Muscle injuries of the rectus femoris muscle. MR …...Muscle injuries of the rectus femoris muscle...
9
Review Rev. Argent. Radiol. 2015;79(4): 182-191 182 Introduction Injury of the quadriceps muscle group is very common in the general population and even more common in athletes, gen- erally due to hyperextension of the hip with knee flexion (in activities which involve kicking, running, martial arts, etc.). It is the most common cause of muscle tear in the lower limbs, second only to the injury of the hamstring muscle group 1,2 . The quadriceps muscle group consists of four muscles: the rectus femoris (RF), vastus lateralis (VL), vastus medialis (VM) and vastus intermedius (VI). Of the four muscles that com- prise this group, the RF is the only one that crosses two joints; therefore, in addition to being part of the group of primary hip flexors, the RF is also a knee extensor 2-5 . Because of this feature, its fusiform shape, its tendency to an eccentric con- traction and its high percentage of type II rapid contraction fibers, the RF is more frequently injured than the rest of the quadriceps vastus muscles 6-9 . Patients with RF injury present with various symptoms; there- fore, imaging methods play an essential role in determining the type of tear, topography and severity. Ultrasound is a low- cost modality and permits examination of muscle fibers and soft tissue, but magnetic resonance imaging (MRI) has higher specificity for diagnosing the etiology, mainly in the subacute and chronic stages of the injury, when soft tissue edema is minor 6,10,11 . This article describes the anatomy and current concepts in MRI of rectus femoris tear, from its proximal insertion site to involvement of the quadriceps tendon. Anatomic aspects of the rectus femoris The RF is the only one of the four portions of the quadriceps that crosses two joints. While the VM, VL and VI extend from the femur to the tibia and are essential for knee extension, the RF extends from the hip bone to the tibia, and also acts as flexor of the coxofemoral joint 12, 13 . The RF is a bipennate muscle; i.e., it is composed of fascicles that are arranged at an angle to the central tendon or oriented with the longitudinal axis of the muscle, giving greater muscle strength 12 . The anatomy of the RF is complex but easily dif- ferentiated on MR imaging (figs. 1 and 2). Its proximal site of insertion is made up of two portions, a direct head (DH) and an indirect or reflected head (IH): the former arises from the anterior inferior iliac spine, while the latter arises from the superior acetabular ridge and the lateral aspect of the hip joint capsule1. The DH acts mainly in the beginning of hip flexion, while the IH acts once the hip joint flexion has started 2 . A few millimeters from their proximal insertion, both heads form a conjoined tendon; however; they are then located at Muscle injuries of the rectus femoris muscle. MR update C.A. Mariluis a, *, J. Cupito b and F. Mamone b a Magnetic Resonance Imaging Department, DIM Centros de Diagnóstico, Ramos Mejía, Buenos Aires, Argentina b Orthopedics Department, DIM Centros de Diagnóstico, Ramos Mejía, Buenos Aires, Argentina Abstract The tear of the anterior rectus femoris is the most frequent injury of the quadriceps muscle group, and one of the most common causes of lower limb muscle lesions (after the injury of the hamstring muscle group). As its anatomy is complex, and symptoms may be unclear, imaging and in particular, Magnetic Resonance Imaging (MRI) provides precise information on the type of tear, topography, extent, and severity. This article presents a detailed description of the anatomy of the RF and a selective study by MRI, with specific technical inputs to optimise this study method. The current concepts of tendinous, myotendinous, and the infrequent myofascial muscle-tendon tears are also addressed, providing key data that must be considered in MRI reports and which are of paramount importance for the orthopedist. © 2015 Sociedad Argentina de Radiología. Published by Elsevier España, S.L.U. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/ licenses/by-nc-nd/4.0/). Keywords: Magnetic Resonance; Recturs femoris; Soft tissue injuries.
Transcript of Muscle injuries of the rectus femoris muscle. MR …...Muscle injuries of the rectus femoris muscle...

Review
Rev. Argent. Radiol. 2015;79(4): 182-191182
Introduction
Injury of the quadriceps muscle group is very common in the general population and even more common in athletes, gen-erally due to hyperextension of the hip with knee flexion (in activities which involve kicking, running, martial arts, etc.). It is the most common cause of muscle tear in the lower limbs, second only to the injury of the hamstring muscle group1,2.The quadriceps muscle group consists of four muscles: the rectus femoris (RF), vastus lateralis (VL), vastus medialis (VM) and vastus intermedius (VI). Of the four muscles that com-prise this group, the RF is the only one that crosses two joints; therefore, in addition to being part of the group of primary hip flexors, the RF is also a knee extensor 2-5. Because of this feature, its fusiform shape, its tendency to an eccentric con-traction and its high percentage of type II rapid contraction fibers, the RF is more frequently injured than the rest of the quadriceps vastus muscles 6-9.Patients with RF injury present with various symptoms; there-fore, imaging methods play an essential role in determining the type of tear, topography and severity. Ultrasound is a low-cost modality and permits examination of muscle fibers and soft tissue, but magnetic resonance imaging (MRI) has higher specificity for diagnosing the etiology, mainly in the subacute and chronic stages of the injury, when soft tissue edema is minor6,10,11.
This article describes the anatomy and current concepts in MRI of rectus femoris tear, from its proximal insertion site to involvement of the quadriceps tendon.
Anatomic aspects of the rectus femoris
The RF is the only one of the four portions of the quadriceps that crosses two joints. While the VM, VL and VI extend from the femur to the tibia and are essential for knee extension, the RF extends from the hip bone to the tibia, and also acts as flexor of the coxofemoral joint12, 13.The RF is a bipennate muscle; i.e., it is composed of fascicles that are arranged at an angle to the central tendon or oriented with the longitudinal axis of the muscle, giving greater muscle strength12. The anatomy of the RF is complex but easily dif-ferentiated on MR imaging (figs. 1 and 2). Its proximal site of insertion is made up of two portions, a direct head (DH) and an indirect or reflected head (IH): the former arises from the anterior inferior iliac spine, while the latter arises from the superior acetabular ridge and the lateral aspect of the hip joint capsule1. The DH acts mainly in the beginning of hip flexion, while the IH acts once the hip joint flexion has started2.A few millimeters from their proximal insertion, both heads form a conjoined tendon; however; they are then located at
Muscle injuries of the rectus femoris muscle. MR updateC.A. Mariluisa,*, J. Cupitob and F. Mamoneb
a Magnetic Resonance Imaging Department, DIM Centros de Diagnóstico, Ramos Mejía, Buenos Aires, Argentinab Orthopedics Department, DIM Centros de Diagnóstico, Ramos Mejía, Buenos Aires, Argentina
AbstractThe tear of the anterior rectus femoris is the most frequent injury of the quadriceps muscle group, and one of the most common causes of lower limb muscle lesions (after the injury of the hamstring muscle group). As its anatomy is complex, and symptoms may be unclear, imaging and in particular, Magnetic Resonance Imaging (MRI) provides precise information on the type of tear, topography, extent, and severity.This article presents a detailed description of the anatomy of the RF and a selective study by MRI, with specific technical inputs to optimise this study method. The current concepts of tendinous, myotendinous, and the infrequent myofascial muscle-tendon tears are also addressed, providing key data that must be considered in MRI reports and which are of paramount importance for the orthopedist.© 2015 Sociedad Argentina de Radiología. Published by Elsevier España, S.L.U. Thisis an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords: Magnetic Resonance; Recturs femoris; Soft tissue injuries.

Rev. Argent. Radiol. 2015;79(4): 182-191
C.A. Mariluis et al.
183
different sites in the thigh. The DH lies in the anterior and slightly medial aspects; it has a short course with a proximal myotendinous junction in the thigh and its tendinous fibers course towards the anterior surface of the RC, blending with the proximal fascia1,14,15. At this level, under normal condi-tions, it may be difficult to anatomically differentiate between the anterior fascia and the myotendinous junction, as there is a slight focal tendon thickening in continuity with the fascia (fig. 1c). On the other hand, the IH has a horizontal ovoid shape; it extends through the muscle belly, then it becomes thinner, reaching the inferior third of the thigh with a lineal shape with a sagittal major axis1,16-18.The quadriceps tendon is a trilaminar structure formed by the coalescence of four tendons. The RF (superficial plane) and vastus intermedius (deep plane) insert on the superior border of the patella, while the VM and VL insert on the medial and lateral aspects, respectively, forming the patellar retinacula
(intermediate plane). Then as the patellar tendon they reach the anterior tuberosity of the tibia19-21.
Magnetic Resonance Imaging
Because of the large size of the RF in the thigh, complete visu-alization of this muscle may be difficult on MRI. For this reason, we suggest first obtaining coronal images with a wide field of view (FOV 400/420 mm) including both thighs, from the anterior-inferior iliac spine to both patellae in order to make a comparative assessment of their volume and determine the site to be studied. Then selective sequences may be obtained with higher resolution, focused on the region of interest.Our study protocol includes coronal and axial T2-weighted fat-suppressed images (repetition time [TR]/echo time [TE] 2500/90 ms), axial double echo T2-weighted images (TR/TE1
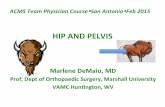
Figure 1, Normal anatomy. Axial proton density (PD)-weighted images: (a) proximal insertion of the DH (black arrow) and (b) of the IH (white arrow); (c) proximal myotendinous junction of the IH (white arrow) and of the DH (black arrow) in the proximal third of the thigh; (d) myotendinous junction of the IH in the middle third of the thigh (white arrow).
a
c
b
d

Rev. Argent. Radiol. 2015;79(4): 182-191
Muscle injuries of the rectus femoris muscle. MR update
184
2400 / 8 ms; TR/TE2 2400/ 110 ms) and coronal T1-weighted images (TR/TE 500/ 18 ms).Optionally, T2-weighted fat-suppressed images may also be obtained in a strict sagittal plane parallel to the thigh axis (pa-tients with myofascial junction injury or myotendinous injury of the DH) and in the sagittal oblique plane paralleling the anterior-inferior iliac spine (when proximal tendinous injuries are suspected). The evaluation may be supplemented with T1-weighted fat-suppressed images to assess blood collec-tions with greater imaging contrast, as they appear sponta-neously hyperintense at the acute stage; gradient echo (GRE) sequences are helpful to identify sequellar lesions with hemo-siderin deposits (blooming effect) appearing as markedly hy-pointense focal areas. Intravenous paramagnetic contrast ad-ministration is not usually necessary, although enhancement may be occasionally observed predominantly in the periphery of acute tears, associated with regionally hypervascularity.
Tear of the rectus femoris and MRI findings
Certain drugs (steroids, fluoroquinolone, among others) as well as a history of diabetes, gout, systemic lupus erythemato-sus, rheumatoid arthritis, kidney failure and obesity may all be predisposing factors for muscle tears. In addition, some cases of bilateral RF tear have been reported in these patients22-25.Muscle injuries most commonly occur in middle-aged male patients due to indirect muscle overload, as a result of dis-
sipation of forces during muscle contraction. Injuries may be caused by a direct mechanism (contusion, laceration) or by an indirect mechanism (stretching of fibers beyond their elastic
Figure 2. Normal anatomy. PD-weighted images in the oblique sagittal plane (a and b) and in the strict sagittal plane (c). (a) The arrow points to the proximal insertion of the DH. (b) The solid arrow points to the insertion of the IH, while the dashed arrow identifies the close contact of both tendon ends proximally. (c) Note the usual trilaminar appearance of the quadriceps tendon with interdigitation of the fatty tissue (arrow).
Figure 3 Patient with a history of direct trauma in the anterior region of the thigh. Axial T2-weighted fat-suppressed image shows hyperintensity of posterolateral fibrillar signal of the RF, demonstrating contusional edema (arrow).
a b c

Rev. Argent. Radiol. 2015;79(4): 182-191
C.A. Mariluis et al.
185
limit by a sudden and forceful contraction). As regards to-pography, these injuries are typically located in the tendon portion, myotendinous junction (most common site of tear) and/or myofascial junction7, 26.Generally, in acute injuries highly marked symptoms often occur immediately after the injury, but in acute injuries of the myotendinous and myofascial junction of the IH of the RF, symptoms may have an insidious onset1, 2. Furthermore, a tear may remain asymptomatic because of recruitment of all other quadriceps muscles, although in this case the patient will not have the same muscle strength he/she had before his/her injury27,28. For this reason, MRI plays an essential role for determining the location, extent and severity of the RF in-jury and, consequently, for establishing a proper therapeutic management. A fibrillar involvement larger than 15% of the muscle area with a length greater than 13 cm and a location central to the muscle belly, has a poor prognosis and longer rehabilitation.An early diagnosis is essential to prevent muscle retraction and formation of scarring29, 30.
Muscle contusion
Contusion is common on the surface of the RF in the thigh. It is characterized by the presence of diffuse myofibrillar edema with no defined tear, with or without associated bruises and
increased muscle volume compared with the contralateral side31 (fig. 3).In cases of RF injury from contusion, or in severe tears, he-matomas are observed, which appear spontaneously hyperin-tense or hypointense on T1-weighted images, depending on the composition and the time of evolution.Hematoma results from intramuscular vein injury and it may be either intramuscular or intermuscular. The former is lim-ited by the intact muscle fascia, which increases intramuscu-lar pressure and consequently compresses bleeding vessels, limiting bleeding and size of hematoma. Instead, the inter-muscular hematoma spreads into the interstitial and inter-fascial spaces due to rupture of the muscle fascia, without an increase in the pressure within the region; therefore the hematoma becomes larger in size31, 32.Chronic hematomas should be differentiated from tumor masses, as both have a heterogeneous appearance. The for-mer may have mural nodules due to neovascularization with a fibrous capsule that appears hypointense in all sequences. Occasionally, the only way to differentiate them is by follow-up, observing a decrease in the size of hematomas2,33,34. For this reason, radiologists should perform an accurate measure-ment of their size and determine the mass effect on adjacent structures, as well as their relationship with the sartorious muscle. If this muscle is compressed, recovery and drainage of metabolites in the area may be impaired1.
Figure 4 Coronal T2-weighted fat-suppressed images show-ing partial tear of the IH (arrow) and slight edema of the proximal myotendinous junction suggestive of grade 1 tear.
Figure 5 Coronal T2-weighted fat-suppressed image shows a peritendinous interstitial edema producing a “feathery” appearance surrounding the IH (arrow), a finding consistent with grade I tear of the myotendinous junction.

Rev. Argent. Radiol. 2015;79(4): 182-191
Muscle injuries of the rectus femoris muscle. MR update
186
Proximal tendon injury
This injury is classified as partial or total (fig. 4). As mentioned above, axial images and sagittal oblique images paralleling the anterior-inferior iliac spine are very useful for determining which tendon is affected (DH and/or IH of the RF), and in the case of complete tears, these images are helpful for an ac-curate measurement of the gap of the tear.These injuries may be associated with avulsion of the anteri-or-inferior iliac spine at the DH, as this tendon acts primarily in early hip flexion, which makes it more vulnerable. Avul-sions typically occur in skeletally immature patients (avulsion of the apophysis of the anterior inferior iliac spine) 2,35,36.Repetitive microtrauma may result in chronic avulsion which must be differentiated from tumors because they present ex-cess bone growth2, 37,38.
Myotendinous junction injury
Myotendinous junction injury is the most common type of tear of the RF (especially for the IH), as this is a point of bio-mechanical weakness of the muscle. As regards the severity of myotendinous junction injuries, there are three categories2:• Grade I: microscopic injury with no functional loss. The MRI
shows edema and peritendinous interstitial hemorrhage with no focal area of tear. Edema extends into adjacent muscle fibers producing a “feathery” appearance (fig. 5). Less than 5% of myofibrils are affected1,6.
• Grade II: partial tear with partial loss of muscle strength and range of motion. The MRI shows partial tear of the myo-tendinous junction; the appearance of the tear will depend on the extent and age of the injury. In acute injuries, there is a fluid-filled partial defect and hemorrhage surrounding the myotendinous junction. In axial T2-weighted sequences the bull’s eye sign has been seen, characterized by a hypoin-tense central tendon surrounded by an area of hyperinten-sity (hemorrhage and peritendinous fluid)2,38 (fig. 6).
• Grade III: complete tear with or without retraction with complete functional impairment2 (fig. 7).
The location of the myotendinous junction injury of the DH is anterior and proximal to the thigh. On MRI, this injury typi-cally presents as edema and fluid between the proximal and anterior third of the RF and the muscle fascia. Because of its proximity to the anterior fascia, it may be difficult to dis-tinguish a myotendinous junction injury from a tear of the myofascial junction. Some authors suggest that myotendi-nous junction injuries of the DH may be associated with some myofascial component1.Anatomically, the myotendinous junction of the IH has a greater cephalocaudal extension than the DH and it is located at the center of the fibers of the RF muscle belly. Therefore, it is far easier to visualize an injury at this level on MRI. Such injuries are usually located between the proximal and middle thirds of the thigh; fluid and edema are irregularly seen, de-pending on the severity of the injury1,2.
Figure 6 Grade II tear of the myotendinous junction of the IH. Axial (a) and coronal (b) T2-weighted fat-suppressed images show peritendinous edema (solid arrow) and focal disconti-nuity of muscle fibers with fluid content (dashed arrow). Note the bull’s eye sign in the axial plane with central IH.
Figure 7 Axial T2-weighted fat-suppressed image showing the absence of the IH with complete discontinuity of the myotendinous junction and a heterogeneous area with intra-muscular hematoma (arrow).

Rev. Argent. Radiol. 2015;79(4): 182-191
C.A. Mariluis et al.
187
Myofascial junction injury
Myofascial junction injury is less common than the above re-ported injuries, and it usually leads to false negative results in ultrasound scans. Even if this injury may be located at any site of the muscle belly with or without facial disruption, it is usu-ally located between the proximal and middle thirds of the thigh. On MRI, this injury presents as muscle fibers that lose their typical morphology and present signs of edema with partial involvement or complete tear of the adjacent fascia. Fluid collections dissect the plane between the fascia and the muscle belly (intact fascia) (fig. 8) and they may also spread into the intermuscular plane (fascial tear)1 (fig. 9).As noted earlier, it may be difficult to distinguish a myotendi-nous junction tear of the DH from a myofascial tear of proxi-mal and anterior fibers, because of their proximity. On the contrary, a posterolateral myofascial tear can be easily distin-guished from a myotendinous tear of the IH, as the former presents as edema and/or fluid collections distributed eccen-trically to the muscle belly, while the latter is located around the IH at the center of the RF muscle.1,2
Distal tendon injury
As reported earlier, the quadriceps tendon typically has a trilaminar appearance (56% of cases), formed by the con-fluence of all four tendons in three layers (superficial layer: RF; intermediate layer: VM and VL, and deep layer: VI) For this reason, visualization of interdigitating fat among these tendons is normal6. Injury at this level may be partial or to-tal, and affect one or several tendons (fig. 10). This lesion is
frequently located in the superficial layer, i.e., in the portion formed by the RF (fig. 11). Complete tears will require surgi-cal therapy and findings will include retraction of the torn ends of the tendon, waviness of the patellar tendon and a decrease in patellar height10, 20, 21.In general, patients with a history of past injury of the quad-riceps or hamstrings have an increased risk for reinjury of the RF1, 20. For this reason, a single scan may show injuries at acute or chronic stages, and/or as exacerbation of an old injury10, 21.Chronic tears often manifest as fatty replacement and myo-fibrillar atrophy, associated with hypointense linear tracts on T1- and T2-weighted images evidencing fibrosis and scar tis-sue around or adjacent to the tendon. Additionally, a bloom-ing effect can be seen on GRE sequences, with a markedly hypointense signal from hemosiderin deposition2 (fig. 12).For educational purposes, two tables are included as a sum-mary: table 1 describes anatomic aspects of the RF that are relevant for MRI and table 2 summarizes the issues that should be addressed in the radiologist’s report and which are relevant for the orthopedic therapy approach.In conclusion, MR imaging of the RF muscle provides accurate data on the severity and extent of the injury, and it is also helpful to determine whether this injury is a de novo tear or an exacerbation of a chronic tear. A general assessment of the thigh (ideally an initial MRI comparing both thighs) followed by a few selective sequences with a higher resolu-tion in the region of interest can provide accurate informa-tion about the location of the injury. Furthermore, MRI scans play an essential role for differential diagnosis in patients with uncertain symptoms, frequently associated with grade I myo-tendinous junction injury or myofascial junction tear that are difficult to visualize on ultrasound.
Figure 8. Axial T2-weighted fat-suppressed image showing myofascial tear with diffuse fibrillar edema at the center of the RF (solid arrow) associated with he-matoma located between the muscle belly and the intact fascia (dashed arrow).
Figure 9 Myofascial tear with fascial dis-continuity. Axial PD-weighted image showing hematoma (solid arrow) with dis-continuity of the muscle fascia in the pos-terolateral site and waviness of the torn end of the fascia (dashed arrow).

Rev. Argent. Radiol. 2015;79(4): 182-191
Muscle injuries of the rectus femoris muscle. MR update
188
Figure 10 Complete tear of the distal tendon of the RF. Coro-nal T1-weighted image showing retraction of the torn end of the distal tendon (solid arrow) associated with waviness of the muscle belly (dashed arrow).
Figure 11 Sagittal T2-weighted fat-suppressed image in a pa-tient with complete tear of the distal tendon of the RF (solid arrow) and intrasubstance injury of the torn end of the tendon. The dashed arrow shows the standard insertion of tendons of the VM and VL (intermediate plane) and VI (deep plane). The scan also shows suprapatellar fat pad edema (asterisk).
Figure 12. Patient with exacerbated chronic tear of the proxi-mal myotendinous junction of the IH (short arrows) and of the posteroalteral myofascial junction of the RF (long arrows). (a) Axial T-weighted fat-suppressed image showing edema from tears in the acute stage. (b) Axial GRE sequence show-ing a hypointense signal from hemosiderin deposit, associ-ated with a past history of sequellar tear.
Table 1: Anatomical and Imaging keys of the rectus femoris.
• The DH contributes to the most medial and anterior aspect of the muscle belly of the rectus femoris and the IH contrib-utes to the posterolateral portion of the RF
• Under normal conditions, the DH can be visualized on MRI at the level of the hip; instead, if there is edema or fluid, it can be visualized in its full length to the proximal third of the thigh.
• Sagittal oblique images paralleling the anterior-inferior iliac spine are helpful for visualization of proximal tendons (DH and IH) and of the gap of the tear.
• Gradient echo (GRE) sequences are helpful to detect hemosiderin deposits in scar injuries. In addition, T1-weighted se-quences identify the presence of fatty replacement in these injuries.
DH: direct head; IH: indirect or reflected head.

Rev. Argent. Radiol. 2015;79(4): 182-191
C.A. Mariluis et al.
189
Ethical responsibilities
Protection of human subjects and animals. The authors de-clare that no experiments were performed on humans or ani-mals for this investigation.Confidentiality of data. The authors declare that this article does not contain patient data.Right to privacy and informed consent. The authors declare that this article does not contain patient data.
Conflicts of interestThe authors declare no conflicts of interest, except for Dr. Mari-luis, who declares a possible conflict of interest as member of the Writing Committee of Revista Argentina de Radiología.
References
1. Kassarjiana A, Rodrigo RM, Santisteban JM. Current concepts in MRI of rectus femorismusculotendinous (myotendinous) and myofascial injuries in elite athletes. Eur J Radiol. 2012;81:3763---71.
2. Bordalo-Rodrigues M, Rosenberg ZS. MR imaging of the proximal rec-tus femoris musculotendinous unit. MagnReson Imaging Clin N Am. 2005;13:717---25.
3. Speer KP, Lohnes J, Garrett WE Jr. Radiographic imaging of muscle strain injury. Am J Sports Med. 1993;21:89---96.
4. Cross TM, Gibbs N, Houang MT, Cameron M. Acute quadriceps muscle strains: magnetic resonance imaging features and prognosis. Am J Sports Med. 2004;32:710---9.
5. Garrett WE Jr. Muscle strain injuries. Am J Sports Med. 1996;24:S2---8.6. Armfield DR, Kim DH, Towers JD, Bradley JP, Robertson DD. Sports-related
muscle injury in the lower extremity. Clin Sports Med. 2006;25:803---42.7. Hughes CT 4th, Hasselman CT, Best TM, Martinez S, Garrett WE Jr. In-
complete, intrasubstance strain injuries of therectus femoris muscle. Am J Sports Med. 1995;23:500---6.
8. Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med. 2001;29:521---33.
9. Nguyen B, Brandser E, Rubin DA. Pains, strains, and fasciculations: lower extremity muscle disorders. Magn Reson Imaging Clin N Am. 2000;8:391---408.
10. Yablon CM, Pai D, Dong Q, Jacobson JA. Magnetic resonance imaging of the extensor mechanism. Magn Reson Imaging Clin N Am. 2014;22:601---20.
11. Swamy GN, Nanjayan SK, Yallappa S, Bishnoi A, Pickering SA. Is ultra-sound diagnosis reliable in acute extensor tendon injuries of the knee? Acta Orthop Belg. 2012;78:764---70.
12. Chaitow L, DeLany J. Human anatomy. En: Chaitow L, DeLany J, editores. Clinical Application of Neuromuscular Techniques: The lower body. Bad-alona, Espa˜na: Paidotribo; 2006. p. 391---501.
13. Latarjet M, Ruiz Liard A. Anatomía humana. Madrid, Espa˜na: Editorial Médica Panamericana; 1999. p. 821---4.
14. Hasselman CT, Best TM, Hughes CT 4th, Martinez S, Garrett WE Jr. An explanation for various rectusfemoris strain injuries using previously unde-scribed muscle architecture. Am JSports Med. 1995;23:493---9.
15. Gyftopoulos S, Rosenberg ZS, Schweitzer ME, Bordalo-Rodrigues M. Normalanatomy and strains of the deep musculotendinous junction of the proximal rectusfemoris: MRI features. AJR Am J Roentgenol. 2008;190:W182---6.
16. Ostlere S. The extensor mechanism of the knee. RadiolClin N Am. 2013;51:393---411.
17. Kramer J, White LM, Recht MP. MR imaging of the extensor mechanism. SeminMusculoskeletRadiol. 2009;13:384---401.
18. Skiadas V, Perdikakis E, Plotas A, Lahanis S. MR imaging of anterior knee pain: a pictorial essay. Knee Surg Sports TraumatolArthrosc. 2013;21:294---304.
19. Zeiss J, Saddemi SR, Ebraheim NA. MR imaging of the quadriceps tendon: normal layered configuration and its importance in cases of tendon rup-ture. AJR Am J Roentgenol. 1992;159:1031---4.
20. Yu JS, Petersilge C, Sartoris DJ, Pathria MN, Resnick D. MR imaging of injuries of the extensor mechanism of the knee. Radiographics. 1994;14:541---51.
21. Perfitt JS, Petrie MJ, Blundell CM, Davies MB. Acute quadriceps tendon rupture: a pragmatic approach to diagnostic imaging. Eur J OrthopSurg-Traumatol. 2014;24:1237---41.
22. Stinner DJ, Orr JD, Hsu JR. Fluoroquinolone-associated bilateral patel-lar tendon rupture: a case report and review of the literature. Mil Med. 2010;175:457---9.
23. Kayali C, Agus H, Turgut A, Taskiran C. Simultaneous bilateral quadriceps tendon rupture in a patient on chronic haemodialysis. (Short-term results of treatment with transpatellar sutures augmented with a quadriceps ten-don flap). OrtopTraumatolRehabil. 2008;10:286---91.
24. Potasman I, Bassan HM. Multiple tendon rupture in systemic lupus ery-thematosus: case report and review of the literature. Ann Rheum Dis. 1984;43:347---9.
25. Ilan DI, Tejwani N, Keschner M, Leibman M. Quadriceps tendon rupture. J Am Acad Orthop Surg. 2003;11:192---200.
26. Souza J, Gottfried C. Muscle injury: review of experimental models. J Elec-tromyogrKinesiol. 2013;23:1253---60.
27. Chang GH, Paz DA, Dwek JR, Chung CB. Lower extremity overuse injuries in pediatric athletes: clinical presentation, imaging findings, and treat-ment. Clin Imaging. 2013;37:836---46.
28. Palmer WE, Kuong SJ, Elmadbouh HM. MR imaging of myotendinous strain. AJR Am J Roentgenol. 1999;173:703---9.
29. Sonin AH, Fitzgerald SW, Bresler ME, Kirsch MD, Hoff FL, Friedman H. MR imaging appearance of the extensor mechanism of the knee: functional anatomy and injury patterns. Radiographics. 1995;15:367---82.
30. Bencardino JT, Rosenberg ZS, Brown RR, Hassankhani A, Lustrin ES, Bel-tran J. Traumatic musculotendinous injuries of the knee:
31. Trojian T. muscle contusion (thigh). Clin Sports Med. 2013;32: 317---24.32. Jarvinen TA, Jarvinen TL, Kaariainen M, Aarimaa V, Vaittinen, Kalimo H,
et al. Muscle injuries: optimising recovery. Best PractRes ClinRheumatol. 2007;21:317---31.
33. Temple HT, Kuklo TR, Sweet DE, Gibbons CL, Murphey MD. Rectus femoris muscle tear appearing as a pseudotumor. Am J Sports Med. 1998;26:544---8.
34. Jaovisidha S, Ryu KN, Hodler J, Schweitzer ME, Sartoris DJ, Resnick D. Hemophilic pseudotumor: spectrum of MR findings. Skeletal Radiol.
Table 2: Magnetic Resonance Imaging report: what does the orthopedist expect?
• Determining the topography of the tear: tendinous (DH and/or IH), myotendinous and/or myofascial junction.• Extent of the tear (approximate percent of fibers affected in a section area).• In cases of complete tear, report measurement of the size of the gap and status of the torn ends of tendons,• Description of the topography and measurement of fluid collections or hematomas (impact on the sartorious muscle?).• Intact or affected muscle fascia.
DH: direct head; IH: indirect or reflected head.

Rev. Argent. Radiol. 2015;79(4): 182-191
Muscle injuries of the rectus femoris muscle. MR update
190
1997;26:468---74.35. Nanka O, Havranek P, Pesl T, Dutka J. Avulsion fracture of the pelvis: sepa-
ration of the secondary ossification center in the superior margin of the acetabulum. Clin Anat. 2003;16: 458---60.
36. Deehan DJ, Beattie TF, Knight D, Jongschaap H. Avulsion fracture of
the straight and reflected heads of rectus femoris. Arch Emerg Med. 1992;9:310---3.
37. Metzmaker JN, Pappas AM. Avulsion fractures of the pelvis. Am J Sports Med. 1985;13:349---58. 38. Boutin RD, Fritz RC, Steinbach LS. Imaging of sports-related.