
Murine Monoclonal Antibodies against Carcinoembryonic Antigen: Immunological … · IMMUNOLOGICAL...
10
[CANCER RESEARCH 50, 2823-2831. May 1, 1990] Murine Monoclonal Antibodies against Carcinoembryonic Antigen: Immunological, Pharmacokinetic, and Targeting Properties in Humans1 Robert M. Sharkey, David M. Goldenberg,2 Hildegard Goldenberg, Robert E. Lee, Cathy Hallante, David Pawlyk, Donald Varga, and Hans J. Hansen Center for Molecular Medicine and Immunology [R. M. S., D, M. G., H. G., R. E. L., C. B., D. P., D. V.], University of Medicine and Dentistry of New Jersey, and Immunomedics, Inc. [H. J. H.J, Newark, New Jersey 07103 ABSTRACT We have examined three I3ll-labeled murine monoclonal antibodies (MAbs) against Carcinoembryonic antigen (CEA), NP-2, NP-3, and NP- 4, after i.v. injection in patients with diverse cancers. Although the MAbs had a similar tumor-targeting ability, several important features were discovered that have led us to the selection of one of these MAbs for further clinical evaluation. We found that it is important to evaluate MAbs with a high immunoreactivity. For example, the M Ah NP-2 was used initially in patients with an immunoreactivity between 35 and 50%. Although the tumor-imaging properties of this M Ah compared favorably with the affinity-purified, goat anti-CEA antibody that we used previ ously, further purification of NP-2 to an immunoreactivity greater than 70% uncovered a previously unknown cross-reactivity with human gran- ulocytes. It was also discovered that the MAbs differed in their ability to complex with CEA in the blood. Plasma samples were analyzed by gel filtration at 1 or 24 h after injection. The formation of complexes with circulating CEA was dependent on the CEA:MAb ratio in the blood. NP- 3 complexed to a greater degree with CEA than MM, but NP-2 did not complex with CEA even at CEA:NP-2 ratios of 55 to 1. NP-3 commonly showed enhanced uptake in the colon by external scintigraphy, and examination of the radioactivity in the stool showed that most of the radioactivity was associated with whole IgG and large-sized fragments of NP-3. We also compared the rate of elimination of radioactivity from the blood for all of the MAbs and compared the clearance of NP-3 to NP-4 at three different ranges of M Ab protein doses (less than 1.0 mg, l to 5 mg, and 5 to 20 mg). The blood clearance rate for NP-3 was fastest among the other MAbs at protein doses exceeding 1.0 mg. Patients given less than 1.0 mg of NP-4 had a significantly (/' < 0.005) shorter elimination half-life than patients given more than 1.0 mg of NP-4. By virtue of NP-4's good targeting properties in patients and its limited complexation with circulating CEA, it was selected as the M Ab of choice for CEA tumor imaging. INTRODUCTION Murine MAbs3 directed against a variety of tumor markers have been examined for their ability to localize human tumors xenografted in animals, as well as in clinical trials (1-3). Per haps the most studied tumor type has been colorectal cancer with antibodies directed against CEA, TAG-72, 17-1A, 19-9, and 79IT (3-10). Since many tumor-reactive MAbs are iden tified during the screening of hybridoma cultures, it is some times difficult to select which MAbs will be most useful for clinical applications. Extensive in vitro assays and in vivo testing in experimental animal models may aid in determining a poten tial candidate for clinical trials, but, more frequently, several MAbs usually remain as primary candidates. In this case, lim ited clinical trials may be necessary to assist the investigator in Received 9/6/89; revised 12/27/89. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1This work was supported in part by USPHS Grant CA39841. 2 To whom requests for reprints should be addressed, at Center for Molecular Medicine and Immunology. 1 Bruce Street. Newark. NJ 07103. 'The abbreviations used are: MAbs. murine monoclonal antibodies; CEA, Carcinoembryonic antigen; EIA. enzyme immunoassay; HAMA, human anti- mouse antibody; HSA, human serum albumin; MA. meconium antigen; MCF, mean channel fluorescence; NCA. nonspecific cross-reacting antigen. selecting a single or even a combination of MAbs that will be best suited for cancer targeting. We have described 4 MAbs against CEA that reacted with 4 distinctly different epitopes on CEA (11, 12). The MAbs were divided into three categories, based on their reactivity with CEA, NCA (13), and MA (14). NP-1 identified an epitope shared among CEA, NCA, and MA; NP-2 and NP-3 reacted with different epitopes that were found only on CEA and MA; and NP-4 identified another epitope that was found only on CEA. Affinity-binding constants measured against I25I-CEA for the MAbs ranged from 5.3 x 10" to 8.9 X 10" (NP-1 > NP-2 > NP-3 > NP-4). NP-1 and NP-2 bind CEA with greater affinity in solutions of low ionic strength, while NP-3 and NP- 4 demonstrate equal affinity for CEA in solutions of low ionic strength and in solutions of physiological ionic strength (11). The presence of these 2 types of determinants on the CEA molecule was first demonstrated with polyclonal antisera (15, 16). It has been our experience that the "ion-sensitive," granu- locyte-cross-reactive determinant is the dominant determinant in raising polyclonal antisera, and, as could be predicted, epi topes present in this determinant are also dominant for the induction of anti-CEA MAbs. In hamsters bearing GW-39 human colonie tumor xenografts in their hind leg muscles, NP- 2 was determined to have the best tumor-targeting properties; the other MAbs were ranked in order of NP-4 = affinity- purified, goat anti-CEA antibody > NP-1 > NP-3 (17). The purpose of this paper is to review our clinical experience with 3 of these MAbs. NP-1 was not used clinically because of its cross-reactivity with NCA, an antigen that is present on human granulocytes (13); by immunohistochemical staining, NP-1 reacted with granulocytes in human tissues (12). During these clinical trials, we discovered additional properties of these MAbs that ultimately influenced our choice of the NP-4 MAb for continued clinical trials. MATERIALS AND METHODS Monoclonal Antibodies. The MAbs used for these studies were de scribed previously by Primus eta!. (11). Since NP-1 had been eliminated from our consideration due to its cross-reactivity with NCA, we con centrated our initial efforts on the purificai ion of NP-2, because it had the highest affinity binding constant of the remaining MAbs. All the MAbs were isolated from mouse ascites. Our initial purification pro cedure for NP-2 involved 3 steps: precipitation with ammonium sulfate (40% saturation); ion exchange chromatography on DEAE-cellulose; followed by adsorption chromatography on hydroxylapatite. This pu rification method later was replaced by Protein A chromatography (see below). These procedures removed all non-IgG proteins from the ascites fluid, as determined by immunoelectrophoresis. When labeled with '"I using the chloramine-T method (18), greater than 90% of the labeled product eluted as IgG. as determined by molecular sieve chromatogra phy (1.6- x 90-cm column of Sephacryl-200; Pharmacia, Piscataway, NJ). The immunoreactivity of the NP-2 purified by the former method, as determined by the percentage of radiolabeled NP-2 that bound to a CEA ¡mmunoadsorbent, was initially 70%, but deteriorated to less than 50% upon storage for 6 mo at 4°Cunder sterile conditions. Although 2823 on March 25, 2020. © 1990 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Transcript of Murine Monoclonal Antibodies against Carcinoembryonic Antigen: Immunological … · IMMUNOLOGICAL...

[CANCER RESEARCH 50, 2823-2831. May 1, 1990]
Murine Monoclonal Antibodies against Carcinoembryonic Antigen: Immunological,Pharmacokinetic, and Targeting Properties in Humans1
Robert M. Sharkey, David M. Goldenberg,2 Hildegard Goldenberg, Robert E. Lee, Cathy Hallante, David Pawlyk,
Donald Varga, and Hans J. HansenCenter for Molecular Medicine and Immunology [R. M. S., D, M. G., H. G., R. E. L., C. B., D. P., D. V.], University of Medicine and Dentistry of New Jersey, andImmunomedics, Inc. [H. J. H.J, Newark, New Jersey 07103
ABSTRACT
We have examined three I3ll-labeled murine monoclonal antibodies(MAbs) against Carcinoembryonic antigen (CEA), NP-2, NP-3, and NP-4, after i.v. injection in patients with diverse cancers. Although the MAbshad a similar tumor-targeting ability, several important features werediscovered that have led us to the selection of one of these MAbs forfurther clinical evaluation. We found that it is important to evaluateMAbs with a high immunoreactivity. For example, the MAh NP-2 wasused initially in patients with an immunoreactivity between 35 and 50%.Although the tumor-imaging properties of this MAh compared favorablywith the affinity-purified, goat anti-CEA antibody that we used previously, further purification of NP-2 to an immunoreactivity greater than70% uncovered a previously unknown cross-reactivity with human gran-ulocytes. It was also discovered that the MAbs differed in their abilityto complex with CEA in the blood. Plasma samples were analyzed by gelfiltration at 1 or 24 h after injection. The formation of complexes withcirculating CEA was dependent on the CEA:MAb ratio in the blood. NP-3 complexed to a greater degree with CEA than MM, but NP-2 did notcomplex with CEA even at CEA:NP-2 ratios of 55 to 1. NP-3 commonlyshowed enhanced uptake in the colon by external scintigraphy, andexamination of the radioactivity in the stool showed that most of theradioactivity was associated with whole IgG and large-sized fragments ofNP-3. We also compared the rate of elimination of radioactivity from theblood for all of the MAbs and compared the clearance of NP-3 to NP-4at three different ranges of M Ab protein doses (less than 1.0 mg, l to 5mg, and 5 to 20 mg). The blood clearance rate for NP-3 was fastestamong the other MAbs at protein doses exceeding 1.0 mg. Patients givenless than 1.0 mg of NP-4 had a significantly (/' < 0.005) shorterelimination half-life than patients given more than 1.0 mg of NP-4. Byvirtue of NP-4's good targeting properties in patients and its limited
complexation with circulating CEA, it was selected as the MAb of choicefor CEA tumor imaging.
INTRODUCTION
Murine MAbs3 directed against a variety of tumor markers
have been examined for their ability to localize human tumorsxenografted in animals, as well as in clinical trials (1-3). Perhaps the most studied tumor type has been colorectal cancerwith antibodies directed against CEA, TAG-72, 17-1A, 19-9,and 79IT (3-10). Since many tumor-reactive MAbs are identified during the screening of hybridoma cultures, it is sometimes difficult to select which MAbs will be most useful forclinical applications. Extensive in vitro assays and in vivo testingin experimental animal models may aid in determining a potential candidate for clinical trials, but, more frequently, severalMAbs usually remain as primary candidates. In this case, limited clinical trials may be necessary to assist the investigator in
Received 9/6/89; revised 12/27/89.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1This work was supported in part by USPHS Grant CA39841.2To whom requests for reprints should be addressed, at Center for Molecular
Medicine and Immunology. 1 Bruce Street. Newark. NJ 07103.'The abbreviations used are: MAbs. murine monoclonal antibodies; CEA,
Carcinoembryonic antigen; EIA. enzyme immunoassay; HAMA, human anti-mouse antibody; HSA, human serum albumin; MA. meconium antigen; MCF,mean channel fluorescence; NCA. nonspecific cross-reacting antigen.
selecting a single or even a combination of MAbs that will bebest suited for cancer targeting.
We have described 4 MAbs against CEA that reacted with 4distinctly different epitopes on CEA (11, 12). The MAbs weredivided into three categories, based on their reactivity withCEA, NCA (13), and MA (14). NP-1 identified an epitopeshared among CEA, NCA, and MA; NP-2 and NP-3 reactedwith different epitopes that were found only on CEA and MA;and NP-4 identified another epitope that was found only onCEA. Affinity-binding constants measured against I25I-CEA forthe MAbs ranged from 5.3 x 10" to 8.9 X 10" (NP-1 > NP-2> NP-3 > NP-4). NP-1 and NP-2 bind CEA with greateraffinity in solutions of low ionic strength, while NP-3 and NP-4 demonstrate equal affinity for CEA in solutions of low ionicstrength and in solutions of physiological ionic strength (11).The presence of these 2 types of determinants on the CEAmolecule was first demonstrated with polyclonal antisera (15,16). It has been our experience that the "ion-sensitive," granu-locyte-cross-reactive determinant is the dominant determinantin raising polyclonal antisera, and, as could be predicted, epitopes present in this determinant are also dominant for theinduction of anti-CEA MAbs. In hamsters bearing GW-39human colonie tumor xenografts in their hind leg muscles, NP-2 was determined to have the best tumor-targeting properties;the other MAbs were ranked in order of NP-4 = affinity-purified, goat anti-CEA antibody > NP-1 > NP-3 (17).
The purpose of this paper is to review our clinical experiencewith 3 of these MAbs. NP-1 was not used clinically because ofits cross-reactivity with NCA, an antigen that is present onhuman granulocytes (13); by immunohistochemical staining,NP-1 reacted with granulocytes in human tissues (12). Duringthese clinical trials, we discovered additional properties of theseMAbs that ultimately influenced our choice of the NP-4 MAbfor continued clinical trials.
MATERIALS AND METHODS
Monoclonal Antibodies. The MAbs used for these studies were described previously by Primus eta!. (11). Since NP-1 had been eliminatedfrom our consideration due to its cross-reactivity with NCA, we concentrated our initial efforts on the purificai ion of NP-2, because it hadthe highest affinity binding constant of the remaining MAbs. All theMAbs were isolated from mouse ascites. Our initial purification procedure for NP-2 involved 3 steps: precipitation with ammonium sulfate(40% saturation); ion exchange chromatography on DEAE-cellulose;followed by adsorption chromatography on hydroxylapatite. This purification method later was replaced by Protein A chromatography (seebelow). These procedures removed all non-IgG proteins from the ascitesfluid, as determined by immunoelectrophoresis. When labeled with '"Iusing the chloramine-T method (18), greater than 90% of the labeledproduct eluted as IgG. as determined by molecular sieve chromatography (1.6- x 90-cm column of Sephacryl-200; Pharmacia, Piscataway,NJ). The immunoreactivity of the NP-2 purified by the former method,as determined by the percentage of radiolabeled NP-2 that bound to aCEA ¡mmunoadsorbent, was initially 70%, but deteriorated to less than50% upon storage for 6 mo at 4°Cunder sterile conditions. Although
2823
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from
IMMUNOLOGICAL AND PHARMACOK1NETIC PROPERTIES OF CEA MAbs
immunoreactivity was reduced on storage, there was no evidence ofchange in the molecular size of the antibody preparation by gel filtration. NP-2 preparations that were affected by prolonged storage will bereferred to as "low immunoreactive" NP-2.
The low immunoreactive NP-2 preparation was used clinically untilwe had developed purification methods by which we were able toimprove and stabilize the immunoreactivity of NP-2 to greater than70%. This was accomplished by using Protein A chromatography inplace of the method given above. The NP-2 preparation purified byProtein A chromatography will be referred to as "high immunoreactive"
NP-2.Ascites fluid was passed over a Protein A-agarose column, and
unbound proteins were eluted with either 0.1 M sodium phosphatebuffer or 0.1 M Tris-HCl buffered saline, pH 8.1. The bound IgG waseluted with 0.1 M sodium citrate buffers of pH 5.5 for NP-3, pH 4.5for NP-4, or pH 3.5 for NP-2. The immunoreactivity of the antibodieswas consistently 80% or higher. In contrast to NP-2, NP-3 and NP-4were stable in storage at 4°Cfor long periods of time. The purity of
these IgG preparations was determined by immunoelectrophoresis,sodium dodecyl sulfate-polyacrylamide gel electrophoresis, and sizeexclusion high-performance liquid chromatography using a MicroPakTSK G3000 SW column (7.5 x 3000 mm; Varian, Walnut Creek, CA).The identity of the pure MAb preparation was established by isoelectricfocusing in agarose gels (Isogel; FMS Bioproducts, Rockland, ME),subclass and light chain-chain type determination was by double geldiffusion, and immunoreactivity was by affinity chromatography of thelabeled antibody on a CEA immunoadsorbent. The bacterial endotoxinlevel was determined for each batch of MAb by a quantitative chrom-ogenic Limulus amoebocyte lysate (LAL) test (Whittaker M. A. Bio-products, Inc., Walkersville, MD). Sterility was tested by the membranefiltration technique (Steritest; Millipore Corp., Bedford, MA) accordingto 21 CRF 610.12. General safety testing was conducted in guinea pigsand mice according to 21 CRF 610.11. Viral and Mycoplasma testswere conducted in accordance with Food and Drug Administrationrecommendations (19).
Radioiodination and Quality Assurance. The MAbs were labeled with'"I purchased from New England Nuclear (North Bellerica, MA). For5- to 10-mCi labeling, the radioisotope was first buffered using 0.1 to0.2 ml of 0.2 M sodium phosphate buffer, pH 7.4. The MAb was addedto the isotope at a ratio of 60 n%of MAb/mCi, and then chloramine-T(0.05 to 0.1 ml) was added at a ratio of 5 ^g/mCi. In all instances, theentire amount of MAb specified for each injection was labeled; i.e.,unlabeled MAb was not added to adjust protein content of the injectate.The iodination proceeded at room temperature for 2 min. Sodiummetabisulfite (0.05 to 0.1 ml) was then added at a ratio of 25 »jg/mCito stop the reaction. The procedure was preparing 25 to 250 mCi ofmI-MAbs required different buffering conditions for the larger volumeof Na'"I and 3- to 5-min reaction time in chloramine-T, but otherwise
similar conditions were followed. The mixture was separated by passageover a PD-10 column (Pharmacia) that was preequilibrated in 0.04 Mphosphate buffer, pH 7.4 (Fisher, Springfield, NJ), containing 0.15 MNaCI and 1% HSA. Radiolabeling efficiencies were greater than 70%with specific activities from 12 to 18 mCi/mg of MAb. Samples fromeach labeling were taken for sterility testing, and a portion of the samplewas diluted in buffer containing 1% HSA for quality assurance testing.Routine quality assurance includes testing for immunoreactivity by-passage over a CEA immunoadsorbent. gel filtration over an S-200column for determination of the amount of unbound radioiodine andmacroaggregated MAb, and the binding to an anti-mouse IgG immunoadsorbent. Typically, there were less than 2% macroaggregated MAband less than 1% unbound radioiodine in each preparation. However,NP-4 preparations had between 3 and 5% unbound iodine. Regardlessof the MAb preparation, greater than 90% of the radioactivity boundto an anti-mouse IgG immunoadsorbent. Immunoreactivities rangedfrom 35 to 50% for the low immunoreactive NP-2. 75 to 85% for thehigh immunoreactive NP-2, 90 to 95% for NP-3, and 80 to 90% forNP-4.
Clinical Studies. For pharmacokinetic and complexing information,patients seen at the Center for Molecular Medicine and Immunologyduring a period from January 1984 to September 1988 were considered.
The total number of évaluablepatients is given in Table 1. The totalnumber of patients évaluablefor tumor targeting by external scintigra-phy is given in Table 8. Many additional patients were évaluablefortargeting with NP-2 than were évaluablefor pharmacokinetic databecause collection of blood was not part of the earlier protocols. Incontrast, pharmacokinetics has been evaluated in additional patientsgiven injections of NP-4 that have not yet been evaluated for tumortargeting because of inadequate follow-up at this time. A more detailedanalysis of the imaging results for these MAbs will be described in alater paper.4
Patients were studied using three different protocols. For many ofthe cases, a diagnostic imaging protocol was followed. In these cases,the patients were given injections of less than 1.0 mg (most frequently0.2 to 0.5 mg) of the radioiodinated MAb (2.5 to 5.0 mCi). In anotherprotocol that was a Phase I/II therapy trial, patients were given injections of 25 to 60 mCi of '"I-NP-2 (2.0 to 5.0 mg) each wk for up to 4
wk (20). A third protocol involved another Phase I/II therapy trialwhere patients were given one injection of 15 to 25 mCi of radiolabeledMAb for radiation dosimetry determinations, and then they receivedanother injection of 50 to 250 mCi (5 to 20 mg) of '"I-labeled MAb 2
wk later.Since some of the patients received prior injections of the same or a
different anti-CEA antibody (goat or MAb), for pharmacokinetic data,we excluded any injection where a measurable HAMA response wasdetected in the preinjection blood sample in order to present theproperties of these MAbs independent of HAMA. We have found thatHAMA causes rapid complexation of the radioantibody, resulting inthe radioantibody being removed more rapidly from the blood than inthe absence of HAM A (20). Although the HAMA titer of most patientsprior to MAb injection was less than 100. we have determined empirically that HAMA titers, measured by the assay used in this study,generally need to exceed 200 to 300 before we observed, by S-200 gelfiltration, macroaggregation of the radiolabeled MAb after its injection.Thus, additional injections were included if the HAMA titer was lessthan 300 prior to the injection of the radioantibody.
After obtaining informed consent, patients were given i.v. injectionsof the radioiodinated MAbs over a 30- to 60-min period. Patients werepretreated with Lugol's (15 drops, 3 times daily) to help reduce radio-
iodine uptake in the thyroid. Potassium perchlorate (200 mg twicedaily) was also given p.o. to reduce gastric uptake of radioiodine. Bothwere prescribed for the duration of these studies. Patients were alsoskin tested prior to radioantibody administration. At 24 and 48 h,planar scans of all body regions were made with a Gemini 700 (Tech-nicare. Solon, OH). Shortly before the imaging studies, "Tc-humanserum albumin and "Tc-pertechnetate (1.0 and 0.5 mCi, respectively)
were injected in order to subtract blood pool and interstitial backgroundactivity, pixel-by-pixel, from the '"I images, according to procedures
published previously (4). At the time of the interpretation, the nuclearmedicine observers were not given any clinical information. The resultswere thereafter correlated with standard clinical detection procedures(computerized tomography, ultrasonography, surgery, etc.), and thesensitivity (true positive/false negative plus true positive) and specificity(true positive plus true negative/total) on a site basis for the chest,hepatic, abdominal, and pelvic regions were determined.
Pharmacokinetic Analysis. The analysis of radioantibody clearancefrom whole blood was determined from samples taken at 5 min, l, 24,48, and 72 h after the end of each injection. More frequent bloodsamples were taken prior to 24 h from patients that were entered in thetherapy trials. The blood clearance curves were fitted as mono- orbiexponential functions according to the least-squares method using acomputer-generated curve-fitting program. The simplest function thatbest fit the data with 95% confidence was used to define the bloodclearance kinetics. The majority of the blood clearance curves fit bestwith a bifunctional curve. The rate of clearance from the blood is givenas the amount of time required for 50% of the radioactivity to beremoved during the single phase or, for 2 phases, distribution («)andelimination (ß)phases with correction for the physical half-life of the
4 D. M. Goldenberg. H. Goldenberg. E. Higginbotham-Ford, R. E. Lee, H. J.Hansen, and R. M. Sharkey. Murine monoclonal antibodies against carcinoem-bryonic antigen: radioimmunodctection findings, manuscript in preparation.
2824
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from
IMMUNOLOGICAL AND PHARMACOKINETICPROPERTIES OF CEA MAbs
Table 1 Summary of ¡henumber of cases évaluablefor blood clearance and complexing studies
MAbNP-2Low
¡mmunoreactivityHighimmunoreactivityNP-3NP-4No.
ofpatients851760No. of injections1752480mg
ofMAb/injection<10511241-5170823>500533
isotope (i.e., values are the biological half-life rather than the effectivehalf-life). Values are also given for the residence time per liter of bloodthat represents the integral under the blood clearance curve normalizedfor the dose injected (mCi).
Radioantibody-CEA Complex Analysis. Since CEA is found in theblood, we examined whether the MAbs would complex with CEA aftertheir injection, and whether complexation significantly changed theblood clearance kinetics. Plasma samples taken at 1 and 24 h afterinjection of the radiolabeled MAbs were passed over 2.6- or 1.6- x 80-to 90-cm columns containing S-200 (Pharmacia). Two- to 5-ml fractions were collected and counted. The columns were periodically calibrated using the initial radiolabeled MAb. In some instances, voidedfractions containing aggregated complexes of the radiolabeled MAbwere analyzed further by incubation with immunoadsorbents containingCEA, goat anti-CEA antibody, or anti-mouse IgG according to methodsdescribed previously (21). Increased binding of the radioactivity fromthe complexée]fraction in comparison with the binding of the initialradiolabeled MAb preparation was used to infer the molecular makeupof the immune complexes. In addition, in vitro complexation studieswere performed to corroborate the in vivo results. For these studies, aplasma sample taken from a patient with 2585 ng/ml of CEA and nodetectable HAMA activity served as a source of CEA. Varying amountsof the plasma were mixed with a constant amount of radiolabeled MAbin a final volume of 1.0 ml. After incubation for l h at 37°C,the
mixture was passed over an S-200 column as described above, and thepercentage of recovered activity in the voided fraction was calculated.Total recoveries exceeded 75%.
Immunoassays for CEA and HAMA. The CEA-EIA used for thesestudies was supplied by Immunomedics, Inc. (Newark, NJ) and hasbeen reported elsewhere (22). The HAMA assay is an enzyme-linkedimmunosorbent assay that has been described previously (22). Briefly,the HAMA assay uses microtiter plates with preadsorbed mouse IgG(2 ^g/well). Serial 10-fold dilution of plasma taken from patients 1 dayprior to radioantibody administration is added to each well and incubated at 37°Cfor 1 h. After washing the plasma for the wells, the wells
are then incubated with peroxidase-conjugated, mouse anti-human IgGFc (Jackson Immunoresearch Laboratories, Inc., Avondale, PA) for 1h. The wells are developed using o-phenylenediamine (Pitman-Moore,Washington Crossing, NJ), and the colored product is read using amicrotiter plate reader at 480 nm. A curve is generated from thedilutions of each plasma sample and the HAMA titer is defined as thedilution of plasma that yields an absorbance reading of 1.0. For eachtest, a plasma sample from a healthy, HAMA-negative donor and aplasma sample from a patient with a previously determined elevatedHAMA titer (55,000) were assayed as negative and positive internalcontrols. The HAMA-negative control titer was consistently less than100. The variation among assays for the HAMA-positive control was10 to 20%.
Fluorescent Flow Cytometry. The MAbs were screened for theirreactivity against human white blood cells using an Ortho Spectrum IIIflow cytometer. Blood from a healthy donor was collected in a vacutai-ner containing EDTA. One hundred ^1 of whole blood were transferredinto a series of conical tubes, and 5 n\ of 2% sodium azide were addedto each. A total of 10, 100, or 1000 ng of each MAb were added to theblood samples in a volume of 0.01 ml. After a 1-h incubation at 37°C,
3 ml of phosphate-buffered saline ingredients, pH 7.2, were added toeach tube, and after centrifugation, the supernatants were removed. Afluorescein-conjugated goat anti-mouse IgG antibody diluted 1:20 inbuffer containing 1% HSA was incubated with the samples for 30 minin an ice water bath. The samples were washed with buffer, and the red
blood cells were lysed using 2 ml of ammonium chloride (8.26 g/liter)in potassium bicarbonate containing tetrasodium EDTA (37 mg/liter).The samples were then analyzed individually by flow cytometry. Evidence of cell binding was apparent only in a region that correspondedto the granulocytes. This region was highlighted, and the number ofcells in this region was quantitated. A blood sample incubated with anantidinitrophenol MAb or only in the fluorescein-conjugated anti-mouse antibody served as negative controls. Region "A" was set according to the fluorescent intensity of the negative control. Region "B"
was defined as those cells with a higher fluorescent intensity than thenegative control. NP-1 was used as a positive control. The reactivity ofthe MAbs against granulocytes is expressed as the percentage of thetotal number of cells in Regions A and B and in the MCF. The MCFdefines the average intensity of the fluorescent signal.
Statistical Analysis. All of the data were analyzed by 3 differentstatistical tests. Included were a one-way analysis of variance using atwo-tailed F test and the Mann-Whitney and Kruskall-Wallis nonpar-ametric tests (23). All 3 tests confirmed significant differences at similarlevels.
RESULTS
Low Immunoreactive NP-2. Eight patients given 1.0 to 3.5mg (35 to 52.5 mCi) of l31I-NP-2 had adequate blood samples
for pharmacokinetic analysis. Table 2 summarizes the individual data for the low immunoreactive NP-2. The average elimination half-life for NP-2 was 50.0 h ±27.8 h (range, 10.1 to95.5 h; median, 44.9 h). Prolonged distribution half-lives (15.3±4.4 h) were observed in the 5 cases with elimination half-livesgreater than 73 h. The average half-life for the distributionphase in the other 6 cases where a biphasic blood clearancecurve was noted was 2.2 ±0.8 h. There was no correlationbetween plasma CEA and radioantibody half-life in the blood(r = 0.36). However, the CEA/NP-2 ratio in the plasma determined at the time of MAb injection was no more than 1.58. In12 of 16 injections, less than 10% of the radiolabeled NP-2 wascomplexed 1 h after completion of the infusion. Complexationdid not increase by 24 h. In the remaining 4 specimens, complexation did not exceed 35% at 1 h, but the blood half-life in3 of 4 of these injections (10.1 to 19.1 h) was noticeably shorterthan the mean half-life. We did not analyze the molecularmakeup of these complexes, but since these 3 injections represented the fourth or fifth injection given to these patients, webelieve that a low-titered HAMA or antiidiotype response mayhave caused the complexation in these samples.
High Immunoreactive NP-2. Expectations of improved tumorlocalization with the high immunoreactive NP-2 were not realized, because there was a high uptake in the bone (presumablyin the marrow) that interfered with the interpretation of theimages (Fig. 1, A and B). This was an unexpected findingbecause, in its initial characterization, NP-2 recognized anepitope on CEA that was not shared with NCA, and immuno-histological staining did not indicate NP-2 reactivity with bloodcells in the tissues. F(ab')2 of NP-2, with an immunoreactivity
of 90%, was prepared and injected into 2 patients, but prominent bone imaging was still seen, thereby ruling out the possibility that the bone uptake was mediated by the Fc portion of
2825
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from
IMMUNOLOGICAL AND PHARMACOKINETIC PROPERTIES OF CEA MAbs
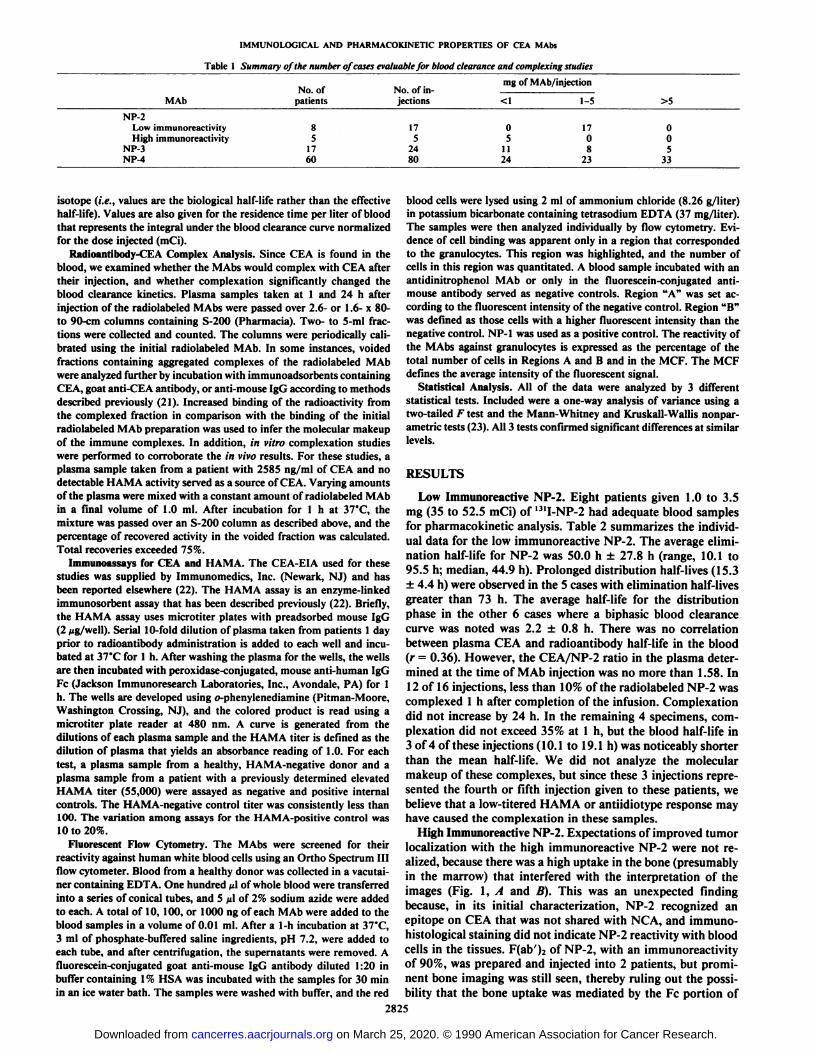
Table 2 Analysis of blood clearance kinetics and completing for low immunoreactive NP-2
PatientCEA
(ng/ml)CEA:NP2
ratio"Complex(%, 1 h)
Blood clearance (r. h)
Distribution Elimination
519
532532
561
566566566
569569569569
612
614614614614
648
17230
454345
8474
118123
79
211472485332
3.7
0.00
0.220.03
0.01
0.030.030.04
0.100.090.130.16
0.15
0.280.481.580.37
0.00
14.0
2.47.5
0.0
0.03.06.0
0.00.00.00.0
25.3
5.54.1
16.235.0
ND*
None
NoneNone
1.7
16.51.82.9
1.18.3
14.520.2
None
2.43.4
NoneNone
17.2
10.1
35.434.8
44.9
75.467.460.1
51.372.684.395.5
29.4
25.932.619.115.4
95.0" The CEA:MAb ratio was calculated, assuming that the molecular weight for CEA is 200.000 and that of M Ab. 160.000, and that the volume of plasma in ;
patient is 4.5% of the body weight.ND, not determined.
Fig. 1. External scintigraphy of patientsgiven injections of '"I-labeled low immunoreactive NP-2 (A), high immunoreactive NP-2(B), or NP-3 (C). Anterior pelvic views taken24 h after radioantibody injection of cases 612il) and 703 (B) illustrate the enhanced boneimaging (B, arrows) with the high immunoreactive NP-2, but not the low immunoreactiveNP-2. In C, the arrows show in Case 686 theactivity present in the transverse and descending colon 72 h after injection of 131I-NP-3.
NP-2. Attempts to circumvent the bone uptake by the pread-ministration of cold NP-2 (1.5 or 20 mg) in 2 patients alsofailed.
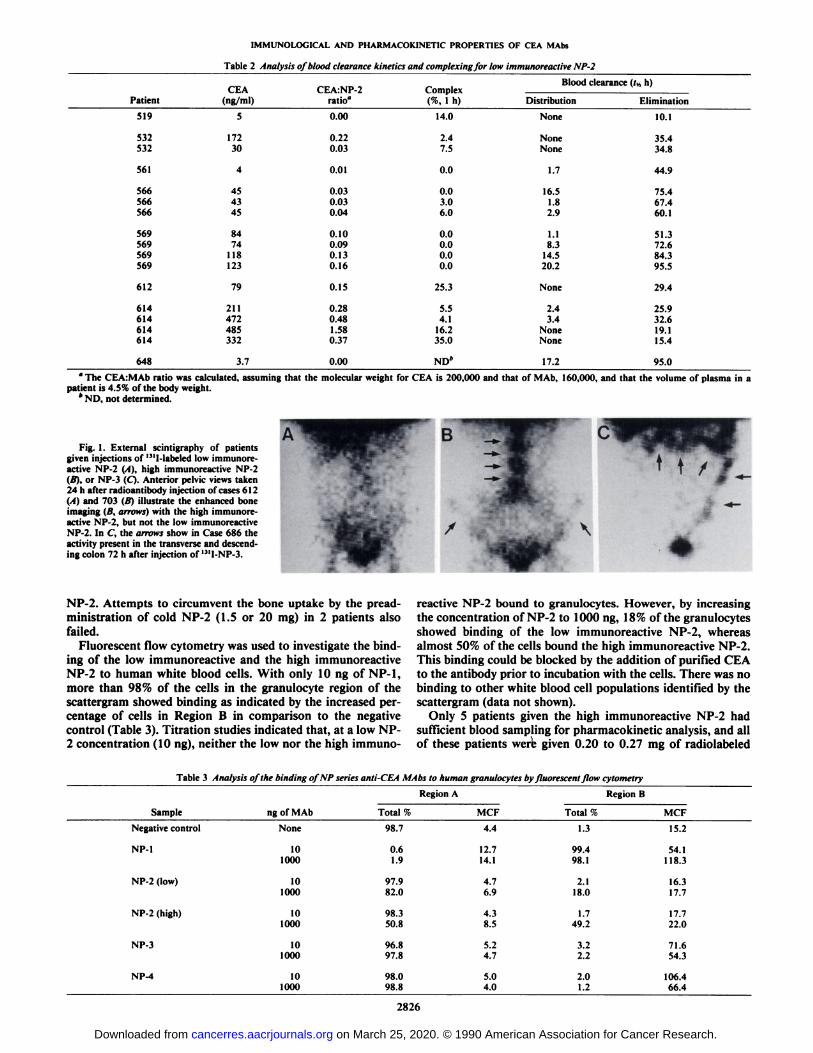
Fluorescent flow cytometry was used to investigate the binding of the low immunoreactive and the high immunoreactiveNP-2 to human white blood cells. With only 10 ng of NP-1,more than 98% of the cells in the granulocyte region of thescattergram showed binding as indicated by the increased percentage of cells in Region B in comparison to the negativecontrol (Table 3). Titration studies indicated that, at a low NP-2 concentration (10 ng), neither the low nor the high immuno
reactive NP-2 bound to granulocytes. However, by increasingthe concentration of NP-2 to 1000 ng, 18% of the granulocytesshowed binding of the low immunoreactive NP-2, whereasalmost 50% of the cells bound the high immunoreactive NP-2.This binding could be blocked by the addition of purified CEAto the antibody prior to incubation with the cells. There was nobinding to other white blood cell populations identified by thescattergram (data not shown).
Only 5 patients given the high immunoreactive NP-2 hadsufficient blood sampling for pharmacokinetic analysis, and allof these patients were given 0.20 to 0.27 mg of radiolabeled
Table 3 Analysis of the binding ofNP series anti-CEA MAbs to human granulocytes byfluorescent flow cytometry
RegionASampleNegative
controlNP-1NP-2
(low)NP-2
(high)NP-3NP-4ng
ofMAbNone10
100010
100010
100010
100010
1000Total
%98.70.6
1.997.9
82.098.3
50.896.8
97.898.0
98.8MCF4.412.7
14.14.76.94.3
8.55.24.75.04.0Region
BTotal
%1.399.4
98.12.1
18.01.749.23.2
2.22.0
1.2MCF15.254.1
118.316.317.717.7
22.071.6
54.3106.4
66.4
2826
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from
IMMUNOLOGICAL AND PHARMACOKINETIC PROPERTIES OF CEA MAbs
Table 4 Blood clearance data for patients receiving high immunoreactive NP-2
CEAiMAbPatientCEA (ng/ml)ratio696699700701703531152283220.591.642.140.030.35Blood
clearance (fwh)Distribution
Elimination0.200.210.230.450.2023.037.433.044.956.8Table
5 Blood clearance and complexation data for patients givenNP-3CF.A:NP-3
ComnlexPatient668708709724730741741744757764769CEA(ng/ml) ratio (%, 1h)16308835484113572615Injected
doseran¡0.206.660.130.010.050.631.010.160.700.110.04Blood
clearance ((»h)DistributionElimination•e,
0.2-1.0mgND°68.08.63.73.020.926.0ND40.313.222.62.90.3None0.3None2.80.8None1.2None0.925.762.749.442.632.514.219.327.016.432.618.7Injected
dose range, 1.0-2.0mg53268468671873774175676533725523307566910063800.050.010.654.481.400.211.890.842.93.442.991.425.422.972.241.7NoneNone1.23.5None2.9None15.140.620.120.142.67.618.126.444.2Injected
dose range, 5.0-17.0mg684686737741765152541600716890.010.200.310.020.245.314.713.04.214.75.91.61.89.39.820.622.223.132.737.0
" ND, not determined.
NP-2 (Table 4). The mean half-life of this NP-2 was 39 ±12.7h (range, 23 to 56.8 h). All of these cases were biphasic with anaverage distribution phase half-life of 0.26 ±0.1 h. Since it wasnot part of the protocol at the time these patients were studied,HAMA titers were not determined, and plasma samples werenot evaluated for complex formation. However, all of theseinjections represented the patients' first exposure to MAb.
Although the low immunoreactive NP-2 could be used fortumor imaging, it was decided that the reactivity with granulo-cytes that resulted in undesirable uptake in the bone limited theuse of NP-2 for more extensive tumor imaging and therapytrials.
NP-3. Preparations of NP-3 were greater than 90% immunoreactive, and there was no evidence of granulocyte binding(Table 3). Seventeen patients (24 injections) were évaluableforpharmacokinetic analysis (Table 5). Ten patients (11 injections)were given less than 1.0 mg of NP-3, 8 patients were given 1-to 2-mg doses, and 5 patients were given 5 to 16 mg. There wasno significant difference in the blood clearance propertiesamong all three dosages of NP-3, but the small number ofsamples for the high dosage of NP-3 may not permit adequatestatistical interpretation. Since all of the patients given morethan 5 mg of NP-3 had prior injections, we compared theclearance kinetics of these paired injections. In 3 of 5 injections(Cases 684, 686, and 765), no differences were found in theirclearance rate. However, differences were found for the pairedinjections of cases 737 and 741. There was no significantdifference between the rate of clearance for high immunoreac
tive NP-2 and NP-3, but the low immunoreactive NP-2 wascleared from the blood at a significantly slower rate than NP-3(/*< 0.01; see Table 7). In 8 of 24 injections the blood clearance
curve was monophasic, but in the remaining 16 cases thedistribution phase averaged 3.8 ±4.2 h.
Gel filtration analysis of plasma taken from these patientsshowed that, in a majority of the cases, radiolabeled NP-3 hadbeen complexed. In several of these cases, anti-mouse IgG,CEA, goat anti-CEA, and anti-human IgG immunoadsorbentswere used to determine the molecular makeup of the complexes(Table 6). The complexes bound to a CEA immunoadsorbentand an anti-CEA immunoadsorbent, indicating that the complexes were composed of NP-3 complexed with CEA, but stillcapable of binding to CEA. The relatively low binding of thecomplexes to the anti-CEA immunoadsorbent may have beendue in part to steric hindrance by the NP-3 bound to CEA inthe complex. Because there was no binding of the radioactivityto the anti-human IgG immunoadsorbent, HAMA was notbelieved to be responsible for the complexation. The amount ofcomplex formation was related directly to the ratio of CEA toNP-3 in the blood at the time of injection, with a correlationof 0.89, and in the patients that had paired injections of 1 to 2mg followed by >5 mg, the amount of complexing decreased asthe CEA:NP-3 ratio decreased.
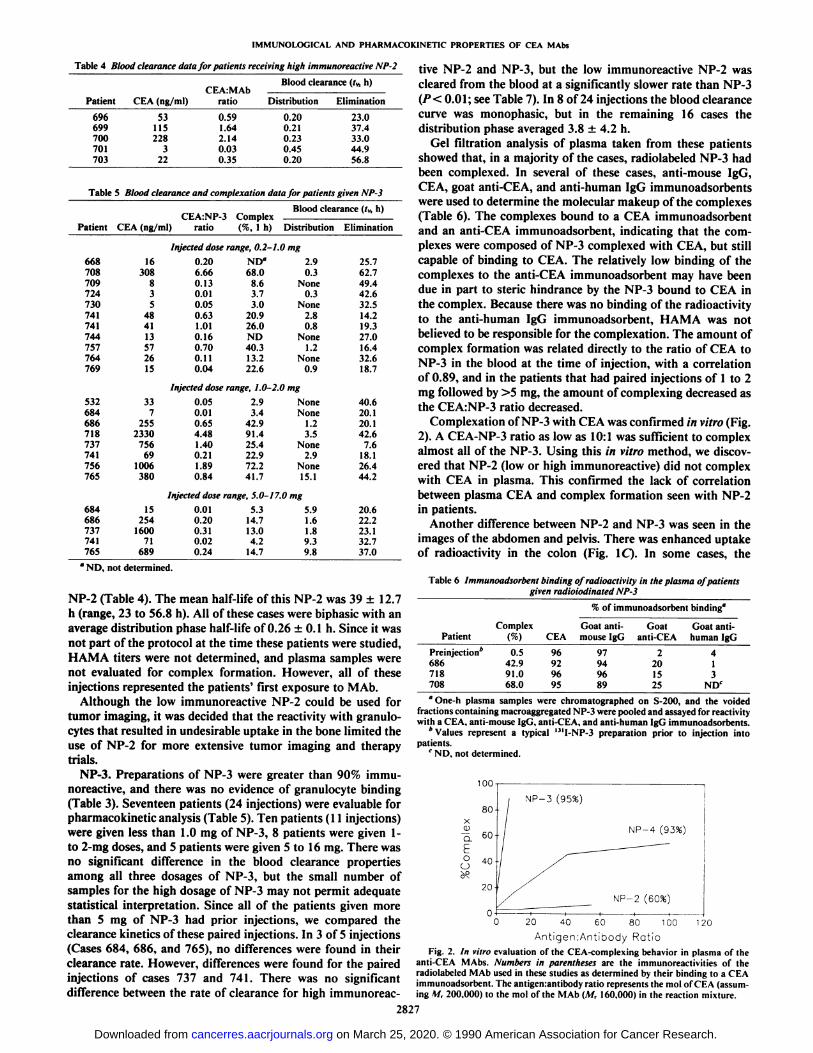
Complexation of NP-3 with CEA was confirmed in vitro (Fig.2). A CEA-NP-3 ratio as low as 10:1 was sufficient to complexalmost all of the NP-3. Using this in vitro method, we discovered that NP-2 (low or high immunoreactive) did not complexwith CEA in plasma. This confirmed the lack of correlationbetween plasma CEA and complex formation seen with NP-2in patients.
Another difference between NP-2 and NP-3 was seen in theimages of the abdomen and pelvis. There was enhanced uptakeof radioactivity in the colon (Fig. 1C). In some cases, the
Table 6 Immunoadsorbent binding of radioactivity in the plasma of patientsgiven radioiodinated NP-3
% of immunoadsorbentbinding"PatientPreinjection*
686718708Complex(%)0.5
42.991.068.0CEA96
929695Goat
anti-
mouseIgG97
949689Goat
anti-CEA2
201525Goat
anti-
humanIgG4
13
NDC
" One-h plasma samples were chromatographed on S-200, and the voided
fractions containing macroaggregated NP-3 were pooled and assayed for reactivitywith a CEA. anti-mouse IgG. anti-CEA, and anti-human IgG ¡mmunoadsorbents.
* Values represent a typical "'I-NP-3 preparation prior to injection into
patients.c ND, not determined.
- DO
6C 80 100 120
Antigen:Antibody RatioFig. 2. In vitro evaluation of the CEA-complc\ing behavior in plasma of the
anti-CEA MAbs. Numbers in parentheses are the immunoreactivities of the
radiolabeled MAb used in these studies as determined by their binding to a CEAimmunoadsorbent. The antigen:antibody ratio represents the mol of CEA (assuming M, 200.000) to the mol of the MAb (M, 160.000) in the reaction mixture.
2827
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from
IMMUNOLOGICAL AND PHARMACOKINETIC PROPERTIES OF CEA MAbs
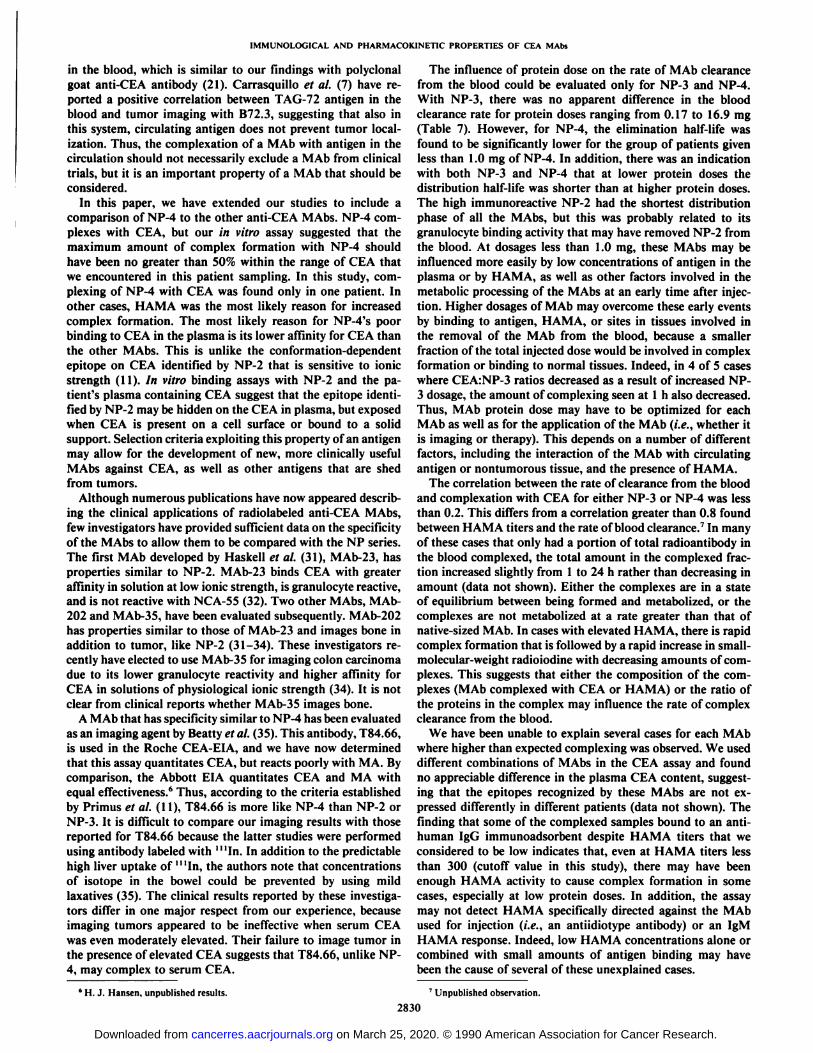
radioactivity appeared to become more distal over time, suggesting that the radioactivity was following the contents of thebowel. In one case, stool taken from a patient 72 h after theinjection of 16.86 mg (250 mCi) of '"I-NP-3 was extractedwith 0.01 Msodium phosphate-buffered saline, pH 7.2. Seventy-five % of the radioactivity in the clarified extract bound to ananti-mouse IgG immunoadsorbent, and by gel filtration, 86.2%of the radioactivity eluted as 2 peaks (Fig. 3). According to thecalibration of the gel filtration column, the first peak was native-sized IgG, and the second peak was probably a large fragmentof the immunoglobulin. Only about 10% of the radioactivityeluted in the total elution volume, indicating that it was a smallmolecular-sized material. The reason for NP-3 localizing in thebowel is unclear, but the fact that NP-3 readily complexed withCEA in the plasma and had undesirable uptake in the colonindicated that this MAb was not suited for more extensiveclinical use.
NP-4. The blood clearance kinetics and complexing wereévaluablein 60 patients (80 injections). Twenty-one patients(24 injections) were given less than 1.0 mg (2.5 to 5.0 mCi) ofNP-4 for diagnostic imaging. An additional 39 patients (56injections) were part of a Phase I/II therapy trial using '"I-NP-
4. Fourteen of these patients were first given 1.0 to 2.5 mg (15to 25 mCi) of NP-4, and about 2 wk later were given 5 to 16mg (70 to 250 mCi) of '"I-NP-4. The remaining patients were
évaluablefor only a single injection of either 1.0 to 2.5 mg or5 to 16mgof '"I-NP-4 IgG.
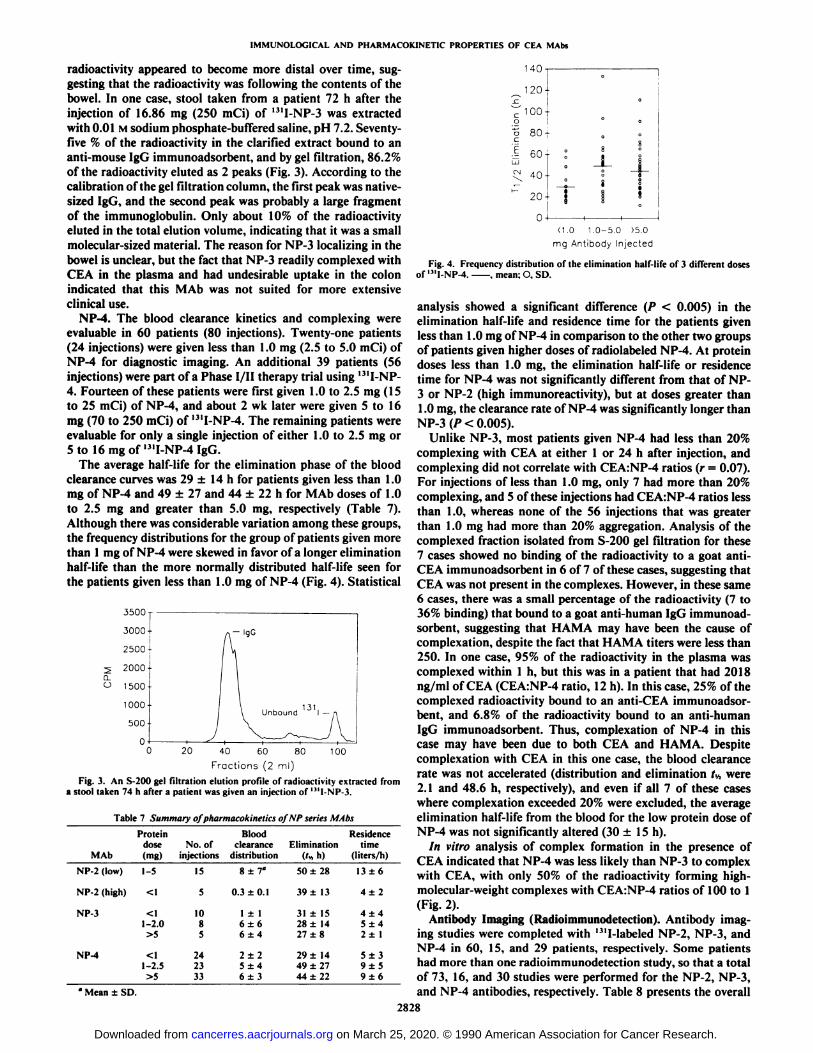
The average half-life for the elimination phase of the bloodclearance curves was 29 ±14 h for patients given less than 1.0mg of NP-4 and 49 ±27 and 44 ±22 h for MAb doses of 1.0to 2.5 mg and greater than 5.0 mg, respectively (Table 7).Although there was considerable variation among these groups,the frequency distributions for the group of patients given morethan 1 mg of NP-4 were skewed in favor of a longer eliminationhalf-life than the more normally distributed half-life seen forthe patients given less than 1.0 mg of NP-4 (Fig. 4). Statistical
3500 r
3000
2500
2000
1500
1000
500-
o
>-lqG
0 20 10040 60 80
Fractions (2 ml)
Fig. 3. An S-200 gel filtration elution profile of radioactivity extracted froma stool taken 74 h after a patient was given an injection of '"I-NP-3.
Table 7 Summary ofpharmacokinetics of NP series MAbs
Protein Blood Residencedose No. of clearance Elimination time
MAb (mg) injections distribution (Iv,h) (liters/h)
NP-2(low)NP-2
(high)NP-3NP-41-5<11-2.01-2.5
>515510
852423
338
±7*0.3
±0.11
±16±66 ±42±2
5±46±350
±2839
±1331
±1528±14
27±829
±1449±2744±2213±64±
24±4
5 ±42±15±3
9±59±6
i tu•120-100-80-60-40-20-•000
08
'
îa-1-§STt
1 !
* Mean ±SD.
<1.0 1.0-5.0 >5.0
mg Antibody Injected
Fig. 4. Frequency distribution of the elimination half-life of 3 different dosesof '"I-NP-4. . mean; O, SD.
analysis showed a significant difference (P < 0.005) in theelimination half-life and residence time for the patients givenless than 1.0 mg of NP-4 in comparison to the other two groupsof patients given higher doses of radiolabeled NP-4. At proteindoses less than 1.0 mg, the elimination half-life or residencetime for NP-4 was not significantly different from that of NP-3 or NP-2 (high immunoreactivity), but at doses greater than1.0 mg, the clearance rate of NP-4 was significantly longer thanNP-3(/><0.005).
Unlike NP-3, most patients given NP-4 had less than 20%complexing with CEA at either 1 or 24 h after injection, andcomplexing did not correlate with CEA:NP-4 ratios (r = 0.07).For injections of less than 1.0 mg, only 7 had more than 20%complexing, and 5 of these injections had CEA:NP-4 ratios lessthan 1.0, whereas none of the 56 injections that was greaterthan 1.0 mg had more than 20% aggregation. Analysis of thecomplexed fraction isolated from S-200 gel filtration for these7 cases showed no binding of the radioactivity to a goat anti-CEA immunoadsorbent in 6 of 7 of these cases, suggesting thatCEA was not present in the complexes. However, in these same6 cases, there was a small percentage of the radioactivity (7 to36% binding) that bound to a goat anti-human IgG immunoadsorbent, suggesting that HAMA may have been the cause ofcomplexation, despite the fact that HAMA titers were less than250. In one case, 95% of the radioactivity in the plasma wascomplexed within 1 h, but this was in a patient that had 2018ng/ml of CEA (CEA:NP-4 ratio, 12 h). In this case, 25% of thecomplexed radioactivity bound to an anti-CEA immunoadsorbent, and 6.8% of the radioactivity bound to an anti-humanIgG immunoadsorbent. Thus, complexation of NP-4 in thiscase may have been due to both CEA and HAMA. Despitecomplexation with CEA in this one case, the blood clearancerate was not accelerated (distribution and elimination tv, were2.1 and 48.6 h, respectively), and even if all 7 of these caseswhere complexation exceeded 20% were excluded, the averageelimination half-life from the blood for the low protein dose ofNP-4 was not significantly altered (30 ±15 h).
In vitro analysis of complex formation in the presence ofCEA indicated that NP-4 was less likely than NP-3 to complexwith CEA, with only 50% of the radioactivity forming high-molecular-weight complexes with CEA:NP-4 ratios of 100 to 1(Fig. 2).
Antibody Imaging (Radioimmunodetection). Antibody imaging studies were completed with '"I-labeled NP-2, NP-3, andNP-4 in 60, 15, and 29 patients, respectively. Some patientshad more than one radioimmunodetection study, so that a totalof 73, 16, and 30 studies were performed for the NP-2, NP-3,and NP-4 antibodies, respectively. Table 8 presents the overall
2828
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from

IMMUNOLOGICAL AND PHARMACOKINET1C PROPERTIES OF CEA MAbs
Table 8 Evaluation of tumor-targeting ability ofanti-CEA MAbs
No. ofpatientsNo.ofstudiesNo.ofsites*No.
of évaluablesitesTruepositiveFalsenegativeTruenegativeFalsepositiveSensitivitySpecificityAccuracyNP-2"6073293192829881382/91
(90.1)*88/101
(87.1)170/192(88.5)NP-31516644817419817/21(81.0)19/27(70.4)36/48
(75.0)NP-429301216925931425/34
(73.5)31/35(88.6)56/69(81.2)
°Low immiinoreactivc NP-2.* Total of all sites in the pelvis, abdomen, liver, and chest.c Numbers in parentheses, percentage.
results summarized for each antibody in terms of sensitivity,specificity, and accuracy based upon sites of tumor in fourregions (chest, liver, abdomen, and pelvis). The sensitivity rateranged from 73.5% for NP-4 to 90.1% for NP-2; the specificityranged from 70.4% for NP-3 to 88.5% for NP-2. A number ofnew tumor sites were revealed by each of the antibodies studied,but the follow-up results and accuracy in revealing occult tumors are beyond the scope of this paper and will, therefore, bediscussed in a subsequent publication.4 It should be noted that
the patients studied with these antibodies represented manydifferent cancer types, but with a predominance of colorectalcarcinoma. Further, the patients had a range of plasma CEAtiters, from normal to very elevated levels, but this did notappear to affect the imaging results with any of the antibodiesstudied. Finally, no difference in the discrimination of tumorsize among the 3 antibodies was appreciated; the usual detectionsensitivity was at about 1.5- to 2.0-cm lesions.
DISCUSSION
We initially identified 3 MAbs that, by in vitro assays, werespecific for CEA without reactivity with NCA (11) and beganclinical trials to assess the utility of these MAbs in comparisonto the polyclonal goat anti-CEA antibody we had used previously for radioimmunodetection studies (4, 5). NP-2 was chosenas the first MAb to be tested, because it had a higher affinityfor CEA than NP-3 or NP-4 (11).
Although NP-2 in our initial clinical trial was only 50%immunoreactive, it compared favorably with the goat antibodyfor tumor imaging, and there was no evidence of uptake innontumorous sites (24). Expectations that the high immunoreactive NP-2 would improve tumor imaging in patients basedon preclinical animal studies that showed a 2-fold increase inthe percentage of uptake in colonie tumor xenografts with thehigh immunoreactive NP-2 in comparison with low immunoreactive NP-25 went unfulfilled when bone imaging was ob
served in patients. Since most patients were given injections ofsmall amounts of NP-2, we did not analyze in vivo the bindingproperties of NP-2 to granulocytes.
Unlike the generally accepted view that higher immunoreac-tivity is better for tumor targeting (25), the results with NP-2show that, for antibodies with cross-reactivity with normaltissues, a lower immunoreactivity may permit tumor targetingwithout interference with normal tissue uptake. The use of highdoses of unlabeled carrier antibody given prior to or coinjectedwith the labeled antibody is another way to reduce normal tissueuptake for those antibodies with cross-reactivity with normaltissues. For examples, Murray et al. (26) have shown that, for
* R. M. Sharkey, unpublished observation.
the 96.5 MAb, uptake in the liver and spleen can be reduced bythe administration of unlabeled 96.5, but not an irrelevantMAb, suggesting that 96.5 MAb binds to normal tissues. Theimmunoreactivity of 96.5 has been reported to vary from 50 to90% due to secretion of nonimmunoreactive MAb from theinitial hybridoma clone (27), but we are unaware of any clinicalcomparisons of low and high immunoreactive 96.5 to determinewhether imaging with the low immunoreactive form was betterthan the high immunoreactivity. Pati et al. (28) found similarprotein dose results with a CEA MAb.
Our experience has shown the importance of adequate MAbpurification in the preclinical screening process to discoverundesirable cross-reactivities with normal tissues. However,even after adequate purification of a MAb, limited clinical trialsare justified because a priori establishment of in vitro assayshas limitations. For example, there was no prior indication thatNP-3 would be taken up in the normal colon, whereas NP-2and NP-4 were not. Since we did not have cytofluorographicfacilities available when the MAbs were first developed, werelied on immunohistochemical staining of tissues and in vitrobinding assays to select the MAbs that did not react with humanwhite blood cells. Obviously, the assays and conditions we chosedid not initially permit us to discover NP-2's cross-reactivity
with granulocytes. Knowledge gained a posteriori enabled us toimprove our understanding of how to design better in vitroscreening methods. Therefore, limited clinical trials can be usedto assist in the selection of MAbs and may help expedite theselection of MAbs with the highest clinical potential.
Animal studies indicated that the high immunoreactive NP-2 had the best tumor targeting of all the anti-CEA MAbs (17).There was no uptake in the bone observed when these animalswere imaged, because the cross-reactive antigen is not found onhamster granulocytes.5 It was interesting that NP-3 had thepoorest tumor-targeting properties in our animal studies, andNP-4 was second to NP-2. Although these findings are nowconsistent with our clinical results, the justification for ourdecision not to use NP-3 for further clinical studies was unrelated to the tumor targeting of NP-3 in xenograft models, butrather other properties of NP-3 that only became apparent aftera limited clinical trial. For example, the excessive amount ofradioactivity in the colon of patients given NP-3 was notapparent in the animal studies, and since CEA is not found inthe plasma of hamsters bearing small GW-39 tumors (29), thecomplexing of NP-3 with CEA was also not found. In addition,the animal studies were done with a single human colonie tumorcell line (GW-39), so we could not be certain that the NP-3epitope was not expressed as well in this tumor as were theother epitopes. Despite NP-3's shortcomings, we were able to
localize tumors in patients to almost the same extent as lowimmunoreactive NP-2 and NP-4, presumably since most of thetumors were distant from the colon. Thus, although animalstudies are useful, by themselves they may not be able to bereliably used to select the most clinically useful MAb.
Goldenberg et al. (30) reported that NP-2 did not complexwith CEA in the blood, but NP-2 bound to CEA that wasaffixed to a solid support, such as Sepharose 4B or Affi-gel. Atthe time, this finding reinforced our consideration of NP-2 forclinical studies, because tumor targeting with NP-2 would notbe influenced by CEA in the plasma. NP-3, on the other hand,complexed with CEA in the blood, but this did not appreciablyinfluence its ability to target tumors (30). Our finding that thecomplexes isolated from the plasma of patients were still ableto bind to a CEA immunoadsorbent may explain the ability ofNP-3 to localize tumors even after complexation with antigen
2829
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from
IMMUNOLOGICAL AND PHARMACOK1NETIC PROPERTIES OF CEA MAbs
in the blood, which is similar to our findings with polyclonalgoat anti-CEA antibody (21). Carrasquillo et al. (7) have reported a positive correlation between TAG-72 antigen in theblood and tumor imaging with B72.3, suggesting that also inthis system, circulating antigen does not prevent tumor localization. Thus, the complexation of a MAb with antigen in thecirculation should not necessarily exclude a MAb from clinicaltrials, but it is an important property of a MAb that should beconsidered.
In this paper, we have extended our studies to include acomparison of NP-4 to the other anti-CEA MAbs. NP-4 complexes with CEA, but our in vitro assay suggested that themaximum amount of complex formation with NP-4 shouldhave been no greater than 50% within the range of CEA thatwe encountered in this patient sampling. In this study, com-plexing of NP-4 with CEA was found only in one patient. Inother cases, HAMA was the most likely reason for increasedcomplex formation. The most likely reason for NP-4's poor
binding to CEA in the plasma is its lower affinity for CEA thanthe other MAbs. This is unlike the conformation-dependentepitope on CEA identified by NP-2 that is sensitive to ionicstrength (11). In vitro binding assays with NP-2 and the patient's plasma containing CEA suggest that the epitope identi
fied by NP-2 may be hidden on the CEA in plasma, but exposedwhen CEA is present on a cell surface or bound to a solidsupport. Selection criteria exploiting this property of an antigenmay allow for the development of new, more clinically usefulMAbs against CEA, as well as other antigens that are shedfrom tumors.
Although numerous publications have now appeared describing the clinical applications of radiolabeled anti-CEA MAbs,few investigators have provided sufficient data on the specificityof the MAbs to allow them to be compared with the NP series.The first MAb developed by Haskell et al. (31), MAb-23, hasproperties similar to NP-2. MAb-23 binds CEA with greateraffinity in solution at low ionic strength, is granulocyte reactive,and is not reactive with NCA-55 (32). Two other MAbs, MAb-202 and MAb-35, have been evaluated subsequently. MAb-202has properties similar to those of MAb-23 and images bone inaddition to tumor, like NP-2 (31-34). These investigators recently have elected to use MAb-35 for imaging colon carcinomadue to its lower granulocyte reactivity and higher affinity forCEA in solutions of physiological ionic strength (34). It is notclear from clinical reports whether MAb-35 images bone.
A MAb that has specificity similar to NP-4 has been evaluatedas an imaging agent by Beatty et al. (35). This antibody, T84.66,is used in the Roche CEA-EIA, and we have now determinedthat this assay quantitates CEA, but reacts poorly with MA. Bycomparison, the Abbott EIA quantitates CEA and MA withequal effectiveness.6 Thus, according to the criteria establishedby Primus et al. (11), T84.66 is more like NP-4 than NP-2 orNP-3. It is difficult to compare our imaging results with thosereported for T84.66 because the latter studies were performedusing antibody labeled with '"In. In addition to the predictablehigh liver uptake of "'In, the authors note that concentrations
of isotope in the bowel could be prevented by using mildlaxatives (35). The clinical results reported by these investigators differ in one major respect from our experience, becauseimaging tumors appeared to be ineffective when serum CEAwas even moderately elevated. Their failure to image tumor inthe presence of elevated CEA suggests that T84.66, unlike NP-4, may complex to serum CEA.
The influence of protein dose on the rate of MAb clearancefrom the blood could be evaluated only for NP-3 and NP-4.With NP-3, there was no apparent difference in the bloodclearance rate for protein doses ranging from 0.17 to 16.9 mg(Table 7). However, for NP-4, the elimination half-life was
found to be significantly lower for the group of patients givenless than 1.0 mg of NP-4. In addition, there was an indicationwith both NP-3 and NP-4 that at lower protein doses thedistribution half-life was shorter than at higher protein doses.The high immunoreactive NP-2 had the shortest distributionphase of all the MAbs, but this was probably related to itsgranulocyte binding activity that may have removed NP-2 fromthe blood. At dosages less than 1.0 mg, these MAbs may beinfluenced more easily by low concentrations of antigen in theplasma or by HAMA, as well as other factors involved in themetabolic processing of the MAbs at an early time after injection. Higher dosages of MAb may overcome these early eventsby binding to antigen, HAMA, or sites in tissues involved inthe removal of the MAb from the blood, because a smallerfraction of the total injected dose would be involved in complexformation or binding to normal tissues. Indeed, in 4 of 5 caseswhere CEA:NP-3 ratios decreased as a result of increased NP-3 dosage, the amount of complexing seen at l h also decreased.Thus, MAb protein dose may have to be optimized for eachMAb as well as for the application of the MAb (i.e., whether itis imaging or therapy). This depends on a number of differentfactors, including the interaction of the MAb with circulatingantigen or nontumorous tissue, and the presence of HAMA.
The correlation between the rate of clearance from the bloodand complexation with CEA for either NP-3 or NP-4 was lessthan 0.2. This differs from a correlation greater than 0.8 foundbetween HAMA titers and the rate of blood clearance.7 In many
of these cases that only had a portion of total radioantibody inthe blood complexed, the total amount in the complexed fraction increased slightly from 1 to 24 h rather than decreasing inamount (data not shown). Either the complexes are in a stateof equilibrium between being formed and metabolized, or thecomplexes are not metabolized at a rate greater than that ofnative-sized MAb. In cases with elevated HAMA, there is rapidcomplex formation that is followed by a rapid increase in small-molecular-weight radioiodine with decreasing amounts of complexes. This suggests that either the composition of the complexes (MAb complexed with CEA or HAMA) or the ratio ofthe proteins in the complex may influence the rate of complexclearance from the blood.
We have been unable to explain several cases for each MAbwhere higher than expected complexing was observed. We useddifferent combinations of MAbs in the CEA assay and foundno appreciable difference in the plasma CEA content, suggesting that the epitopes recognized by these MAbs are not expressed differently in different patients (data not shown). Thefinding that some of the complexed samples bound to an anti-human IgG immunoadsorbent despite HAMA titers that weconsidered to be low indicates that, even at HAMA titers lessthan 300 (cutoff value in this study), there may have beenenough HAMA activity to cause complex formation in somecases, especially at low protein doses. In addition, the assaymay not detect HAMA specifically directed against the MAbused for injection (i.e., an antiidiotype antibody) or an IgMHAMA response. Indeed, low HAMA concentrations alone orcombined with small amounts of antigen binding may havebeen the cause of several of these unexplained cases.
*H. J. Hansen, unpublished results. 7 Unpublished observation.
2830
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from
IMMUNOLOGICAL AND PHARMACOKINETIC PROPERTIES OF CEA MAbs
In conclusion, these studies show that carefully selectedMAbs against CEA can be used for imaging of cancer in patientswithout concern of complexation to CEA. The granulocytebinding of NP-2 and the excessive complex formation withundesirable imaging of the colon for NP-3 have resulted in ourchoice of NP-4 for further clinical use. Fortunately, NP-4 hasfavorable pharmacokinetic, complexing, and tumor-targetingproperties. We expect that the knowledge gained by thesestudies will assist us in the selection of other MAbs directedagainst CEA as well as other tumor markers for targeting ofcancer in patients.
ACKNOWLEDGMENTS
We thank F. James Primus, Ph.D., for his contributions and assistance in certain aspects of this project.
REFERENCES
1. Goldenberg, D. M. Current status of cancer imaging with radiolabeledantibodies. J. Cancer Res. Clin. Oncol., 113: 203-208. 1987.
2. Schlom, J. Basic principles and applications of monoclonal antibodies in themanagement of carcinomas. Cancer Res., 46: 3225-3238, 1986.
3. Goldenberg, D. M., Goldenberg, H.. Sharkey, R. M., Lee, R. E., Higgin-botham-Ford, E., Horowtiz, J. A., Hall, T. C, Pinsky, C. M., and Hansen,H. J. Imaging of colorectal cancer with radiolabeled antibodies. Semin. NucÃ.Med., 19: 262-281. 1989.
4. Goldenberg, D. M., DeLand, F. H., Kim, E., Bennett, S. J., Primus, F. J.,van Nagell, J. R., Jr., Estes, N., DeSimone, P.. and Rayburn, P. Use ofradiolabeled antibodies to carcinoembryonic antigen for the detection andlocalization of diverse cancers by external photoscanning. N. Engl. J. Med.,29«:1384-1388, 1978.
5. Goldenberg, D. M., Kim, E. E., Benne»,S. J.. Nelson, M. O., and Deland,F. H. Carcinoembryonic antigen radioimmunodetection in the evaluation ofcolorectal cancer and in the detection of occult neoplasms. Gastroenterology,84: 524-532, 1983.
6. Mach, J. P., Buchegger, F., Forni, M., Ritschard, J., Berche, C., Lumbroso,J. D., Schreyer, M., Girardet, C., Accolla, R. S., and Carrel, S. Use ofradiolabeled monoclonal anti-CEA antibodies for the detection of humancarcinomas by external photoscanning and tomoscintigraphy. Immunol. Today, 12: 239-249, 1981.
7. Carrasquillo, J. A., Sugarbaker. P.. Colcher, D., Reynolds, J. C., Esteban, J.,Bryan, G., Keenan, A. M.. Perentesis, P.. Yokoyama, K., Simpson. D. E.,Ferroni, P., Farkas, R., Schlom, J., and Larson, S. M. Radioimmunodetection of colon cancer with iodine-131-labeled B72.3 monoclonal antibody. J.NucÃ.Med., 29: 1022-1030, 1988.
8. Chatal, J. F., Thedrez. P., Blottiere, H., Kremer, M., Bianco-Arco, A.,Doullard, J. Y., Curtet. C.. Maurel, C., and LeMevel, B. Comparativecharacteristics of 17-1A and GA-733 monoclonal antibodies for immuno-scintigraphic application. Hybridoma. 5 (Suppl. 1): S87-S96, 1986.
9. Pimm, M. V., Embleton, M. J., Perkins, A. C., Price, M. R., Robins, R. A.,Robinson, G. R., and Baldwin, R. W. In vivo localization of anti-osteogenicsarcoma xenografts. Int. J. Cancer, 30: 75-85, 1982.
10. Chatal, J. F., Saccavini, J. C., Fumoleau, P.. Doullard, J-Y., Curtet, C.,Kremer, M., Le Mevel, B., and Koprowski, H. Immunoscintigraphy of coloncarcinoma. J. NucÃ.Med., 25: 307-314, 1984.
11. Primus, F. J., Newell, K. D., Blue, A., and Goldenberg, D. M. Immunologicalheterogenicity of carcinoembryonic antigen: antigenic determinants on carcinoembryonic antigen distinguished by monoclonal antibodies. Cancer Res.,«.-686-692,1983.
12. Primus, F. J., Kuhns, W. J., and Goldenberg, D. M. Immunological heterogeneity of carcinoembryonic antigen: ¡mmunohistochemical detection ofcarcinoembryonic antigen determinants in colonie tumors with monoclonalantibodies. Cancer Res.. «.-693-701. 1983.
13. Burtin, P., Chavane!, G., Hendrich, J. C., and Frenoy, N. Antigenic variantsof the nonspecific cross-reacting antigen (NCA). J. Immunol., 137:839-845,1986.
14. Primus, F. J., Freeman, J. W., and Goldenberg. D. M. Immunologicalheterogeneity of carcinoembryonic antigen: purification from meconium ofan antigen related to carcinoembryonic antigen. Cancer Res., 43: 679-685,1983.
15. Hansen, H. J., and Logerfo, P. Demonstrations of a tumor-associated antigenic site in carcinoembryonic antigen preparations. In: N. G. Anderson andJ. H. Coggin. Jr. (eds.). The First Conference and Workshops on Embryonic
and Fetal Antigens in Cancer, pp. 389-392. Oak Ridge, TN: Oak RidgeNational Laboratory. 1971.
16. Kupcik. H. Z., Hansen, H. J., Sorokin, J. J., and Zamcheck, N. Comparisonof radioimmunoassays for carcinoembryonic antigens. In: N. G. Anderson,J. H. Coggin, Jr., E. Cole, and J. W. Holleman (eds.). Proceedings of theSecond Conference and Workshop on Embryonic and Fetal Antigens inCancer, pp. 261-265. Oak Ridge, TN: Oak Ridge National Laboratory,1972.
17. Sharkey, R. M., Primus, F. J., Shochat, D., and Goldenberg, D. M. Comparison of tumor targeting of mouse monoclonal and goat polyclonal antibodies to carcinoembryonic antigen in the GW-39 human tumor-hamsterhost model. Cancer Res., 48: 1823-1828. 1988.
18. Greenwood, F., and Hunter, W. The preparation of I-131-labeled humangrowth hormone of high specific radioactivity. Biochem. J., 89: 114-123,1963.
19. Hoffman, T. Points to Consider in the Manufacture and Testing of Monoclonal Antibody Products for Human Use. Washington, DC: Office ofBiologies Research and Review Center for Drugs and Biologies. FDA. 1987.
20. DeJager, R. F.. Primus. F. J., Ford, E. H., Mahal, P. S., Bapat, A. R., Alger,E. A., and Goldenberg. D. M. Phase I clinical trial of radioimmunotherapywith 1-131 labeled anti-CEA or anti-AFP in solid tumors producing CEA orAFP. Proc. Am. Soc. Clin. Oncol., 4: 224, 1985.
21. Primus, F. J., Bennett, S. J., Kim, E. E., Deland, F. H., Zahn, M. C., andGoldenberg, D. M. Circulating immune complexes in cancer patients receiving goat radiolocalizing antibodies to carcinoembryonic antigen. Cancer Res.,Â¥0:497-501, 1980.
22. Primus. F. J., Kelley, E. A., Hansen, H. J., and Goldenberg, D. M. Sandwich-type immunoassay of carcinoembryonic antigen in patients receiving murinemonoclonal antibodies for diagnosis and therapy. Clin. Chem.. 34:261-264,1988.
23. Sokal, R. R., and Rohlf, F. J. (eds.). Biometry: The Principles and Practiceof Statistics in Biological Research. San Francisco. CA: W. H. Freeman andCo., 1969.
24. Goldenberg, D. M., Ford, E. H., Primus, F. J., Goldenberg. H., Alger, E. A.,and DeJager, R. L. Clinical evaluation of CEA monoclonal antibodies forcancer radioimmunodetection. Proc. Am. Assoc. Cancer Res., 27: 336, 1986.
25. Larson, S. M. A tentative biological model for the localization of radiolabeledantibody in tumor: the importance of immunoreactivity. NucÃ.Med. Biol.,13: 393-399, 1986.
26. Murray. J. L.. Lamki. L. M., Shanken, L. J.. Blake, M. E., Plager, C. E.,Benjamin, R. S., Schweighardt, S., Unger, M. W., and Rosenblum, M. G.Immunospecific saturable clearance mechanisms for indium-111 -labeled anti-melanoma monoclonal antibody 96.5 in humans. Cancer Res., 48: 4417-4422, 1988.
27. Hochschwender, S., Bartholomew, R., Sanchez, N., Vasquez, P., Wolfert,R., and Carlo, D. J. Immunoreactivity of the monoclonal antibody (MAb)96.5 against the p97 melanoma associated antigen is directly related toproduction of inactive variants. J. NucÃ.Med., 27: 958, 1986.
28. Patt. Y. Z., Lamki, L. M., Haynie, T. P., Unger, M. W.. Rosenblum, M. G.,Shirkhoda, A., and Murray, J. L. Improved tumor localization with increasing dose of indium-111 -labeled anti-carcinoembryonic antigen monoclonalantibody ZCE-025 in metastatic colorectal cancer. J. Clin. Oncol.. 6: 1220-1230, 1988.
29. Primus. F. J., Wang, R. H., Cohen, E., Hansen, H. J., and Goldenberg. D.M. Antibody to carcinoembryonic antigen in hamsters bearing GW-39 humantumors. Cancer Res., 26: 2176-2181. 1976.
30. Goldenberg. D. M., Primus, F. J., Ford, E. H., Brennan, K., and Goldenberg,H. Monoclonal antibodies to CEA: use in cancer radioimmunodetection. J.NucÃ.Med., 27: 897, 1986.
31. Haskell, C. M., Buchegger, F., Schreyer, M., Carrel, S., and Mach, J-P.Monoclonal antibodies to carcinoembryonic antigen: ion strength as a factorin selection of antibodies for immunoscintigraphy. Cancer Res., 43: 3857-3864, 1983.
32. Buchegger, F., Schreyer, M., Carrel, S., and Mach, J-P. Monoclonal antibodies identify a CEA cross-reacting antigen of 95 kD (NCA-95) distinct inantigenicity and tissue distribution from the previously described NCA of 55kD. Int. J. Cancer. 33:643-649, 1984.
33. Buchegger, F.. Haskell, C. M., Schreyer. M., Scazziga, B. R., Randiu, S.,Carrel, S., and Mach, J-P. Radiolabeled fragments of monoclonal antibodiesagainst carcinoembryonic antigen for localization of human colon carcinomagrafted into nude mice. J. Exp. Med., 158: 413-427. 1983.
34. Delaloye, B., Bischof-Delaloye, A.. Buchegger, F., von Flieder, V., Grob, J-P., Volan, J-C., Petteval, J., and Mach, J-P. Detection of colorectal carcinoma by emission-computerized tomography after injection of 123-I-labeledFab or F(ab)2 fragments from monoclonal anti-carcinoembryonic antigenantibodies. J. Clin. Invest.. 77: 301-311, 1986.
35. Beatty, J. D., Duda, R. B., Williams, L. E., Sheibani. K., Paxton, R. J.,Beatty, B. G., Philben, V. J., Werner, J. L., Shively, J. E., Vlahos, W. G.,Kokal, W. A., Riihimaki, D. U., Terz, J. J., and Wagmen, L. D. Preoperativeimaging of colorectal carcinoma with 111-In-labeled anticarcinoembryonicantigen monoclonal antibody. Cancer Res., 46: 6494-6502. 1986.
2831
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from
1990;50:2823-2831. Cancer Res Robert M. Sharkey, David M. Goldenberg, Hildegard Goldenberg, et al. Properties in HumansAntigen: Immunological, Pharmacokinetic, and Targeting Murine Monoclonal Antibodies against Carcinoembryonic
Updated version
http://cancerres.aacrjournals.org/content/50/9/2823
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/50/9/2823To request permission to re-use all or part of this article, use this link
on March 25, 2020. © 1990 American Association for Cancer Research.cancerres.aacrjournals.org Downloaded from


















