Muscle Relaxant
9
PHARMACOLOGY Muscle relaxants: past, present and future C. Prior Department of Physiology and Pharmacology, Strathclyde Institute for Biomedical Sciences, University of Strathclyde, 27 Taylor Street, Glasgow G4 0NR, UK KEYWORDS Neuromuscular non- depolarizing agents, Neuromuscular junction, Acetylcholine, Nicotinic Summary Muscle relaxants are an irreplaceable item within the modern surgical toolkit.Their almost universal use during surgical procedures of medium-to-long dura- tion means that it is essential that all anaesthetists must have a comprehensive knowl- edge of their history and the future prospects for their continued evolution. In the context of identifying the ‘ideal’ muscle relaxant, this review focuses on those areas of muscle relaxant action that are either highly desirable or highly undesirableFand dis- cusses the extent to which any identi¢ed problems have, or have not, been overcome with the existing range of clinically available muscle relaxant compounds. Pharmacody- namic topics covered include the actions of muscle relaxants on the range of di¡erent subtypes of nicotinic acetylcholine receptors, the actions of muscle relaxants on motor nerve terminals and the major non-neuromuscular actions of muscle relaxants. From a pharmacokinetic perspective, how the pharmacological and chemical properties of muscle relaxants in£uence the clinical properties and uses of the compounds are discussed. c 2003 Elsevier Science Ltd All rights reserved. INTRODUCTION Muscle relaxants selectively depress skeletal muscle function, producing a paralysis of normal motor activity. They are primarily used to prevent movement during surgical procedures, although they also have an impor- tant role in the intensive care unit (ICU) where they are used to paralyse patients requiring mechanical ventila- tion. Many agents produce skeletal muscle paralysis in- cluding high doses of general anaesthetics, centrally acting agents such as the benzodiazepines that depress motor cortex out£ow, local anaesthetics that inhibit ac- tion potential conduction in motor axons and com- pounds such as dantrolene sodium that inhibits Ca 2+ mobilization within skeletal muscle ¢bres. However, none of these produces the total and selective paralysis required for surgical procedures. From a practical per- spective, clinical muscle relaxants block acetylcholine (ACh) mediated transmission at the neuromuscular junc- tion. They do this by virtue of an action on the nicotinic acetylcholine receptors (nAChRs) located on the motor endplate. Depolarizing muscle relaxants such as suxa- methonium are agonists at nAChRs. They produce neu- romuscular block since over-stimulation of the nAChRs leads to the skeletal muscle membrane surrounding the motor endplate becoming inexcitable. Non-depolarizing muscle relaxants (Fig.1) are antagonists of the action of ACh on motor endplate nAChRs and, as such, can pre- vent signal conduction and produce neuromuscular block. Along with the introduction of antimicrobial drugs and aseptic techniques, the development of safe and ef- fective muscle relaxant drugs ranks as one of the most signi¢cant advances in surgical procedures in the 20th century. Any anaesthetic agent, given in a su⁄ciently high dose, will produce skeletal muscle paralysis, but this carries with it the serious risk of adverse cardiovascular and respiratory depression. Being able to produce skele- tal muscle paralysis independent of a depressant e¡ect on CNS function means that lower, and safer, doses of the general anaesthetic can be employed.Thus, muscle relax- ants will always remain a very important part of any sur- gical drug regime and an awareness of the current developments in the ¢eld of muscle relaxants is impor- tant to surgeons and anaesthetists throughout the world. This review will present an overview of our current understanding of the pharmacodynamic and Correspondence to: CP.Tel: +44(0)141548 2459; Fax: +44 (0) 141552 2562; E-mail: [email protected] Current Anaesthesia & Critical Care (2003) 14, 38^46 0953 -7112/03/$ - see front matter c 2003 Elsevier Science Ltd. All rights reserved. doi:10.1016/S0953 -7112(03)00056 -5
-
Upload
blinkbumbum -
Category
Documents
-
view
24 -
download
1
description
obat pelemas otot
Transcript of Muscle Relaxant

Current Anaesthesia & Critical Care (2003) 14, 38^460953-7112/03/$ - see frontmatter �c 2003 Elsevier Science Ltd. All rights reserved.doi:10.1016/S0953-7112(03)00056-5
PHARMACOLOGY
Muscle relaxants: past, present and futureC.Prior
Department of Physiology and Pharmacology, Strathclyde Institute for Biomedical Sciences,University of Strathclyde, 27 Taylor Street,GlasgowG4 0NR,UK
KEYWORDSNeuromuscular non-depolarizing agents,Neuromuscular junction,Acetylcholine,Nicotinic
Summary Muscle relaxants are an irreplaceable item within the modern surgicaltoolkit.Their almost universal use during surgical procedures ofmedium-to-long dura-tion means that it is essential that all anaesthetists must have a comprehensive knowl-edge of their history and the future prospects for their continued evolution. In thecontext of identifying the‘ideal’muscle relaxant, this review focuses on those areas ofmuscle relaxant action that are either highly desirable or highly undesirableFand dis-cusses the extent towhich any identi¢ed problems have, or have not, been overcomewith the existing range of clinically available muscle relaxant compounds. Pharmacody-namic topics covered include the actions of muscle relaxants on the range of di¡erentsubtypes of nicotinic acetylcholine receptors, the actions of muscle relaxants onmotornerve terminals and the major non-neuromuscular actions of muscle relaxants. Froma pharmacokinetic perspective, how the pharmacological and chemical propertiesof muscle relaxants in£uence the clinical properties and uses of the compounds arediscussed.�c 2003 Elsevier Science Ltd Allrights reserved.
INTRODUCTIONMuscle relaxants selectively depress skeletal musclefunction, producing a paralysis of normalmotor activity.They are primarily used to prevent movement duringsurgical procedures, although they also have an impor-tant role in the intensive care unit (ICU) where they areused to paralyse patients requiring mechanical ventila-tion. Many agents produce skeletal muscle paralysis in-cluding high doses of general anaesthetics, centrallyacting agents such as the benzodiazepines that depressmotor cortex out£ow, local anaesthetics that inhibit ac-tion potential conduction in motor axons and com-pounds such as dantrolene sodium that inhibits Ca2+
mobilization within skeletal muscle ¢bres. However,none of these produces the total and selective paralysisrequired for surgical procedures. From a practical per-spective, clinical muscle relaxants block acetylcholine(ACh) mediated transmission at the neuromuscular junc-tion.They do this by virtue of an action on the nicotinicacetylcholine receptors (nAChRs) located on the motorendplate. Depolarizing muscle relaxants such as suxa-
Correspondence to: CP.Tel: +44(0)141548 2459; Fax: +44 (0) 1415522562; E-mail: [email protected]
methonium are agonists at nAChRs.They produce neu-romuscular block since over-stimulation of the nAChRsleads to the skeletal muscle membrane surrounding themotor endplate becoming inexcitable.Non-depolarizingmuscle relaxants (Fig.1) are antagonists of the action ofACh on motor endplate nAChRs and, as such, can pre-vent signal conduction and produce neuromuscularblock.Along with the introduction of antimicrobial drugs
and aseptic techniques, the development of safe and ef-fective muscle relaxant drugs ranks as one of the mostsigni¢cant advances in surgical procedures in the 20thcentury. Any anaesthetic agent, given in a su⁄cientlyhigh dose, will produce skeletalmuscle paralysis, but thiscarries with it the serious risk of adverse cardiovascularand respiratory depression. Being able to produce skele-talmuscleparalysis independentof a depressante¡ectonCNS function means that lower, and safer, doses of thegeneral anaesthetic canbe employed.Thus,muscle relax-ants will always remain a very important part of any sur-gical drug regime and an awareness of the currentdevelopments in the ¢eld of muscle relaxants is impor-tant to surgeons and anaesthetists throughout theworld. This review will present an overview of ourcurrent understanding of the pharmacodynamic and

Rocuronium
Pancuronium Vecuronium Rapacuronium
R1 CH3 --- ---
R2 CH3 CH3 CH2CHCH2
R3 OC(O)CH3 OC(O)CH3 OC(O)CH3
R4 OC(O)CH3 OC(O)CH3 OC(O)CH2CH3
Tubocurarine
Atracurium
Mivacurium
HOO
O
HOH
H
H3CO
OCH3
N+ CH3
CH3
N+
H3C
H3C
N
ON+
HO
OCH3C
O
CH2
CH2
CH2
N
N+
R1 R2
R3
R4
N+
CH2
OCH3
OCH3
OCH3
OCH3
CH3
CH2CH2C
O
O(CH2)5OCCH2CH2
N+CH3
H3CO
H3CO
CH2
H3CO
O
OCH3
(CH2)2
O
O C CH CH (CH2)2 C
O
O(CH2)3N+
CH3
H3CO
H3CO
CH2
H3CO
OCH3
OCH3
(CH2)3
H3CO
CH3
OCH3
OCH3
OCH3
OCH3
CH2
N+
Rocuronium
Pancuronium Vecuronium Rapacuronium
R1 CH3 --- ---
R2 CH3 CH3 CH2CHCH2
R3 OC(O)CH3 OC(O)CH3 OC(O)CH3
R4 OC(O)CH3 OC(O)CH3 OC(O)CH2CH3
Tubocurarine
Atracurium
Mivacurium
HOO
O
HOH
H
H3CO
OCH3
N+ CH3
CH3
N+
H3C
H3C
N
ON+
HO
OCH3C
O
CH2
CH2
CH2
N
N+
R1 R2
R3
R4
N+
CH2
OCH3
OCH3
OCH3
OCH3
CH3
CH2CH2C
O
O(CH2)5OCCH2CH2
N+CH3
H3CO
H3CO
CH2
H3CO
O
OCH3
(CH2)2
O
O C CH CH (CH2)2 C
O
O(CH2)3N+
CH3
H3CO
H3CO
CH2
H3CO
OCH3
OCH3
(CH2)3
H3CO
CH3
OCH3
OCH3
OCH3
OCH3
CH2
N+
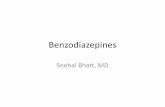
Figure 1 Chemical structures of the main non-depolarizing muscle relaxants that are, or have been, used in clinical practice.Twomain groupings of compounds exist.Those based on an aminosteroid nucleus (top panels) and those based on benzoisoquinolinemoieties (lowerpanels).
MUSCLERELAXANTS:PAST,PRESENTANDFUTURE 39
pharmacokinetic actions of non-depolarizing muscle re-laxants and how these relate to their clinical pro¢les.Such a review will, inevitably, be fairly general, but it ishoped that su⁄cient leads will be provided to allow theinterested reader to explore further into what is still,even in the modern age of genomics and proteomics,a complex and sometimes poorly understood area ofmedicine.
PHARMACOLOGICALACTIONOFMUSCLERELAXANTS
Actions ofmuscle relaxants on nAChRs
To appreciate the pharmacological actions of non-depolarizingmuscle relaxants, it is necessary to be famil-iar with the structure and function of nAChRs. As longago as 1950, it was recognized that nAChRs are hetero-geneous, and that subtypes can be pharmacologically
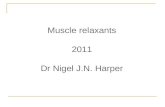
identi¢ed.The earliest, and probablymost important di-vision of nAChRs into subtypes was the recognition of‘C6’ and ‘C10’ receptors.1C6-receptors were character-ized in the autonomic ganglia of the cat superior cervicalganglia, were blocked by hexamethonium (hence thename) and are often now referred to as the ‘neuronal-type’ of nAChR. C10-receptors were characterizedas the postjunctional nicotinic ACh receptor at theneuromuscular junction, were blocked (depolarizing)preferentially by decamethonium (hence C10) and areoften now referred to as the ‘muscle-type’ of nAChR.Modernmolecular genetics has taken our understandingof the subtypes of nAChRs considerably further.2 Geneproducts for at least17 di¡erent peptide subunits of thenAChRhavenowbeen identi¢ed (10 di¡erent a-subunits,four di¡erent b-subunits, one g-subunit, one d-subunitand one e-subunit). All nAChR are ligand-gated non-selective transmembrane cation channels assembledfrom ¢ve of these subunits (Fig. 2).Muscle-type nAChRsare composed of two x a1-subunits along with one each

Figure 2 Molecular composition of nAChRs: (A) Cross-sectional view from the side showing the goblet-shaped structure of thetransmembrane assembly. (B) View fromtop showing the arrangementof the ¢ve subunits around the central ion channel pore (top,muscle-typenAChR; centre, heteromeric neuronal-typenAChR; bottom, homomeric neuronal-typenAChR).Thetwo AChbindingsites are atthe interface of the a-subunits and their neighbouring subunit.The homomeric neuronal-type nAChR is proposed to have¢ve ACh binding sites.However, in commonwith all other subtypes of nAChRs, it is thoughtto openwhen ACh is bound to justtwonon-adjacent sites.
40 CURRENT ANAESTHESIA & CRITICALCARE
of the b1 and d-subunits and either an e-subunit (fetalreceptors) or a g-subunit (adult receptors). Neuronal-type nAChRs are composed of either two a-subunitsand three b-subunits (heteromeric neuronal-type recep-tors) or, in the case of the a7, a8, a9 and a10 subunits canbe composed of ¢ve identical subunits (homomeric neu-ronal-type receptors).The exact combination of the dif-ferent subunits in the heteromeric neuronal-type ofnAChRs is unknown and probably variedFgiving riseto further multiple subtypes of neuronal-type nAChRs.In addition to the various subtypes of nAChRs di¡eringwith respect to their pharmacological speci¢city, theyalso show some functional variability. Although the sub-types of nAChRs are all referred to as ‘non-selective’cation channels in that they all show approximately equalpermeabilities to sodium and potassium ions, there is agreater variability in the selectivity of the subtypes ofthe receptors for Ca2+ and this is believed to be of func-tional signi¢cance in certain circumstances.The molecular biology revolution has provided new
tools for the investigation of drug action. Perhaps themostwidely used of these is the ability to express recep-tors in cultured cell lines to allow a detailed analysis offundamental drug^receptor interactions. Several re-searchgroupshave exploitedgene expression techniquesto investigate the interactions of muscle relaxants withsubtypes of nAChRs.These studies have givenmuch use-ful information on how muscle relaxants interact withnAChRs at themolecular level, includingmeasures of ab-solute antagonistic potencies,3 identi¢cation of receptorbinding determinants4 and how multiple drug combina-
tions a¡ect drug^receptor interactions.5 In terms ofthe drug discovery process, an obvious advantage of ex-pression systems is that one can rapidly (and cheaply)identify drug candidates that have both high potencyand high receptor subtype speci¢city. However, a disad-vantage is that even having identi¢ed a potential candi-date, knowing how the compound does, or does not,interact with the various subtypes of nAChRs gives lim-ited information about its clinical pro¢le since much ofthiswillbe governedbyunexploredpharmacokinetic fac-tors.Nevertheless, expression systemsmay help to pre-dict the occurrence of certain well-characterizedadverse side-e¡ects.Clinically, one would expect the cleanest pro¢le for a
muscle relaxant to be achieved by it having a very highselectivity for themuscle-type nAChR at the neuromus-cular junction,without any inhibitorye¡ecton anyof theneuronal-type subtypes of nAChRs. Some agents, suchas tubocurarine are poorly selective for themuscle typenAChR, also showing considerable potency at neuronal-type nAChRs.Others, such as vecuronium show a verymarked selectivity for the muscle type of receptors.The actual clinical consequences of a lack of receptorsubtype selectivity are, in reality, di⁄cult to quantify.All nAChR antagonists are mono- or bisquaternaryammonium compounds and, as such, are highly chargedmolecules at physiological pH. This means that, undernormal circumstances, they cannot cross the blood^brain barrier and interact with nAChRs in the brain.Therefore, the incidence of side-e¡ects due to anaction in the brain is practically non-existent, even for

MUSCLERELAXANTS:PAST,PRESENTANDFUTURE 41
compounds such as tubocurarine. The only area ofsusceptibility for the block of neuronal-type nAChRs isin autonomic gangliaFthat lie outside the blood^brainbarrier. Block of neuronal-type nAChRs in autonomicganglia by compounds such as hexamethonium andtrimetaphan does cause marked hypotension. However,the only muscle relaxant to produce hypotension asone of its more serious side-e¡ects is tubocurarineand, despite its potency at neuronal-type nAChRs, thise¡ect is more likely to be due to histamine releasethan ganglion block, since it is abolishedby antihistamineagents.6
Actions ofmuscle relaxants onmotor nerveterminals
Within a few years of the introduction of musclerelaxants into surgical practice it was already being sug-gested that they might have an e¡ect on motor nerveterminals in addition to their postjunctional actions.Athigh frequencies of nerve stimulation, itwas observedthat antagonists of muscle-type nAChRs, even atlow concentrations, could produce a waning of tetanictension (Fig. 3). This tetanic fade was attributed to acombined e¡ect of the compounds to both reduce post-junctional sensitivity toACh and tomodulate the releaseof ACh from the motor nerve terminals. Many studieshave attempted to determine the nature of the prejunc-tional e¡ects of muscle relaxants during tetanic stimula-tion and, although there is now widespread acceptancethat muscle relaxants do modulate ACh release, thecellular mechanisms responsible are still, even today, thesubjects of much controversy. An understanding ofthese processes is of particular importance in the ¢eldof anaesthesia where the presence of either tetanicor train-of-four fade during postoperative recovery isroutinely used as an indication of the level of residualneuromuscular block still present.Given that tetanic and train-of-four fade have been
observed with all experimental and clinically evaluatedmuscle relaxants, the most obvious candidate for a pre-
0.1 Hz 2 Hz 50 Hz
CONTROL
0.1 Hz 2 Hz 50 Hz
Figure 3 Representative examples of the train-of-four and tetantype nAChRs, a-conotoxin GI.Tension traces in the absence (left)isolated piece of rat hemi-diaphragm skeletalmuscle stimulated indiCalibrations bars: vertical, 2 g in all trace exceptthe control 50Hz tand 50Hz traces.
junctional site of action of muscle relaxants is a nicotinicACh autoreceptor situatedon themotornerve terminal.It is true that certain muscle relaxants are known tohave pharmacological actions aside from their e¡ectson nAChRs that couldmanifest themselves as a prejunc-tional e¡ect. Examples are the ability of tubocurarine toblock potassium channels7 or the ability of pancuroniumto block certain subtypes of muscarinic ACh recep-tors.8,9 However, such actions tend to be idiosyncraticand it is hard to imagine that all muscle relaxants wouldpossess at least one action to a¡ect nerve terminalfunction that was unrelated to their ability to inhibitthe action of ACh on postjunctional nAChRs. Based ontheir location on axon terminals, and the ability ofmuscle relaxants such as tubocurarine to blockganglionic responses,10 most researchers have assumedthat the prejunctional autoreceptors are neuronal-typenAChRs and that low speci¢city of muscle relaxants forthe postjunctional muscle-type nAChRs accounts fortheir prejunctional e¡ects.11,12 However, one £aw withthis assumption, not resolved in early studies, is that allmuscle relaxants, including those such as vecuroniumthat possess negligible pharmacological activity ganglia13
and in the CNS,14 produce tetanic fade.Not only is there uncertainty surrounding the nature
of the prejunctional nAChR, there is also a disagreementas to the e¡ectsmediated through thereceptors.Ononehand, it has been argued that the prejunctional nAChRsare autofacilitatory receptors that normally serve to en-hance themobilization of ACh for release during periodsof sustained secretory activity.12 Blocking this autofacili-tatory e¡ect with a muscle relaxant depresses ACh re-lease and hence enhances neuromuscular block duringhigh-frequency nerve stimulation. Alternatively, it hasbeen suggested that the prejunctional nAChRs are auto-inhibitory and normally ACh acts at these receptors todepress its own release during periods of low secretoryactivity.11 Muscle relaxants, by blocking these receptorswould enhance the release of ACh at low frequenciesof stimulation, leading to an exaggerated frequency-dependent depression in ACh release and this, coupled
0.1 Hz 2 Hz 50 Hz
2 µµM α-CONOTOXIN GI
0.1 Hz 2 Hz 50 Hz
ic fade produced by the naturally occurring antagonist ofmuscle-and presence (right) of 2 mMa-conotoxin were recorded from anrectly (via its phrenic nerve) at 0.1, 2 Hz for 2 s and 50 Hz for 2 s.etanuswhere it is10 g; horizontal, 300 s for 0.1Hz traces, 5 s for 2

Motor nerveterminal
ACh
Motor endplate of skeletal muscle fibre
(+) (-)
Muscle-type nAChR nAChR
Motor nerveterminal
ACh
Motor endplate of skeletal muscle fibre
(+) (-)
Muscle-type nAChR
Neuronal-typenAChR
Figure 4 Model of putative nicotinic ACh autoreceptor regu-lation of AChrelease frommotornerve terminals.
42 CURRENT ANAESTHESIA & CRITICALCARE
with the normal postjunctional blocking action of thecompounds underlies their ability to produce tetanicand train-of-four fade.Within the last 5 years, extensive analysis of the pre-
junctional e¡ects of a range of subtype selective nAChRagonists and antagonists has led to amodel of autorecep-tor regulation at themammalian neuromuscular junctionthat reconcilesmany previous apparently con£icting stu-dies (Fig. 4). It has been proposed that there are bothneuronal-type (inhibitory) andmuscle-type (facilitatory)nicotinic ACh autoreceptors on motor nerve terminalsthat serve to regulate the supply of ACh for release atlow and high frequencies of stimulation, respectively.15,16
How would ACh, acting through two di¡erent subtypesof prejunctional nAChRs, both presumablymediating anincrease in cation permeability, produce both a facilita-tory and an inhibitorye¡ectonAChrelease? The answerto this is largely unknown but it is likely that it might in-volve di¡erences in the distribution of the two classes ofnAChR around the nerve terminal and also di¡erencesin the functional ion selectivity of the two classesof nAChR, possibly with respect to their permeabilityto Ca2+.
NON-NEUROMUSCULAR ACTIONSOFMUSCLERELAXANTS
Anti-muscarinic actions ofmuscle relaxants
The ability of muscle relaxants to interact with nAChRshas been discussed in detail above. However, ACh alsoacts at muscarinic ACh receptors (mAChRs) and there-fore it is not surprising that some muscle relaxants alsohave some antimuscarinic actions, particularly at the M-2 and M-3 subtypes of mAChRs.Clinically, little action isseen that is attributable to inhibition of mAChRs in the
GI tract or the CNS (the latter presumably due to a lackof access). However, the most important sites at whichmuscle relaxants can (and do) interact with mAChRsare the sino-atrial node of the heart and the lungs.An antagonistic action at pre- and postsynaptic M-2receptors in theheart leads tovagal-block,which is char-acterized by tachycardia, some hypertension and/or amarked attenuation of the bradycardial response tovagal nerve stimulation. In agreement with their relativeM-2 receptor potencies,8,9 vagal-block is most promi-nent with gallamine and the aminosteroid muscle relax-ants such as pancuronium and rocuronium, being lessmarked with either the monoquaternary aminosteroids(e.g. vecuronium) or the benzoisoquinolines (e.g. atra-curium, mivacurium).The relatively predictable vagolyticactions of compounds such as pancuronium and rocuro-nium are not usually seen as problematical and are eventhought by some to be a good counter to the cardiode-pressant e¡ect of most general anaesthetics. In additionto an e¡ect on M-2 receptors in the heart somemusclerelaxants are thought, at clinical doses, to block post-junctional M-3 and prejunctional M-2 receptors at theparasympathetic (vagal) neuroe¡ector junctions in thelungs. The former would inhibit ACh-induced broncho-constriction whilst the latter, by blocking a negative-feedback e¡ect of ACh on vagal nerve terminals, wouldincrease bronchoconstriction.Thus, any clinical e¡ect ofmuscle relaxants on airway calibre is di⁄cult to predict,being critically dependent on the relativemix of pharma-cological actions. However, the M-2 receptor blocking-e¡ect has beenmooted as themechanism for the severebronchospasm that can be seen with rapacuroniumunder certain conditions.17
Non-cholinergic actions ofmuscle relaxants
Probably, the most serious side-e¡ect of muscle relax-ants not associatedwith cholinergic systems is the abilityof the benzoisoquinolinium-based compounds (e.g. tu-bocurarine, atracurium andmivacurium) to triggermastcell degranulation andhencehistaminerelease.18 This canresult in skin £ushing, bronchospasm, tachycardia and atransient fall in blood pressure.The hypotension seen asa side-e¡ect of tubocurarine is due to this e¡ect and notdue to ganglion block since it is attenuated by antihista-mine drugs such as promethazine.6 The histamine-re-leasing problems associated with atracurium have beenresolved through the development of cisatracurium.Atracuriumhas four chiral centres and the synthetic pro-cessby which the compound is producedresults in amix-ture of 10 di¡erent optical enantiomers. Each of theseenantiomers has a di¡erent pharmacology. Cisatracur-ium (Nimbex, 51W89) is one of the active enantiomerscomprising around15% of the total.On its own, cisatra-curium is amorepotentmuscle relaxant that atracurium(approximately four-fold) with a slightly longer duration

0.01 0.10 1.00 10.000
100
200
300
Dose (mg/kg)
On
set
tim
e (s
)
Vecuronium
Rapacuronium (2.5)
Rapacuronium (1.5)
Rocuronium
Mivacurium
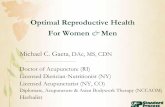
Figure 5 Graphical representation of the relationship be-tween clinical potency and onset time for a group of four di¡er-entmuscle relaxants.Plotted points aremean and SD and data isfromTable1of ref. 36.Eachrelaxanthasbeenused at an approxi-mately equi-e¡ective neuromuscular blocking dose. Despitethis, note the nearly seven-fold range of onsettimes.
MUSCLERELAXANTS:PAST,PRESENTANDFUTURE 43
of action.However, unlike the raw isomeric mix of atra-curium, cisatracurium is devoid of histamine releaseproperties19 and so does not produce any hypotension.When compared to atracurium, the onlymajor problemassociated with cisatracurium is pharmacoeconomic.Production of a single optical enantiomer requires eithera complex stereospeci¢c synthetic pathway or alterna-tively an e¡ective enantiomer separation technique,both of which will potentially increase the productioncost.
KINETICSOFMUSCLERELAXANTACTION
Onset of action
Aclean, side-e¡ect free, action is an importantprerequi-site for any muscle relaxant. However, it is not the onlyfactor that in£uences clinical success. Of equal impor-tance is the time course of action of the agent.The nat-ure of their use requires that muscle relaxants have apredictable time course of action and that, within thegroup of available compounds, the entire range of re-quired clinical durations is covered.One particular areathat has been the focus of much research over the last20 years has been the development of muscle relaxantswith a short onset and short duration of action that canbe safely used for rapid-sequence intubation. Currently,themost widely used agent for this purpose is the depo-larizing muscle relaxant suxamethonium, which pro-duces a rapid onset (around 1min) and short-lived(2^6min) neuromuscular block. However, the agonist-basedmechanism of action of suxamethonium creates anumber of potential problems including damagingmusclefasciculations, excessive stimulation of mAChRs and aninability to intentionally reverse the neuromuscularblock should any problems arise. For this reason, formany individuals the development of a rapid onset non-depolarizing muscle relaxant that can successfully com-pete with, and even replace suxamethonium has longbeen the life-ful¢lling goal of their endeavours.In order to develop a clinically acceptable non-
depolarizing muscle relaxant with a rapid onset andshort duration of action, it is necessary to have someidea as to what pharmacodynamic and pharmacokineticfactors can in£uence the time course of action of amus-cle relaxant. There is little doubt that one importantpharmacodynamic factor that in£uences the onset of ac-tion ofmuscle relaxants is the potency of the compound.It has been shown thatmolar potency is inverselyrelatedto speed of onset for a range ofmuscle relaxants of verydi¡erent clinical durations20,21 (see also Fig. 5). The onlyexception to this general rule appears to be atracurium,possibly because it is an enantiomeric mixture of severalactive compounds of markedly di¡ering neuromuscular
blocking potencies.22 There are two unfortunate conse-quence of any relationship between potency and onset.The ¢rst is pharmacoeconomic in that any developmen-tal strategy that deliberately focuses on the search for alowpotencydrug in thehope of ¢nding somethingwith afast onset will inevitably result in a product with rela-tively higher manufacture (and therefore market) cost.The second issue is pharmacological. As the potency ofthe muscle relaxant at the neuromuscular junction goesdown, the incidence of untoward side-e¡ects at clinicallye¡ective doseswill increase.Rapacuronium is an aminos-teroid muscle relaxant that is 15^20 times less potentthan vecuronium, requiring around 2mg kg-1 for skeletalmuscle paralysis in human. In terms of its onset, it canproduce maximum neuromuscular block in around 60 s,comparable with suxamethonium and suggesting thatthe goal of a non-depolarizing alternative to suxametho-niummightbe achievable.23,24However, a number of clin-ical studies have shown that rapacuroniumcanproduce adose-related increase in airway pressure25 and even, inchildren, severe bronchspasm,26 probably because of ablock of M-2 mAChRs in the lungs17 (see above).This hasled to serious concern as to its widespread introduction.If the goal of a fast onset neuromuscular block is not
to be found in the development of new nAChR antago-nists with optimized pharmacodynamic pro¢les thenwhat other pharmacokinetic strategies might exist tohelp achieve the desired end-point using existingmedium-duration muscle relaxants. Firstly, using asupra-maximal dose of muscle relaxant is one means toaccelerate its onset of action. Thus, a bolus injection ofrocuronium at twice its ED95 for neuromuscular blockwill produce paralysis within 60^120 s and can be usedfor rapid-sequence intubation.27 An obvious drawbackwith this high-dose approach is an increased subsequentduration of action of the muscle relaxant and anincreased risk of dose-related adverse side-e¡ects.Two other possibilities include the use of cocktails and

44 CURRENT ANAESTHESIA & CRITICALCARE
priming doses. Many clinicians have experimented withcombinations of two or more muscle relaxants basedon the notion of a supra-additive (e.g. synergistic) actionof the mixture. Clinical evidence28^31 does support theexistence of synergism with certain drug combinationsparticularly where an aminosteroid relaxant (e.g.vecuronium, rocuronium) is combined with a benzo-isoquinoliniumrelaxant (e.g. cisatracurium,mivacurium).However, this is likely to be a result of pharmacokineticinteractions rather than pharmacodynamic interactionsat the level of the postjunctional nAChRs since isolatedreceptor studies have mostly failed to demonstrate anye¡ect other than a simple additive action.5
In priming, pretreatment of a patient with a small (ty-pically 10% of ED95 dose) subparalytic dose of a musclerelaxant shortly before paralysis is required allows fullmuscle relaxation to be achieved rapidly with the re-mainder of the intubating dose. The priming principlehas been widely attempted with many di¡erent musclerelaxants, with variable reported success.However, it isgenerally accepted that the bene¢cial e¡ects of the ap-proach are small and the potential for untoward pro-blems great. In particular, the large variability in patientresponse to the priming dose often means that even at10% of the ED95, an unacceptable percentage of patientsmay develop clinical weakness from the priming dosealone.31Also the e¡ectiveness and safetyof priming is cri-tically dependent on the drug used, the exact regimeused (i.e. percentage priming dose and time betweenpriming dose and main dose) and the patient status; in
rActive
receptor/agonist complex
ACh nAChR
A
Anti-AChE AChE
(+)
(+)
(-)
rActive
receptor/agonist complex
ACh nAChR
A
Anti-AChE AChE
(+)
(+)
(-)
rActive
receptor/agonist complex
ACh nAChR
A
Anti-AChE AChE
(+)
(+)
(-)
rActive
receptor/agonist complex
ACh nAChR
A
Anti-AChE AChE
(+)
(+)
(-)
Figure 6 Schematicdiagramofthe fourmainmechanisms availabnon-depolarizingmuscle relaxant; including inhibition of AChmetaofthemusclerelaxant andchemicalchelationofthemusclerelaxantingagent; (+), promotesneuromuscular transmission; (�), reduces
particular age.32 Thus, it is very di⁄cult to predict theexact outcome of any particular regime in a patient.These problemsmean that it is unlikely that priming willever become widely established as a means to facilitaterapid-sequence intubationwithmedium-durationmusclerelaxants.
Reversal of action
Any prolonged period of postoperative muscle paralysisis associated with costly patient monitoring (because ofthe need for continued ventilatory support) and an in-creased risk of adverse complications such as hypostaticpneumonia. Therefore, considerable importance isplaced on the ability to rapidly terminate the action ofmuscle relaxants at the conclusion of the surgical proce-dure. Several di¡erent approaches have been taken todeveloping muscle relaxant regimes that can be rapidlyterminated (Fig. 6). One of these is the development ofcompounds with an inherent molecular instability thatare rapidly degraded (either spontaneously or throughenzymatic action) once injected into the body. Perhapsthe best example of how degradation can in£uence thetime course of action of a muscle relaxant comes notfrom the competitive (non-depolarizing) class of agentsbut from the depolarizing (non-competitive) class. Theelimination of suxamethonium is known to involve itsmetabolism by pseudocholinesterase in the plasma.Thise¡ect is very rapid, the drug having a typical duration ofaction of 2^6min following intravenous administration.
Inactiveeceptor/antagonist
complex
B D C
MR
(+) (+)
(+)
(-)
CA
Inactiveeceptor/antagonist
complex
B D C
MR
(+) (+)
(+)
(-)
CA
Inactiveeceptor/antagonist
complex
B D C
MR
(+) (+)
(+)
(-)
CA
Inactiveeceptor/antagonist
complex
B D C
MR
(+) (+)
(+)
(-)
CA
le for the rapidreversal oftheneuromuscular blockingaction of abolism (A), spontaneous (B) and AChE-facilitated (C) degradation(D).MR,musclerelaxant;AChE, acetylcholinesterase;CA, chelat-neuromuscular transmission.

Rocuronium
Molecule
O
O
OH
OH
CH2SCH2CH2CO2Na
O
OOH
OH
CH
2S
CH
2C
H2C
O2N
a
O
O
OH
OH
CH2SCH2CH2CO2Na
O
O OH
OH
CH
2S
CH
2C
H2C
O2N
a
O
O
OH
OH
CH2 S
CH2 C
H2 C
O2 N
a
O
O
OH
OH
CH 2
SCH 2
CH 2
CO2Na
O
O
OH
OH
CH2S
CH2C
H2C
O2N
a
O
O
OH
OH
CH2SCH2CH2CO2Na
Rocuronium
Molecule
O
O
OH
OH
CH2SCH2CH2CO2Na
O
O
OH
OH
CH2SCH2CH2CO2Na
O
OOH
OH
CH
2S
CH
2C
H2C
O2N
a
O
OOH
OH
CH
2S
CH
2C
H2C
O2N
a
O
O
OH
OH
CH2SCH2CH2CO2Na
O
O
OH
OH
CH2SCH2CH2CO2Na
O
O OH
OH
CH
2S
CH
2C
H2C
O2N
a
O
O OH
OH
CH
2S
CH
2C
H2C
O2N
a
O
O
OH
OH
CH2 S
CH2 C
H2 C
O2 N
a
O
O
OH
OH
CH2 S
CH2 C
H2 C
O2 N
a
O
O
OH
OH
CH 2
SCH 2
CH 2
CO2Na
O
O
OH
OH
CH 2
SCH 2
CH 2
CO2Na
O
O
OH
OH
CH2S
CH2C
H2C
O2N
a
O
O
OH
OH
CH2S
CH2C
H2C
O2N
a
O
O
OH
OH
CH2SCH2CH2CO2Na
O
O
OH
OH
CH2SCH2CH2CO2Na
Figure 7 Chemical structure of Org 25969.Themolecule is aring of eight1^4 linked glucose molecules, eachwith a thiolatedacid residue (positively charged) on carbon-6. The acid side-chains increase the attraction between the cyclodextrin mole-cule and the basic (negativelycharged) rocuroniummolecule.
MUSCLERELAXANTS:PAST,PRESENTANDFUTURE 45
Individuals with impaired pseudocholinesterase activityare known to su¡er prolonged neuromuscular block fol-lowing administration of suxamethonium that, becauseof the depolarizing nature of the neuromuscular block,is unresponsive to any therapeutic intervention.Compounds whose action is in£uenced by their che-
mical degradation usually have a short duration of actionand require either repeatedbolus administration or con-tinuous infusion tomaintain paralysis for a long period oftime.When delivery of new drug is stopped, the rapidelimination of any compoundremaining in the circulationleads to a rapid recovery from neuromuscular block.One clear advantage of this form of drug elimination isthat it is independent of metabolismwithin either the li-ver or kidneys and therefore the kinetics of these com-pounds are not unduly altered in patients with impairedrenal or hepatic function. Atracurium and cisatracuriumundergo spontaneous degradation through a processknown as Hofmann elimination while mivacurium is me-tabolized by plasma pseudocholinesterase. Mivacurium,like suxamethonium, produces an inappropriately longneuromuscular block in patients with low or atypicalpseudocholinesterase activity but, unlike suxametho-nium, this can be terminatedby the action of an anticho-linesterase drug (see below).Not all clinically e¡ective competitive nAChR antago-
nists are fragile enough to rely on spontaneous (or enzy-matic) degradation for the termination of their action.However, the establishedmechanism for the reversal ofneuromuscular block is to inhibit themetabolism of AChat the neuromuscular junction with a selective acetyl-cholinesterase agent such as neostigmine. It is preciselybecause competitive (non-depolarizing) but not non-competitive (depolarizing) muscle relaxants can be re-versed by an anticholinesterase that so much time ande¡ort has been placed on looking for a fast-acting non-depolarizing replacement for suxamethonium over thelast few decades. However, anticholinesterase agentsthemselves are not without their own set of problems.They facilitate the action of ACh at all cholinergic sy-napses.Therefore, in addition to their neuromuscular ef-fect, they will lead to an over-stimulation of ganglionicnicotinic synapses (resulting in marked e¡ects on thecardiovascular system such as bradycardia and hypoten-sion) and an over-stimulation of muscarinic synapses inthe parasympathetic nervous system (resulting in in-creased bronchial and salivary secretions, diarrhoea andabdominal cramps)Falthough these latter e¡ects aremoderated by the co-administration of the mAChR an-tagonist atropine. Therefore, one of the most excitingrecent developments in the area of neuromuscularreversal is the emerging concept of using chelation as ameans to remove a muscle relaxant from the systemand hence accelerate recovery. The experimental com-pound Org25969 (Fig. 7) is a substituted cyclodextrinderivative that has extremely high binding a⁄nities for
the aminosteroidal neuromuscular blocking drugs, andin particular rocuronium. The muscle relaxant binds tothe cyclodextrin in a one-to-onemolecular complexren-dering it pharmacologically inactive.Preclinical investiga-tions have established that the chelating agent canproduce reversal of neuromuscular block comparable tothat seenwith the anticholinesterase agent neostigmine.However, the cyclodextrin has no signi¢cant cardiovas-cular e¡ects of its own and as such represents a signi¢-cant improvement over neostigmine.33,34
WHATDOESTHEFUTUREHOLDFORMUSCLERELAXANTS?Since their introduction nearly half a century ago,musclerelaxants have undergone an evolutionary process thatstarted with ‘dirty’ compounds such as tubocurarine,fazidinium and gallamine with their long time course ofaction and serious cholinergic and non-cholinergicside-e¡ects and, most recently, has reached the stagewhere anaesthetists have access to compounds such asrocuronium and cisatracurium that have short-to-intermediate duration of action and a relatively cleanclinical pro¢le. Will the evolution continue? What arethe next targets to aim for? Many have now acceptedthat rapid onset comes at an appreciable cost (increasedincidence of side-e¡ects) and ultimately, whether anynew muscle relaxant ever establishes itself within theanaesthetist’s armamentarium will depend on a patient-by-patient analysis of the cost:bene¢t ratio. Certainly,

46 CURRENT ANAESTHESIA & CRITICALCARE
there are still those who believe the goal of a short-act-ing non-depolarizing replacement for suxamethonium isstill achievable, typi¢ed by the recent extensive study ofthe tropinyl diester derivativeTAAC3, a non-depolariz-ing muscle relaxant with a rapid onset and ultra-shortduration of action.35Whether such newcompounds farebetter than rapacuronium, which showed considerablepromise prior to its widespread introduction and theconsequent identi¢cation of use-limiting adverse side-ef-fects, is yet to be seen.
REFERENCES
1. Paton W D, Zaimis E J. The methonium compounds. Pharmacol
Rev 1952; 4: 219–253.
2. Deneris E S, Connolly J, Rogers S W, Duvoisin R. Pharmacological
and functional diversity of neuronal nicotinic acetylcholine
receptors. Trends Pharmacol Sci 1991; 12(1): 34–40.
3. Paul M, Kindler C H, Fokt R M, Dresser M J, Dipp N C, Yost C S.
The potency of new muscle relaxants on recombinant muscle-type
acetylcholine receptors. Anesth Analg 2002; 94(3): 597–603.
4. Garland C M, Foreman R C, Chad J E, Holden-Dye L, Walker R J.
The actions of muscle relaxants at nicotinic acetylcholine receptor
isoforms. Eur J Pharmacol 1998; 357(1): 83–92.
5. Paul M, Kindler C H, Fokt R M, Dipp N C, Yost C S.
Isobolographic analysis of non-depolarising muscle relaxant
interactions at their receptor site. Eur J Pharmacol 2002; 438
(1–2): 35-43.
6. Hatano Y, Fukuda K, Arai T, Tamai S, Harioka T. Histamine H1
antagonist alone attenuates d-tubocurarine-induced hypotension.
Anesthesiology 1985; 63(6): 730–731.
7. Ishii T M, Maylie J, Adelman J P. Determinants of apamin and d-
tubocurarine block in SK potassium channels. J Biol Chem 1997;
272(37): 23195–23200.
8. Vizi E S, Lendvai B. Side effects of nondepolarizing muscle
relaxants: relationship to their antinicotinic and antimuscarinic
actions. Pharmacol Ther 1997; 73(2): 75–89.
9. Hou V Y, Hirshman C A, Emala C W. Neuromuscular relaxants as
antagonists for M2 and M3 muscarinic receptors. Anesthesiology
1998; 88(3): 744–750.
10. Birmingham A T, Hussain S Z. A comparison of the skeletal
neuromuscular and autonomic ganglion-blocking potencies of five
non-depolarizing relaxants. Br J Pharmacol 1980; 70(3): 501–506.
11. Wilson D F, West A E, Lin Y. Inhibitory action of nicotinic
antagonists on transmitter release at the neuromuscular junction
of the rat. Neurosci Lett 1995; 186(1): 29–32.
12. Bowman W C, Prior C, Marshall I G. Presynaptic receptors in the
neuromuscular junction. Ann N Y Acad Sci 1990; 604: 69–81.
13. Durant N N, Marshall I G, Savage D S, Nelson D J, Sleigh T,
Carlyle I C. The neuromuscular and autonomic blocking activities
of pancuronium, Org NC 45, and other pancuronium analogues, in
the cat. J Pharm Pharmacol 1979; 31(12): 831–836.
14. Chiodini F C, Tassonyi E, Fuchs-Buder T, Fathi M, Bertrand D,
Muller D. Effects of neuromuscular blocking agents on excitatory
transmission and gamma-aminobutyric acidA-mediated inhibi-
tion in the rat hippocampal slice. Anesthesiology 1998; 88(4):
1003–1013.
15. Tian L, Prior C, Dempster J, Marshall I G. Nicotinic antagonist-
produced frequency-dependent changes in acetylcholine release
from rat motor nerve terminals. J Physiol 1994; 476(3): 517–529.
16. Prior C, Tian L, Dempster J, Marshall I G. Prejunctional actions of
muscle relaxants: synaptic vesicles and transmitter mobilization as
sites of action. Gen Pharmacol 1995; 26(4): 659-666.
17. Emala C W, Hirshman C A. A Mechanism for bronchospasm
induced by rapacuronium: M-2 muscarinic receptor antagonism.
Anesthesiology 2001; 95: A1360.
18. Naguib M, Samarkandi A H, Bakhamees H S, Magboul M A, el-
Bakry A K. Histamine-release haemodynamic changes produced
by rocuronium, vecuronium, mivacurium, atracurium and tubo-
curarine. Br J Anaesth 1995; 75(5): 588–592.
19. Doenicke A, Soukup J, Hoernecke R, Moss J. The lack of histamine
release with cisatracurium: a double-blind comparison with
vecuronium. Anesth Analg 1997; 84(3): 623–628.
20. Kopman A F. Pancuronium, gallamine, and d-tubocurarine
compared: is speed of onset inversely related to drug potency?
Anesthesiology 1989; 70(6): 915–920.
21. Kopman A F, Klewicka M M, Kopman D J, Neuman G G. Molar
potency is predictive of the speed of onset of neuromuscular
block for agents of intermediate, short, and ultrashort duration.
Anesthesiology 1999; 90(2): 425–431.
22. Kopman A F, Klewicka M M, Neuman G G. Molar potency is not
predictive of the speed of onset of atracurium. Anesth Analg 1999;
89(4): 1046–1049.
23. Wierda J M, van den Broek L, Proost J H, Verbaan B W, Hennis P
J. Time course of action and endotracheal intubating conditions of
Org 9487, a new short-acting steroidal muscle relaxant; a com-
parison with succinylcholine. Anesth Analg 1993; 77(3): 579–584.
24. Miguel R, Witkowski T, Nagashima H et al. Evaluation of
neuromuscular and cardiovascular effects of two doses of
rapacuronium (ORG 9487) versus mivacurium and succinylcho-
line. Anesthesiology 1999 Dec; 91(6): 1648-1654.
25. Blobner M, Mirakhur R K, Wierda J M et al. Rapacuronium 2.0 or
2.5 mg kg�1 for rapid-sequence induction: comparison with
succinylcholine 1.0 mg kg�1. Br J Anaesth 2000; 85(5): 724–731.
26. Meakin G H, Pronske E H, Lerman J et al. Bronchospasm after
rapacuronium in infants and children. Anesthesiology 2001; 94(5):
926–927.
27. Cooper R, Mirakhur R K, Clarke R S, Boules Z. Comparison of
intubating conditions after administration of Org 9246 (rocur-
onium) and suxamethonium. Br J Anaesth 1992; 69(3): 269–273.
28. Meretoja O A, Brandom B W, Taivainen T, Jalkanen L. Synergism
between atracurium and vecuronium in children. Br J Anaesth
1993 71(3): 440-442.
29. Motamed C, Donati F. Intubating conditions and blockade after
mivacurium, rocuronium and their combination in young and
elderly adults. Can J Anaesth 2000; 47(3): 225–231.
30. Kim K S, Chun Y S, Chon S U, Suh J K. Neuromuscular interaction
between cisatracurium and mivacurium, atracuvium, vecuronium
or rocuronium administered in combination. Anesth 1998; 53:
872–878.
31. Kopman A F, Khan N A, Neuman G G. Precurarization and
priming: a theoretical analysis of safety and timing. Anaesth Analg
2002; 93 (5): 1253-1256.
32. Aziz L, Jahangir S M, Choudhury S N, Rahman K, Ohta Y, Hirakawa
M. The effect of priming with vecuronium and rocuronium on
young and elderly patients. Anesth Analg 1997; 85(3): 663–666.
33. Bom A, Cameron K, Clark J K et al. Chemical chelation as a novel
method of NMB reversalFdiscovery of Org 25969. Eur J
Anaesthesiol 2001; 18 (Suppl 23): 99 (Abstract 16).
34. van Egmond J, van de Pol F, Booji L, Bom A. Neuromuscular
blockade induced by steroidal NMBs can be rapidly reversed by
Org 25969 in the anaesthetised monkey. Eur J Anaesthesiol 2001;
18 (Suppl 23): 100 (Abstract 19).
35. Gyermek L, Lee C, Cho Y M, Nguyen N, Tsai S K. Neuromuscular
pharmacology of TAAC3, a new nondepolarizing muscle relaxant
with rapid onset and ultrashort duration of action. Anesth Analg
2002; 94(4): 879–885.
36. Mirakhur R K, McCourt K C. Rapacuronium: clinical pharmacol-
ogy. Eur J Anaesthesiol 2001; 23 Suppl: 77–82.