Genomes & Developmental Control Myogenic regulatory factors Myf5
Upload
conrad-houstonCategory
view
219download
0
MUSCLES DISORDERSMUSCLES DISORDERS
Definition:
Diseases involving the muscle fibers (myogenic)Unlike: neuronopathies: secondary to LMN Heterogenous etiology, genotype, phenotype…
Devastating evolution…No specific treatment for most of them


Myoblasts fusing to form large multi-nucleate muscle cells






white = fast (speed)
red = slow (endurance)

They move independently.
If so how do the individual myosin heads avoid interfering with each other?
They move together like oars on a 8 oar rowing shell, or the multiple oars of a Roman ship
How do the myosin heads coordinate How do the myosin heads coordinate to slide the actin filament?to slide the actin filament?

ATP dependent Calcium pump = Ca++ ATPase pumps calcium from the cytoplasm surrounding the sarcomers back into sarcoplasmic reticulum


Clinical: Muscle weakness: main feature
Gower’s sign (proximaly dominating deficit)
Contractures +/- severe: advanced stagesPain: in inflamm. Disorders onlyAtrophy (+/- pseudohypertrophy in X-linked) Deformity: advanced diseaseDTR: normal, diminished or absentTone: slightly or normal Other systems may be involved
Common Features:Common Features:

Common Features:Common Features:
Laboratory Investigations:
CBC, LFT.. Normal ESR: high in inflammatory only U&E: abnormalities in some endocrinopathies and
periodic paralysis C.K & aldolase: generaly: raised (normal in few
sittings: metabolic, endocrine…) Lactic acid Genetic study: location & type of chromozomal
abnormalities:

Common Features:Common Features:
Neurophysiology
NCS: normalEMG:
– Spontaneous activities +/- in inflammatory disorders
– Interferential tracing
– MUPs: small A Short D
polyphsics




Common Features:Common Features:
Pathology
+/- Severe reduction in the muscle fibersMuscles fibers are replaced by fat orfibrosisCentralized nucleiFibrosis+ Inflammatory infiltrate in inflamm disordersType / I type II Electron microscopy:
– abnormal mithochondries in mithochondriopathies


ETIOLOGY / CLASSIFICATIONETIOLOGY / CLASSIFICATION
Inherited myopathies– Muscular dystrophies – Congenital myopathies– Inherited channelopathies – Periodic paralysis – Inherited metabolic myopathies
Disorders of glycolysis
Disorders of oxidative metabolism
Lipid myopathies
Mitochondrial myopathies

Acquired myopathies
Inflammatory myopathies
Acquired metabolic myopathies
Toxic myopathies

Hereditary transmitted (Muscles Dystrophies)
X- linked:-Duchenne ( cardiac involv..)
-BeckerEmery-Dreifuss (+ severe cardiomyopathy)
Non-X linek:
Limb Girdle Facio-scapulo-humoral
Scapulo-peroneal
Scapulo-humeral
Ocular-pharyngeal….

Inflammatory muscle disorders :
Autoimmune:
Primary dysautoimmune or complicating systemic diseases: SLE..– Polymyositis – Dermatomyositis
Paraneoplastic
Viral
Infective: toxoplasmosis,trichinosis..
Toxic & drug induced muscle disorders.

Muscle DystrophiesMuscle Dystrophies

Muscular DystrophyMuscular DystrophyDuchenne/
BeckerEmery-Dreifuss,
CongenitalLimb-Girdle,
Distal Myopathy
Onset 2-6 years Childhood to early teens, infancy
Late childhood-middle age
Muscle groups affected
Life expectancy Rarely beyond 20’s varies Middle age +
Inheritance X-linked recessive X-linked recessive, autosomal dom & rec.
Autosomal dominant & recessive
Genetic linkage Dystrophin Emerin, lamin, merosin, etc.
Calpain-3, Dysferlin, Caveolin-3, α-sargoglycans, etc.
Source: www.mdausa.org

X-linked: DystrophinopathiesX-linked: Dystrophinopathies
Groupe of hereditary myopathies Pathophysiology: defective or absent Dystrophin Dystrophin:
– Has integral role in sarcolemmal stability– Consist in 2 globular heads with flexible rod-shaped center
– Associated in a complex with sarcoglycans & dystroglycans (transmembrane proteins & glycoproteins)
– Coding gene: on Chromosom X short arm : Xp21 location
– Function loss: cascade of events (including loss of other
components of dystrophin-associated glycoprotein complex, sarcolemmal breakdown with attendant Ca ion influx phosphlipase activation, oxidative cellular injury) and ultimately myonecrosis

X- Linked: Ducenne, Beker..X- Linked: Ducenne, Beker..
X- linked, recessive transmissionAffects malesFemales are CarrierOnset: 2-5 years in Duchenne, end 1st decade in
Becker)Proximal muscles: mainly , (early)Severe disease (+ other systemes: cardiac..) death in the 2d decade

DUCHENNE MDDUCHENNE MDprogressive skeletal muscle weakness.Absence of the dystrophin protein weakens the
connections between proteins in the muscle fibers & the cell membrane. (?the cell membrane becomes weaker & ruptures)
As a result: ions such as Ca can move in & out of the ruptured cell membrane contraction at the damaged site the muscle fibers will break the muscle will begin to waste away.

Prevalence of DMDPrevalence of DMD(1)(1)
Affects one in 3500 to 5000 newborn males
1/3 of these with previous family history
2/3 sporadic

Clinically: onset of DMDClinically: onset of DMD
Delayed developmental milestones
Loss of motor skills
Characteristic gait
Calf “hypertrophy” (pseudohypertrophy)
Clumsiness/frequent falls

Symptoms of DMDSymptoms of DMD
Muscle weakness: Difficulty in walking/running
Difficulty climbing stairs or hills
& Difficulty in rising (Gower’s sign)

DIAGNOSIS: Clinical,
Lab Invest.: CPK
Neurophysiol. (EMG): myogenic changes
Muscle biopsy
Genetic study (Immunoblot homogenate allow diffenrentiation between Duchenne & Becker)
Asymptomatic female Foetus diagnsis possible (as early as 8 weeks)

DMD: where is the Gene?DMD: where is the Gene?The gene for dystrophin production sits on the X
chromosome.
If a normal gene for dystrophin is present, then the protein will be made.
If the gene is missing or altered, dystrophin may not be produced at all or only in abnormal forms, resulting in Duchenne muscular dystrophy


Dystrophin connects the
myofibrils to a complex of proteins
in the muscle cell membrane.
This in turn connects to the
extracellular matrix protein
laminin, stabilizing the
membrane

Spectrin connects the actin cytoskeleton in Red Blood Cells to the membrane

What is Utophin?What is Utophin?
Utophin is a protein that acts the same as dystrophin where the nerve cells meet muscular tissue.
Dystrophin and Utophin both help to protect muscle tissue through wear and tear.
Dystrophin works as a shock absorber to the muscles. Utophin does also

What is the connection between What is the connection between Dystrophin and UtophinDystrophin and Utophin??
Studies done on mice showed that if there is
an abnormally high amount of Utophin in the
body, the symptoms of MD reverse.


Dystrophinopathies. Dystrophic muscle Dystrophinopathies. Dystrophic muscle

Dystrophinopathies: dystrophin stainingDystrophinopathies: dystrophin staining
Normal Normal dystrophindystrophin
Intermediate dystrophin Intermediate dystrophin BeckerBecker MD MD
Duchenne dystrophyDuchenne dystrophy

Treatments for DMDTreatments for DMD
To improve breathing:– O2 therapy
– Ventilator
– Scoliosis surgery
– Tracheotomy

Treatments (cont.)Treatments (cont.)
To improve mobility:– Physical therapy
– Surgery on tight joints
– Prednisone
– Non-steroidal medications
– Wheelchair

Treatments (cont.)Treatments (cont.)
To improve mobility:– Physical therapy
– Surgery on tight joints
– Prednisone
– Non-steroidal medications
– Wheelchair

Advances in Gene TherapyAdvances in Gene Therapy
Researches have developed "minigenes," which carry instructions for a slightly smaller version of dystrophin, that can fit inside a virus
Researchers have also created the so-called gutted virus, a virus that has had its own genes removed so that it is carrying only the dystrophin gene

Problems with Gene TherapyProblems with Gene Therapy
Muscle tissue is large and relatively impenetrable
Viruses might provoke the immune system and cause the destruction of muscle fibers with the new genes

Other MDOther MD
Limb Girdle MDLimb Girdle MD

Common featuresCommon features– Expression in either male or female sex – Onset usually in the late first or second decade of
life (but also middle age) – Usually autosomal recessive and less frequently
autosomal dominant – Involvement of shoulder or pelvic-girdle muscles
with variable rates of progression – Severe disability within 20-30 years – Muscular pseudohypertrophy and/or contractures
uncommon

Molecular genetics revolutionized LGMD classification
Rrecent classification (clinical and molecular characteristics) – autosomal dominant (LGMD1) – autosomal recessive (LGMD2) – The list continues to expand– Genetic linkages have been identified for 6 autosomal
dominant and 11 autosomal recessive LGMDs, – Myofibrillar myopathies share several phenotypic
characteristics with the LGMDs.

Limb Girdle MDLimb Girdle MD
LGMD may show an autosomal recessive (autosomal dominant forms reported)
or sporadic method of inheritance.
Some forms of LGMD dramatically affect young adults, while other types progress so slowly that they are not detected until much later in life.

LGMD protein defects occur in several pathways
proteins associated with the sarcolemma
proteins associated with the contractile apparatus
Various enzymes involved in muscle function.

Autosomal recessive LGMDAutosomal recessive LGMD
This childhood form
Affects both males and females
First decade of life. In general
The course is of gradual progression over years.
Distribution of weakness is typically in the pelvis (80-90% of cases)
later in life, involvement of the shoulder girdle (30%)
No hypertrophy of the calves (contrast to other forms of MD

CPK: elevated (2-3 times)
The inheritance pattern is strongly autosomal recessive with consanguinity
Positive family history often is reported.
The abnormal gene is linked to chromosome arm 15q.
Autosomal recessive LGMDAutosomal recessive LGMD

Pelvifemoral atrophy Pelvifemoral atrophy (Leyden-Mobius)(Leyden-Mobius) Most heterogeneous of all limb-girdle dystrophies. 60-70% of cases are sporadic (few cases: familial)Symmetric or asymmetric involvement of the pelvic
girdle. Late onset : second to sixth decades. Slow progression clinical arrest (ambulate into 70s)
The survival rate: seventh decade of life.CPK: vary from normal to significant elevation. No identified gene yet.

Scapulo-humeral dystrophy (Erb) Scapulo-humeral dystrophy (Erb)
Involves mainly the upper extremities. Autosomal recessive in some cases. starts later in life (second to the fifth decades), “Benign” (years before it is diagnosed). Weakness generally is asymmetric: may spare the
deltoid, supra-spinatus, and infra-spinatus muscles. lower extremities involvement very late in life show The progression: very slow (normal life
expectancy). Minimal, disability

Late-onset autosomal myopathyLate-onset autosomal myopathy
Third to the fifth decades of life.
The course is benign
Upper & lower extremity weakness :little functional impairment.
Patients: ambulate well into their 6th and 7th decade
Affects males and females.

OculopharyngealOculopharyngeal
Late onset
Ocular and bulbar symptoms
Slowly progressing

autosomal-recessive disease
Severe proximal weakness at birth (or within 6/12) Slowly progressive or nonprogressive. Contractures are common
central nervous system (CNS) abnormalities can occur.
Biopsy: signs of dystrophy, a marked in endomysial and perimysial connective tissue, and fiber size variability with small round & immature fibers, less commonly, necrosis
No distinguishing features (as in congenital myopathies)
Congenital Muscular DystrophyCongenital Muscular Dystrophy

Congenital Muscular DystrophyCongenital Muscular DystrophyThe pathophysiology of CMD depend on specific
associated genetic defect (known with 4 of the CMDs)
Functions of the disrupted proteins: defined in 2:– Deficiency of laminin-alpha2 (merosin), a skeletal
muscle extracellular matrix protein that binds the dystrophin-associated glycoprotein complex (see Picture 1)
– Deficiency of integrin-alpha7 beta1, a skeletal muscle membrane protein that binds laminin-2
The pathophysiology of the other CMDs is unknown


Muscular dystrophyMuscular dystrophyCongenital
Duchenne, Becker
Emery-Dreifuss
Limb girdle

Distal myopathy : Miyoshi (1967, 1986)– Locus 2p13.3– DYSF gene mutation (Bashir et al ; Liu et al, 1998)
Type 2B limb girdle myopathy:– Firstly described in Palestinian families (Mahjneh et al,
1992)– Chromosome 2p linked (Bashir et al, 1994)
Both MM and LGMD phenotype in the same family (Illiaroshkin et al ; Weiler et al, 1996)
DysferlinopathiesDysferlinopathies

Distal myopathy : Miyoshi (1967, 1986)– Locus 2p13.3– DYSF gene mutation
(Bashir et al ; Liu et al, 1998)
Type 2B limb girdle myopathy:– Firstly described in Palestinian families
(Mahjneh et al, 1992)– Chromosome 2p linked
(Bashir et al, 1994)
Both MM and LGMD phenotype in the same family
(Illiaroshkin et al ; Weiler et al, 1996)


Geographical distributionMM identified in Japan LGMD (Palestinian, Lybian Jews)
Dysferlin mutation 1/3000 Lybian Jews (Argov et al, 2000)
Most frequent distal myopathy (except Scandinavia)LGMD2B= second cause of LGMD (Tagawa et al)Dysferlinopathies : about 25% of unindentified
muscular dystrophy
Dysferlinopathies: EpidemiologyDysferlinopathies: Epidemiology

Dysferlin is located to muscle cell membranes, and is missing in patients with severe limb girdle muscular dystrophy

Model
for the
function
of
Dysferlin
in
muscle
repair

AR inheritance Normal developmental milestones, sport possible prior to
first symptoms Onset between 15 – 35 y (young adults) LL : distal, proximo-distal, or proximal wk calf involvment
++ UL : biceps atrophy, moderate scapular involvment Facial, bulbar muscles = spared Normal cardiac and respiratory function CK (10 to 123 N) Unspecific myopathic pattern, necrosis, no vacuoles Various severity
Dysferlinopathies: Common traitsDysferlinopathies: Common traits

Distal myopathy– Posterior leg (Miyoshi myopathy)– Anterior leg compartment
Proximal myopathy « limb girdle » (LGMD2B)
High CPK
Polymyositis-like
Exercise intolerance



Dysferlin

Myotonic DystrophyMyotonic Dystrophy
Myotonic dystrophy Autosommal dominant disorder with highly variable
expression of the disease phenotypeThe molecular abnormality is an expansion of a
CTG nucleic acid triplet repeat sequence on the nineteenth chromosome
The muscle weakness can be mildMarked facial weakness, ptosisGreater distal weakness

Difficulty in releasing hand grip. At the bedside, myotonia
Frontal balding: usually more prominent in men
Premature cataracts, arrhythmias, diabetes, and testicular atrophy
Myotonia can be a disturbing symptom or does not
In disabling myotonia, quinine, Phenytoin, henytoin
Mexiletine should not be used if cardiac manifestations

Myotonic dystrophyMyotonic dystrophy
Type 1 (most common, 98%)– an expansion of CTG repeats in the DMPK gene on
chromosome 19– Prevalence in West: 13.5 per 100,000
Type 2– an expansion of CCTG repeats in the ZNF9 gene on
chromosome 3
Type 3 ?

Inflammatory MyopathiesInflammatory Myopathies- Age: young/adult- +/- Skin rash- Main feature: weakness + Muscle pain
+tenderness Investigations- High C.K.- EMG- Muscle biopsy
Diagnosis: Treatment Immune suppressive = steroids


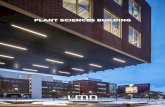
Polymyosite
Maladie hépatique
CMT
Myopathie
métabolique
BMD
FSH
0 2 4 6 8 10 12 14 16
Err
an
ce d
iag
nosti
qu
e
Nombre de patients

Metabolic myopathies Metabolic myopathies
Thyroid disease Hypothyroid or hyperthyroid ophthalmopathy periodic paralysis Pituitary and adrenal disease Cushing's syndrome Steroid myopathy Adrenal insufficiency Primary hyperaldosteronism Acromegaly Hyperparathyroidism Hypoparathyroidism

MYASTHENIA GRAVISMYASTHENIA GRAVIS

MYASTHENIA GRAVISMYASTHENIA GRAVIS
DEFINITION: Disorder of the NMJ (postsynaptic membr)
Forms: Transient neonatal (~10% of neonate myasthenic mothers)
– Different prognosis, effective treatment
Congenital myasthenia Common myasthenia gravis
– Any age: 2 pics: 20-30 (F > M) & 60-70 M > F)– Usually progressing (remission are possible but: relapse later)



MYASTHENIA GRAVISMYASTHENIA GRAVIS
CLINICAL FEATURES - Onset: insidious- Fluctuating weakness: with exercise- Fatigability (worsening with exercise & improvement in rest)
- Precipitating factors: Infection, Pregnancy, stress, hot temperature, drugs: muscle relaxants, BZDZ,phenytoin antibiotics (neomycin)
Clinical presentation: - Ocular: – ptosis, diplopia opthalmoplegia- Bulbar: dysphagia, dysphonia, +/-facial weakness- Generalized: +/-respiratory muscles weakness risk of
death

MYASTHENIA GRAVISMYASTHENIA GRAVIS
Clsassification: Osserman classification
I ocular
II (A & B): mild to moderate generalised, ++/- drug response, no crises
III Acute fulminant + crises, risk of death, high mortality
IV late severe MG
Associated disorder:-- Dysthyroidism- Rh. Arthritis, P. anaemia, SLE



The Spectrum of autoimmune Diseases
Hashimoto’s thyroiditis Pernicious anaemia Insulin dependent diabetes
Myasthenia gravis Multiple sclerosis
Ulcerative colitisRheumatoid arthritis
Systemic lupus erythematous
Systemic Organ specific

PATHOPHYSIOLOGYPATHOPHYSIOLOGY
Neuromuscular junction transmission autoimmune disorder (Post synaptic membrane)
Destruction of the Ach. receptors on the post synaptic membrane by the AB insufficient muscle fibers contraction
Ach.receptor Anti-bodies: – circulating: level can be done– Origine: thymus (hyperplasia, thymoma)
association of HLA, A1 + B8.

Auto reactive T cell
Genetically predisposed
Tr
IL-6, etc
B cell
CD8
Tissue damage
Cytokines
Cytokines


Diagnosis Clinical presentation, excrcise test, rest test Tensilon Test: 10 mg Edrophonium IV carrefullty &
slowly Investigations
Investigations Laboratory Investigations.
– Acetycholine receptor antibodies level– Straited muscle AB, other antibodies
Neurophsiology– EMG: decrement test
Imaging: Chest x-ray and chest CT scan / MRI Others: PFT…..

MANAGEMENTMANAGEMENT
Medical treatment Anticholinesterase
Immunosupressant: Steroids
Azathioprin
Plasmaphoresis
Immunoglobulins
Surgery: Thymectomy

PrognosisPrognosis
Remission ~ 30 %.– More likely in patient with short history– Less in prominent thymic hyperplasia/thymoma
Approach through suprasternal or transsternal– (extensive, large thymectomy)
Medical treatment:
may be D/C, need for low doses, same doses
or worsening + other ttt

Myasthenic crisesMyasthenic crises
Severe situationNeeds urgent managementDiferentiate from cholinergic crises

Myasthenic syndromeMyasthenic syndrome
Clinically: differencesPathophysiology: presynaptic membraneNeurophsiology: increamentPoor response to Anti Ch-esterase Etiology: paraneoplastic