Multiple pregnancy
26
Multiple Pregnancy
-
Upload
rosetta-davis -
Category
Health & Medicine
-
view
898 -
download
1
description
All about multiple pregnancy : Twins
Transcript of Multiple pregnancy

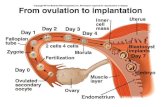
Multiple Pregnancy

When one or more fetus simultaneously develops in the
uterus, it is called multiple pregnancy.

TWINS

VARIETIES
• Dizygotic Twins (80%)
•Monozygotic Twins (20%)

Placenta Communicating Vessels
Intervening Membranes
Sex Genetic Features
Skin Grafting
Resemblance
Monozygotic One Present 2 amnions
Always identical
Same Acceptance Usually Identical
Dizygotic Two Absent 4 : 2 amnions,2 chorions
May differ
Differ Rejection Not identical

Monozygotic Dizygotic

The Cause of twinning is not known.
Dizygotic twin pregnancies are slightly more likely when the following factors are present in the woman:
•She is between the age of 30 and 40 years
•She is greater than average height and weight
•She has had several previous pregnancies.
•Women undergoing certain fertility treatments may have a greater chance of
dizygotic multiple births.
•The risk of twin birth can vary depending on what types of fertility treatments are
used. With in vitro fertilisation (IVF), this is primarily due to the insertion of multiple
embryos into the uterus.
•Ovarian hyperstimulation without IVF has a very high risk of multiple birth.
•Reversal of anovulation with clomifene has a relatively less but yet significant risk of
multiple pregnancy.
Predisposing factors


Maternal Physiological Changes
1. There is increase in weight gain
and cardiac output.
2. Plasma volume is increased by an
addition of 500ml.
3. There is no corresponding
increase in red cell volume
resulting in exaggerated
haemodilution and anaemia.
4. There is increased alpha
fetoprotein level, tidal volume
and glomerular filtration rate.

LIE AND PRESENTATION
Commonest lie is Longitudinal
Both Vertex (50%)
First Vertex and
second breech(30%)
First breech
and second vertex (10%)
Both Breech (10%)
Rarest oneBoth
transverse(Rule out conjoined
twins)

Diagnosis
History of ovulation inducing drugs.
Family history of Twinning
Minor ailments of normal
pregnancy are exaggerated
Abdominal examination
Internal examination

Abdominal Examination
More “barrel shaped” inspection
Abdominal girth more than 100cm.Too many fetal parts on palpation.
Two distinct fetal heart sounds on Auscultation.
Not easy due to presence
of hydramnios

Ultrasonography
Confirmation of pregnancy as early as 10th week of
pregnancy
Chorionicity
Presentation and Lie of the fetus
Viability of fetus
Fetal growth monitoring for IUGR
Fetal AnomaliesAmniotic fluid volume
Placental Localization
Twin transfusion

Lambda or twin peak sign
The sign describes the triangular appearance to chorion insinuating between the layers of the inter twin membrane and strongly suggests a dichorionic twin pregnancy. It is best seen in the first trimester (between 10-14 weeks).
In contrast the T sign refers to the appearance of the intertwin membrane in a monochorionic twin pregnancy. The sign should not be confused with the lambda sign of sarcoidosis.

A potential space exists in the intertwin
membrane, which is filled by proliferating placental villi giving rise to the twin peak
sign.

Differential Diagnosis
Hydramnios
Big Baby
Fibroid or ovarian tumour
with pregnancy.
Ascites with pregnancy

Complications
Maternal Fetal
Pregnancy
Labour
Puerperium

During Pregnancy
Anaemia
Pre-eclampsia (25%) Hydramnios
(10%)Antepartum Haemorrage
Malpresentation
Preterm Labour (50%) Mechanical
Distress

During Labour
Early Rupture of membranes and cord prolapse
Prolonged labour
Increased operative interference
Bleeding
Postpartum Haemorrhage

During Puerperium
Increased incidence of
Subinvolution.Infection.Lactation Failure.

Increased risk of miscarriage
Premature rate (80%)
Twin-twin transfusion syndrome
Placental insuffiency
IUGR
Structural anomalies
Intrauterine death of one fetus
Asphyxia and stillbirth

Management during Labour
What happens during a twin birth?
Most twins are born before 38 weeks. If you haven't gone into labour by then, you may be recommended to have your labour induced.
During labour, regular monitoring of your twins with electronic fetal monitors (EFM) is standard practice. This is used to listen to your babies' heartbeats and the intensity and frequency of your contractions. Your doctor may place a needle in a vein in your arm (a drip) in case it is needed later.
Discuss your pain relief preferences with your midwife during pregnancy and write them in your birth plan. But keep in mind that labour and birth are unpredictable. Your midwife may need to recommend a course of action at any time which is not what you had originally hoped for, but which will always be in the best interests of you and your baby.

Once your first baby is born, your midwife or doctor will check the position of your second twin by feeling your tummy and doing a vaginal examination, or an ultrasound scan.
If your second baby is in a good position to be born, the waters surrounding him will be broken. Your second baby should be born very soon after the first, because your cervix is already fully dilated. If your contractions stop after your first twin is born, hormones are added to the drip to restart them.
You'll usually be recommended to have a managed third stage. This is when the placenta is delivered with the help of a hormone injection, instead of a natural delivery. This is because there is an increased risk of bleeding when the placenta is larger, and the uterus (womb) will have been stretched by two babies.

Triplets Quadruplets
Female usually outnumber the number of male one. Perinatal loss is markedly increased due to prematurity.
Average time for delivery in quadruplets is 30-31 weeks.
Selective reduction: If there are 4 or more fetuses, selective reduction of the fetuses leaving behind only two is done to improve the outcome. This can be done by intracardiac injection of potassium chloride between 11-13 weeks.
Selective termination of a fetus with structural or genetic abnormalities may be done in a chorionic multiple pregnancy in the second trimester.


Thank
you…