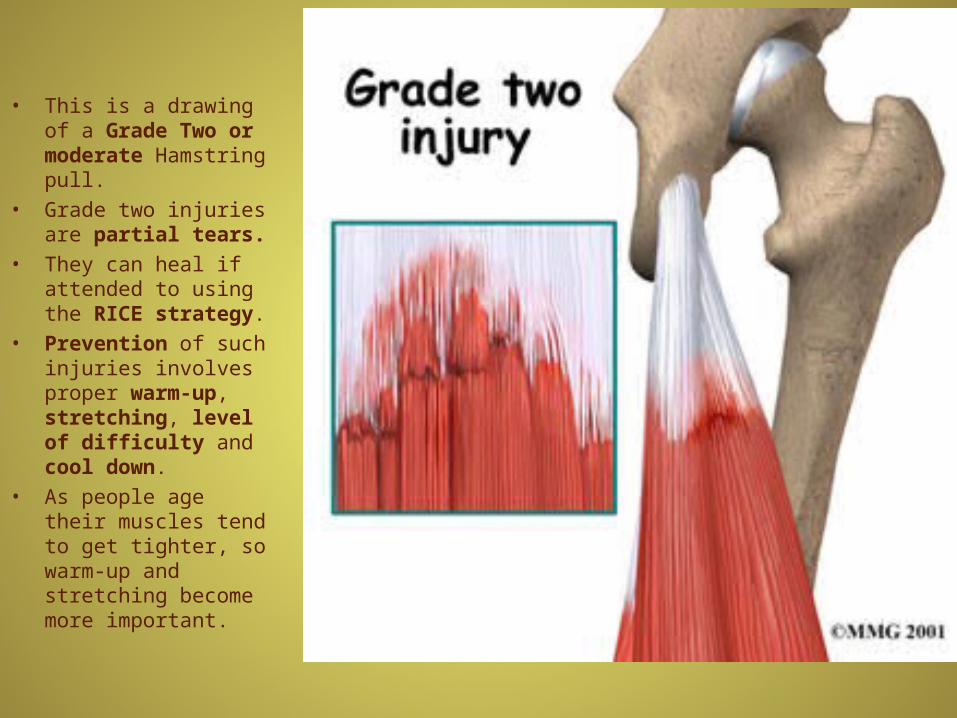
• This is a drawing of a Grade Two or moderate Hamstring pull.
• Grade two injuries are partial tears.
• They can heal if attended to using the RICE strategy.
• Prevention of such injuries involves proper warm-up, stretching, level of difficulty and cool down.
• As people age their muscles tend to get tighter, so warm-up and stretching become more important.

• Grade three injuries are complete tears.
• Along with RICE ibuprofen often prescribed, to help relieve the swelling and pain.
• For many muscle injuries, pain relief may be the major benefit of ibuprofen.
• Surgery will be required to reconnect the hamstring if there is a complete rupture.
• Orthopaedic surgeons perform this type of surgery.
• After surgery, there will be a period of rest, which may involve using crutches.
• A physical therapist will work with the patient to help them learn exercises for rehabilitation after surgery.

Other Ruptured Muscles• It is rare, but possible for part of other muscles, besides the hamstrings to completely tear.
• The same initial treatment is applied, RICE.
• This photo shows a tear in one of the Quadriceps muscles.
• Many muscle tears of this severity need to be repaired surgically.

Tendon Rupture
• A tendon is the fibrous tissue that attaches muscle to bone in the human body.
• The forces applied to a tendon may be more than 5 times your body weight.
• In some rare instances, tendons can snap or rupture.
• Conditions that make a rupture more likely include the injection of steroids into a tendon, certain diseases (such as gout or hyperparathyroidism), and having type O blood.

Tendon rupture
• Although uncommon, a tendon rupture can be a serious problem and may result in excruciating pain and permanent disability if untreated.
• Each type of tendon rupture has its own signs and symptoms and can be treated either surgically or medically depending on the severity of the rupture.

Tendon rupture
• Achilles tendon ruptures are very serious.
• They usually need surgery and extensive physical therapy.
• This athlete may well need an entire year to heal.

Muscular dystrophy
• A group of genetic diseases characterized by progressive weakness of the skeletal muscles.
• There are many forms of the disease.
• Duchenne, which primarily affects young boys, is the most common.
• There is no cure but the patient can receive therapy to improve their quality of life.

Muscular Dystrophy cont.
• It was shown that DMD is due to a gene defect on the X chromosome.
• Normally the gene enables muscle fibers to make a protein called dystrophin.
• Muscle fibers in people affected with DMD are deficient in dystrophin.
• Dystrophin plays a role as part of a large complex in muscle fiber membranes.
• When dystrophin is missing it leads to degeneration of muscle tissue.
• When the muscles ability to regenerate is exhausted, muscle wasting occurs.
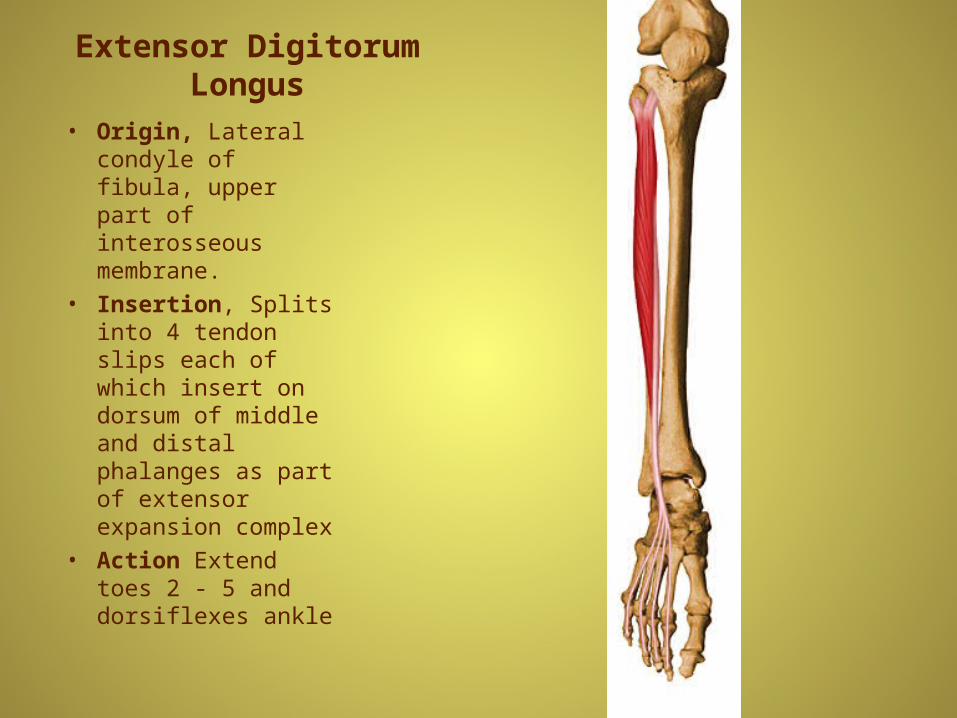
Extensor Digitorum Longus
• Origin, Lateral condyle of fibula, upper part of interosseous membrane.
• Insertion, Splits into 4 tendon slips each of which insert on dorsum of middle and distal phalanges as part of extensor expansion complex
• Action Extend toes 2 - 5 and dorsiflexes ankle

Extensor hallucis longus
• Origin: middle portion of tibia: interosseous membrane between tibia and fibula.
• Action: Extends great toe and dorsiflexes the foot.
• Innervation: Peroneal nerve.
• Comments: It fibers of origin may be fused with those of extensor digitorum longus.

Flexor Digitorum Longus
• Origin, Posterior surface of tibia distal to popliteal line
• Insertion, Splits into four slips after passing through medial intermuscular septum of plantar surface of foot; these slips then insert on plantar surface of bases of 2nd - 5th distal phalanges
• Action; Flexes toes 2 - 5; also helps in plantar flexion of ankle

Flexor hallucis longus• Origin; inferior portion of fibula.
• Action: Flexes Great toe and plantar-flexes foot.
• Innervation: Tibial nerve
• Comments: A deep muscle that inserts upon the distal phalanx of the great toe.
• The x’es in the diagram mark places of pain that are associated with muscle strain for those muscles.

Peroneus Longus
• Origin; Head of fibula, upper 1/2 - 2/3 of lateral fibular shaft surface.
• Insertion; Plantar posterolateral aspect of medial cuneiform and lateral side of 1st metatarsal base
• Action; Everts foot and plantar flexes ankle; also helps to support the transverse arch of the foot

Tibialis Anterior
• Origin; Lateral condyle of tibia, proximal 1/2 - 2/3 or lateral surface of tibial shaft, interosseous membrane, and the deep surface of the fascia cruris
• Insertion; Medial and plantar surfaces of 1st cuneiform and on base of first metatarsal
• Action; Dorsiflexor of ankle and invertor of foot

Plantaris
• Origin; Inferior aspect of lateral supracondylar line of distal femur
• Insertion; Middle 1/3 of the posterior calcaneal surface, just medial to Achilles tendon
• Action; Plantar flexor of ankle; also flexes knee

Biceps Femoris - Long Head
• Origin, Long head from common tendon with semitendinosus from the ischial tuberosity; short head from lateral lip of linea aspera, lateral supracondylar ridge of femur, and lateral intermuscular septum of thigh
• Insertion Primarily on fibular head; also on lateral collateral ligament and lateral tibial condyle
• Action Flexes the knee, and also rotates the tibia laterally; long head also extends the hip joint






Name the numbered muscles

Name the numbered muscles
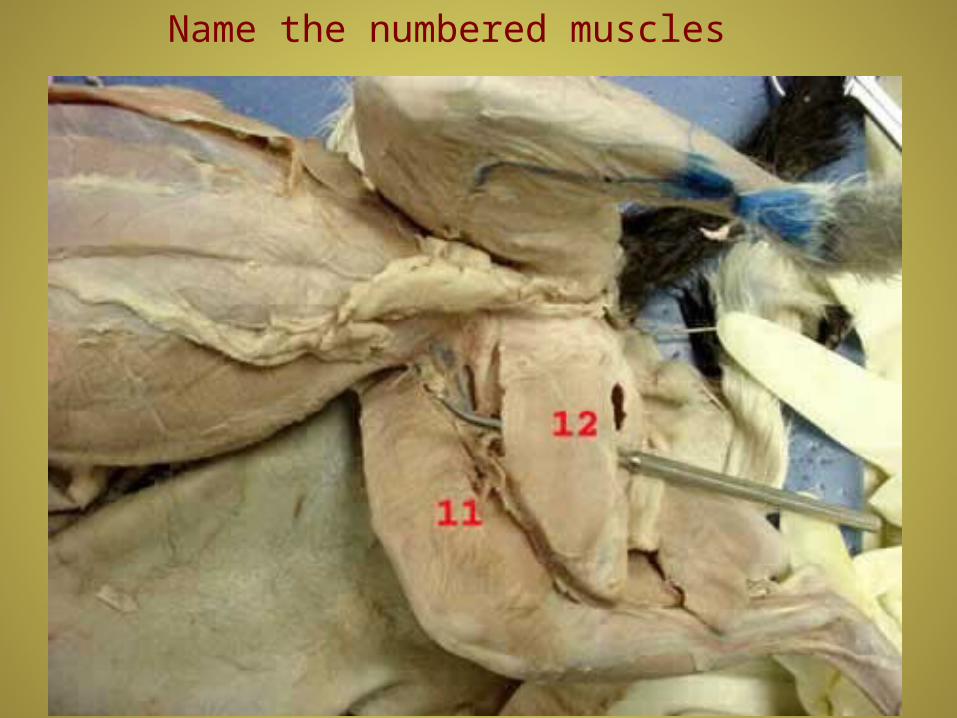
Name the numbered muscles

Name the numbered muscles
Performance Enhancing Drugs• Athletes feel pressure to run faster, jump higher or swim stronger.
• Many turn to performance-enhancing drugs to fuel their competitive edge.
• Anabolic Steroids are drugs that are similar to the male sex hormone, testosterone.
• They can make your muscles bulk up.
• They can make teen girls develop male characteristics, including smaller breasts, a deeper voice, irregular periods and excess facial and body hair.
• Steroids can also make pimples pop up, hair fall out and send you on aggressive, violent rampages dubbed "roid rages"